
Understanding Social Behaviour in a Health-Care Facility from Localization Data: A Case Study

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
1.1. Alzheimer’s Disease
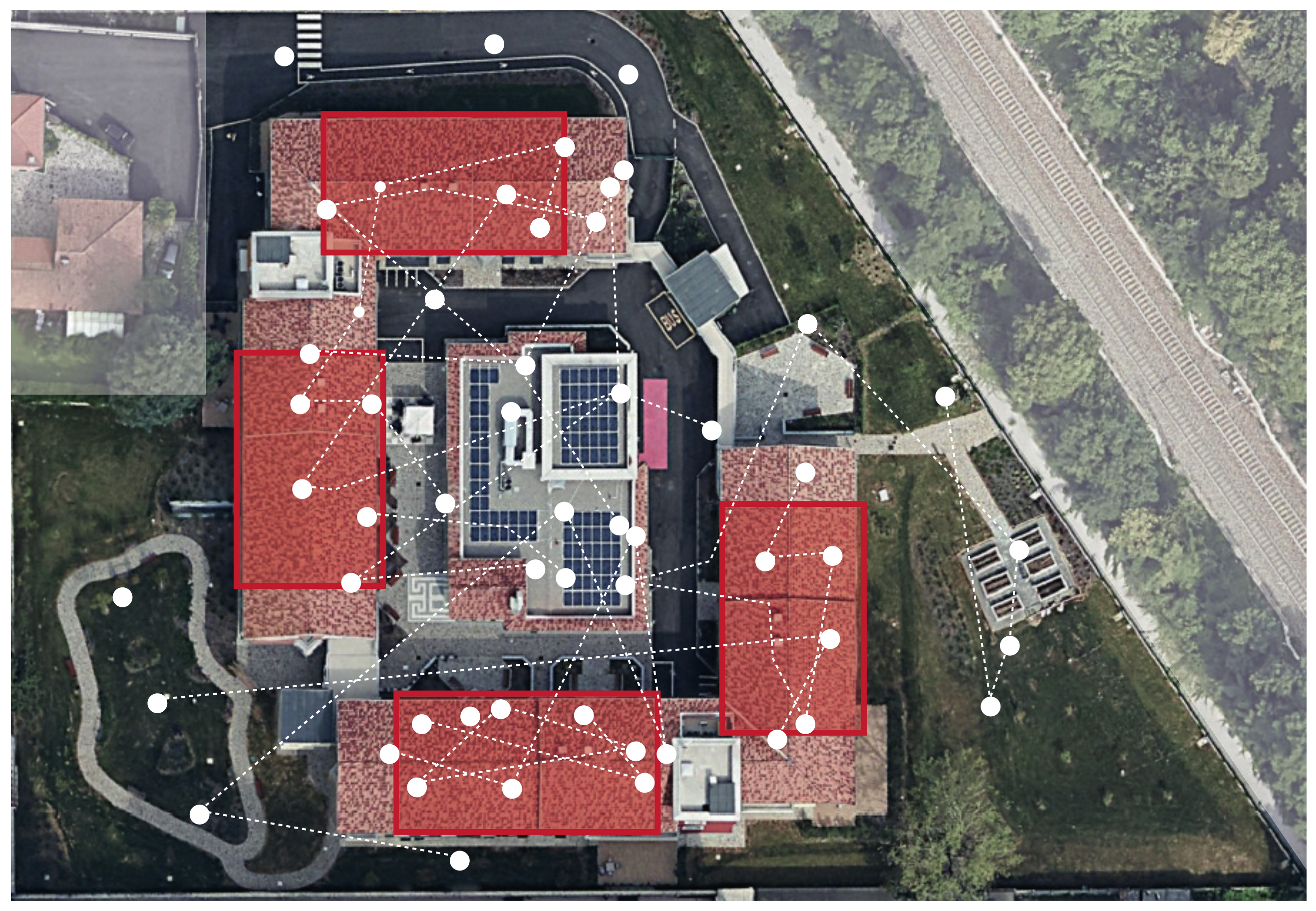
1.2. Case Study: Il Paese Ritrovato
1.3. Supporting AD Patients: State of the Art
- Retirement housing, appropriate for individuals in early-stage Alzheimer’s.
- AAL, which offers a combination of housing, meals, supportive services and health care.
- Nursing homes, which provide around-the-clock care and long-term medical treatment.
- Alzheimer’s special care units, most often cluster settings in which persons living with dementia are grouped on a floor or a unit within a larger residential care building.
- Continuing care retirement communities, which provide different levels of care (independent, AAL and nursing home) based on individual needs.
