
Validation of Non-Restrictive Inertial Gait Analysis of Individuals with Incomplete Spinal Cord Injury in Clinical Settings


Abstract
:1. Introduction
2. Materials and Methods
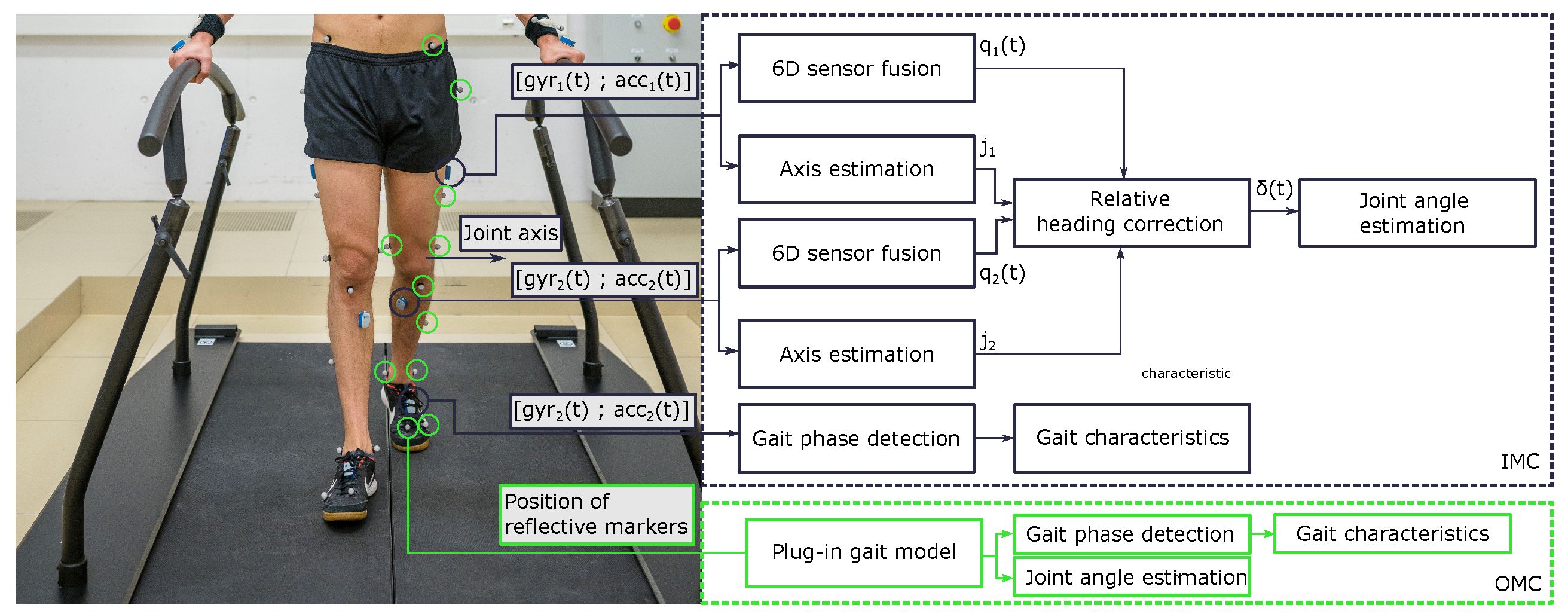
2.1. Measurement System
2.2. Participants
