
Inertial Sensor Reliability and Validity for Static and Dynamic Balance in Healthy Adults: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
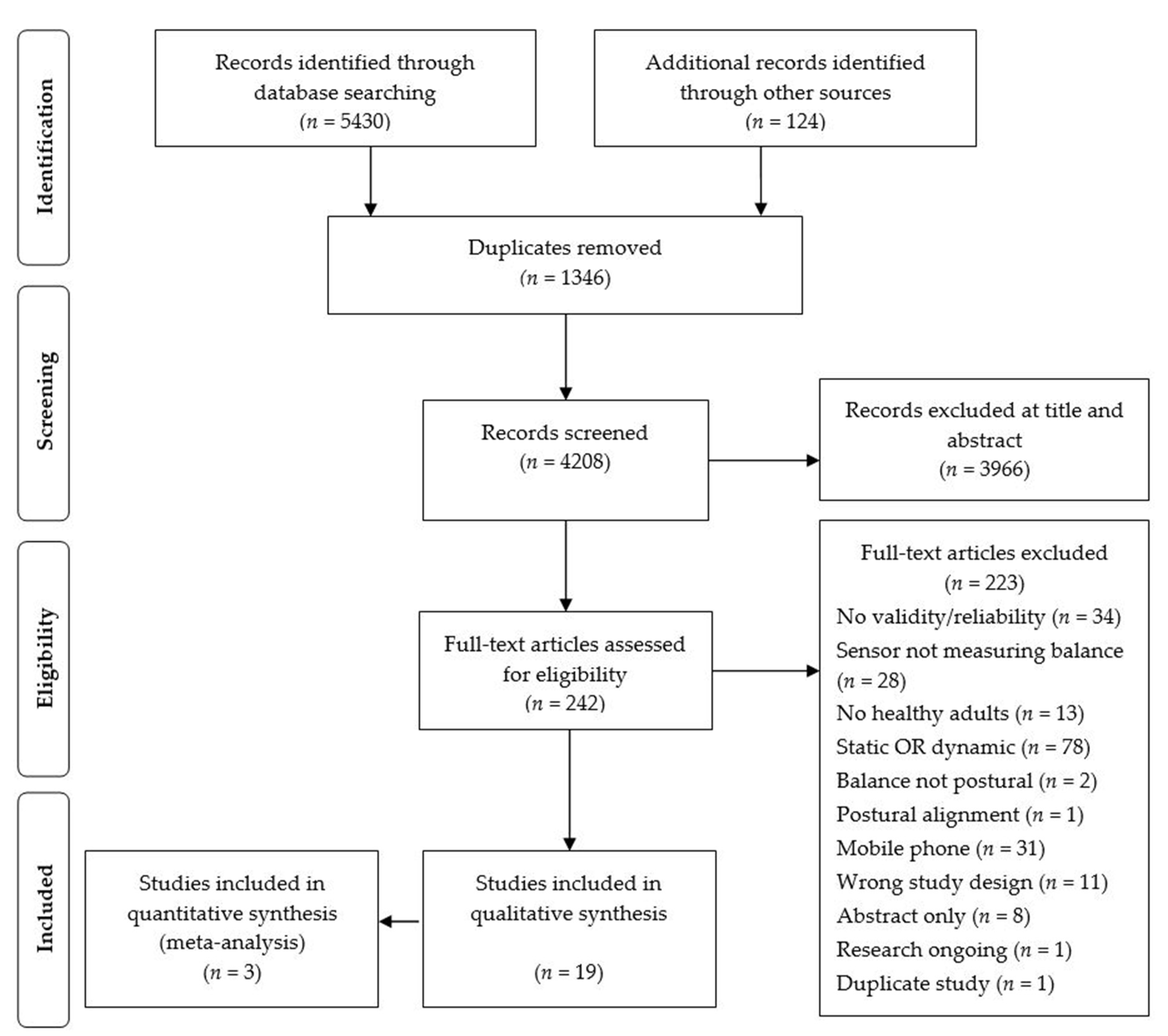
2.1. Search Strategy
2.2. Eligibility, Quality and Data Extraction
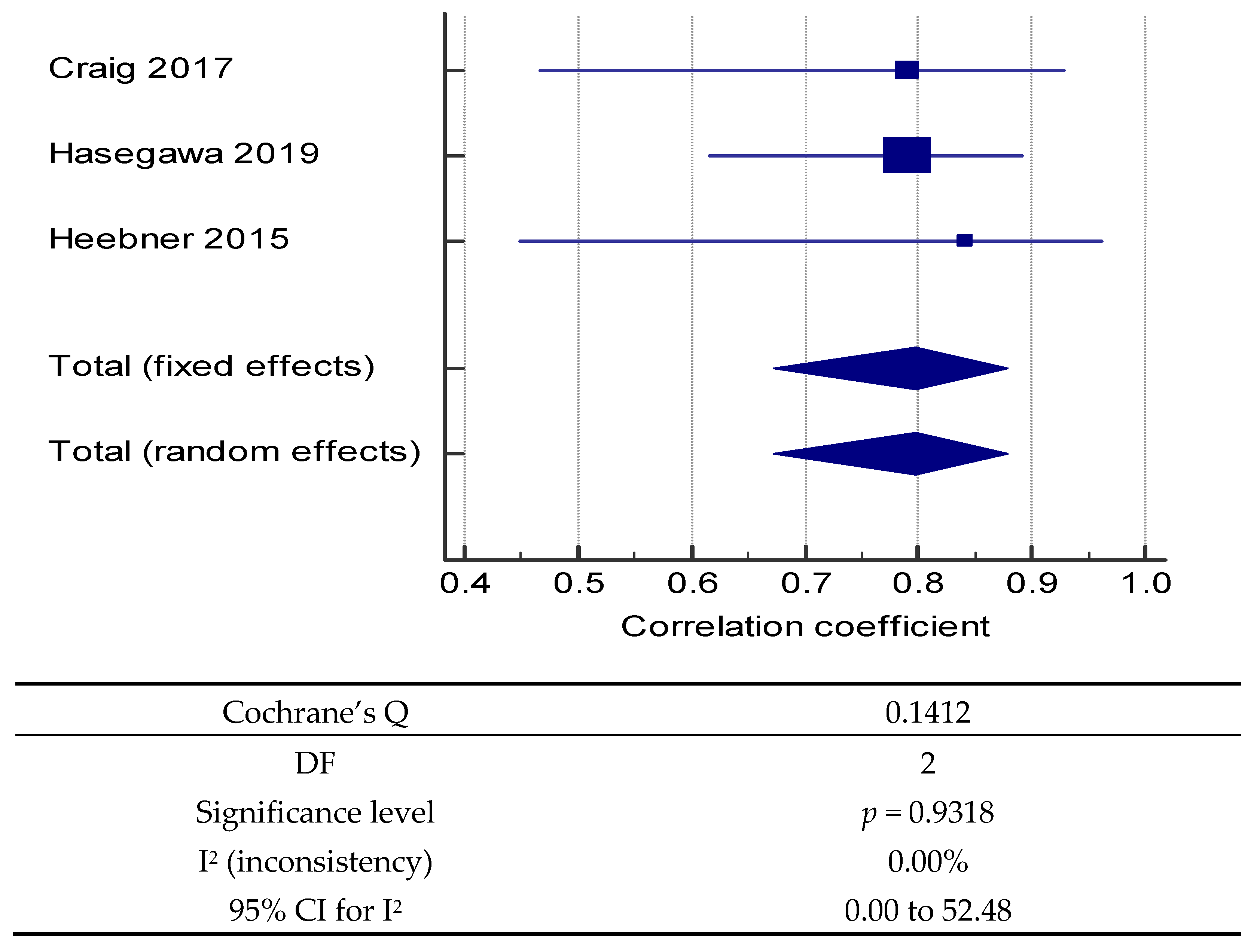
2.3. Data Pooling
2.4. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Quality Assessment
3.3. Sensors
3.4. Validity
3.5. Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| # | Searches | Results |
|---|---|---|
| 1 | postural balance/or posture/or standing position/ | 81,783 |
| 2 | (balance* or postur* or sway* or stability or equilibrium).ti,ab,kf. | 854,996 |
| 3 | (“center of pressure” or “centre of pressure”).ti,ab,kf. | 4573 |
| 4 | (stumbl* or near* fall* or misstep* or mis step*).ti,ab,kf. | 1635 |
| 5 | or/1–4 [Balance concept] | 900,273 |
| 6 | mobile applications/or cell phone/or smartphone/ | 15,528 |
| 7 | Accelerometry/or Magnetometry/ | 5247 |
| 8 | ((body or motion or wearable*) adj2 sensor*1).ti,ab,kf. | 4717 |
| 9 | (acceleromet* or gyroscop* or magnetomet* or goniomet* or inclinomet* or baromet*).ti,ab,kf. | 28,201 |
| 10 | or/6–9 | 84,193 |
| 11 | “reproducibility of results”/or “sensitivity and specificity”/or “predictive value of tests”/ | 774,004 |
| 12 | (accura* or assessment* or measur* or evaluat* or reliab* or reproduc* or consistenc* or repeatab* or validit* or sensitiv* or specificity or respons* or clinimetric or correlat* or concord* or discrim*).ti,ab,kf. | 11,023,968 |
