
A Systematic Survey of Research Trends in Technology Usage for Parkinson’s Disease


Abstract
:1. Introduction
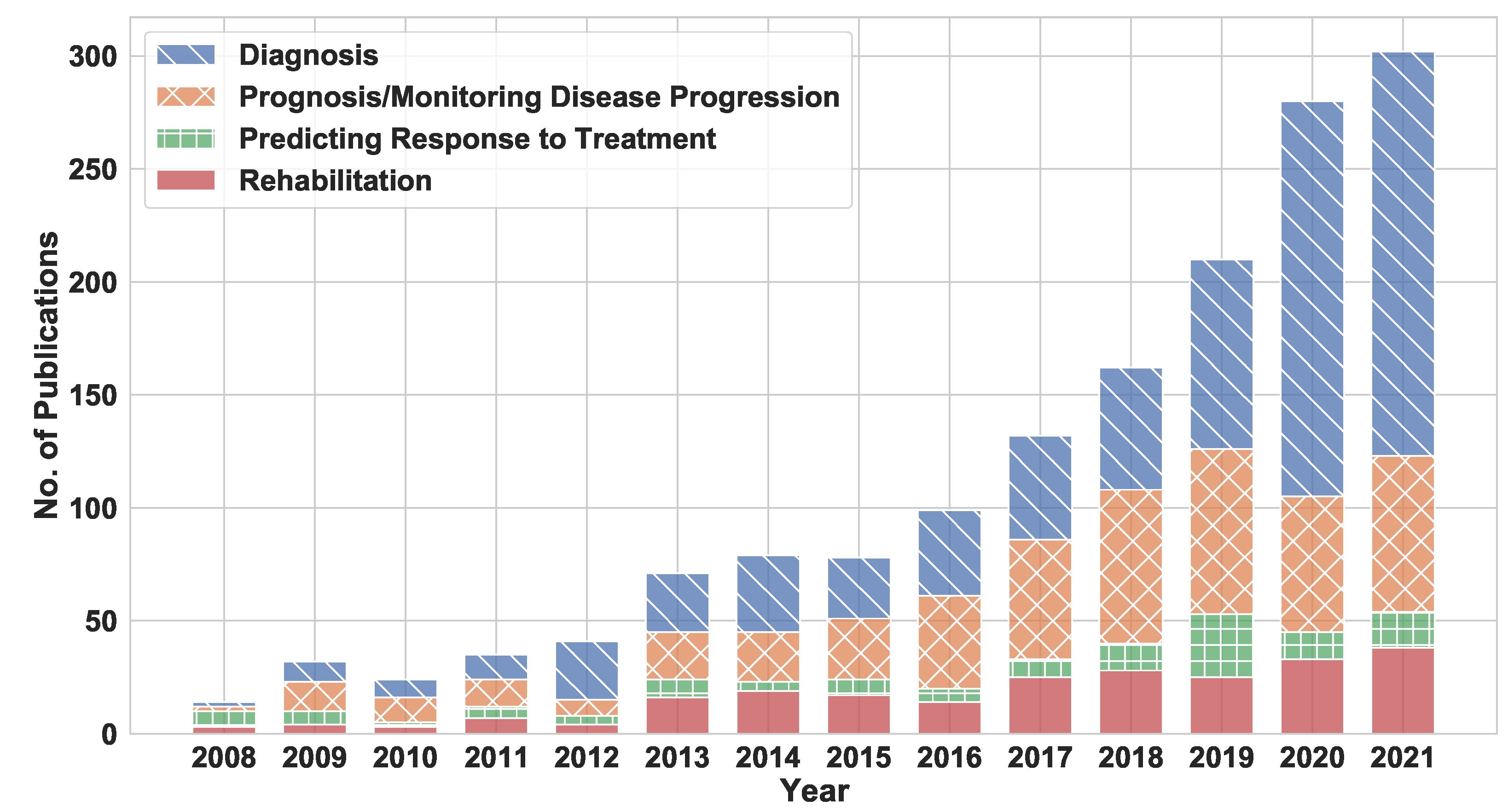
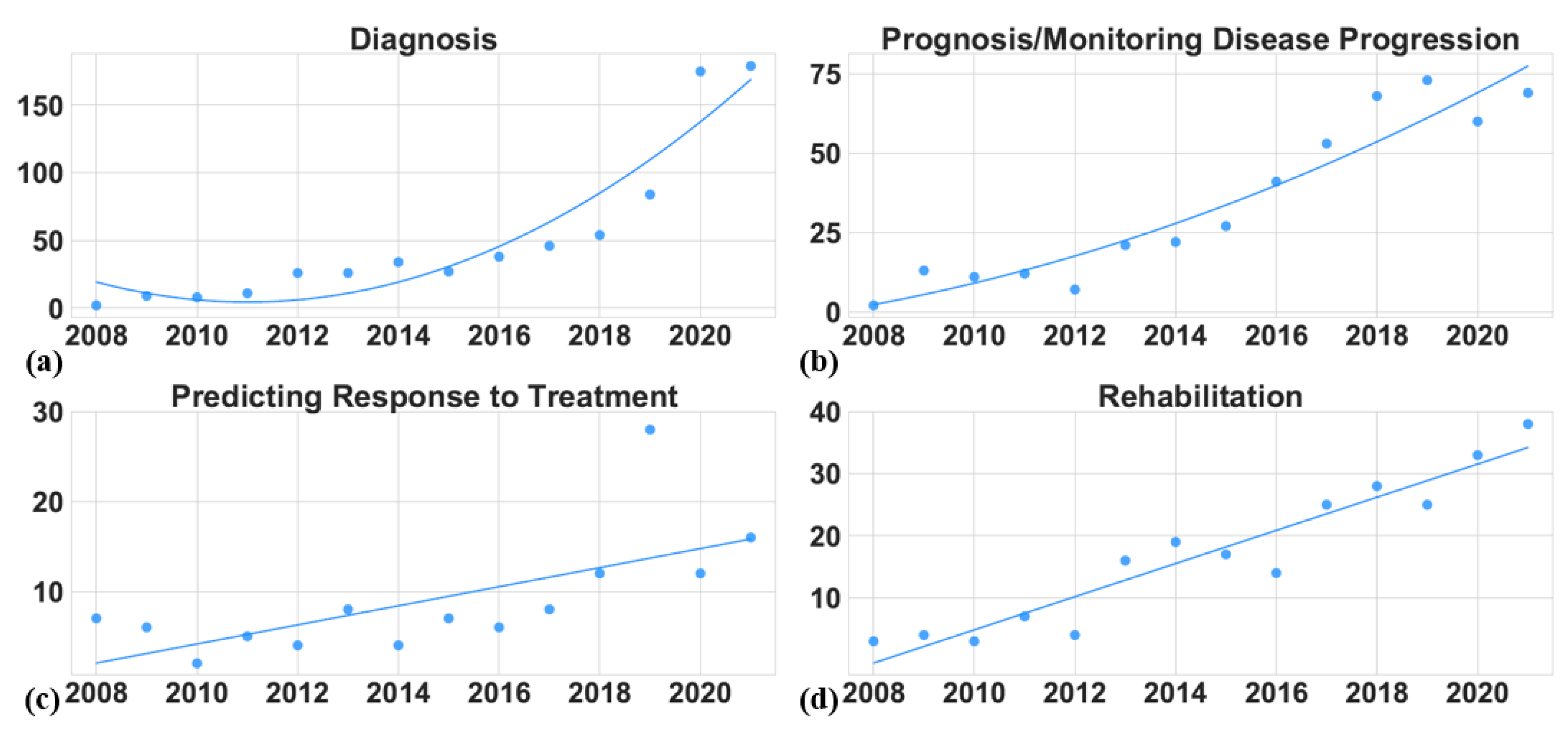
- Analyze the trends in use of technology for PD research. For example, we used the available data to identify the most popular application areas and the areas receiving increased attention (Section 2.2),
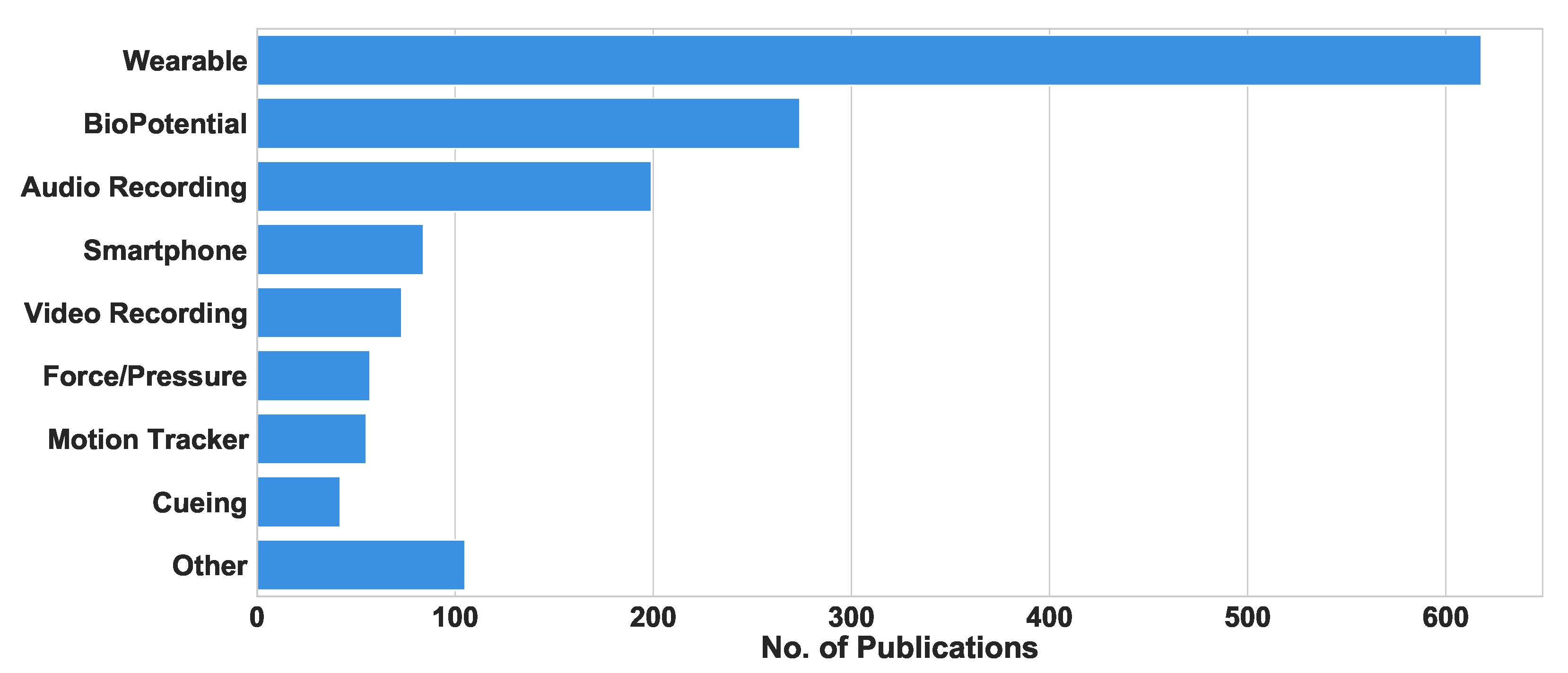
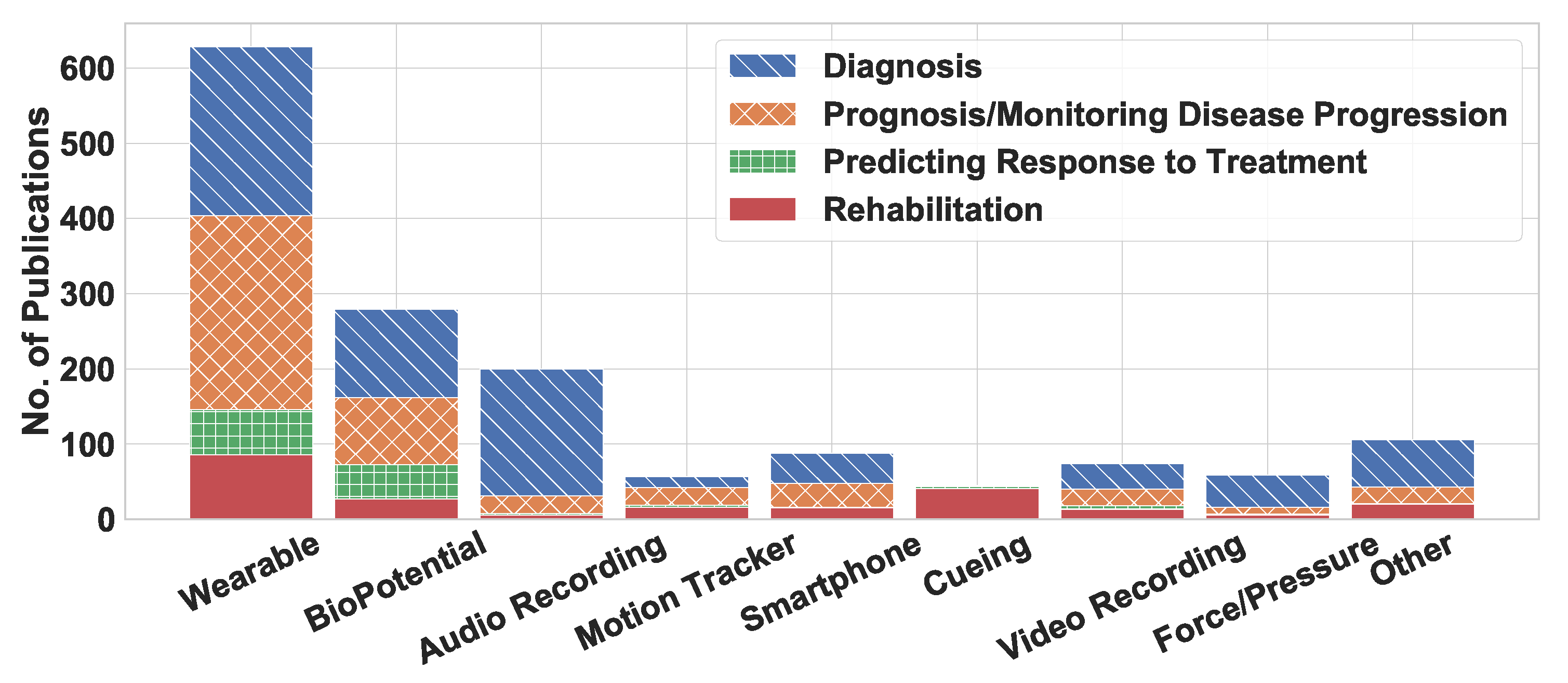
