
Precordial Vibrations: A Review of Wearable Systems, Signal Processing Techniques, and Main Applications

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction and Physiological Sources of Displacement Cardiography
- Isovolumetric ventricular contraction: at first, isovolumetric ventricular contraction causes ventricular pressure to rise above atrial pressure, forcing the atrioventricular (AV) valves to close. The continuing contraction with the valves closed increases ventricular pressure.
- Ventricular ejection: occurs when ventricular pressure rises above arterial pressure and the semilunar valves open. As blood is ejected into the arteries, ventricular volume decreases, and ventricles begin to repolarize and relax. Ventricular pressure decreases and contraction ends.
- Isovolumetric ventricular relaxation: repolarization of the ventricular muscle cells initiates isovolumetric ventricular relaxation. As the ventricles relax, pressure in the ventricles drops and the semilunar valves close, preventing blood reflux. Valve closure produces a dicrotic wave on the aortic pressure curve. This isovolumetric relaxation makes pressure drop quickly.
- Passive ventricular filling: as all four chambers of the heart are relaxed and the AV valves open, passive ventricular filling starts. Atrial depolarization triggers atrial contraction and a new cardiac cycle begins.
2. Precordial Vibrations Recording Using Accelerometers
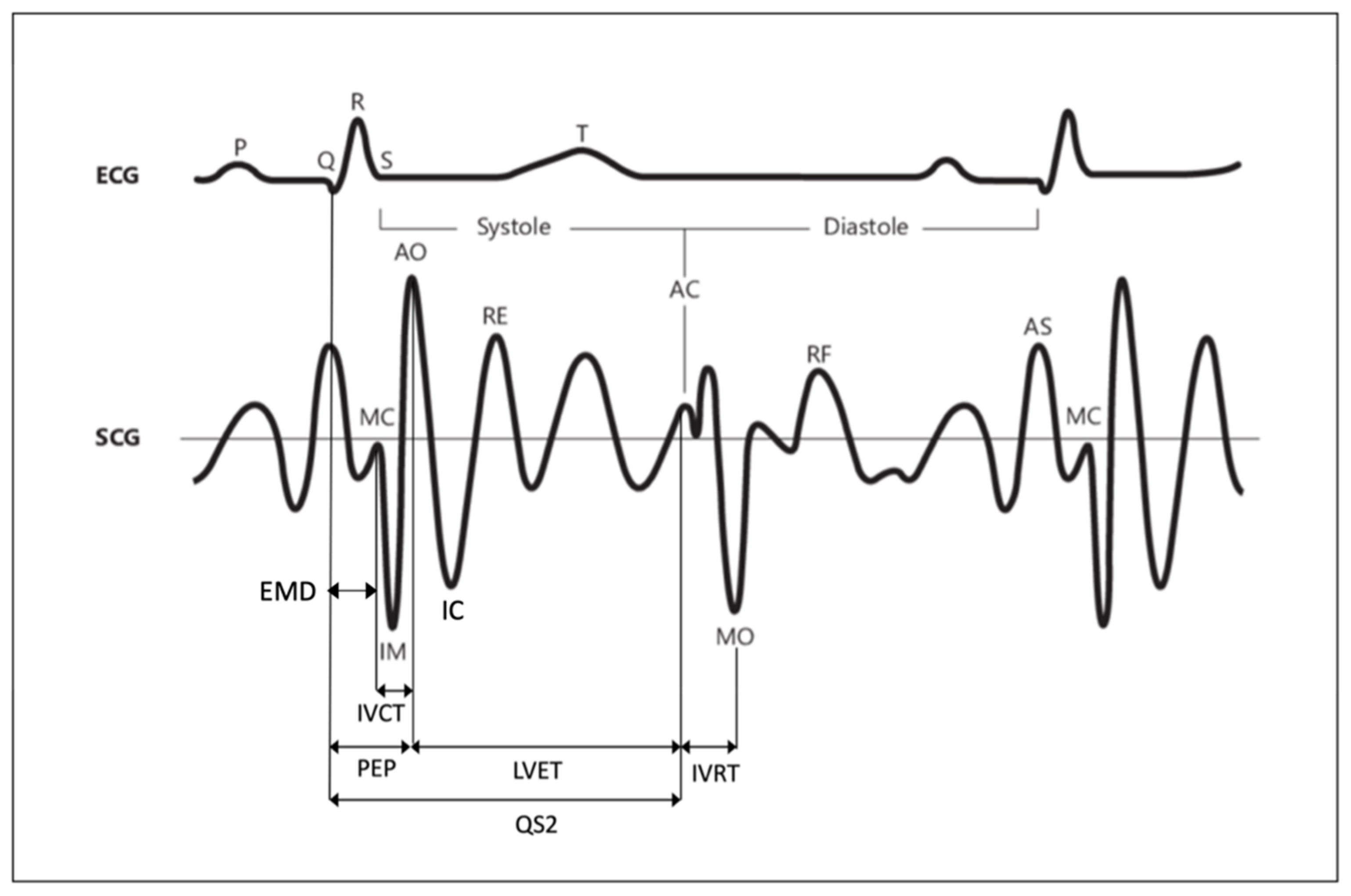
2.1. SCG Signal
- The pre-ejection period (PEP), which is the time interval between electrical depolarization of the left ventricle (QRS on the ECG) and the onset of ventricular ejection;
- The left-ventricular period (LVET), defined as the time interval between the opening and closing of the aortic valve. It is the phase of systole during which the left ventricle ejects blood into the aorta;
- The QS2, which is the time period between the onset of the QRS complex and the first aortic vibration of the second heart sound. The sum of PEP and LVET gives the total time of electromechanical systole.
- The electromechanical delay (EMD), which is the interval between the ECG Q wave and the closure of mitral valve.
- The isovolumic relaxation time (IVRT), defined as the time interval between the end of aortic ejection and the beginning of ventricular filling.
