Characterizing Behavioral Activity Rhythms in Older Adults Using Actigraphy

 , , ,
, , ,
Abstract
:1. Introduction
2. Approaches for Estimating Circadian Rhythms from Actigraphy Data
2.1. Parametric Approaches
2.2. Non-Parametric Approches
3. Characterizing Actigraphy-Derived Behavioral Activity Rhythms in Older Adults
3.1. Behavioral Activity Rhythms, Age, and Cognitive Status
3.2. Behavioral Activity Rhythms, Mortality, and Quality of Life
3.3. Behavioral Activity Rhythms in the Study of Mood in Older adults
3.4. Methodological Concerns
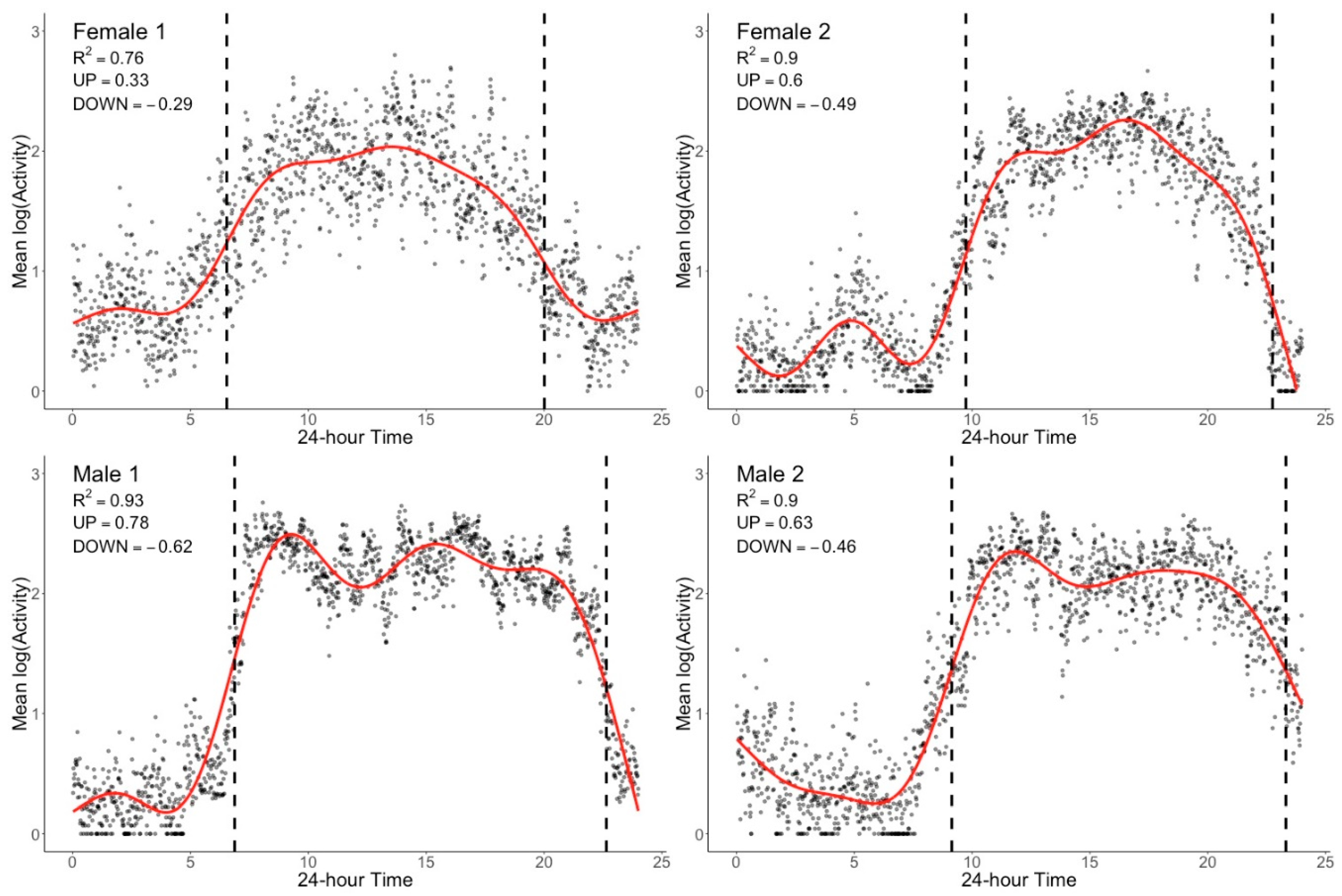
4. Describing Actigraphy-Derived BAR in Older Adults—A Graphical Approach
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Scullin, M.K.; Bliwise, D.L. Sleep, cognition, and normal aging: Integrating a half century of multidisciplinary research. Perspect. Psychol. Sci. 2015, 10, 97–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foley, D.; Ancoli-Israel, S.; Britz, P.; Walsh, J. Sleep disturbances and chronic disease in older adults: Results of the 2003 national sleep foundation sleep in America Survey. J. Psychosom. Res. 2004, 56, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, S.; Brenes, G.A.; Levine, D.; Sevick, M.A.; Shumaker, S.A.; Craven, T. Factors related to sleep disturbance in older adults experiencing knee pain or knee pain with radiographic evidence of knee osteoarthritis. J. Am. Geriatr. Soc. 2000, 48, 1241–1251. [Google Scholar] [CrossRef] [PubMed]
- Musiek, E.S.; Holtzman, D.M. Mechanisms linking circadian clocks, sleep, and neurodegeneration. Science 2016, 354, 1004–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundeen, J.; McCall, W.V.; Krystal, A.; Looney, S. Validating functional data analysis measures from 24-h actigraphy data. Biol. Rhythm. Res. 2018, 49, 797–810. [Google Scholar] [CrossRef]
- Kelly, J.M.; Strecker, R.E.; Bianchi, M.T. Recent developments in home sleep-monitoring devices. ISRN Neurol. 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Casaccia, S.; Braccili, E.; Scalise, L.; Revel, G.M. Experimental Assessment of Sleep-Related Parameters by Passive Infrared Sensors: Measurement Setup, Feature Extraction, and Uncertainty Analysis. Sensors 2019, 19, 3773. [Google Scholar] [CrossRef] [Green Version]
- Kripke, D.F.; Mullaney, D.; Messin, S.; Wyborney, V.G. Wrist actigraphic measures of sleep and rhythms. Electroencephalogr. Clin. Neurophysiol. 1978, 44, 674–676. [Google Scholar] [CrossRef]
- Mullaney, D.; Kripke, D.; Messin, S. Wrist-actigraphic estimation of sleep time. Sleep 1980, 3, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Ancoli-Israel, S.; Cole, R.; Alessi, C.; Chambers, M.; Moorcroft, W.; Pollak, C.P. The role of actigraphy in the study of sleep and circadian rhythms. Sleep 2003, 26, 342–392. [Google Scholar] [CrossRef] [Green Version]