1.4. Purpose and Contributions
2. Materials and Methods
2.1. Sensors and Data
2.2. Interfacing with the Database
2.3. Indexes Measuring the Strength of Relationships
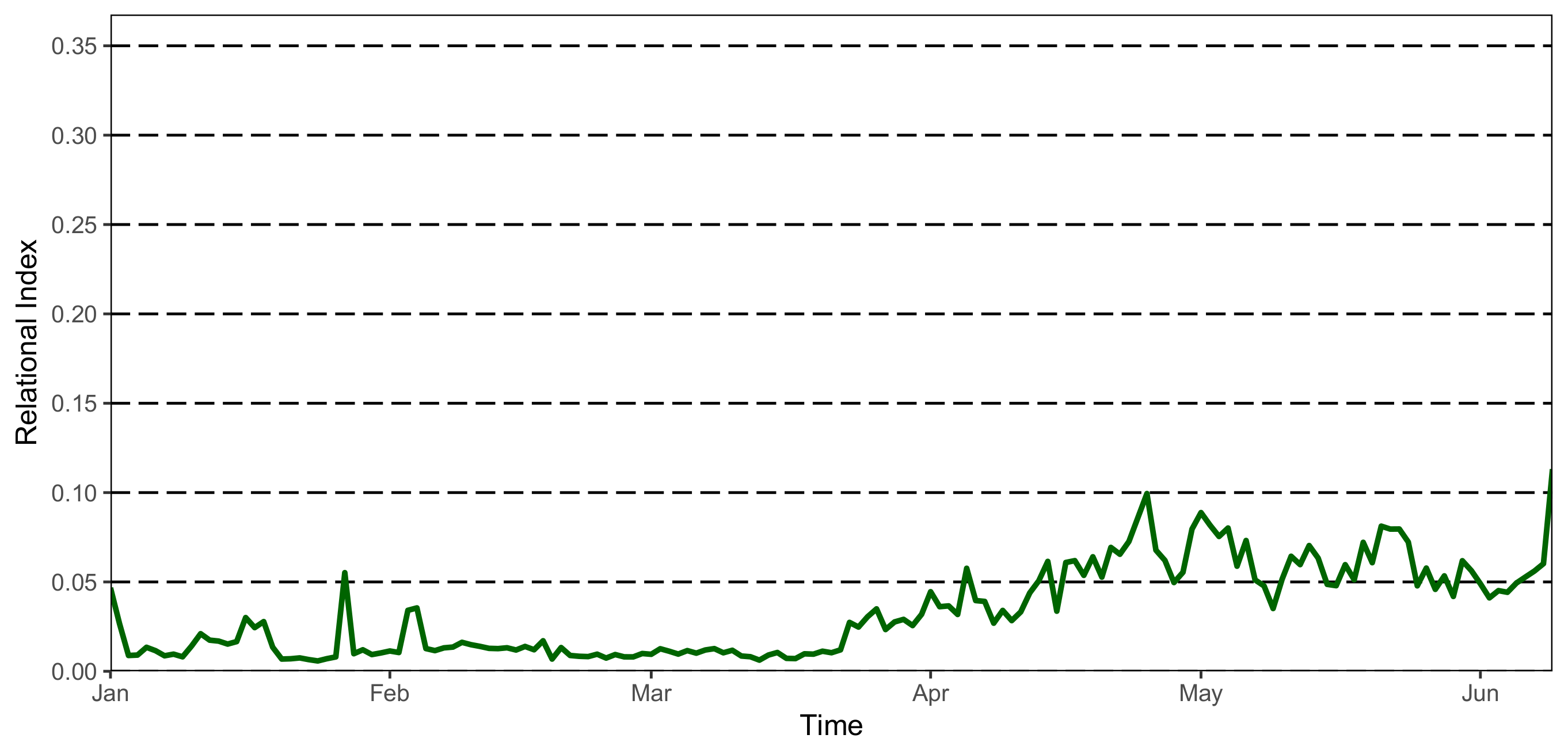
2.3.1. The Relational Index
2.3.2. Time-Specific Relational Index
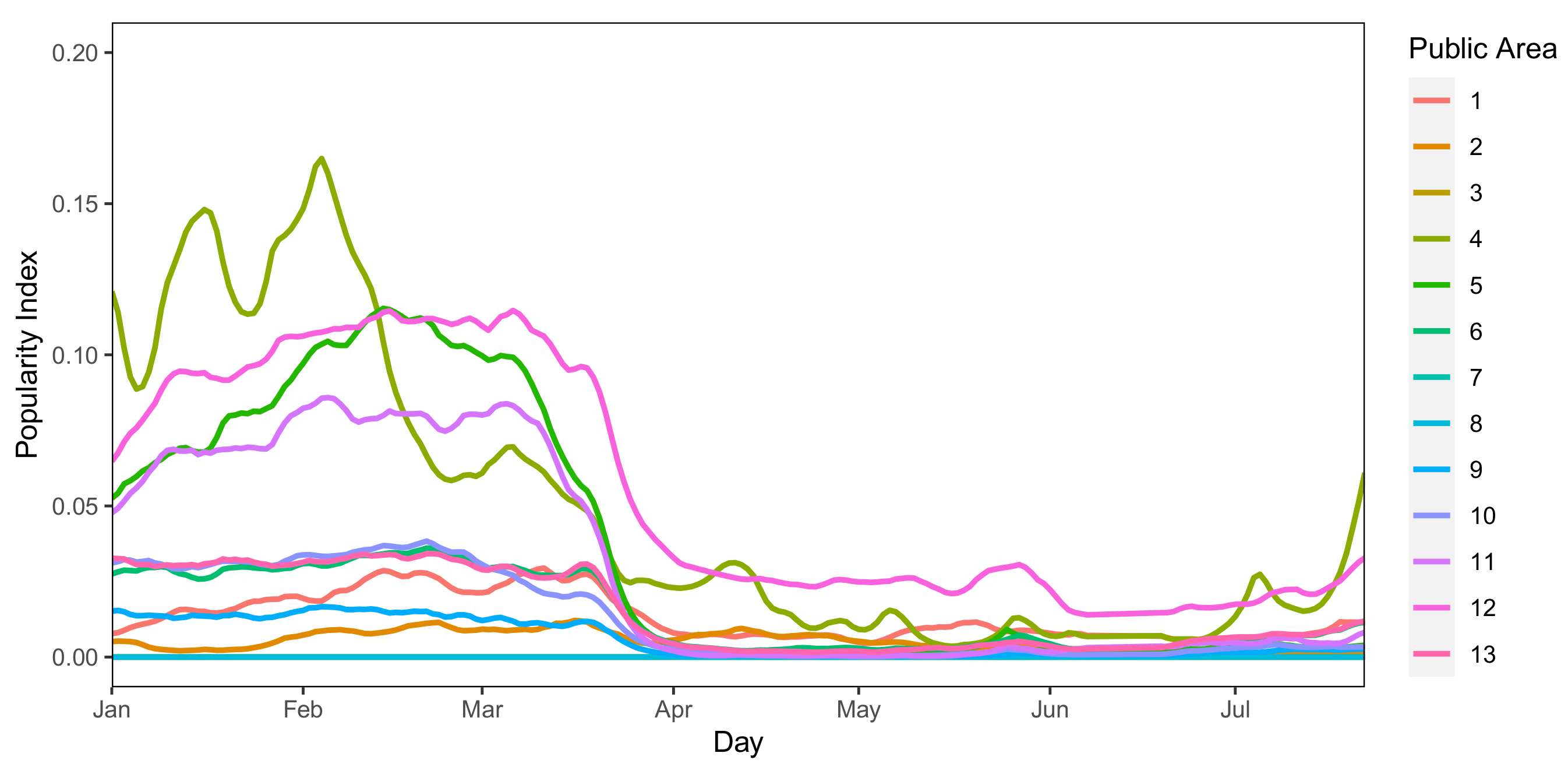