- Analyze the devices used in each application area (Section 2.3),
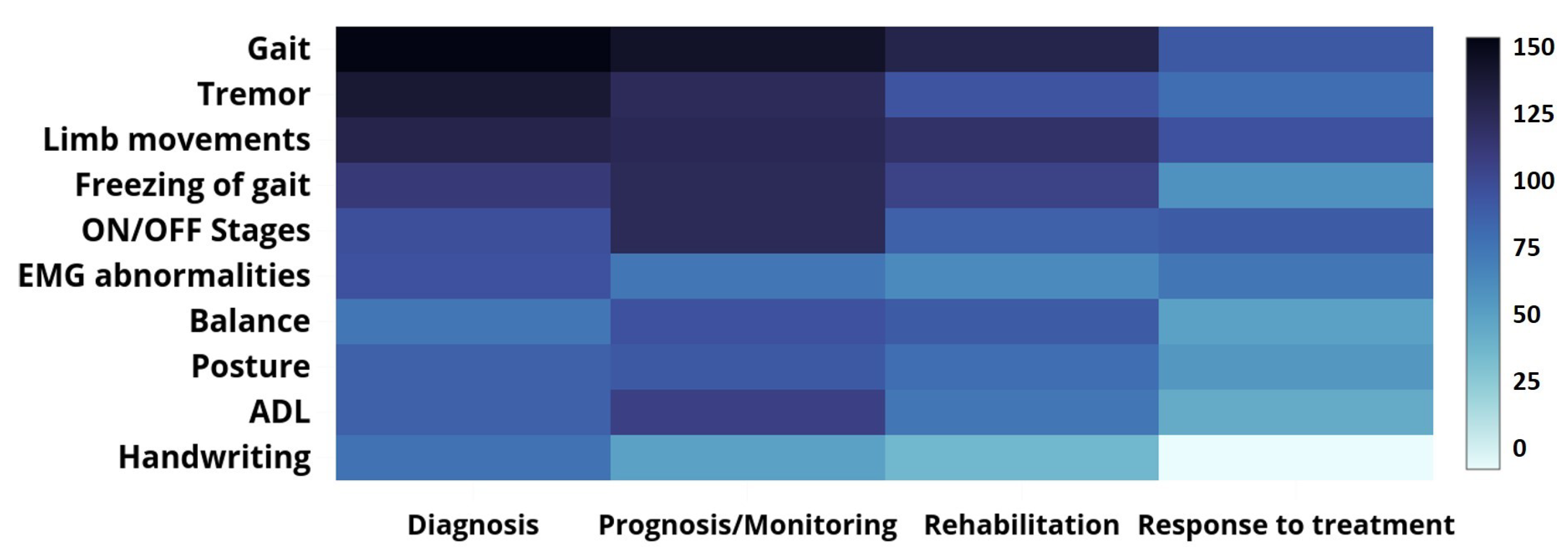
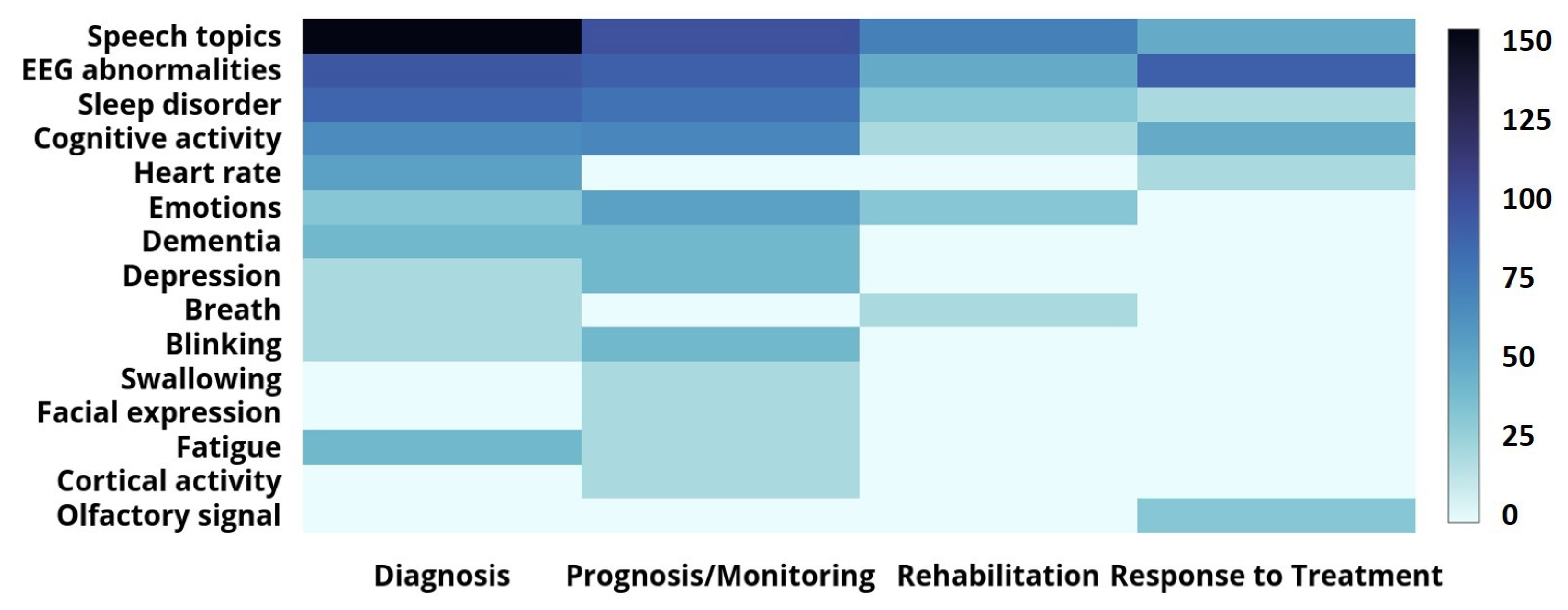
- Analyze the symptoms measured in each application area and identify the most commonly used devices for measuring the different traits (Section 4.1),
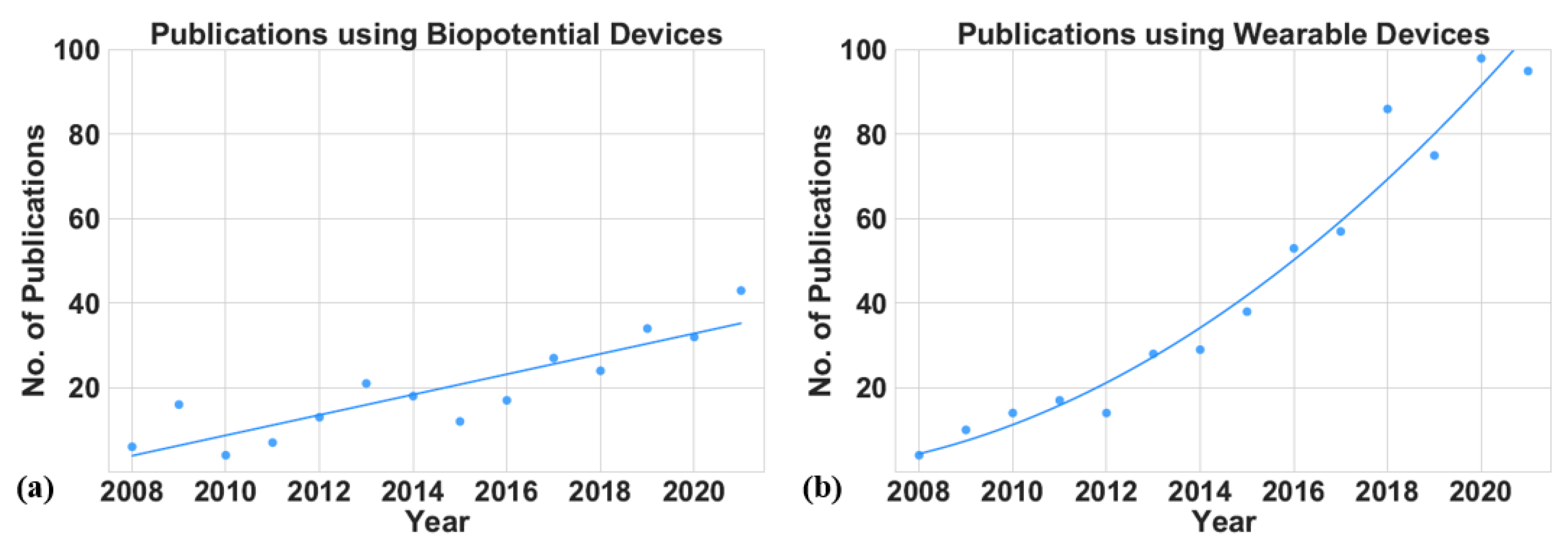
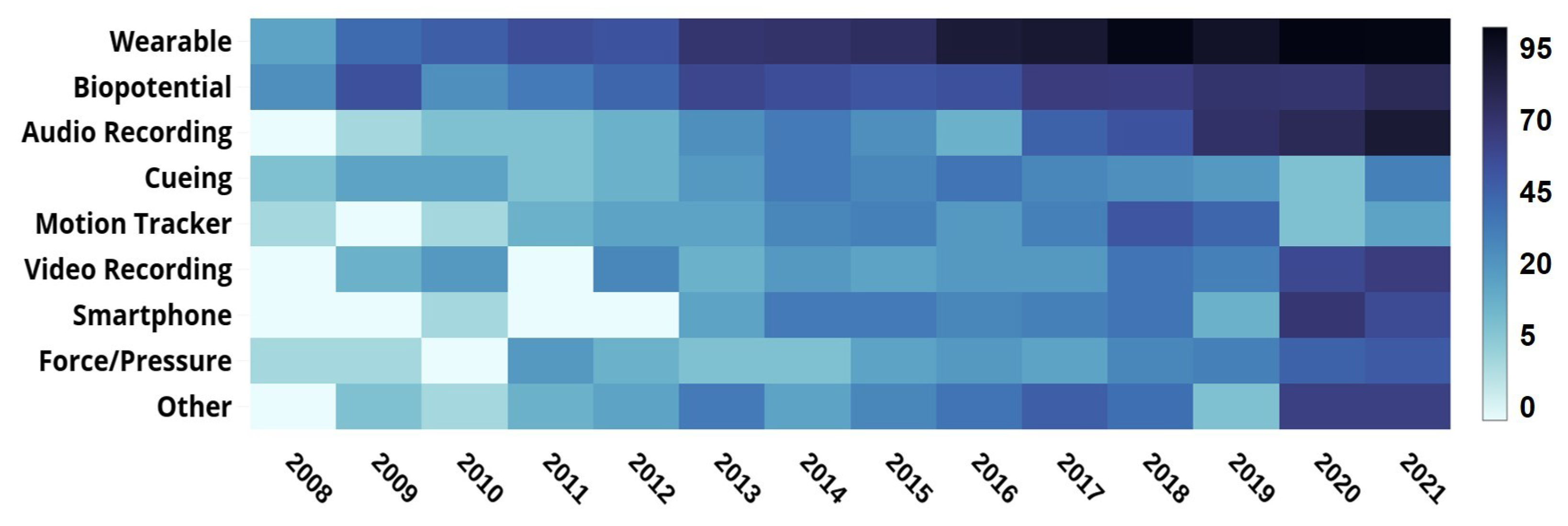
- Analyze the overall research trends in this field and how it progresses in the coming years (Section 4.2 and Section 4.3).