- The isovolumic contraction time (IVCT), which is the interval between the closing of the atrioventricular valves and the opening of the semilunar valves.
- The pulse transit time (PTT), which is the time required for the travel of the blood pressure wave from one location to another. As PTT is inversely proportional to the blood pressure value, its evaluation is considered a promising method for continuous, noninvasive, and cuffless blood pressure monitoring. The most common type of PTT that can effectively estimate blood pressure is the time delay between a proximal-location pressure wave and a distal arterial-location pressure wave. This metric is called aortic PTT.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fiducial Point | Physiological Event |
|---|---|
| Aortic valve opening (AO) | Aortic valve passively opens because of pressure differences on either side of the valve and allows the ejection of blood into the vascular tree |
| Isovolumic contraction (IC) | Event occurring in early systole during which the ventricles contract with no corresponding volume change |
| Peak of rapid systolic ejection (RE) | Rapid ejection of blood into the aorta and pulmonary arteries from the left and right ventricles, respectively |
| Aortic valve closure (AC) | Closure of the aortic valve at two-thirds of ejection |
| Mitral valve opening (MO) | Mitral valve opening when the left ventricle relaxes |
| Peak of rapid diastolic filling (RF) | The period in which the ventricle fills with blood from the left atrium from the onset of mitral valve opening to mitral valve closure |
| Peak of atrial systole (AS) | Peak of arterial blood pressure during systole, normally from 90 mmHg to 120 mmHg |
| Mitral valve closure (MC) | Mitral valve closure in correspondence with the left-ventricle contraction |
| Isovolumic movement (IM) | Ventricular isovolumetric contraction |
2.2. SCG Signal Collection and Analysis
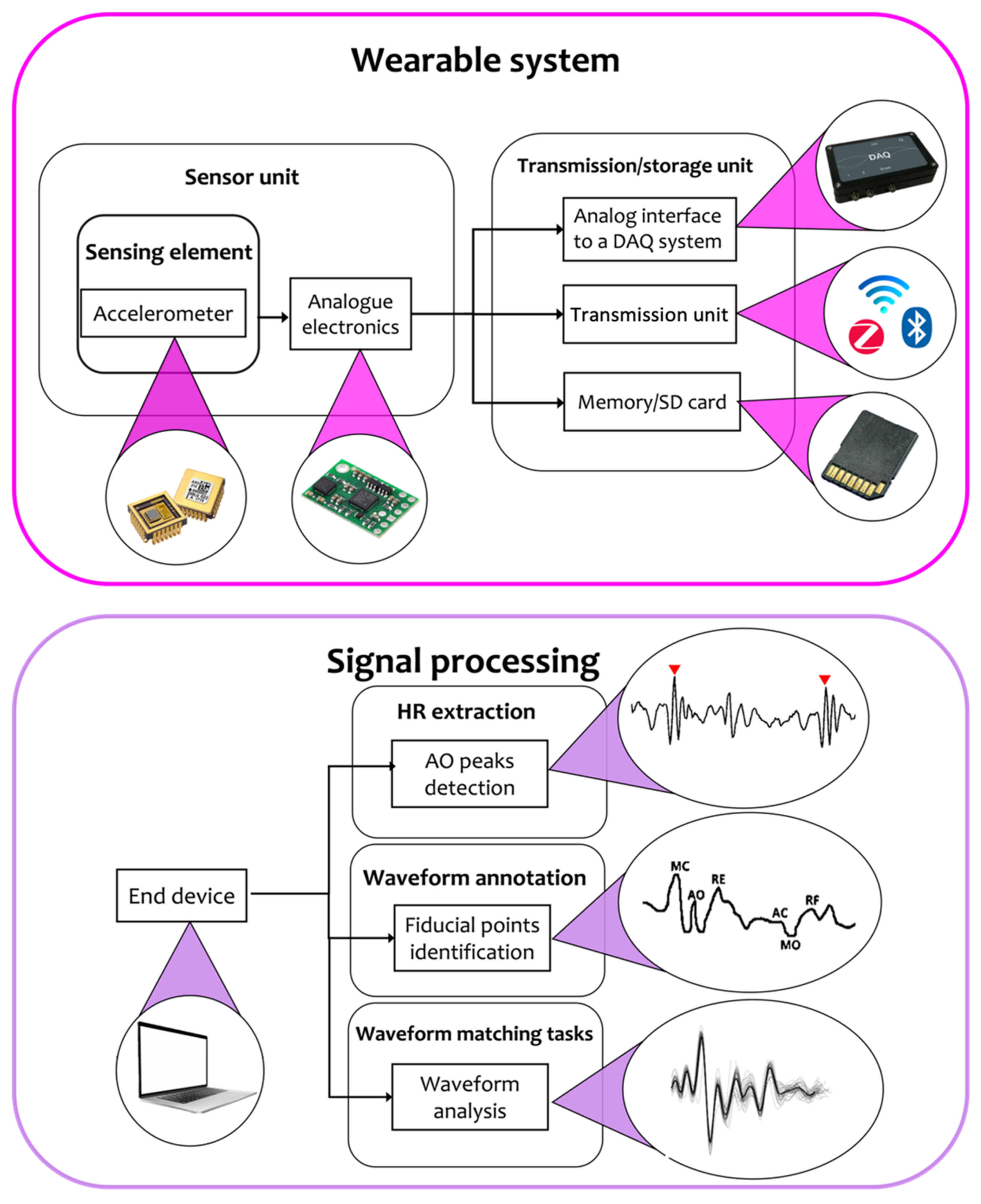
2.2.1. Wearable Systems for SCG Monitoring
2.2.2. Signal Processing
2.2.3. Experimental Setup and Application Scenarios
3. Precordial Vibration Recording Using Gyroscopes
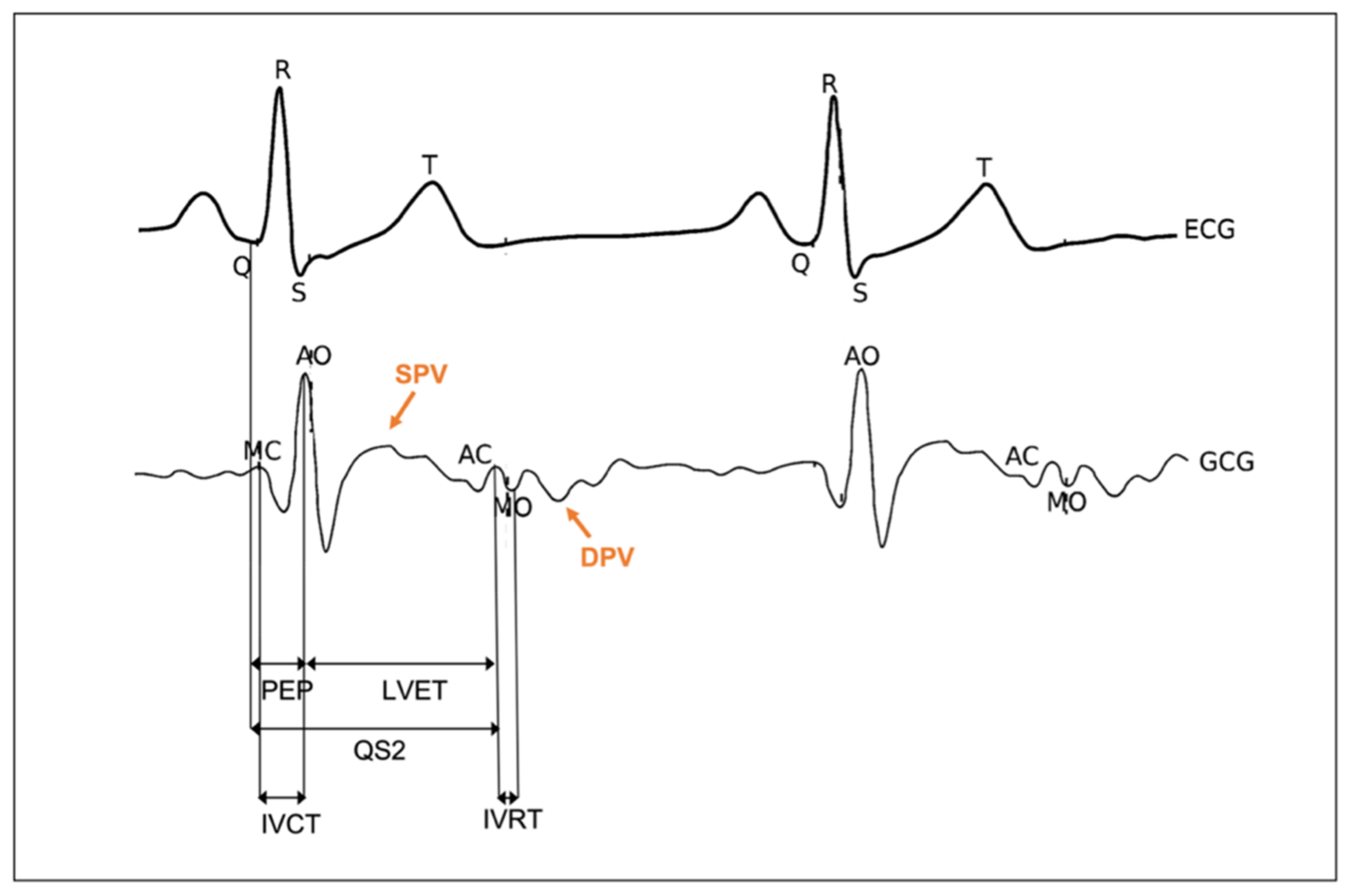
3.1. GCG Signal
3.2. GCG Signal Collection and Analysis
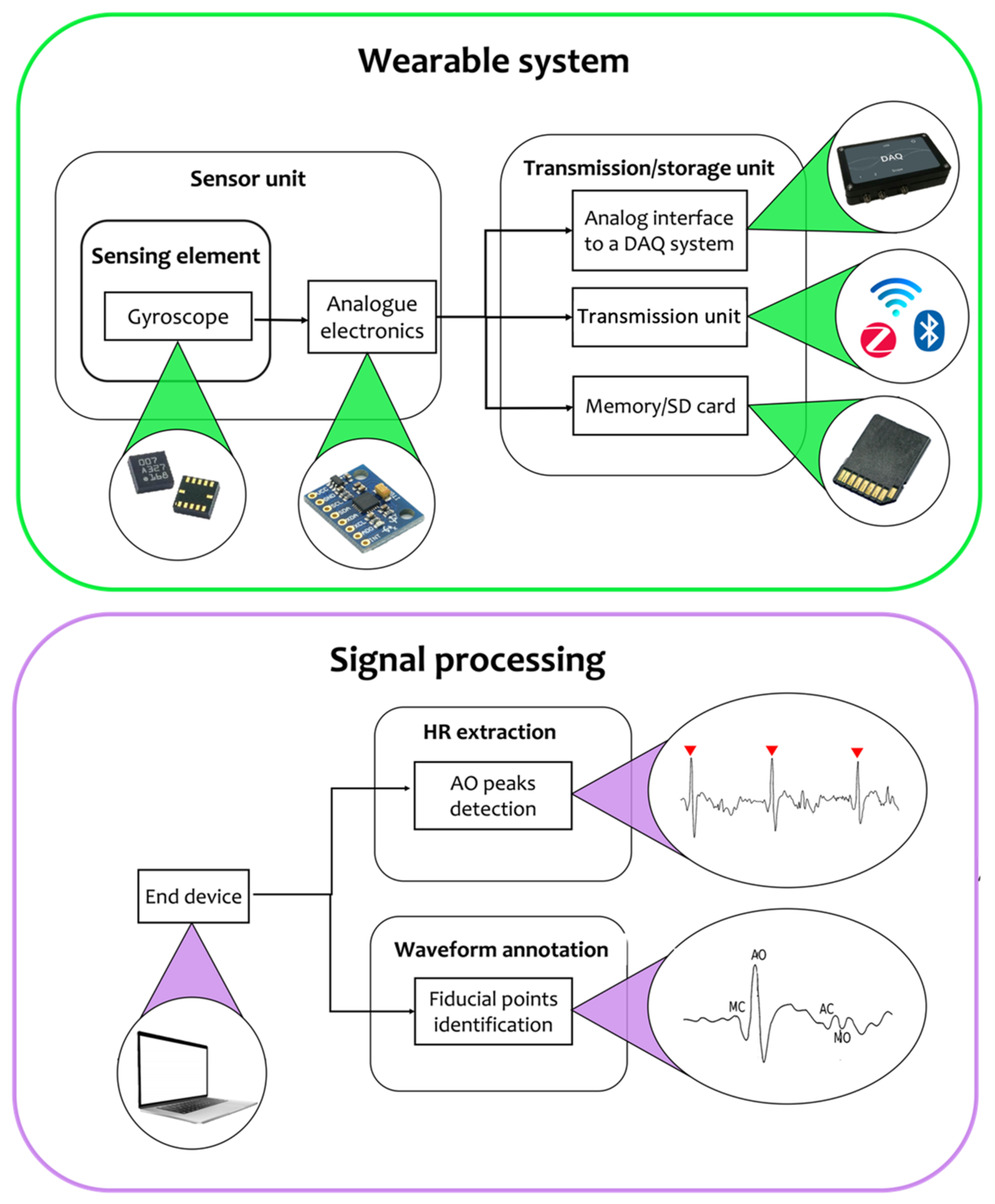
3.2.1. Wearable Systems for GCG Monitoring
- Angle random walk (ARW), which describes the error resulting from broadband white noise, which is caused in MEMS devices by detection electronics.