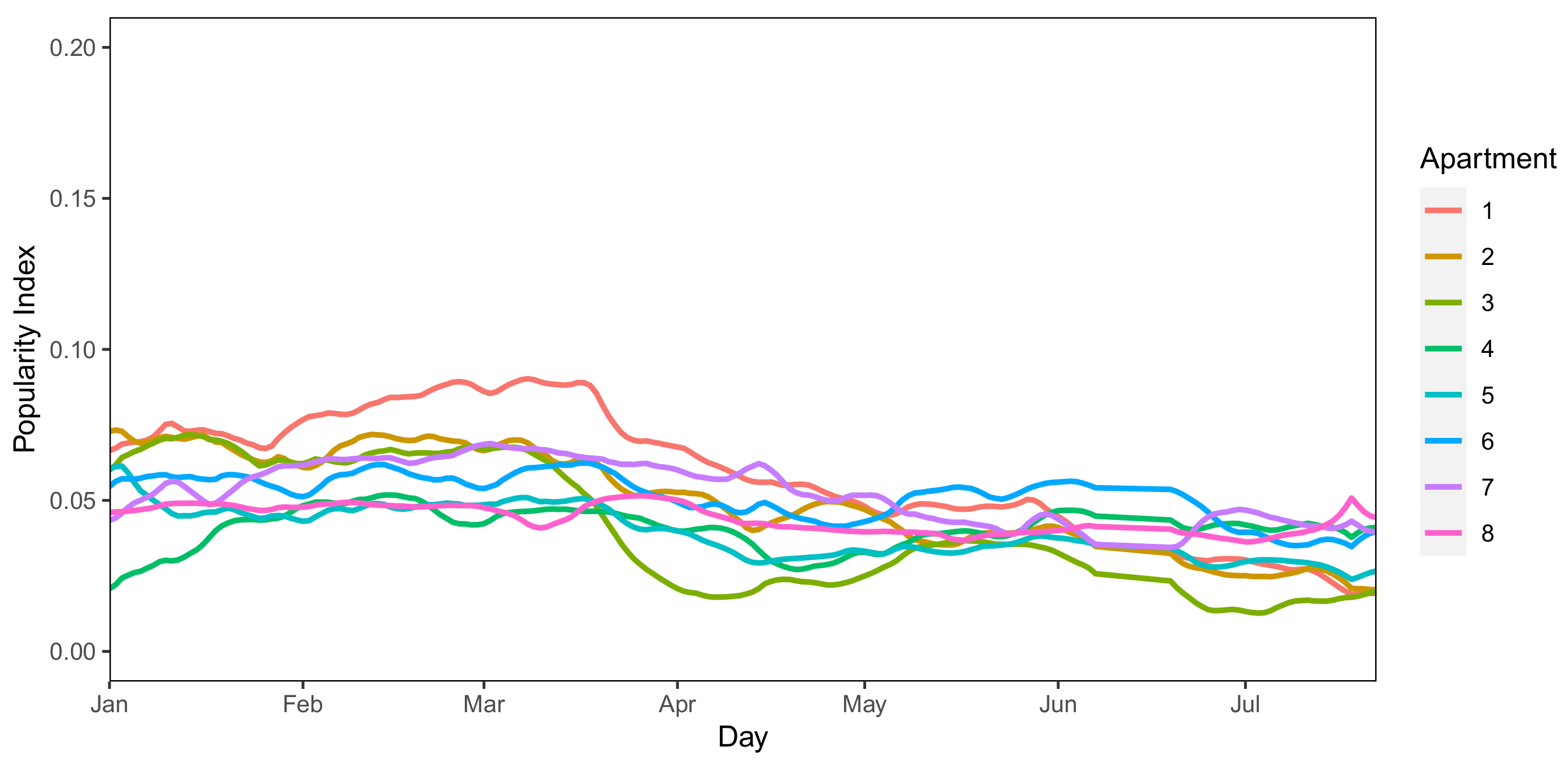
2.4. Indexes Assessing the Attendance of Places
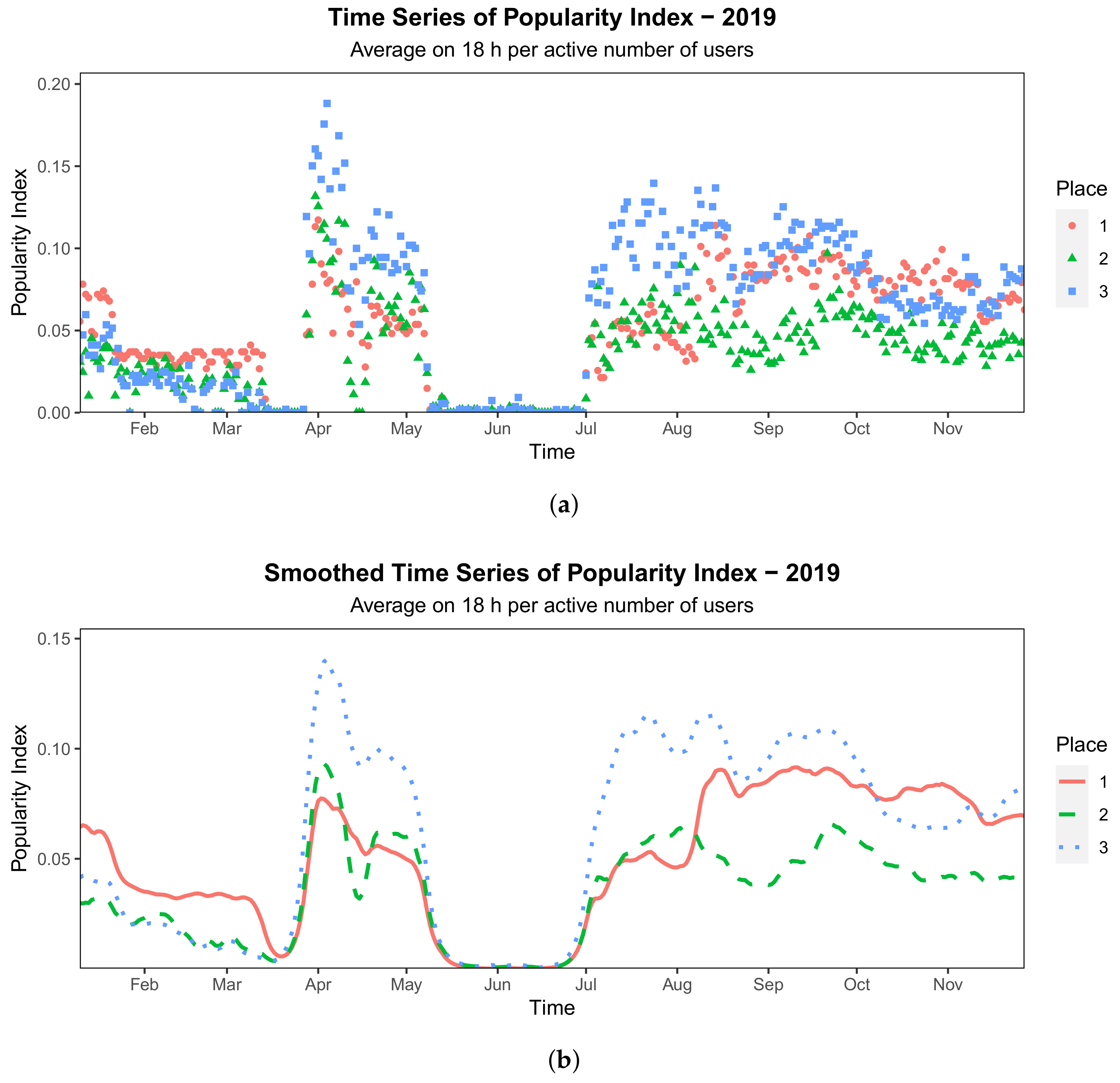
The Popularity Index
- gain some regularity of the function since, at third order, functions are of class ;
- preserve the non-negativeness of the functions since we choose to penalize, through a parameter , the first derivative of the smoothed curves, thus letting us free to smooth strong peaks of noise;
- avoid fixing the dimension of the basis space since with this type of splines the dimension is automatically selected to generate curves that blindly follow the original data.
