A New Methodology Based on EMD and Nonlinear Measurements for Sudden Cardiac Death Detection

 ,
,  ,
,
Abstract
:1. Introduction
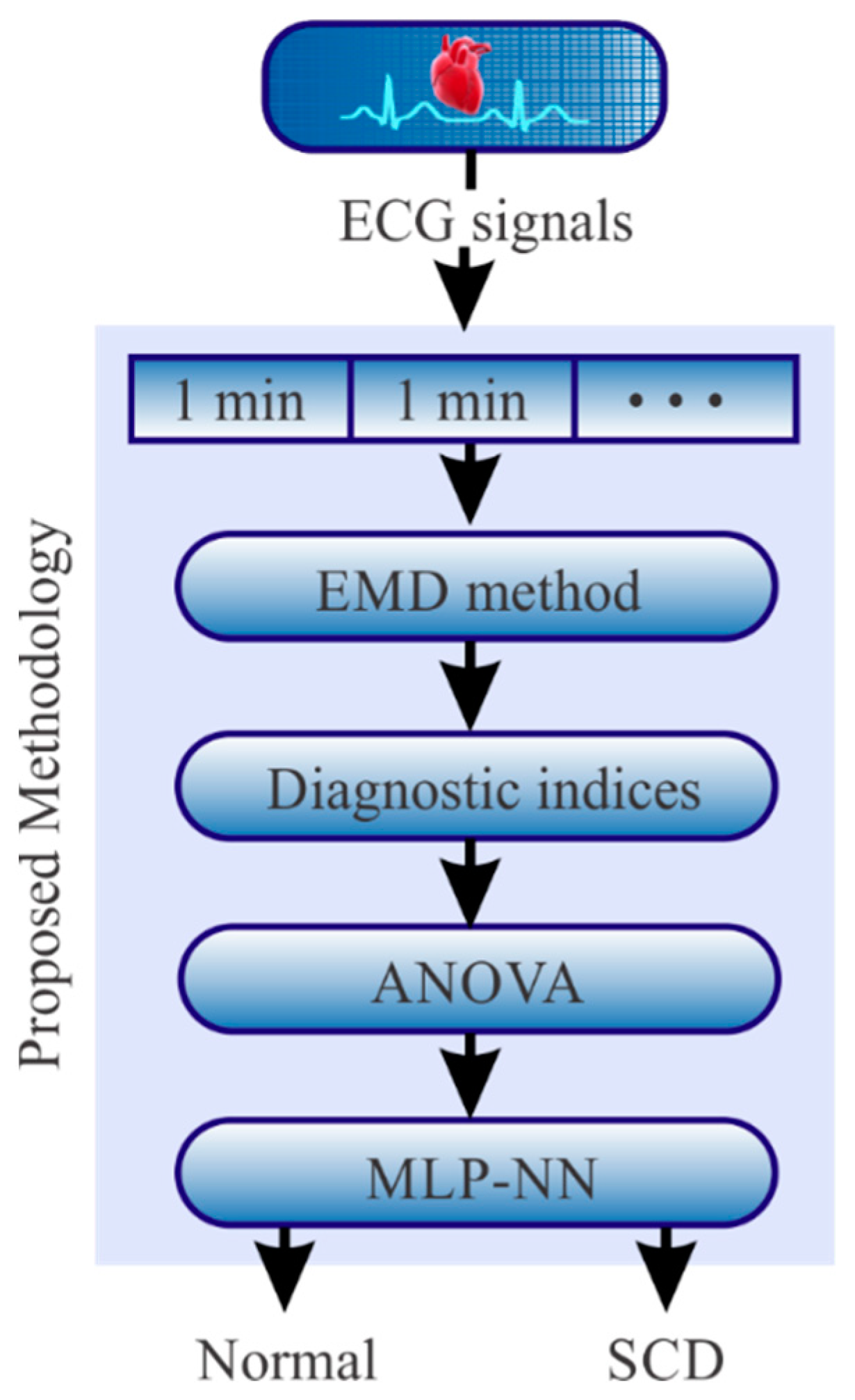
2. Methodology
2.1. Empirical Mode Decomposition (EMD) Method
- Step 1: Obtain the extrema points (maxima and minima) of the input signal given by x(t).