- Ancoli-Israel, S.; Martin, J.L.; Blackwell, T.; Buenaver, L.; Liu, L.; Meltzer, L.J.; Sadeh, A.; Spira, A.P.; Taylor, D.J. The SBSM guide to actigraphy monitoring: Clinical and research applications. Behav. Sleep Med. 2015, 13, S4–S38. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.M.; Wielgus, K.K.; Young-McCaughan, S.; Fischer, P.; Farr, L.; Lee, K.A. Methodological challenges when using actigraphy in research. J. Pain Symptom Manag. 2008, 36, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Morgenthaler, T.; Alessi, C.; Friedman, L.; Owens, J.; Kapur, V.; Boehlecke, B.; Brown, T.; Chesson, A., Jr.; Coleman, J.; Lee-Chiong, T. Practice parameters for the use of actigraphy in the assessment of sleep and sleep disorders: An update for 2007. Sleep 2007, 30, 519–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadeh, A.; Alster, J.; Urbach, D.; Lavie, P. Actigraphically based automatic bedtime sleep-wake scoring: Validity and clinical applications. J. Ambul. Monit. 1989, 2, 209–216. [Google Scholar]
- Martin, J.L.; Hakim, A.D. Wrist actigraphy. Chest 2011, 139, 1514–1527. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, L.J.; Montgomery-Downs, H.E.; Insana, S.P.; Walsh, C.M. Use of actigraphy for assessment in pediatric sleep research. Sleep Med. Rev. 2012, 16, 463–475. [Google Scholar] [CrossRef] [Green Version]
- Sadeh, A.; Acebo, C. The role of actigraphy in sleep medicine. Sleep Med. Rev. 2002, 6, 113–124. [Google Scholar] [CrossRef] [Green Version]
- Sadeh, A. The role and validity of actigraphy in sleep medicine: An update. Sleep Med. Rev. 2011, 15, 259–267. [Google Scholar] [CrossRef]
- Littner, M.; Kushida, C.A.; Anderson, W.M.; Bailey, D.; Berry, R.B.; Davila, D.G.; Hirshkowitz, M.; Kapen, S.; Kramer, M.; Loube, D. Practice parameters for the role of actigraphy in the study of sleep and circadian rhythms: An update for 2002. Sleep 2003, 26, 337–341. [Google Scholar] [CrossRef]
- Plasqui, G.; Bonomi, A.; Westerterp, K. Daily physical activity assessment with accelerometers: New insights and validation studies. Obes. Rev. 2013, 14, 451–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, M.; Kiel, K.; Alexander, D.; Powell, G. Computer-Compatible activity measurement of children: Wrist actigraph standardization. Comput. Nurs. 1984, 2, 125–129. [Google Scholar] [PubMed]
- Brown, A.; Smolensky, M.; D′Alonzo, G.; Redmond, D.; Conrad, E.; Hsi, B. Circadian rhythm in human activity objectively quantified by actigraphy. Prog. Clin. Biol. Res. 1990, 341, 77. [Google Scholar]
- Brown, A.C.; Smolensky, M.H.; D’Alonzo, G.E.; Redman, D.P. Actigraphy: A means of assessing circadian patterns in human activity. Chronobiol. Int. 1990, 7, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Van Someren, E.; Lazeron, R.; Vonk, B. Wrist acceleration and consequences for actigraphic rest-activity registration in young and elderly subjects. Sleep-Wake Res. Neth. 1995, 6123–6125. [Google Scholar]
- Redmond, D.P.; Hegge, F.W. Observations on the design and specification of a wrist-worn human activity monitoring system. Behav. Res. Methods Instrum. Comput. 1985, 17, 659–669. [Google Scholar] [CrossRef]
- Neikrug, A.B.; Donaldson, G.; Iacob, E.; Williams, S.L.; Hamilton, C.A.; Okifuji, A. Activity rhythms and clinical correlates in fibromyalgia. Pain 2017, 158, 1417–1429. [Google Scholar] [CrossRef]
