

Recapitulating the Key Advances in the Diagnosis and Prognosis of High-Grade Gliomas: Second Half of 2021 Update

Abstract
:1. Introduction
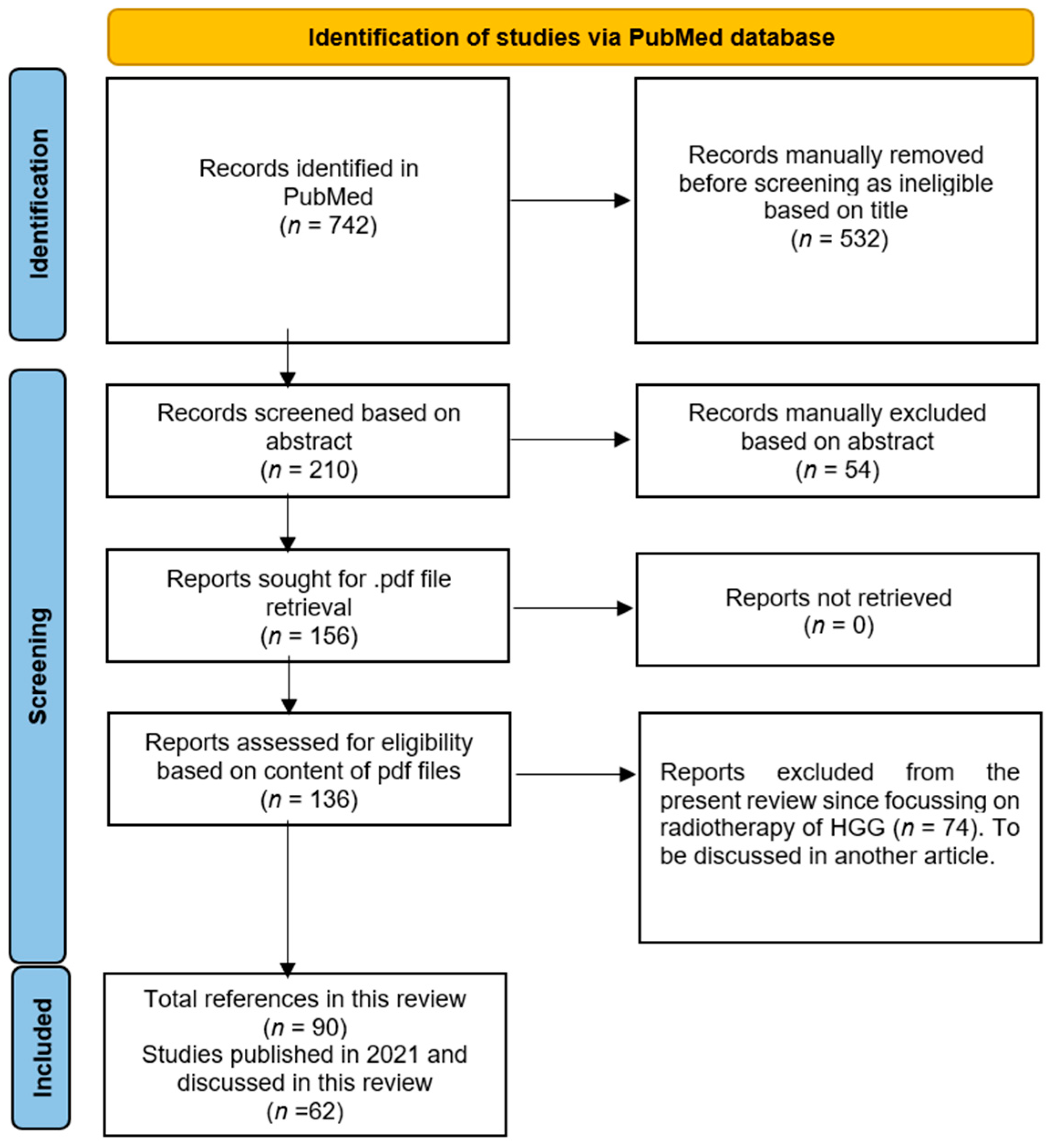
2. Methods
3. Advances in Diagnosis
3.1. The 2021 WHO Classification of Tumors of the CNS

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Major Finding | Experimental System | LE 1 | Ref |
|---|---|---|---|
| The 2021 WHO Classification of CNS Tumors | |||
| The fifth edition of the world health organization (WHO) classification of central nervous system (CNS) tumors in 2021 introduced advancements in the role of molecular diagnostics in CNS tumor classification. At the same time, it remained wedded to other established approaches to tumor diagnosis, such as histology and immunohistochemistry (IHC), paving the way for integrated approaches to both CNS tumor nomenclature and grading. | New CNS tumor types and subtypes were classified, and some were based on technological advances such as next-generation sequencing (NGS) and DNA methylome profiling. Over 40 tumor types and subtypes were eventually defined. | IV | [9] |
| Advances in imaging diagnosis of HGG | |||
| Advances in MRI | |||
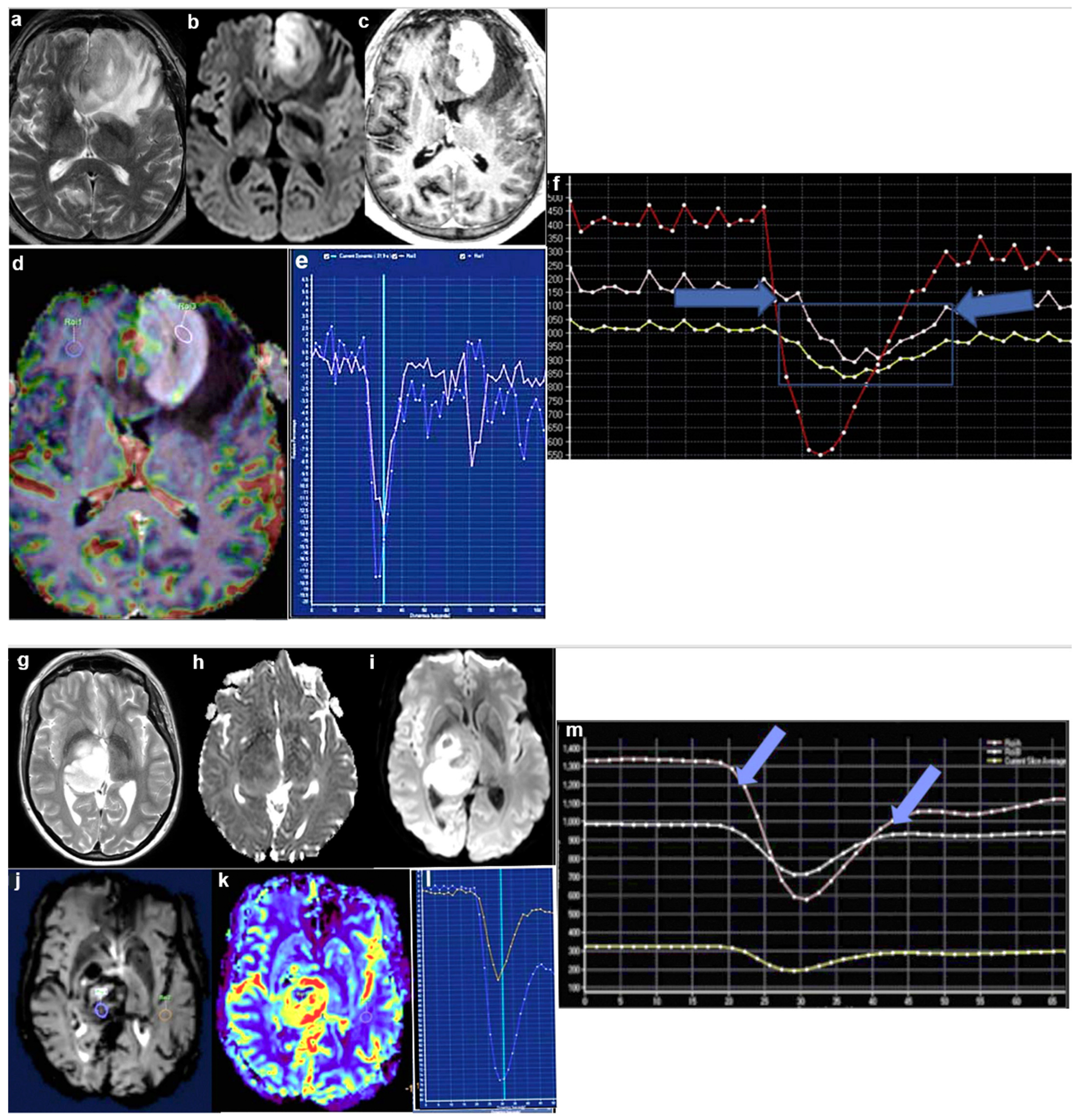
| The relative cerebral blood volume (rCBV) and percentage signal recovery (PSR) ratio are different in HGG and primary central nervous system lymphoma (PCNSL) at both the group level and subject level. Incorporation of perfusion in routine magnetic resonance imaging (MRI) of contrast-enhancing lesions may have an impact on patient management. | Patients who underwent diagnostic imaging for a primary brain lesion were retrospectively examined. Fifteen immunocompetent patients with PCNSL containing a total of 15 lesions, and 11 patients with high-grade glioma (HGG), containing a total of 11 lesions, were identified and analyzed. | VIII | [15] |
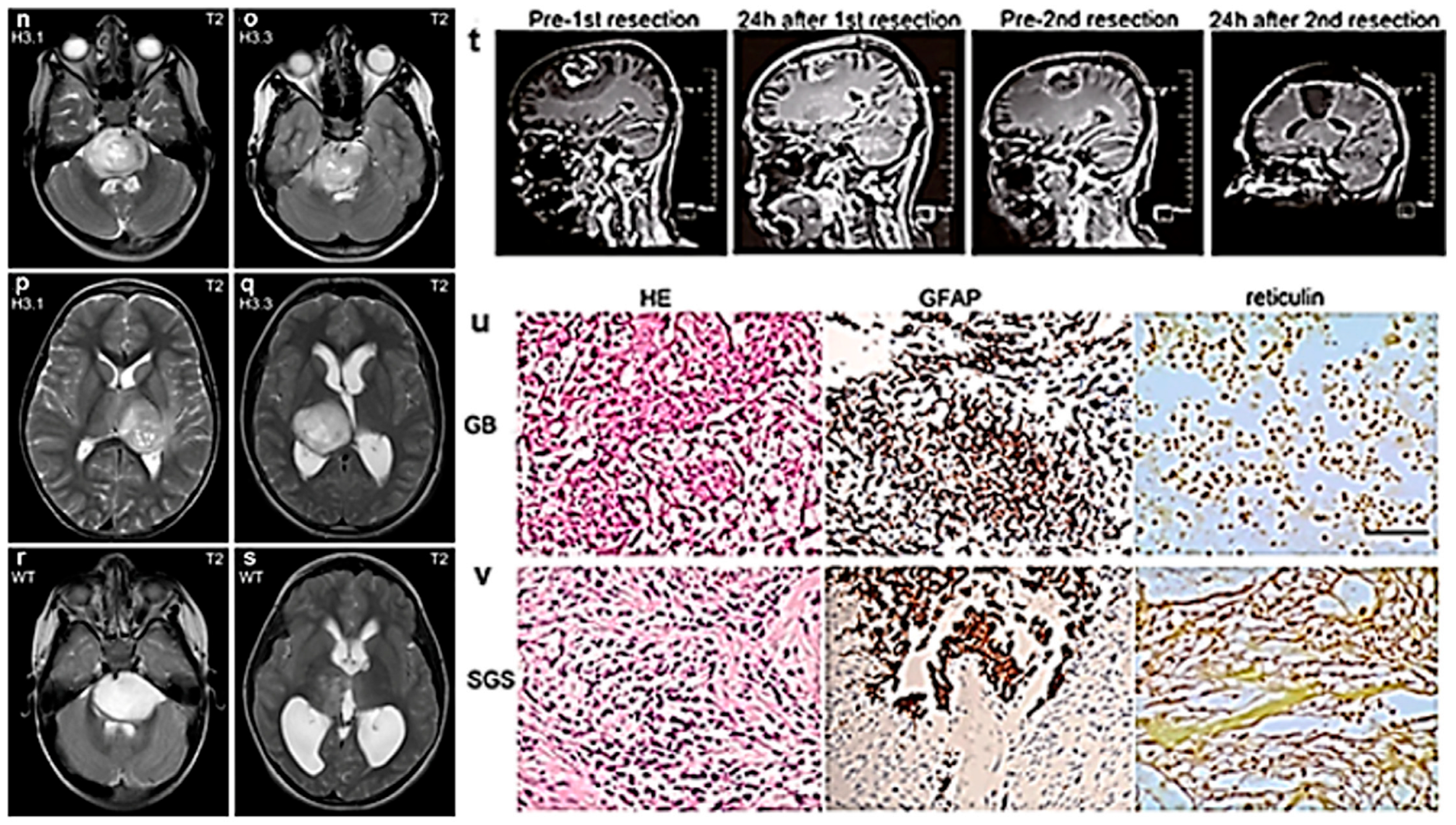