| 13 | or/11–12 | 11,173,078 |
| 14 | and/5, 10, 13 | 4689 |
| 15 | limit 14 to (english language and yr = “2019–Current”) | 711 |
References
- Pollock, A.S.; Durward, B.R.; Rowe, P.J.; Paul, J.P. What is balance? Clin. Rehabil. 2000, 14, 402–406. [Google Scholar] [CrossRef]
- Haagsma, J.A.; Olij, B.F.; Majdan, M.; Van Beeck, E.F.; Vos, T.; Castle, C.D.; James, S.L. Falls in older aged adults in 22 European countries: Incidence, mortality and burden of disease from 1990 to 2017. Inj. Prev. 2020, 26, i67–i74. [Google Scholar] [CrossRef]
- Pang, I.; Okubo, Y.; Sturnieks, D.; Lord, S.R.; Brodie, M.A. Detection of Near Falls Using Wearable Devices: A Systematic Review. J. Geriatr. Phys. Ther. 2019, 42, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Nagai, K.; Yamada, M.; Komatsu, M.; Tamaki, A.; Kanai, M.; Miyamoto, T.; Tsuboyama, T. Near falls predict substantial falls in older adults: A prospective cohort study. Geriatr. Gerontol. Int. 2017, 17, 1477–1480. [Google Scholar] [CrossRef]
- Peeters, G.; van Schoor, N.M.; Cooper, R.; Tooth, L.; Kenny, R.A. Should prevention of falls start earlier? Co-ordinated analyses of harmonised data on falls in middle-aged adults across four population-based cohort studies. PLoS ONE 2018, 13, e0201989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, N.; Grimmer, K.; Gordon, S. Balance provocation tests identify near-falls in healthy community adults aged 40–75 years: An observational study. Physiother. Theory Pract. under Review.
