Real-Time Wireless Platform for In Vivo Monitoring of Bone Regeneration

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
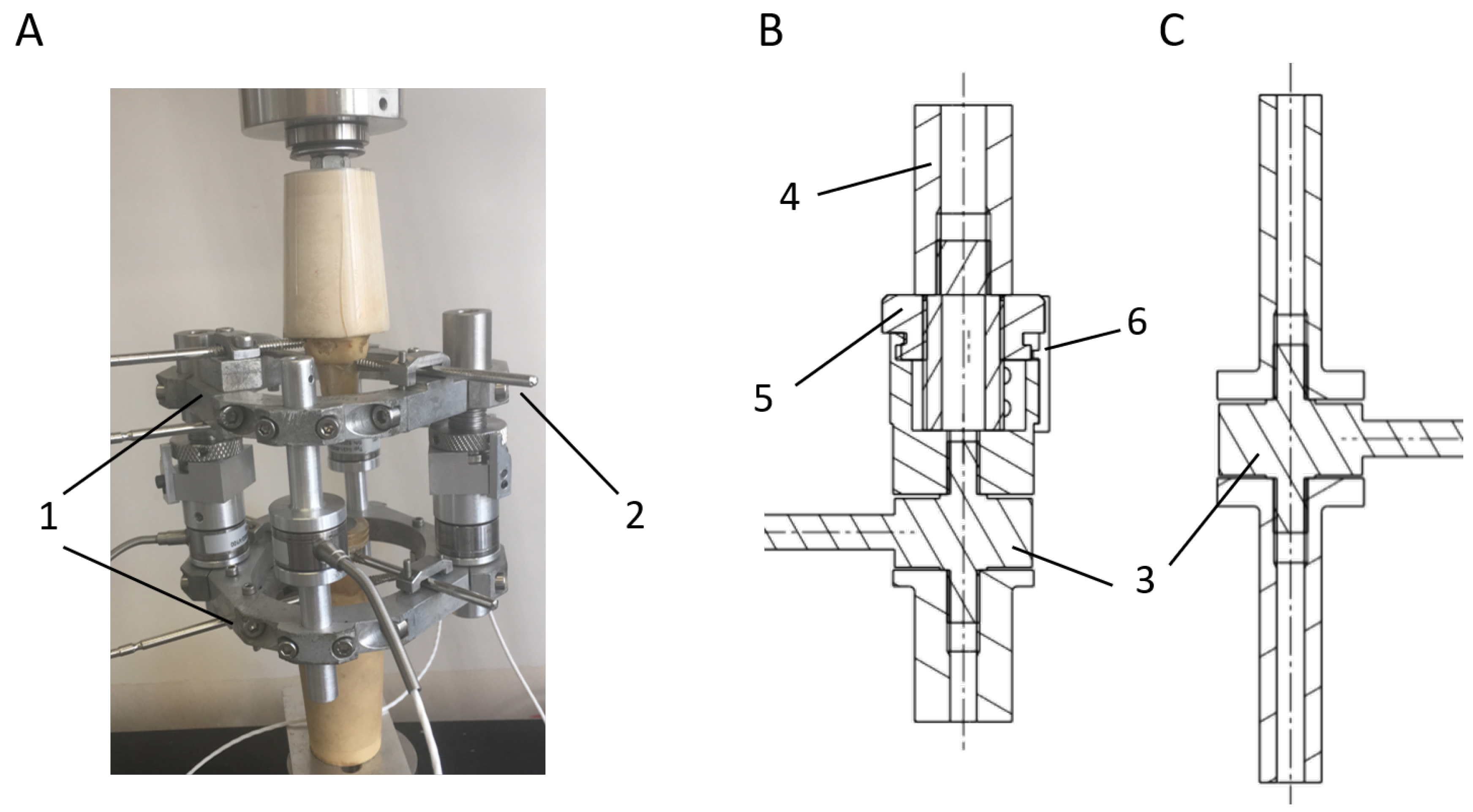
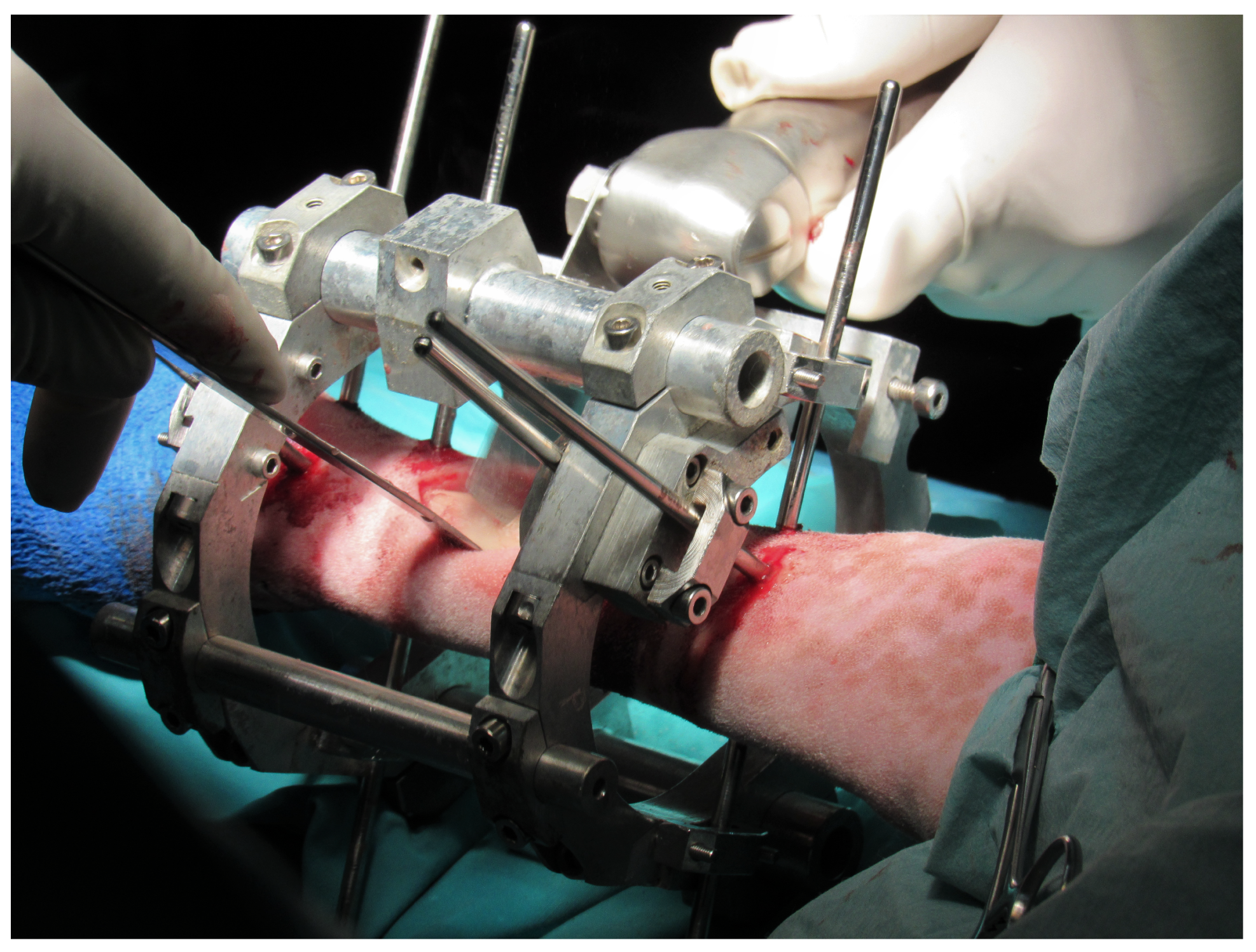
2.1. Distractor, Mechanical Design
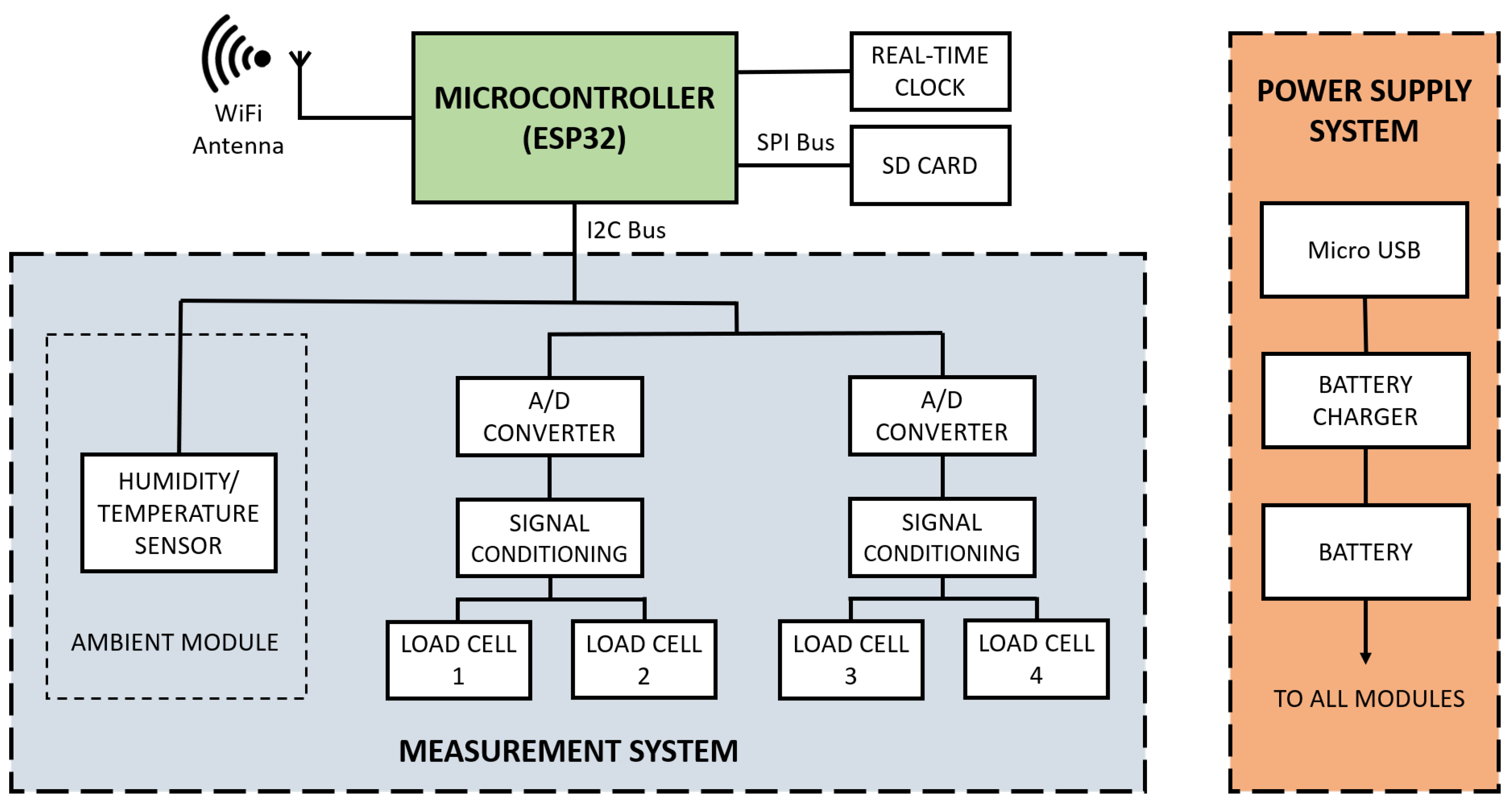
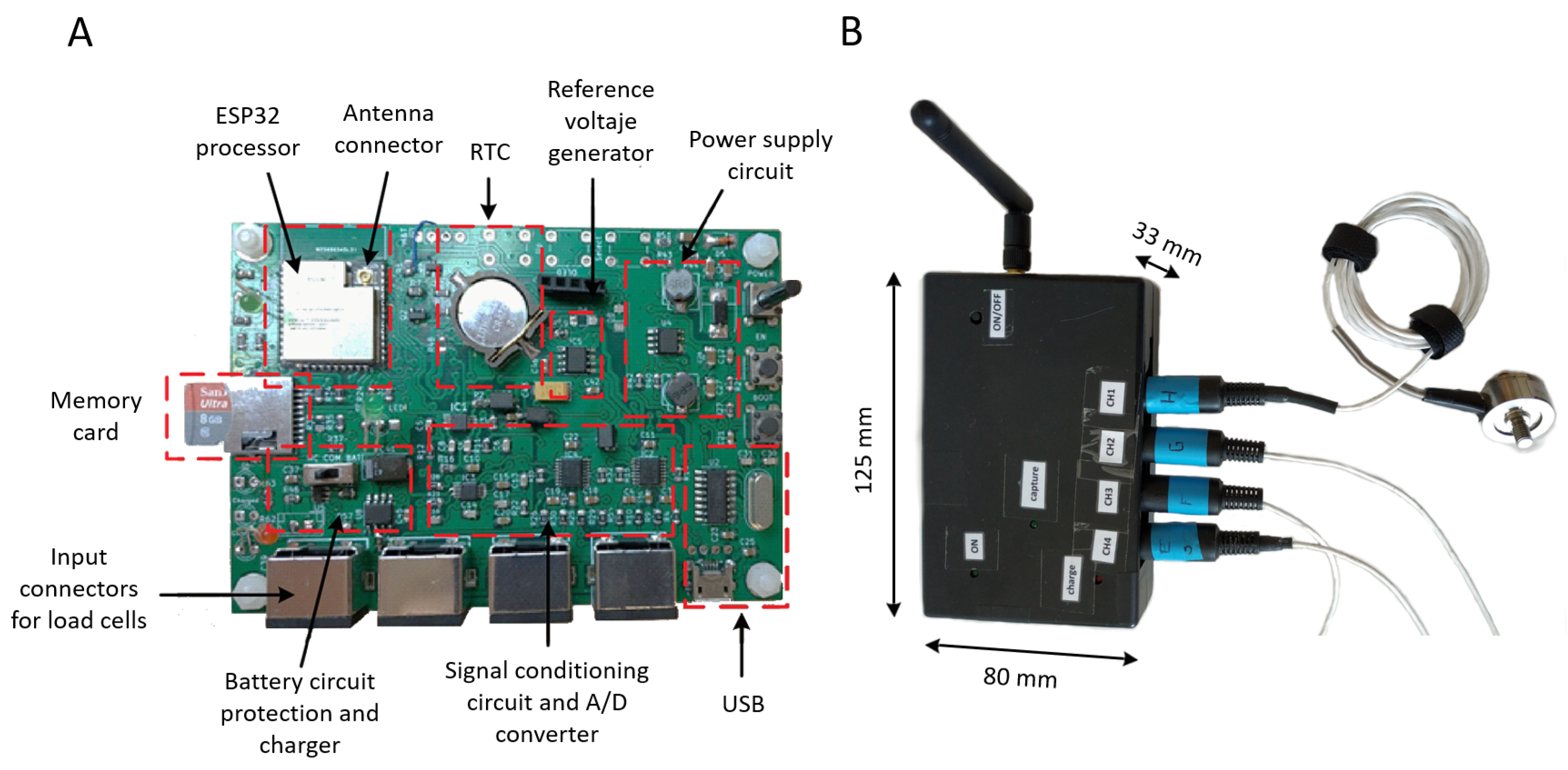
2.2. Hardware Design
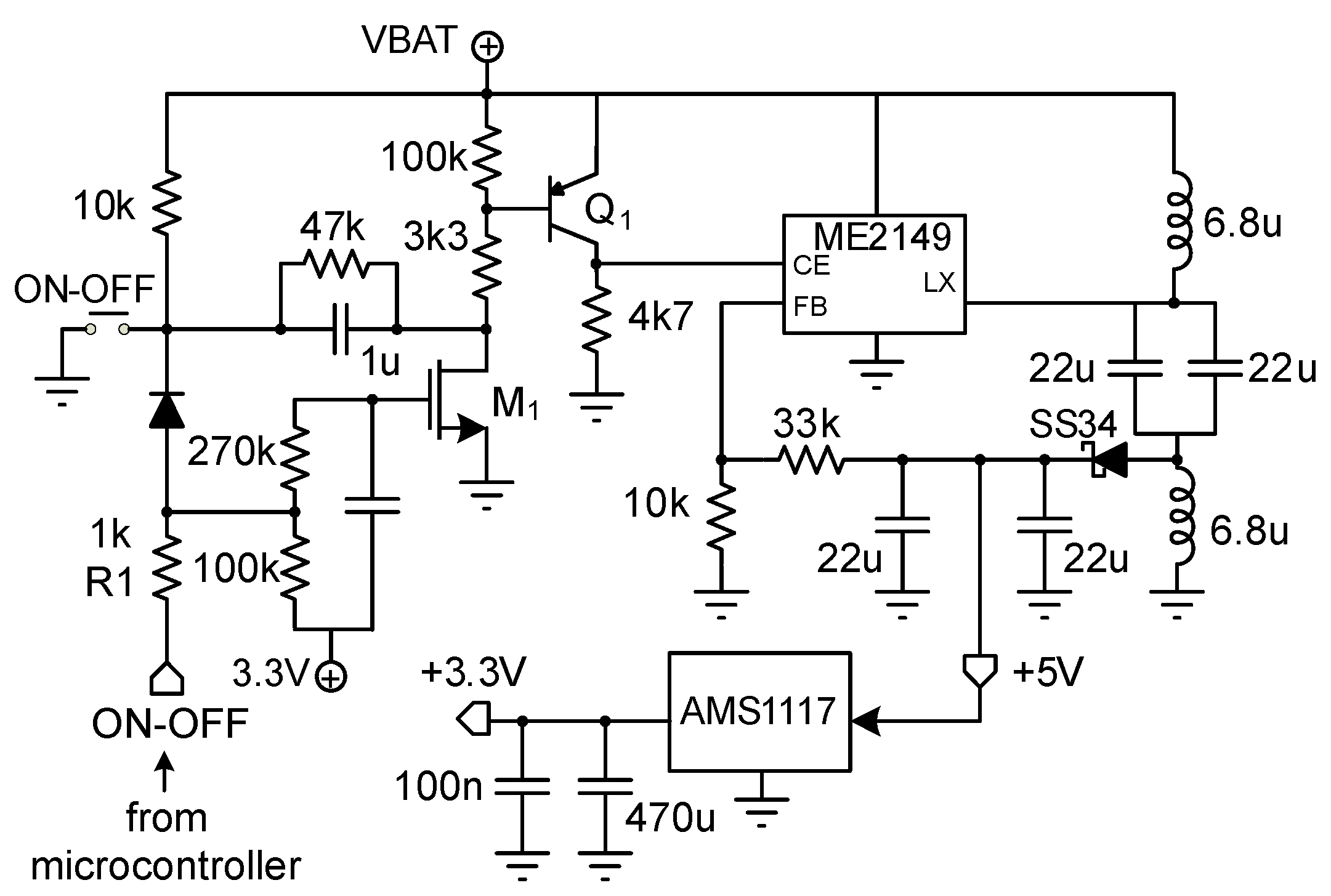
2.2.1. Power Supply System
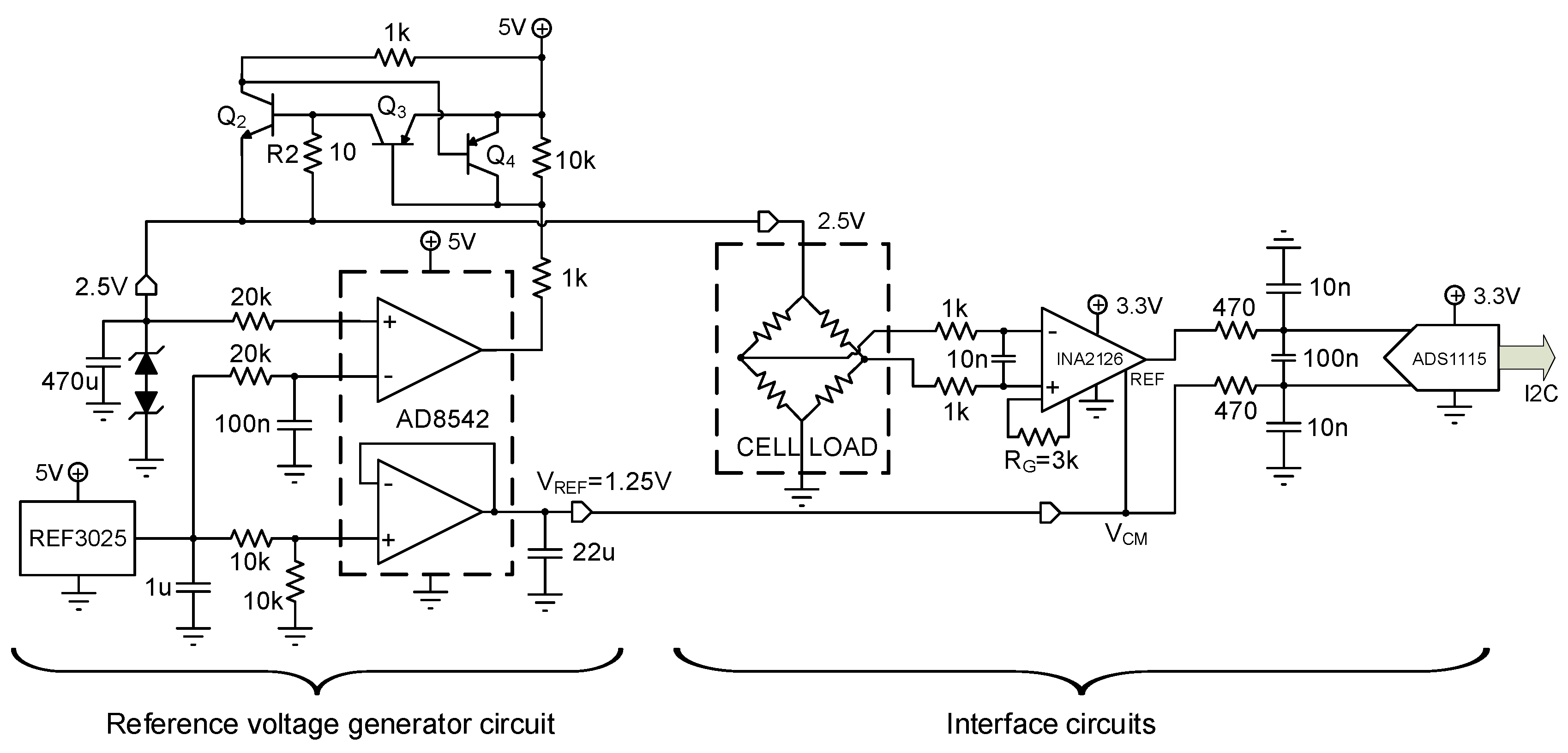
2.2.2. Signal Conditioning and A/D Conversion
2.3. Firmware
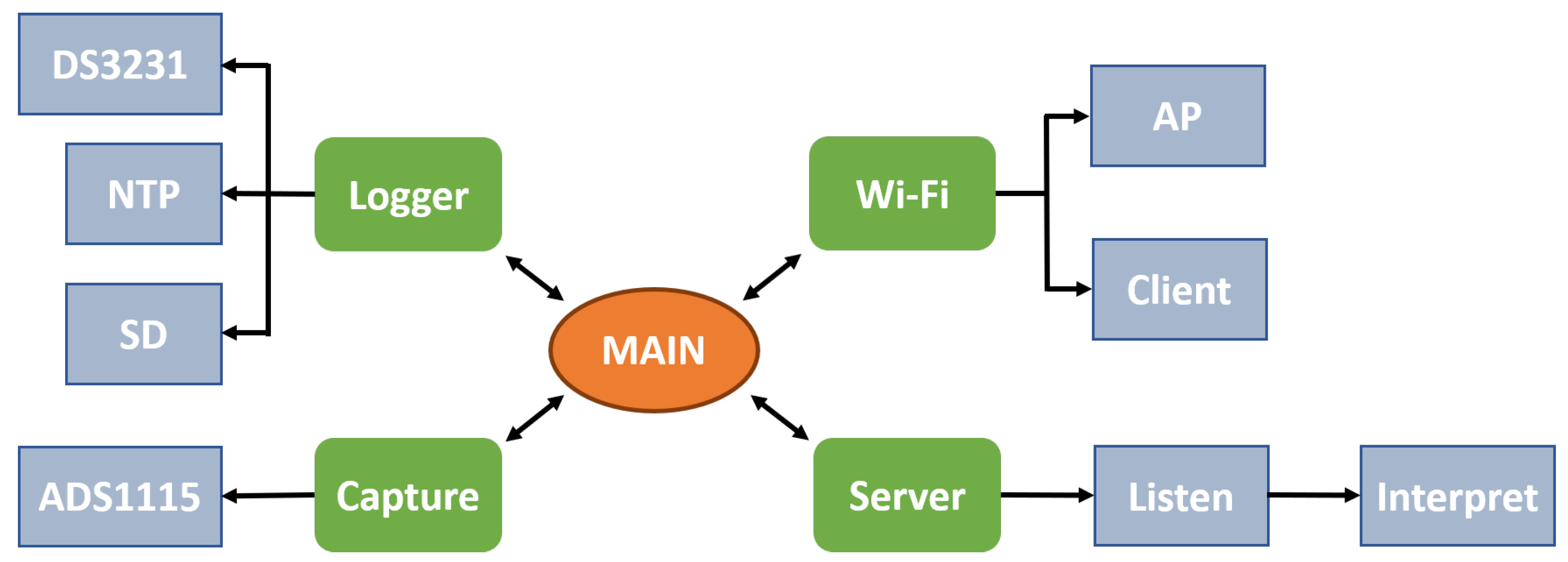
- Main: the central program responsible for initializing system tasks and leaving it in standby mode. Before calling the main program, it executes the initial configuration and other internal