
Development of Intraoperative Near-Infrared Fluorescence Imaging System Using a Dual-CMOS Single Camera

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
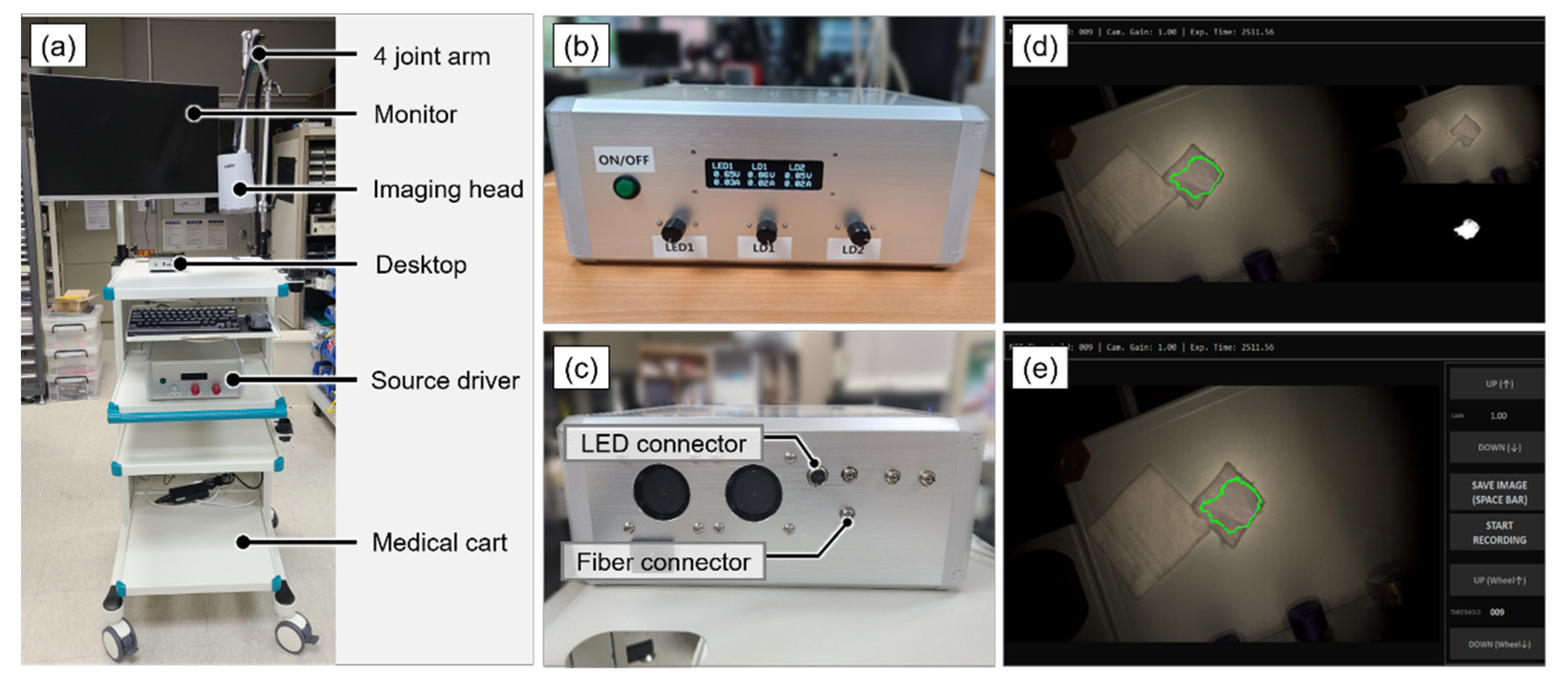
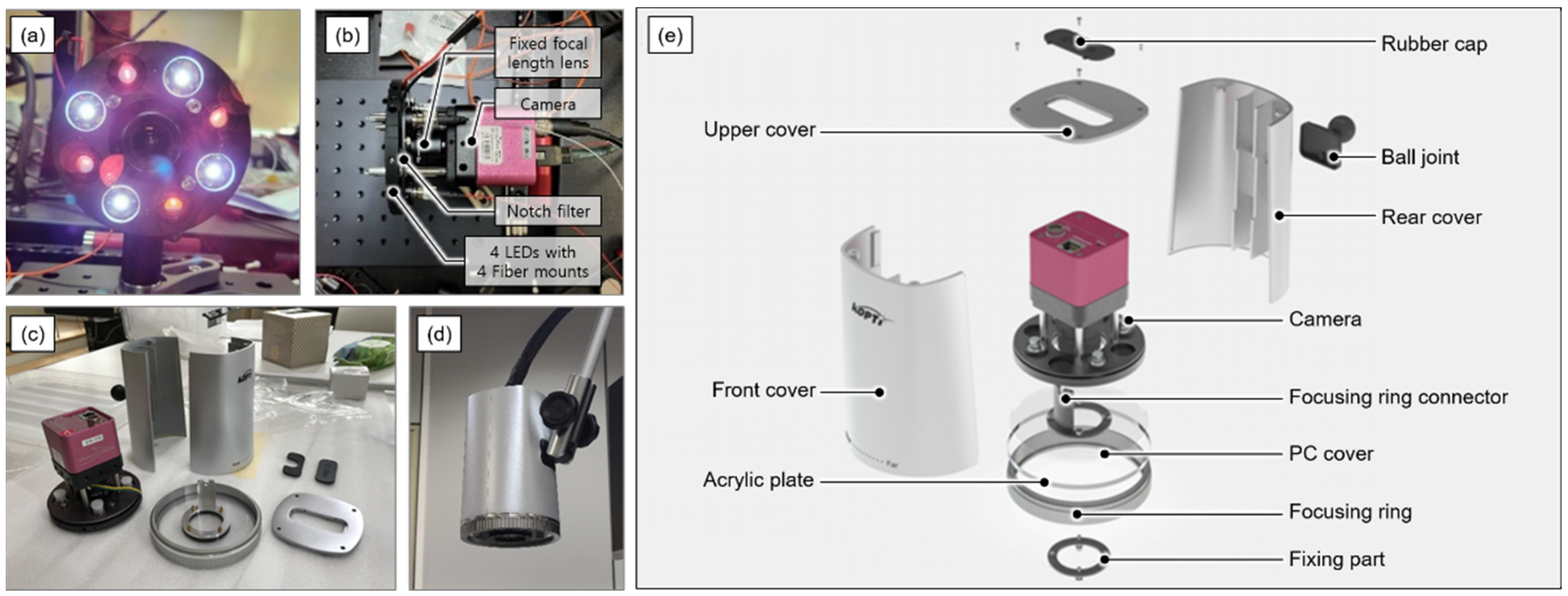
2.1. System Design and Development
2.2. System Characterization
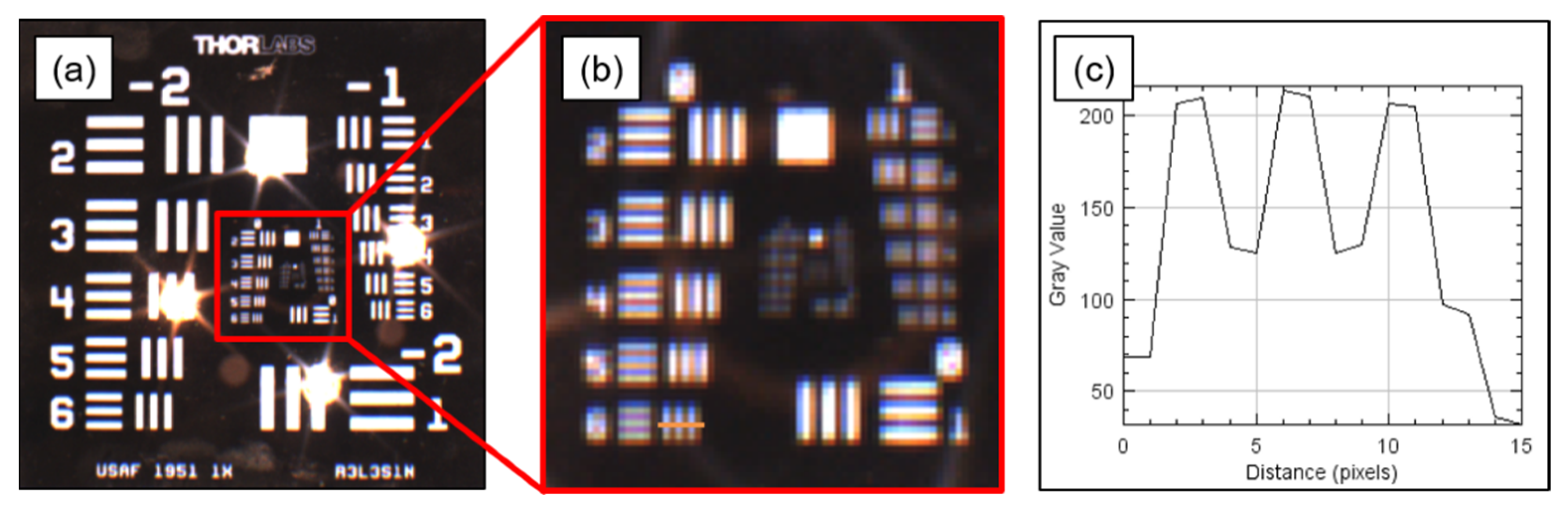
2.2.1. Optical Characteristics
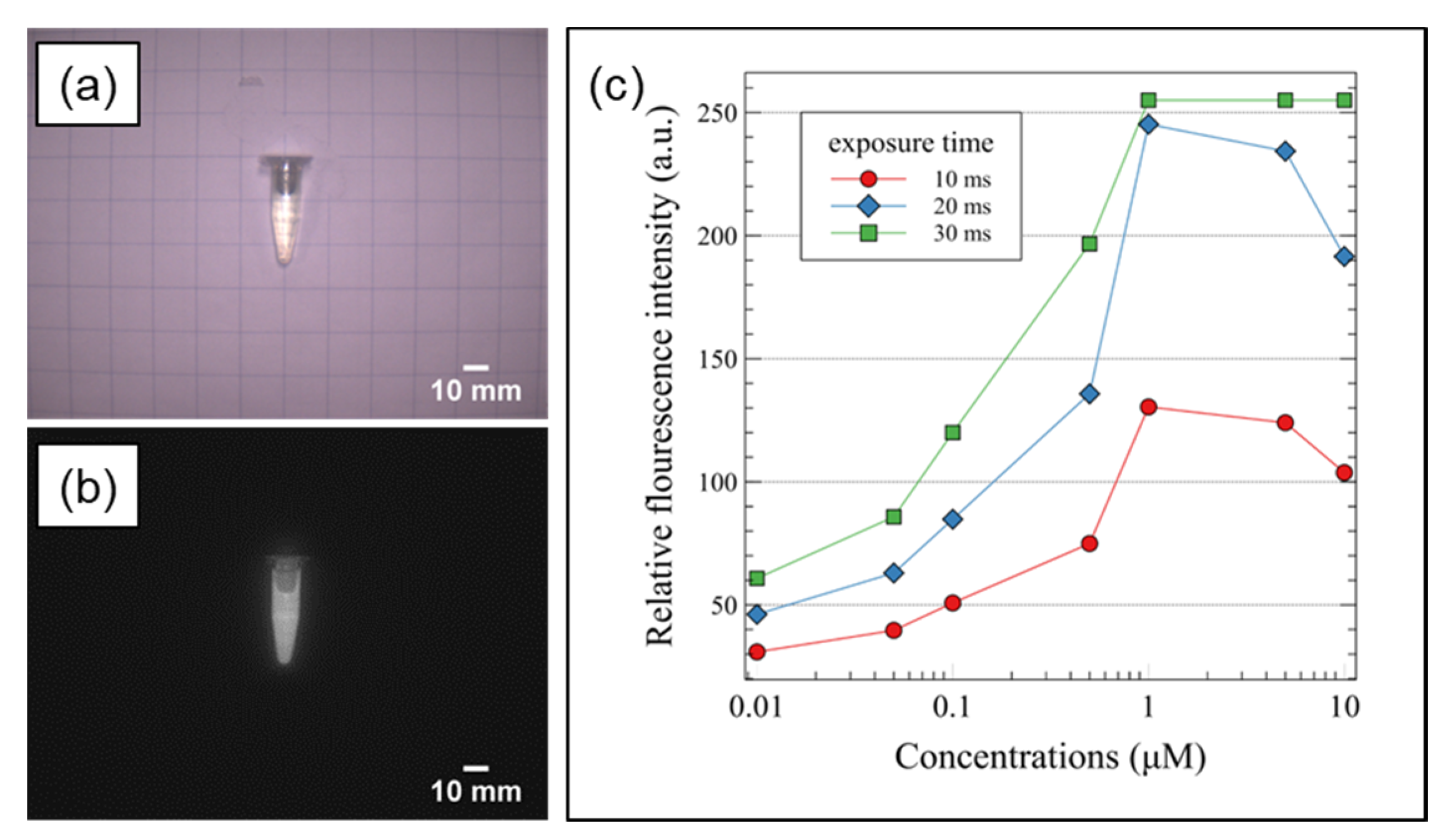
2.2.2. Sensitivity and Signal-to-Background Ratio (SBR)
2.2.3. Laser Diode Safety Test
2.3. In Vivo Imaging Test
3. Results
3.1. System Characteristics
3.1.1. Optical Characteristics
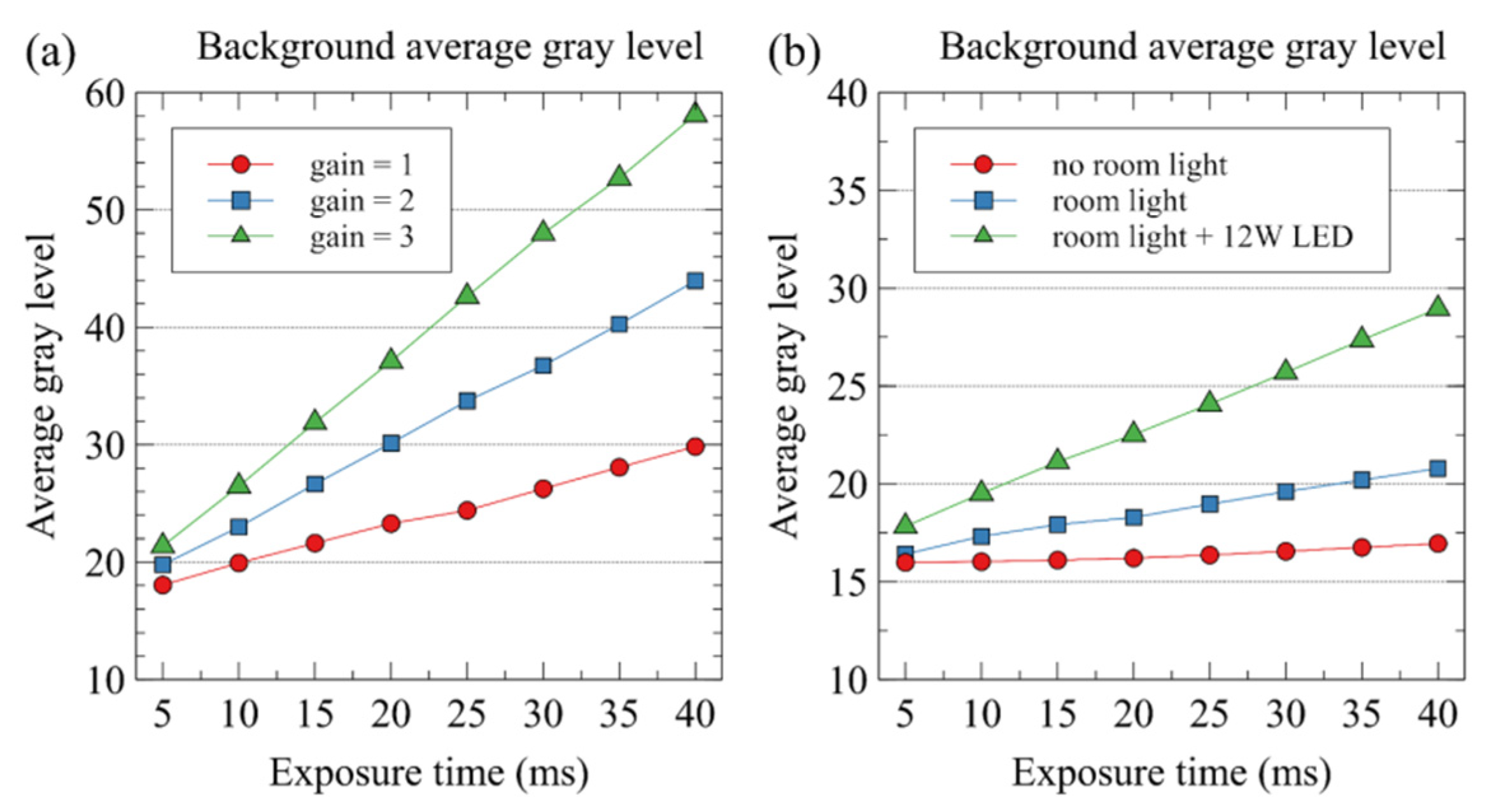
3.1.2. Sensitivity
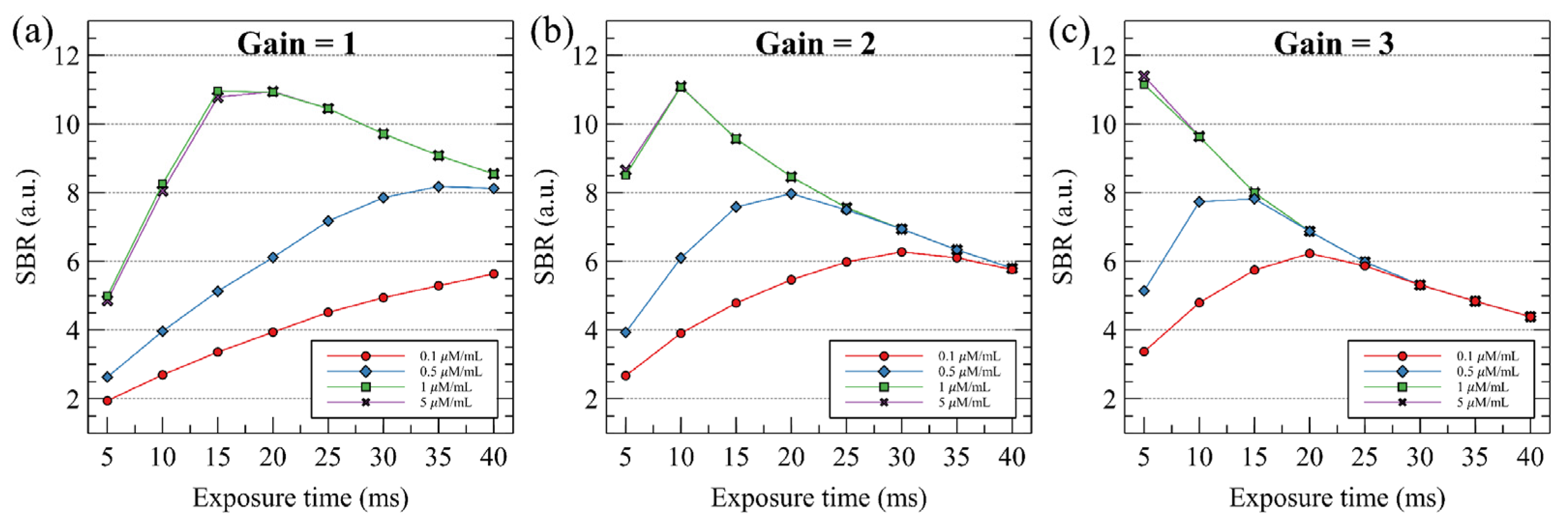
3.1.3. Signal-to-background Ratio (SBR)
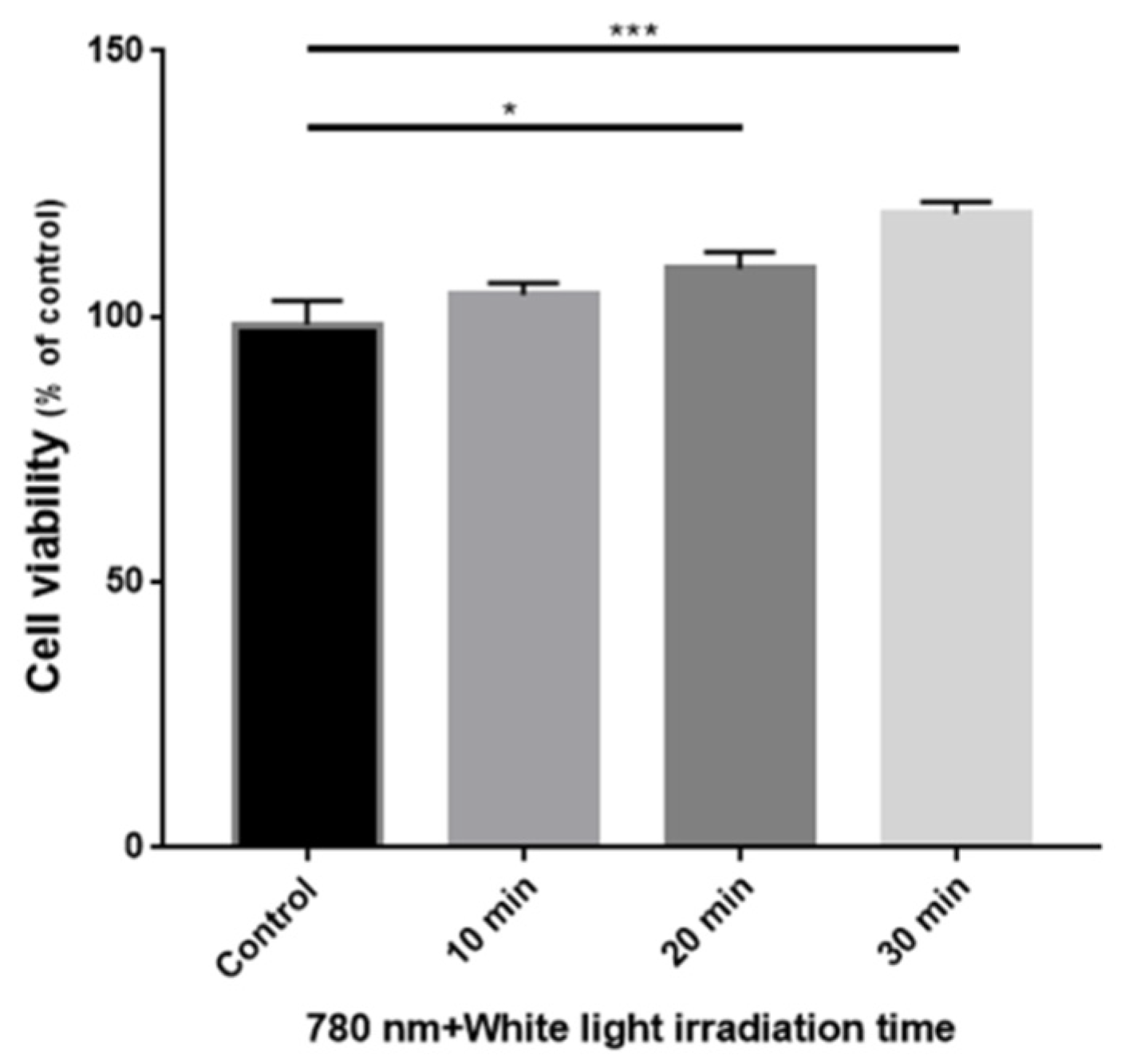
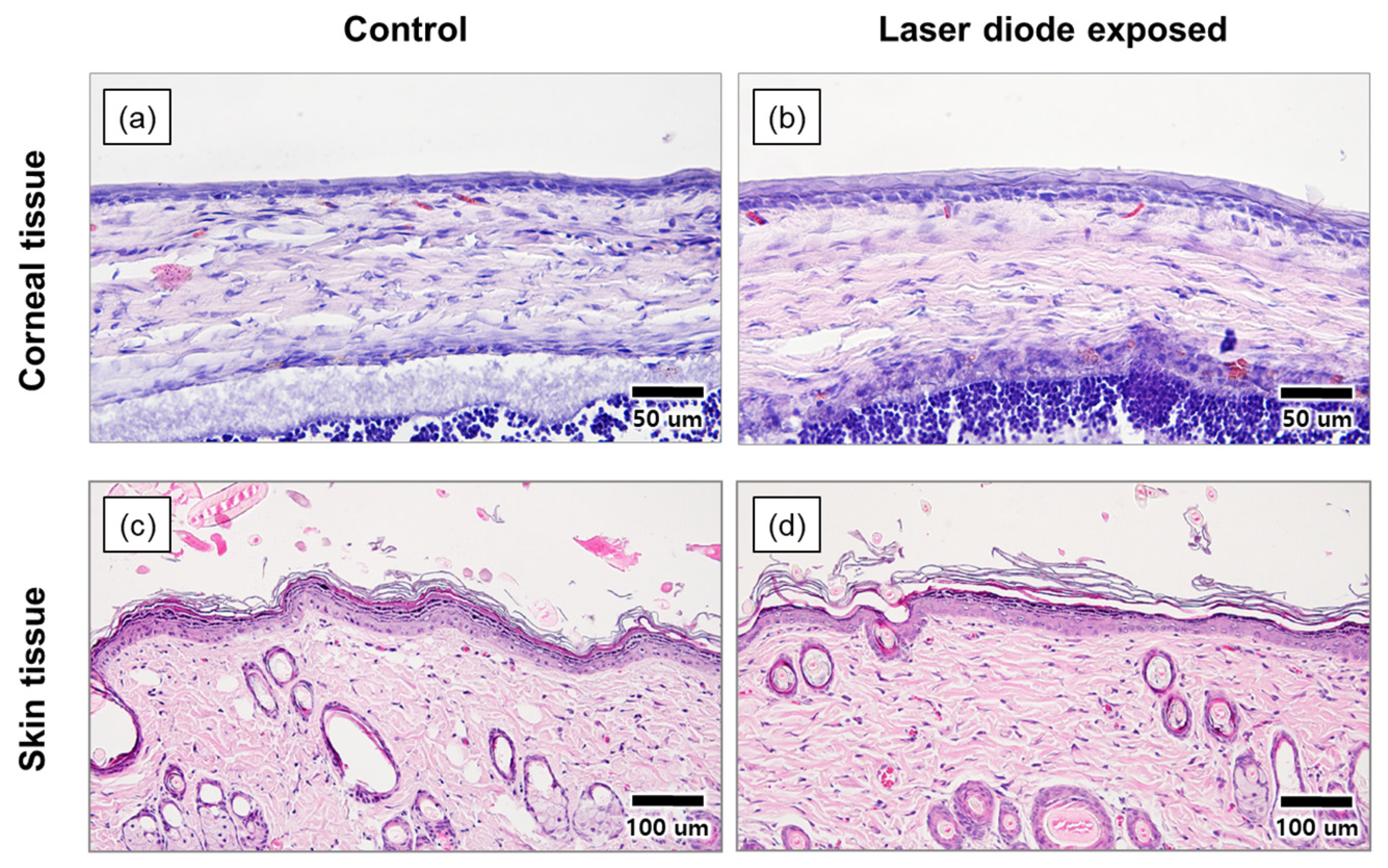
3.1.4. Laser Diode Safety Test
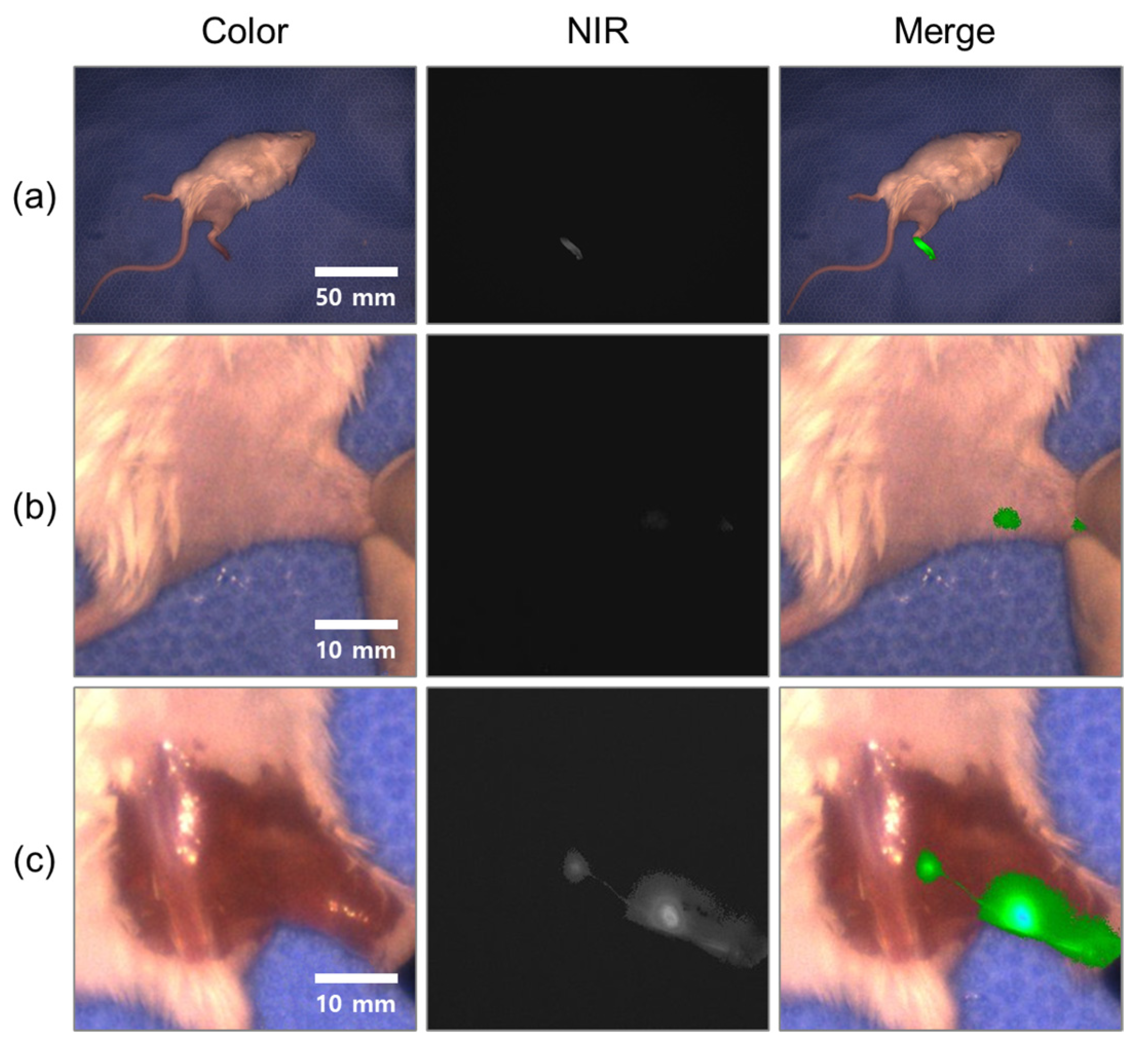
3.2. In Vivo Imaging
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fujimoto, J.G.; Pitris, C.; Boppart, S.A.; Brezinski, M.E. Optical Coherence Tomography: An Emerging Technology for Biomedical Imaging and Optical Biopsy. Neoplasia 2000, 2, 9–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, M.; Wang, L.V. Photoacoustic imaging in biomedicine. Rev. Sci. Instrum. 2006, 77, 041101. [Google Scholar] [CrossRef] [Green Version]