| Detailed MRI data on h3k27m mutant diffuse midline glioma (DMG) pediatric patients were provided. | A total of 85 pediatric patients with DMG were retrieved from registries. Histopathological and molecular genetic data, including h3k27 mutation status, as well as MRI studies of diagnosis, were compared. | VIII | [16] |
| Secondary gliosarcoma (SGS) components likely have a monoclonal origin, and the clone possessing mutations in NF1 and TP53 was likely the founding clone in a case of SGS. | Case report: Somatic mutation profiles in a glioblastoma (GB), and then an SGS patient, were examined using whole-genome sequencing and deep-whole-exome sequencing. Mutation signatures were characterized to investigate the relationship between chemo-RT and SGS pathogenesis. | VIII | [17] |
| Combined analysis of susceptibility-weighted imaging (SWI) and diffusion-weighted imaging (DWI) could differentiate atypical GB from PCNSL and distinguish major genomic subtypes between these tumors. | Thirty-one immuno-competent patients with PCNSL stratified by BCL2 and MYC rearrangement, and fifty-seven patients with atypical GB (no visible necrosis) grouped according to idh1 mutation status underwent 3.0-T MRI before treatment in this retrospective study. | VIII | [18] |
| A transfer learning approach suggested that convolutional neural networks may provide accurate diagnostic information to assist radiologists in distinguishing PCNSL from GB. | Preoperative brain tumor MRIs were retrospectively analyzed among 320 patients with either GB or PCNSL from two academic institutions. | VIII | [19] |
| A machine learning classifier based on the analysis of longitudinal perfusion time points and combined structural and perfusion features may enhance the classification outcome. | Study participants were separated into two groups: group I had a single dynamic susceptibility contrast (DSC) time point, and group II had longitudinal DSC time points. Structural MRI and DSC-MRI scans were retrospectively analyzed. | VIII | [20] |