- Step 2: Construct the upper and lower envelopes with the maxima and minima, respectively, using cubic-splines.
- Step 3: Compute the mean signal from both envelopes and name it m1(t).
- Step 4: Obtain the difference between x(t) and m1(t) as h1(t) = x(t)-m1(t).
- Step 5: Check if h1(t) is an IMF (conditions i and ii). If h1(t) is not an IMF, steps from 1 to 4 are repeated in a new k-iteration; otherwise, hk(t) becomes the first IMF, i.e., IMF1.
- Step 6: Obtain the residual signal between x(t) and IMF1 as r1(t) = x(t)-IMF1.
- Step 7: Check if r1(t) is a monotonic function, i.e., a signal from which no more IMFs can be extracted. If r1(t) is not a monotonic signal, r1(t) becomes x(t) and the aforementioned steps are repeated in order to obtain the remaining IMFs. The process ends when rk(t) becomes a monotonic function.
2.2. Diagnostic Indices
2.2.1. Entropy
Shannon Entropy Index (SEI)
Permutation Entropy Index (PEI)
2.3. Fractal Dimension (FD)
2.3.1. Katz Index (KI)
2.3.2. Higuchi Index (HI)
- Step 1. Decompose the analyzed IMF into several discrete-time sequenceswhere q = 1, 2, 3, ..., Qmax, q and p are integer values which determine the initial IMF value and the number of skipped samples, respectively. Qmax is the maximum number of skipped samples.
- Step 2. Calculate the length of the generated sequences using Equation (9).
- Step 3. Compute the sum of all the generated sequences by means of Equation (10).
- Step 4. Calculate the slope of the line that best fits the plotted plane (ln(1/q), ln(L(q)). The obtained slope is the HI value.
2.3.3. Box Dimension Index (BDI)
2.4. The Analysis of Variance (ANOVA)
2.5. Multilayer Perceptron (MLP)
3. Materials
4. Experimentation and Results
Results Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hernandez-Contreras, D.; Peregrina-Barreto, H.; Rangel-Magdaleno, J.; Gonzalez-Bernal, J.A.; Altamirano-Robles, L. A quantitative index for classification of plantar thermal changes in the diabetic foot. Inf. Phys. Technol. 2017, 81, 242–249. [Google Scholar] [CrossRef]
- Yang, W.; Dall, T.M.; Tan, E.; Byrne, E.; Iacobucci, W.; Chakrabarti, R.; Loh, F.E. Diabetes diagnosis and management among insured adults across metropolitan areas in the US. Prev. Med. Rep. 2018, 10, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Acharya, U.R.; Bhat, S.; Koh, J.E.; Bhandary, S.V.; Adeli, H. A novel algorithm to detect glaucoma risk using texture and local configuration pattern features extracted from fundus images. Compt. Biol. Med. 2017, 88, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Raghavendra, U.; Bhandary, S.V.; Gudigar, A.; Acharya, U.R. Novel expert system for glaucoma identification using non-parametric spatial envelope energy spectrum with fundus images. Biocybern. Biomed. Eng. 2018, 38, 170–180. [Google Scholar] [CrossRef]