tasks responsible for the maintenance of the system and other parts of the ESP32 (WiFi system, internal storage system, or the run-time support).
- Logger: This module ensures the correct time and date at startup employing the real-time clock (DS3231 RTC), which has its own battery. In case of incorrect data, it attempts to connect to WiFi to retrieve the time information from a time server using the Network Time Protocol (NTP). The module also writes and reads collected data and diagnostic messages to the micro-SD memory. This storage on the micro-SD card is independent of the wireless transmission, ensuring the proper collection of the in vivo measures in cases of the loss of WiFi signal.
- WiFi: ensures the connections and the correct operation during experimentation, operating as a client or as an access point (AP).
- Server: This module, which was developed using the netconn library of the ESP32 SDK, activates and waits for clients to connect. Once the client is connected, the access to a command interpreter is available, allowing making calls to different system functions: acquisition, capture, or reading configuration and information download from the disk.
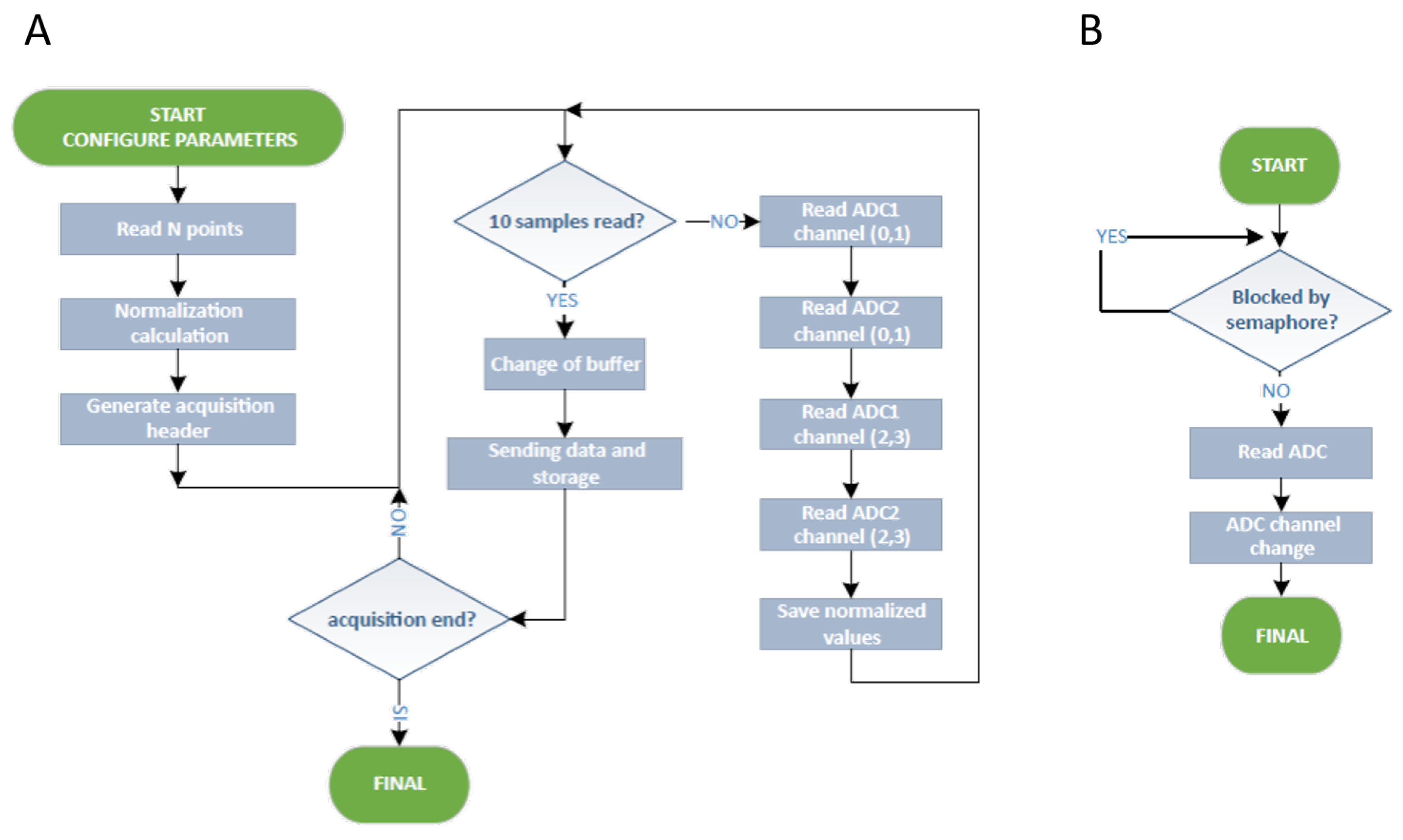
- Capture: performs the process of reading the sensors, integrating two synchronized tasks: the data capture task and the data storing task. The two A/D accessible via the I2C port are used so that, every 2 readings, a signal multiplexing is performed to change the capture channel.