2. Background
2.1. Related Work
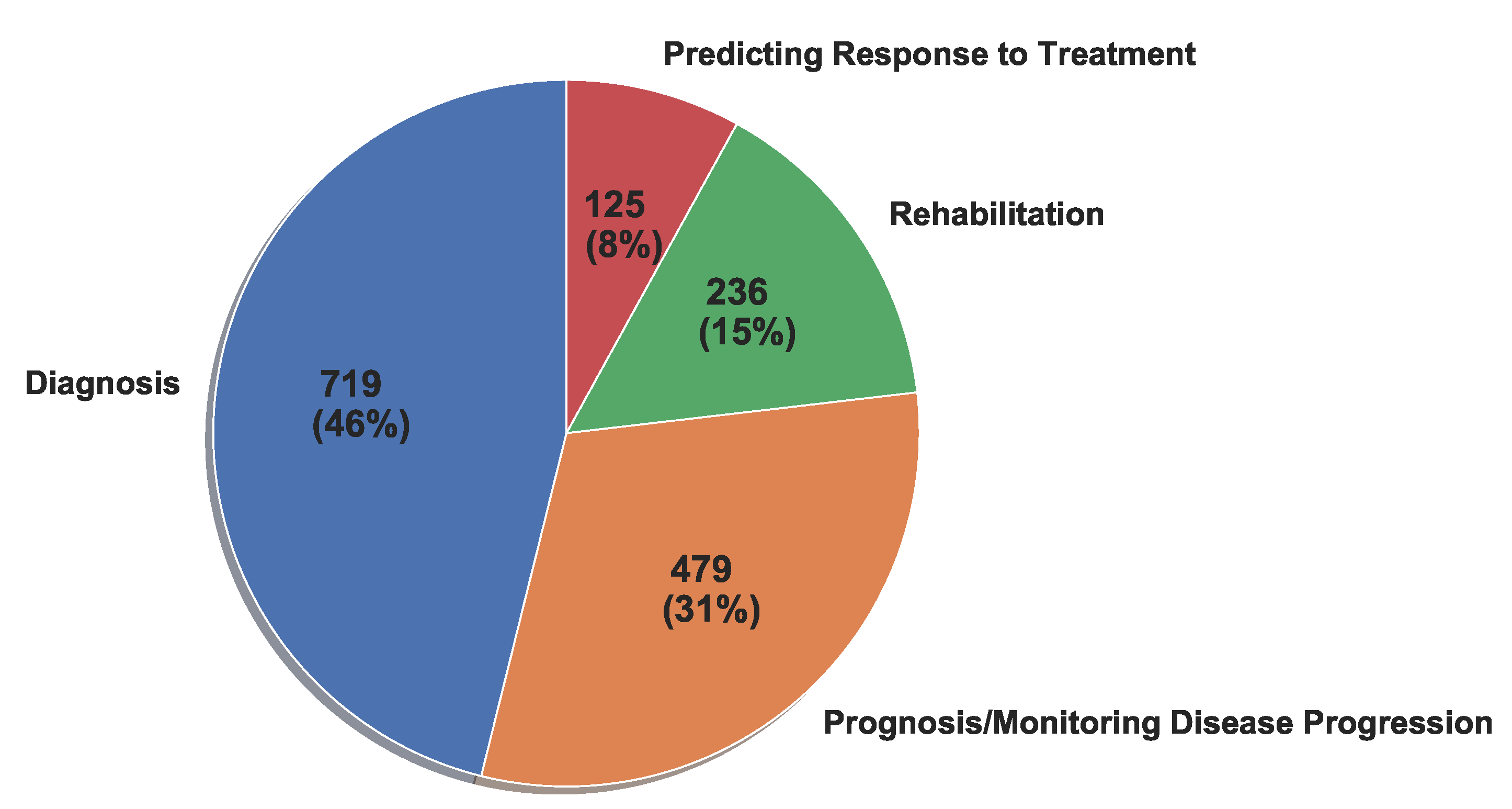
2.2. Application Areas
2.2.1. Diagnosis
- Early diagnosis of patients with PD;
- Detecting PD symptoms in people with untreated PD;
- Distinguishing PD patients from either healthy controls or patients with non-PD neurological disorders;
- Distinguishing PD-related symptoms from similar symptoms not caused by PD (e.g., distinguishing PD tremors from essential tremors).
2.2.2. Prognosis and Monitoring the Severity of Symptoms
- Home-based or remote monitoring of PD patients;
- Evaluating the PD progression in a diagnosed patient;
- Evaluating the severity of PD symptoms for a diagnosed patient.
2.2.3. Predicting Response to Treatment
- Measuring the effects of such treatments as deep brain stimulation on the suppression of patients’ symptoms over time;
- Measuring the intended effects of medications on patient symptoms;
- Measuring the unintended effects (i.e., the side effects) of medications on patients (e.g., levodopa-induced dyskinesia).
2.2.4. Rehabilitation
- Audio, visual, or haptic cue for gait or movement training;
- Sensory feedback to suppress a symptom such as FoG or tremor.
2.3. Technology in Parkinson’s Disease Research
2.3.1. Wearable Devices
- IMUs with integrated accelerometers, gyroscopes, and magnetometer sensors;
- Insole force- or pressure-based sensors that can measure the ground reaction force (GRF);
- Wearable devices that use sensors such as EEG and EMG to measure neural responses and muscle activities;
- Clothing-integrated sensors, such as strain or accelerometer sensors, that measure hand tremors;
- Other wearable devices, including smart glasses and smart hats, that can record patients’ emotions and other specific parameters.
2.3.2. Biopotential Devices
2.3.3. Cueing Devices
2.3.4. Optical Motion Tracker
2.3.5. Audio Recording
2.3.6. Video Recording
2.3.7. Force/Pressure
2.3.8. Smartphone
2.3.9. Other
3. Methodology for Article Selection and Classification
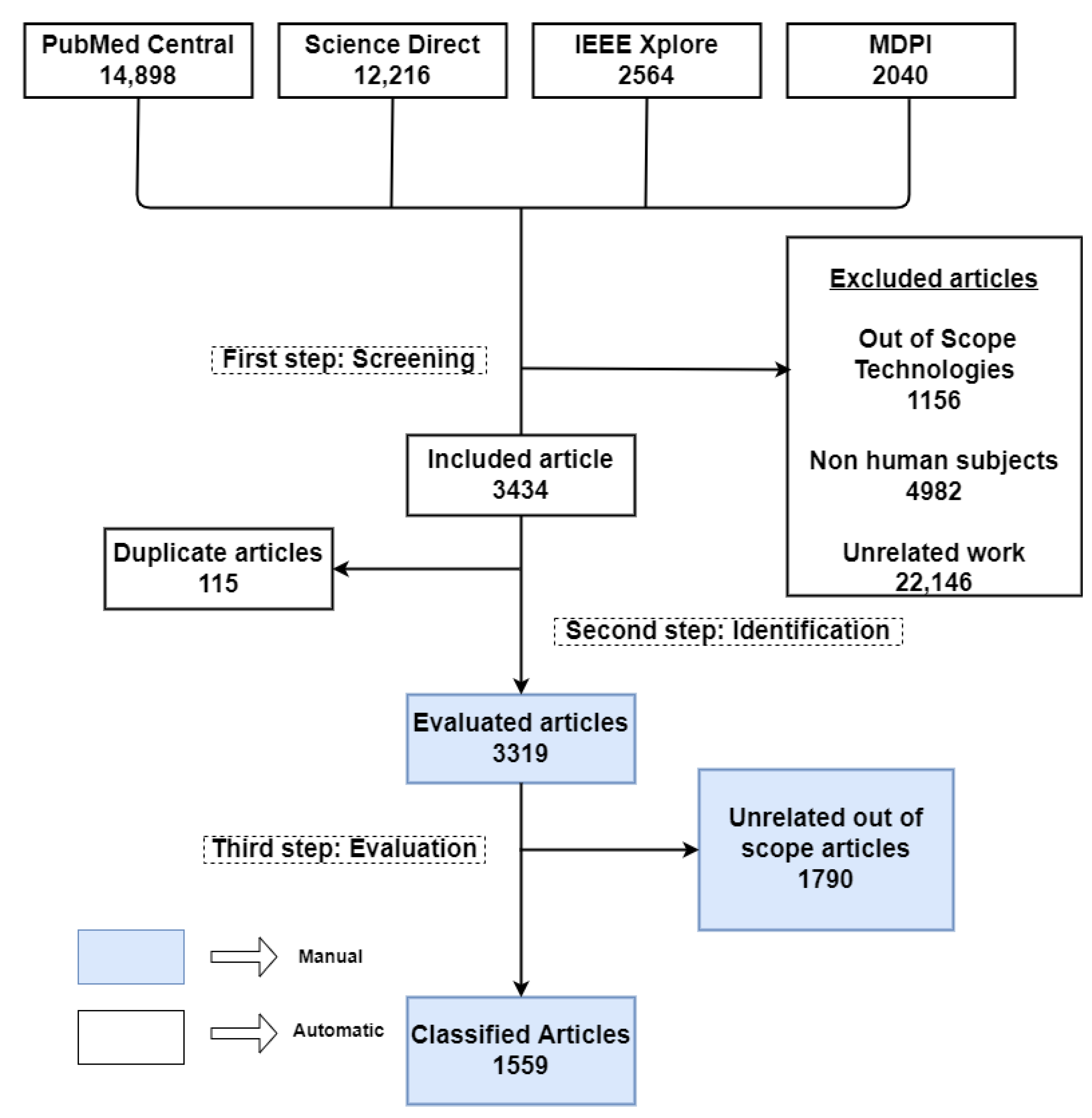
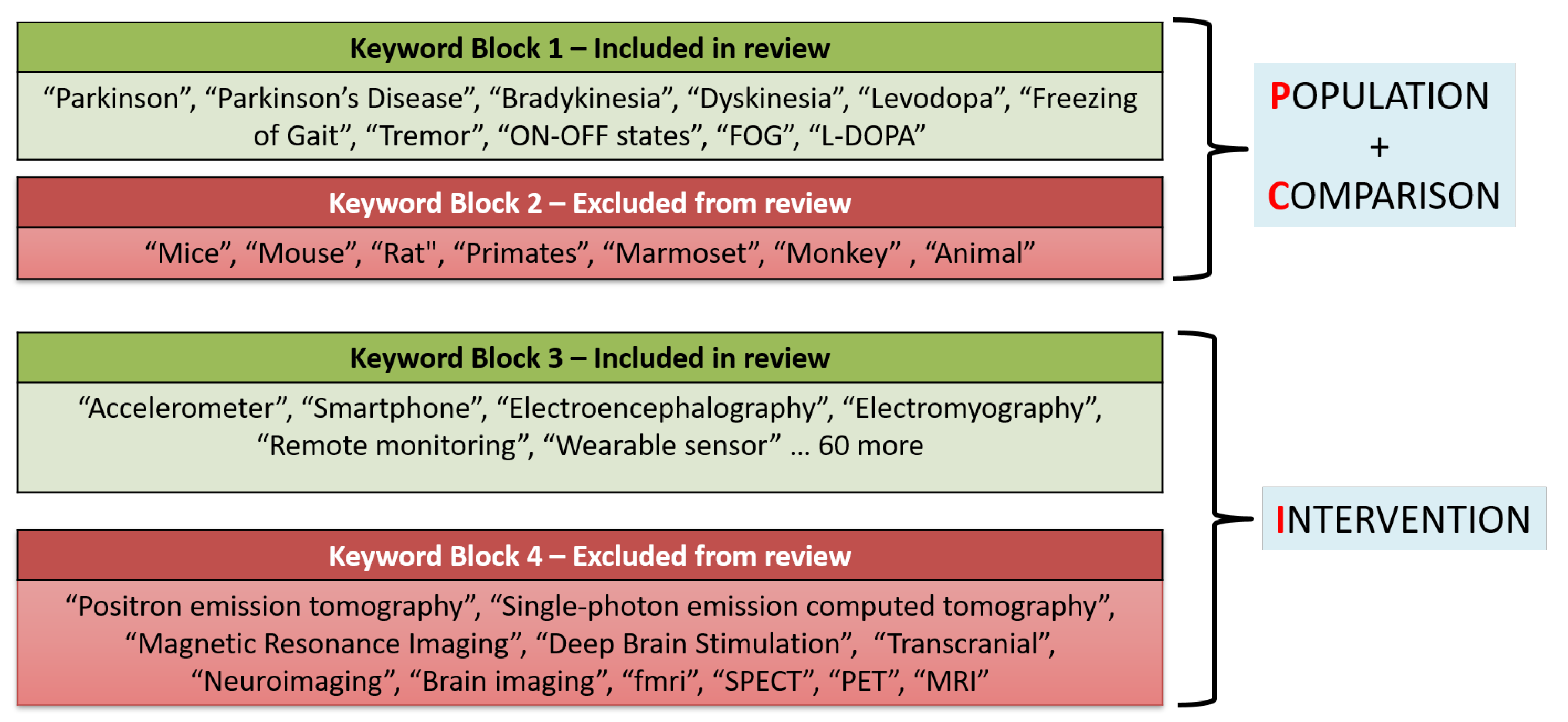
3.1. Search Methodology
3.2. Filtering Methodology
3.3. Classification Methodology
4. Results and Discussion
4.1. Application Areas
4.1.1. Diagnosis
4.1.2. Prognosis and Monitoring Disease Progression
4.1.3. Predicting Response to Treatment
4.1.4. Rehabilitation
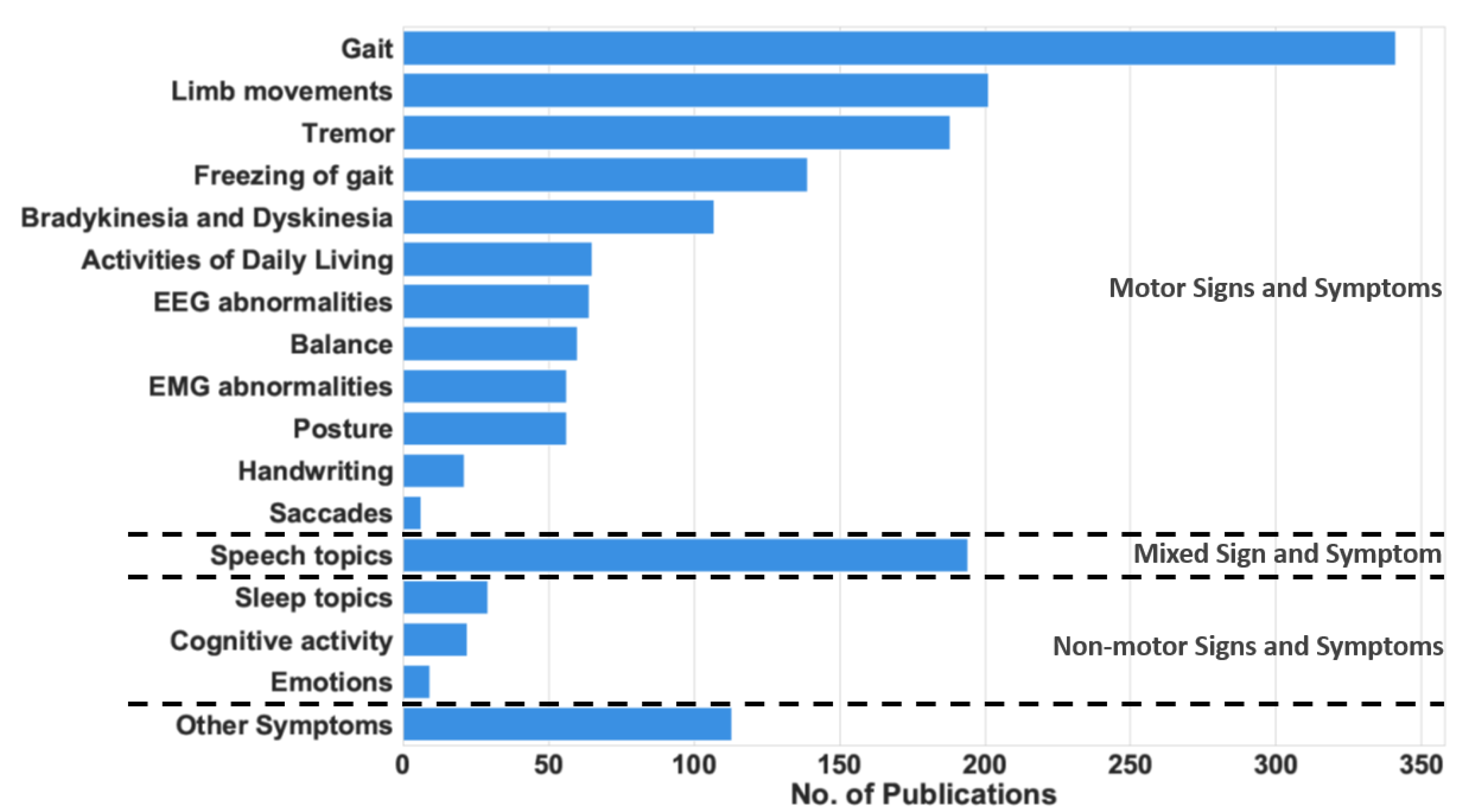
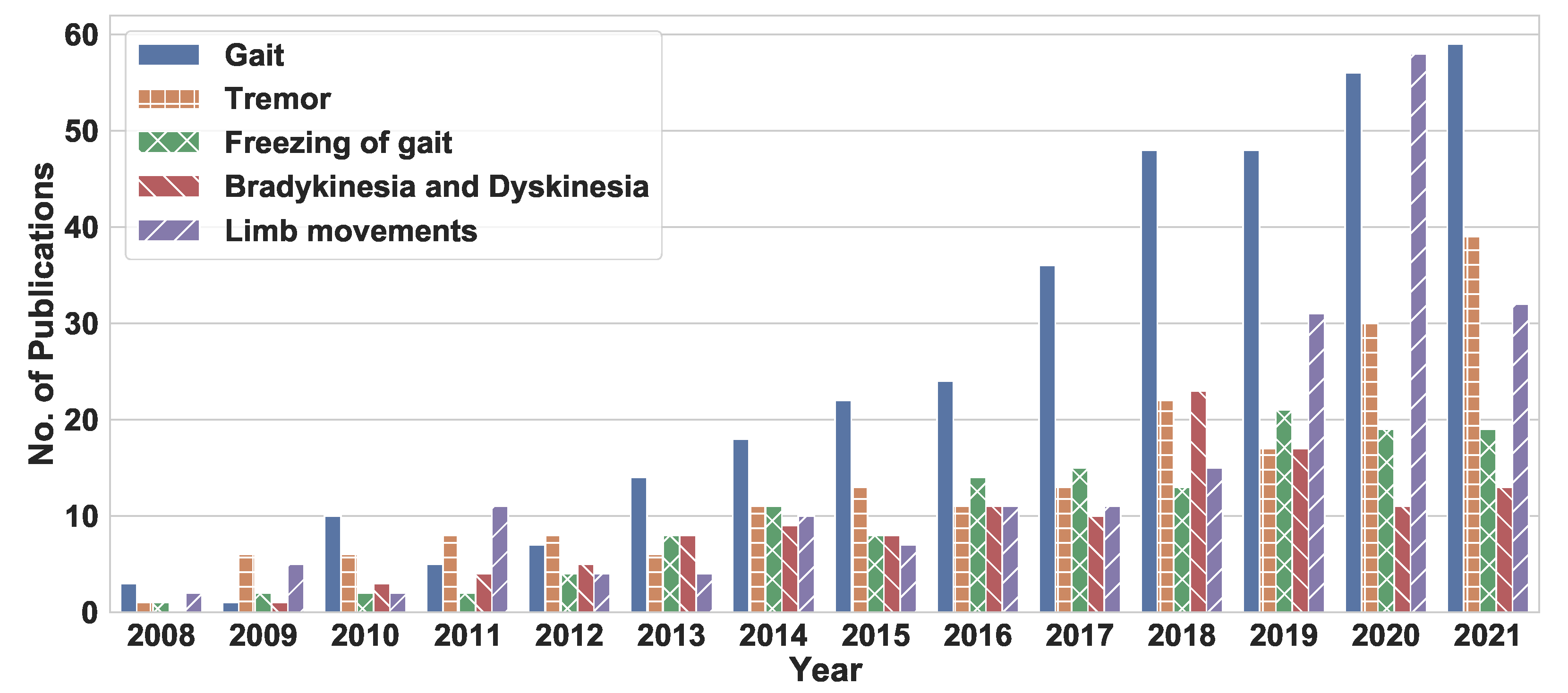
4.2. Trends in Symptoms Measured by PD Research Papers
4.3. Trends in Device Usage from 2008 to 2021
5. Conclusions, Gaps in Literature, and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Data Collection
Appendix B. List of Papers in Each Application Area
Appendix C. Keywords Used for Automated Filtering

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Year | Application | Aspect Area | Device | Additional Device | Sensors | No. of Subjects (n) |
|---|---|---|---|---|---|---|---|
| Jobi S. George et al. [7] | 2013 | Predicting Response to treatment | Bradykinesia and Dyskinesia | Biopotential | EEG | 10 < n ≤ 20 | |
| Damian M. Herz et al. [75] | 2014 | Predicting Response to treatment | EEG Signals | Biopotential | EEG | 10 < n ≤ 20 | |
| Verneri Ruonala et al. [76] | 2018 | Predicting Response to treatment | Muscle activity | Wearable | Biopotential | EMG | 10 < n ≤ 20 |
| George Rigas et al. [77] | 2010 | Predicting Response to treatment | EEG Signals | Biopotential | EEG | u/k | |
| Paulo H. S Pelicioni et al. [78] | 2018 | Predicting Response to treatment | Gait, Posture, Balance | Wearable | Accelerometer | >30 | |
| Samer D. Tabbal et al. [124] | 2008 | Predicting Response to treatment | Limb movements | Wearable | Force sensor, Gyroscope | >30 | |
| Y. Rakhshani Fatmehsari et al. [79] | 2011 | Predicting Response to treatment | Gait | Wearable | Gyroscope, Accelerometer | ≤10 | |
| Roongroj Bhidayasiri et al. [10] | 2016 | Predicting Response to treatment | Nocturnal Hypokinesia | Wearable | Accelerometer, Gyroscope | ≤10 | |
| Verneri Ruonala et al. [76] | 2018 | Predicting Response to treatment | EMG Signal | Wearable | Biopotential | EMG | |
| Saara M. Rissanen et al. [125] | 2015 | Predicting Response to treatment | EMG Signal | Wearable | Biopotential | EMG, Accelerometer | |
| Wesley JE Teskey et al. [8] | 2012 | Predicting Response to treatment | Bradykinesia and Dyskinesia | Wearable | Accelerometer, Gyroscope | 20 < n ≤ 30 |
| Reference | Year | Application | Aspect Area | Device | Additional Device | Sensor/Actuator | No. of Subjects |
|---|---|---|---|---|---|---|---|
| Taylor Chomiak et al. [81] | 2017 | Rehabilitation | Limb movements | Cueing | Wearable | Audio cue | 10 < n ≤ 20 |
| William R. Young et al. [82] | 2016 | Rehabilitation | Freezing of Gait | Cueing | Audio cue | 10 < n ≤ 20 | |
| E. Jovanov et al. [83] | 2009 | Rehabilitation | Freezing of Gait | Wearable | Cueing | Audio cue, Accelerometer, Gyroscope | ≤10 |
| Steven T. Moore et al. [84] | 2008 | Rehabilitation | Gait, Freezing of Gait | Wearable | Accelerometer | 10 < n ≤ 20 | |
| M.E. Jenkins et al. [5] | 2009 | Rehabilitation | Muscle activity | Biopotential | EMG | >30 | |
| Vishnu Vidya et al. [85] | 2017 | Rehabilitation | Tremor | Cueing | Vibration cue | u/k | |
| Pieter Ginis et al. [126] | 2017 | Rehabilitation | Gait | Motion Tracker | Motion capture | ≤10 | |
| Juan Camilo Vasquez-Correa et al. [127] | 2018 | Rehabilitation | Gait, Speech topics, Handwriting | Wearable | Audio Recording, Other | Touchscreen, Microphone, Accelerometer, Gyroscope | |
| Syed Haidar Shah et al. [128] | 2018 | Rehabilitation | Freezing of Gait | Wearable | Accelerometer, Gyroscope | ||
| W Nanhoe-Mahabier et al. [129] | 2012 | Rehabilitation | Balance | Wearable | Cueing | Gyroscope, Vibration cue | 10 < n ≤ 20 |
| EEH van Wegen et al. [130] | 2018 | Rehabilitation | Posture, Balance | Wearable | Cueing | Accelerometer, Vibration cue | |
| William Omar Contreras Lopez et al. [131] | 2014 | Rehabilitation | Gait | Wearable | Cueing | Audio cue, Accelerometer | |
| Filippo Casamassima et al. [115] | 2014 | Rehabilitation | Gait | Wearable | Smartphone, Cueing | Accelerometer, Gyroscope, Magnetometer, Audio cue |
| Reference | Year | Application | Aspect Area | Device | Additional Device | Sensor/Actuator | No. of Subjects |
|---|---|---|---|---|---|---|---|