2.5. Predictive Tools for the Sociability of the Community
- attribute of a day being a workday;
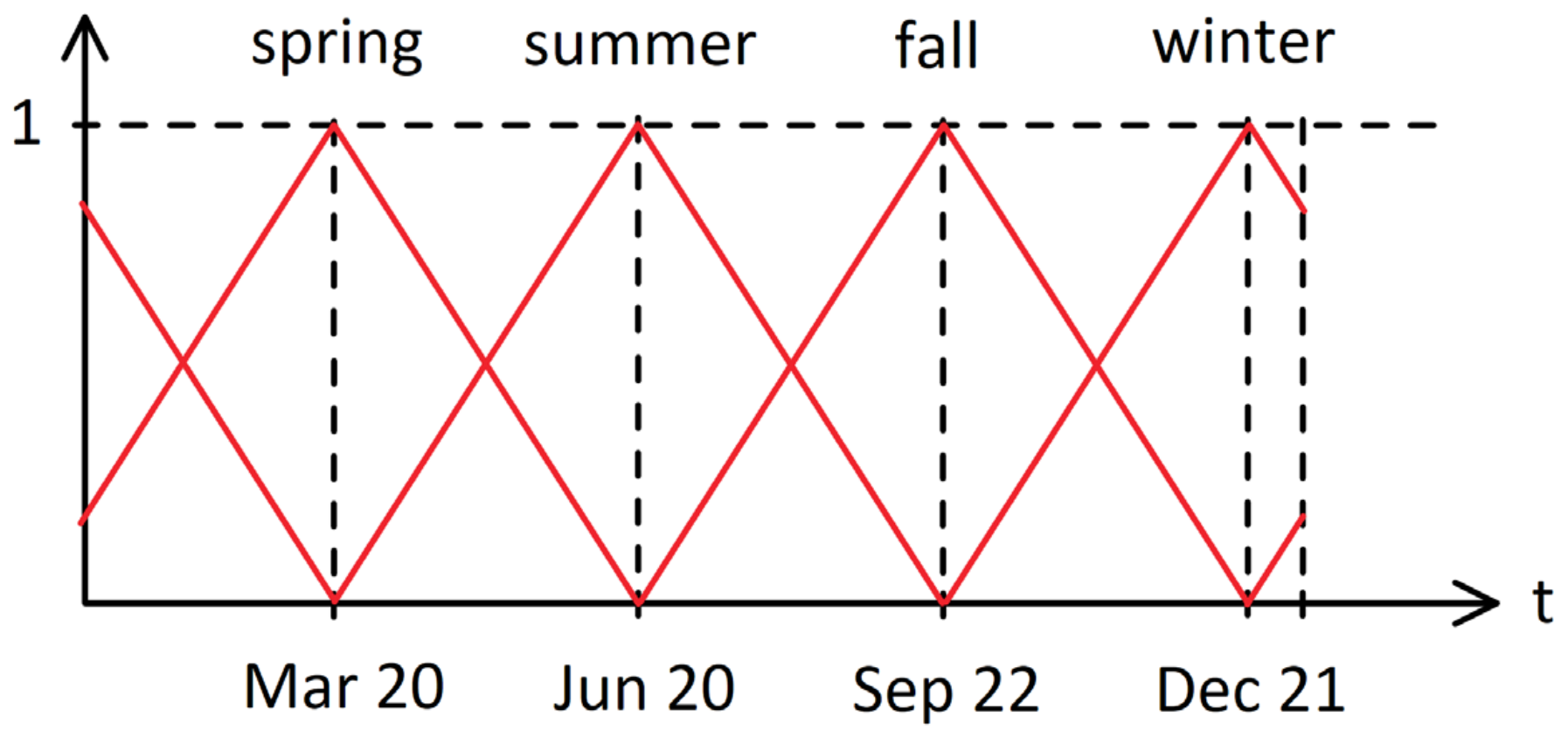
- season;
- temperature;
- predisposition to walk on a specific day and specific time of the day.
