
Blue as an Underrated Alternative to Green: Photoplethysmographic Heartbeat Intervals Estimation under Two Temperature Conditions †

Abstract
:1. Introduction
2. Materials and Methods
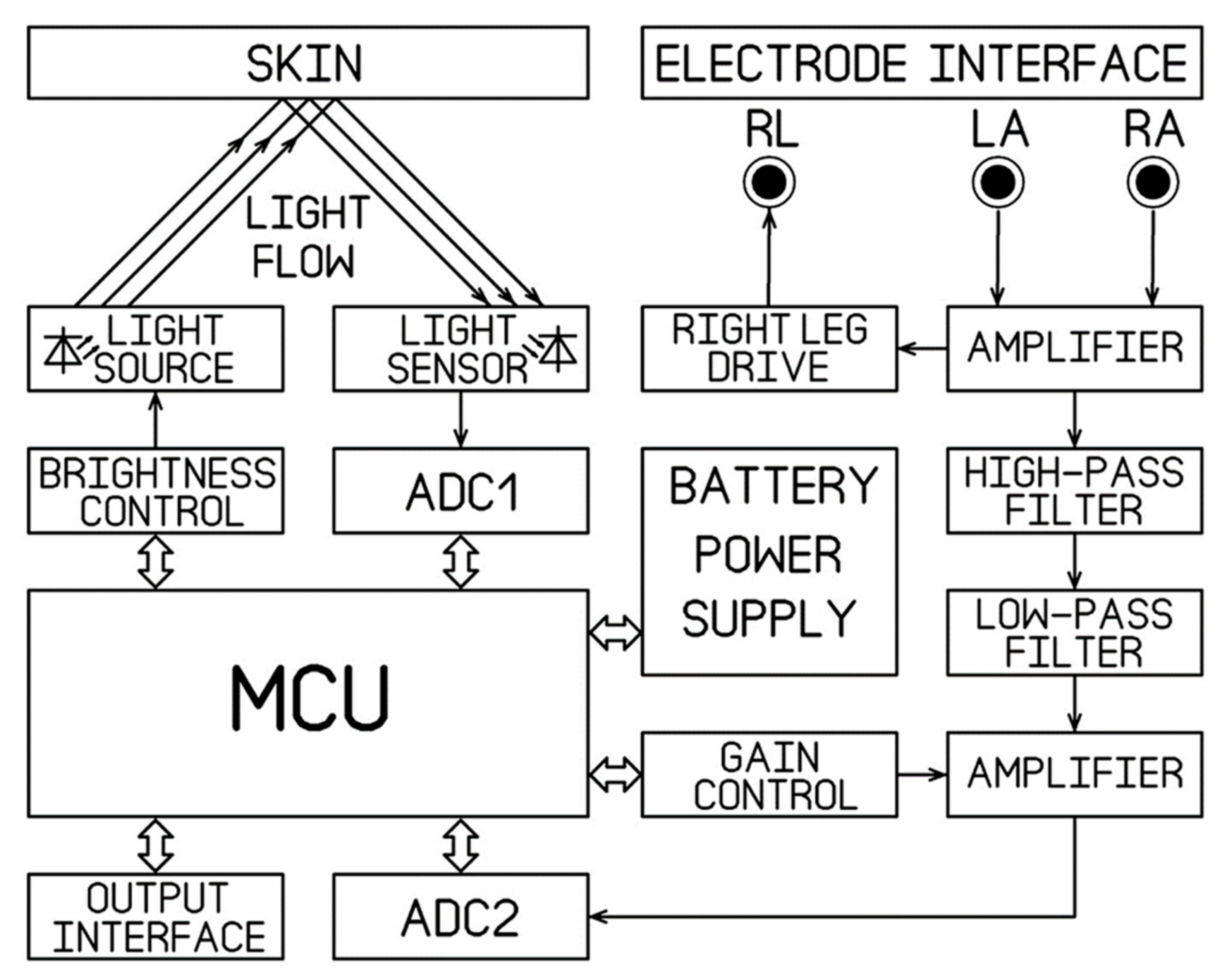
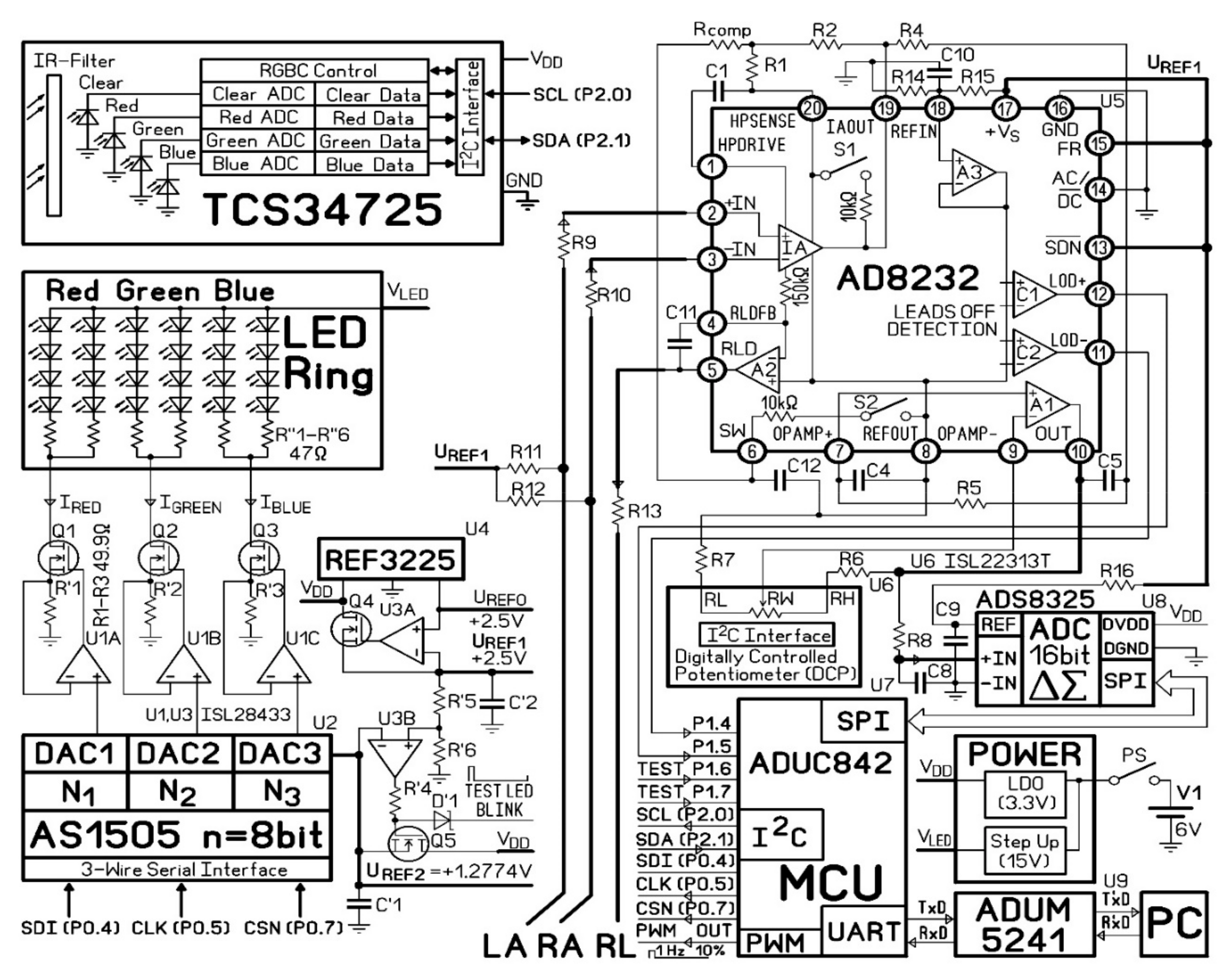
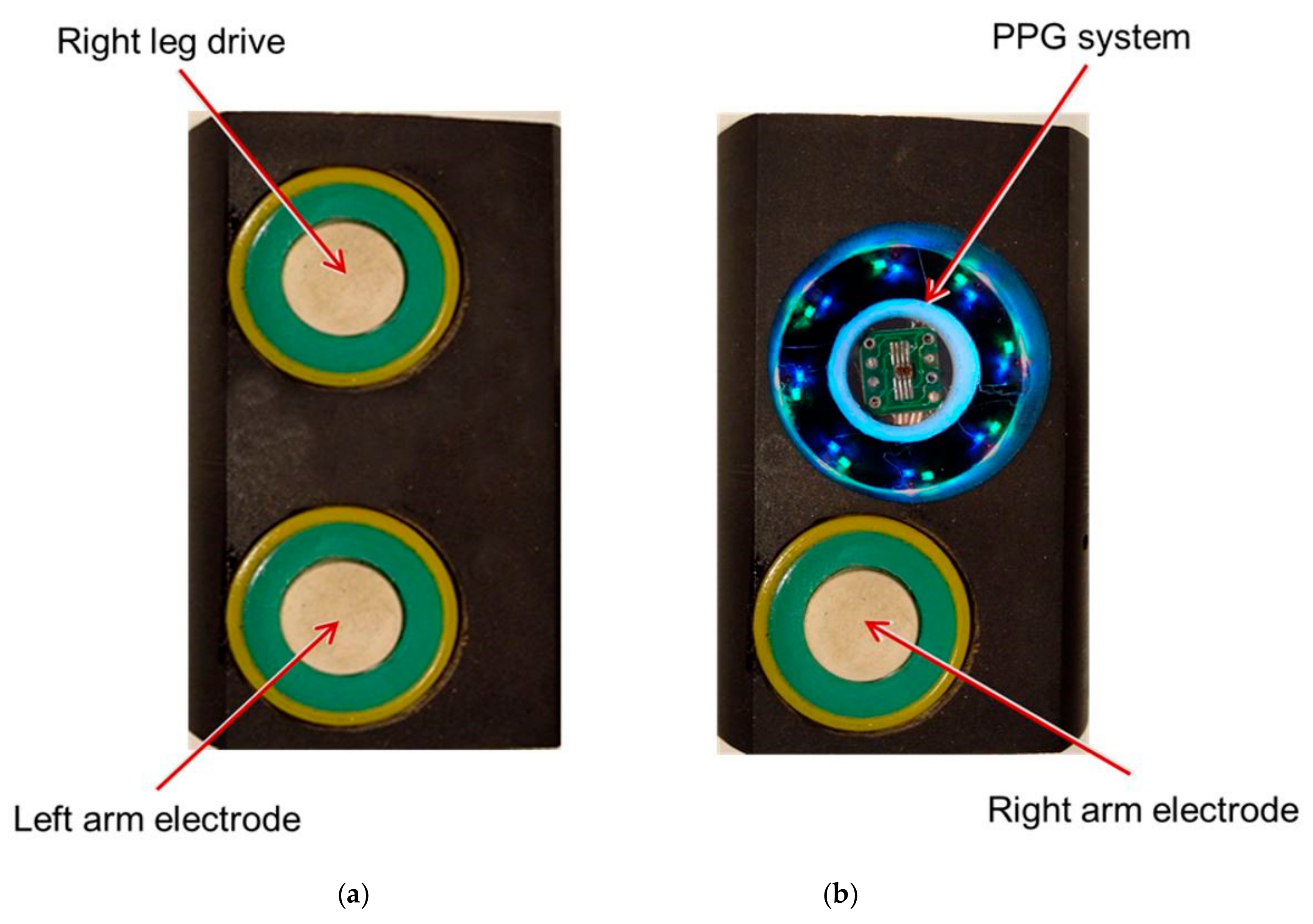
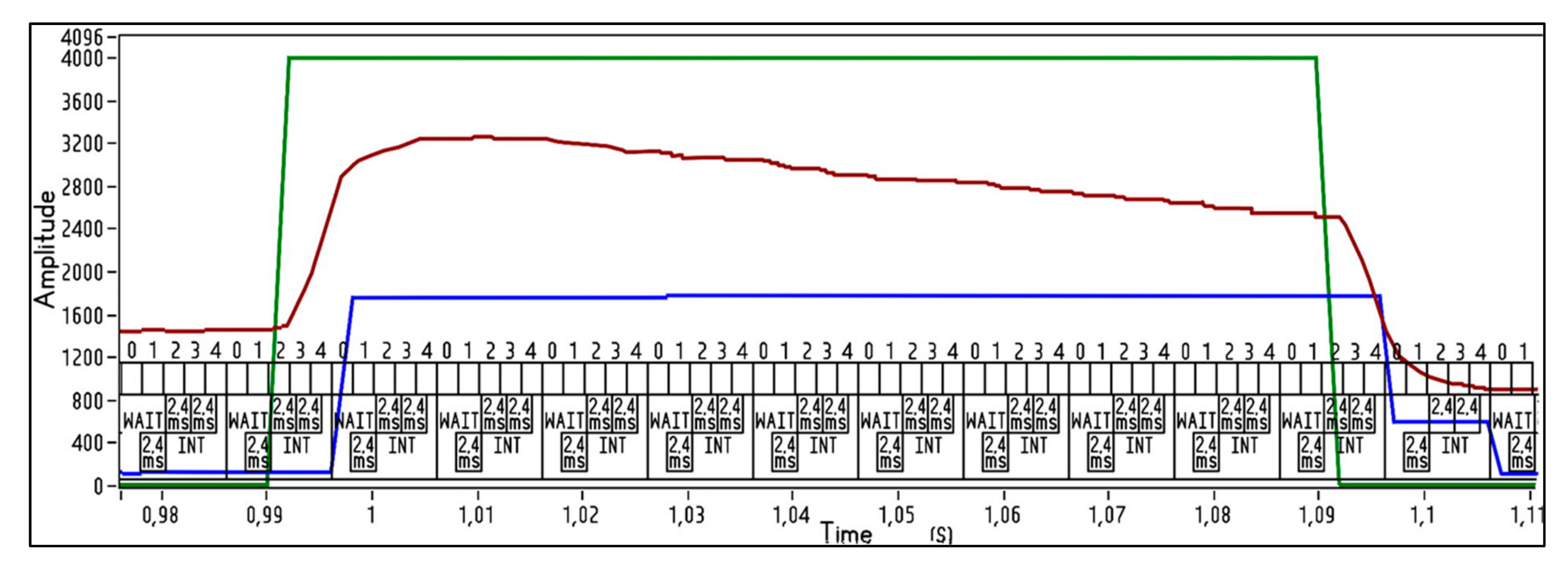
2.1. The PPG Measurement System
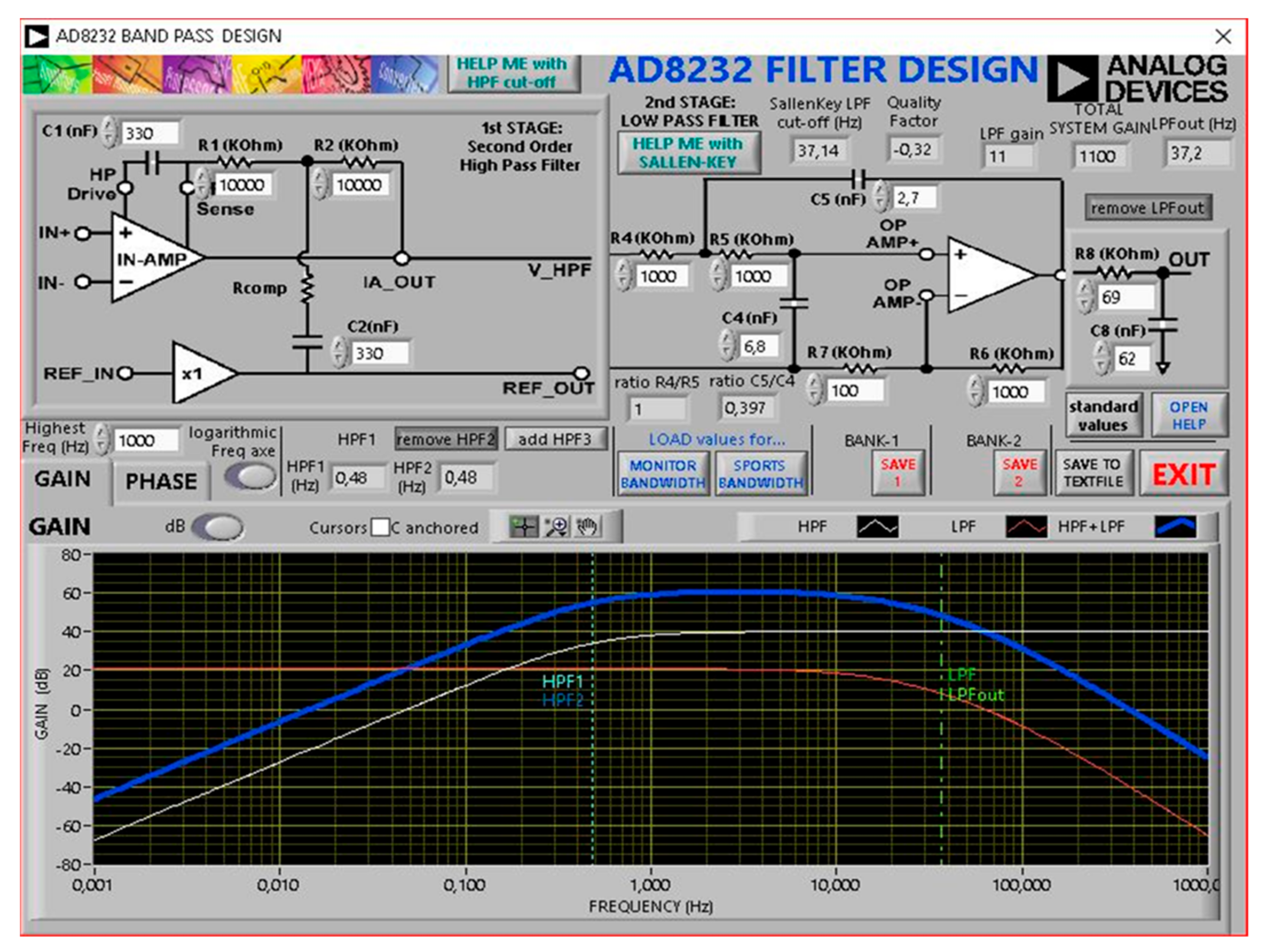
2.2. Electrocardiography (ECG) Measurement System
2.3. Participants and Experimental Procedure
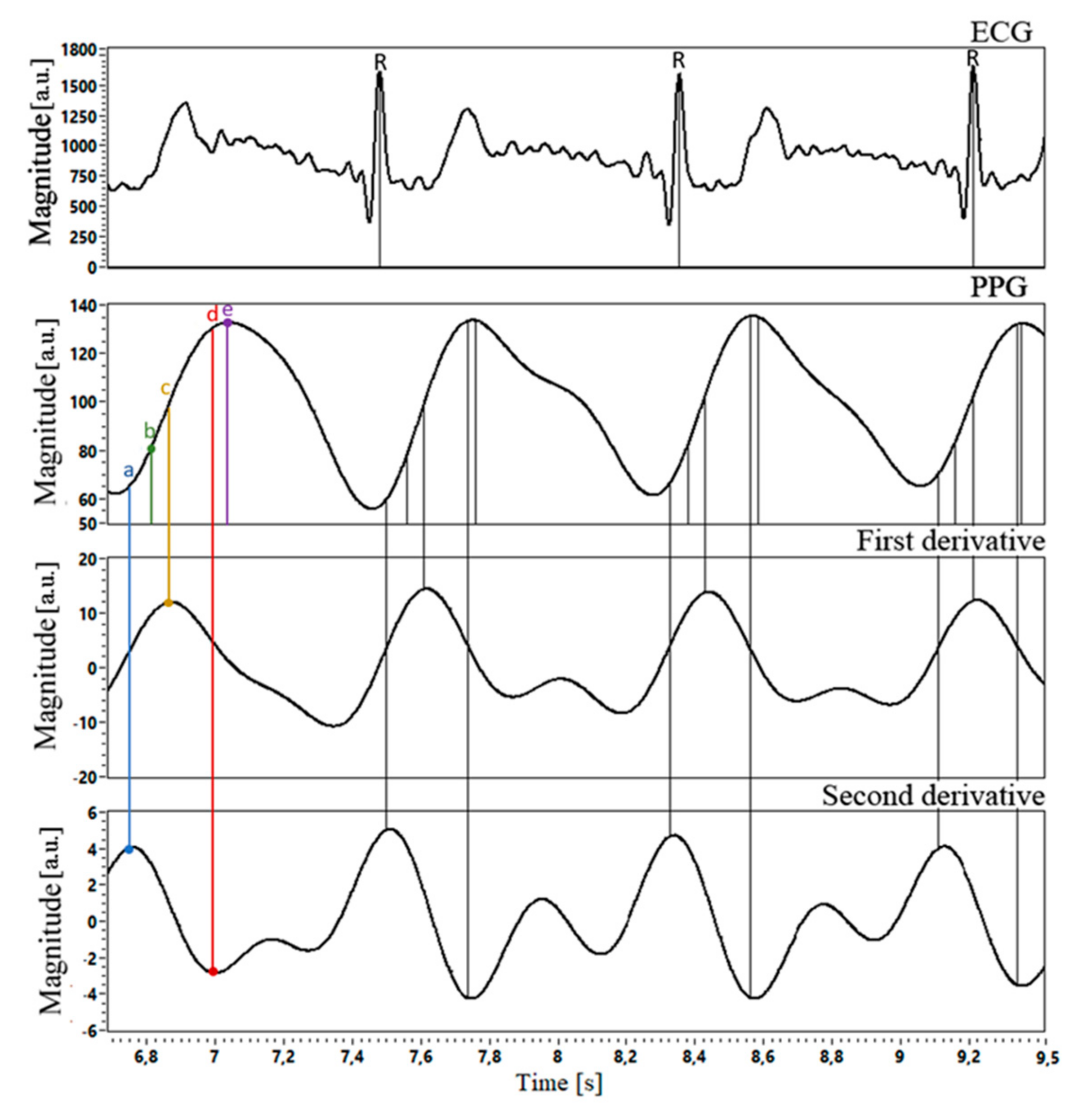
2.4. Signals Acquisition and Processing
2.5. Signals Alignment