2.3. Data Collection
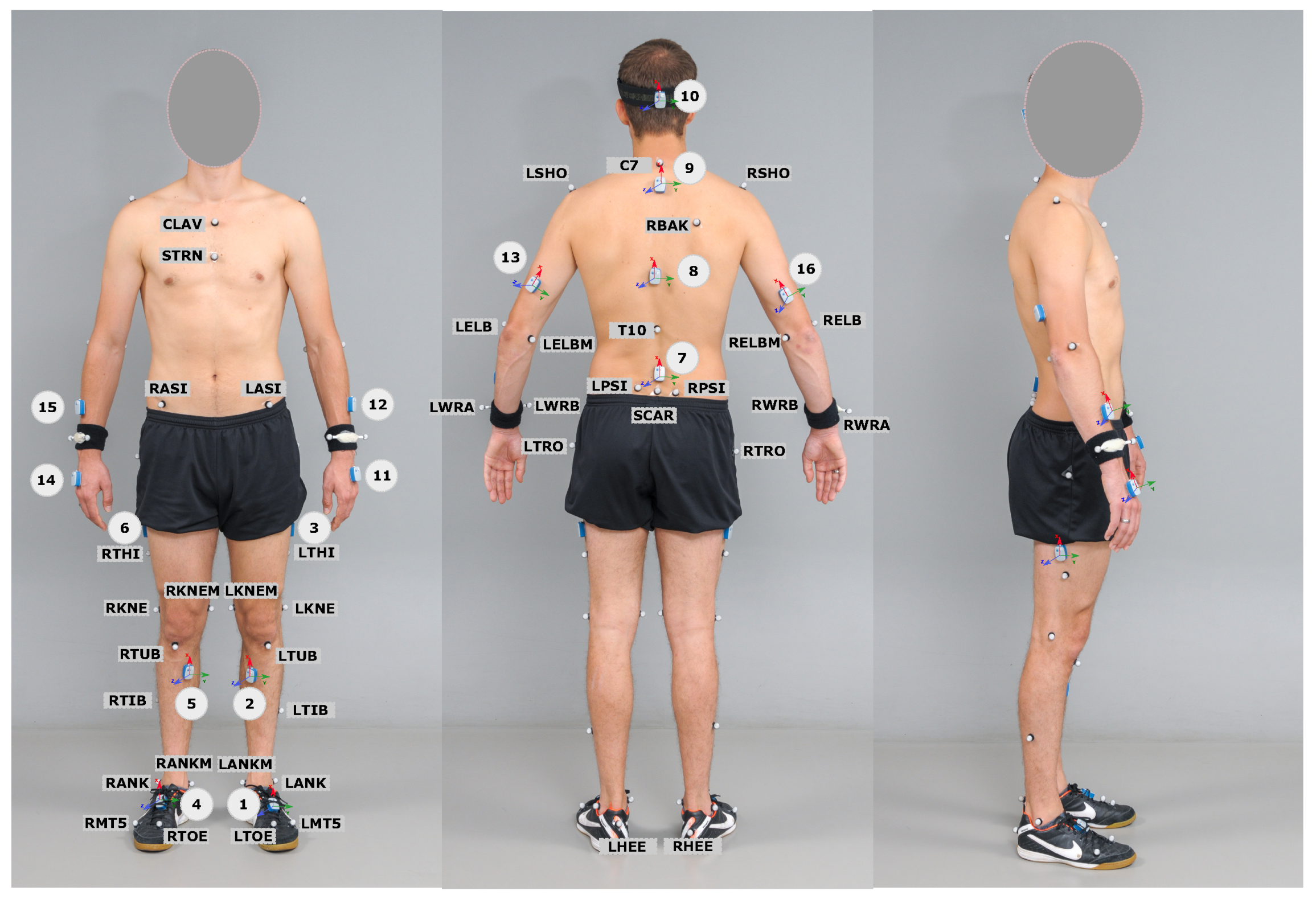
2.3.1. Preparation Procedure—OMC Setup
2.3.2. Preparation Procedure—IMC Setup
2.4. Data Processing and Analysis
2.4.1. Extraction of Temporal and Kinematic Gait Characteristics—OMC System
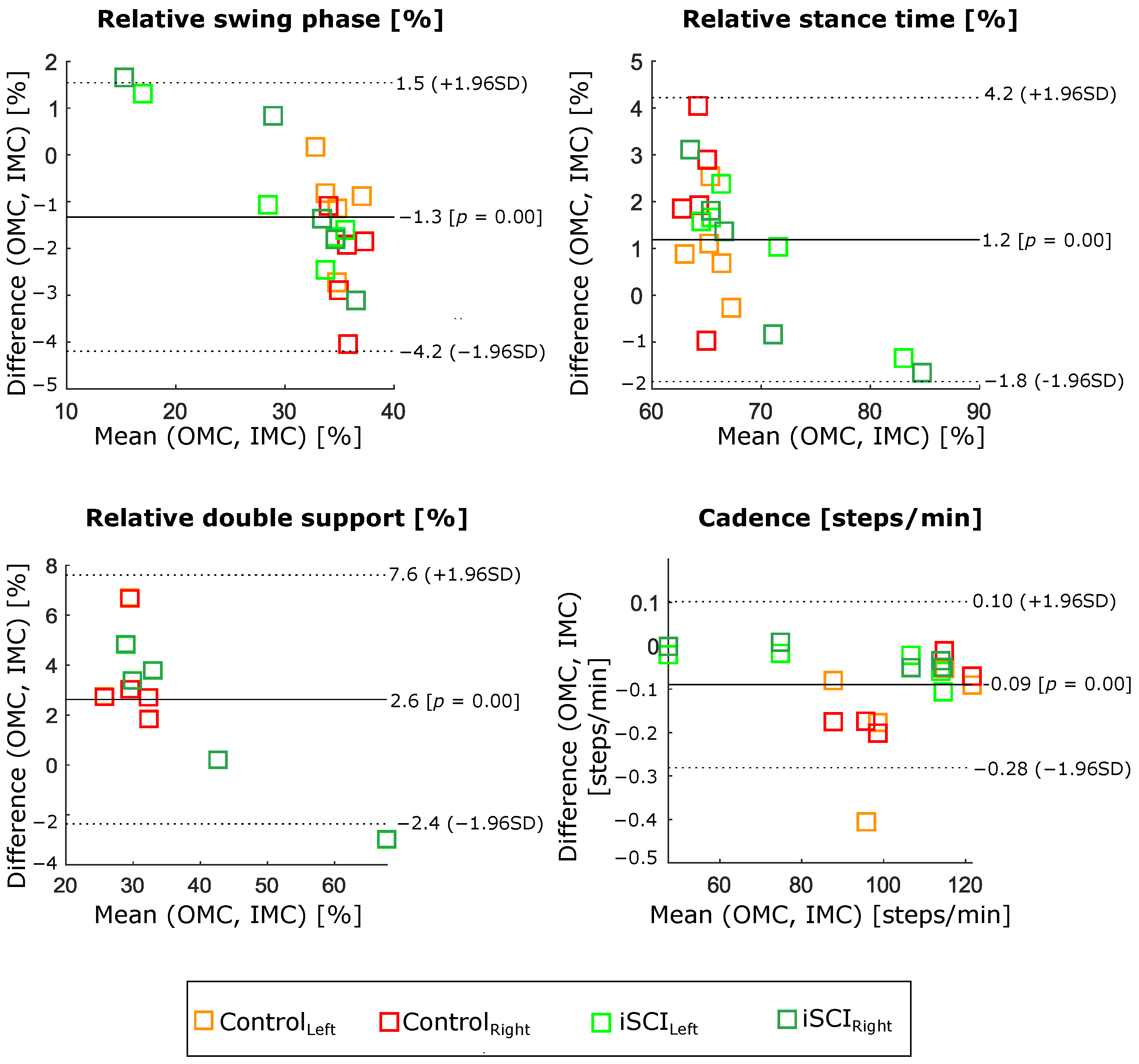
2.4.2. Gait Temporal Characteristics—IMC System
- Relative swing phase: swing phase time/stride time;
- Relative stance phase: stance phase time/stride time;
- Relative double support phase: double support time/stride time;
- Cadence: number of steps/minute.
