
An ESR1-Related Gene Signature Identifies Head and Neck Squamous Cell Carcinoma with Imputed Susceptibility to Endocrine Therapy


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. ESR1-Related Gene Set in the TCGA-HNSC Cohort
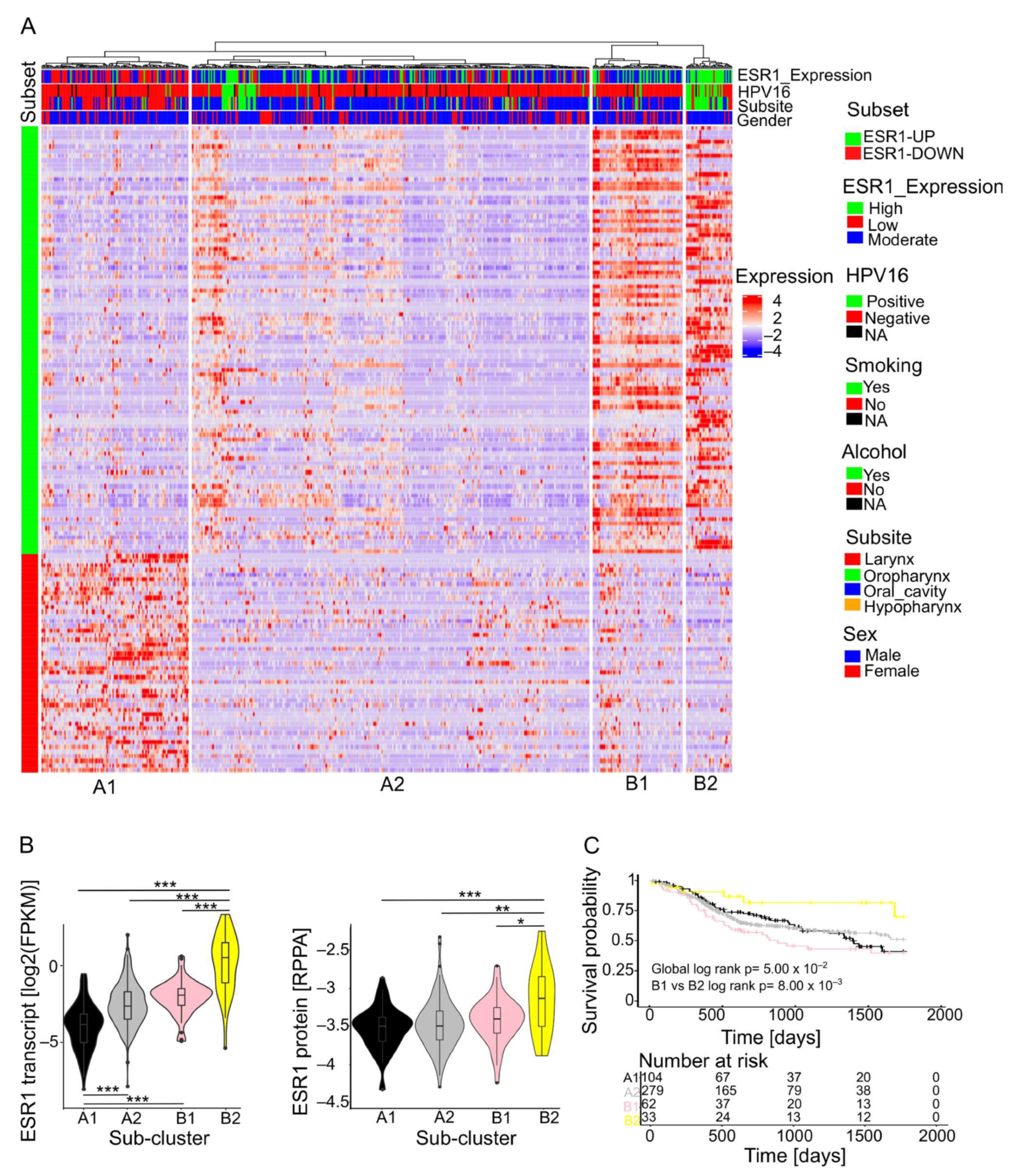
2.2. Stratification of HNSCC Subgroups Based on the ESR1-Related 139-Gene Set
2.3. Establishment of a Prognostic Risk Model with TCGA-HNSC as a Training Cohort
2.4. Validation of the Risk Model in an Independent HNSCC Cohort and Other Solid Tumors from TCGA
2.5. In Silico Drug Response Prediction
3. Discussion
4. Materials and Methods
4.1. Cohorts
4.2. Differential Gene Expression
4.3. Unsupervised Hierarchical Clustering
4.4. Cross-Tabulation Analysis
4.5. GSVA Analysis
4.6. Survival Analysis
4.7. Risk Model
4.8. In Silico Drug Response Prediction
4.9. Data Visualization
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Mann, D.; Sinha, U.K.; Kokot, N.C. The molecular mechanisms of increased radiosensitivity of HPV-positive oropharyngeal squamous cell carcinoma (OPSCC): An extensive review. J. Otolaryngol. -Head Neck Surg. 2018, 47, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.Q. Head and neck cancer. New Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Machiels, J.P.; Leemans, C.R.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef] [PubMed]
- De Felice, F.; Tombolini, V.; de Vincentiis, M.; Magliulo, G.; Greco, A.; Valentini, V.; Polimeni, A. Multidisciplinary team in head and neck cancer: A management model. Med. Oncol. 2019, 36, 2. [Google Scholar] [CrossRef]
- Koenigs, M.B.; Lefranc-Torres, A.; Bonilla-Velez, J.; Patel, K.B.; Hayes, D.N.; Glomski, K.; Busse, P.M.; Chan, A.W.; Clark, J.R.; Deschler, D.G.; et al. Association of estrogen receptor alpha expression with survival in oropharyngeal cancer following chemoradiation therapy. JNCI J. Natl. Cancer Inst. 2019, 111, 933–942. [Google Scholar] [CrossRef]
- Schrank, T.P.; Kothari, A.; Weir, W.H.; Stepp, W.H.; Rehmani, H.; Liu, X.; Wang, X.; Sewell, A.; Li, X.; Tasoulas, J.; et al. Noncanonical HPV carcinogenesis drives radiosensitization of head and neck tumors. Proc. Natl. Acad. Sci. USA 2023, 120, e2216532120. [Google Scholar] [CrossRef]
- Sommer, S.; Fuqua, S.A. Estrogen Receptor and Breast Cancer. In Seminars in Cancer Biology; Elsevier: Amsterdam, The Netherlands, 2001. [Google Scholar]
- Early Breast Cancer Trialists’ Collaborative Group. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: Patient-level meta-analysis of randomised trials. Lancet 2011, 378, 771–784. [Google Scholar] [CrossRef]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved survival of patients with human papillomavirus–positive head and neck squamous cell carcinoma in a prospective clinical trial. J. Natl. Cancer Inst. 2008, 100, 261–269. [Google Scholar] [CrossRef]
- Chung, S.-H.; Lambert, P.F. Prevention and treatment of cervical cancer in mice using estrogen receptor antagonists. Proc. Natl. Acad. Sci. USA 2009, 106, 19467–19472. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. New Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Egloff, A.M.; Rothstein, M.E.; Seethala, R.; Siegfried, J.M.; Grandis, J.R.; Stabile, L.P. Cross-talk between estrogen receptor and epidermal growth factor receptor in head and neck squamous cell carcinoma. Clin. Cancer Res. 2009, 15, 6529–6540. [Google Scholar] [CrossRef] [PubMed]