- Sarikaya, I.; Povoski, S.P.; Al-Saif, O.H.; Kocak, E.; Bloomston, M.; March, S.; Cao, Z.; Murrey, D.A.; Zhang, J.; Hall, N.C.; et al. Combined use of preoperative 18 F FDG-PET imaging and intraoperative gamma probe detection for accurate assessment of tumor recurrence in patients with colorectal cancer. World J. Surg. Oncol. 2007, 5, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valdés Olmos, R.A.; Vidal-Sicart, S.; Nieweg, O.E. SPECT-CT and Real-Time Intraoperative Imaging: New Tools for Sentinel Node Localization and Radioguided Surgery? Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Troyan, S.L.; Kianzad, V.; Gibbs-Strauss, S.L.; Gioux, S.; Matsui, A.; Oketokoun, R.; Ngo, L.; Khamene, A.; Azar, F.; Frangioni, J.V. The FLARETM Intraoperative Near-Infrared Fluorescence Imaging System: A First-in-Human Clinical Trial in Breast Cancer Sentinel Lymph Node Mapping. Ann. Surg. Oncol. 2009, 16, 2943–2952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Themelis, G.; Yoo, J.S.; Soh, K.; Schulz, R.B.; Ntziachristos, V. Real-Time Intraoperative Fluorescence Imaging System Using Light-Absorption Correction. J. Biomed. Opt. 2009, 14, 064012. [Google Scholar] [CrossRef] [Green Version]