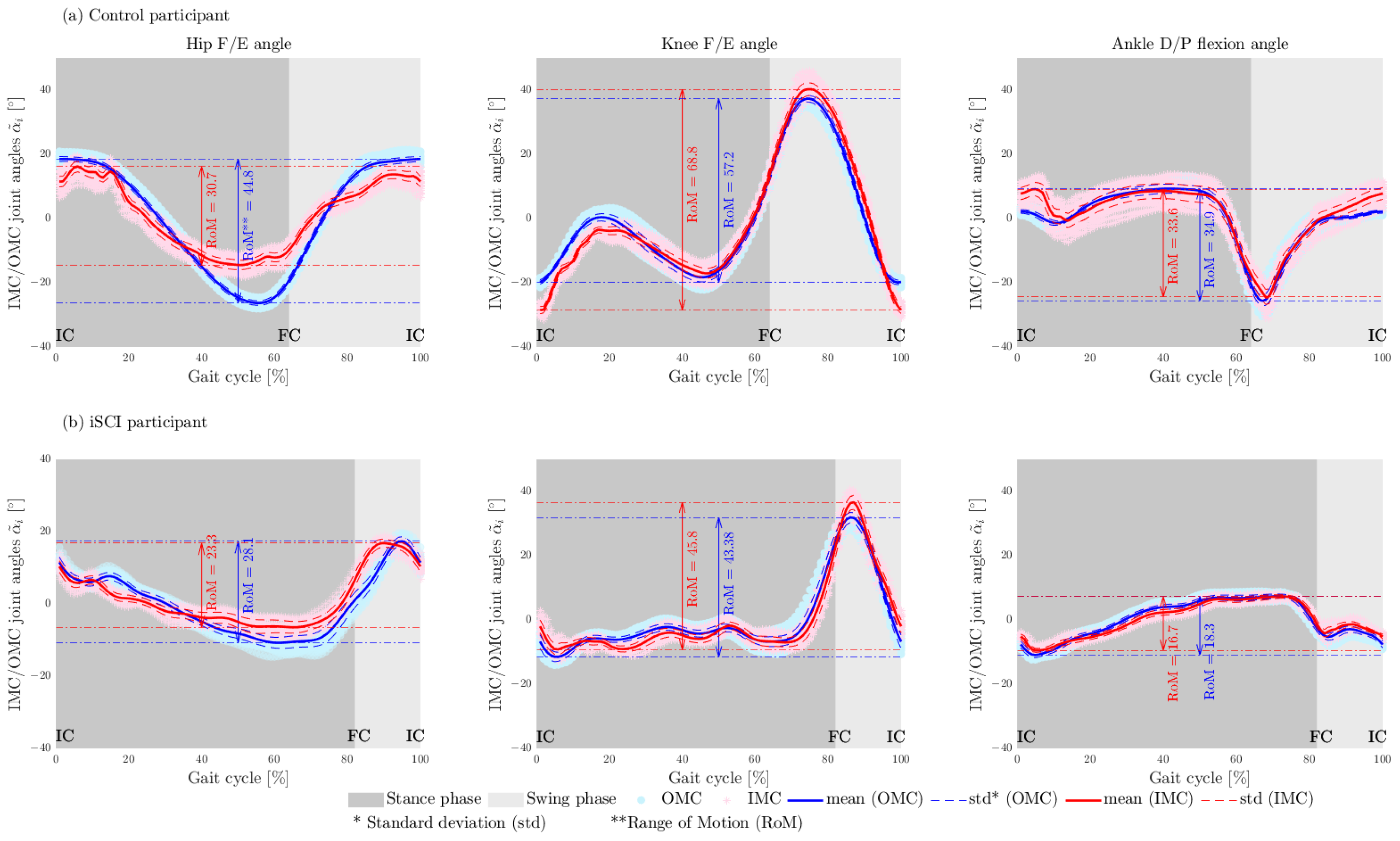
2.4.3. Gait Kinematic Characteristics—IMC System
2.4.4. Comparison Matrices
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| iSCI | incomplete Spinal Cord Injured |
| IMU | Inertial Measurement Unit |
| OMC | Optical Motion Capture |
| RMSE | Root Mean Square Error |
| RoME | Range of Motion Error |
| CSI | Cubic Spline Interpolation |
| std | standard deviation |
| MAD | Mean Absolute Difference |
| IC | Initial Contact |
| FC | Final Contact |
| STDD | STandard Deviation of Difference |
| RoM | Range of Motion |
| WISCI II | Walking Index for Spinal Cord Injury |
| F/E | Flexion/Extension |
| D/P | Dorsi/Plantar |
| A/A | Abduction/Adduction |
| RMSE | Root Mean Square Error |
References
- Bolliger, M.; Blight, A.R.; Field-Fote, E.C.; Musselman, K.; Rossignol, S.; Barthélemy, D.; Bouyer, L.; Popovic, M.R.; Schwab, J.M.; Boninger, M.L.; et al. Lower extremity outcome measures: Considerations for clinical trials in spinal cord injury. Spinal Cord 2018, 56, 628–642. [Google Scholar] [CrossRef] [PubMed]
- Bridenbaugh, S.A.; Kressig, R.W. Laboratory review: The role of gait analysis in seniors’ mobility and fall prevention. Gerontology 2011, 57, 256–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eichelberger, P.; Ferraro, M.; Minder, U.; Denton, T.; Blasimann, A.; Krause, F.; Baur, H. Analysis of accuracy in optical motion capture—A protocol for laboratory setup evaluation. J. Biomech. 2016, 49, 2085–2088. [Google Scholar] [CrossRef] [Green Version]
- Mayagoitia, R.E.; Nene, A.V.; Veltink, P.H. Accelerometer and rate gyroscope measurement of kinematics: An inexpensive alternative to optical motion analysis systems. J. Biomech. 2002, 35, 537–542. [Google Scholar] [CrossRef]
- Routhier, F.; Duclos, N.C.; Lacroix, É.; Lettre, J.; Turcotte, E.; Hamel, N.; Michaud, F.; Duclos, C.; Archambault, P.S.; Bouyer, L.J. Clinicians’ perspectives on inertial measurement units in clinical practice. PLoS ONE 2020, 15, e0241922. [Google Scholar] [CrossRef] [PubMed]
- DeLuca, P.A.; Davis, R.B.; Õunpuu, S.; Rose, S.; Sirkin, R. Alterations in surgical decision making in patients with cerebral palsy based on three-dimensional gait analysis. J. Pediatr. Orthop. 1997, 17, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Salarian, A.; Russmann, H.; Vingerhoets, F.J.; Dehollain, C.; Blanc, Y.; Burkhard, P.R.; Aminian, K. Gait assessment in Parkinson’s disease: Toward an ambulatory system for long-term monitoring. IEEE Trans. Biomed. Eng. 2004, 51, 1434–1443. [Google Scholar] [CrossRef]