- Luik, A.I.; Zuurbier, L.A.; Direk, N.; Hofman, A.; Van Someren, E.J.; Tiemeier, H. 24-hour activity rhythm and sleep disturbances in depression and anxiety: A population-based study of middle-aged and older persons. Depress. Anxiety 2015, 32, 684–692. [Google Scholar] [CrossRef]
- Smagula, S.F.; Krafty, R.T.; Thayer, J.F.; Buysse, D.J.; Hall, M.H. Rest-activity rhythm profiles associated with manic-hypomanic and depressive symptoms. J. Psychiatr. Res. 2018, 102, 238–244. [Google Scholar] [CrossRef]
- Neikrug, A.B.; Rissling, M.; Trofimenko, V.; Liu, L.; Natarajan, L.; Lawton, S.; Parker, B.A.; Ancoli-Israel, S. Bright light therapy protects women from circadian rhythm desynchronization during chemotherapy for breast cancer. Behav. Sleep Med. 2012, 10, 202–216. [Google Scholar] [CrossRef]
- Tranah, G.J.; Blackwell, T.; Ancoli-Israel, S.; Paudel, M.L.; Ensrud, K.E.; Cauley, J.A.; Redline, S.; Hillier, T.A.; Cummings, S.R.; Stone, K.L. Circadian activity rhythms and mortality: The study of osteoporotic fractures. J. Am. Geriatr. Soc. 2010, 58, 282–291. [Google Scholar] [CrossRef]
- Smagula, S.F.; Ancoli-Israel, S.; Blackwell, T.; Boudreau, R.; Stefanick, M.L.; Paudel, M.L.; Stone, K.L.; Cauley, J.A. Osteoporotic Fractures in Men (MrOS) Research Group. Circadian rest–activity rhythms predict future increases in depressive symptoms among community-dwelling older men. Am. J. Geriatr. Psychiatry 2015, 23, 495–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCurry, S.M.; Shortreed, S.M.; Von Korff, M.; Balderson, B.H.; Baker, L.D.; Rybarczyk, B.D.; Vitiello, M.V. Who benefits from CBT for insomnia in primary care? Important patient selection and trial design lessons from longitudinal results of the Lifestyles trial. Sleep 2014, 37, 299–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitiello, M.V.; McCurry, S.M.; Shortreed, S.M.; Balderson, B.H.; Baker, L.D.; Keefe, F.J.; Rybarczyk, B.D.; Von Korff, M. Cognitive-behavioral treatment for comorbid insomnia and osteoarthritis pain in primary care: The lifestyles randomized controlled trial. J. Am. Geriatr. Soc. 2013, 61, 947–956. [Google Scholar] [CrossRef] [PubMed]
- Vitiello, M.V.; McCurry, S.M.; Shortreed, S.M.; Baker, L.D.; Rybarczyk, B.D.; Keefe, F.J.; Von Korff, M. Short-term improvement in insomnia symptoms predicts long-term improvements in sleep, pain, and fatigue in older adults with comorbid osteoarthritis and insomnia. PAIN® 2014, 155, 1547–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Korff, M.; Vitiello, M.V.; McCurry, S.M.; Balderson, B.H.; Moore, A.L.; Baker, L.D.; Yarbro, P.; Saunders, K.; Keefe, F.J.; Rybarczyk, B.D. Group interventions for co-morbid insomnia and osteoarthritis pain in primary care: The Lifestyles cluster randomized trial design. Contemp. Clin. Trials 2012, 33, 759–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marler, M.R.; Gehrman, P.; Martin, J.L.; Ancoli-Israel, S. The sigmoidally transformed cosine curve: A mathematical model for circadian rhythms with symmetric non-sinusoidal shapes. Stat. Med. 2006, 25, 3893–3904. [Google Scholar] [CrossRef]