- DSouza, A.V.; Lin, H.; Henderson, E.R.; Samkoe, K.S.; Pogue, B.W. Review of Fluorescence Guided Surgery Systems: Identification of Key Performance Capabilities beyond Indocyanine Green Imaging. J. Biomed. Opt. 2016, 21, 080901. [Google Scholar] [CrossRef]
- Kitai, T.; Inomoto, T.; Miwa, M.; Shikayama, T. Fluorescence Navigation with Indocyanine Green for Detecting Sentinel Lymph Nodes in Breast Cancer. Breast Cancer 2005, 12, 211–215. [Google Scholar] [CrossRef]
- Tagaya, N.; Yamazaki, R.; Nakagawa, A.; Abe, A.; Hamada, K.; Kubota, K.; Oyama, T. Intraoperative Identification of Sentinel Lymph Nodes by Near-Infrared Fluorescence Imaging in Patients with Breast Cancer. Am. J. Surg. 2008, 195, 850–853. [Google Scholar] [CrossRef]
- Verbeek, F.P.R.; Troyan, S.L.; Mieog, J.S.D.; Liefers, G.-J.; Moffitt, L.A.; Rosenberg, M.; Hirshfield-Bartek, J.; Gioux, S.; van de Velde, C.J.H.; Vahrmeijer, A.L.; et al. Near-Infrared Fluorescence Sentinel Lymph Node Mapping in Breast Cancer: A Multicenter Experience. Breast Cancer Res. Treat. 2014, 143, 333–342. [Google Scholar] [CrossRef] [Green Version]
