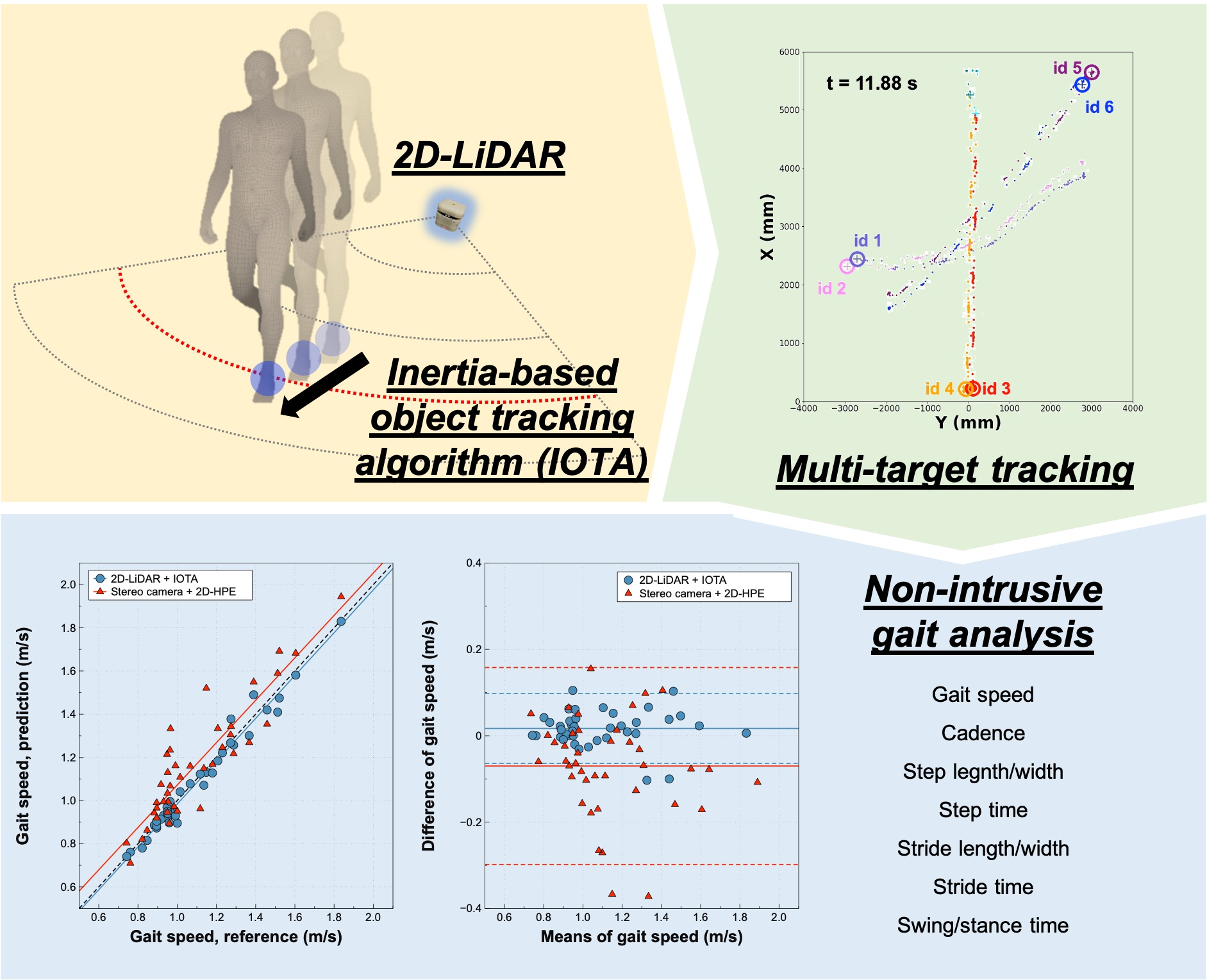
Development and Validation of 2D-LiDAR-Based Gait Analysis Instrument and Algorithm

 ,
, 
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
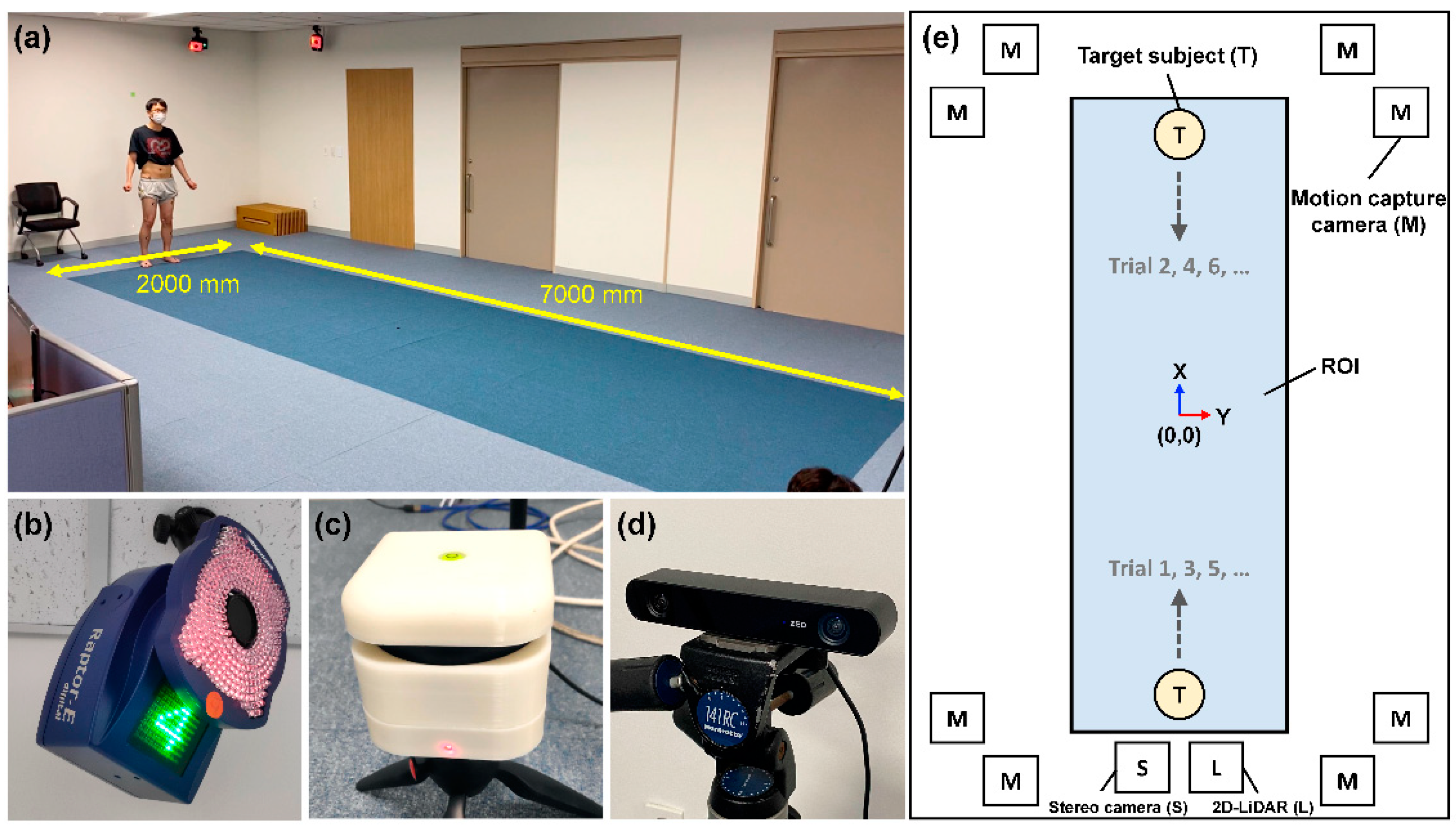
2.1. Sensors and Installation in Test Environment
2.2. Participants
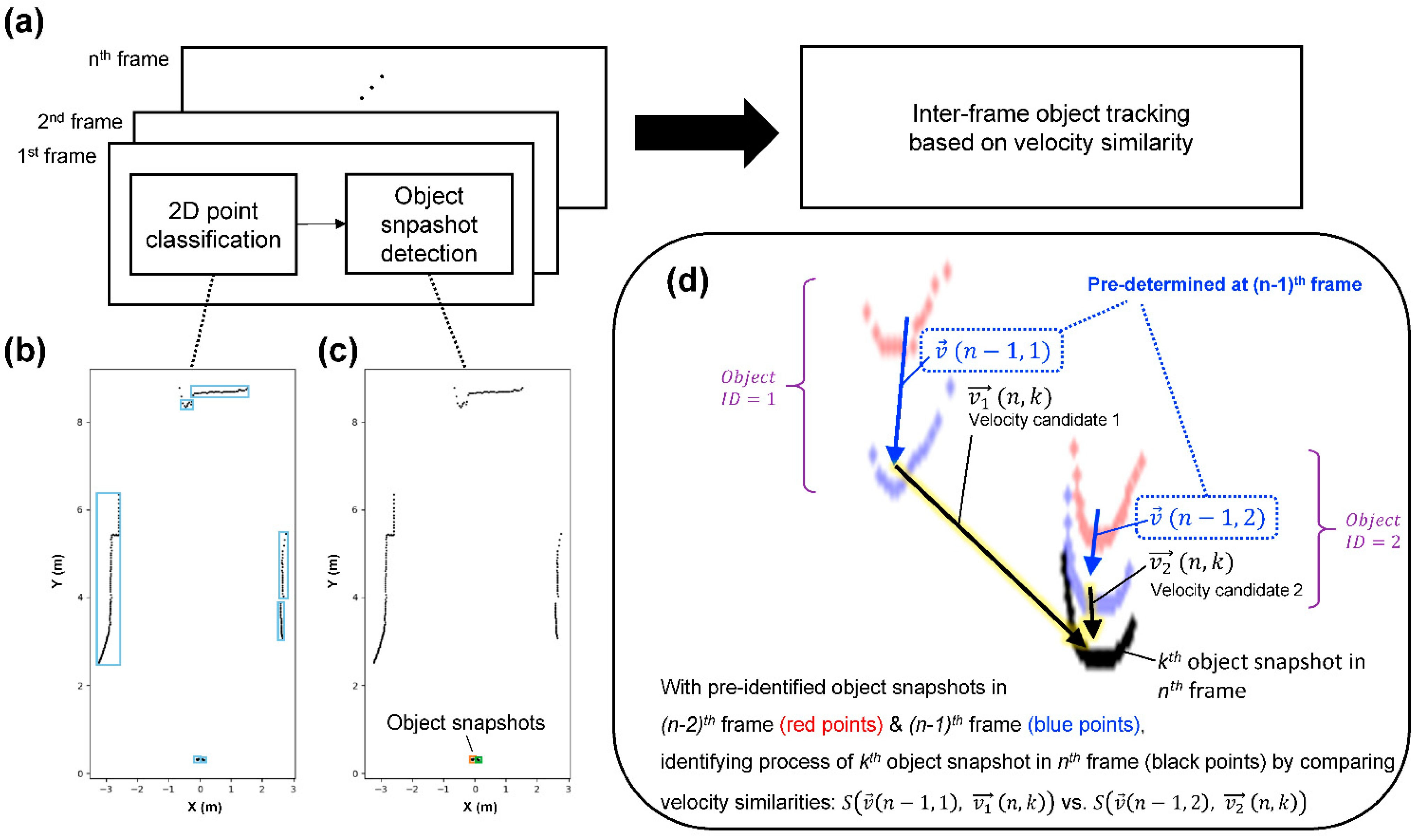
2.3. Object Tracking Algorithm for 2D-LiDAR Sensor
2.4. Object Tracking Algorithm for Stereo Camera
2.5. Performance Evaluation Methods for Object Tracking and Gait Parameters
3. Results
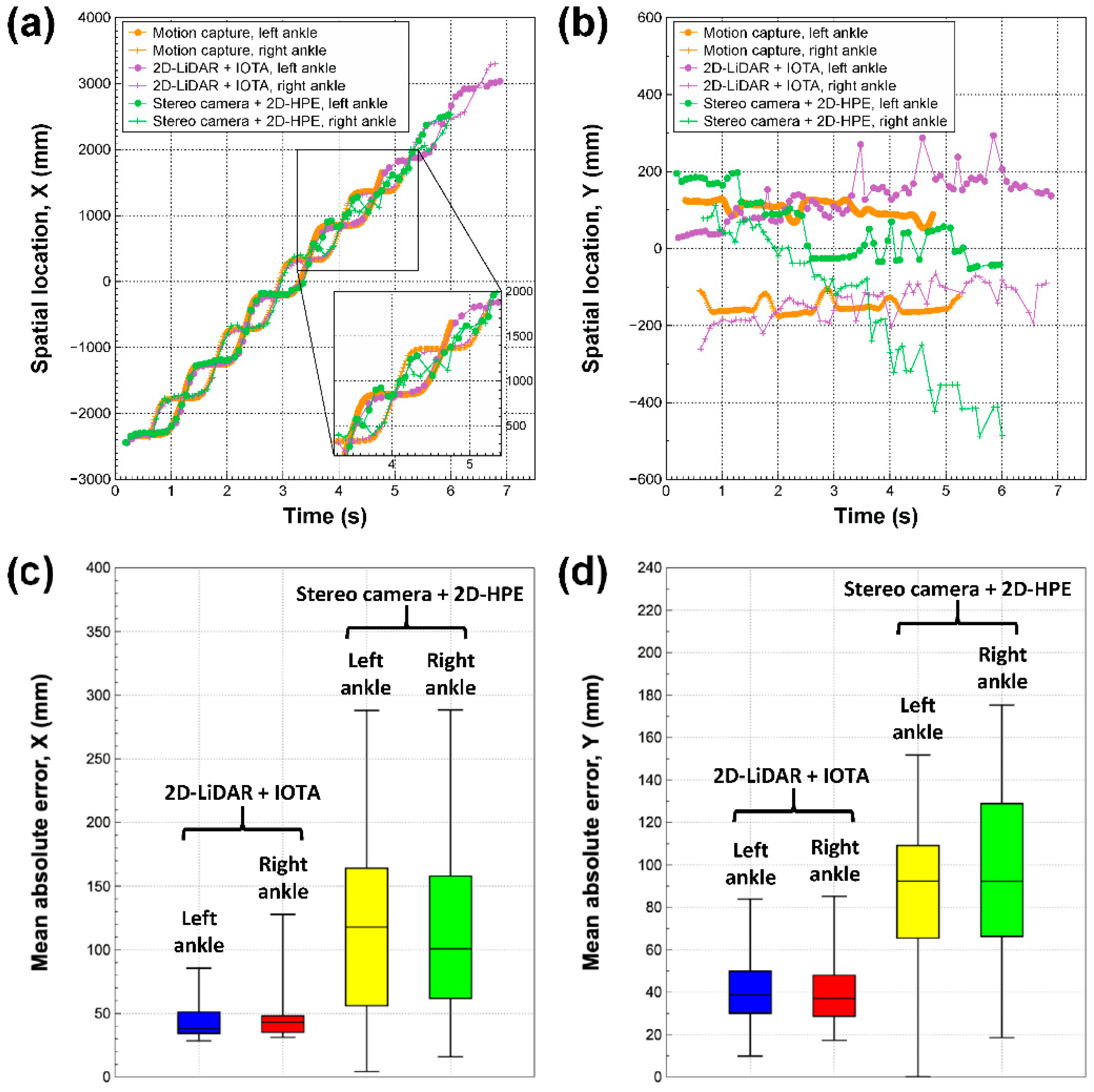
3.1. Spatiotemporal Tracking of Ankle Locations
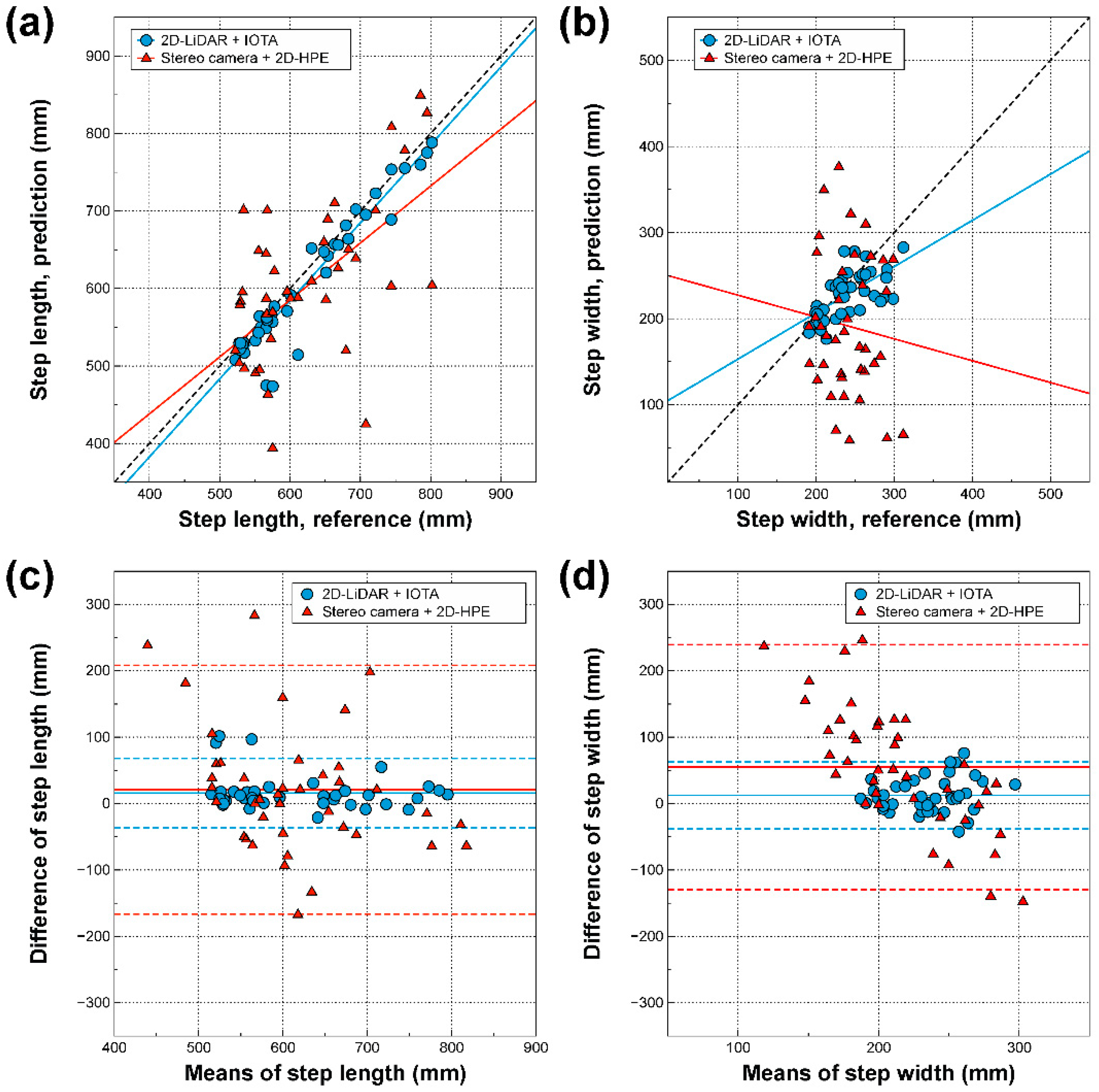
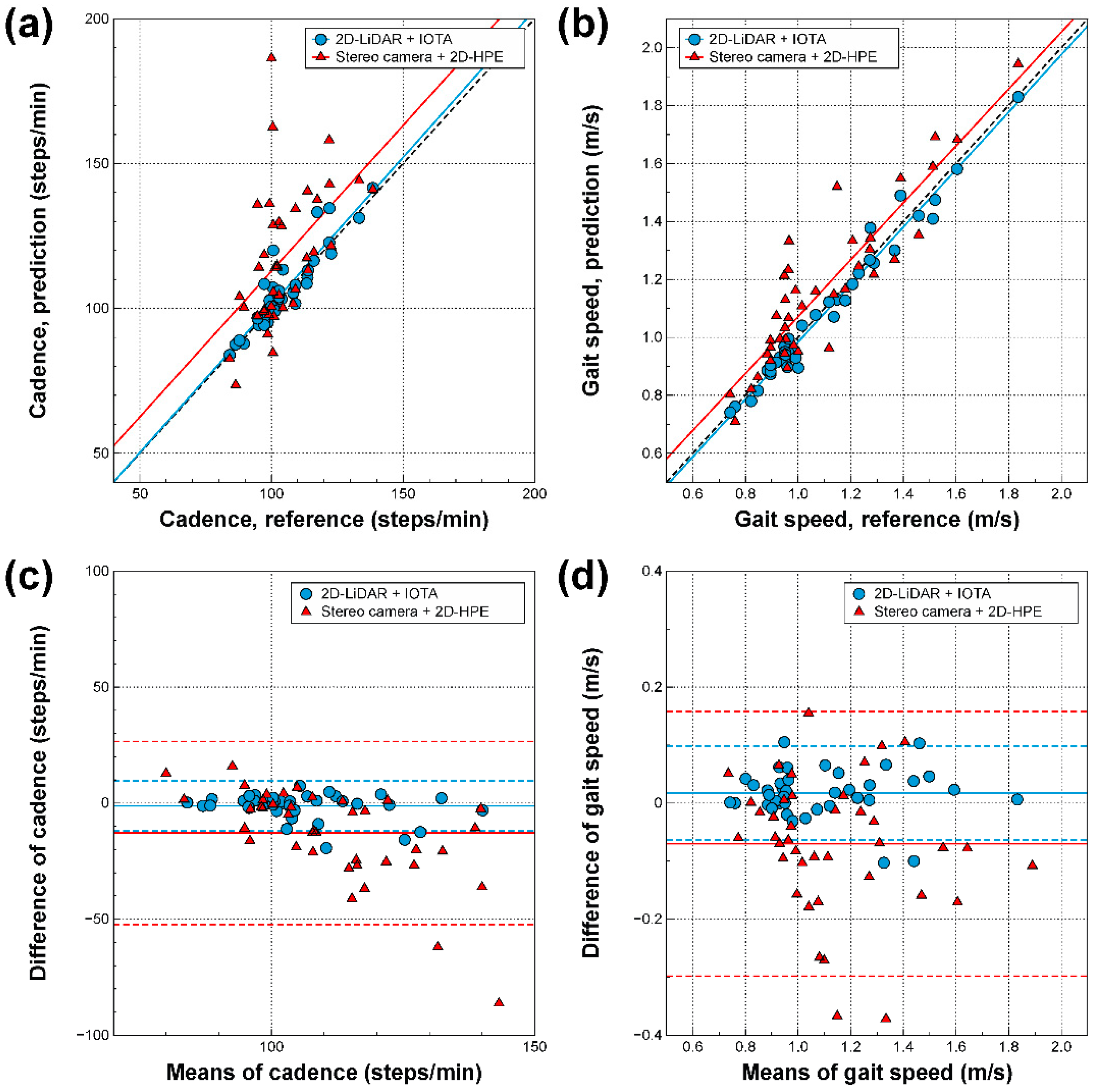
3.2. Correlations Between Gait Parameters Derived from Three Different Modalities
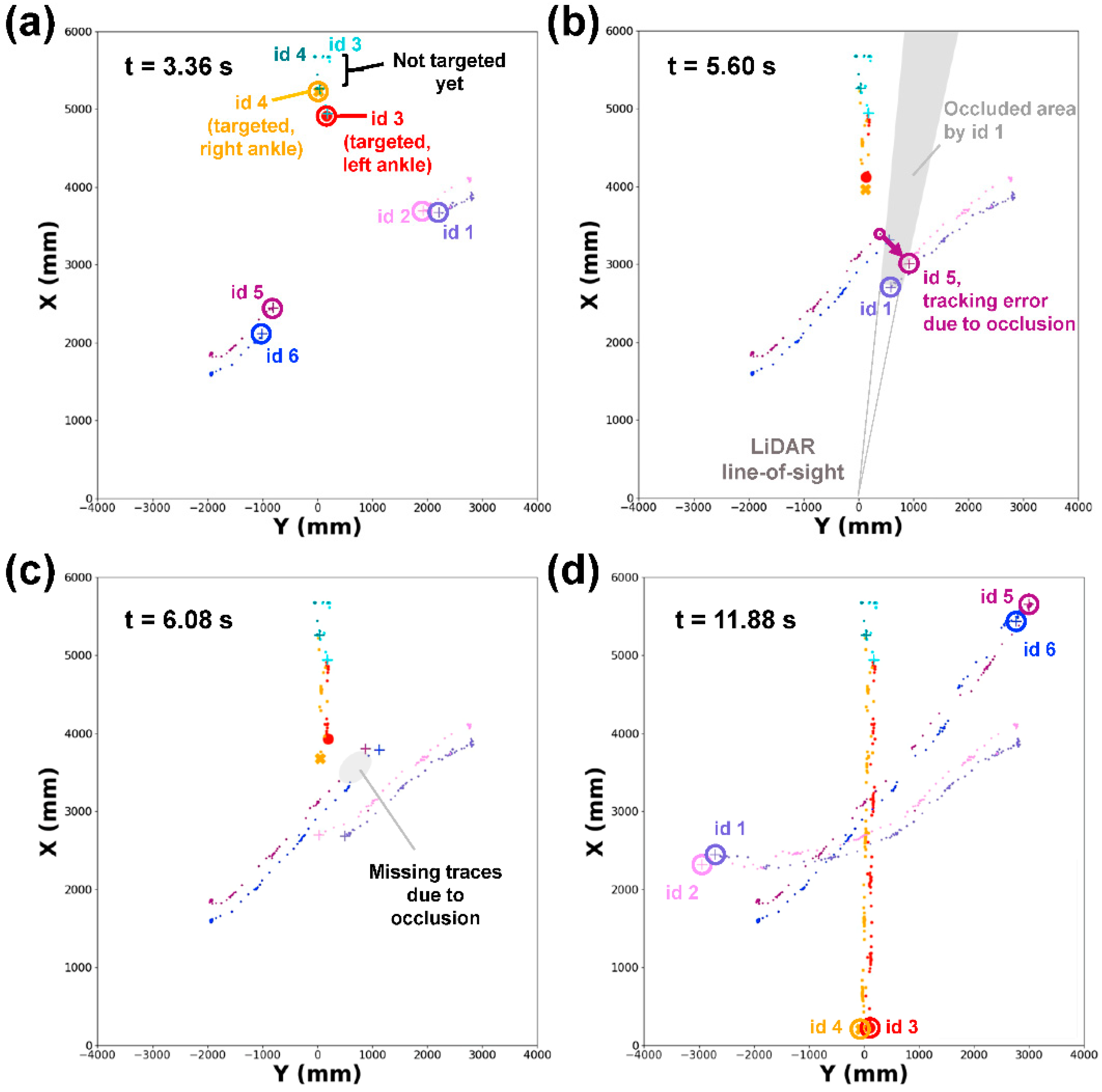