- Grünow, J.; Rong, C.; Hischmann, J.; Zaoui, K.; Flechtenmacher, C.; Weber, K.-J.; Plinkert, P.; Hess, J. Regulation of submaxillary gland androgen-regulated protein 3A via estrogen receptor 2 in radioresistant head and neck squamous cell carcinoma cells. J. Exp. Clin. Cancer Res. 2017, 36, 25. [Google Scholar] [CrossRef] [PubMed]
- Selli, C.; Dixon, J.M.; Sims, A.H. Accurate prediction of response to endocrine therapy in breast cancer patients: Current and future biomarkers. Breast Cancer Res. 2016, 18, 118. [Google Scholar] [CrossRef] [PubMed]
- Law, C.W.; Chen, Y.; Shi, W.; Smyth, G.K. Voom: Precision weights unlock linear model analysis tools for RNA-seq read counts. Genome Biol. 2014, 15, R29. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.D.; McCarthy, D.J.; Smyth, G.K. EdgeR: A Bioconductor package for differential expression analysis of digital gene expression data. Bioinformatics 2009, 26, 139–140. [Google Scholar] [CrossRef]
- Gu, Z.; Eils, R.; Schlesner, M. Complex heatmaps reveal patterns and correlations in multidimensional genomic data. Bioinformatics 2016, 32, 2847–2849. [Google Scholar] [CrossRef] [PubMed]
- Hänzelmann, S.; Castelo, R.; Guinney, J. GSVA: Gene set variation analysis for microarray and RNA-seq data. BMC Bioinform. 2013, 14, 7. [Google Scholar] [CrossRef]
- Kassambara, A.; Kosinski, M.; Biecek, P.; Fabian, S. Package ‘Survminer’. Drawing Survival Curves Using ‘ggplot2’, R package version 03 1; The R Project for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Borgan, Ø. Modeling Survival Data: Extending the Cox Model; Therneau, T.M., Grambsch, P.M., Eds.; Springer: New York, NY, USA, 2000; 350p. [Google Scholar]
- Friedman, J.; Hastie, T.; Tibshirani, R.; Narasimhan, B.; Tay, K.; Simon, N.; Qian, J. Package ‘glmnet’. J. Stat. Softw. 2021, 33, 595. [Google Scholar]
- Hothorn, T.; Hothorn, M.T. The maxstat Package; Version 0.7-25; The R Project for Statistical Computing: Vienna, Austria, 2007. [Google Scholar]
- Maeser, D.; Gruener, R.F.; Huang, R.S. OncoPredict: An R package for predicting in vivo or cancer patient drug response and biomarkers from cell line screening data. Brief. Bioinform. 2021, 22, bbab260. [Google Scholar] [CrossRef]
- Wickham, H. ggplot2. Wiley Interdiscip. Rev. Comput. Stat. 2011, 3, 180–185. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almouhanna, F.; Hess, J. An ESR1-Related Gene Signature Identifies Head and Neck Squamous Cell Carcinoma with Imputed Susceptibility to Endocrine Therapy. Int. J. Mol. Sci. 2024, 25, 1244. https://doi.org/10.3390/ijms25021244
Almouhanna F, Hess J. An ESR1-Related Gene Signature Identifies Head and Neck Squamous Cell Carcinoma with Imputed Susceptibility to Endocrine Therapy. International Journal of Molecular Sciences. 2024; 25(2):1244. https://doi.org/10.3390/ijms25021244
Chicago/Turabian StyleAlmouhanna, Firas, and Jochen Hess. 2024. "An ESR1-Related Gene Signature Identifies Head and Neck Squamous Cell Carcinoma with Imputed Susceptibility to Endocrine Therapy" International Journal of Molecular Sciences 25, no. 2: 1244. https://doi.org/10.3390/ijms25021244