- Hutteman, M.; van der Vorst, J.R.; Gaarenstroom, K.N.; Peters, A.A.W.; Mieog, J.S.D.; Schaafsma, B.E.; Löwik, C.W.G.M.; Frangioni, J.V.; van de Velde, C.J.H.; Vahrmeijer, A.L. Optimization of Near-Infrared Fluorescent Sentinel Lymph Node Mapping for Vulvar Cancer. Am. J. Obstet. Gynecol. 2012, 206, 89.e1–89.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Vorst, J.R.; Schaafsma, B.E.; Verbeek, F.P.R.; Swijnenburg, R.J.; Hutteman, M.; Liefers, G.J.; van de Velde, C.J.H.; Frangioni, J.V.; Vahrmeijer, A.L. Dose Optimization for Near-Infrared Fluorescence Sentinel Lymph Node Mapping in Patients with Melanoma: Dose Optimization for Melanoma SLN Mapping. Br. J. Dermatol. 2013, 168, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Schaafsma, B.E.; Verbeek, F.P.R.; Elzevier, H.W.; Tummers, Q.R.J.G.; van der Vorst, J.R.; Frangioni, J.V.; van de Velde, C.J.H.; Pelger, R.C.M.; Vahrmeijer, A.L. Optimization of Sentinel Lymph Node Mapping in Bladder Cancer Using Near-Infrared Fluorescence Imaging: Optimizing SLN Biopsy in Bladder Cancer. J. Surg. Oncol. 2014, 110, 845–850. [Google Scholar] [CrossRef] [Green Version]
- Sound, S.; Okoh, A.; Yigitbas, H.; Yazici, P.; Berber, E. Utility of Indocyanine Green Fluorescence Imaging for Intraoperative Localization in Reoperative Parathyroid Surgery. Surg. Innov. 2015, 26, 774–779. [Google Scholar] [CrossRef]