- Ghislieri, M.; Gastaldi, L.; Pastorelli, S.; Tadano, S.; Agostini, V. Wearable Inertial Sensors to Assess Standing Balance: A Systematic Review. Sensors 2019, 19, 4075. [Google Scholar] [CrossRef] [Green Version]
- Roetenberg, D.; Holler, C.; Mattmuller, K.; Degen, M.; Allum, J.H. Comparison of a Low-Cost Miniature Inertial Sensor Module and a Fiber-Optic Gyroscope for Clinical Balance and Gait Assessments. J. Healthc. Eng. 2019, 2019, 9816961. [Google Scholar] [CrossRef] [Green Version]
- Alqahtani, B.A.; Sparto, P.J.; Whitney, S.L.; Greenspan, S.L.; Perera, S.; Brach, J.S. Psychometric properties of instrumented postural sway measures recorded in community settings in independent living older adults. BMC Geriatr. 2020, 20, 82. [Google Scholar] [CrossRef] [Green Version]
- Hubble, R.P.; Naughton, G.A.; Silburn, P.A.; Cole, M.H. Wearable sensor use for assessing standing balance and walking stability in people with Parkinson’s disease: A systematic review. PLoS ONE 2015, 10, e0123705. [Google Scholar] [CrossRef] [Green Version]
- Sun, R.; McGinnis, R.; Sosnoff, J.J. Novel technology for mobility and balance tracking in patients with multiple sclerosis: A systematic review. Expert Rev. Neurother. 2018, 18, 887–898. [Google Scholar] [CrossRef] [PubMed]
- Gordt, K.; Gerhardy, T.; Najafi, B.; Schwenk, M. Effects of Wearable Sensor-Based Balance and Gait Training on Balance, Gait, and Functional Performance in Healthy and Patient Populations: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Gerontology 2017, 64, 74–89. [Google Scholar] [CrossRef]
- Bet, P.; Castro, P.C.; Ponti, M.A. Foreseeing future falls with accelerometer features in active community-dwelling older persons with no recent history of falls. Exp. Gerontol. 2020, 143, 111139. [Google Scholar] [CrossRef] [PubMed]
- Roeing, K.L.; Hsieh, K.L.; Sosnoff, J.J. A systematic review of balance and fall risk assessments with mobile phone technology. Arch. Gerontol. Geriatr. 2017, 73, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Baker, N.; Gough, C.; Gordon, S.J. Classification of balance assessment technology a scoping review of systematic reviews. In IT-Based Approaches Supporting Health Behaviours. Studies in Health Technology and Informatics Series; IOT Press: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Johnston, W.; O’Reilly, M.; Argent, R.; Caulfield, B. Reliability, Validity and Utility of Inertial Sensor Systems for Postural Control Assessment in Sport Science and Medicine Applications: A Systematic Review. Sports Med. 2019, 49, 783–818. [Google Scholar] [CrossRef] [Green Version]
- Pinho, A.S.; Salazar, A.P.; Hennig, E.M.; Spessato, B.C.; Domingo, A.; Pagnussat, A.S. Can we rely on mobile devices and other gadgets to assess the postural balance of healthy individuals? A systematic review. Sensors 2019, 19, 2972. [Google Scholar] [CrossRef] [Green Version]
- Sang, V.N.; Yano, S.; Kondo, T. On-body sensor positions hierarchical classification. Sensors 2018, 18, 3612. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017; Available online: https://reviewersmanual.joannabriggs.org/ (accessed on 10 February 2021).