2.6. Predictive Tools for the Popularity of Places
- place identifier;
- period of the year;
- period of the day;
- weather;
- temperature.
2.6.1. Place Identifier
2.6.2. Period of the Year
2.6.3. Hour of the Day
2.6.4. Weather
2.6.5. Temperature
- The first layer receives the place id one-hot vector as input, to encode it in a 3-dimensional latent space. The idea behind this choice is to reduce the dimensionality of the place id vector, thus reducing the complexity of the network.
- The second layer takes as input the remaining 9 values from the remaining input variables, along with the 3-dimensional vector encoded by the first layer (representing the place). The output dimension of this second layer varies between 16, 64 and 256 in our grid search.
- The final layer consists of a single output neuron, having a Leaky ReLU activation function at training time and a ReLU activation function at prediction time [33]. This allows avoiding zero-gradient problems when training while correcting negative outputs when inferring, as the is always non-negative.
- the hidden layers dimension, with 3 possible values: {16, 64, 256};
- the scaling factor, that is, the factor for which the layer dimension was multiplied by when moving from a layer to the subsequent one, with 2 possible values: {0.5, 1};
- the number of hidden layers, from 1 to 5.
3. Results
3.1. Predictive Models Evaluation
3.1.1. Community Time-Specific Relational Index
3.1.2. Popularity Index
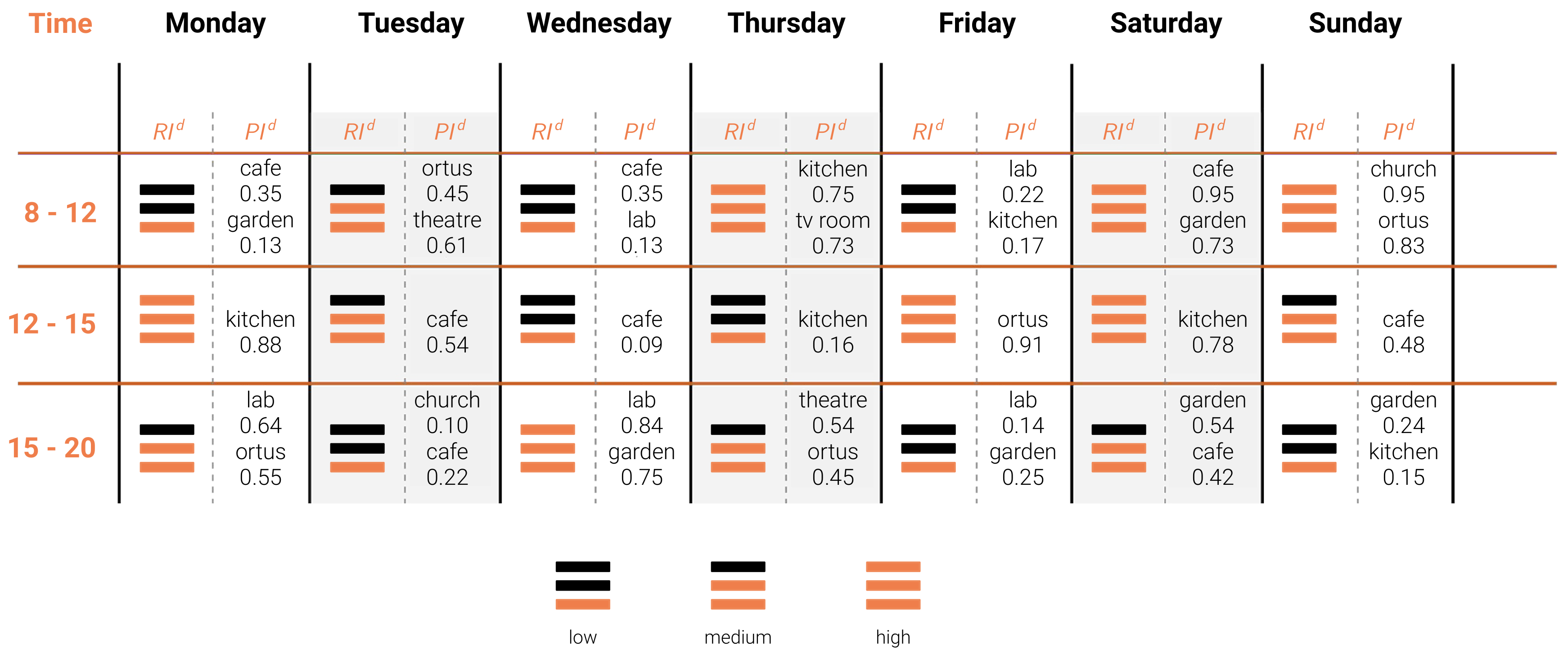
3.2. Community Behaviour Prediction Table
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAL | Ambient Assisted Living |
| AD | Alzheimer’s Disease |
| ALZGAR | Alzheimer’s Garden |
| BLE | Bluetooth Low Energy |
| CBPT | Community behaviour Prediction Table |
| Popularity Index | |
| Relational Index |
References
- United Nations. World Population Ageing 2019; United Nations: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Laurance, J. Why an Ageing Population Is the Greatest Threat to Society. Available online: https://www.independent.co.uk/news/uk/home-news/why-ageing-population-greatest-threat-society-5361944.html (accessed on 15 April 2020).