- Angell, J.E.; Khemees, T.A.; Abaza, R. Optimization of Near Infrared Fluorescence Tumor Localization during Robotic Partial Nephrectomy. J. Urol. 2013, 190, 1668–1673. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.E.; Tummers, W.S.; Teraphongphom, N.; van den Berg, N.S.; Hasan, A.; Ertsey, R.D.; Nagpal, S.; Recht, L.D.; Plowey, E.D.; Vogel, H.; et al. First-in-Human Intraoperative near-Infrared Fluorescence Imaging of Glioblastoma Using Cetuximab-IRDye800. J. Neurooncol. 2018, 139, 135–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbeek, F.P.R.; Schaafsma, B.E.; Tummers, Q.R.J.G.; van der Vorst, J.R.; van der Made, W.J.; Baeten, C.I.M.; Bonsing, B.A.; Frangioni, J.V.; van de Velde, C.J.H.; Vahrmeijer, A.L.; et al. Optimization of Near-Infrared Fluorescence Cholangiography for Open and Laparoscopic Surgery. Surg. Endosc. 2014, 28, 1076–1082. [Google Scholar] [CrossRef]
- Lee, B.T.; Matsui, A.; Hutteman, M.; Lin, S.J.; Winer, J.H.; Laurence, R.G.; Frangioni, J.V. Intraoperative Near-Infrared Fluorescence Imaging in Perforator Flap Reconstruction: Current Research and Early Clinical Experience. J. Reconstr. Microsurg. 2010, 26, 59–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Zhu, N.; Pacheco, S.; Wang, X.; Liang, R. Single Camera Imaging System for Color and Near-Infrared Fluorescence Image Guided Surgery. Biomed. Opt. Express 2014, 5, 2791–2797. [Google Scholar] [CrossRef] [Green Version]