3.3. Demonstration of Multiple Target Tracking by 2D-LiDAR with IOTA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2018, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- High, K.P.; Zieman, S.; Gurwitz, J.; Hill, C.; Lai, J.; Robinson, T.; Schonberg, M.; Whitson, H. Use of Functional Assessment to Define Therapeutic Goals and Treatment. J. Am. Geriatr. Soc. 2019, 67, 1782–1790. [Google Scholar] [CrossRef] [PubMed]
- Pavasini, R.; Guralnik, J.; Brown, J.C.; di Bari, M.; Cesari, M.; Landi, F.; Vaes, B.; Legrand, D.; Verghese, J.; Wang, C.; et al. Short Physical Performance Battery and all-cause mortality: Systematic review and meta-analysis. BMC Med. 2016, 14, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, J.M.; Verlaan, S.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; McMurdo, M.E.; Mets, T.; Seal, C.; Wijers, S.L. Effects of a vitamin D and leucine-enriched whey protein nutritional supplement on measures of sarcopenia in older adults, the PROVIDE study: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2015, 16, 740–747. [Google Scholar] [CrossRef]
- Jang, I.Y.; Jung, H.W.; Park, H.; Lee, C.K.; Yu, S.S.; Lee, Y.S.; Lee, E.; Glynn, R.J.; Kim, D.H. A Multicomponent Frailty Intervention for Socioeconomically Vulnerable Older Adults: A Designed-Delay Study. Clin. Interv. Aging 2018, in press. [Google Scholar] [CrossRef] [Green Version]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking speed: The functional vital sign. J. Aging Phys. Act. 2015, 23, 314–322. [Google Scholar] [CrossRef]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The Impact of Mild Cognitive Impairment on Gait and Balance: A Systematic Review and Meta-Analysis of Studies Using Instrumented Assessment. Gerontology 2017, 63, 67–83. [Google Scholar] [CrossRef] [Green Version]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. J. Am. Med. Assoc. 