- Bias offset error, which is the nonzero output of the gyroscope when the input rotation is null. This static error is typically 25 °C for an ideal environment, and it can be easily corrected.
- Bias instability, which is the instability of the bias offset at constant temperature and in an ideal environment. It introduces a dynamic error difficult to compensate for, and it strongly affects sensor accuracy over a long time.
- Temperature sensitivity, which defines performance changes over temperature changes.
- Shock and vibration sensitivity, which denotes the degradation in performance caused by vibration and shock inputs.
3.2.2. Signal Processing
3.2.3. Application Scenarios and Influencing Factors
4. Precordial Vibrations Recording Using Fiber Bragg Grating Sensors
4.1. Strain-Derived SCG Signal
4.2. Strain-Derived SCG Signal Collection and Analysis
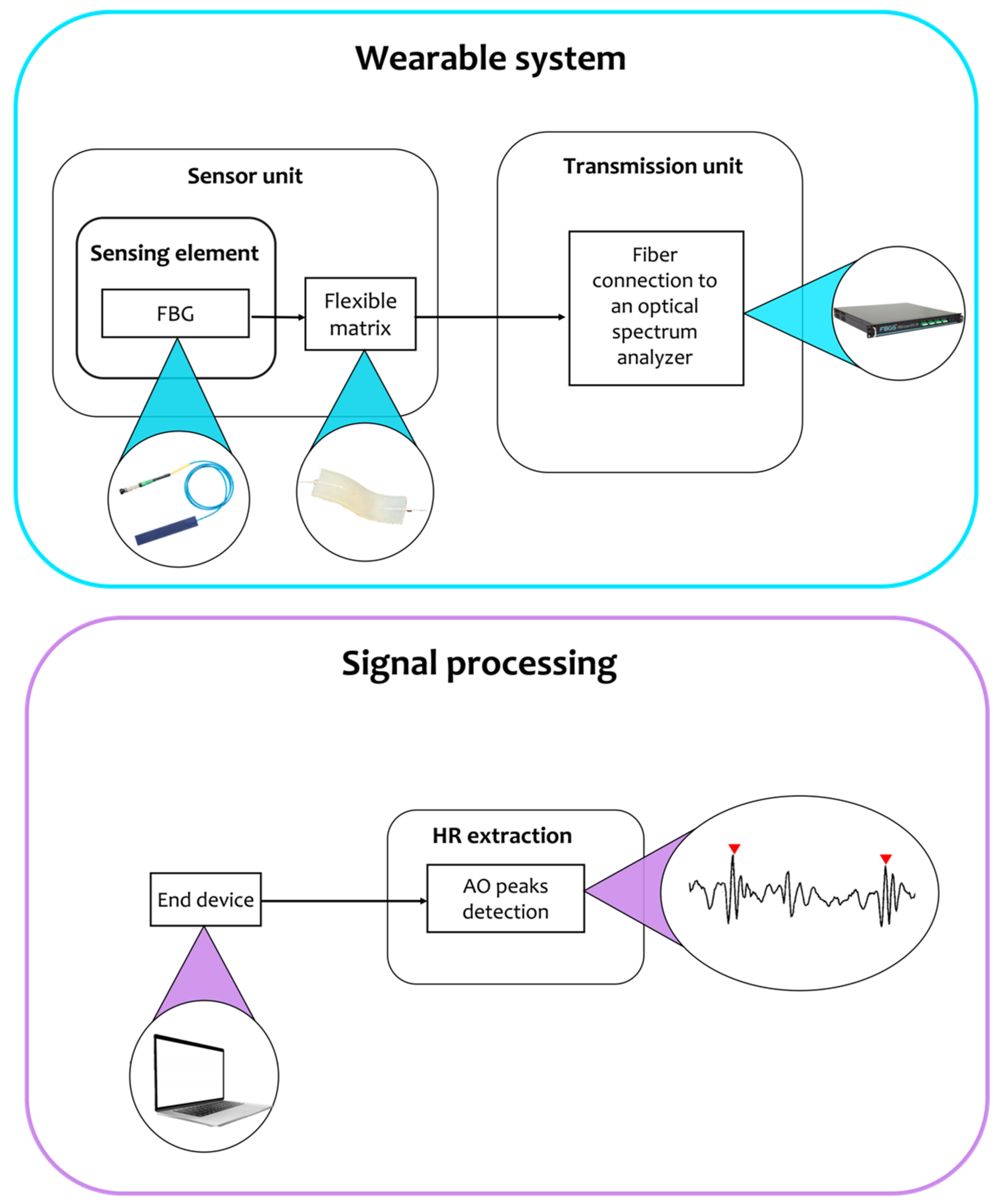
4.2.1. Wearable Systems for Strain-Derived SCG Monitoring Using FBGs
4.2.2. Signal Processing
4.2.3. Application Scenarios and Influencing Factors
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Mensah, G.A.; Roth, G.A.; Fuster, V. The Global Burden of Cardiovascular Diseases and Risk Factors: 2020 and Beyond. J. Am. Coll. Cardiol. 2019, 74, 2529–2532. [Google Scholar] [CrossRef] [PubMed]
- Adamson, P.B.; Magalski, A.; Braunschweig, F.; Böhm, M.; Reynolds, D.; Steinhaus, D.; Luby, A.; Linde, C.; Ryden, L.; Cremers, B.; et al. Ongoing right ventricular hemodynamics in heart failure: Clinical value of measurements derived from an implantable monitoring system. J. Am. Coll. Cardiol. 2003, 41, 565–571. [Google Scholar] [CrossRef] [Green Version]
- Ping, N.C. Mechanisms Underlying Isovolumic Contraction and Ejection Peaks in Seismocardiogram Morphology. Bone 2013, 23, 103–110. [Google Scholar]
- Presti, D.L.; Massaroni, C.; Leitao, C.S.J.; Domingues, M.D.F.; Sypabekova, M.; Barrera, D.; Floris, I.; Massari, L.; Oddo, C.M.; Sales, S.; et al. Fiber Bragg Gratings for Medical Applications and Future Challenges: A Review. IEEE Access 2020, 8, 156863–156888. [Google Scholar] [CrossRef]
- Nogata, F.; Yokota, Y.; Kawamura, Y.; Professor, E. Distribution of Vibration of Chest Surface with Heart Movement. Front. Sens. 2014, 2, 26–31. Available online: www.seipub.org/fs (accessed on 17 March 2022).
- Massaroni, C.; Zaltieri, M.; Presti, D.L.; Nicolo, A.; Tosi, D.; Schena, E. Fiber Bragg Grating Sensors for Cardiorespiratory Monitoring: A Review. IEEE Sensors J. 2020, 21, 14069–14080. [Google Scholar] [CrossRef]
- Rai, D.; Thakkar, H.K.; Rajput, S.S.; Santamaria, J.; Bhatt, C.; Roca, F. A Comprehensive Review on Seismocardiogram: Current Advancements on Acquisition, Annotation, and Applications. Mathematics 2021, 9, 2243. [Google Scholar] [CrossRef]
- Sieciński, S.; Kostka, P.S.; Tkacz, E.J. Gyrocardiography: A Review of the Definition, History, Waveform Description, and Applications. Sensors 2020, 20, 6675. [Google Scholar] [CrossRef]
- Salerno, D.M.; Zanetti, J. Seismocardiography for Monitoring Changes in Left Ventricular Function during Ischemia. Chest 1991, 100, 991–993. [Google Scholar] [CrossRef] [Green Version]
- D’Mello, Y.; Skoric, J.; Xu, S.; Roche, P.J.R.; Lortie, M.; Gagnon, S.; Plant, D.V. Real-Time Cardiac Beat Detection and Heart Rate Monitoring from Combined Seismocardiography and Gyrocardiography. Sensors 2019, 19, 3472. [Google Scholar] [CrossRef] [Green Version]
- Nedoma, J.; Kepak, S.; Fajkus, M.; Cubik, J.; Siska, P.; Martinek, R.; Krupa, P. Magnetic Resonance Imaging Compatible Non-Invasive Fibre-Optic Sensors Based on the Bragg Gratings and Interferometers in the Application of Monitoring Heart and Respiration Rate of the Human Body: A Comparative Study. Sensors 2018, 18, 3713. [Google Scholar] [CrossRef] [Green Version]
- Grainger, D. Safety Guidelines for Magnetic Resonance Imaging Equipment in Clinical Use; Medicines and Healthcare Products Regulatory Agency: London, UK, 2021; pp. 1–86. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/958486/MRI_guidance_2021-4-03c.pdf (accessed on 22 March 2022).