- Boddington, S.; Sutton, E.J.; Jones, E.; Purcell, D.D.; Henning, T.D.; Tavri, S.; Meier, R.; Sista, A.; Fu, Y.; Daldrup-Link, H. Improved Fluorescence of Indocyanine Green in Vitro and in Vivo after Simple Cooling Procedures. Contrast Media Mol. Imaging 2008, 3, 191–197. [Google Scholar] [CrossRef]
- Engel, E.; Schraml, R.; Maisch, T.; Kobuch, K.; König, B.; Szeimies, R.-M.; Hillenkamp, J.; Bäumler, W.; Vasold, R. Light-Induced Decomposition of Indocyanine Green. Investig. Ophthalmol. Vis. Sci. 2008, 49, 1777–1783. [Google Scholar] [CrossRef] [PubMed]
- Geralde, M.C.; Geralde, M.C.; Pratavieira, S.; Bagnato, V.S. Stability of Indocyanine Green for Clinical Use. In Proceedings of the Medical Laser Applications and Laser-Tissue Interactions VIII, Munich, Germany, 25 June 2017; SPIE: Bellingham, WA, USA, 2017; p. 104170S. [Google Scholar]
- O’Hare, S.; Atterwill, C.K. (Eds.) Vitro Toxicity Testing Protocols; Humana Press: Totowa, NJ, USA, 1995. [Google Scholar]