- Garduño-Ramón, M.A.; Vega-Mancilla, S.G.; Morales-Henández, L.A.; Osornio-Rios, R.A. Supportive noninvasive tool for the diagnosis of breast cancer using a thermographic camera as sensor. Sensors 2017, 17, 497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gogoi, U.R.; Bhowmik, M.K.; Bhattacharjee, D.; Ghosh, A.K. Singular value based characterization and analysis of thermal patches for early breast abnormality detection. Australas. Phys. Eng. Sci. Med. 2018, 41, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Valderas, M.T.; Bolea, J.; Laguna, P.; Bailón, R.; Vallverdú, M. Mutual information between heart rate variability and respiration for emotion characterization. Phys. Meas. 2019, 40, 084001. [Google Scholar] [CrossRef] [PubMed]
- delEtoile, J.; Adeli, H. Graph Theory and Brain Connectivity in Alzheimer’s Disease. Neuroscience 2017, 23, 616–626. [Google Scholar] [CrossRef]
- Khedher, L.; Illán, I.A.; Górriz, J.M.; Ramírez, J.; Brahim, A.; Meyer-Baese, A. Independent Component Analysis-Support Vector Machine-Based Computer-Aided Diagnosis System for Alzheimer’s with Visual Support. Int. J. Neural Syst. 2017, 27, 1650050. [Google Scholar] [CrossRef]
- Lopez-de-Ipina, K.; Martinez-de-Lizarduy, U.; Calvo, P.M.; Mekyska, J.; Beitia, B.; Barroso, N.; Ecay-Torres, M. Advances on automatic speech analysis for early detection of Alzheimer disease: A non-linear multi-task approach. Curr. Alzheimer Res. 2018, 15, 139–148. [Google Scholar] [CrossRef]
- Duraisamy, B.; Shanmugam, J.V.; Annamalai, J. Alzheimer disease detection from structural MR images using FCM based weighted probabilistic neural network. Brain Imaging Behav. 2018, 13, 1–24. [Google Scholar] [CrossRef]
- Amezquita-Sanchez, J.P.; Adeli, A.; Adeli, H. A new methodology for automated diagnosis of mild cognitive impairment (MCI) using magnetoencephalography (MEG). Behav. Brain Res. 2016, 305, 174–180. [Google Scholar] [CrossRef] [PubMed]
- López-Sanz, D.; Garcés, P.; Álvarez, B.; Delgado-Losada, M.L.; López-Higes, R.; Maestú, F. Network Disruption in the Preclinical Stages of Alzheimer’s Disease: From Subjective Cognitive Decline to Mild Cognitive Impairment. Int. J. Neural Syst. 2017, 27, 1750041. [Google Scholar] [CrossRef]
- Mammone, N.; Bonanno, L.; Salvo, S.D.; Marino, S.; Bramanti, P.; Bramanti, A.; Morabito, F.C. Permutation disalignment index as an indirect, EEG-based, measure of brain connectivity in MCI and AD patients. Int. J. Neural Syst. 2017, 27, 1750020. [Google Scholar] [CrossRef] [PubMed]
- Amezquita-Sanchez, J.P.; Mammone, N.; Morabito, F.C.; Marino, S.; Adeli, H. A novel methodology for automated differential diagnosis of mild cognitive impairment and the Alzheimer’s disease using EEG signals. J. Neurosci. Meth. 2019, 322, 88–95. [Google Scholar] [CrossRef]