2.4. Force Measurements
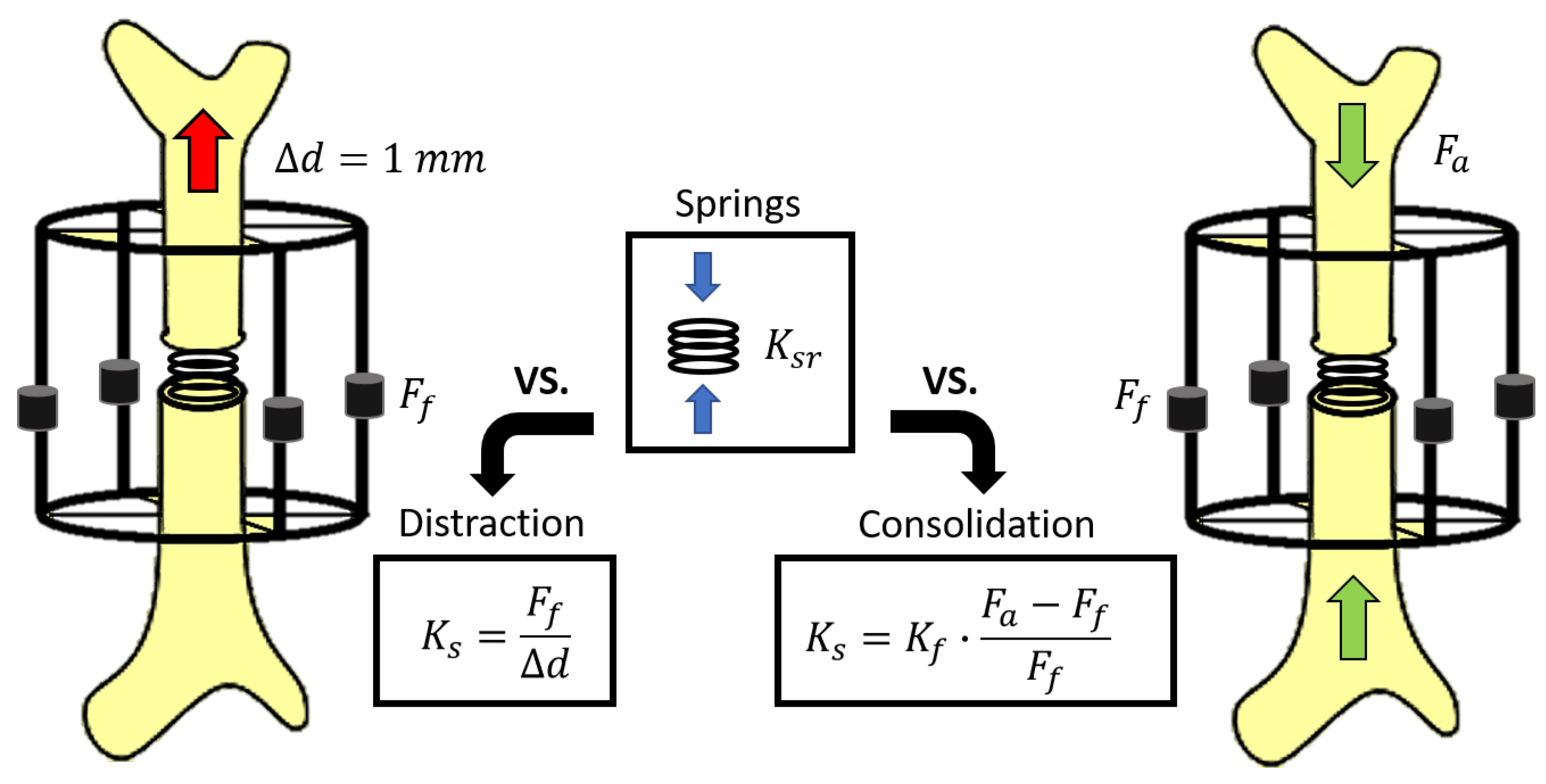
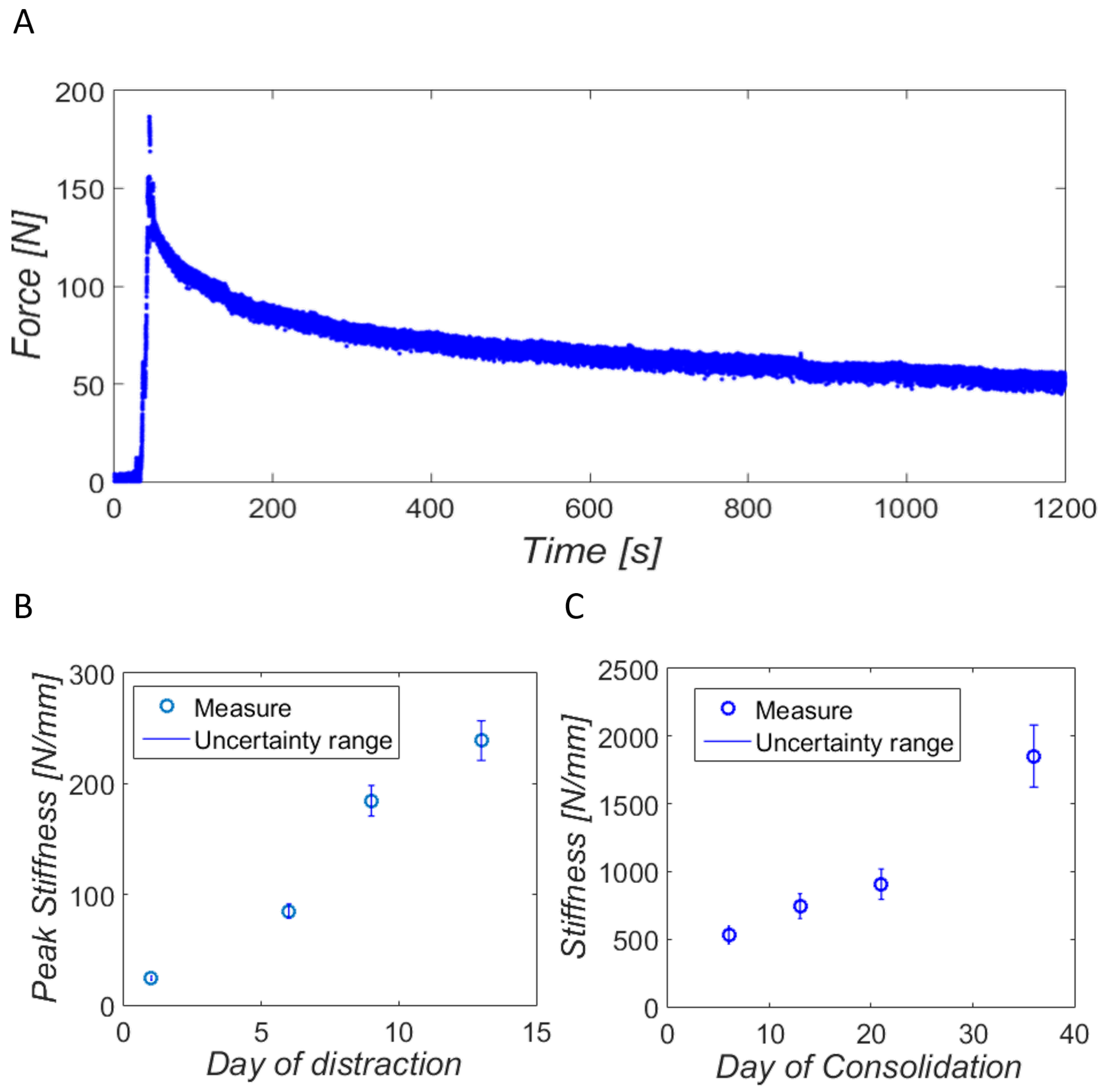
- Distraction measures: After applying a displacement of a bony fragment, the reaction force of hard and soft tissues to distraction is measured by means of the external fixator and the acquisition system () at rest [26,44]. Assuming the absence of movement in the treated limb, the monitored force corresponds to the traction force applied on the bone callus () for its axial deformation.