- Basu, A. How to conduct a metaanalysis: A basic tutorial. PeerJ 2017, 5, e2978v1. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. An application of hierarchical Kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics 1977, 33, 363–374. [Google Scholar] [CrossRef]
- Belur, J.; Tompson, L.; Thornton, A.; Simon, M. Interrater Reliability in Systematic Review Methodology. Sociol. Methods Res. 2018. [Google Scholar] [CrossRef] [Green Version]
- Spain, R.I.; Mancini, M.; Horak, F.B.; Bourdette, D. Body-worn sensors capture variability, but not decline, of gait and balance measures in multiple sclerosis over 18 months. Gait Posture 2014, 39, 958–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heebner, N.R.; Akins, J.S.; Lephart, S.M.; Sell, T.C. Reliability and validity of an accelerometry based measure of static and dynamic postural stability in healthy and active individuals. Gait Posture 2015, 41, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Mendez, R.; Sekine, M.; Tamura, T. Detection of anticipatory postural adjustments prior to gait initiation using inertial wearable sensors. J. Neuroeng. Rehabil. 2011, 8, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leiros-Rodriguez, R.; Arce, M.E.; Miguez-Alvarez, C.; Garcia-Soidan, J.L. Definitions of the proper placement point for balance assessment with accelerometers in older women. Rev. AndaI. Med. Deporte 2016. [Google Scholar] [CrossRef]
- Greene, B.R.; McGrath, D.; Walsh, L.; Doheny, E.P.; McKeown, D.; Garattini, C.; Cunningham, C.; Crosby, L.; Caulfield, B.; Kenny, R.A. Quantitative falls risk estimation through multi-sensor assessment of standing balance. Physiol. Meas. 2012, 33, 2049–2063. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, X.; Lockhart, T. Fall Risk Assessments Based on Postural and Dynamic Stability Using Inertial Measurement Unit. Saf. Health Work 2012, 3, 192–198. [Google Scholar] [CrossRef]
- Rivolta, M.W.; Aktaruzzaman, M.; Rizzo, G.; Lafortuna, C.L.; Ferrarin, M.; Bovi, G.; Sassi, R. Evaluation of the Tinetti score and fall risk assessment via accelerometry-based movement analysis. Artif. Intell. Med. 2019, 95, 38–47. [Google Scholar] [CrossRef]
- Tang, W.L.; Fulk, G.; Zeigler, S.; Zhang, T.; Sazonov, E. Estimating Berg Balance Scale and Mini Balance Evaluation System Test Scores by Using Wearable Shoe Sensors. In Proceedings of the IEEE International Conference on Biomedical & Health Informatics, Chicago, IL, USA, 19–22 May 2019; IEEE: New York, NY, USA, 2019. [Google Scholar]
- Bzduskova, D.; Valkovic, P.; Hirjakova, Z.; Kimijanova, J.; Hlavacka, F. Parkinson’s disease versus ageing: Different postural responses to soleus muscle vibration. Gait Posture 2018, 65, 169–175. [Google Scholar] [CrossRef]
- De Vos, M.; Prince, J.; Buchanan, T.; FitzGerald, J.J.; Antoniades, C.A. Discriminating progressive supranuclear palsy from Parkinson’s disease using wearable technology and machine learning. Gait Posture 2020, 77, 257–263. [Google Scholar] [CrossRef]
- Hasegawa, N.; Shah, V.V.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B.; Mancini, M. How to Select Balance Measures Sensitive to Parkinson’s Disease from Body-Worn Inertial Sensors-Separating the Trees from the Forest. Sensors 2019, 19, 3320. [Google Scholar] [CrossRef] [Green Version]
- Mancini, M.; Chiari, L.; Holmstrom, L.; Salarian, A.; Horak, F.B. Validity and reliability of an IMU-based method to detect APAs prior to gait initiation. Gait Posture 2016, 43, 125–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, J.J.; Bruetsch, A.P.; Lynch, S.G.; Horak, F.B.; Huisinga, J.M. Instrumented balance and walking assessments in persons with multiple sclerosis show strong test-retest reliability. J. Neuroeng. Rehabil. 2017, 14, 43. [Google Scholar] [CrossRef]