| Daphne G. M. Zwartjes et al. [6] | 2010 | Prognosis/Monitoring Disease Progression | Limb movements, Tremor, Movement disorder | Wearable | Video Recording | Accelerometer, Gyroscope, Video camera | 10 < n ≤ 20 |
| R. Contreras et al. [4] | 2016 | Prognosis/Monitoring Disease Progression | Tremor | Wearable | Smartphone | Accelerometer, Gyroscope | 10 < n ≤ 20 |
| Shaohua Wan et al. [132] | 2018 | Prognosis/Monitoring Disease Progression | Speech topics, ADL | Smartphone | Accelerometer, Microphone | u/k | |
| Luis A. Sanchez-Perez et al. [133] | 2018 | Prognosis/Monitoring Disease Progression | Tremor | Wearable | Accelerometer, Gyroscope, Magnetometer | >30 | |
| M Bächlin et al. [74] | 2010 | Prognosis/Monitoring Disease Progression | Gait, Freezing of Gait | Wearable | Cueing | Accelerometer, Audio cue | ≤10 |
| Àngels Bayés et al. [9] | 2018 | Prognosis/Monitoring Disease Progression | Bradykinesia and Dyskinesia | Wearable | Smartphone | Accelerometer | u/k |
| Arash Salarian et al. [126] | 2010 | Prognosis/Monitoring Disease Progression | Posture, Gait | Wearable | Accelerometer, Gyroscope | 10 < n ≤ 20 | |
| JA Robichaud et al. [134] | 2009 | Prognosis/Monitoring Disease Progression | EMG Signal | Biopotential | EMG | 20 < n ≤ 30 | |
| Mevludin Memedi et al. [135] | 2015 | Prognosis/Monitoring Disease Progression | Handwriting | Other | Touchscreen | >30 | |
| J Dietz et al. [19] | 2013 | Prognosis/Monitoring Disease Progression | Emotions, Depression | Biopotential | EEG | 10 < n ≤ 20 | |
| Lucia Ricciardi et al. [20] | 2015 | Prognosis/Monitoring Disease Progression | Emotions | Video Recording | Video camera | >30 | |
| Shyamal Patel et al. [67] | 2009 | Prognosis/Monitoring Disease Progression | Tremor, Bradykinesia and Dyskinesia | Wearable | Video Recording | Accelerometer, Video camera | 10 < n ≤ 20 |
| Reference | Year | Applicaton | Aspect Area | Device | Additional Device | Sensors | No. of Subjects (n) |
|---|---|---|---|---|---|---|---|
| Jan Raethjen et al. [71] | 2009 | Diagnosis | EEG signals, EMG signals | Biopotential | EEG, EMG | 20 < n ≤ 30 | |
| Mitsuru Yoneyama et al. [55] | 2013 | Diagnosis | Gait | Wearable | Accelerometer | ≤10 | |
| Srivani Padma G et al. [136] | 2015 | Diagnosis | Tremor | Other | Fiber Bragg Grating Tremor Measurement (FBGTM) | u/k | |
| Bin Zhang et al. [72] | 2018 | Diagnosis | Tremor | Biopotential | Wearable | Accelerometer, EMG | >30 |
| VF Annese et al. [137] | 2018 | Diagnosis | Gait, EMG Signal | Biopotential | EMG | ≤10 | |
| A.Iu Meigal et al. [56] | 2009 | Diagnosis | EMG Signal | Biopotential | EMG | 10 < n ≤ 20 | |
| Johannes C Ayena et al. [138] | 2015 | Diagnosis | Balance | Biopotential | Smartphone | Force sensor | 20 < n ≤ 30 |
| R Soubra et al. [139] | 2018 | Diagnosis | Gait | Wearable | Force sensor | u/k | |
| Raffaele Ferri et al. [57] | 2012 | Diagnosis | Sleep Topics | Biopotential | EMG | 20 < n ≤ 30 | |
| Heinrich Garn et al. [18] | 2017 | Diagnosis | Dementia | Biopotential | EEG | >30 | |
| Yolanda Camnos-Roca et al. [58] | 2018 | Diagnosis | Speech Topics | Audio Recording | Microphone | >30 | |
| Athanasios Tsanas et al. [66] | 2012 | Diagnosis | Speech Topics | Audio Recording | Microphone | >30 | |
| Kotsavasiloglou C et al. [140] | 2017 | Diagnosis | Handwriting | Other | Touch screen | 20 < n ≤ 30 | |
| Lidia Ghosh et al. [17] | 2017 | Diagnosis | Cognitive Activity | Biopotential | EEG | 20 < n ≤ 30 | |
| Dung Phan et al. [12] | 2018 | Diagnosis | Bradykinesia and Dyskinesia | Wearable | Accelerometer, Gyroscope | ||
| M. Yokoe et al. [141] | 2009 | Diagnosis | Limb movements | Wearable | Accelerometer, Touch sensor |
References
- The Parkinson’s Foundation. Parkinson’s Foundation: Better Lives Together. Available online: https://bit.ly/2Uc6ikj (accessed on 25 June 2022).
- Marras, C.; Beck, J.; Bower, J.; Roberts, E.; Ritz, B.; Ross, G.; Abbott, R.; Savica, R.; Van Den Eeden, S.; Willis, A.; et al. Prevalence of Parkinson’s disease across North America. NPJ Park. Dis. 2018, 4, 21. [Google Scholar] [CrossRef] [Green Version]
- Harish, K.; Rao, M.V.; Borgohain, R.; Sairam, A.; Abhilash, P. Tremor quantification and its measurements on parkinsonian patients. In Proceedings of the 2009 International Conference on Biomedical and Pharmaceutical Engineering, Singapore, 2–4 December 2009; pp. 1–3. [Google Scholar]
- Contreras, R.; Huerta, M.; Sagbay, G.; LLumiguano, C.; Bravo, M.; Bermeo, A.; Clotet, R.; Soto, A. Tremors quantification in parkinson patients using smartwatches. In Proceedings of the 2016 IEEE Ecuador Technical Chapters Meeting (ETCM), Guayaquil, Ecuador, 12–14 October 2016; pp. 1–6. [Google Scholar]
- Jenkins, M.; Almeida, Q.; Spaulding, S.; Van Oostveen, R.; Holmes, J.; Johnson, A.M.; Perry, S. Plantar cutaneous sensory stimulation improves single-limb support time, and EMG activation patterns among individuals with Parkinson’s disease. Park. Relat. Disord. 2009, 15, 697–702. [Google Scholar] [CrossRef]
- Zwartjes, D.G.; Heida, T.; Van Vugt, J.P.; Geelen, J.A.; Veltink, P.H. Ambulatory monitoring of activities and motor symptoms in Parkinson’s disease. IEEE Trans. Biomed. Eng. 2010, 57, 2778–2786. [Google Scholar] [CrossRef]
- George, J.S.; Strunk, J.; Mak-McCully, R.; Houser, M.; Poizner, H.; Aron, A.R. Dopaminergic therapy in Parkinson’s disease decreases cortical beta band coherence in the resting state and increases cortical beta band power during executive control. NeuroImage Clin. 2013, 3, 261–270. [Google Scholar] [CrossRef] [Green Version]
- Teskey, W.J.; Elhabiby, M.; El-Sheimy, N. Inertial sensing to determine movement disorder motion present before and after treatment. Sensors 2012, 12, 3512–3527. [Google Scholar] [CrossRef] [Green Version]
- Bayés, À.; Samá, A.; Prats, A.; Pérez-López, C.; Crespo-Maraver, M.; Moreno, J.M.; Alcaine, S.; Rodriguez-Molinero, A.; Mestre, B.; Quispe, P.; et al. A “HOLTER” for Parkinson’s disease: Validation of the ability to detect on-off states using the REMPARK system. Gait Posture 2018, 59, 1–6. [Google Scholar] [CrossRef]
- Bhidayasiri, R.; Sringean, J.; Anan, C.; Boonpang, K.; Thanawattano, C.; Chaudhuri, K.R. Quantitative demonstration of the efficacy of night-time apomorphine infusion to treat nocturnal hypokinesia in Parkinson’s disease using wearable sensors. Park. Relat. Disord. 2016, 33, S36–S41. [Google Scholar] [CrossRef]