- Dementia, World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 15 April 2020).
- Evans, J.; Brown, M.; Coughlan, T.; Lawson, G.; Craven, M.P. A systematic review of dementia focused assistive technology. In Proceedings of the International Conference on Human-Computer Interaction, Los Angeles, CA, USA, 2–7 August 2015; pp. 406–417. [Google Scholar]
- Burns, A.; Iliffe, S. Alzheimer’s disease. BMJ 2009, 338, b158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Förstl, H.; Kurz, A. Clinical features of Alzheimer’s disease. Eur. Arch. Psychiatry Clin. Neurosci. 1999, 249, 288–290. [Google Scholar] [CrossRef] [PubMed]
- Donovan, N.J.; Wu, Q.; Rentz, D.M.; Sperling, R.A.; Marshall, G.A.; Glymour, M.M. Loneliness, depression and cognitive function in older U.S. adults. Int. J. Geriatr. Psychiatry 2016, 32, 564–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biamonti, A. Design & Alzheimer: Dalle Esperienze Degli Habitat Terapeutici al Modello GRACE; Serie di Architettura e Design; Franco Angeli Edizioni: Milano, Italy, 2018. [Google Scholar]
- Valla, P. Alzheimer: Architetture e Giardini Come Strumento Terapeutico; Guerini e Associati: Milano, Italy, 2002. [Google Scholar]
- Il Paese Ritrovato. Available online: https://ilpaeseritrovato.it (accessed on 15 April 2020).
- Cooperativa La Meridiana. Available online: https://cooplameridiana.it (accessed on 15 April 2020).
- Hogeweyk. Available online: https://hogeweyk.dementiavillage.com (accessed on 15 April 2020).
- Masciadri, A.; Comai, S.; Salice, F. Wellness Assessment of Alzheimer’s Patients in an Instrumented Health-Care Facility. Sensors 2019, 19, 3658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amato, F.; Bianchi, S.; Comai, S.; Crovari, P.; Pasquarelli, M.G.G.; Imtiaz, A.; Masciadri, A.; Toldo, M.; Yuyar, E. CLONE: A Promising System for the Remote Monitoring of Alzheimer’s Patients: An Experimentation with a Wearable Device in a Village for Alzheimer’s Care. In Proceedings of the 4th EAI International Conference on Smart Objects and Technologies for Social Good, Bologna, Italy, 28–30 November 2018; pp. 255–260. [Google Scholar]
- Alzheimer’s Association: Stages of Alzheimer’s. Available online: https://www.alz.org/alzheimers-dementia/stages (accessed on 15 April 2020).
- National Institute on Aging. How Is Alzheimer’s Disease Treated? Available online: https://www.nia.nih.gov/health/how-alzheimers-disease-treated (accessed on 15 April 2020).
- Alzheimer’s Association. Residential Care. Available online: https://www.alz.org/help-support/caregiving/care-options/residential-care (accessed on 15 April 2020).