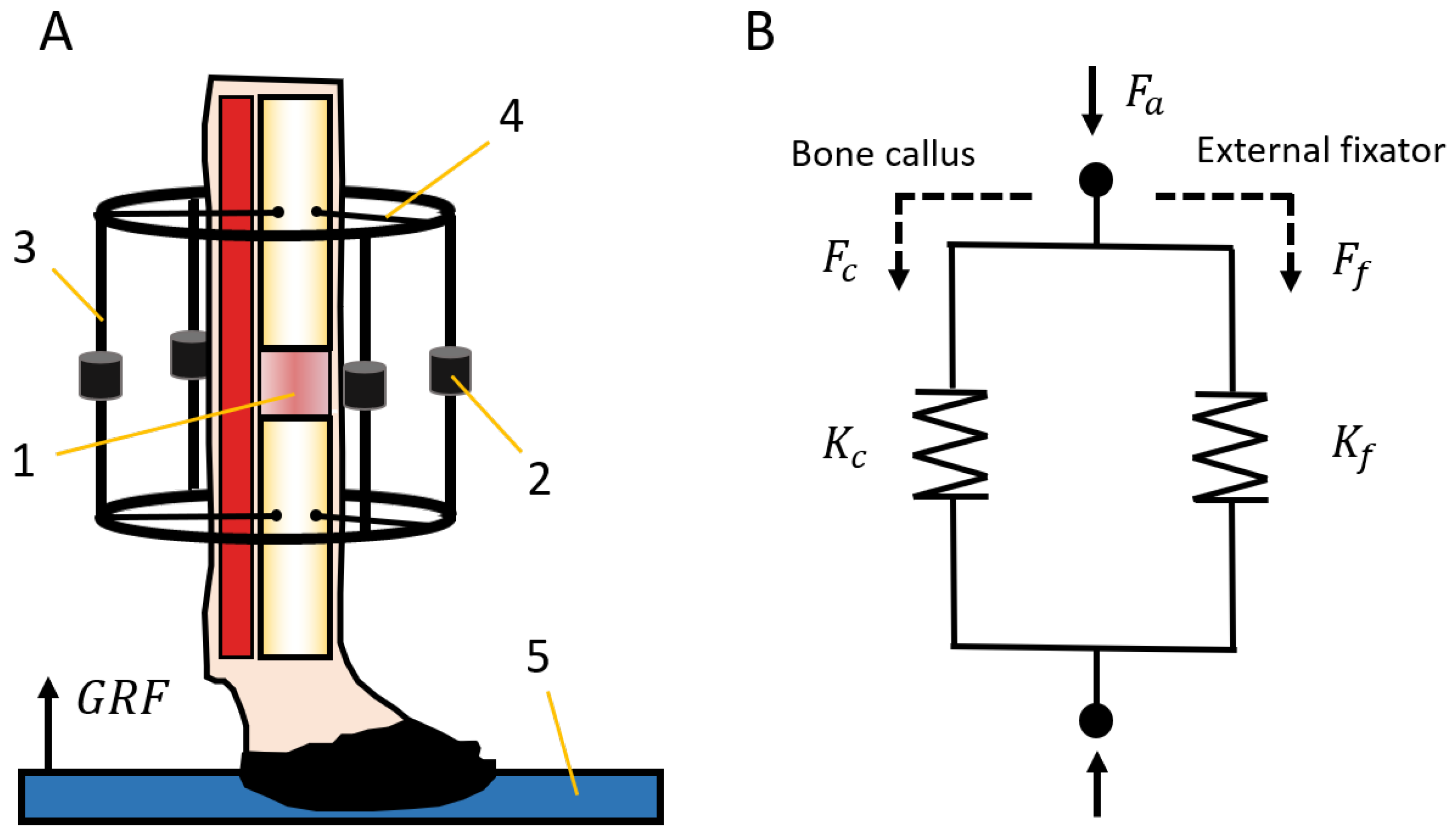
- Consolidation measures: Gait analysis is a common non-invasive technique that allows quantitatively assessing the evolution of multiple bone pathologies during the consolidation phase [25,38,45]. In bone regeneration processes, these measurements require monitoring the forces through an instrumented fixator and the ground reaction force (GRF) during the steps of the animal [25,38]. The GRF, which is commonly quantified by a load platform (Figure 8A), is an important input in biomechanical analysis and represents a part of the internal force through the skeletal structure of the animal (). Muscles and soft tissues store the rest of the internal force during a stance phase, and this is not directly quantifiable. In the operated limb, forces through the skeletal structure () are divided between the external fixator () and the bone callus () depending on its degree of mineralization (Figure 8B). Therefore, the load through the bone callus was calculated from both previous loads using Equation (1).
2.5. Models for Stiffness Estimation
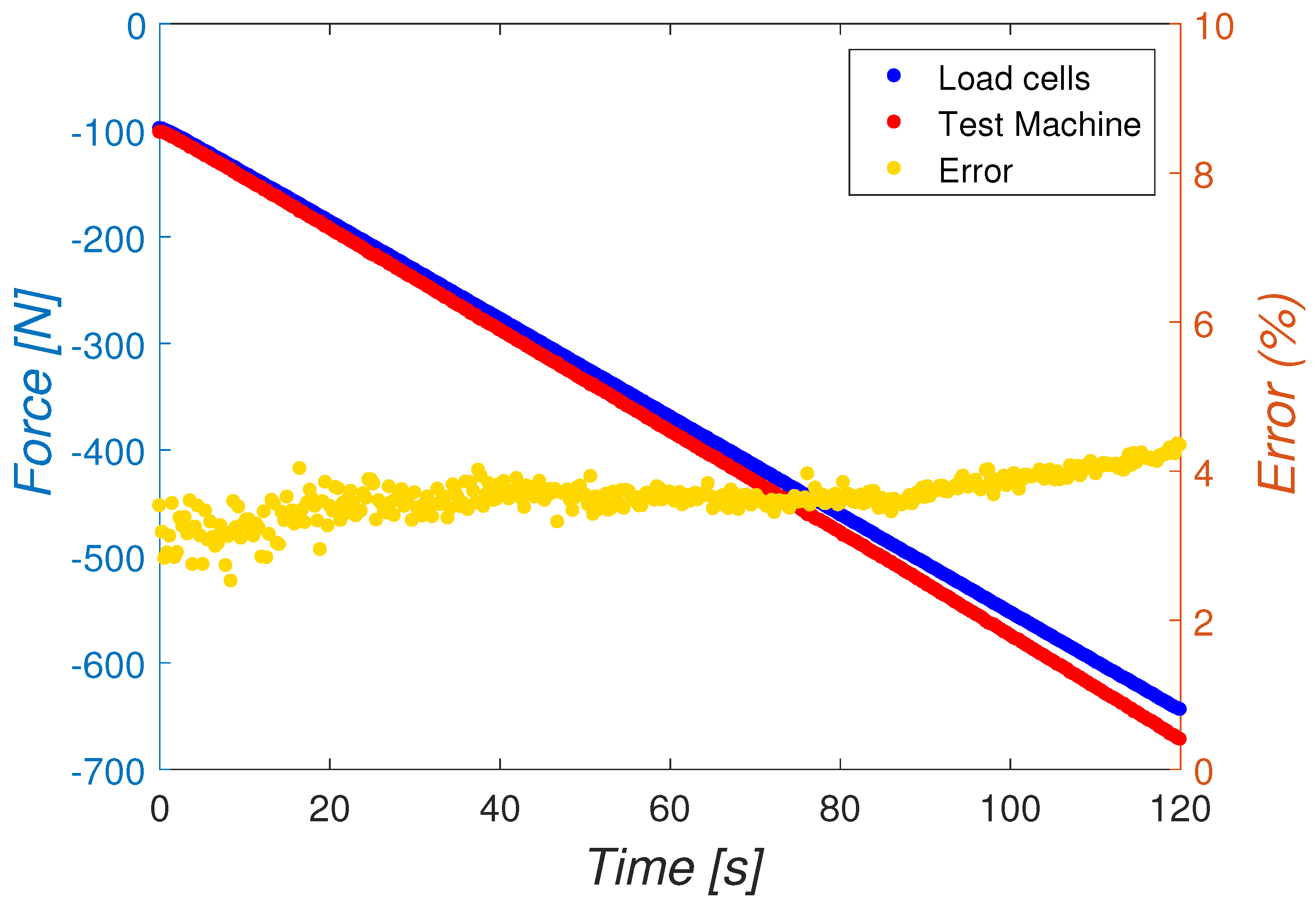
2.6. In Vitro Calibration
2.7. In Vivo Measurements
3. Results
3.1. In Vitro Results
3.2. In Vivo Validation
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Monitoring Application
- Main: This is the module where the main program is located, which is responsible for managing the user interface of the main window and calling the other modules.
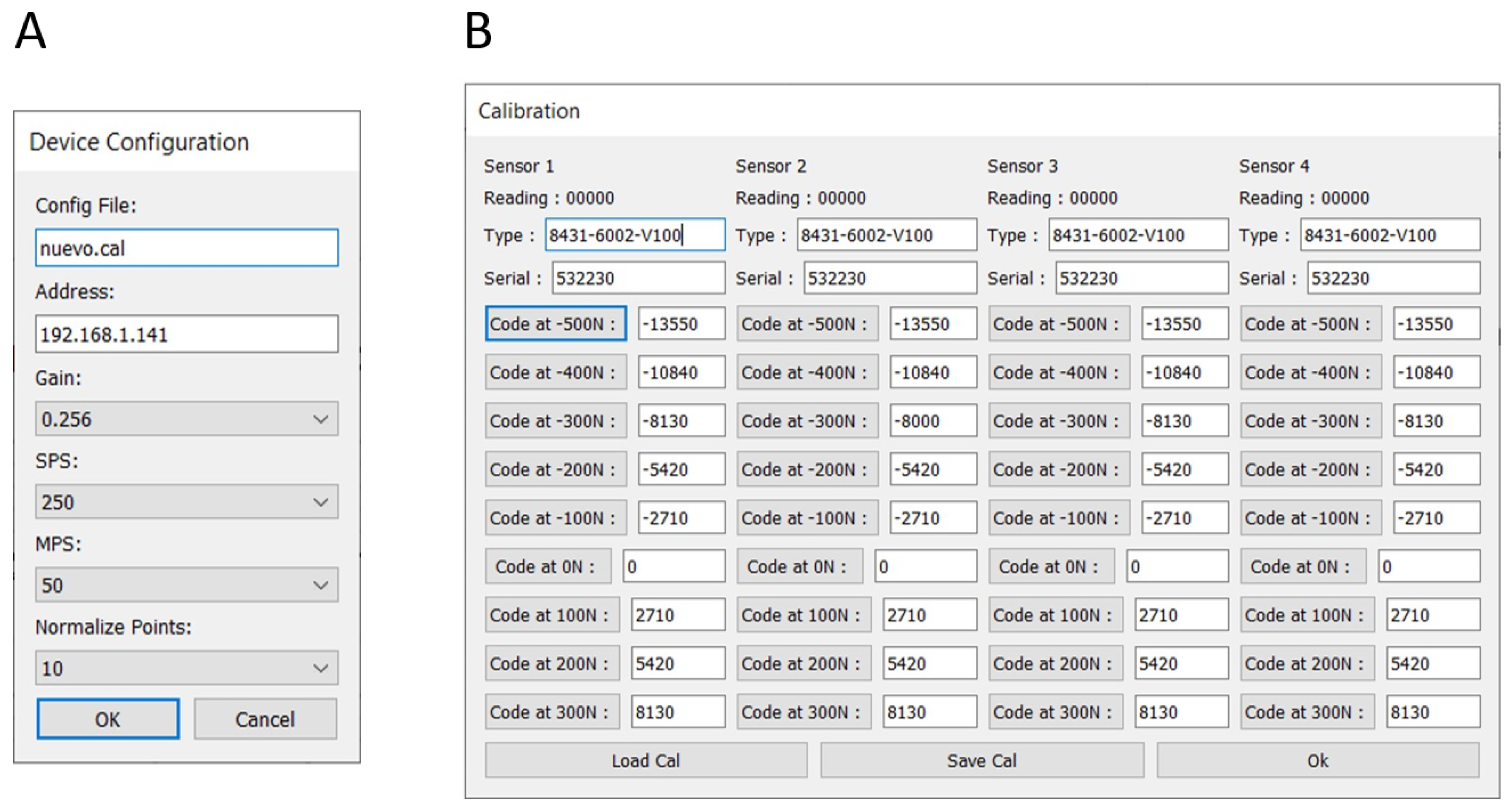
- Config: It manages the configuration, which is saved in a file: client.ini. This file includes the capture parameters, the IP address of the remote device, and the calibration configuration file. When the program starts, it looks for the configuration file and loads the data. If the file does not exist, a new one is created with the default values. In this case, a default calibration file is also created.