- Simon, S.R. Quantification of human motion: Gait analysis—Benefits and limitations to its application to clinical problems. J. Biomech. 2004, 37, 1869–1880. [Google Scholar] [CrossRef]
- Taheri, O.; Salarieh, H.; Alasty, A. Human Leg Motion Tracking by Fusing IMUs and RGB Camera Data Using Extended Kalman Filter. arXiv 2020, arXiv:2011.00574. [Google Scholar]
- Roetenberg, D.; Luinge, H.; Slycke, P. Xsens MVN: Full 6DOF human motion tracking using miniature inertial sensors. Xsens Motion Technol. BV Tech. Rep 2009, 1, 1–7. [Google Scholar]
- Favre, J.; Jolles, B.; Aissaoui, R.; Aminian, K. Ambulatory measurement of 3D knee joint angle. J. Biomech. 2008, 41, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Favre, J.; Aissaoui, R.; Jolles, B.M.; de Guise, J.A.; Aminian, K. Functional calibration procedure for 3D knee joint angle description using inertial sensors. J. Biomech. 2009, 42, 2330–2335. [Google Scholar] [CrossRef] [PubMed]
- Cutti, A.G.; Ferrari, A.; Garofalo, P.; Raggi, M.; Cappello, A.; Ferrari, A. ‘Outwalk’: Aa protocol for clinical gait analysis based on inertial and magnetic sensors. Med Biol. Eng. Comput. 2010, 48, 17–25. [Google Scholar] [CrossRef] [PubMed]
- O’Donovan, K.J.; Kamnik, R.; O’Keeffe, D.T.; Lyons, G.M. An inertial and magnetic sensor based technique for joint angle measurement. J. Biomech. 2007, 40, 2604–2611. [Google Scholar] [CrossRef]
- Dejnabadi, H.; Jolles, B.M.; Aminian, K. A new approach to accurate measurement of uniaxial joint angles based on a combination of accelerometers and gyroscopes. IEEE Trans. Biomed. Eng. 2005, 52, 1478–1484. [Google Scholar] [CrossRef]
- Solin, A.; Särkkä, S.; Kannala, J.; Rahtu, E. Terrain navigation in the magnetic landscape: Particle filtering for indoor positioning. In Proceedings of the 2016 European Navigation Conference (ENC), Helsinki, Finland, 30 May–2 June 2016; pp. 1–9. [Google Scholar]
- Olsson, F.; Kok, M.; Seel, T.; Halvorsen, K. Robust plug-and-play joint axis estimation using inertial sensors. Sensors 2020, 20, 3534. [Google Scholar] [CrossRef]
- Lehmann, D.; Laidig, D.; Deimel, R.; Seel, T. Magnetometer-free inertial motion tracking of arbitrary joints with range of motion constraints. IFAC PapersOnLine 2020, 53, 16016–16022. [Google Scholar] [CrossRef]
- Laidig, D.; Jocham, A.J.; Guggenberger, B.; Adamer, K.; Fischer, M.; Seel, T. Calibration-Free Gait Assessment by Foot-Worn Inertial Sensors. Front. Digit. Health 2021, 3, 736418. [Google Scholar] [CrossRef]