- Mancini, M.; Salarian, A.; Carlson-Kuhta, P.; Zampieri, C.; King, L.; Chiari, L.; Horak, F.B. ISway: A sensitive, valid and reliable measure of postural control. J. Neuroeng. Rehabil. 2012, 9, 59. [Google Scholar] [CrossRef] [Green Version]
- Phan, D.; Horne, M.; Pathirana, P.; Farzanehfar, P. Measurement of Axial Rigidity and Postural Instability Using Wearable Sensors. Sensors 2018, 18, 495. [Google Scholar] [CrossRef] [Green Version]
- Baram, Y.; Lenger, R. Gait improvement in patients with cerebral palsy by visual and auditory feedback. Neuromodulation Technol. Neural Interface 2012, 15, 48–52. [Google Scholar] [CrossRef]
- Mileti, I.; Germanotta, M.; Alcaro, S.; Pacilli, A.; Imbimbo, I.; Petracca, M.; Erra, C.; Di Sipio, E.; Aprile, I.; Rossi, S.; et al. Gait partitioning methods in Parkinson’s disease patients with motor fluctuations: A comparative analysis. In Proceedings of the 2017 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rochester, MN, USA, 7–10 May 2017; pp. 402–407. [Google Scholar]
- De Lima, A.L.S.; Evers, L.J.; Hahn, T.; Bataille, L.; Hamilton, J.L.; Little, M.A.; Okuma, Y.; Bloem, B.R.; Faber, M.J. Freezing of gait and fall detection in Parkinson’s disease using wearable sensors: A systematic review. J. Neurol. 2017, 264, 1642–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Güntekin, B.; Hanoğlu, L.; Güner, D.; Yılmaz, N.H.; Çadırcı, F.; Mantar, N.; Aktürk, T.; Emek-Savaş, D.D.; Özer, F.F.; Yener, G.; et al. Cognitive impairment in parkinson’s disease is reflected with gradual decrease of EEG delta responses during auditory discrimination. Front. Psychol. 2018, 9, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, L.; Parui, S.; Rakshit, P.; Konar, A. EEG analysis for working memory modeling in face recognition task. In Proceedings of the 2017 Third International Conference on Research in Computational Intelligence and Communication Networks (ICRCICN), Kolkata, India, 3–5 November 2017; pp. 33–38. [Google Scholar]
- Garn, H.; Coronel, C.; Waser, M.; Caravias, G.; Ransmayr, G. Differential diagnosis between patients with probable Alzheimer’s disease, Parkinson’s disease dementia, or dementia with Lewy bodies and frontotemporal dementia, behavioral variant, using quantitative electroencephalographic features. J. Neural Transm. 2017, 124, 569–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietz, J.; Bradley, M.; Jones, J.; Okun, M.; Perlstein, W.; Bowers, D. The late positive potential, emotion and apathy in Parkinson’s disease. Neuropsychologia 2013, 51, 960–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricciardi, L.; Bologna, M.; Morgante, F.; Ricciardi, D.; Morabito, B.; Volpe, D.; Martino, D.; Tessitore, A.; Pomponi, M.; Bentivoglio, A.R.; et al. Reduced facial expressiveness in Parkinson’s disease: A pure motor disorder? J. Neurol. Sci. 2015, 358, 125–130. [Google Scholar] [CrossRef]
- Deb, R. How Does Technology Development Influence the Assessment of Parkinson’s Disease? A Systematic Review. Ph.D. Thesis, Arizona State University, Tempe, AZ, USA, 2019. [Google Scholar]
- Fahn, S. UPDRS Development Comittee. Unified Parkinson’s disease rating scale. Recent Dev. Park. Dis. 1987, 2. [Google Scholar]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. Off. J. Mov. Disord. Soc. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1998, 50, 318. [Google Scholar] [CrossRef]
- Ozanne, A.; Johansson, D.; Hällgren Graneheim, U.; Malmgren, K.; Bergquist, F.; Alt Murphy, M. Wearables in epilepsy and Parkinson’s disease—A focus group study. Acta Neurol. Scand. 2018, 137, 188–194. [Google Scholar] [CrossRef]
- Bhat, G.; Deb, R.; Ogras, U.Y. OpenHealth: Open-source platform for wearable health monitoring. IEEE Des. Test 2019, 36, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Yang, K.; Xiong, W.X.; Liu, F.T.; Sun, Y.M.; Luo, S.; Ding, Z.T.; Wu, J.J.; Wang, J. Objective and quantitative assessment of motor function in Parkinson’s disease—from the perspective of practical applications. Ann. Transl. Med. 2016, 4, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boland, D.F.; Stacy, M. The economic and quality of life burden associated with Parkinson’s disease: A focus on symptoms. Am. J. Manag. Care 2012, 18, S168–S175. [Google Scholar] [PubMed]
- Lukowicz, P.; Kirstein, T.; Tröster, G. Wearable systems for health care applications. Methods Inf. Med. 2004, 43, 232–238. [Google Scholar] [PubMed]
- Nagy, R.B.; Popenţiu-Vlădicescu, F. Exploring the Potential of Internet of Things Systems in Heath Care Context. eLearning Softw. Educ. 2018, 3, 461–468. [Google Scholar]
- Pantelopoulos, A.; Bourbakis, N.G. A survey on wearable sensor-based systems for health monitoring and prognosis. IEEE Trans. Syst. Man, Cybern. Part C Appl. Rev. 2010, 40, 1–12. [Google Scholar] [CrossRef] [Green Version]
- An, S.; Ogras, U.Y. MARS: mmWave-based Assistive Rehabilitation System for Smart Healthcare. ACM Trans. Embed. Comput. Syst. TECS 2021, 20, 1–22. [Google Scholar] [CrossRef]
- An, S.; Tuncel, Y.; Basaklar, T.; Krishnakumar, G.K.; Bhat, G.; Ogras, U.Y. Mgait: Model-based gait analysis using wearable bend and inertial sensors. ACM Trans. Internet Things 2021, 3, 1–24. [Google Scholar] [CrossRef]
- Bhat, G.; Tuncel, Y.; An, S.; Lee, H.G.; Ogras, U.Y. An ultra-low energy human activity recognition accelerator for wearable health applications. ACM Trans. Embed. Comput. Syst. TECS 2019, 18, 1–22. [Google Scholar] [CrossRef]
- Bhat, G.; Tuncel, Y.; An, S.; Ogras, U.Y. Wearable IoT Devices for Health Monitoring; TechConnect Briefs: Boston, MA, USA, 2019; pp. 357–360. [Google Scholar]
- Basaklar, T.; Tuncel, Y.; An, S.; Ogras, U. Wearable devices and low-power design for smart health applications: Challenges and opportunities. In Proceedings of the 2021 IEEE/ACM International Symposium on Low Power Electronics and Design (ISLPED), Boston, MA, USA, 26–28 July 2021. [Google Scholar]
- An, S.; Ogras, U.Y. Fast and Scalable Human Pose Estimation using mmWave Point Cloud. arXiv 2022, arXiv:2205.00097. [Google Scholar]
- Volpe, D.; Pavan, D.; Morris, M.; Guiotto, A.; Iansek, R.; Fortuna, S.; Frazzitta, G.; Sawacha, Z. Underwater gait analysis in Parkinson’s disease. Gait Posture 2017, 52, 87–94. [Google Scholar] [CrossRef]