- Witting, W.; Kwa, I.; Eikelenboom, P.; Mirmiran, M.; Swaab, D. Alterations in the circadian rest-activity rhythm in aging and Alzheimer’s disease. Biol. Psychiatry 1990, 27, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Van Someren, E.J.; Swaab, D.F.; Colenda, C.C.; Cohen, W.; McCall, W.V.; Rosenquist, P.B. Bright light therapy: Improved sensitivity to its effects on rest-activity rhythms in Alzheimer patients by application of nonparametric methods. Chronobiol. Int. 1999, 16, 505–518. [Google Scholar] [CrossRef]
- Cornelissen, G. Cosinor-based rhythmometry. Theor. Biol. Med. Model. 2014, 11, 16. [Google Scholar] [CrossRef] [Green Version]
- Neikrug, A.; Jungquist, C.; Donaldson, G.; Okifuji, A.; Perlis, M. Measuring activity by actigraphy—Are we using the right methods? In SLEEP; Oxford Univ Press Inc.: Cary, NC, USA, 2001; p. A145. [Google Scholar]
- Satlin, A.; Volicer, L.; Stopa, E.G.; Harper, D. Circadian locomotor activity and core-body temperature rhythms in Alzheimer’s disease. Neurobiol. Aging 1995, 16, 765–771. [Google Scholar] [CrossRef]
- Gössel-Symank, R.; Grimmer, I.; Korte, J.; Siegmund, R. Actigraphic monitoring of the activity-rest behavior of preterm and full-term infants at 20 months of age. Chronobiol. Int. 2004, 21, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Van Someren, E.; Mirmiran, M.; Swaab, D. Non-pharmacological treatment of sleep and wake disturbances in aging and Alzheimer’s disease: Chronobiological perspectives. Behav. Brain Res. 1993, 57, 235–253. [Google Scholar] [CrossRef] [Green Version]
- van Someren, E.J.; Hagebeuk, E.E.; Lijzenga, C.; Scheltens, P.; de Rooij, S.E.; Jonker, C.; Pot, A.-M.; Mirmiran, M.; Swaab, D.F. Circadian rest—Activity rhythm disturbances in alzheimer’s disease. Biol. Psychiatry 1996, 40, 259–270. [Google Scholar] [CrossRef] [Green Version]
- Van Someren, E.J.; Kessler, A.; Mirmiran, M.; Swaab, D.F. Indirect bright light improves circadian rest-activity rhythm disturbances in demented patients. Biol. Psychiatry 1997, 41, 955–963. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.-L.; Liu, R.-Y.; Wang, Q.-S.; Van Someren, E.J.; Xu, H.; Zhou, J.-N. Age-associated difference in circadian sleep–wake and rest–activity rhythms. Physiol. Behav. 2002, 76, 597–603. [Google Scholar] [CrossRef]
- Jean–Louis, G.; Kripke, D.F.; Ancoli–Israel, S.; Klauber, M.R.; Sepulveda, R.S.; Mowen, M.-A.; Assmus, J.D.; Langer, R.D. Circadian sleep, illumination, and activity patterns in women: Influences of aging and time reference. Physiol. Behav. 2000, 68, 347–352. [Google Scholar] [CrossRef]
- Robillard, R.; Naismith, S.L.; Smith, K.L.; Rogers, N.L.; White, D.; Terpening, Z.; Ip, T.K.; Hermens, D.F.; Whitwell, B.; Scott, E.M. Sleep-Wake cycle in young and older persons with a lifetime history of mood disorders. PLoS ONE 2014, 9, e87763. [Google Scholar] [CrossRef] [Green Version]