- Oh, J.; Cho, D.; Park, J.; Na, S.H.; Kim, J.; Heo, J.; Shin, C.S.; Kim, J.-J.; Park, J.Y.; Lee, B. Prediction and early detection of delirium in the intensive care unit by using heart rate variability and machine learning. Phys. Meas. 2018, 39, 035004. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.K.; Cai, Q.; Yang, Y.X.; Dong, N.; Zhang, S.S. Visibility graph from adaptive optimal kernel time-frequency representation for classification of epileptiform EEG. Int. J. Neural Syst. 2017, 27, 1750005. [Google Scholar] [CrossRef] [PubMed]
- Symonds, J.D.; Zuberi, S.M.; Johnson, M.R. Advances in epilepsy gene discovery and implications for epilepsy diagnosis and treatment. Cur. Op. Neurol. 2017, 30, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Acharya, U.R.; Oh, S.L.; Hagiwara, Y.; Tan, J.H.; Adeli, H. Deep convolutional neural network for the automated detection and diagnosis of seizure using EEG signals. Comp. Biol. Med. 2018, 100, 270–278. [Google Scholar] [CrossRef]
- Atri, R.; Mohebbi, M. Obstructive sleep apnea detection using spectrum and bispectrum analysis of single-lead ECG signal. Phys. Meas. 2015, 36, 1963. [Google Scholar] [CrossRef]
- Jonmohamadi, Y.; Poudel, G.R.; Innes, C.C.; Jones, R.D. Microsleeps are Associated with Stage-2 Sleep Spindles from Hippocampal-Temporal Network. Int. J. Neural Syst. 2016, 26, 1650015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruder, J.C.; Dümpelmann, M.; Piza, D.L.; Mader, M.; Schulze-Bonhage, A.; Jacobs-Le Van, J. Physiological Ripples Associated with Sleep Spindles Differ in Waveform Morphology from Epileptic Ripples. Int. J. Neural Syst. 2017, 27, 1750011, (15 pages). [Google Scholar] [CrossRef] [PubMed]
- Karan, B.; Sahu, S.S.; Mahto, K. Parkinson disease prediction using intrinsic mode function based features from speech signal. Biocybern. Biomed. Eng. 2019, in press. [Google Scholar] [CrossRef]
- Nilashi, M.; Ibrahim, O.; Ahmadi, H.; Shahmoradi, L.; Farahmand, M. A hybrid intelligent system for the prediction of Parkinson’s Disease progression using machine learning techniques. Biocybern. Biomed. Eng. 2018, 38, 1–15. [Google Scholar] [CrossRef]
- Ahmadlou, M.; Adeli, H. Complexity of weighted graph: A new technique to investigate structural complexity of brain activities with applications to aging and autism. Neurosci. Lett. 2017, 650, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Akar, S.A.; Kara, S.; Latifoğlu, F.; Bilgiç, V. Analysis of the complexity measures in the EEG of schizophrenia patients. Int. J. Neural Syst. 2016, 26, 1650008. [Google Scholar] [CrossRef]
- Schmidt, M.; Schumann, A.; Müller, J.; Bär, K.-J.; Rose, G. ECG derived respiration: Comparison of time-domain approaches and application to altered breathing patterns of patients with schizophrenia. Phys. Meas. 2017, 38, 601. [Google Scholar] [CrossRef]
- Mammone, N.; Ieracitano, C.; Adeli, H.; Bramanti, A.; Morabito, F.C. Permutation Jaccard Distance-Based Hierarchical Clustering to Estimate EEG Network Density Modifications in MCI Subjects. IEEE Trans. Neural Netw. Learn. Syst. 2018, 29, 5122–5135. [Google Scholar] [CrossRef]