- Spain, R.I.; St George, R.J.; Salarian, A.; Mancini, M.; Wagner, J.M.; Horak, F.B.; Bourdette, D. Body-worn motion sensors detect balance and gait deficits in people with multiple sclerosis who have normal walking speed. Gait Posture 2012, 35, 573–578. [Google Scholar] [CrossRef] [Green Version]
- Dalton, A.; Khalil, H.; Busse, M.; Rosser, A.; van Deursen, R.; Olaighin, G. Analysis of gait and balance through a single triaxial accelerometer in presymptomatic and symptomatic Huntington’s disease. Gait Posture 2013, 37, 49–54. [Google Scholar] [CrossRef]
- Jimenez-Moreno, A.C.; Charman, S.J.; Nikolenko, N.; Larweh, M.; Turner, C.; Gorman, G.; Lochmuller, H.; Catt, M. Analyzing walking speeds with ankle and wrist worn accelerometers in a cohort with myotonic dystrophy. Disabil. Rehabil. 2019, 41, 2972–2978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsushima, A.; Yoshida, K.; Genno, H.; Murata, A.; Matsuzawa, S.; Nakamura, K.; Nakamura, A.; Ikeda, S. Clinical assessment of standing and gait in ataxic patients using a triaxial accelerometer. Cerebellum Ataxias 2015, 2, 9. [Google Scholar] [CrossRef] [Green Version]
- Velazquez-Perez, L.; Rodriguez-Labrada, R.; Gonzalez-Garces, Y.; Arrufat-Pie, E.; Torres-Vega, R.; Medrano-Montero, J.; Ramirez-Bautista, B.; Vazquez-Mojena, Y.; Auburger, G.; Horak, F.; et al. Prodromal Spinocerebellar Ataxia Type 2 Subjects Have Quantifiable Gait and Postural Sway Deficits. Mov. Disord. 2020. [Google Scholar] [CrossRef]
- O’Brien, M.K.; Hidalgo-Araya, M.D.; Mummidisetty, C.K.; Vallery, H.; Ghaffari, R.; Rogers, J.A.; Lieber, R.; Jayaraman, A. Augmenting Clinical Outcome Measures of Gait and Balance with a Single Inertial Sensor in Age-Ranged Healthy Adults. Sensors 2019, 19, 4537. [Google Scholar] [CrossRef] [Green Version]
- Senanayake, S.M.; Malik, O.A.; Iskandar, M.; Zaheer, D. 3-D kinematics and neuromuscular signals’ integration for post ACL reconstruction recovery assessment. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2013, 7221–7225. [Google Scholar] [CrossRef]
- Patel, M.; Pavic, A.; Goodwin, V.A. Wearable inertial sensors to measure gait and posture characteristic differences in older adult fallers and non-fallers: A scoping review. Gait Posture 2020, 76, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Noamani, A.; Nazarahari, M.; Lewicke, J.; Vette, A.H.; Rouhani, H. Validity of using wearable inertial sensors for assessing the dynamics of standing balance. Med. Eng. Phys. 2020, 77, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Valldeperes, A.; Altuna, X.; Martinez-Basterra, Z.; Rossi-Izquierdo, M.; Benitez-Rosario, J.; Perez-Fernandez, N.; Rey-Martinez, J. Wireless inertial measurement unit (IMU)-based posturography. Europ. Arch. Oto-Rhino-Laryngol. 2019, 276, 3057–3065. [Google Scholar] [CrossRef] [PubMed]
- Ofori, E.K.; Wang, S.; Bhatt, T. Validity of Inertial Sensors for Assessing Balance Kinematics and Mobility during Treadmill-Based Perturbation and Dance Training. Sensors 2021, 21, 3065. [Google Scholar] [CrossRef] [PubMed]
- Handelzalts, S.; Alexander, N.B.; Mastruserio, N.; Nyquist, L.V.; Strasburg, D.M.; Ojeda, L.V. Detection of real-world trips in at-fall risk community dwelling older adults using wearable sensors. Front. Med. 2020, 7, 514. [Google Scholar] [CrossRef]
- Abbaspour, S.; Ghazvini, F.F. Mobile smart systems to detect balance motion in rehabilitation. In Lecture Notes in Electrical Engineering; Springer: Berlin/Heidelberg, Germany, 2019; Volume 480, pp. 777–785. [Google Scholar]
- Donath, L.; Kurz, E.; Roth, R.; Zahner, L.; Faude, O. Leg and trunk muscle coordination and postural sway during increasingly difficult standing balance tasks in young and older adults. Maturitas 2016, 91, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Cimolin, V.; Cau, N.; Albedi, G.M.; Aspesi, V.; Merenda, V.; Galli, M.; Capodaglio, P. Do wearable sensors add meaningful information to the Timed Up and Go test? A study on obese women. J. Electromyogr. kinesiol. 2019, 44, 78–85. [Google Scholar] [CrossRef] [PubMed]