- Borlan, R.; Focsan, M.; Maniu, D.; Astilean, S. Interventional NIR Fluorescence Imaging of Cancer: Review on Next Generation of Dye-Loaded Protein-Based Nanoparticles for Real-Time Feedback during Cancer Surgery. Int. J. Nanomed. 2021, 16, 2147–2171. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Bai, G.; Zeng, S.; Hao, J. Theranostic Carbon Dots with Innovative NIR-II Emission for in Vivo Renal-Excreted Optical Imaging and Photothermal Therapy. ACS Appl. Mater. Interfaces 2019, 11, 4737–4744. [Google Scholar] [CrossRef] [PubMed]
- Šafranko, S.; Stanković, A.; Hajra, S.; Kim, H.-J.; Strelec, I.; Dutour-Sikirić, M.; Weber, I.; Bosnar, M.H.; Grbčić, P.; Pavelić, S.K.; et al. Preparation of Multifunctional N-Doped Carbon Quantum Dots from Citrus clementina Peel: Investigating Targeted Pharmacological Activities and the Potential Application for Fe3+ Sensing. Pharmaceuticals 2021, 14, 857. [Google Scholar] [CrossRef]
- Kong, S.-H.; Bae, S.-W.; Suh, Y.-S.; Lee, H.-J.; Yang, H.-K. Near-Infrared Fluorescence Lymph Node Navigation Using Indocyanine Green for Gastric Cancer Surgery. J. Minim. Invasive Surg. 2018, 21, 95–105. [Google Scholar] [CrossRef] [Green Version]
- van den Bos, J.; Al-Taher, M.; Schols, R.M.; van Kuijk, S.; Bouvy, N.D.; Stassen, L.P.S. Near-Infrared Fluorescence Imaging for Real-Time Intraoperative Guidance in Anastomotic Colorectal Surgery: A Systematic Review of Literature. J. Laparoendosc Adv. Surg. Tech. 2018, 28, 157–167. [Google Scholar] [CrossRef]