2011, 305, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Quach, L.; Galica, A.M.; Jones, R.N.; Procter-Gray, E.; Manor, B.; Hannan, M.T.; Lipsitz, L.A. The nonlinear relationship between gait speed and falls: The Maintenance of Balance, Independent Living, Intellect, and Zest in the Elderly of Boston Study. J. Am. Geriatr. Soc. 2011, 59, 1069–1073. [Google Scholar] [CrossRef] [Green Version]
- Alfredsson, J.; Stebbins, A.; Brennan, J.M.; Matsouaka, R.; Afilalo, J.; Peterson, E.D.; Vemulapalli, S.; Rumsfeld, J.S.; Shahian, D.; Mack, M.J.; et al. Gait Speed Predicts 30-Day Mortality after Transcatheter Aortic Valve Replacement: Results from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry. Circulation 2016, 133, 1351–1359. [Google Scholar] [CrossRef]
- Taniguchi, Y.; Yoshida, H.; Fujiwara, Y.; Motohashi, Y.; Shinkai, S. A prospective study of gait performance and subsequent cognitive decline in a general population of older Japanese. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 67, 796–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Holst, H.M.; Tuladhar, A.M.; Zerbi, V.; van Uden, I.W.M.; de Laat, K.F.; van Leijsen, E.M.C.; Ghafoorian, M.; Platel, B.; Bergkamp, M.I.; van Norden, A.G.W.; et al. White matter changes and gait decline in cerebral small vessel disease. Neuroimage Clin. 2017, 17, 731–738. [Google Scholar] [CrossRef]
- Freire Junior, R.C.; Porto, J.M.; Rodrigues, N.C.; Brunelli, R.M.; Braga, L.F.; de Abreu, D.C. Spatial and temporal gait characteristics in pre-frail community-dwelling older adults. Geriatr. Gerontol. Int. 2016, 16, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Bilney, B.; Morris, M.; Webster, K. Concurrent