- Doshi-Velez, F.; Li, W.; Battat, Y.; Charrow, B.; Curthis, D.; Park, J.G.; Hemachandra, S.; Velez, J.; Walsh, C.; Fredette, D.; et al. Improving safety and operational efficiency in residential care settings with WiFi-based localization. J. Am. Med. Dir. Assoc. 2012, 13, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Serra-Añó, P.; Pedrero-Sánchez, J.F.; Hurtado-Abellán, J.; Inglés, M.; Espí-López, G.V.; López-Pascual, J. Mobility assessment in people with Alzheimer disease using smartphone sensors. J. Neuroeng. Rehabil. 2019, 16, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levasseur, M.; Richard, L.; Gauvin, L.; Raymond, É. Inventory and analysis of definitions of social participation found in the aging literature: Proposed taxonomy of social activities. Soc. Sci. Med. 2010, 71, 2141–2149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruthirakuhan, M.; Luedke, A.C.; Tam, A.; Goel, A.; Kurji, A.; Garcia, A. Use of Physical and Intellectual Activities and Socialization in the Management of Cognitive Decline of Aging and in Dementia: A Review. J. Aging Res. 2012, 2012, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cevizci, S.; Murat, H.; Gunes, F.; Karaahmet, E. Animal Assisted Therapy and Activities in Alzheimer’s Disease. In Understanding Alzheimer’s Disease; InTechOpen: London, UK, 2013. [Google Scholar] [CrossRef] [Green Version]
- Chancellor, B.; Duncan, A.; Chatterjee, A. Art Therapy for Alzheimer’s Disease and Other Dementias. J. Alzheimer’s Dis. 2014, 39, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mace, N.L. Principles of Activities for Persons with Dementia. Phys. Occup. Ther. Geriatr. 1987, 5, 13–28. [Google Scholar] [CrossRef]
- Barnes, L.L.; Mendes de Leon, C.F.; Wilson, R.S.; Bienias, J.L.; Evans, D.A. Social resources and cognitive decline in a population of older African Americans and whites. Neurology 2004, 63, 2322–2326. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Krueger, K.R.; Arnold, S.E.; Schneider, J.A.; Kelly, J.F.; Barnes, L.L.; Tang, Y.; Bennett, D.A. Loneliness and Risk of Alzheimer Disease. Arch. Gen. Psychiatry 2007, 64, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellini, G.; Cipriano, M.; De Angeli, N.; Gargano, J.P.; Gianella, M.; Goi, G.; Rossi, G.; Masciadri, A.; Comai, S. Alzheimer’s Garden: Understanding Social Behaviors of Patients with Dementia to Improve Their Quality of Life. In Proceedings of the International Conference on Computers Helping People with Special Needs, Lecco, Italy, 9–11 September 2020; pp. 384–393. [Google Scholar]
- iBeacon. Available online: https://developer.apple.com/ibeacon/ (accessed on 20 December 2020).
- Lucero, M.; Hutchinson, S.; Leger-Krall, S.; Wilson, H.S. Wandering in Alzheimer’s Dementia Patients. Clin. Nurs. Res. 1993, 2, 160–175. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, J.; Silverman, B. Functional Data Analysis; Springer: New York, NY, USA, 2005. [Google Scholar]
- Eilers, P.H.; Marx, B.D. Flexible smoothing with B-splines and penalties. Stat. Sci. 1996, 11, 89–102. [Google Scholar] [CrossRef]
- Russell, S.; Norvig, P. Artificial Intelligence: A Modern Approach; Pearson Education Limited: London, UK, 2013. [Google Scholar]
- Nwankpa, C.; Ijomah, W.; Gachagan, A.; Marshall, S. Activation functions: Comparison of trends in practice and research for deep learning. arXiv 2018, arXiv:1811.03378. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- PyTorch. Available online: https://pytorch.org (accessed on 15 April 2020).
- DeepAI. Feed Forward Neural Network. Available online: https://deepai.org/machine-learning-glossary-and-terms/feed-forward-neural-network (accessed on 15 April 2020).
- Caruana, R.; Lawrence, S.; Giles, C.L. Overfitting in neural nets: Backpropagation, conjugate gradient, and early stopping. In Advances in Neural Information Processing Systems; MIT: Boston, MA, USA, 2001; pp. 402–408. [Google Scholar]
- World Health Organization. Coronavirus disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 20 December 2020).
- La Gatta, V.; Moscato, V.; Postiglione, M.; Sperli, G. An Epidemiological Neural network exploiting Dynamic Graph Structured Data applied to the COVID-19 outbreak. IEEE Trans. Big Data 2020, 7, 45–55. [Google Scholar] [CrossRef]
- Sixsmith, A.; Gibson, G. Music and the wellbeing of people with dementia. Ageing Soc. 2007, 27, 127. [Google Scholar] [CrossRef]
- Empatica. Available online: https://empatica.com (accessed on 20 December 2020).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | … | |
| 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | … | |
| 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | … |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellini, G.; Cipriano, M.; Comai, S.; De Angeli, N.; Gargano, J.P.; Gianella, M.; Goi, G.; Ingrao, G.; Masciadri, A.; Rossi, G.; et al. Understanding Social Behaviour in a Health-Care Facility from Localization Data: A Case Study. Sensors 2021, 21, 2147. https://doi.org/10.3390/s21062147
Bellini G, Cipriano M, Comai S, De Angeli N, Gargano JP, Gianella M, Goi G, Ingrao G, Masciadri A, Rossi G, et al. Understanding Social Behaviour in a Health-Care Facility from Localization Data: A Case Study. Sensors. 2021; 21(6):2147. https://doi.org/10.3390/s21062147
Chicago/Turabian StyleBellini, Gloria, Marco Cipriano, Sara Comai, Nicola De Angeli, Jacopo Pio Gargano, Matteo Gianella, Gianluca Goi, Giovanni Ingrao, Andrea Masciadri, Gabriele Rossi, and et al. 2021. "Understanding Social Behaviour in a Health-Care Facility from Localization Data: A Case Study" Sensors 21, no. 6: 2147. https://doi.org/10.3390/s21062147