| DSC–MRI radio genomics in HGG may allow the increased predictive performance of idh mutation status. | A multicenter study featuring an exploratory set for radiomics model development and external validation using two independent cohorts. | VIII | [21] |
| AC/DC coils might be used synergistically with optimized acquisition schemes to improve metabolic imaging in HGG patients. This methodology may be applicable to other neurological disorders. | Four HGG patients and five volunteers that underwent 3.0 T MRI were analyzed. | VIII | [22] |
| Diffusion variance decomposition (DIVIDE) imaging is a promising technique for glioma characterization and diagnosis. | Ninety-three participants with suspected glioma according to preliminary CT and MRI results were analyzed. | VIII | [23] |
| Training a classifier to predict both idh-mutation and 1p/19q-codeletion status outperformed a tiered structure that first predicted idh-mutation, then 1p/19q-codeletion. Including apparent diffusion coefficient (ADC), a surrogate marker of cellularity, more accurately detected differences between subgroups. | Three hundred and eighty-four patients with newly diagnosed gliomas who underwent preoperative MRI with standard anatomical and DWI and one hundred and forty-seven patients from an external cohort with anatomical imaging were analyzed. | VIII | [24] |
| Amide proton transfer (APT) imaging can be used to differentiate HGG from low grade gliomas (LGG) in pediatric patients and provide added value beyond quantitative relaxation times. | In this prospective study, APT imaging and relaxation time mapping were performed in 203 pediatric patients suspected of having gliomas. | VII | [25] |
| Brainstem glioma (BSG) patients with h3k27m mutant had higher max APT values than the wild-type patients did. APT-derived radiomics could accurately predict a h3k27m mutant status in BSG patients. | Eighty-one BSG patients with APT imaging at 3.0-T MRI and known H3K27M status were retrospectively studied. | VIII | [26] |