- Paukkunen, M.; Parkkila, P.; Hurnanen, T.; Pankaala, M.; Koivisto, T.; Nieminen, T.; Kettunen, R.; Sepponen, R. Beat-by-Beat Quantification of Cardiac Cycle Events Detected from Three-Dimensional Precordial Acceleration Signals. IEEE J. Biomed. Health Inform. 2016, 20, 435–439. [Google Scholar] [CrossRef] [Green Version]
- Baevskii, L.A.; Egorov, R.M.; Kazarian, A.D. The method of Seismocardiography. Kardiologiia 1964, 18, 87–89. [Google Scholar]
- Dăuş, L.; Beiu, V. Lower and Upper Reliability Bounds for Consecutive-k-Out-of-n:F Systems. IEEE Trans. Reliab. 2015, 64, 1128–1135. [Google Scholar] [CrossRef]
- Taebi, A.; Mansy, H.A. Grouping similar seismocardiographic signals using respiratory information. In Proceedings of the 2017 IEEE Signal Processing in Medicine and Biology Symposium (SPMB), Philadelphia, PA, USA, 2 December 2017; pp. 1–6. [Google Scholar] [CrossRef] [Green Version]
- Johnson, E.M.I.; Heller, J.A.; Vicente, F.G.; Sarnari, R.; Gordon, D.; McCarthy, P.M.; Barker, A.J.; Etemadi, M.; Markl, M. Detecting Aortic Valve-Induced Abnormal Flow with Seismocardiography and Cardiac MRI. Ann. Biomed. Eng. 2020, 48, 1779–1792. [Google Scholar] [CrossRef]
- Chuo, Y.; Tavakolian, K.; Kamińska, B. Evaluation of a Novel Integrated Sensor System for Synchronous Measurement of Cardiac Vibrations and Cardiac Potentials. J. Med. Syst. 2011, 35, 445–455. [Google Scholar] [CrossRef]
- Johnson, E.M.I.; Etemadi, M.; Malaisrie, S.C.; McCarthy, P.M.; Markl, M.; Barker, A.J. Seismocardiography and 4D flow MRI reveal impact of aortic valve replacement on chest acceleration and aortic hemodynamics. J. Card. Surg. 2020, 35, 232–235. [Google Scholar] [CrossRef]
- Morra, S.; Pitisci, L.; Su, F.; Hossein, A.; Rabineau, J.; Racape, J.; Gorlier, D.; Herpain, A.; Migeotte, P.F.; Creteur, J. Quantification of Cardiac Kinetic Energy and Its Changes During Transmural Myocardial Infarction Assessed by Multi-Dimensional Seismocardiography. Front. Cardiovasc. Med. 2021, 8, 603319. [Google Scholar] [CrossRef]
- Inan, O.T.; Pouyan, M.B.; Javaid, A.Q.; Dowling, S.; Etemadi, M.; Dorier, A.; Heller, J.A.; Bicen, A.O.; Roy, S.; De Marco, T.; et al. Novel Wearable Seismocardiography and Machine Learning Algorithms Can Assess Clinical Status of Heart Failure Patients. Circ. Heart Fail. 2018, 11, e004313. [Google Scholar] [CrossRef]
- Shafiq, G.; Tatinati, S.; Ang, W.T.; Veluvolu, K.C. Automatic Identification of Systolic Time Intervals in Seismocardiogram. Sci. Rep. 2016, 6, 37524. [Google Scholar] [CrossRef] [Green Version]
- Tadi, M.J.; Koivisto, T.; Pänkäälä, M.; Paasio, A.; Knuutila, T.; Teräs, M.; Hänninen, P. A new algorithm for segmentation of cardiac quiescent phases and cardiac time intervals using seismocardiography. In Proceedings of the Sixth International Conference on Graphic and Image Processing (ICGIP 2014), Beijing, China, 24–26 October 2015; Volume 9443, p. 94432K. [Google Scholar] [CrossRef]
- Lewis, R.P.; Rittgers, S.E.; Forester, W.F.; Boudoulas, H. A Critical Review of the Systolic Time Intervals. Circulation 1977, 56, 146–158. [Google Scholar] [CrossRef] [Green Version]
- Tavakolian, K.; Blaber, A.P.; Akhbardeh, A.; Ngai, B.; Kaminska, B. Estimating Cardiac Stroke Volume from the Seismocardiogram Signal. CMBES Proc. 2010, 33. [Google Scholar]
- Tavakolian, K.; Blaber, A.P.; Ngai, B.; Kaminska, B. Estimation of hemodynamic parameters from seismocardiogram. Comput. Cardiol. 2010, 37, 1055–1058. [Google Scholar]
- Tavakolian, K.; Ngai, B.; Akhbardeh, A.; Kaminska, B.; Blaber, A. Comparative analysis of infrasonic cardiac signals. Comput. Cardiol. 2009, 36, 757–760. [Google Scholar]
- Wilson, R.A.; Bamrah, V.S.; Lindsay, J.; Schwaiger, M.; Morganroth, J. Diagnostic accuracy of seismocardiography compared with electrocardiography for the anatomic and physiologic diagnosis of coronary artery disease during exercise testing. Am. J. Cardiol. 1993, 71, 536–545. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Ha, B.; Lee, S. Micromachined inertial sensors. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems. Human and Environment Friendly Robots with High Intelligence and Emotional Quotients (Cat. No. 99CH36289), Kyongju, Korea, 17 October 1999; pp. 1049–1056. [Google Scholar] [CrossRef]
- Narasimhan, V.; Li, H.; Jianmin, M. Micromachined high-g accelerometers: A review. J. Micromechanics Microengineering 2015, 25, 033001. [Google Scholar] [CrossRef]
- Elies, S. Sensors & Transducers Performance Analysis of Commercial Accelerometers: A Parameter Review. Sens. Transducers 2015, 193, 179–190. Available online: http://www.sensorsportal.com (accessed on 15 May 2022).