- Davis III, R.B.; Ounpuu, S.; Tyburski, D.; Gage, J.R. A gait analysis data collection and reduction technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- VICON, Frequently Asked Questions. Available online: https://www.vicon.com/support/faqs/?q=how-much-time-do-vicon-cameras-need-to-warm-up-prior-to-use (accessed on 23 May 2022).
- Woltring, H.J. A Fortran package for generalized, cross-validatory spline smoothing and differentiation. Adv. Eng. Softw. (1978) 1986, 8, 104–113. [Google Scholar] [CrossRef]
- Sabatini, A.M. Estimating three-dimensional orientation of human body parts by inertial/magnetic sensing. Sensors 2011, 11, 1489–1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seel, T.; Ruppin, S. Eliminating the Effect of Magnetic Disturbances on the Inclination Estimates of Inertial Sensors. IFAC PapersOnLine 2017, 50, 8798–8803. [Google Scholar] [CrossRef]
- Laidig, D.; Schauer, T.; Seel, T. Exploiting kinematic constraints to compensate magnetic disturbances when calculating joint angles of approximate hinge joints from orientation estimates of inertial sensors. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 971–976. [Google Scholar]
- Seel, T.; Raisch, J.; Schauer, T. IMU-based joint angle measurement for gait analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berner, K.; Cockcroft, J.; Morris, L.D.; Louw, Q. Concurrent validity and within-session reliability of gait kinematics measured using an inertial motion capture system with repeated calibration. J. Bodyw. Mov. Ther. 2020, 24, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Dorschky, E.; Nitschke, M.; Seifer, A.K.; van den Bogert, A.J.; Eskofier, B.M. Estimation of gait kinematics and kinetics from inertial sensor data using optimal control of musculoskeletal models. J. Biomech. 2019, 95, 109278. [Google Scholar] [CrossRef] [PubMed]
- Van Den Noort, J.C.; Ferrari, A.; Cutti, A.G.; Becher, J.G.; Harlaar, J. Gait analysis in children with cerebral palsy via inertial and magnetic sensors. Med. Biol. Eng. Comput. 2013, 51, 377–386. [Google Scholar] [CrossRef]
- Nüesch, C.; Roos, E.; Pagenstert, G.; Mündermann, A. Measuring joint kinematics of treadmill walking and running: Comparison between an inertial sensor based system and a camera-based system. J. Biomech. 2017, 57, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity, test-retest reliability and long-term stability of magnetometer free inertial sensor based 3D joint kinematics. Sensors 2018, 18, 1980. [Google Scholar] [CrossRef] [Green Version]