2.6. Statistical Analyses
3. Results
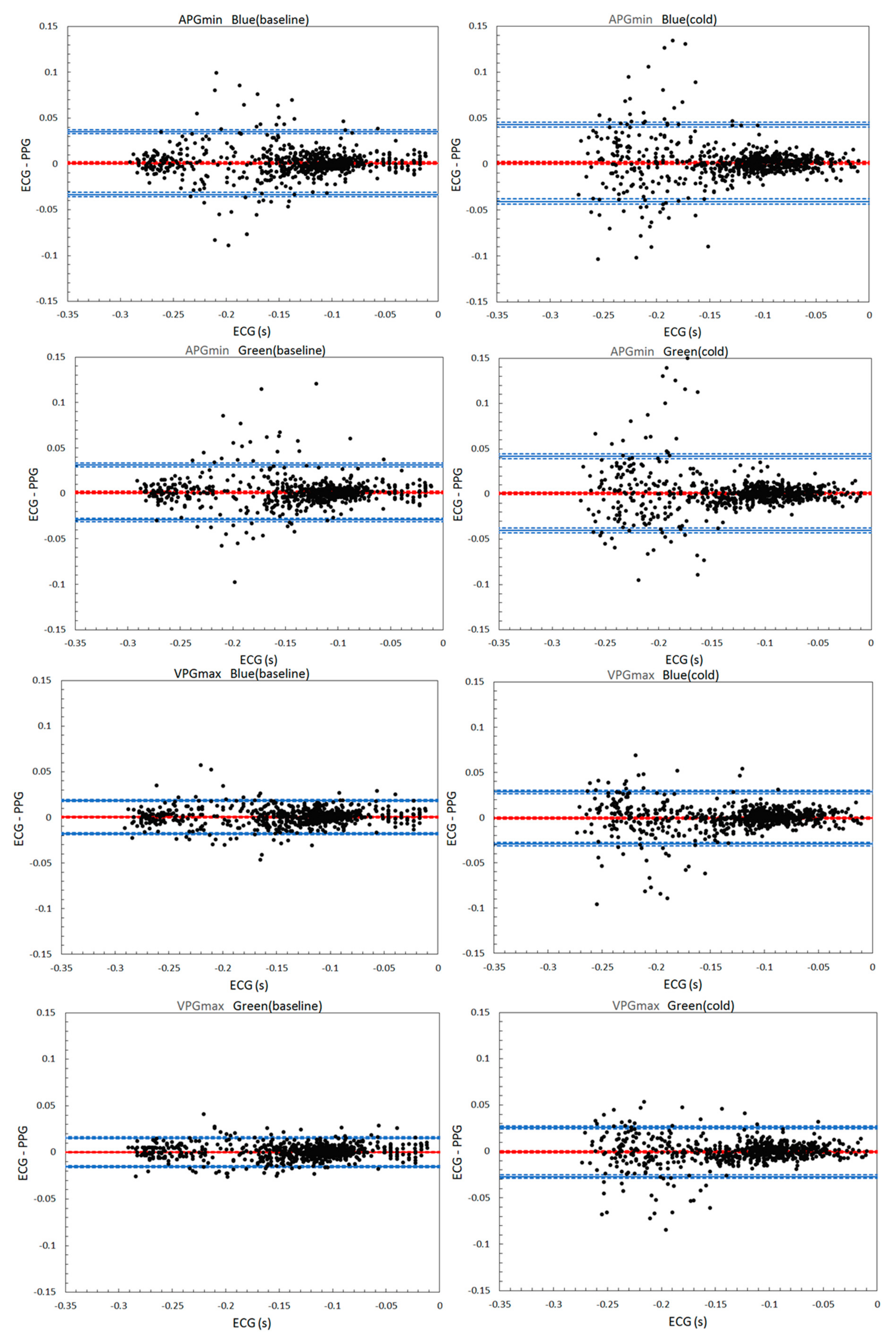
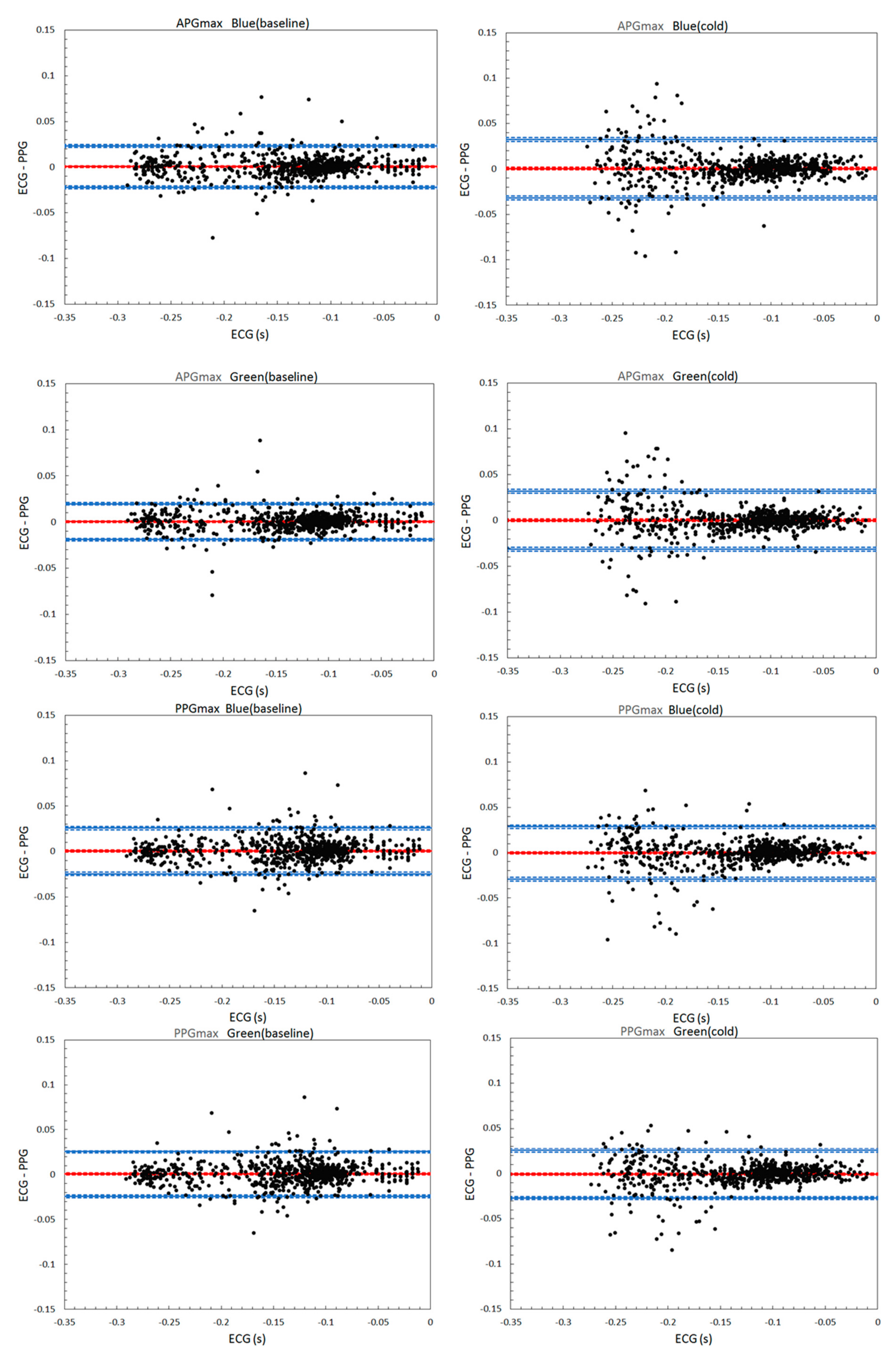
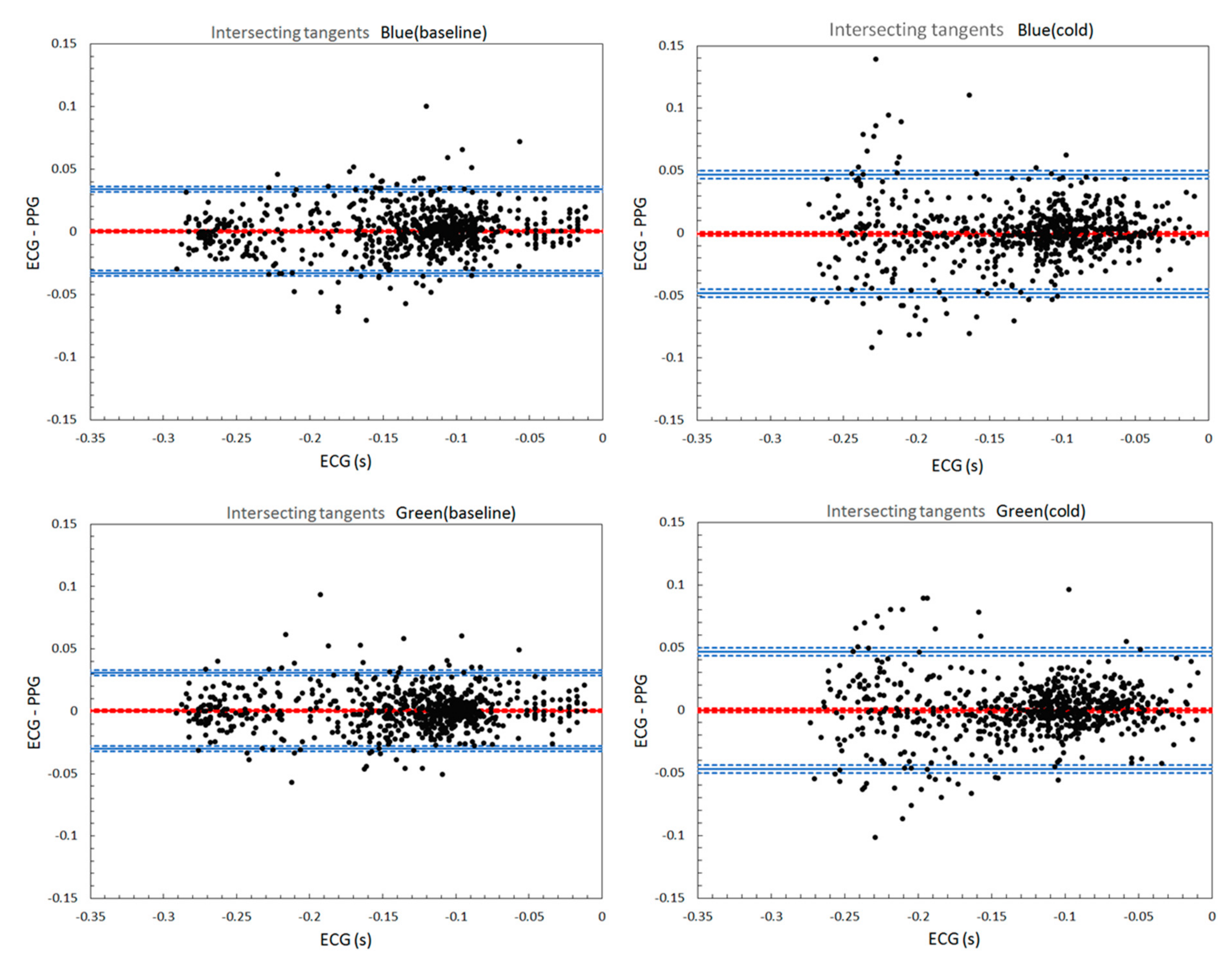
3.1. Bland-Altman Analysis
3.2. Passing-Bablok Regression Analysis
4. Discussion
- The influence of the pulse transit time, investigated in Kuntamalla et al.’s study [17];
- The changes in pulse wave morphology due to the skin temperature fluctuations. On the Bland-Altman plots for both wavelengths, PPG estimates’ precision tended to degrade upon a significant drop in the skin temperature. In the cold condition, the precision reduced