related validity of the GAITRite walkway system for quantification of the spatial and temporal parameters of gait. Gait Posture 2003, 17, 68–74. [Google Scholar] [CrossRef]
- Blumrosen, G.; Miron, Y.; Intrator, N.; Plotnik, M. A Real-Time Kinect Signature-Based Patient Home Monitoring System. Sensors 2016, 16, 1965. [Google Scholar] [CrossRef] [Green Version]
- Blumrosen, G.; Fishman, B.; Yovel, Y. Noncontact wideband sonar for human activity detection and classification. IEEE Sens. J. 2014, 14, 4043–4054. [Google Scholar] [CrossRef]
- Borel, S.; Schneider, P.; Newman, C.J. Video analysis software increases the interrater reliability of video gait assessments in children with cerebral palsy. Gait Posture 2011, 33, 727–729. [Google Scholar] [CrossRef]
- Muro-de-la-Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef] [Green Version]
- Caldas, R.; Mundt, M.; Potthast, W.; de Lima Neto, F.B.; Markert, B. A systematic review of gait analysis methods based on inertial sensors and adaptive algorithms. Gait Posture 2017, 57, 204–210. [Google Scholar] [CrossRef]
- Blumrosen, G.; Luttwak, A. Human body parts tracking and kinematic features assessment based on RSSI and inertial sensor measurements. Sensors 2013, 13, 11289–11313. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.W.; Roh, H.C.; Kim, S.W.; Kim, S.; Kim, M.; Won, C.W. Cross-Comparisons of Gait Speeds by Automatic Sensors and a Stopwatch to Provide Converting Formula Between Measuring Modalities. Ann. Geriatr. Med. Res. 2019, 23, 71–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OpenVINO Toolkit, 4th ed.; Available online: https://docs.openvinotoolkit.org/2019_R1/_human_pose_estimation_0001_description_human_pose_estimation_0001.html (accessed on 3 June 2020).