- Volpe, D.; Spolaor, F.; Sawacha, Z.; Guiotto, A.; Pavan, D.; Bakdounes, L.; Urbani, V.; Frazzitta, G.; Iansek, R. Muscular activation changes in lower limbs after underwater gait training in Parkinson’s disease: A surface emg pilot study. Gait Posture 2020, 80, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Hale, L.A.; Pal, J.; Becker, I. Measuring free-living physical activity in adults with and without neurologic dysfunction with a triaxial accelerometer. Arch. Phys. Med. Rehabil. 2008, 89, 1765–1771. [Google Scholar] [CrossRef] [PubMed]
- Aubin, P.M.; Serackis, A.; Griskevicius, J. Support Vector Machine Classification of Parkinson’s Disease, Essential Tremor and Healthy Control Subjects Based on Upper Extremity Motion. In Proceedings of the 2012 International Conference on Biomedical Engineering and Biotechnology, Macau, Macao, 28–30 May 2012; pp. 900–904. [Google Scholar]
- Jeon, H.; Lee, W.; Park, H.; Lee, H.; Kim, S.; Kim, H.; Jeon, B.; Park, K. Automatic classification of tremor severity in Parkinson’s disease using a wearable device. Sensors 2017, 17, 2067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.C.; Hsu, Y.L.; Shih, K.S.; Lu, J.M. Real-time gait cycle parameter recognition using a wearable accelerometry system. Sensors 2011, 11, 7314–7326. [Google Scholar] [CrossRef] [Green Version]
- Mustufa, Y.A.; Barton, J.; O’Flynn, B.; Davies, R.; McCullagh, P.; Zheng, H. Design of a smart insole for ambulatory assessment of gait. In Proceedings of the 2015 IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Cambridge, MA, USA, 9–12 June 2015; pp. 1–5. [Google Scholar]
- Sijobert, B.; Azevedo-Coste, C.; Andreu, D.; Verna, C.; Geny, C. Effects of sensitive electrical stimulation based cueing in Parkinson’s disease: A preliminary study. Eur. J. Transl. Myol. 2016, 26, 6018. [Google Scholar] [CrossRef] [Green Version]
- Espay, A.J.; Bonato, P.; Nahab, F.B.; Maetzler, W.; Dean, J.M.; Klucken, J.; Eskofier, B.M.; Merola, A.; Horak, F.; Lang, A.E.; et al. Technology in Parkinson’s disease: Challenges and opportunities. Mov. Disord. 2016, 31, 1272–1282. [Google Scholar] [CrossRef] [Green Version]
- Godinho, C.; Domingos, J.; Cunha, G.; Santos, A.T.; Fernandes, R.M.; Abreu, D.; Gonçalves, N.; Matthews, H.; Isaacs, T.; Duffen, J.; et al. A systematic review of the characteristics and validity of monitoring technologies to assess Parkinson’s disease. J. Neuroeng. Rehabil. 2016, 13, 24. [Google Scholar] [CrossRef] [Green Version]
- Rovini, E.; Maremmani, C.; Cavallo, F. How wearable sensors can support Parkinson’s disease diagnosis and treatment: A systematic review. Front. Neurosci. 2017, 11, 555. [Google Scholar] [CrossRef]
- Hasan, H.; Athauda, D.S.; Foltynie, T.; Noyce, A.J. Technologies assessing limb bradykinesia in Parkinson’s disease. J. Park. Dis. 2017, 7, 65–77. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, M.M.; Pai, V.M.; Conroy, R.S. Recent advances in wearable sensors for health monitoring. IEEE Sens. J. 2015, 15, 3119–3126. [Google Scholar] [CrossRef]
- Butt, A.H.; Rovini, E.; Esposito, D.; Rossi, G.; Maremmani, C.; Cavallo, F. Biomechanical parameter assessment for classification of Parkinson’s disease on clinical scale. Int. J. Distrib. Sens. Netw. 2017, 13, 1550147717707417. [Google Scholar] [CrossRef] [Green Version]
- Daneault, J.F. Could wearable and mobile technology improve the Management of essential tremor? Front. Neurol. 2018, 9, 257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vienne, A.; Barrois, R.P.; Buffat, S.; Ricard, D.; Vidal, P.P. Inertial sensors to assess gait quality in patients with neurological disorders: A systematic review of technical and analytical challenges. Front. Psychol. 2017, 8, 817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassubek, J. Diagnostic procedures during the course of Parkinson’s Disease. Basal Ganglia 2014, 4, 15–18. [Google Scholar] [CrossRef]
- Yoneyama, M.; Kurihara, Y.; Watanabe, K.; Mitoma, H. Accelerometry-Based gait analysis and its application to parkinson’s disease assessment—Part 2: A new measure for quantifying walking behavior. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 999–1005. [Google Scholar] [CrossRef]
- Meigal, A.I.; Rissanen, S.; Tarvainen, M.; Karjalainen, P.; Iudina-Vassel, I.; Airaksinen, O.; Kankaanpää, M. Novel parameters of surface EMG in patients with Parkinson’s disease and healthy young and old controls. J. Electromyogr. Kinesiol. 2009, 19, e206–e213. [Google Scholar] [CrossRef]
- Ferri, R.; Fulda, S.; Cosentino, F.I.; Pizza, F.; Plazzi, G. A preliminary quantitative analysis of REM sleep chin EMG in Parkinson’s disease with or without REM sleep behavior disorder. Sleep Med. 2012, 13, 707–713. [Google Scholar] [CrossRef]
- Camnos-Roca, Y.; Calle-Alonso, F.; Perez, C.J.; Naranjo, L. Computational Diagnosis of Parkinson’s Disease from Speech Based on Regularization Methods. In Proceedings of the 2018 26th European Signal Processing Conference (EUSIPCO), Rome, Italy, 3–7 September 2018; pp. 1127–1131. [Google Scholar]
- Stone, A.A.; Shiffman, S.; Schwartz, J.E.; Broderick, J.E.; Hufford, M.R. Patient compliance with paper and electronic diaries. Control. Clin. Trials 2003, 24, 182–199. [Google Scholar] [CrossRef]
- Papapetropoulos, S. Patient diaries as a clinical endpoint in Parkinson’s disease clinical trials. CNS Neurosci. Ther. 2012, 18, 380–387. [Google Scholar] [CrossRef]
- Forte, R.; Tocci, N.; De Vito, G. The Impact of Exercise Intervention with Rhythmic Auditory Stimulation to Improve Gait and Mobility in Parkinson Disease: An Umbrella Review. Brain Sci. 2021, 11, 685. [Google Scholar] [CrossRef]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Marques, G.; Villasana, M.V.; Garcia, N.M.; Zdravevski, E.; Spinsante, S. Identification of diseases based on the use of inertial sensors: A systematic review. Electronics 2020, 9, 778. [Google Scholar] [CrossRef]
- Bhat, G.; Tran, N.; Shill, H.; Ogras, U.Y. w-HAR: An Activity Recognition Dataset and Framework Using Low-Power Wearable Devices. Sensors 2020, 20, 5356. [Google Scholar] [CrossRef] [PubMed]
- Lachat, E.; Macher, H.; Landes, T.; Grussenmeyer, P. Assessment and calibration of a RGB-D camera (Kinect v2 Sensor) towards a potential use for close-range 3D modeling. Remote Sens. 2015, 7, 13070–13097. [Google Scholar] [CrossRef] [Green Version]
- Vicon. Vicon Motion Capture System. Available online: https://www.vicon.com (accessed on 25 June 2022).