- Benmessaoud, M.; Nasreddine, M.M. Optimization of MEMS capacitive accelerometer. Microsyst. Technol. 2013, 19, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Gomathi, T.; Shaby, S.M. Capacitive accelerometers for microelectromechanical applications: A review. In Proceedings of the IEEE International Conference on Control, Instrumentation, Communication and Computational Technologies (ICCICCT), Kumaracoil, India, 16–17 December 2016; pp. 486–490. [Google Scholar] [CrossRef]
- De Reus, R.; Gulløv, J.O.; Scheeper, P.R. Fabrication and characterization of a piezoelectric accelerometer. J. Micromechanics Microengineering 1999, 9, 123–126. [Google Scholar] [CrossRef]
- Naduvinamani, S.; Iyer, N.C. Design and simulation of PZT based MEMS piezoelectric accelerometer. In Proceedings of the IEEE International Conference on Electrical, Electronics, and Optimization Techniques (ICEEOT), Chennai, India, 3 March 2016; pp. 3715–3721. [Google Scholar] [CrossRef]
- Han, R.-H.; Wang, J.-Y.; Xu, M.-H.; Guo, H. Design of a tri-axial micro piezoelectric accelerometer. In Proceedings of the 2016 Symposium on Piezoelectricity, Acoustic Waves, and Device Applications (SPAWDA), Xi’an, China, 21–24 October 2016; pp. 66–70. [Google Scholar] [CrossRef]
- Laine, J.; Mougenot, D. A high-sensitivity MEMS-based accelerometer. Lead. Edge 2014, 33, 1234–1242. [Google Scholar] [CrossRef] [Green Version]
- Khosrow-Khavar, F.; Tavakolian, K.; Menon, C. Moving toward automatic and standalone delineation of seismocardiogram signal. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 7163–7166. [Google Scholar] [CrossRef]
- Khosrow-Khavar, F.; Tavakolian, K.; Blaber, A.; Menon, C. Automatic and Robust Delineation of the Fiducial Points of the Seismocardiogram Signal for Noninvasive Estimation of Cardiac Time Intervals. IEEE Trans. Biomed. Eng. 2017, 64, 1701–1710. [Google Scholar] [CrossRef]
- Sørensen, K.; Schmidt, S.E.; Jensen, A.S.; Søgaard, P.; Struijk, J. Definition of Fiducial Points in the Normal Seismocardiogram. Sci. Rep. 2018, 8, 15455. [Google Scholar] [CrossRef] [Green Version]
- Khosrow-Khavar, F.; Tavakolian, K.; Blaber, A.P.; Zanetti, J.M.; Fazel-Rezai, R.; Menon, C. Automatic Annotation of Seismocardiogram with High-Frequency Precordial Accelerations. IEEE J. Biomed. Health Inform. 2015, 19, 1428–1434. [Google Scholar] [CrossRef] [PubMed]
- Gamage, P.T.; Azad, K.; Taebi, A.; Sandler, R.H.; Mansy, H.A. Clustering Seismocardiographic Events using Unsupervised Machine Learning. In Proceedings of the IEEE Signal Processing in Medicine and Biology Symposium (SPMB), Philadelphia, PA, USA, 1 December 2018; pp. 1–5. [Google Scholar] [CrossRef]
- Taebi, A.; Solar, B.E.; Mansy, H.A. An Adaptive Feature Extraction Algorithm for Classification of Seismocardiographic Signals. In Proceedings of the IEEE SoutheastCon, St. Petersburg, FL, USA, 19–22 April 2018; pp. 1–5. [Google Scholar] [CrossRef] [Green Version]
- Mora, N.; Cocconcelli, F.; Matrella, G.; Ciampolini, P. A Unified Methodology for Heartbeats Detection in Seismocardiogram and Ballistocardiogram Signals. Computers 2020, 9, 41. [Google Scholar] [CrossRef]
- Choudhary, T.; Bhuyan, M.K.; Sharma, L.N. A Novel Method for Aortic Valve Opening Phase Detection Using SCG Signal. IEEE Sens. J. 2020, 20, 899–908. [Google Scholar] [CrossRef]
- Hsu, P.-Y.; Lee, T.-H.; Liu, H.-L. Heart Rate and Respiratory Rate Monitoring Using Seismocardiography. In Proceedings of the 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 6876–6879. [Google Scholar] [CrossRef]
- Ramos-Castro, J.; Moreno, J.; Miranda-Vidal, H.; Garcia-Gonzalez, M.A.; Fernández-Chimeno, M.; Rodas, G.; Capdevila, L. Heart rate variability analysis using a seismocardiogram signal. In Proceedings of the 34th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August 2012–1 September 2012; pp. 5642–5645. [Google Scholar] [CrossRef]
- Tipo 4381|Brüel & Kjær. Available online: https://www.bksv.com/it/transducers/vibration/accelerometers/charge/4381 (accessed on 29 June 2022).
- Pcb Piezoelectronics. Available online: https://www.pcb.com/products?m=356A32, (accessed on 29 June 2022).
- Lin, W.-Y.; Tsai, T.-H.; Lee, M.-Y.; Chou, W.-C.; Chang, P.-C.; Chou, C.-C.; Wen, M.-S.; Ho, M.-Y.; Lee, W.-C.; Hsieh, M.-J.; et al. Identification of Location Specific Feature Points in a Cardiac Cycle Using a Novel Seismocardiogram Spectrum System. IEEE J. Biomed. Health Inform. 2018, 22, 442–449. [Google Scholar] [CrossRef]
- Choudhary, T.; Bhuyan, M.K.; Sharma, L.N. Delineation and Analysis of Seismocardiographic Systole and Diastole Profiles. IEEE Trans. Instrum. Meas. 2020, 70, 1–8. [Google Scholar] [CrossRef]
- Dinh, A.; Choi, Y.; Ko, S.B. A heart rate sensor based on seismocardiography for vital sign monitoring systems. In Proceedings of the 24th Canadian Conference on Electrical and Computer Engineering (CCECE), Niagara Falls, ON, Canada, 8–11 May 2011; pp. 000665–000668. [Google Scholar]
- LIS331DLH—3-axis Digital Accelerometer, Ultra Low Power Operational Modes, Advanced Power Saving, Smart Sleep to Wake-Up Functions—Stmicroelectronics. Available online: https://www.st.com/en/mems-and-sensors/lis331dlh.html (accessed on 30 April 2022).
- Shafiq, G.; Tatinati, S.; Veluvolu, K.C. Automatic annotation of peaks in seismocardiogram for systolic time intervals. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 2672–2675. [Google Scholar] [CrossRef]
- Wick, C.A.; Su, J.-J.; McClellan, J.H.; Brand, O.; Bhatti, P.T.; Buice, A.L.; Stillman, A.E.; Tang, X.; Tridandapani, S. A System for Seismocardiography-Based Identification of Quiescent Heart Phases: Implications for Cardiac Imaging. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 869–877. [Google Scholar] [CrossRef]
- Tadi, M.J.; Lehtonen, E.; Koivisto, T.; Pankaala, M.; Paasio, A.; Teras, M. Seismocardiography: Toward heart rate variability (HRV) estimation. In Proceedings of the 37th IEEE International Symposium on Medical Measurements and Applications (MeMeA), Turin, Italy, 7–9 May 2015; pp. 261–266. [Google Scholar] [CrossRef]
- Lin, Y.-D.; Jhou, Y.-F. Estimation of heart rate and respiratory rate from the seismocardiogram under resting state. Biomed. Signal Process. Control 2020, 57, 101779. [Google Scholar] [CrossRef]
- Hsu, P.-Y.; Liu, H.-L. Exploring seismocardiogram biometrics with wavelet transform. In Proceedings of the 25th International Conference on Pattern Recognition (ICPR), Milan, Italy, 10–15 January 2021; pp. 4450–4457. [Google Scholar] [CrossRef]
- Zia, J.; Kimball, J.; Shandhi, M.H.; Inan, O.T. Automated identification of persistent time-domain features in seismocardiogram signals. In Proceedings of the IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Chicago, IL, USA, 19–22 May 2019. [Google Scholar] [CrossRef]
- Garcia-Gonzalez, M.A.; Argelagos-Palau, A.; Fernandez-Chimeno, M.; Ramos-Castro, J. A comparison of heartbeat detectors for the seismocardiogram. Comput. Cardiol. 2013, 40, 461–464. [Google Scholar]
- Pandia, K.; Ravindran, S.; Cole, R.; Kovacs, G.; Giovangrandi, L. Motion artifact cancellation to obtain heart sounds from a single chest-worn accelerometer. In Proceedings of the IEEE International Conference on Acoustics, Speech and Signal Processing, Dallas, TX, USA, 14–19 March 2010; pp. 590–593. [Google Scholar] [CrossRef]
- Yang, C.; Tavassolian, N. Combined Seismo- and Gyro-Cardiography: A More Comprehensive Evaluation of Heart-Induced Chest Vibrations. IEEE J. Biomed. Health Inform. 2018, 22, 1466–1475. [Google Scholar] [CrossRef]
- Choudhary, T.; Das, M.; Sharma, L.; Bhuyan, M. Analyzing seismocardiographic approach for heart rate variability measurement. Biomed. Signal Process. Control 2021, 68, 102793. [Google Scholar] [CrossRef]
- Chen, C. The Applications of K-means Clustering and Dynamic Time Warping Average in Seismocardiography Template Generation. In Proceedings of the IEEE International Conference on Systems, Man, and Cybernetics (SMC), Toronto, ON, Canada, 11–14 October 2020; pp. 1000–1007. [Google Scholar]
- Shandhi, M.H.; Fan, J.; Heller, J.A.; Etemadi, M.; Klein, L.; Inan, O.T. Estimation of Changes in Intracardiac Hemodynamics Using Wearable Seismocardiography and Machine Learning in Patients with Heart Failure: A Feasibility Study. IEEE Trans. Biomed. Eng. 2022, 69, 2443–2455. [Google Scholar] [CrossRef]
- Elnaggar, I.; Hurnanen, T.; Lahdenoja, O.; Airola, A.; Kaisti, M.; Vasankari, T.; Pykari, J.; Savontaus, M.; Koivisto, T. Detecting Aortic Stenosis Using Seismocardiography and Gryocardiography Combined with Convolutional Neural Networks. Comput. Cardiol. 2021, 48, 2–5. [Google Scholar] [CrossRef]
- López-Rico, O.Y.; Ramírez-Chavarría, R.G. Smart Seismocardiography: A Machine Learning Approach for Automatic Data Processing. Eng. Proc. 2021, 10, 24. [Google Scholar] [CrossRef]
- Choudhary, T.; Sharma, L.N.; Bhuyan, M.K. Automatic Detection of Aortic Valve Opening Using Seismocardiography in Healthy Individuals. IEEE J. Biomed. Health Inform. 2018, 23, 1032–1040. [Google Scholar] [CrossRef]
- Combined Measurement of ECG, Breathing and Seismocardiogram (CEBS Database). 2013. Available online: https://archive.physionet.org/physiobank/database/cebsdb/ (accessed on 19 May 2022).