- Shafique, A.; Sayeed, M.; Tsakalis, K. Nonlinear Dynamical Systems with Chaos and Big Data: A Case Study of Epileptic Seizure Prediction and Control. In Guide to Big Data Applications. Studies in Big Data; Srinivasan, S., Ed.; Springer: Cham, Switzerland, 2018; Volume 26. [Google Scholar]
- Ebrahimzadeh, E.; Manuchehri, M.S.; Amoozegar, S.; Araabi, B.N.; Soltanian-Zadeh, H. A time local subset feature selection for prediction of sudden cardiac death from ECG signal. Med Biol. Eng. Comp. 2018, 56, 1253–1270. [Google Scholar] [CrossRef]
- Amezquita-Sanchez, J.P.; Valtierra-Rodriguez, M.; Adeli, H.; Perez-Ramirez, C.A. A Novel Wavelet Transform-Homogeneity Model for Sudden Cardiac Death Prediction Using ECG Signals. J. Med. Sys. 2018, 42, 176. [Google Scholar] [CrossRef]
- Myerburg, R.J.; Junttila, M.J. Sudden cardiac death caused by coronary heart disease. Circulation 2012, 125, 1043–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finocchiaro, G.; Papadakis, M.; Sharma, S.; Sheppard, M. Sudden Cardiac Death. Eur. Heart J. 2017, 38, 1280–1282. [Google Scholar] [CrossRef] [Green Version]
- Pagidipati, N.J.; Gaziano, T.A. Estimating deaths from cardiovascular disease: A review of global methodologies of mortality measurement. Circulation 2013, 127, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Myerburg, R.J. Cardiac arrest and sudden cardiac death. In Heart Disease, a Textbook of Cardiovascular Medicine; W.B. Saunders: Philadelphia, PA, USA, 1992; pp. 756–789. [Google Scholar]
- Murukesan, L.; Murugappan, M.; Iqbal, M.; Saravanan, K. Machine learning approach for sudden cardiac arrest prediction based on optimal heart rate variability features. J. Med. Imaging Health Inf. 2014, 4, 521–532. [Google Scholar] [CrossRef]
- Murugappan, M.; Murukesan, L.; Omar, I.; Khatun, S.; Murugappan, S. Time Domain Features Based Sudden Cardiac Arrest Prediction Using Machine Learning Algorithms. J. Med. Imaging Health Inf. 2015, 5, 1267–1271. [Google Scholar] [CrossRef]
- Acharya, U.R.; Fujita, H.; Sudarshan, V.K.; Sree, V.S.; Eugene, L.W.J.; Ghista, D.N.; San Tan, R. An integrated index for detection of sudden cardiac death using discrete wavelet transform and nonlinear features. Knowl. Based Sys. 2015, 83, 149–158. [Google Scholar] [CrossRef]
- Fujita, H.; Acharya, U.R.; Sudarshan, V.K.; Ghista, D.N.; Sree, S.V.; Eugene, L.W.J.; Koh, J.E. Sudden cardiac death (SCD) prediction based on nonlinear heart rate variability features and SCD index. Appl. Soft Comp. 2016, 43, 510–519. [Google Scholar] [CrossRef]
- Ebrahimzadeh, E.; Pooyan, M.; Bijar, A. A novel approach to predict sudden cardiac death (SCD) using nonlinear and time-frequency analyses from HRV signals. PLoS ONE 2014, 9, e81896. [Google Scholar] [CrossRef] [PubMed]
- MIT/BIH-NSR. Database. Available online: https://www.physionet.org/physiobank/database/nsrdb/ (accessed on 1 September 2019).
- MIT/BIH-SCDH. Available online: https://physionet.org/physiobank/database/sddb/#clinical-information/databased (accessed on 1 September 2019).