- Tsanas, A.; Little, M.A.; McSharry, P.E.; Spielman, J.; Ramig, L.O. Novel speech signal processing algorithms for high-accuracy classification of Parkinson’s disease. IEEE Trans. Biomed. Eng. 2012, 59, 1264–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, S.; Lorincz, K.; Hughes, R.; Huggins, N.; Growdon, J.; Standaert, D.; Akay, M.; Dy, J.; Welsh, M.; Bonato, P. Monitoring motor fluctuations in patients with Parkinson’s disease using wearable sensors. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 864–873. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a knowledge representation for clinical questions. In AMIA Annual Symposium Proceedings; American Medical Informatics Association: Rockville, ML, USA, 2006; Volume 2006, p. 359. [Google Scholar]
- Sánchez-Ferro, Á.; Elshehabi, M.; Godinho, C.; Salkovic, D.; Hobert, M.A.; Domingos, J.; Van Uem, J.M.; Ferreira, J.J.; Maetzler, W. New methods for the assessment of Parkinson’s disease (2005 to 2015): A systematic review. Mov. Disord. 2016, 31, 1283–1292. [Google Scholar] [CrossRef]
- Raethjen, J.; Govindan, R.; Muthuraman, M.; Kopper, F.; Volkmann, J.; Deuschl, G. Cortical correlates of the basic and first harmonic frequency of Parkinsonian tremor. Clin. Neurophysiol. 2009, 120, 1866–1872. [Google Scholar] [CrossRef]
- Zhang, B.; Huang, F.; Liu, J.; Zhang, D. A Novel Posture for Better Differentiation Between Parkinson’s Tremor and Essential Tremor. Front. Neurosci. 2018, 12, 317. [Google Scholar] [CrossRef]
- Salarian, A.; Horak, F.B.; Zampieri, C.; Carlson-Kuhta, P.; Nutt, J.G.; Aminian, K. iTUG, a sensitive and reliable measure of mobility. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 303–310. [Google Scholar] [CrossRef] [Green Version]
- Bächlin, M.; Plotnik, M.; Roggen, D.; Maidan, I.; Hausdorff, J.M.; Giladi, N.; Tröster, G. Wearable assistant for Parkinson’s disease patients with the freezing of gait symptom. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 436–446. [Google Scholar] [CrossRef]
- Herz, D.M.; Siebner, H.R.; Hulme, O.J.; Florin, E.; Christensen, M.S.; Timmermann, L. Levodopa reinstates connectivity from prefrontal to premotor cortex during externally paced movement in Parkinson’s disease. Neuroimage 2014, 90, 15–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruonala, V.; Pekkonen, E.; Airaksinen, O.; Kankaanpää, M.; Karjalainen, P.A.; Rissanen, S.M. levodopa-induced changes in electromyographic Patterns in Patients with advanced Parkinson’s Disease. Front. Neurol. 2018, 9, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rigas, G.; Bougia, P.; Baga, D.; Tsipouras, M.; Tzallas, A.; Tripoliti, E.; Tsouli, S.; Chondrogiorgi, M.; Konitsiotis, S.; Fotiadis, D.I. A decision support tool for optimal Levodopa administration in Parkinson’s disease. In Proceedings of the 10th IEEE International Conference on Information Technology and Applications in Biomedicine, Corfu, Greece, 3–5 November 2010; pp. 1–6. [Google Scholar]
- Pelicioni, P.H.; Brodie, M.A.; Latt, M.D.; Menant, J.C.; Menz, H.B.; Fung, V.S.; Lord, S.R. Head and trunk stability during gait before and after levodopa intake in Parkinson’s disease subtypes. Exp. Gerontol. 2018, 111, 78–85. [Google Scholar] [CrossRef]
- Fatmehsari, Y.R.; Bahrami, F. Lempel-ziv complexity criteria for nonlinear analysis of gait in patients with parkinson’s disease. In Proceedings of the 2011 18th Iranian Conference of Biomedical Engineering (ICBME), Tehran, Iran, 14–16 December 2011; pp. 137–141. [Google Scholar]
- Basaklar, T.; Tuncel, Y.; Ogras, U.Y. Subject-Independent Freezing of Gait (FoG) Prediction in Parkinson’s Disease Patients. In Proceedings of the 2021 IEEE Biomedical Circuits and Systems Conference (BioCAS), Berlin, Germany, 7–9 October 2021; pp. 1–6. [Google Scholar]
- Chomiak, T.; Watts, A.; Meyer, N.; Pereira, F.V.; Hu, B. A training approach to improve stepping automaticity while dual-tasking in Parkinson’s disease: A prospective pilot study. Medicine 2017, 96, e5934. [Google Scholar] [CrossRef] [PubMed]
- Young, W.R.; Shreve, L.; Quinn, E.J.; Craig, C.; Bronte-Stewart, H. Auditory cueing in Parkinson’s patients with freezing of gait. What matters most: Action-relevance or cue-continuity? Neuropsychologia 2016, 87, 54–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jovanov, E.; Wang, E.; Verhagen, L.; Fredrickson, M.; Fratangelo, R. deFOG—A real time system for detection and unfreezing of gait of Parkinson’s patients. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 5151–5154. [Google Scholar]
- Moore, S.T.; MacDougall, H.G.; Ondo, W.G. Ambulatory monitoring of freezing of gait in Parkinson’s disease. J. Neurosci. Methods 2008, 167, 340–348. [Google Scholar] [CrossRef]
- Vidya, V.; Poornachandran, P.; Sujadevi, V.; Dharmana, M.M. Suppressing Parkinson’s diseases induced involuntary movements using wearables. In Proceedings of the 2017 International Conference on Technological Advancements in Power and Energy (TAP Energy), Kollam, India, 21–23 December 2017; pp. 1–4. [Google Scholar]
- Nijssen, P.C.; Brekelmans, G.J.; Roos, R.A. Electroencephalography in autosomal dominant adult neuronal ceroid lipofuscinosis. Clin. Neurophysiol. 2009, 120, 1782–1786. [Google Scholar] [CrossRef] [PubMed]
- Fogelson, N.; Fernandez-del Olmo, M.; Santos-Garcia, D. Contextual processing deficits in Parkinson’s disease: The role of the frontostriatal system. Clin. Neurophysiol. 2011, 122, 539–545. [Google Scholar] [CrossRef]
- Casula, E.P.; Bassi, M.S.; Pellicciari, M.C.; Ponzo, V.; Veniero, D.; Peppe, A.; Brusa, L.; Stanzione, P.; Caltagirone, C.; Stefani, A.; et al. Subthalamic stimulation and levodopa modulate cortical reactivity in Parkinson’s patients. Park. Relat. Disord. 2017, 34, 31–37. [Google Scholar] [CrossRef]
- Brazète, J.R.; Gagnon, J.F.; Postuma, R.B.; Bertrand, J.A.; Petit, D.; Montplaisir, J. Electroencephalogram slowing predicts neurodegeneration in rapid eye movement sleep behavior disorder. Neurobiol. Aging 2016, 37, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Margis, R.; Schönwald, S.V.; Carvalho, D.Z.; Gerhardt, G.J.; Rieder, C.R. NREM sleep alpha and sigma activity in Parkinson’s disease: Evidence for conflicting electrophysiological activity? Clin. Neurophysiol. 2015, 126, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Christensen, J.A.; Zoetmulder, M.; Koch, H.; Frandsen, R.; Arvastson, L.; Christensen, S.R.; Jennum, P.; Sorensen, H.B. Data-driven modeling of sleep EEG and EOG reveals characteristics indicative of pre-Parkinson’s and Parkinson’s disease. J. Neurosci. Methods 2014, 235, 262–276. [Google Scholar] [CrossRef] [PubMed]
- Utianski, R.L.; Caviness, J.N.; van Straaten, E.C.; Beach, T.G.; Dugger, B.N.; Shill, H.A.; Driver-Dunckley, E.D.; Sabbagh, M.N.; Mehta, S.; Adler, C.H.; et al. Graph theory network function in Parkinson’s disease assessed with electroencephalography. Clin. Neurophysiol. 2016, 127, 2228–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javaid, M.; Amassian, V.; Glazman, S.; Fesharaki, A.; Stefanov, D.; Bodis-Wollner, I. Cortical control of voluntary saccades in Parkinson’s disease and pre-emptive perception. Park. Relat. Disord. 2012, 18, S100–S103. [Google Scholar] [CrossRef]
- Caliandro, P.; Ferrarin, M.; Cioni, M.; Bentivoglio, A.R.; Minciotti, I.; D’urso, P.; Tonali, P.A.; Padua, L. Levodopa effect on electromyographic activation patterns of tibialis anterior muscle during walking in Parkinson’s disease. Gait Posture 2011, 33, 436–441. [Google Scholar] [CrossRef]
- Powell, D.; Threlkeld, A.J.; Fang, X.; Muthumani, A.; Xia, R. Amplitude-and velocity-dependency of rigidity measured at the wrist in Parkinson’s disease. Clin. Neurophysiol. 2012, 123, 764–773. [Google Scholar] [CrossRef] [Green Version]
- Dionisio, V.C.; de Biagi Curtarelli, M.; de Souza, L.A.P.S. Sitting movement in elderly subjects with and without Parkinson’s disease: A biomechanical study. J. Electromyogr. Kinesiol. 2013, 23, 948–957. [Google Scholar] [CrossRef]
- Athukorala, R.P.; Jones, R.D.; Sella, O.; Huckabee, M.L. Skill training for swallowing rehabilitation in patients with Parkinson’s disease. Arch. Phys. Med. Rehabil. 2014, 95, 1374–1382. [Google Scholar] [CrossRef]
- Margraf, N.G.; Rogalski, M.; Deuschl, G.; Kuhtz-Buschbeck, J.P. Trunk muscle activation pattern in parkinsonian camptocormia as revealed with surface electromyography. Park. Relat. Disord. 2017, 44, 44–50. [Google Scholar] [CrossRef]
- Kiyono, K.; Hayano, J.; Kwak, S.; Watanabe, E.; Yamamoto, Y. Non-Gaussianity of low frequency heart rate variability and sympathetic activation: Lack of increases in multiple system atrophy and Parkinson disease. Front. Physiol. 2012, 3, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbasi, O.; Hirschmann, J.; Storzer, L.; Özkurt, T.E.; Elben, S.; Vesper, J.; Wojtecki, L.; Schmitz, G.; Schnitzler, A.; Butz, M. Unilateral deep brain stimulation suppresses alpha and beta oscillations in sensorimotor cortices. Neuroimage 2018, 174, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Lohnes, C.A.; Earhart, G.M. Saccadic eye movements are related to turning performance in Parkinson disease. J. Park. Dis. 2011, 1, 109–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hossen, A.; Muthuraman, M.; Raethjen, J.; Deuschl, G.; Heute, U. Discrimination of Parkinsonian tremor from essential tremor by implementation of a wavelet-based soft-decision technique on EMG and accelerometer signals. Biomed. Signal Process. Control 2010, 5, 181–188. [Google Scholar] [CrossRef]
- Rissanen, S.M.; Kankaanpää, M.; Tarvainen, M.P.; Meigal, A.Y.; Nuutinen, J.; Tarkka, I.M.; Airaksinen, O.; Karjalainen, P.A. Analysis of dynamic voluntary muscle contractions in Parkinson’s disease. IEEE Trans. Biomed. Eng. 2009, 56, 2280–2288. [Google Scholar] [CrossRef]
- Boroojerdi, B.; Ghaffari, R.; Mahadevan, N.; Markowitz, M.; Melton, K.; Morey, B.; Otoul, C.; Patel, S.; Phillips, J.; Sen-Gupta, E.; et al. Clinical feasibility of a wearable, conformable sensor patch to monitor motor symptoms in Parkinson’s disease. Park. Relat. Disord. 2018, 60, 70–76. [Google Scholar] [CrossRef]
- Lalo, E.; Riff, J.; Parry, R.; Jabloun, M.; Roussel, J.; Chen, C.C.; Welter, M.L.; Buttelli, O. Design of technology and technology of design. Activity analysis as a resource for a personalised approach for patients with Parkinson disease. IRBM 2016, 37, 90–97. [Google Scholar] [CrossRef] [Green Version]
- Zhao, A.; Qi, L.; Li, J.; Dong, J.; Yu, H. A hybrid spatio-temporal model for detection and severity rating of Parkinson’s Disease from gait data. Neurocomputing 2018, 315, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Medeiros, L.; Almeida, H.; Dias, L.; Perkusich, M.; Fischer, R. A Gait Analysis Approach to Track Parkinson’s Disease Evolution Using Principal Component Analysis. In Proceedings of the 2016 IEEE 29th International Symposium on Computer-Based Medical Systems (CBMS), Belfast and Dublin, Ireland, 20–24 June 2016; pp. 48–53. [Google Scholar]