- Casanella, R.; Khosrow-Khavar, F.; Schmidt, S.; Zanetti, J.; Tavakolian, K. Cardiac Mechanical Signals; Springer: Singapore, 2019. [Google Scholar]
- Tadi, M.J.; Lehtonen, E.; Saraste, A.; Tuominen, J.; Koskinen, J.; Teräs, M.; Airaksinen, J.; Pänkäälä, M.; Koivisto, T. Gyrocardiography: A New Non-invasive Monitoring Method for the Assessment of Cardiac Mechanics and the Estimation of Hemodynamic Variables. Sci. Rep. 2017, 7, 6823. [Google Scholar] [CrossRef]
- Yoon, J.-W.; Noh, Y.-S.; Kwon, Y.-S.; Kim, W.-K.; Yoon, H.-R. Improvement of Dynamic Respiration Monitoring Through Sensor Fusion of Accelerometer and Gyro-sensor. J. Electr. Eng. Technol. 2014, 9, 334–343. [Google Scholar] [CrossRef] [Green Version]
- Passaro, V.M.N.; Cuccovillo, A.; Vaiani, L.; De Carlo, M.; Campanella, C.E. Gyroscope Technology and Applications: A Review in the Industrial Perspective. Sensors 2017, 17, 2284. [Google Scholar] [CrossRef] [Green Version]
- Kaisti, M.; Tadi, M.J.; Lahdenoja, O.; Hurnanen, T.; Saraste, A.; Pankaala, M.; Koivisto, T. Stand-Alone Heartbeat Detection in Multidimensional Mechanocardiograms. IEEE Sens. J. 2019, 19, 234–242. [Google Scholar] [CrossRef]
- Dehkordi, P.K.; Tavakolian, K.; Tadi, M.J.; Zakeri, V.; Khosrow-Khavar, F. Investigating the estimation of cardiac time intervals using gyrocardiography. Physiol. Meas. 2020, 41, 055004. [Google Scholar] [CrossRef]
- Sieciński, S.; Kostka, P.S.; Tkacz, E.J. Heart Rate Variability Analysis on Electrocardiograms, Seismocardiograms and Gyrocardiograms on Healthy Volunteers. Sensors 2020, 20, 4522. [Google Scholar] [CrossRef]
- Dehkordi, P.; Bauer, E.P.; Tavakolian, K.; Xiao, Z.G.; Blaber, A.P.; Khosrow-Khavar, F. Detecting Coronary Artery Disease Using Rest Seismocardiography and Gyrocardiography. Frontiers in Physiology, 2021, 12. Front. Physiol. 2021, 12. [Google Scholar]
- Yang, C.; Fan, F.; Aranoff, N.; Green, P.; Li, Y.; Liu, C.; Tavassolian, N. An Open-Access Database for the Evaluation of Cardio-Mechanical Signals from Patients with Valvular Heart Diseases. Front. Physiol. 2021, 12, 750221. [Google Scholar] [CrossRef]
- Mechanocardiograms with ECG Reference. IEEE DataPort. Available online: https://ieee-dataport.org/documents/mechanocardiograms-ecg-reference (accessed on 29 June 2022).
- Chen, S.; Qi, J.; Fan, S.; Qiao, Z.; Yeo, J.C.; Lim, C.T. Flexible Wearable Sensors for Cardiovascular Health Monitoring. Adv. Health Mater. 2021, 10, 2100116. [Google Scholar] [CrossRef]
- Lu, N.; Ameri, S.K.; Ha, T.; Nicolini, L.; Stier, A.; Wang, P. Epidermal electronic systems for sensing and therapy. In Proceedings of the Nanosensors, Biosensors, Info-Tech Sensors and 3D Systems, Portland, OR, USA, 17 April 2017; Volume 10167, p. 101670. [Google Scholar] [CrossRef]
- Ha, T.; Tran, J.; Liu, S.; Jang, H.; Jeong, H.; Mitbander, R.; Huh, H.; Qiu, Y.; Duong, J.; Wang, R.L.; et al. A Chest-Laminated Ultrathin and Stretchable E-Tattoo for the Measurement of Electrocardiogram, Seismocardiogram, and Cardiac Time Intervals. Adv. Sci. 2019, 6, 1900290. [Google Scholar] [CrossRef] [Green Version]
- Hesar, M.E.; Khan, D.; Seyedsadrkhani, N.S.; Ingebrandt, S. Contactless, Battery-free, and Stretchable Wearable for Continuous Recording of Seismocardiograms. ACS Appl. Electron. Mater. 2021, 3, 11–20. [Google Scholar] [CrossRef]
- You, I.; Kim, B.; Park, J.; Koh, K.; Shin, S.; Jung, S.; Jeong, U. Stretchable E-Skin Apexcardiogram Sensor. Adv. Mater. 2016, 28, 6359–6364. [Google Scholar] [CrossRef]
- Lo Presti, D.; Santucci, F.; Massaroni, C.; Formica, D.; Setola, R.; Schena, E. A multi-point heart rate monitoring using a soft wearable system based on fiber optic technology. Sci. Rep. 2021, 11, 21162. [Google Scholar] [CrossRef]
- Dziuda, Ł.; Skibniewski, F.W.; Krej, M.; Baran, P.M. Fiber Bragg grating-based sensor for monitoring respiration and heart activity during magnetic resonance imaging examinations. J. Biomed. Opt. 2013, 18, 057006. [Google Scholar] [CrossRef] [Green Version]
- Nedoma, J.; Fajkus, M.; Martinek, R.; Nazeran, H. Vital Sign Monitoring and Cardiac Triggering at 1.5 Tesla: A Practical Solution by an MR-Ballistocardiography Fiber-Optic Sensor. Sensors 2019, 19, 470. [Google Scholar] [CrossRef] [Green Version]
- Obermeyer, Z.; Samra, J.K.; Mullainathan, S. Individual differences in normal body temperature: Longitudinal big data analysis of patient records. BMJ 2017, 359, j5468. [Google Scholar] [CrossRef] [Green Version]
- Othonos, A.; Kalli, K.; Pureur, D.; Mugnier, A. Fibre Bragg Gratings. In Wavelength Filters in Fibre Optics; Springer: Berlin/Heidelberg, Germany, 2006; Volume 123. [Google Scholar]
- Othonos, A.; Kalli, K.; Kohnke, G.E. Fiber Bragg Gratings: Fundamentals and Applications in Telecommunications and Sensing. Phys. Today 2000, 53, 61–62. [Google Scholar] [CrossRef] [Green Version]
- Nedoma, J.; Fajkus, M.; Siska, P.; Martinek, R.; Vasinek, V. Non-Invasive Fiber Optic Probe Encapsulated into PolyDiMethylSiloxane for Measuring Respiratory and Heart Rate of the Human Body. Adv. Electr. Electron. Eng. 2017, 15, 93–100. [Google Scholar] [CrossRef]
- Lo Presti, D.; Massaroni, C.; D’Abbraccio, J.; Massari, L.; Caponero, M.; Longo, U.G.; Formica, D.; Oddo, C.M.; Schena, E. Wearable System Based on Flexible FBG for Respiratory and Cardiac Monitoring. IEEE Sens. J. 2019, 19, 7391–7398. [Google Scholar] [CrossRef]
- Presti, D.L.; Massaroni, C.; Di Tocco, J.; Schena, E.; Formica, D.; Caponero, M.A.; Longo, U.G.; Carnevale, A.; D’Abbraccio, J.; Massari, L.; et al. Cardiac monitoring with a smart textile based on polymer-encapsulated FBG: Influence of sensor positioning. In Proceedings of the IEEE International Symposium on Medical Measurements and Applications (MeMeA), Istanbul, Turkey, 26–28 June 2019; pp. 3–8. [Google Scholar] [CrossRef]
- Tavares, C.; Leitão, C.; Presti, D.L.; Domingues, M.D.F.F.; Alberto, N.; Silva, H.; Antunes, P. Respiratory and heart rate monitoring using an FBG 3D-printed wearable system. Biomed. Opt. Express 2022, 13, 2299. [Google Scholar] [CrossRef] [PubMed]
- Chethana, K.; Prasad, A.S.G.; Omkar, S.N.; Asokan, S. Fiber bragg grating sensor based device for simultaneous measurement of respiratory and cardiac activities. J. Biophotonics 2016, 10, 278–285. [Google Scholar] [CrossRef]





| Paper | Recorded Signals | Reference Signals | Extracted Features/Parameters | Filtering Technique | Acquisition Device | Location of Device | Application Scenario | Public Database | Enrolled Individuals |
|---|---|---|---|---|---|---|---|---|---|
| Choudhary et al. 2020 [52] | SCG at 1 kHz | ECG, PPG | —Fiducial points (IM, AO, IC, AC, pAC, MO) | BP 1 filter (20–30 Hz) | PCB that integrates an accelerometer (ADXL335, ±3 g), a pre-amplifier, a Butterworth LP 2 filter (50 Hz), and a buffer | Lower sternum | During both normal breathing and apnea. | — | 8 healthy male subjects |
| Khosrow-Khavar et al. 2015 [39] | SCG | ECG | —Fiducial points (IM, AO, AC) | HP 3 filter (0.5, 5, 10, 20, and 30 Hz) | Accelerometer (Brüel and Kjær model 4381) | Upper sternal border | The lower part of the body in supine position was placed in a negative pressure chamber from −20 to −50 mmHg in steps of −10 mmHg. | — | 18 healthy subjects (15 male + 3 female) |