- Katz, M.J. Fractals and the analysis of waveforms. Comp. Biol. Med. 1988, 18, 145–156. [Google Scholar] [CrossRef]
- Higuchi, T. Approach to an irregular time series on the basis of the fractal theory. Phys. D 1988, 31, 277–283. [Google Scholar] [CrossRef]
- Wang, B.Y. Detection of structural damage using fractal dimension technique. J. Vib. Shock 2005, 24, 87–88. [Google Scholar]
- Shannon, C.E. A mathematical theory of communication. Bell Sys. Tech. J. 1948, 27, 379–423. [Google Scholar] [CrossRef] [Green Version]
- Bandt, C.; Pompe, B. Permutation entropy: A natural complexity measure for time series. Phys. Rev. Lett. 2002, 88, 174102. [Google Scholar] [CrossRef] [PubMed]
- Acharya, U.R.; Suri, S.J.; Spaan, J.A.E.; Krishnan, S.M. (Eds.) Advances in Cardiac Signal Processing; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Lin, C.-H.; Du, Y.-C. Fractal QRS-complexes pattern recognition for imperative cardiac arrhythmias. Digital Signal. Process. 2010, 20, 1274–1285. [Google Scholar] [CrossRef]
- Billeci, L.; Costi, M.; Lombardi, D.; Chiarugi, F.; Varanini, M. Automatic Detection of Atrial Fibrillation and Other Arrhythmias in ECG Recordings Acquired by a Smartphone Device. Electronics 2018, 7, 199. [Google Scholar] [CrossRef] [Green Version]
- Huang, N.E.; Shen, Z.; Long, S.R.; Wu, M.C.; Shih, H.H.; Zheng, Q.; Yen, N.C.; Tung, C.C.; Liu, H.H. The empirical mode decomposition and the Hilbert spectrum for nonlinear and non-stationary time series analysis. Proc. R. Soc. Lond. A Math. Phys. Eng. Sci. 1998, 454, 903–995. [Google Scholar] [CrossRef]
- Subasi, A. Practical Guide for Biomedical Signal. Analysis Using Machine Learning Techniques; Academic Press: Cambridge, MA, USA, 2019. [Google Scholar]
- Ghritlahre, H.K.; Prasad, R.K. Investigation of thermal performance of unidirectional flow porous bed solar air heater using MLP, GRNN, and RBF models of ANN technique. Sci. Eng. Prog. 2018, 6, 226–235. [Google Scholar] [CrossRef]
- Lopez-Ramirez, M.; Ledesma-Carrillo, L.; Cabal-Yepez, E.; Rodriguez-Donate, C.; Miranda-Vidales, H.; Garcia-Perez, A. EMD-Based Feature Extraction for Power Quality Disturbance Classification Using Moments. Energies 2016, 9, 565. [Google Scholar] [CrossRef] [Green Version]
- Murtagh, F. Multilayer perceptrons for classification and regression. Neurocomputing 1992, 2, 183–197. [Google Scholar] [CrossRef]
- Kopsinis, Y.; McLaughlin, S. Development of EMD-Based Denoising Methods Inspired by Wavelet Thresholding. IEEE Trans. Signal. Process. 2009, 57, 1351–1362. [Google Scholar] [CrossRef]
- Myerburg, R.J.; Interian, A., Jr.; Mitrani, R.M.; Kessler, K.M.; Castellanos, A. Frequency of Sudden Cardiac Death and Profiles of Risk. Am. J. Cardiol. 1997, 80, 10F–19F. [Google Scholar] [CrossRef]