- Jamthe, A.; Chakraborty, S.; Ghosh, S.K.; Agrawal, D.P. An implementation of wireless sensor network in monitoring of parkinson’s patients using received signal strength indicator. In Proceedings of the 2013 IEEE International Conference on Distributed Computing in Sensor Systems, Cambridge, MA, USA, 20–23 May 2013; pp. 442–447. [Google Scholar]
- Lee, C.N.; Fong, V.H.; Chu, Y.T.; Cheng, L.; Chuang, H.W.; Lo, C.Y. A Wearable Device Of Gait Tracking For Parkinson’S Disease Patients. In Proceedings of the 2018 International Conference on Machine Learning and Cybernetics (ICMLC), Chengdu, China, 15–18 July 2018; Volume 2, pp. 462–466. [Google Scholar]
- Niazmand, K.; Tonn, K.; Kalaras, A.; Fietzek, U.M.; Mehrkens, J.H.; Lueth, T.C. Quantitative evaluation of Parkinson’s disease using sensor based smart glove. In Proceedings of the 2011 24th International Symposium on Computer-Based Medical Systems (CBMS), Bristol, UK, 27–30 June 2011; pp. 1–8. [Google Scholar]
- Daliri, M.R. Chi-square distance kernel of the gaits for the diagnosis of Parkinson’s disease. Biomed. Signal Process. Control 2013, 8, 66–70. [Google Scholar] [CrossRef]
- Baby, M.S.; Saji, A.; Kumar, C.S. Parkinsons disease classification using wavelet transform based feature extraction of gait data. In Proceedings of the 2017 International Conference on Circuit, Power and Computing Technologies (ICCPCT), Kollam, India, 20–21 April 2017; pp. 1–6. [Google Scholar]
- Orlosky, J.; Itoh, Y.; Ranchet, M.; Kiyokawa, K.; Morgan, J.; Devos, H. Emulation of physician tasks in eye-tracked virtual reality for remote diagnosis of neurodegenerative disease. IEEE Trans. Vis. Comput. Graph. 2017, 23, 1302–1311. [Google Scholar] [CrossRef]
- Buated, W.; Sriyudthsak, M.; Sribunruangrit, N.; Bhidayasiri, R. A low-cost intervention for improving gait in Parknson’s disease patients: A cane providing visual cues. Eur. Geriatr. Med. 2012, 3, 126–130. [Google Scholar] [CrossRef]
- Casamassima, F.; Ferrari, A.; Milosevic, B.; Ginis, P.; Farella, E.; Rocchi, L. A wearable system for gait training in subjects with Parkinson’s disease. Sensors 2014, 14, 6229–6246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Costa Capato, T.T.; Tornai, J.; Ávila, P.; Barbosa, E.R.; Piemonte, M.E.P. Randomized controlled trial protocol: Balance training with rhythmical cues to improve and maintain balance control in Parkinson’s disease. BMC Neurol. 2015, 15, 162. [Google Scholar]
- Ringenbach, S.D.; Van Gemmert, A.W.; Shill, H.A.; Stelmach, G.E. Auditory instructional cues benefit unimanual and bimanual drawing in Parkinson’s disease patients. Hum. Mov. Sci. 2011, 30, 770–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenzi, P.; Rao, R.; Romano, G.; Kita, A.; Serpa, M.; Filesi, F.; Irrera, F.; Bologna, M.; Suppa, A.; Berardelli, A. Smart sensors for the recognition of specific human motion disorders in Parkinson’s disease. In Proceedings of the 2015 6th International Workshop on Advances in Sensors and Interfaces (IWASI), Gallipoli, Italy, 18–19 June 2015; pp. 131–136. [Google Scholar]
- Pepa, L.; Capecci, M.; Verdini, F.; Ceravolo, M.G.; Spalazzi, L. An architecture to manage motor disorders in Parkinson’s disease. In Proceedings of the 2015 IEEE 2nd World Forum on Internet of Things (WF-IoT), Milan, Italy, 14–16 December 2015; pp. 615–620. [Google Scholar]
- McCandless, P.J.; Evans, B.J.; Janssen, J.; Selfe, J.; Churchill, A.; Richards, J. Effect of three cueing devices for people with Parkinson’s disease with gait initiation difficulties. Gait Posture 2016, 44, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Cando, O.A.; Hidalgo, K.R.; Palacios, B.C. A low-cost vibratory stimulus system to mitigate freezing of gait in Parkinson’s disease. In Proceedings of the 2016 IEEE ANDESCON, Arequipa, Peru, 19–21 October 2016; pp. 1–4. [Google Scholar]
- Fung, A.; Lai, E.C.; Lee, B.C. Usability and Validation of the Smarter Balance System: An Unsupervised Dynamic Balance Exercises System for Individuals With Parkinson’s Disease. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 798–806. [Google Scholar] [CrossRef]
- Most, N. Metapub. PyPI. Available online: https://pypi.org/project/metapub/ (accessed on 25 June 2022).
- Tabbal, S.D.; Ushe, M.; Mink, J.W.; Revilla, F.J.; Wernle, A.R.; Hong, M.; Karimi, M.; Perlmutter, J.S. Unilateral subthalamic nucleus stimulation has a measurable ipsilateral effect on rigidity and bradykinesia in Parkinson disease. Exp. Neurol. 2008, 211, 234–242. [Google Scholar] [CrossRef] [Green Version]
- Rissanen, S.M.; Ruonala, V.; Pekkonen, E.; Kankaanpää, M.; Airaksinen, O.; Karjalainen, P.A. Signal features of surface electromyography in advanced Parkinson’s disease during different settings of deep brain stimulation. Clin. Neurophysiol. 2015, 126, 2290–2298. [Google Scholar] [CrossRef] [Green Version]
- Ginis, P.; Pirani, R.; Basaia, S.; Ferrari, A.; Chiari, L.; Heremans, E.; Canning, C.G.; Nieuwboer, A. Focusing on heel strike improves toe clearance in people with Parkinson’s disease: An observational pilot study. Physiotherapy 2017, 103, 485–490. [Google Scholar] [CrossRef]
- Vasquez-Correa, J.C.; Arias-Vergara, T.; Orozco-Arroyave, J.; Eskofier, B.M.; Klucken, J.; Noth, E. Multimodal assessment of Parkinson’s disease: A deep learning approach. IEEE J. Biomed. Health Inform. 2018, 23, 1618–1630. [Google Scholar] [CrossRef]
- Shah, S.H.; Iqbal, K.; Riaz, A. Constrained Optimization-Based Extreme Learning Machines with Bagging for Freezing of Gait Detection. Big Data Cogn. Comput. 2018, 2, 31. [Google Scholar] [CrossRef] [Green Version]
- Nanhoe-Mahabier, W.; Allum, J.; Pasman, E.; Overeem, S.; Bloem, B. The effects of vibrotactile biofeedback training on trunk sway in Parkinson’s disease patients. Park. Relat. Disord. 2012, 18, 1017–1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Wegen, E.; de Goede, C.; Kwakkel, G.; van Kordelaar, J. Sensor assisted self-management in Parkinson’s disease: A feasibility study of ambulatory posture detection and feedback to treat stooped posture. Park. Relat. Disord. 2018, 46, S57–S61. [Google Scholar] [CrossRef] [PubMed]
- Lopez, W.O.C.; Higuera, C.A.E.; Fonoff, E.T.; de Oliveira Souza, C.; Albicker, U.; Martinez, J.A.E. Listenmee® and Listenmee® smartphone application: Synchronizing walking to rhythmic auditory cues to improve gait in Parkinson’s disease. Hum. Mov. Sci. 2014, 37, 147–156. [Google Scholar] [CrossRef]
- Wan, S.; Liang, Y.; Zhang, Y.; Guizani, M. Deep multi-layer perceptron classifier for behavior analysis to estimate parkinson’s disease severity using smartphones. IEEE Access 2018, 6, 36825–36833. [Google Scholar] [CrossRef]
- Sanchez-Perez, L.A.; Sanchez-Fernandez, L.P.; Shaout, A.; Martinez-Hernandez, J.M.; Alvarez-Noriega, M.J. Rest tremor quantification based on fuzzy inference systems and wearable sensors. Int. J. Med. Inform. 2018, 114, 6–17. [Google Scholar] [CrossRef]
- Robichaud, J.A.; Pfann, K.D.; Leurgans, S.; Vaillancourt, D.E.; Comella, C.L.; Corcos, D.M. Variability of EMG patterns: A potential neurophysiological marker of Parkinson’s disease? Clin. Neurophysiol. 2009, 120, 390–397. [Google Scholar] [CrossRef] [Green Version]
- Memedi, M.; Sadikov, A.; Groznik, V.; Žabkar, J.; Možina, M.; Bergquist, F.; Johansson, A.; Haubenberger, D.; Nyholm, D. Automatic spiral analysis for objective assessment of motor symptoms in Parkinson’s disease. Sensors 2015, 15, 23727–23744. [Google Scholar] [CrossRef]
- Umesh, S.; Asokan, U.; Srinivas, T. Parkinsonian hand Tremor Measurement device based on Fiber Bragg Grating sensor. In Proceedings of the 2015 International Conference on Smart Sensors and Systems (IC-SSS), Bangalore, India, 21–23 December 2015; pp. 1–3. [Google Scholar]
- Annese, V.; Mezzina, G.; Gallo, V.; Scarola, V.; De Venuto, D. Wearable platform for automatic recognition of Parkinson Disease by muscular implication monitoring. In Proceedings of the 2017 7th IEEE International Workshop on Advances in Sensors and Interfaces (IWASI), Vieste, Italy, 15–16 June 2017; pp. 150–154. [Google Scholar]
- Ayena, J.C.; Otis, M.J.; Menelas, B.A. An efficient home-based risk of falling assessment test based on Smartphone and instrumented insole. In Proceedings of the 2015 IEEE International Symposium on Medical Measurements and Applications (MeMeA) Proceedings, Turin, Italy, 7–9 May 2015; pp. 416–421. [Google Scholar]
- Soubra, R.; Diab, M.O.; Moslem, B. Identification of Parkinson’s disease by using multichannel Vertical Ground Reaction Force signals. In Proceedings of the 2016 International Conference on Bio-engineering for Smart Technologies (BioSMART), Dubai, United Arab Emirates, 4–7 December 2016; pp. 1–4. [Google Scholar]
- Kotsavasiloglou, C.; Kostikis, N.; Hristu-Varsakelis, D.; Arnaoutoglou, M. Machine learning-based classification of simple drawing movements in Parkinson’s disease. Biomed. Signal Process. Control 2017, 31, 174–180. [Google Scholar] [CrossRef]
- Yokoe, M.; Okuno, R.; Hamasaki, T.; Kurachi, Y.; Akazawa, K.; Sakoda, S. Opening velocity, a novel parameter, for finger tapping test in patients with Parkinson’s disease. Park. Relat. Disord. 2009, 15, 440–444. [Google Scholar] [CrossRef]













| Motor Signs and Symptoms | Non-Motor Signs and Symptoms | Mixed Signs and Symptoms |
|---|---|---|
| Gait | EEG abnormalities | |
| Limb movements | Cognitive activity | |
| EMG abnormalities | Depression | |
| FoG | Dementia | |
| Tremor | Heart rate | Speech topics |
| Activities of Daily Living (ADL) | Emotions | Swallowing |
| Bradykinesia and Dyskinesia | Fatigue | |
| Posture | Sleep topics | |
| Balance | Blinking | |
| Nocturnal Hypokinesia | Facial expression | |
| Handwriting | Breath | |
| Saccades | Cortical activity |
| Database | Query | Years | Hits |
|---|---|---|---|
| Pubmed Central | parkinson [Body-Key Terms] OR parkinson [Abstract] OR parkinson [Title] | 2008–2021 | 14,898 |
| Science Direct | “parkinson” in Abstract OR Keyword OR Title | 2008–2021 | 12,216 |
| IEEE Xplore | “parkinson” in Abstract OR Keyword OR Title | 2008–2021 | 2564 |
| MDPI | “parkinson” in Abstract OR Keyword OR Title | 2008–2021 | 2040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deb, R.; An, S.; Bhat, G.; Shill, H.; Ogras, U.Y. A Systematic Survey of Research Trends in Technology Usage for Parkinson’s Disease. Sensors 2022, 22, 5491. https://doi.org/10.3390/s22155491
Deb R, An S, Bhat G, Shill H, Ogras UY. A Systematic Survey of Research Trends in Technology Usage for Parkinson’s Disease. Sensors. 2022; 22(15):5491. https://doi.org/10.3390/s22155491
Chicago/Turabian StyleDeb, Ranadeep, Sizhe An, Ganapati Bhat, Holly Shill, and Umit Y. Ogras. 2022. "A Systematic Survey of Research Trends in Technology Usage for Parkinson’s Disease" Sensors 22, no. 15: 5491. https://doi.org/10.3390/s22155491