| Khosrow-Khavar et al. 2017 [40] | SCG | ECG | —Fiducial points (IM, AO, AC) —CTIs (LVET, PEP) | BP 1 filter (0.3–40 Hz) | Accelerometer (Brüel and Kjær model 4381, Nærum, Denmark) | Upper sternum | The lower part of the body in supine position was placed in a negative pressure chamber from −20 to −50 mmHg in steps of −10 mmHg. | — | LBNP 4 raining dataset: 48 subjects (32 male + 16 female) SFU_GYM 5 test dataset: 65 healthy subjects BGH 6 test dataset: 25 patients with a history of cardiac disease (12 female + 3 male) TC 7 test dataset: 15 healthy old subjects |
| Sørensen et al. 2018 [41] | SCG at 5 kHz | SCG (reference for the second heart sound), echocardiography, ECG | —Fiducial points (AO, AC, AS, MO, MC) | 1st-order LP 2 Butterworth filter (90 Hz) | Accelerometer (Silicon Designs 1521) | Xiphoid process | Supine position while the ECG and SCG were simultaneously recorded pre, during, and post echography. | — | 45 healthy subjects (male + female) |
| Hsu et al. 2020 [59] | SCG | ECG | —SCG biometric matching tasks | BP 1 (0.5 Hz–100 Hz) and 3rd-order Savitzky–Golay filter with a time interval of 0.01s with signal detrending. | — | — | — | PhysioNet CEBS 8 database | — |
| Lin et al. 2018 [51] | SCG at 400 Hz | ECG, echocardiography | —Fiducial points (LCV, SCV, AF, PF, MFA, MFE) | BP 1 filter (0.3–50 Hz) | 3-axis accelerometer (LIS331DLH, da STMicro- electronics, Ginevra, Svizzera) | 4 sensors placed at the 4 cardiac auscultation sites in correspondence with the mitral, tricuspid, aortic, and pulmonary valves | ECG and SCG were simultaneously collected, for each subject, in the supine position. Then, these signals were recorded during echocardiography. | — | 25 healthy subjects (13 male + 12 female) |
| Zia et al. 2019 [60] | SCG | ECG, ICG | —Identification of consistent time features that co-vary with AO and PEP metrics | FIR filter (1–40 Hz) with kaiser window | 3-axis accelerometer and gyroscope | Sternum | Standing, walking at 3 mph on a treadmill, exercise (squat) and post-exercise rest. | — | 17 healthy subjects (10 male + 7 female) |
| Gamage et al. 2019 [43] | SCG at 10 kHz | — | —Cluster SCG events based on their morphology and group the clustered events with respect to lung volume phases and respiratory flow signals | BP 1 filter (0.5–40 Hz) | 3-axis accelerometer (Model 356A32, PCB Piezotronics, Depew, NY) | 4th intercostal space near the left lower sternal border | — | — | 5 healthy male subjects |
| Taebi et al. 2018 [44] | SCG at 10 kHz | — | —Feature extraction during different lung phases —Cluster SCG events into classes of HLV 12 and LLV 13 | LP 2 filter (100 Hz) | 3-axis accelerometer (Model 356A32, PCB Piezotronics, Depew, NY) | 4th intercostal space and left sternal border | Supine on a bed with the chest tilted at 45°. | — | 7 healthy male subjects |
| Shafiq et al. 2016 [55] | SCG at 500 Hz | ECG | —Fiducial points (AO e AC) | 5th-order Butterworth BP 1 filter (1–35 Hz) | Accelerometer | Xiphoid process | Supine position while breathing normally. | — | 5 healthy subjects |
| Khosrow-Khavar et al. 2015 [42] | SCG | ECG | —Fiducial points (IM, AC) | 5th-order LP 2 Butterworth filter (30 Hz) | Accelerometer (Brüel and Kjær model 4381, Nærum, Denmark) | — | The lower half of the body of the subject was placed in a sealed chamber in which the pressure was gradually reduced to -50 mmHg. | — | LBNP 4 training dataset: 18 healthy subjects (15 male + 3 female) SFU_GYM 5 test dataset: 67 healthy subjects (35 male + 32 female) |
| Wick et al. 2012 [56] | SCG at 1.2 kHz | ECG, echocardiography | —Fiducial points (AC) —CTIs (R-AC delay) | HP 3 filter (50 Hz). | Custom device integrating two 3-axis accelerometers (ADXL327, Analog Devices, Inc., Norwood, MA) | 4th intercostal space | Echocardiography, ECG, and SCG data were simultaneously recorded using both the custom device and the ultrasound machine in static conditions | — | 2 healthy subjects (1 male + 1 female) |
| Tavakolian et al. 2010 [27] | SCG at 2.5 kHz | ECG, ICG, suprasternal pulsed Doppler | —STI (LVET, PEP, and QS2) —Stroke volume estimation | — | Accelerometer (Model 393C, PCB Piezotronics) | Midline of the sternum with the lower edge of the sensor on the xiphoid process | Suprasternal Doppler, SCG, ECG, and ICG were simultaneously recorded. For stroke volume estimation, the signal acquisition was conducted in two separate sessions at least a day apart. The signal from the first session was used for training and the second day for testing. | — | 24 subjects (21 male + 3 female): 20 healthy subjects + 4 patients of the BGH 6 who had a history of heart attack and very low ejection fraction. |
| Choudhary et al. 2020 [46] | SCG at 5 kHz | — | —Fiducial points (AO) | — | Custom device integrating an accelerometer (ADXL335, ±3 g) | Xiphoid process | Under both normal breathing and apnea in static conditions. The test was repeated in supine position during normal breathing and apnea, while sitting and standing, and during post-exercise recovery. | Test on CEBS 8 database | 5 healthy male subjects + 20 healthy subjects from CEBS 8 database |
| Mora et al. 2020 [45] | SCG (SCG-1: 100 Hz; SCG-2: 5 kHz) | ECG | —Template generation | BP 1 FIR 15 filter (2–14 Hz) | 3-axis accelerometer (ADXL 355 from Analog Devices, Inc.) | Xiphoid process for datasets SCG-1 and SCG-2 | 2 datasets of SCG and ECG signals. SCG-1: SCG recorded on 13 healthy volunteers in sitting position. SCG-2: public dataset | Dataset SCG-2: dataset CEBS | Dataset SCG-1: 13 healthy subjects Dataset SCG-2: 20 healthy subjects |
| Choudhary et al. 2019 [69] | SCG at 5 kHz | — | —Fiducial points (AO) | 5th-order median filter | — | — | — | CEBS 8 database | — |
| Hsu et al. 2021 [47] | SCG at 150Hz | Blood pressure | —HR estimation | 3rd-order Savitzky–Golay filter of 100 ms span, 6th-order LP 2 Butterworth filter (35 Hz), and interpolation with spline cubic curves at 750 Hz | 3-axis accelerometer (MPU-6050) | Sternum | During both static (sitting) and dynamic (walking) conditions. | — | 20 healthy subjects (14 male + 6 female) |
| Lin et al. 2020 [58] | SCG at 5 kHz | ECG | —HR estimation | — | — | — | — | CEBS 8 database | 20 healthy subjects (12 male + 8 female) |
| Garcia-Gonzales et al. 2013 [61] | SCG at 5 kHz | ECG | —HR estimation | 4th-order BP 1 Butterworth filter (5–30 Hz) | 3-axis accelerometer (LIS344ALH, ST Microelectronics) | — | During static condition (supine position on a single bed). After 5 min of basal state, subjects listened to music for ~50 min. Finally, all subjects were monitored for 5 min after the music ended. | — | 17 healthy subjects (11 male + 6 females). |
| Dinh et al. 2011 [53] | SCG at 400 Hz | ECG | —HR estimation | 2 stages of LP 2 filtering (40 Hz) | PCB with a 3-axis accelerometer (MMA7260QT, made by Freescale). | — | Pre-exercise (in sitting, standing, and supine position), during exercise (walking), post-exercise (standing) | — | 1 healthy subject |
| Choudhary et al. 2021 [64] | SCG (CEBS database: 5 kHz; private database: 1 kHz) | ECG | —Fiducial points (AO) —HRV estimation | — | — | — | — | CEBS 8 database + private database 14 | CEBS 8 database: 20 healthy subjects Private database 14: 3 healthy male subjects |
| Ramos-Castro et al. 2012 [48] | SCG at 1 kHz | ECG | —HR estimation | 4th-order Butterworth BP 1 filter (6–25 Hz) | In the first group, a 3-axis accelerometer (ADXL330, Analog Devices) with a low-pass frequency of 100 Hz was used, while, in the second group, an iPhone 4 was used. | Sternum | In supine position | — | 12 healthy subjects |
| Tadi et al. 2015 [57] | SCG at 800 Hz | ECG | —HRV estimation | BP 1 filter (4–50 Hz) with moving average filter (window duration of 10 and 20 ms) | 3-axis capacitive digital accelerometer (MMA8451Q from Freescale Semiconductor) | Sternum | Supine position on a bed | — | 20 healthy male subjects |