- Chugh, S.S.; Reinier, K.; Teodorescu, C.; Evanado, A.; Kehr, E.; Al Samara, M.; Mariani, R.; Gunson, K.; Jui, J. Epidemiology of Sudden Cardiac Death: Clinical and Research Implications. Progr. Cardiovasc. Dis. 2008, 51, 213–228. [Google Scholar] [CrossRef] [Green Version]
- Kaltman, J.R.; Thompson, P.D.; Lantos, J.; Berul, C.I.; Botkin, J.; Cohen, J.T.; Cook, N.R.; Corrado, D.; Drezner, J.; Frick, K.D.; et al. Screening for Sudden Cardiac Death in the Young. Circulation 2011, 123, 1911–1918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajendra Acharya, U.; Joseph, K.P.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Compt. 2006, 44, 1031–1051. [Google Scholar] [CrossRef] [PubMed]
- Shen, T.W.; Shen, H.P.; Lin, C.; Ou, Y. Detection and prediction of Sudden Cardiac Death (SCD) for personal healthcare. In Proceedings of the 29th Annual International Conference of the IEEE, Buenos Aires, Argentina, 22–26 August 2007; pp. 2575–2578. [Google Scholar]
- Ebrahimzadeh, E.; Pooyan, M. Early detection of sudden cardiac death by using classical linear techniques and time-frequency methods on electrocardiogram signals. J. Biomed. Sci. Eng. 2011, 4, 699–706. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Group | Subjects (Sex) | Age |
|---|---|---|---|
| NSR | Normal | 18 (13 female) | 35 ± 15 |
| SCDH | SCD | 23 (8 female) | 49.5 ± 32.5 |
| Normal | SCD | ||||
|---|---|---|---|---|---|
| Fractal | μ ± σ | Minute | Fractal | μ ± σ | p-Value |
| HI | 1.4061 ± 0.0892 | 25 | HI | 1.1875 ± 0.1077 | 4.71 × 10−07 |
| PEI | 1.0793 ± 0.0143 | PEI | 1.0505 ± 0.0126 | 1.25 × 10−06 | |
| 24 | HI | 1.2055 ± 0.1231 | 3.77 × 10−07 | ||
| PEI | 1.0556 ± 0.0138 | 4.42 × 10−05 | |||
| 23 | HI | 1.2014 ± 0.1187 | 1.71 × 10−07 | ||
| PEI | 1.0533 ± 0.0128 | 7.37 × 10−06 | |||
| 22 | HI | 1.2050 ± 0.1082 | 2.16 × 10−07 | ||
| PEI | 1.0528 ± 0.0113 | 2.28 × 10−06 | |||
| 21 | HI | 1.1948 ± 0.1051 | 1.02 × 10−06 | ||
| PEI | 1.0517 ± 0.0110 | 1.02 × 10−06 | |||
| 20 | HI | 1.1885 ± 0.1038 | 2.31 × 10−08 | ||
| PEI | 1.0539 ± 0.0119 | 6.28 × 10−06 | |||
| 19 | HI | 1.1829 ± 0.0874 | 8.24 × 10−08 | ||
| PEI | 1.0498 ± 0.0114 | 4.11 × 10−07 | |||
| 18 | HI | 1.1943 ± 0.1167 | 5.04 × 10−06 | ||
| PEI | 1.0507 ± 0.0191 | 4.19 × 10−05 | |||
| 17 | HI | 1.1915 ± 0.1065 | 1.50 × 10−06 | ||
| PEI | 1.0507 ± 0.0163 | 1.09 × 10−05 | |||
| 16 | HI | 1.1902 ± 0.1173 | 8.04 × 10−07 | ||
| PEI | 1.0521 ± 0.0166 | 2.51 × 10−05 | |||
| 15 | HI | 1.1925 ± 0.1270 | 6.35 × 10−07 | ||
| PEI | 1.0527 ± 0.0136 | 7.55 × 10−06 | |||
| 14 | HI | 1.2034 ± 0.1191 | 6.55 × 10−06 | ||
| PEI | 1.0511 ± 0.0151 | 7.00 × 10−06 | |||
| 13 | HI | 1.2160 ± 0.1026 | 3.07 × 10−05 | ||
| PEI | 1.0550 ± 0.0147 | 4.98 × 10−05 | |||
| 12 | HI | 1.2165 ± 0.1071 | 1.54 × 10−05 | ||
| PEI | 1.0544 ± 0.0146 | 3.42 × 10−05 | |||
| 11 | HI | 1.2086 ± 0.1126 | 3.37 × 10−06 | ||