- Luik, A.I.; Zuurbier, L.A.; Hofman, A.; Van Someren, E.J.; Tiemeier, H. Stability and fragmentation of the activity rhythm across the sleep-wake cycle: The importance of age, lifestyle, and mental health. Chronobiol. Int. 2013, 30, 1223–1230. [Google Scholar] [CrossRef]
- Satlin, A.; Teicher, M.H.; Lieberman, H.R.; Baldessarini, R.J.; Volicer, L.; Rheaume, Y. Circadian locomotor activity rhythms in Alzheimer’s disease. Neuropsychopharmacology 1991, 5, 115–126. [Google Scholar]
- Ancoli-Israel, S.; Gehrman, P.; Martin, J.L.; Shochat, T.; Marler, M.; Corey-Bloom, J.; Levi, L. Increased light exposure consolidates sleep and strengthens circadian rhythms in severe Alzheimer’s disease patients. Behav. Sleep Med. 2003, 1, 22–36. [Google Scholar] [CrossRef]
- Pollak, C.P.; Stokes, P.E. Circadian rest-activity rhythms in demented and nondemented older community residents and their caregivers. J. Am. Geriatr. Soc. 1997, 45, 446–452. [Google Scholar] [CrossRef]
- Oosterman, J.M.; Van Someren, E.J.; Vogels, R.L.; Van Harten, B.; Scherder, E.J. Fragmentation of the rest-activity rhythm correlates with age-related cognitive deficits. J. Sleep Res. 2009, 18, 129–135. [Google Scholar] [CrossRef]
- Carvalho-Bos, S.S.; Riemersma-van der Lek, R.F.; Waterhouse, J.; Reilly, T.; Van Someren, E.J. Strong association of the rest–activity rhythm with well-being in demented elderly women. Am. J. Geriatr. Psychiatry 2007, 15, 92–100. [Google Scholar] [CrossRef] [Green Version]
- Tranah, G.J.; Blackwell, T.; Stone, K.L.; Ancoli-Israel, S.; Paudel, M.L.; Ensrud, K.E.; Cauley, J.A.; Redline, S.; Hillier, T.A.; Cummings, S.R. Circadian activity rhythms and risk of incident dementia and mild cognitive impairment in older women. Ann. Neurol. 2011, 70, 722–732. [Google Scholar] [CrossRef] [Green Version]
- Gehrman, P.; Marler, M.; Martin, J.L.; Shochat, T.; Corey-Bloom, J.; Ancoli-Israel, S. The relationship between dementia severity and rest/activity circadian rhythms. Neuropsychiatr. Dis. Treat. 2005, 1, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Ancoli-Israel, S.; Martin, J.L.; Kripke, D.F.; Marler, M.; Klauber, M.R. Effect of light treatment on sleep and circadian rhythms in demented nursing home patients. J. Am. Geriatr. Soc. 2002, 50, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, A.; Robertson, I.H.; Coogan, A.N. Association between circadian rhythms, sleep and cognitive impairment in healthy older adults: An actigraphic study. J. Neural Transm. 2012, 119, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Gehrman, P.; Marler, M.; Martin, J.L.; Shochat, T.; Corey-Bloom, J.; Ancoli-Israel, S. The timing of activity rhythms in patients with dementia is related to survival. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, M1050–M1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paudel, M.L.; Taylor, B.C.; Ancoli-Israel, S.; Blackwell, T.; Stone, K.L.; Tranah, G.; Redline, S.; Cummings, S.R.; Ensrud, K.E. Osteoporotic Fractures in Men (MrOS) Study Group. Rest/activity rhythms and mortality rates in older men: MrOS Sleep Study. Chronobiol. Int. 2010, 27, 363–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, J.; Jeste, D.V.; Caliguiri, M.P.; Patterson, T.; Heaton, R.; Ancoli-Israel, S. Actigraphic estimates of circadian rhythms and sleep/wake in older schizophrenia patients. Schizophr. Res. 2001, 47, 77–86. [Google Scholar] [CrossRef] [Green Version]