- White, A.M.; Tooth, L.R.; Peeters, G.M.E.E. Fall risk factors in mid-age women: The Australian Longitudinal Study on Women’s Health. Am. J. Prev. Med. 2018, 54, 51–63. [Google Scholar] [CrossRef]


| Author, Year, Setting, Country [Reference] | Study Population, Number (Sex) Age in Years Mean ± SD (Range) | Healthy Group Number (Sex) Age in Years Mean ± SD (Range) | Static Balance Activity | Dynamic Balance Activity | Clinical Balance Measure | Outcome Measure |
|---|---|---|---|---|---|---|
| Bzduskova et al., 2018, NA, Slovak Republic, [32] | PD n = 13 (8M 5F) 63.7 ± 5.7 y | Young n = 13 (4M 9F) 25.0 ± 2.3 y Older n = 13 (4M 9F) 70.1 ± 4.5 y | FA EO, FA EC | Step with vibration | NA | RMS acc AP ML, jerk, mean veloc, peak veloc, stride length, stride veloc, cadence, stance time |
| Craig et al., 2017, Lab, USA [36] | MS n = 15 (3M 12F) 48.2 ± 8.7 y | HC n = 15 (3M 12F) 47.8 ± 9.5 y | FA EO | 7 m TUG | TUG | RMS acc ML AP V |
| Dalton et al., 2013, Lab, Wales, UK [38] | HD Pre-manifest n = 10 (4M 6F) 44.8 ± 11.7 y Manifest n = 14 (8M 6F) 51.8 ± 14.8 y | HC n = 10 (5M 5F) 56.4 ± 10.9 y | FT EO, FT EC | 5 m walk | Romberg | ENMO |
| De Vos et al., 2020, Lab, England, UK [33] | PSP n = 21 (12M 9F) 71 y (63–89) PD n = 20 (11M 9F) 66.4 y (50–79) | HC n = 39 (19M 20F) 67.1 y (51–82) | FA EC | TUG, 2 min walk | TUG | min, max, mean acc AP ML V |
| Greene et al., 2012, Hospital clinic, Ireland [28] | Fallers n = 100 (NA) Whole study (57M 63F) 73.3 ± 5.8 y | Non-faller n = 20 (NA) | Semi TS EO 40 s, FT EC 30 s, Turn head | STS, stand to sit, transfer, fwd reach, pick up object, turn 360, place foot on stool | BBS | Peak accel, jerk, stride length, stride veloc, cadence, stance time. |
| Hasegawa et al., 2019, NA, USA [34] | PD n = 144 (93M 51F) 68.4 ± 8.0 y | HC n = 79 (48M 31F) 68.2 ± 8.1 y | FT EO, FT EC, FT EO soft, FT EC soft, LOS, APA, APR | Step, ISAW, ISAW single task, ISAW dual task | ISAW MiniBEST | RMS acc ML AP; cadence. |
| Heebner et al., 2015, NA, USA [25] | NA | Healthy Reliability n = 10 (10M 0F) 24.3 ± 4.2 y Validity n = 13 (13M 0F) 24.1 ± 3.1 y | FA EO, FA EC, FAEO soft, FAEC soft, TS EO, TS EC, SLS EO, SLS EC. | DPSI-AP, DPSI-ML | NA | RMS acc AP ML, mean acc AP ML, stride length, stride veloc, stance time. |
| Jimenez-Moreno et al., 2019, NA, England UK [39] | MD n = 30 (20M 10F) 48 y (25–72) | HC n = 14 (6M 8F) 32 y (23–47) | FA EO | 6 minWT, 10 mWT, 10 m Walk/Run Test | 6 minWT | Peak trunk veloc sagittal. |
| Leiros-Rodriguez et al., 2016, NA, Spain [27] | NA | n = 66 (0M 66F) 64.9 ± 7.6 y | SLS EC, SLS EO soft | walk 10 m, turn, walk 10 m | NA | RMS acc ML AP, stride length, cadence. |
| Liu et al., 2012, NA, USA [29] | Fallers n = 4 (2M 2F) 74.5 ± 2.7 y | Young n = 4 (1M 3F) 21.8 y ± 1.0 y Older n = 4 (2M 2F) 73.3 ± 7.1 y | FA EO, FT EO, FA EC 10 s | Treadmill walk | NA | RMS acc AP ML V, jerk, sway area, path length, mean velocity, cadence. |
| Mancini et al., 2016, Lab (validity), clinic (reliability) USA [35] | PD Validity n = 10 (8M 2F) 67.2 ± 5 y Reliability n = 17 (12M 5F) 67.1 ± 7.0 y | HC Validity n = 12 (9M 3F) 68.0 ± 5.0 y Reliability n = 17 (6M 11F) 67.9 ± 6.0 y | FA EO | APA, first step, walk | NA | Peak acc ML AP, angular veloc, APA duration, step length, step velocity. |
| Martinez-Mendez et al., 2011, NA, Japan [26] | NA | n = 10 (7M 3F) 26 ± 3 y | FA 2 cm EO | APA, step fwd | NA | RMS acc AP ML, peak acc AP ML, sway area, jerk, trunk veloc sagittal, stride length, stride veloc, stance time, cadence. |
| Matsushima et al., 2015, NA, Japan [40] | SCA or CA n = 51 (24M 27F) 60.3 ± 10.4 y | HC n = 56 (28M 28F) 57.2 ± 14.1 y | FA EO, FA EC, FT EO, FT EC | walk 10 m | NA | VM horizontal acc; gait velocity, cadence, step length, step regularity, RMS ratio. |