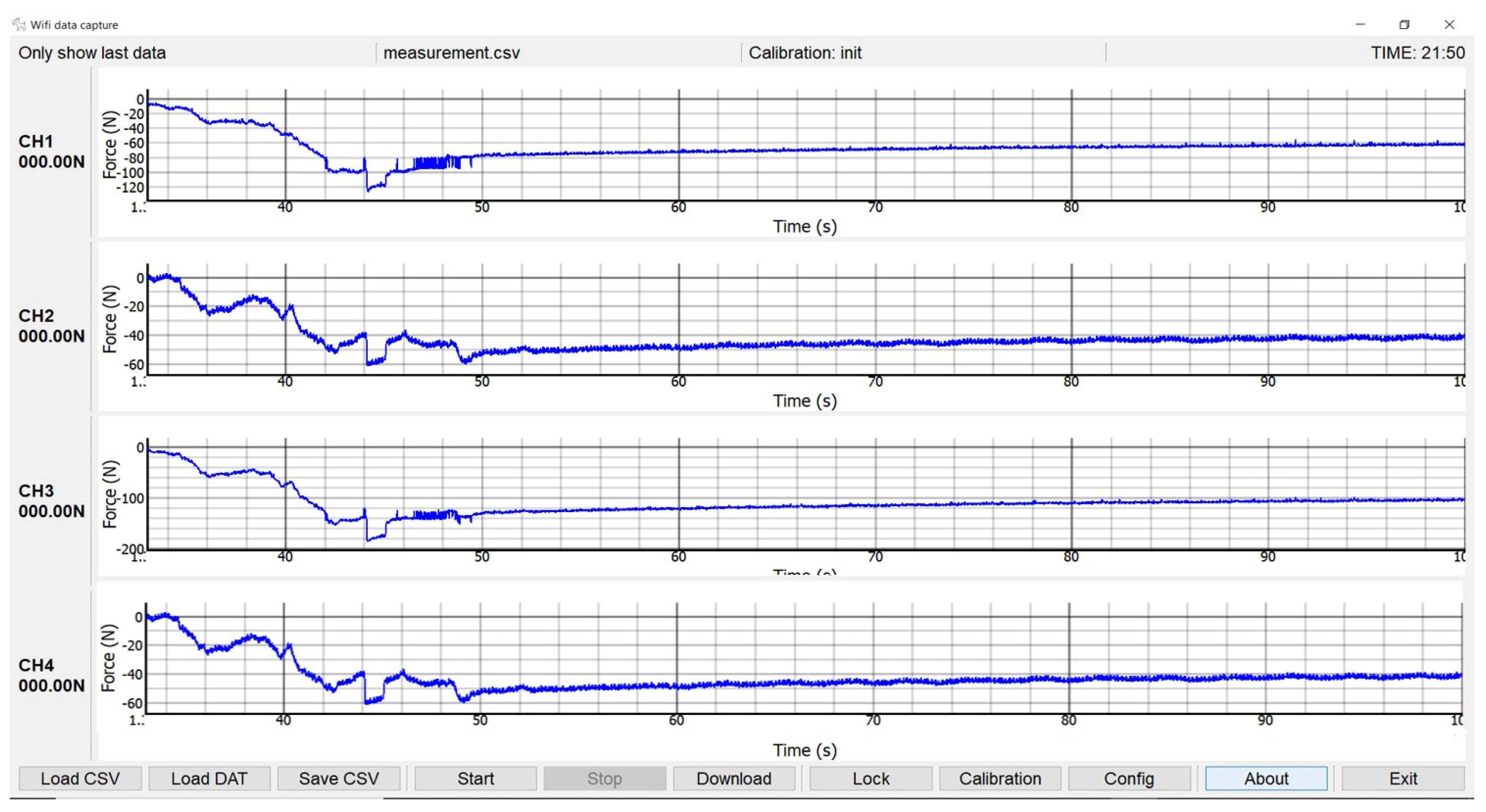
- Graph: It is the module in charge of the graphic representation, updating of data curves and saving them in a CSV file.
- Tcp_txrx: It receives the data from the remote device through a TCP connection; it decrypts and interpolates it and saves the corresponding CSV files. It can also download and delete files residing in the storage of the remote device (microSD card).
- Mb_tools: It integrates auxiliary subroutines, such as error message windows.
- About: It displays debug information and allows firmware loading on the ESP32 processor from the data acquisition card.


Appendix B. Uncertainties Calculation
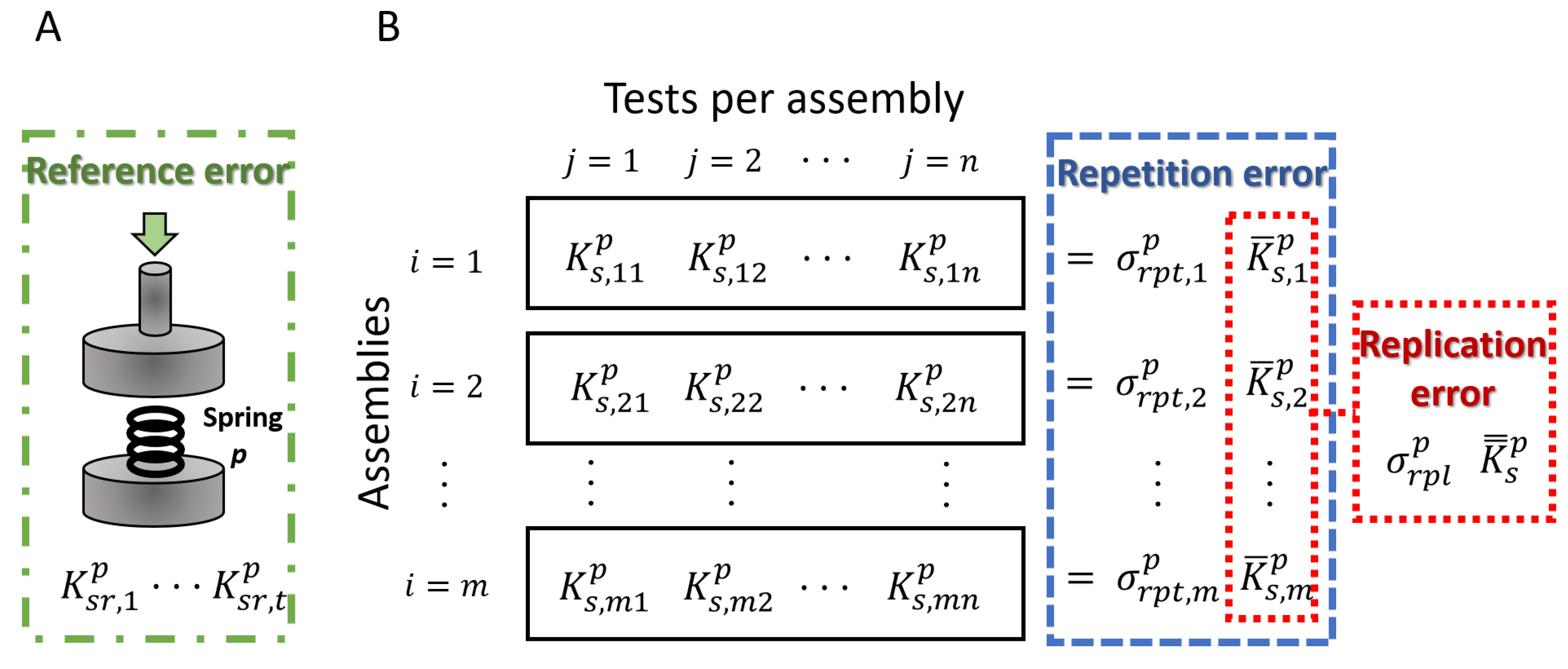
- Reference uncertainty: evaluates the error in the estimation of the real values of the reference elastic springs. Firstly, the stiffness of the spring is determined for each in vitro test (, t = 1...5). Consequently, the mean () and standard deviation () of the reference stiffness values were calculated, and the associated reference uncertainty () was computed using Equation (A1).
- Repetition uncertainty: quantifies the variations in the repetition of the measurements for the same set-up because of factors unrelated to the fixator assembly, e.g., environmental conditions or unremarkable differences in the performance of the test machine. The means () and standard deviations () of the estimated stiffness value (Figure A3, blue) for each assembly (i) allow the calculation of an associated uncertainty per assembly applying Equation (A3).where n is the number of tests per assembly, in this case n = 5. From these calculations, the global repetition uncertainty is assumed as the maximum of uncertainties per assembly (Equation (A4)).