| Shandhi et al. 2022 [66] | SCG at 500 Hz | ECG | —Estimate changes in PAM 9 and PCWP 10 | BP 1 filter (1–40 Hz) | Custom-built wearable patch embedding a PCB with a 3-axis accelerometer (BMA280 from Bosch Sensortec GmbH, Reutlingen, Germany) | Middle of the sternum | During RHC 11 procedure | — | 20 patients with HF |
| Chen et al. 2020 [65] | SCG at 1 kHz | ECG | —Cluster waveforms based on similar morphology —Template generation | HP 3 filter (40 Hz) | Accelerometer | 4 sensors placed at the 4 cardiac auscultation sites in correspondence with the mitral, tricuspid, aortic, and pulmonary valves | Supine position at rest | — | 16 total subjects: 8 healthy subjects + 8 patients with HF |
| Paper | Recorded Signals | Reference Signals | Extracted Features/Parameters | Filtering Technique | Acquisition Device | Location of Device | Application Scenario | Public Database | Enrolled Individuals |
|---|---|---|---|---|---|---|---|---|---|
| Yang et al. 2017 [63] | GCG and first derivative of GCG (DGCG) at 256 Hz | ECG, ICG, SCG | —Fiducial points (IM, A0, AC) —CTIs (LVET, PEP) | BP 1 Butterworth filter (0.8–25 Hz) | IMU (Shimmer 3 from Shimmer Sensing): 3-axis accelerometer (Kionix KXRB5-2042, Kionix, Inc.) + 3-axis gyroscope (Invensense MPU9150, Invensense, Inc., San Jose, CA, USA). | Along the second and third rib at the middle of the sternum | Sitting on a chair pre-exercise, steps climbing and resting post-exercise | — | 5 healthy subjects (3 male + 2 female) |
| D’Mello et al. 2019 [11] | SCG combined with GCG (VCG 16) at 250 Hz | ECG | —Fiducial points (AO) —HR estimation | HP 3 brick wall filter (0.4 Hz). | InvenSense Motion Processing UnitTM 9250 consisting of a MEMS gyroscope and accelerometer | Xiphoid process | Resting supine, high intensity physical exercise and resting post-exercise. | — | 25 healthy male subjects |
| Dehkordi et al. 2020 [76] | GCG standalone and combined with SCG at 1 kHz | SCG, ECG, ICG, echocardiogram | —Fiducial points (AO, AC, MO, MC) —CTIs (EMD, PEP, ST, Q-MO, LVET, IVCT, IVRT) —Tei index | — | IMU (ASC GmbH, ASC IMU 7.002LN.0750, Pfaffenhofen, Germany): low-noise 3-axis MEMS joint accelerometer-gyroscope sensor | — | — | — | 50 healthy subjects (23 male + 27 female) |
| Tadi et al. 2017 [72] | GCG at 800 Hz | SCG, ECG, echocardiogram | —Fiducial points (AVO, AVC, MVO, MVC) —CTIs (LVET, PEP, QS2, IVRT, IVCT, Q-SPV, Q-DPV) | 4th-order BP 1 Butterworth IIR 17 filter (1–20 Hz) | Custom-made IMU: 3-axis low-power capacitive digital accelerometer (Freescale Semiconductor, MMA8451Q, Austin, TX, USA) + low-power low-noise 3-axis gyroscope (Maxim Integrated, MAX21000, San Jose, CA, USA) | Middle of the sternum | Lying down in the supine position with the upper body slightly tilted. | — | 9 healthy male subjects |
| Kaisti et al. 2019 [75] | GCG combined with SCG at 800 Hz | ECG | —HR estimation | Filtered with a 3rd-order BP 1 Butterworth IIR 17 filter (0.5–20 Hz) |
IMU: 3-axis capacitive digital accelerometer (Freescale Semiconductor, MMA8451Q, Austin, TX, USA) + 3-axis gyroscope (Maxim Integrated, MAX21000, San Jose, CA, USA) | Sternum | Lying either in the supine position or on left or right side. | — | Dataset 1: 29 healthy male subjects. Dataset 2: 12 patients with coronary artery disease (10 male + 2 female) |
| Sieciński et al. 2020 [77] | GCG and SCG at 800 Hz | ECG | —HRV analysis | 3rd-order Butterworth BP 1 filter (4–50 Hz) with zero-phase FIR moving average filter with the window width of 15 ms; to align the baseline with zero, the signals resulted from beat detection were filtered with the 3rd-order BP 1 Butterworth filter (1 Hz and 40 Hz) | — | — | — | Mechanocardiograms with ECG Reference data set 18 | — |
| Paper | Recorded Signals | Reference Signals | Extracted Features/Parameters | Filtering Technique | Acquisition Device | Location of Device | Application Scenario | Public Database | Enrolled Individuals |
|---|---|---|---|---|---|---|---|---|---|
| Lo Presti et al. 2019 [93] | SCG | PPG | —HR estimation | 2nd-order BP 1 Butterworth filter (0.8–2 Hz) | A commercial FBG (λB of 1547 nm, grating length of 10 mm, and reflectivity of 90%; AtGrating Technologies) encapsulated into a frame of Dragon skin®20 silicone rubber (Smooth-On, Inc., Macungie, PA, USA) of dimensions 90 mm × 24 mm × 1 mm. | Lower thorax | Each volunteer was asked to perform two tests consisting of a stage during both quiet breathing and apnea | — | 2 healthy subjects (1 male + 1 female) |
| Chethana et al. 2017 [96] | SCG | Stethoscope | —HR estimation (average HR per minute) | HP 3 filter (0.5 Hz) | The sensor is made of a cone-shaped structure whose end is made up of polyvinyl chloride, a micrometer, and a flexible silicon diaphragm. A 9/125 μm diameter germania-doped photosensitive silica fiber was used in the fabrication of FBG sensors of 3 mm gauge length. The fabricated FBG sensor was tightly bonded across the diaphragm using a thin layer of cyanoacrylate adhesive. | Around 2nd and 3rd interspace of pulmonic area | Under different breathing conditions (slow, automatic inhalation and exhalation, forced inhalation and exhalation) | — | 4 healthy subjects (2 male + 2 female) |
| Nedoma et al. 2019 [88] | SCG at 1 kHz | ECG | —HR estimation | 3rd-order Butterworth BP 1 filter (5–20 Hz) | The sensor (dimensions 30 × 10 × 0.8 mm and weight 2 g) is made of a fiberglass structure (type Epikote Resin MGS LR 285 and Curing Agent MGS LH 285) of length 1.8 mm, which encapsulates a Bragg grating with a λB of 1550.218 nm. The sensor was designed as part of a contact elastic belt. | Around the pulmonic area near to the heart | During MRI procedures | — | 10 healthy subjects (6 male + 4 female) |
| Nedoma et al. 2017 [92] | SCG at 300 Hz | — | —HR estimation | BP 1 Butterworth IIR 17 -filter (1–5 Hz). | The measuring probe consists of the uniform FBG with polyamide protection with λB of 1554.1207 nm. The width of the reflecting spectrum was 2.3241 nm, and reflectivity was 95.7%. It was encapsulated into a PDMS polymer of rectangular shape. | Left side of the upper chest in an area of the heart | standing, sitting and supine | — | 5 healthy subjects |
| Tavares et al. 2022 [95] | SCG at 1 kHz | ECG | —HR estimation | BP 1 filter (0.8–2.0 Hz) | The sensor consists of an elastic material (Flexible, Fish box mini model, Avistron, Bergheim, Germany) printed by a 3D printer (Ultimaker 3D Extended, Ultimaker, Utrecht, Netherlands) and a single optical fiber with a single FBG. | Left side of the chest | During apnea and normal breathing while lying down on a physiotherapy bed | — | 3 healthy subjects |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santucci, F.; Lo Presti, D.; Massaroni, C.; Schena, E.; Setola, R. Precordial Vibrations: A Review of Wearable Systems, Signal Processing Techniques, and Main Applications. Sensors 2022, 22, 5805. https://doi.org/10.3390/s22155805
Santucci F, Lo Presti D, Massaroni C, Schena E, Setola R. Precordial Vibrations: A Review of Wearable Systems, Signal Processing Techniques, and Main Applications. Sensors. 2022; 22(15):5805. https://doi.org/10.3390/s22155805
Chicago/Turabian StyleSantucci, Francesca, Daniela Lo Presti, Carlo Massaroni, Emiliano Schena, and Roberto Setola. 2022. "Precordial Vibrations: A Review of Wearable Systems, Signal Processing Techniques, and Main Applications" Sensors 22, no. 15: 5805. https://doi.org/10.3390/s22155805