drastically for short HBI durations (corresponding to faster heart rates) while being less affected in longer HBIs. This finding is in line with the work of Zhang et al. [18], where the HR measurements during exercises had larger errors compared to the HR estimates during sleep and rest. Studies on PPG validation in different HBI ranges are needed to ensure proper application of the method and correct data interpretation. Probably, some cardiovascular parameters can be accurately estimated only within a certain range of HBI durations.
- Characteristic point used for HBI estimation. Our results indicate that in both wavelengths, VPGmax algorithm yielded the best accuracy with the smallest bias, the CI of bias and LOA in the Bland-Altman test. Our findings are congruent with the earlier studies [7,9,10]. In contrast, the IT algorithm demonstrated a low level of agreement with the ECG compared to PPGmax, APGmax, and VPGmax. That is different from the previous studies [8,19]. APGmin, similarly to IT, underperformed in our study. The discrepancy in results probably originates from several factors: different skin patches being probed, properties of the light source and detector, sampling rate, signal processing methods, and so on. There are still no internationally recognized PPG research methodology standards, making it difficult to compare different approaches. For instance, in a large body of literature on photoplethysmography, the fourth-order Butterworth filter has been the most widely used filter type. Different from these studies, in our work, Chebyshev II filter was employed. Liang et al.’s work [20] showed that Chebyshev II improved the PPG signal quality more effectively than other filters (Wavelet, Butterworth, Chebyshev I, Elliptic, Median filter, Moving-average filter, FIR-hamming window, and FIR-least squares), while preserving valuable components of the signal. Maintaining the morphology of the PPG waveform is essential for characteristic point detection and for extracting additional features from the signal. The inconsistency in literature on the PPG characteristic points selection suggests that the following approaches can improve the PPG diagnostic value: (1) tailoring a characteristic point selection to signal acquisition parameters and conditions and the area of application. This approach is relevant for devices with limited computational resources; (2) using machine learning techniques.