- Neumann, L.; Vedaldi, A. Tiny People Pose. In Asian Conference on Computer Vision; Springer: Perth, WA, Austraila, 2018; pp. 558–574. [Google Scholar]
- Van Ancum, J.M.; van Schooten, K.S.; Jonkman, N.H.; Huijben, B.; van Lummel, R.C.; Meskers, C.G.M.; Maier, A.B.; Pijnappels, M. Gait speed assessed by a 4-m walk test is not representative of daily-life gait speed in community-dwelling adults. Maturitas 2019, 121, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.W.; Kang, M.G.; Choi, J.Y.; Yoon, S.J.; Kim, S.W.; Kim, K.I.; Kim, C.H. Simple Method of Screening for Frailty in Older Adults Using a Chronometer and Tape Measure in Clinic. J. Am. Geriatr. Soc. 2018, 66, 157–160. [Google Scholar] [CrossRef] [Green Version]
- Jang, I.Y.; Kim, H.R.; Lee, E.; Jung, H.W.; Park, H.; Cheon, S.H.; Lee, Y.S.; Park, Y.R. Impact of a Wearable Device-Based Walking Programs in Rural Older Adults on Physical Activity and Health Outcomes: Cohort Study. JMIR mHealth uHealth 2018, 6, e11335. [Google Scholar] [CrossRef] [PubMed]
- Piau, A.; Mattek, N.; Crissey, R.; Beattie, Z.; Dodge, H.; Kaye, J. When will my patient fall? Sensor-based in-home walking speed identifies future falls in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 968–973. [Google Scholar] [CrossRef] [PubMed]
- Cumbee, S.R.; Pryor, R.E.; Linzer, M. Cardiac loop ECG recording: A new noninvasive diagnostic test in recurrent syncope. South. Med. J. 1990, 83, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Sanders, K.J.C.; Kneppers, A.E.M.; van de Bool, C.; Langen, R.C.J.; Schols, A.M.W.J. Cachexia in chronic obstructive pulmonary disease: New insights and therapeutic perspective. J. Cachexia Sarcopenia Muscle 2016, 7, 5–22. [Google Scholar] [CrossRef]
- Eliason, G.; Abdel-Halim, S.; Arvidsson, B.; Kadi, F.; Piehl-Aulin, K. Physical performance and muscular characteristics in different stages of COPD. Scand. J. Med. Sci. Sports 2009, 19, 865–870. [Google Scholar] [CrossRef]
- Tanaka, S.; Kamiya, K.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Nakamura, T.; Yamashita, M.; Maekawa, E.; Noda, C.; Yamaoka-Tojo, M.; et al. Short-Term Change in Gait Speed and Clinical Outcomes in Older Patients with Acute Heart Failure. Circ. J. 2019, 83, 1860–1867. [Google Scholar] [CrossRef] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, S.; Jung, H.-W.; Jung, H.; Kim, K.; Hong, S.-K.; Roh, H.; Oh, B.-M. Development and Validation of 2D-LiDAR-Based Gait Analysis Instrument and Algorithm. Sensors 2021, 21, 414. https://doi.org/10.3390/s21020414
Yoon S, Jung H-W, Jung H, Kim K, Hong S-K, Roh H, Oh B-M. Development and Validation of 2D-LiDAR-Based Gait Analysis Instrument and Algorithm. Sensors. 2021; 21(2):414. https://doi.org/10.3390/s21020414
Chicago/Turabian StyleYoon, Seongjun, Hee-Won Jung, Heeyoune Jung, Keewon Kim, Suk-Koo Hong, Hyunchul Roh, and Byung-Mo Oh. 2021. "Development and Validation of 2D-LiDAR-Based Gait Analysis Instrument and Algorithm" Sensors 21, no. 2: 414. https://doi.org/10.3390/s21020414