| PEI | 1.0516 ± 0.0165 | 1.92 × 10−05 | |||
| 10 | HI | 1.2160 ± 0.1241 | 1.42 × 10−05 | ||
| PEI | 1.0531 ±0.0172 | 5.66 × 10−05 | |||
| 9 | HI | 1.1960 ± 0.0905 | 1.85 × 10−07 | ||
| PEI | 1.0527 ± 0.0125 | 4.16 × 10−06 | |||
| 8 | HI | 1.2052 ± 0.0742 | 2.01 × 10−06 | ||
| PEI | 1.0549 ± 0.0180 | 8.71 × 10−05 | |||
| 7 | HI | 1.2114 ± 0.0923 | 3.75 × 10−06 | ||
| PEI | 1.0557 ± 0.0164 | 8.92 × 10−05 | |||
| 6 | HI | 1.2039 ± 0.0811 | 2.66 × 10−06 | ||
| PEI | 1.0524 ± 0.0156 | 1.88 × 10−05 | |||
| 5 | HI | 1.2076 ± 0.0819 | 8.69 × 10−06 | ||
| PEI | 1.0541 ± 0.0184 | 1.55 × 10−04 | |||
| 4 | HI | 1.2144 ± 0.0861 | 2.07 × 10−05 | ||
| PEI | 1.0547 ± 0.0172 | 1.21 × 10−04 | |||
| 3 | HI | 1.2052 ± 0.1038 | 2.85 × 10−06 | ||
| PEI | 1.0546 ± 0.0184 | 9.37 × 10−05 | |||
| 2 | HI | 1.2192 ± 0.1194 | 2.23 × 10−05 | ||
| PEI | 1.0553 ± 0.0197 | 9.24 × 10−04 | |||
| 1 | HI | 1.2019 ± 0.1108 | 2.87 × 10−06 | ||
| PEI | 1.0530 ± 0.0168 | 4.29 × 10−05 | |||
| Minute | Accuracy |
|---|---|
| 1 | 90% |
| 2 | 100% |
| 3 | 90% |
| 4 | 100% |
| 5 | 90% |
| 6 | 100% |
| 7 | 90% |
| 8 | 100% |
| 9 | 100% |
| 10 | 90% |
| 11 | 90% |
| 12 | 90% |
| 13 | 100% |
| 14 | 90% |
| 15 | 100% |
| 16 | 90% |
| 17 | 90% |
| 18 | 100% |
| 19 | 90% |
| 20 | 100% |
| 21 | 100% |
| 22 | 90% |
| 23 | 90% |
| 24 | 100% |
| 25 | 100% |
| Author | Signal | Methodology | Prediction Time (Accuracy) |
|---|---|---|---|
| Shen et al., (2007) [61] | ECG |
| 2 min (67.44%) |
| Ebrahimzadeh and Pooyan (2011) [62] | HRV |
| 4 min (83.96%) |
| Ebrahimzadeh et al., (2014) | HRV |
| 1 min (99.16%) |
| Acharya et al., (2015) | ECG |
| 4 min (92.11%) |
| Fujita et al., (2016) | HRV |
| 4 min (94.7%) |
| Amezquita-Sanchez et al., (2018) | ECG |
| 20 min (95.8%) |
| This work | ECG |
| 25 min (94%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vargas-Lopez, O.; Amezquita-Sanchez, J.P.; De-Santiago-Perez, J.J.; Rivera-Guillen, J.R.; Valtierra-Rodriguez, M.; Toledano-Ayala, M.; Perez-Ramirez, C.A. A New Methodology Based on EMD and Nonlinear Measurements for Sudden Cardiac Death Detection. Sensors 2020, 20, 9. https://doi.org/10.3390/s20010009
Vargas-Lopez O, Amezquita-Sanchez JP, De-Santiago-Perez JJ, Rivera-Guillen JR, Valtierra-Rodriguez M, Toledano-Ayala M, Perez-Ramirez CA. A New Methodology Based on EMD and Nonlinear Measurements for Sudden Cardiac Death Detection. Sensors. 2020; 20(1):9. https://doi.org/10.3390/s20010009
Chicago/Turabian StyleVargas-Lopez, Olivia, Juan P. Amezquita-Sanchez, J. Jesus De-Santiago-Perez, Jesus R. Rivera-Guillen, Martin Valtierra-Rodriguez, Manuel Toledano-Ayala, and Carlos A. Perez-Ramirez. 2020. "A New Methodology Based on EMD and Nonlinear Measurements for Sudden Cardiac Death Detection" Sensors 20, no. 1: 9. https://doi.org/10.3390/s20010009