5. Conclusions
6. Limitations and Future Work
- The experiments were conducted only in a relatively small sample of healthy volunteers with no history of cardiovascular diseases. It is established that the PPG waveform can be influenced by many factors, such as properties of blood vessels and physical condition of an individual (sleeping hours, physical activities) [23]. For a comprehensive wavelength comparison, it is needed to recruit a more heterogeneous group of subjects.
- The study results were based on the perfect characteristic point detection. Before HBI measurements, every characteristic point misdetected by the algorithm was manually corrected upon visual inspection. The performance of the detection algorithms in real time was not assessed.
- B and G PPG were compared only in terms of HBIs estimation accuracy. HRV, pulse arrival time and other metrics were not calculated. Several cardiovascular parameters extracted from G an B PPG signals should be validated concerning the reference measurements in different HBIs ranges for a comprehensive evaluation.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A



References
- Gajinov, Z.; Mati, M.; Prcic, S.; Duran, V. Optical properties of the human skin. Serb. J. Dermatol. Venereol. 2010, 2, 131–136. [Google Scholar] [CrossRef]
- Lee, J.; Matsumura, K.; Yamakoshi, K.; Rolfe, P.; Tanaka, S.; Yamakoshi, T. Comparison between red, green and blue light reflection photoplethysmography for heart rate monitoring during motion. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 1724–1727. [Google Scholar] [CrossRef] [Green Version]
- Matsumura, K.; Rolfe, P.; Lee, J.; Yamakoshi, T. iPhone 4s photoplethysmography: Which light color yields the most accurate heart rate and normalized pulse volume using the iPhysioMeter application in the presence of motion artifact. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Maeda, Y.; Sekine, M.; Tamura, T.; Moriya, A.; Suzuki, T.; Kameyama, K. Comparison of reflected green light and infrared photoplethysmography. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 2270–2272. [Google Scholar] [CrossRef]
- Shchelkanova, E.; Shchelkanov, A.; Shchapova, L.; Shibata, T. An Exploration of Blue PPG Signal Using a Novel Color Sensor-based PPG System. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 4414–4420. [Google Scholar] [CrossRef]
- Peralta, E.; Lazaro, J.; Bailon, R.; Marozas, V.; Gil, E. Optimal fiducial points for pulse rate variability analysis from forehead and finger photoplethysmographic signals. Physiol. Meas. 2019, 40, 025007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinheiro, N.; Couceiro, R.; Henriques, J.; Muehlsteff, J.; Quintal, I.; Goncalves, L.; Carvalho, P. Can PPG be used for HRV analysis? Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2016, 2016, 2945–2949. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.C.; Zhou, X.L.; Lin, W.H.; Zhang, Y.T. Extraction of heart rate variability from smartphone photoplethysmograms. Comput. Math. Methods Med. 2015, 2015, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Guede-Fernández, F.; Ferrer-Mileo, V.; Mateu-Mateus, M.; Ramos-Castro, J.; García-González, M.Á.; FernándezChimeno, M. A photoplethysmography smartphone-based method for heart rate variability assessment: Device model and breathing influences. Biomed. Signal Process. Control 2019, 57, 1–9. [Google Scholar] [CrossRef]
- Ferrer-Mileo, V.; Guede-Fernandez, F.; Fernández-Chimeno, M.; Ramos-Castro, J.; García-González, M.A. Accuracy of heart rate variability estimation by photoplethysmography using a smartphone: Processing optimization and fiducial point selection. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 5700–5703. [Google Scholar] [CrossRef] [Green Version]
- McDonagh, A.F.; Lightner, D.A. Phototherapy and the photobiology of bilirubin. Semin. Liver Dis. 1988, 8, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Ash, C.; Harrison, A.; Drew, S.; Whittall, R. A randomized controlled study for the treatment of acne vulgaris using high-intensity 414 nm solid state diode arrays. J. Cosmet. Laser Ther. 2015, 17, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Piacquadio, D.J.; Chen, D.M.; Farber, H.F.; Fowler, J.F., Jr.; Glazer, S.D.; Goodman, J.J.; Hruza, L.L.; Jeffes, E.W.B.; Ling, M.R.; Phillips, T.J.; et al. Photodynamic therapy with aminolevulinic acid topical solution and visible blue light in the treatment of multiple actinic keratoses of the face and scalp: Investigator-blinded phase 3 multicenter trials. Arch. Dermatol. 2004, 140, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Avdeeva, D.K.; Ivanov, M.L.; Yuzhakov, M.M.; Turushev, N.V.; Kodermiatov, R.A.; Maksimov, I.V.; Zimin, I.A. Novel high-resolution nanosensor-based measuring equipment for ECG recording. Meas. J. Int. Meas. Confed. 2019, 146, 215–229. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Passing, H.; Bablok, W. A new biometrical procedure for testing the equality of measurements from two different analytical methods. Application of linear regression procedures for method comparison studies in Clinical Chemistry, Part. I. J. Clin. Chem Clin. Biochem 1983, 21, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Kuntamalla, S.; Lekkala, R.G.R. Quantification of error between the heartbeat intervals measured from photoplethysmogram and electrocardiogram by synchronization. J. Med. Eng. Technol. 