- Replication uncertainty: takes into consideration the slight differences in measurements from the replication of the tests in different assemblies of the external fixator, e.g., due to the restraint of the pins or the placement of the bars between frames. For its calculation, the mean of the stiffness of each individual assembly was used (, i = 1…m) (Figure A3B, red), from which the global mean () and standard deviation () were calculated. Finally, the global replication uncertainty was determined using Equation (A2):

References
- Dimitriou, R.; Jones, E.; McGonagle, D.; Giannoudis, P.V. Bone regeneration: Current concepts and future directions. BMC Med. 2011, 9, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oryan, A.; Kamali, A.; Moshiri, A.; Baghaban Eslaminejad, M. Role of mesenchymal stem cells in bone regenerative medicine: What is the evidence? Cell Tissues Organs. 2017, 204, 59–83. [Google Scholar] [CrossRef] [PubMed]
- Glatt, V.; Evans, C.H.; Tetsworth, K. A concert between biology and biomechanics: The influence of the mechanical environment on bone healing. Front. Physiol. 2016, 7, 678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meazzini, M.C.; Mazzoleni, F.; Gabriele, C.; Bozzetti, A. Mandibular distraction osteogenesis in hemifacial microsomia: Long-term follow-up. J. Craniomaxillodac. Surg. 2005, 33, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Ilizarov, G.A.; Kaplunov, A.G.; Degtiarev, V.E.; Lediaev, V.I. Treatment of pseudarthroses and ununited fractures, complicated by purulent infection, by the method of compression-distraction osteosynthesis. Orthop. Travmetol. Protez. 1972, 33, 10–14. [Google Scholar]
- Hatefi, S.; Etamadi Sh, M.; Yihun, Y.; Mansouri, R.; Akhlaghi, A. Continuous distraction osteogenesis device with MAAC controller for mandibular reconstruction applications. Biomed. Eng. Online 2019, 18, 43. [Google Scholar] [CrossRef] [Green Version]
- Machado, P.; Li, J.; Blackman, R.; Liu, J.; Kepler, C.; Fang, T.; Muratore, R.; Winder, J.; Winder, A.; Forsberg, F. Acceleration of fracture healing: A comparison between clinical available low intensity pulsed ultrasound (LIPUS) and a novel BiModal acoustic signal system. In Proceedings of the 2019 IEEE International Ultrasonic Symposium (IUS), Glasgow, UK, 6–9 October 2019; pp. 1304–1307. [Google Scholar]
- Russo, T.; D’Amora, U.; Gloria, A.; Tunesi, M.; Sandri, M.; Rodilossi, S.; Albani, D.; Forloni, G.; Giordano, C.; Cigada, A.; et al. Systematic analysis of injectable materials and 3D rapid prototyped magnetic scaffolds: From CNS applications to soft and hard tissue repair/regeneration. Procedia Eng. 2013, 59, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Paredes, C.; Martínez-Vázquez, F.J.; Pajares, A.; Miranda, P. Development by robocasting and mechanical characterization of hybrid HA/PCL coaxial scaffolds for biomedical applications. J. Eur. Ceram. Soc. 2019, 39, 4375–4383. [Google Scholar] [CrossRef]
- Lienemann, P.S.; Metzger, S.; Kiveliö, A.-S.; Blanc, A.; Papageorgiou, P.; Astolfo, A.; Pinzer, B.R.; Cinelli, P.; Weber, F.E.; Schibli, R.; et al. Longitudinal in vivo evaluation of bone regeneration by combined measurement of multi-pinhole SPECT and micro-CT for tissue engineering. Sci. Rep. 2015, 5, 10238. [Google Scholar] [CrossRef] [Green Version]
- Trejo-Iriarte, C.G.; Serrano-Bello, J.; Gutiérrez-Escalona, R.; Mercado-Marques, C.; García-Honduvilla, N.; Buján-Varela, J.; Medina, L.A. Evaluation of bone regeneration in critical size cortical bone defect in rat mandible using microCT and histological analysis. Arch. Oral Biol. 2019, 101, 165–171. [Google Scholar] [CrossRef]
- Ohyama, M.; Miyasaka, Y.; Sakurai, M.; Yokobori, A.T., Jr.; Sasaki, S. The mechanical behavior and morphological structure of callus in experimental callotasis. Biomed. Mater. Eng. 1994, 4, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Luk, H.K.; Lai, Y.M.; Qin, L.; Huang, Y.-P.; Zheng, Y.-P. Computed radiographic and ultrasonic evaluation of bone regeneration during tibial distraction osteogenesis in rabbits. Ultrasound Med. Biol. 2012, 38, 1744–1758. [Google Scholar] [CrossRef] [PubMed]
- Webb, J.; Herling, G.; Gardner, T.; Kenwright, J.; Simpson, A.H. Manual assessment of fracture stiffness. Injury 1996, 27, 319–320. [Google Scholar] [CrossRef]
- Panjabi, M.M.; Lindsey, R.W.; Walter, S.D.; White, A.A., 3rd. The clinician’s ability to evaluate the strength of healing fractures from plain radiographs. J. Orthop. Trauma 1989, 3, 29–32. [Google Scholar] [CrossRef]
- Storani de Almeida, M.; Dias Maciel, C.; Pereira, J.C. Proposal for an ultrasonic tool to monitor osseointegration of dental implants. Sensors 2007, 7, 1224–1237. [Google Scholar] [CrossRef] [Green Version]
- Bliven, E.K.; Greinwald, M.; Hackl, S.; Augat, P. External fixation of the lower extremities: Biomechanical perspective and recent innovations. Injury 2019, 50 (Suppl. 1), S10–S17. [Google Scholar] [CrossRef]
- Watanabe, Y.; Takai, S.; Arai, Y.; Yoshino, N.; Hirasawa, Y. Prediction of mechanical properties of healing fractures using acoustic emission. J. Orthop. Res. 2001, 19, 548–553. [Google Scholar] [CrossRef]
- Rubin, C.T.; Sommerfeldt, D.W.; Judex, S.; Qin, Y.-X. Inhibition of osteopenia by low magnitude, high-frecuency mechanical stimuli. Drug. Discov. Today 2001, 6, 848–858. [Google Scholar] [CrossRef]
- Gómez-Benito, M.J.; González-Torres, L.A.; Reina-Romo, E.; Grasa, J.; Seral, B.; García-Aznar, J.M. Influence of high-frequency cyclical stimulation on the bone fracture-healing process: Mathematical and experimental models. Philos. Trans. A Math. Phys. Eng. Sci. 2011, 369, 4278–4294. [Google Scholar]
- Tower, S.S.; Beals, R.K.; Duwelius, P.J. Resonant frequency analysis of the tibia as a measure of fracture healing. J. Orthop. Trauma 1993, 7, 552–557. [Google Scholar] [CrossRef]
- Claes, L.E.; Cunningham, J.L. Monitoring the mechanical properties of healing bone. Clin. Orthop. Relat. Res. 2009, 467, 1964–1971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claes, L.; Grass, R.; Schmickal, T.; Kisse, B.; Eggers, C.; Gerngross, H.; Mutschler, W.; Arand, M.; Wintermeyer, T.; Wentzensen, A. Monitoring and healing analysis of 100 tibial shaft fractures. Langenbecks Arch. Surg. 2002, 387, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, J.L.; Kenwright, J.; Kershaw, C.J. Biomechanical measurement of fracture healing. J. Med. Eng. Technol. 1990, 14, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Mora-Macías, J.; Reina-Romo, E.; López-Pliego, M.; Giráldez-Sánchez, M.A.; Domínguez, J. In Vivo Mechanical Characterization of the Distraction Callus During Bone Consolidation. Ann. Biomed. Eng. 2015, 43, 2663–2674. [Google Scholar] [CrossRef]
- Mora-Macías, J.; Reina-Romo, E.; Domínguez, J. Model of the distraction callus tissue behavior during bone transport based in experiments in vivo. J. Mech. Behav. Biomed. Mater. 2016, 61, 419–430. [Google Scholar] [CrossRef]
- Grasa, J.; Gómez-Benito, M.J.; González-Torres, L.A.; Asiaín, D.; Quero, F.; García-Aznar, J.M. Monitoring in vivo load transmission through an external fixator. Ann. Biomed. Eng. 2010, 38, 605–612. [Google Scholar] [CrossRef]
- Bonnet, A.S.; Dubois, G.; Lipinski, P.; Schouman, T. In vivo study of human mandibular distraction osteogenesis. Part I: Bone transport force determination. Acta Bioeng. Biomech. 2012, 14, 3–14. [Google Scholar]
- Mattei, L.; Di Puccio, F.; Marchetti, S. In vivo impact testing on a lengthened femur with external fixation: A future option for the non-invasive monitoring of fracture healing? J. R. Soc. Interface 2018, 15. [Google Scholar] [CrossRef] [Green Version]
- Mora-Macías, J.; Reina-Romo, E.; Domínguez, J. Distraction osteogenesis device to estimate the axial stiffness of the callus In Vivo. Med. Eng. Phys. 2015, 37, 969–978. [Google Scholar] [CrossRef]
- Tan, Y.; Hu, J.; Ren, L.; Zhu, J.; Yang, J.; Liu, D. A passive and wireless sensor for bone plate strain monitoring. Sensors 2017, 17, 2635. [Google Scholar]
- Chiu, W.K.; Vien, B.S.; Russ, M.; Fitzgerald, M. Towards a Non-Invasive technique for healing assessment of internally fixated Femur. Sensors 2019, 19, 857. [Google Scholar] [CrossRef] [Green Version]
- Rahman, T.; Akins, R.E.; Wee, J. Continuous force measurement in limb lengthening. J. Bioeng. Biomed. Sci. 2011, 1, 104. [Google Scholar] [CrossRef] [Green Version]
- Reifenrath, J.; Gottschalk, D.; Angrisani, N.; Besdo, S.; Meyer-Lindenberg, A. Axial forces and bending moments in the loaded rabbit tibia in vivo. Acta Vet. Scand. 2012, 54, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattei, L.; Di Puccio, F.; Marchetti, S. Fracture healing monitoring by impact tests: Single case study of a fractured tibia with external fixator. IEEEE J. Transl. Eng. Health Med. 2019, 7, 2100206. [Google Scholar] [CrossRef]
- Meyers, N.; Schülke, J.; Ignatius, A.; Claes, L. Novel systems for the application of isolated tensile, compressive, and shearing stimulation of distraction callus tissue. PLoS ONE 2017, 12, e0189432. [Google Scholar] [CrossRef] [Green Version]