- Alton, F.; Baldey, L.; Caplan, S.; Morrissey, M. A kinematic comparison of overground and treadmill walking. Clin. Biomech. 1998, 13, 434–440. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | Gender | Age [Year] | Height [cm] | Weight [kg] | Lesion Level (and Impairment Scale) | WISCI II |
|---|---|---|---|---|---|---|
| C01 | Male | 35 | 173 | 71 | − | − |
| C02 | Female | 32 | 175 | 60 | − | − |
| C03 | Male | 37 | 180 | 79 | − | − |
| C04 | Female | 28 | 165 | 58 | − | − |
| C05 | Female | 26 | 173 | 63 | − | − |
| P01 | Male | 65 | 183 | 86 | C6, ASIA D | 20 |
| P02 | Male | 62 | 193 | 100 | C7, ASIA D | 20 |
| P03 | Female | 37 | 167 | 45 | C6, ASIA D | 19 |
| P04 | Male | 28 | 198 | 93 | L2, ASIA C | 20 |
| P05 | Female | 33 | 160 | 74 | C5, ASIA D | 8 |
| Mean(±std) | − | − |
| Sensor | Position | Description |
|---|---|---|
| 1 | Left foot | Dorsal side of the left foot |
| 2 | Left shank | Anterior and medially along the tibial bone |
| 3 | Left thigh | Laterally, 2× palm above knee |
| 4 | Right foot | Dorsal side of the right foot |
| 5 | Right shank | Anterior and medially along the tibial bone |
| 6 | Right thigh | Laterally, 2× palm above knee |
| 7 | Pelvis | Body of sacrum |
| Joints | RoM Comparison [MAD (± STDD )] | ||
|---|---|---|---|
| Control (n = 5, Strides = 450) | iSCI (n = 5, Strides = 373) | Mean (n = 10, Strides = 823) | |
| Hip F/E angle [] | |||
| Hip A/A angle [] | |||
| Knee F/E angle [] | (± ) | ||
| Ankle D/P flexion angle [] | |||
| Mean [] | (± ) | ||
| Gait Parameters | Comparison of Gait Parameters [MAD (±STDD )] | ||
|---|---|---|---|
| Control (n = 5, Strides = 450) | iSCI (n = 5, Strides = 373) | Mean (n = 10, Strides = 823) | |
| Relative swing phase [%] | |||
| Relative stance phase [%] | |||
| Relative double support [%] | |||
| Cadence [steps/min] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haji Hassani, R.; Willi, R.; Rauter, G.; Bolliger, M.; Seel, T. Validation of Non-Restrictive Inertial Gait Analysis of Individuals with Incomplete Spinal Cord Injury in Clinical Settings. Sensors 2022, 22, 4237. https://doi.org/10.3390/s22114237
Haji Hassani R, Willi R, Rauter G, Bolliger M, Seel T. Validation of Non-Restrictive Inertial Gait Analysis of Individuals with Incomplete Spinal Cord Injury in Clinical Settings. Sensors. 2022; 22(11):4237. https://doi.org/10.3390/s22114237
Chicago/Turabian StyleHaji Hassani, Roushanak, Romina Willi, Georg Rauter, Marc Bolliger, and Thomas Seel. 2022. "Validation of Non-Restrictive Inertial Gait Analysis of Individuals with Incomplete Spinal Cord Injury in Clinical Settings" Sensors 22, no. 11: 4237. https://doi.org/10.3390/s22114237