- Steinbacher, J.; Yoshimatsu, H.; Meng, S.; Hamscha, U.M.; Chan, C.-S.; Weninger, W.J.; Wu, C.-T.; Cheng, M.-H.; Tzou, C.-H.J. Visualization of Skin Perfusion by Indocyanine Green Fluorescence Angiography—A Feasibility Study. Plast Reconstr. Surg. Glob. Open 2017, 5, e1455. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.; Shin, J.G.; Kwon, H.-S.; Tak, Y.-O.; Park, H.J.; Ahn, J.-C.; Eom, J.B.; Seo, Y.; Park, J.W.; Choi, Y.; et al. Development of Intraoperative Near-Infrared Fluorescence Imaging System Using a Dual-CMOS Single Camera. Sensors 2022, 22, 5597. https://doi.org/10.3390/s22155597
Choi J, Shin JG, Kwon H-S, Tak Y-O, Park HJ, Ahn J-C, Eom JB, Seo Y, Park JW, Choi Y, et al. Development of Intraoperative Near-Infrared Fluorescence Imaging System Using a Dual-CMOS Single Camera. Sensors. 2022; 22(15):5597. https://doi.org/10.3390/s22155597
Chicago/Turabian StyleChoi, Janghoon, Jun Geun Shin, Hyuk-Sang Kwon, Yoon-Oh Tak, Hyeong Ju Park, Jin-Chul Ahn, Joo Beom Eom, Youngseok Seo, Jin Woo Park, Yongdoo Choi, and et al. 2022. "Development of Intraoperative Near-Infrared Fluorescence Imaging System Using a Dual-CMOS Single Camera" Sensors 22, no. 15: 5597. https://doi.org/10.3390/s22155597