- Tufekci, P.; Tavakoli, A.; Dlaska, C.; Neumann, M.; Shanker, M.; Saifzadeh, S.; Steck, R.; Schuetz, M.; Epari, D. Early mechanical stimulation only permits timely bone healing in sheep. J. Orthop. Res. 2018, 36, 1790–1796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mora-Macías, J.; Reina-Romo, E.; Morgaz, J.; Domínguez, J. In vivo gait analysis during bone transport. Ann. Biomed. Eng. 2015, 43, 2090–2100. [Google Scholar] [CrossRef]
- Duda, G.N.; Eckert-Hübner, K.; Sokiranski, R.; Kreutner, A.; Miller, R.; Claes, L. Analysis of inter-fragmentary movement as a function of musculoskeletal loading conditions in sheep. J Biomech. 1998, 31, 201–210. [Google Scholar] [CrossRef]
- Fürmetz, J.; Soo, C.; Behrendt, W.; Thaller, P.H.; Siekmann, H.; Böhme, J.; Josten, C. Bone transport for limb reconstruction following severe tibial fractures. Orthop. Rev. (Pavia) 2016, 8, 6384. [Google Scholar] [CrossRef] [Green Version]
- Hasler, C.C.; Krieg, A.H. Current concepts of leg lengthening. J. Child. Orthop. 2012, 6, 89–104. [Google Scholar] [CrossRef] [Green Version]
- Coppola, C.; Maffulli, N. Limb shortening for the management of leg length discrepancy. J. R. Coll. Surg. Edinb. 1999, 44, 46–54. [Google Scholar] [PubMed]
- Gubin, A.; Borzunov, D.; Malkova, T. lizarov method for bone lengthening and defect management review of contemporary literature. Bull. Hosp. Jt. Dis. 2016, 74, 145–154. [Google Scholar]
- Meyers, N.; Schülke, J.; Ignatius, A.; Claes, L. Evolution of callus tissue behavior during stable distraction osteogenesis. J. Mech. Behav. Biomed. Mater. 2018, 85, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Krizsan-Agbas, D.; Winter, M.K.; Eggimann, L.S.; Meriwether, J.; Berman, N.E.; Smith, P.G.; McCarson, K.E. Gait analysis at multiple speeds reveals differential functional and structural outcomes in response to graded spinal cord injury. J. Neurotrauma 2014, 31, 846–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunner, U.H.; Cordey, J.; Schweiberer, L.; Perren, S.M. Force required for bone segment transport in the treatment of large bone defects using medullary nail fixation. Clin. Orthop. Relat. Res. 1994, 301, 147–155. [Google Scholar] [CrossRef]
- Wee, J.; Rahman, T.; Akins, R.E.; Seliktar, R.; Levine, D.G.; Richardson, D.W.; Dodge, G.R.; Thabet, A.M.; Holmes, L.; Mackenzie, W.G. Using distraction forces to drive an autodistractor during limb lengthening. Med. Eng. Phys. 2011, 33, 1001–1007. [Google Scholar] [CrossRef]
- Forriol, F.; Goenaga, I.; Mora, G.; Viñolas, J.; Cañadell, J. Measurement of bone lengthening forces: An experimental model in the lamb. Clin. Biomech. 1997, 12, 17–21. [Google Scholar] [CrossRef]
- Newman, E.; Turner, A.S.; Wark, J.D. The potential of sheep for the study of osteopenia: Current status and comparison with other models. Bone 1995, 16, S277–S284. [Google Scholar] [CrossRef]
- den Boer, F.C.; Patka, P.; Bakker, F.C.; Wippermann, B.W.; van Lingen, A.; Vink, G.Q.M.; Boshuizen, K.; Haarman, H.J.T.M. New segmental long bone defect model in sheep: Quantitative analysis of healing with dual energy x-ray absorptiometry. J. Orthop. Res. 1999, 17, 654–660. [Google Scholar] [CrossRef]
- Reichert, J.C.; Saifzadeh, S.; Wullschleger, M.E.; Epari, D.R.; Schütz, M.A.; Duda, G.N.; Schell, H.; van Griensven, M.; Redl, H.; Hutmacher, D.W. The challenge of establishing preclinical models for segmental bone defect research. Biomaterials 2009, 30, 2149–2163. [Google Scholar] [CrossRef] [Green Version]
- Field, J.R.; McGee, M.; Wildenauer, C.; Kurmis, A.; Margerrison, E. The utilization of a synthetic bone void filler (JAX) in the repair of a femoral segmental defect. Vet. Comp. Orthop. Traumatol. 2009, 22, 87–95. [Google Scholar] [PubMed]
- Kienast, B.; Kowald, B.; Seide, K.; Aljudaibi, M.; Faschingbauer, M.; Juergens, C.; Gille, J. An electronically instrumented internal fixator for the assessment of bone healing. Bone Jt. Res. 2016, 5, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Claes, L.; Laule, J.; Wenger, K.; Suger, G.; Liener, U.; Kinzl, L. The influence of stiffness of the fixator on maturation of callus after segmental transport. J. Bone Jt. Surg. Br. 2000, 82, 142–148. [Google Scholar] [CrossRef]
- Marsell, R.; Einhorn, T.A. The biology of fracture healing. Injury 2011, 42, 551–555. [Google Scholar] [CrossRef] [Green Version]
- Hosny, G.A. Limb lengthening history, evolution, complications and current concepts. J. Orthop. Traumatol. 2020, 21, 3. [Google Scholar] [CrossRef]
- Windhagen, H.; Bail, H.; Schmeling, A.; Kolbeck, S.; Weiler, A.; Raschke, M. A new device to quantify regenerate torsional stiffness in distraction osteogenesis. J. Biomech. 1999, 32, 857–860. [Google Scholar] [CrossRef]
- Hente, R.; Cordey, J.; Perren, S.M. In vivo measurement of bending stiffness in fracture healing. Biomed. Eng. Online 2003, 2, 8. [Google Scholar] [CrossRef] [Green Version]
- Eastaugh-Waring, S.J.; Hardy, J.R.W.; Cunningham, J.L. Fracture stiffness measurement using orthometer: Reproducibility and sources of error. Clin. Biomech. 2000, 15, 140–142. [Google Scholar] [CrossRef]
- Vauhkonen, M.; Peltonen, J.; Karaharju, E.; Aalto, K.; Alitalo, I. Collagen synthesis and mineralization in the early phase of distraction bone healing. Bone Miner. 1990, 10, 171–181. [Google Scholar] [CrossRef]
- Ai-Aql, Z.S.; Alagl, A.S.; Graves, D.T.; Gerstenfeld, L.C.; Einhorn, T.A. Molecular mechanisms controlling bone formation during fracture healing and distraction osteogenesis. J. Dent. Res. 2008, 87, 107–118. [Google Scholar] [CrossRef]
- Richards, M.; Goulet, J.A.; Schaffler, M.B.; Goldstein, S.A. Temporal and spatial characterization of regenerate bone in the lengthened rabbit tibia. J. Bone Miner. Res. 2009, 14, 1978–1986. [Google Scholar] [CrossRef] [PubMed]
- Leong, P.L.; Morgan, E.F. Measurement of fracture callus material properties via nanoindentation. Acta Biomater. 2008, 4, 1569–1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mora-Macías, J.; Pajares, A.; Miranda, P.; Domínguez, J.; Reina-Romo, E. Mechanical characterization via nanoindentation of the woven bone developed during bone transport. J. Mech. Behav. Biomed. Mater. 2017, 74, 236–244. [Google Scholar] [CrossRef] [PubMed]
- European Co-operation for Accreditation. Evaluation of Uncertainty of Measurement in Calibration; EA-4/02 M; EA Laboratory Committee, EA: Brussels, Belgium, 2013. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Distraction | Consolidation | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| (N/mm) | (N/mm) | (N/mm) | e (%) | U (%) | (N/mm) | (N/mm) | (N/mm) | e (%) | U (%) |
| 16.75 | 17.25 | 1.20 | 3.01 | 8.91 | 103.01 | 98.79 | 16.52 | 4.09 | 21.92 |
| 39.93 | 35.65 | 2.86 | 10.72 | 10.74 | 208.83 | 194.29 | 14.62 | 6.96 | 9.65 |
| 65.45 | 62.88 | 4.03 | 3.93 | 8.29 | 416.37 | 398.33 | 31.86 | 4.33 | 14.22 |
| 102.77 | 92.15 | 3.21 | 10.33 | 5.01 | 1979.03 | 1960.38 | 148.25 | 0.94 | 12.15 |
| 175.01 | 167.09 | 4.90 | 4.52 | 3.81 | 5050.13 | 4572.29 | 539.96 | 9.46 | 16.02 |
| 208.83 | 192.39 | 9.03 | 7.87 | 8.26 | 7448.78 | 7716.09 | 567.94 | 3.59 | 10.28 |
| average | 6.73 | 7.50 | average | 4.90 | 14.04 | ||||
| Study | Hardware/Software | Real-Time | Size (mm) | Weight (g) | Portable | 2nd Storage |
|---|---|---|---|---|---|---|
| Grasa et al. [27] | N.D./Specific | Yes | 150 × 100 × 45 | >315 | Yes | No |
| Mora-Macías et al. [30] | Commercial | Yes | 250 × 200 × 65 | 2430 | Yes | No |
| Reifenrath et al. [34] | Commercial | Yes | 120 × 80 × 55 | 420 | No | No |
| Meyers et al. [36] | Commercial | Yes | N.D. | N.D. | No | No |
| Wee et al. [47] | Commercial | No | 15 Ø × 38 L | 30 | Yes | N.D. |
| This work | Specific | Yes | 125 × 80 × 33 | 173 | Yes | Yes |
| Study | Measurement | Errors |
|---|---|---|
| Mora-Macías et al. [30] | Bone callus axial stiffness in bone transport | 7.8%/9.5% * |
| Widhagen et al. [57] | Bone callus torsional stiffness in distraction osteogenesis | ∼15% |
| Hente et al. [58] | Bending stiffness in fracture healing | ∼29.3% |
| Eastaugh-Waring et al. [59] | Tissue stiffness in fracture healing | ∼10% |
| This work | Tissue axial stiffness in several processes | 6.7%/4.9% * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blázquez-Carmona, P.; Sanchez-Raya, M.; Mora-Macías, J.; Gómez-Galán, J.A.; Domínguez, J.; Reina-Romo, E. Real-Time Wireless Platform for In Vivo Monitoring of Bone Regeneration. Sensors 2020, 20, 4591. https://doi.org/10.3390/s20164591
Blázquez-Carmona P, Sanchez-Raya M, Mora-Macías J, Gómez-Galán JA, Domínguez J, Reina-Romo E. Real-Time Wireless Platform for In Vivo Monitoring of Bone Regeneration. Sensors. 2020; 20(16):4591. https://doi.org/10.3390/s20164591
Chicago/Turabian StyleBlázquez-Carmona, Pablo, Manuel Sanchez-Raya, Juan Mora-Macías, Juan Antonio Gómez-Galán, Jaime Domínguez, and Esther Reina-Romo. 2020. "Real-Time Wireless Platform for In Vivo Monitoring of Bone Regeneration" Sensors 20, no. 16: 4591. https://doi.org/10.3390/s20164591