| h3.1k27m-mutated tumors have higher ADC and lower perfusion values than h3.3k27m ones do, without direct correlation with microvascular or nuclear density. | Twenty-seven treatment-naïve children with histopathologically confirmed h3k27m mutant diffuse intrinsic pontine glioma (DIPG) were prospectively analyzed. | VIII | [27] |
| Dynamic nuclear polarization (DNP)-MRI might represent a useful technique with which to evaluate HGG metabolism before and after RT in the clinical setting. | DNP-MRI chemical shift imaging with hyperpolarized [1−13C] pyruvate was conducted to evaluate the metabolic change in glycolytic profiles after radiation of two glioma initiating cell (GIC)-driven (GBMJ1 and NSC11) and an adherent human HGG cell line (U251) in an orthotopic xenograft mouse model. | VIII | [28] |
| Sequential administration of 5-aminolevulinic acid (ALA) and iron supplements increases the iron deposition in HGG cells, enabling clinical 3.0-T MRI to detect HGG using R2′ or quantitative susceptibility mapping (qSM). | Intra-cellular iron accumulation in HGG cells treated with ALA and/or ferric ammonium citrate (FAC) was measured. Cell phantoms containing HGG cells and Wistar rats bearing the C6 HGG were imaged using a 3.0-T MRI scanner after sequential administration of ALA and FAC. Relaxivity and qSM analysis were performed on the images. | VIII | [29] |
| Advances in PET | |||
| Although L1 amino acid transporter (LAT1) is reported to mediate the uptake of O-(2-18F-fluoroethyl)-L-tyrosine (18F-FET) into tumour cells, the levels of LAT1 expression do not correlate with the levels of 18F-FET uptake in idh mutant HGG. In particular, the lack of tracer uptake in 18F-FET-negative HGG cannot be explained by a reduced LAT1 expression. | Forty newly diagnosed idh mutant HGG without 1p/19q codeletion were evaluated: (n = 20 18F-FET-negative (tumor-to-background ratio (TBR) < 1.6) and n = 20 18F-FET-positive (TBR > 1.6) HGG. | VIII | [30] |