| O’Brien et al., 2019, NA, USA [42] | Stroke n = 1 (1M 0F) 57 y | Young n = 14 (8M 6F) 26.4 ± 3.9 y Middle n = 19 (8M 11F) 43.7 ± 5.8 y Older n = 16 (8M 8F) 61.8 ± 5.1 y | FA EO, FA EC, FT EO, TS EO, SLS EO | 10 mWT normal veloc, 10 mWT high veloc, TUG | BBS TUG | Max/mean acc AP ML V, stride length. |
| Rivolta et al., 2019, Rehab Centre, Italy [30] | Inpatient Fallers n = 33 (26M 7F) 72.7 ± 15.2 y | Inpatient n = 46 (30M 16F) 72.5 ± 11.5 y Volunteers n = 11 (0M 11F) 35.7 ± 14.0 y | FA EO, FA EC, FA EC nudge | 360° turn, walk 10 m, sit to stand, stand to sit | Tinetti test | RMS acc AP ML V; mean acc AP ML V; VM; step height/length/symmetry/continuity, trunk sway. |
| Senanayake et al., 2013, NA, Brunei Darussalam [43] | ACLR rehab n = 8 (6M 2F) 31.0 ± 4.1 y | HC n = 4 (3M 1F) 31.0 ± 8.3 y | SLS EO, SLS EC | Treadmill 4 kph; Treadmill 6 kph | NA | RMS acc AP ML. |
| Spain, St George et al., 2012, NA, USA [37] | MS n = 31 (12M 19F) 39.8 y (24–67) | HC n = 28 (9M 19F) 37.4 y (26–60) | FA EO, FA EC | T25FW, 7 m TUG | ABC, MSWS12, EDSS TUG | RMS accel AP ML, jerk, mean/peak/sway veloc, stride length, cadence, turning time, trunk rotation. |
| Tang et al., 2019, Uni, USA [31] | Fallers n = 14 Whole study n = 30 (13M 17F) 76.0 ± 10.5 y | Non faller n = 16 (NA) | FA EO | MiniBEST including TUG and dual task TUG; BBS | BBS, MiniBEST, TUG | Peak acc AP ML V, cadence, stride/step/swing, stance time. |
| Velazquez-Perez et al., 2020, research centre, Cuba [41] | SCA n = 30 (7M 23F) 43.5 ±10.5 y | HC n = 30 (7M 23F) 43.3 ± 10.2 y | FA EO FT, TS | 10 m walk, Tandem walk 10 steps |
| Author, Year, [Reference] | Inclusion Criteria Defined | Subject, Setting Described | Exposure Valid Reliable | Objective Standard Criteria | Confounders Identified | Confounder Strategies | Outcomes Valid Reliable | Appropriate Stats Analysis |
|---|---|---|---|---|---|---|---|---|
| Bzduskova, 2018 [32] | + | - | + | + | + | + | + | + |
| Craig, 2017 [36] | + | + | + | + | + | + | + | + |
| Dalton, 2013 [38] | - | + | + | + | - | - | + | + |
| De Vos, 2020 [33] | + | + | + | + | + | + | + | + |
| Greene, 2012 [28] | + | + | + | + | + | + | + | + |
| Hasegawa, 2019 [34] | + | - | + | + | - | - | + | + |
| Heebner, 2015 [25] | + | - | + | + | - | - | + | + |
| Jimenez-Moreno, 2019 [39] | - | - | + | - | + | + | + | + |
| Leiros-Rodriguez, 2016 [27] | - | - | + | + | + | + | + | + |
| Liu, 2012 [29] | - | - | + | + | - | - | + | + |
| Mancini 1, 2016 [35] | + | + | + | + | + | + | + | + |
| Martinez-Mendez, 2011 [26] | + | - | + | + | - | - | + | + |
| Matsushima, 2015 [40] | + | - | + | + | + | + | + | + |
| O’Brien, 2019 [42] | + | - | + | + | + | + | + | + |
| Rivolta, 2019 [30] | + | + | + | + | + | + | + | + |
| Senanayake, 2013 [43] | + | - | + | + | + | + | + | + |
| Spain, 2012 [37] | + | - | + | + | + | + | + | + |
| Tang, 2019 [31] | + | + | + | + | + | + | + | + |
| Velazquez-Perez, 2020 [41] | + | + | + | + | + | + | + | + |
| Reference, Year | Sensor Type (Brand) | Number, (Body Location), Fixation | Sampling Frequency | Variables | Data Analysis Tool |
|---|---|---|---|---|---|
| Bzduskova et al., 2018 [32] | Dual axis accel (ADXL202) | 2, (T4, L5), NS | 100 Hz | Low pass filtered; cut-off frequency 5 Hz; Butterworth filter; calibration for ±30° range body tilt | MATLAB software |
| Craig et al., 2017 [36] | Triaxial accel/gyro (Opal) | 6, (sternum, L5, bilat wrists, bilat ankles), elastic straps | 128 Hz | Accel ranges ± 16 g, ±200 g; gyro range ±2000 deg/s | Mobility Lab software (APDM) |
| Dalton et al., 2013 [38] | Triaxial accel (AD-BRC) | 1, (sternum), NS | 250 Hz | Range ± 2.5–10 g, calibration by rotation through established angles; high pass filtered, 3rd order normalized elliptical filter, passband frequency 0.25 Hz | MATLAB software |