2018, 42, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Weaver, R.G.; Armstrong, B.; Burkart, S.; Zhang, S.; Beets, M.W. Validity of Wrist-Worn photoplethysmography devices to measure heart rate: A systematic review and meta-analysis. J. Sports Sci. 2020, 38, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.P.; Kyriacou, P.A. Comparison of methods for determining pulse arrival time from Doppler and photoplethysmography signals. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Chicago, IL, USA, 26–30 August 2014; pp. 3809–3812. [Google Scholar] [CrossRef]
- Liang, Y.; Elgendi, M.; Chen, Z.; Ward, R. An optimal filter for short photoplethysmogram signals. Sci. Data 2018, 5, 180076. [Google Scholar] [CrossRef] [PubMed]
- Zein, R.; Selting, W.; Hamblin, M. Review of light parameters and photobiomodulation efficacy: Dive into complexity. J. Biomed. Opt. 2018, 23, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Wang, Y.; Wang, L. The effect of light conditions on photoplethysmographic image acquisition using a commercial camera. J. Transl. Eng. Health Med. 2014, 2, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Akay, M. Wiley Encyclopedia of Biomedical Engineering; Wiley-Interscience: Hoboken, NJ, USA, 2006; p. 4152. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| POINT | BIAS | BIAS CI Range | 1/2 LOA | BAR | ALoA | BIAS %ECG |
|---|---|---|---|---|---|---|
| IT BB | 0.0005 | 0.0025 | 0.033 | 0.045 | 0.148 | −0.4 |
| IT BC | −0.0006 | 0.0036 | 0.047 | 0.063 | 0.151 | 0.5 |
| IT GB | 0.0005 | 0.0023 | 0.030 | 0.041 | 0.148 | −0.4 |
| IT GC | −0.0003 | 0.0036 | 0.047 | 0.062 | 0.151 | 0.2 |
| APGmax BB | 0.0005 | 0.0017 | 0.023 | 0.031 | 0.148 | −0.4 |
| APGmax BC | 0.0004 | 0.0025 | 0.032 | 0.043 | 0.151 | −0.3 |
| APGmax GB | 0.0004 | 0.0015 | 0.019 | 0.026 | 0.148 | −0.3 |
| APGmax GC | 0.0003 | 0.0024 | 0.032 | 0.042 | 0.151 | −0.2 |
| VPGmax BB | 0.0003 | 0.0014 | 0.018 | 0.025 | 0.148 | −0.2 |
| VPGmax BC | −0.0004 | 0.0022 | 0.029 | 0.038 | 0.151 | 0.3 |
| VPGmax GB | 0.0003 | 0.0012 | 0.015 | 0.021 | 0.148 | −0.2 |
| VPGmax GC | −0.0006 | 0.0020 | 0.026 | 0.035 | 0.151 | 0.5 |
| PPGmax BB | 0.0006 | 0.0019 | 0.025 | 0.034 | 0.148 | −0.4 |
| PPGmax BC | −0.0004 | 0.0022 | 0.029 | 0.038 | 0.151 | 0.3 |
| PPGmax GB | 0.0006 | 0.0019 | 0.025 | 0.034 | 0.148 | −0.4 |
| PPGmax GC | −0.0006 | 0.0020 | 0.026 | 0.035 | 0.151 | 0.5 |
| APGmin BB | 0.0009 | 0.0026 | 0.034 | 0.046 | 0.147 | −0.7 |
| APGmin BC | 0.0012 | 0.0032 | 0.042 | 0.055 | 0.151 | −0.9 |
| APGmin GB | 0.0011 | 0.0023 | 0.030 | 0.041 | 0.147 | −0.8 |
| APGmin GC * | 0.0008 | 0.0031 | 0.041 | 0.055 | 0.151 | −0.6 |
| Characteristic Point | Intercept (95% CI) | Slope (95% CI) | Residual SD |
|---|---|---|---|
| BASELINE CONDITION | |||
| IT Blue | −0.011 (−0.025–0.000) | 1.014 (1.000–1.033) | 0.020 |
| IT Green | −0.014 (−0.027–0.000) | 1.019 (1.000–1.038) | 0.018 |
| APGmax Blue | 0 (0.000–0.009) | 1 (0.988–1.000) | 0.013 |
| APGmax Green | 0 (0.000–0.007) | 1 (0.989–1.000) | 0.011 |
| VPGmax Blue | 0 (0.000–0.007) | 1 (0.990–1.000) | 0.011 |
| VPGmax Green | 0 (0.000–0.006) | 1 (0.992–1.000) | 0.009 |
| PPGmax Blue | −0.002 (−0.008–0.005) | 1 (0.992–1.011) | 0.015 |
| PPGmax Green | 0 (−0.011–0.000) | 1 (1.000–1.014) | 0.014 |
| APGmin Blue | 0 (−0.012–0.002) | 1 (0.998–1.016) | 0.019 |
| APGmin Green | 0 (−0.012–0.000) | 1 (1.000–1.015) | 0.017 |
| COLD CONDITION | |||
| IT Blue | −0.013 (−0.032–0.002) | 1.019 (1.000–1.042) | 0.027 |
| IT Green | −0.010 (−0.029–0.006) | 1.014 (0.993–1.039) | 0.026 |
| APGmax Blue | 0 (−0.014–0.008) | 1 (0.989–1.018) | 0.017 |
| APGmax Green | 0 (−0.014–0.004) | 1 (0.994–1.017) | 0.017 |
| VPGmax Blue | 0 (−0.017–0.007) | 1 (0.991–1.015) | 0.016 |
| VPGmax Green | 0 (−0.000–0.000) | 1 (0.983–1.000) | 0.015 |
| PPGmax Blue | 0 (−0.000–0.013) | 1 (0.991–1.015) | 0.016 |
| PPGmax Green | 0 (−0.025–0.000) | 1 (0.983–1.000) | 0.015 |
| APGmin Blue | −0.013 (−0.027–0.002) | 1.014 (1.000–1.033) | 0.022 |
| APGmin Green | 0 (−0.015–0.009) | 1 (0.988–1.018) | 0.021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shchelkanova, E.; Shchapova, L.; Shchelkanov, A.; Shibata, T. Blue as an Underrated Alternative to Green: Photoplethysmographic Heartbeat Intervals Estimation under Two Temperature Conditions. Sensors 2021, 21, 4241. https://doi.org/10.3390/s21124241
Shchelkanova E, Shchapova L, Shchelkanov A, Shibata T. Blue as an Underrated Alternative to Green: Photoplethysmographic Heartbeat Intervals Estimation under Two Temperature Conditions. Sensors. 2021; 21(12):4241. https://doi.org/10.3390/s21124241
Chicago/Turabian StyleShchelkanova, Evgeniia, Liia Shchapova, Alexander Shchelkanov, and Tomohiro Shibata. 2021. "Blue as an Underrated Alternative to Green: Photoplethysmographic Heartbeat Intervals Estimation under Two Temperature Conditions" Sensors 21, no. 12: 4241. https://doi.org/10.3390/s21124241