- Whitehead, D.L.; Davies, A.D.; Playfer, J.R.; Turnbull, C.J. Circadian rest-activity rhythm is altered in Parkinson’s disease patients with hallucinations. Mov. Disord. Off. J. Mov. Disord. Soc. 2008, 23, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Mormont, M.-C.; Waterhouse, J.; Bleuzen, P.; Giacchetti, S.; Jami, A.; Bogdan, A.; Lellouch, J.; Misset, J.-L.; Touitou, Y.; Lévi, F. Marked 24-h rest/activity rhythms are associated with better quality of life, better response, and longer survival in patients with metastatic colorectal cancer and good performance status. Clin. Cancer Res. 2000, 6, 3038–3045. [Google Scholar] [PubMed]
- Mormont, M.-C.; Waterhouse, J. Contribution of the rest–activity circadian rhythm to quality of life in cancer patients. Chronobiol. Int. 2002, 19, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Schulberg, H.C.; Mulsant, B.; Schulz, R.; Rollman, B.L.; Houck, P.R.; Reynolds, C.F., III. Characteristics and course of major depression in older primary care patients. Int. J. Psychiatry Med. 1998, 28, 421–436. [Google Scholar] [CrossRef] [PubMed]
- Germain, A.; Kupfer, D.J. Circadian rhythm disturbances in depression. Hum. Psychopharmacol. Clin. Exp. 2008, 23, 571–585. [Google Scholar] [CrossRef] [Green Version]
- McClung, C.A. Circadian rhythms and mood regulation: Insights from pre-clinical models. Eur. Neuropsychopharmacol. 2011, 21, S683–S693. [Google Scholar] [CrossRef] [Green Version]
- McClung, C.A. How might circadian rhythms control mood? Let me count the ways. Biol. Psychiatry 2013, 74, 242–249. [Google Scholar] [CrossRef]
- Maglione, J.E.; Ancoli-Israel, S.; Peters, K.W.; Paudel, M.L.; Yaffe, K.; Ensrud, K.E.; Tranah, G.J.; Stone, K.L. Depressive symptoms and circadian activity rhythm disturbances in community-dwelling older women. Am. J. Geriatr. Psychiatry 2014, 22, 349–361. [Google Scholar] [CrossRef] [Green Version]
- Smagula, S.F.; Boudreau, R.M.; Stone, K.; Reynolds, C.F., III; Bromberger, J.T.; Ancoli-Israel, S.; Dam, T.-T.; Barrett-Connor, E.; Cauley, J.A. Latent activity rhythm disturbance sub-groups and longitudinal change in depression symptoms among older men. Chronobiol. Int. 2015, 32, 1427–1437. [Google Scholar] [CrossRef] [Green Version]
- Dunn, A.L.; Trivedi, M.H.; O’Neal, H.A. Physical activity dose-response effects on outcomes of depression and anxiety. In Database of Abstracts of Reviews of Effects (DARE): Quality-Assessed Reviews [Internet]; Centre for Reviews and Dissemination (UK): England, UK, 2001. [Google Scholar]
- Zhai, L.; Zhang, Y.; Zhang, D. Sedentary behaviour and the risk of depression: A meta-analysis. Br. J. Sports Med. 2015, 49, 705–709. [Google Scholar] [CrossRef]