| De Vos et al., 2020 [33] | Triaxial accel/gyro (Opal) | 6, (sternum, L5, bilat wrists, bilat feet), NS | 100 Hz | Wireless data stream to laptop | Mobility Lab software |
| Greene et al., 2012 [28] | Triaxial accel/gyro (SHIMMER) | 1, (L3), adhesive tape | 102.4 Hz | Calibration using standard method; data streamed via Bluetooth to laptop | MATLAB |
| Hasegawa et al., 2019 [34] | Triaxial accel/gyro (Opal) | 8, (sternum, L5, bilat wrists, bilat shins, bilat feet), elastic straps | 128 Hz | Unscented Kalman Filter | Mobility Lab (APDM) and MATLAB |
| Heebner et al., 2015 [25] | Triaxial accel (ADXL78) | 1, (L5), neoprene belt | 100 Hz | Range ± 16 g, built in data acquisition and storage, low pass filter 50 Hz | MATLAB |
| Jimenez-Moreno et al., 2019 [39] | Triaxial accel (GENEActiv) | 4, (bilat wrists, bilat ankles), elastic band | 100 Hz | Output metric ENMO–mg. | R software |
| Leiros-Rodriguez et al., 2016 [27] | Triaxial accel (GT3 Plus) | 3, (T4, L4, L5), adhesive tape | 100 Hz | Configured 1 s timeframe. Concurrent analysis video & accelerometry data; reviewed analysis. | ActiLife software |
| Liu et al., 2012 [29] | Triaxial accel/gyro (MTX Xsens) | 2, (L5, ankle), NS | 50 Hz | Maximum Lyapunov exponent | MATLAB |
| Mancini et al., 2016 [35] | Triaxial accel/gyro (Opal validity; MTX Xsens reliability) | 6 validity/3 reliability (sternum, L5, bilat wrists, bilat ankles) elastic straps | 128 Hz Opal; 50 Hz MTX Xsens | 3.5 Hz cut-off, zero-phase, low-pass Butterworth filter. Resampling from inertial sensor, force platform and infrared cameras at 50 Hz. | MATLAB |
| Martinez-Mendez et al., 2011 [26] | Unit with triaxial accel (MMA, Freescale) & gyros (X3500 Epson; ENC-03RC Matura) | 2, (L3/4, ankle of dominant foot), NS | 100 Hz | Accel range ± 1.5 g, gyro range ± 80 deg/s; response freq 0.01–58 Hz. Bluetooth transmission | MATLAB |
| Matsushima et al., 2015 [40] | Triaxial accel (Jukudai Mate) | 1, (L3), elastic belt | 20 Hz | Detection range ± 10 g; resolution power 0.02 g | BIMUTAS II |
| O’Brien et al., 2019 [42] | Triaxial accel/gyro (BioStampRC) | 1, (L5), Tegaderm adhesive film | 31.25 Hz | Accel ± 4 g; gyro ± 2000 deg/s; 4th order low pass Butterworth filter 2 Hz; acquisition with BioStampRC | MATLAB |
| Rivolta et al., 2019 [30] | Triaxial accel (GENEActiv) | 1, (chest), elastic band | 50 Hz | 12 bits over range ± 8 g; chronometer for starting time; high pass 3rd order Butterworth filter | Manually segmented accel signals; GENEActiv software |
| Senanayake et al., 2013 [43] | Triaxial accel/gyro (KinetiSense) | 4, (bilat thighs, bilat shins), NS | 128 Hz | Wireless transmission via USB | KinetiSense and MATLAB |
| Spain, St George et al., 2012 [37] | Triaxial accel/gyro (XSens) | 6, (sternum, L5, bilat wrists, bilat ankles), NS | 50 Hz | Accel range ± 1.7 g; gyro range ± 300 deg/s. Filtered with 3.5 Hz cutoff, zero phase, low pass Butterworth filter | MATLAB |
| Tang et al., 2019 [31] | Triaxial accel (ADXL330) | 2, (hip, foot), NS | 400 Hz, down sampled to 25 Hz | Common and Activity Specific features extracted; mRMR feature selection | MATLAB |
| Velazquez-Perez et al., 2020 [41] | Triaxial accel/gyro (Opal) | 6, (Hands, feet, sternum, L5), NS | NS | NS | STATISTICA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baker, N.; Gough, C.; Gordon, S.J. Inertial Sensor Reliability and Validity for Static and Dynamic Balance in Healthy Adults: A Systematic Review. Sensors 2021, 21, 5167. https://doi.org/10.3390/s21155167
Baker N, Gough C, Gordon SJ. Inertial Sensor Reliability and Validity for Static and Dynamic Balance in Healthy Adults: A Systematic Review. Sensors. 2021; 21(15):5167. https://doi.org/10.3390/s21155167
Chicago/Turabian StyleBaker, Nicky, Claire Gough, and Susan J. Gordon. 2021. "Inertial Sensor Reliability and Validity for Static and Dynamic Balance in Healthy Adults: A Systematic Review" Sensors 21, no. 15: 5167. https://doi.org/10.3390/s21155167