- Hasler, B.P.; Buysse, D.J.; Kupfer, D.J.; Germain, A. Phase relationships between core body temperature, melatonin, and sleep are associated with depression severity: Further evidence for circadian misalignment in non-seasonal depression. Psychiatry Res. 2010, 178, 205–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, S.N. Generalized Additive Models: An Introduction with R; Chapman and Hall/CRC: Boca Raton, FL, USA, 2017. [Google Scholar]
- Wood, S.N. Fast stable restricted maximum likelihood and marginal likelihood estimation of semiparametric generalized linear models. J. R. Stat. Soc. Ser. B (Stat. Methodol.) 2011, 73, 3–36. [Google Scholar] [CrossRef] [Green Version]
- Team R C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Ravindra, K.; Rattan, P.; Mor, S.; Aggarwal, A.N. Generalized additive models: Building evidence of air pollution, climate change and human health. Environ. Int. 2019, 132, 104987. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Approach | Variables | Definition | Interpretation |
|---|---|---|---|
| Cosinor model fitting | Midline-estimating statistic of rhythm (mesor) | Mean activity level over the 24 h period | Higher values indicate more average activity across day and night |
| Amplitude | Distance between the mean activity level (mesor) and the peak | Higher values indicate higher overall maximum activity amount and more rhythmic changes | |
| Phi/Acrophase | Time of peak activity in the 24 h period | Later values indicate later peak of activity and may reflects a more delayed phase | |
| R-Squared | Measure of statistical reliability and consistency of the model-fitted rhythm | Higher values indicate greater robustness of the predicted circadian rhythm | |
| Extended Cosinor Model | Midline-estimating statistic of rhythm (mesor) | Half-way between minimum and maximum | Higher levels indicate more estimated average activity |
| Amplitude | Differences between the maximum modelled activity level and the minimum modelled activity level | Higher values indicate higher overall rhythmicity | |
| Phi/Acrophase | Time of peak activity in the 24 h period | Later values indicate later peak of activity and may reflect a more delayed phase | |
| Minimum | The lowest point of the fitted curve | Higher values indicate more night-time activity | |
| Up-mesor | Time from above the mesor to below the mesor | Larger values indicate later time of increasing activity | |
| Down-mesor | Time from above the mesor to below the mesor | Larger values indicate later time of declining activity | |
| Alpha | Width of the rhythm | Larger values (wide troughs and narrow peaks) indicates more night time activity | |
| Beta | Steepness of the rise and fall of the fitted curve | Larger values indicate steeper rise and fall | |
| R-Squared | Model fit measure | Larger values indicate greater robustness of model fit and more rhythmicity | |
| F-statistic | An adjustment to the R-Squared while accounting for the number of observations in the model | Larger values indicate greater robustness of the rhythmic pattern and hence overall more rhythmicity | |
| Nonparametric approach | Inter-daily stability (IS) | Invariability of the 24 h rhythm between different days | Higher values indicate better coupling/synchronization of rest-activity rhythm to external zeitgebers (i.e., 24 h cycle) |
| Intra-daily variability (IV) | Fragmentation of the 24 h rest-activity rhythm | Higher values indicate increased fragmentation, which may reflect the occurrence of daytime naps and/or nocturnal awakenings | |
| Daily activity (M10) | Mean activity level during the most active 10 h period of the day | Higher values indicated more active wake period | |
| Nocturnal activity (L5) | Mean activity level during the least active 5 h period, which usually occurs during sleep and nocturnal arousals | Higher values indicate less restful sleep | |
| Relative amplitude (RA) | Normalized difference between the most active 10 h period (M10) and least active 5 h period (L5) | Higher values indicate a more robust 24 h rhythm, reflecting higher activity during wake and relatively lower activity during the night |
| Measure | Description | Interpretation | Summary Values (Mean, SD, Range) |
|---|---|---|---|
| UP Slope | Slope of fitted curve during period of activity onset where the slope is at its steepest (positive value, Δlog(activity)/hour) | Higher numbers indicate faster (or steeper) increase in activity post awakening. | 0.57, 0.16, 0.16–0.98 |
| UP Slope Time | Time within 24 h period at which activity slope is at its steepest (24 h time) | Later values indicate later time of morning increase of activity and may reflect a more delayed awakening time and more delayed phase | 07:26, 02:05, 02:59–15:11 |
| DOWN Slope | Slope of fitted curve during period of activity ‘wind-down’ where the slope is at its steepest (negative value, Δlog(activity)/hour) | Higher absolute numbers indicate faster (or steeper) decrease in activity towards the next period of rest. | −0.47, 0.13, −0.12–−0.96 |
| DOWN Slope Time | Time within 24 h period at which activity slope is at its steepest (24 h time) | Later values indicate later time of evening decrease of activity and may reflect a more delayed sleep time and more delayed phase | 22:01, 03:52 11:02–05:20 |
| R2 | Percentage of variance accounted for by model | Larger values indicate greater robustness of model fit and more rhythmicity | 0.82, 0.09, 0.28–0.94 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neikrug, A.B.; Chen, I.Y.; Palmer, J.R.; McCurry, S.M.; Von Korff, M.; Perlis, M.; Vitiello, M.V. Characterizing Behavioral Activity Rhythms in Older Adults Using Actigraphy. Sensors 2020, 20, 549. https://doi.org/10.3390/s20020549
Neikrug AB, Chen IY, Palmer JR, McCurry SM, Von Korff M, Perlis M, Vitiello MV. Characterizing Behavioral Activity Rhythms in Older Adults Using Actigraphy. Sensors. 2020; 20(2):549. https://doi.org/10.3390/s20020549
Chicago/Turabian StyleNeikrug, Ariel B., Ivy Y. Chen, Jake R. Palmer, Susan M. McCurry, Michael Von Korff, Michael Perlis, and Michael V. Vitiello. 2020. "Characterizing Behavioral Activity Rhythms in Older Adults Using Actigraphy" Sensors 20, no. 2: 549. https://doi.org/10.3390/s20020549