| Residual 3,4-dihydroxy-6-18F-fluoro-L-phenylalanine (18FDOPA) hypermetabolic burden predicted overall survival (OS) for isocitrate dehydrogenase (IDH) wild-type gliomas, regardless of the tumor grade. | Thirty-four patients with treatment-naïve IDH wild-type gliomas (WHO grade II 6, III 15, and IV 13) were retrospectively included. | VIII | [31] |
| Radiomics based on time-to-peak (TTP) images extracted from dynamic 18F-FET PET can predict the ptert-mutation status of IDH wild-type diffuse astrocytic HGG preoperatively. | A total of 159 patients with newly diagnosed IDH wild-type diffuse astrocytic HGG and dynamic 18F-FET PET prior to surgical intervention were enrolled and randomly divided into training (n = 112) and testing (n = 47) cohorts. | VII | [32] |
| Tumor isocontour T-maps and the combined analysis of cerebral blood flow (CBF) and 18F DOPA-PET uptake resulted in diagnosis for differentiating between progression and pseudo-progression in treated gliomas. The sensitivity is particularly high for GBs. | Fifty-eight patients with treated unilateral gliomas who were included in the study constituted groups with ten (17.2%) LGG and forty-eight (82.8%) HGG patients. | VIII | [33] |
| In lymphomatosis and gliomatosis, fluorodeoxyglucose (FDG) accumulates in only part of the lesion. FDG is thus less suitable than MET is for depicting those lesions. | Ten patients had lymphomatosis or gliomatosis of the brain. The underlying pathologies included intravascular lymphoma (n = 1), lymphomatosis (n = 3), and gliomatosis (n = 6). | VIII | [34] |
| A possible step forward in the clinical translation of cancer vaccination as a potential HGG therapy, as well as having the benefits of monitoring efficacy of these treatments using immunoPET imaging of T cell activation. | A subcutaneous vaccination approach with CpG oligodeoxynucleotide, OX40 mAb, and tumor lysate at a remote site in a murine orthotopic HGG model was developed to induce the activation of T cells distantly, while monitoring their distribution in stimulated lymphoid organs with respect to the observed therapeutic effects. | VIII | [35] |
| Advances in non-imaging diagnosis of HGG | |||
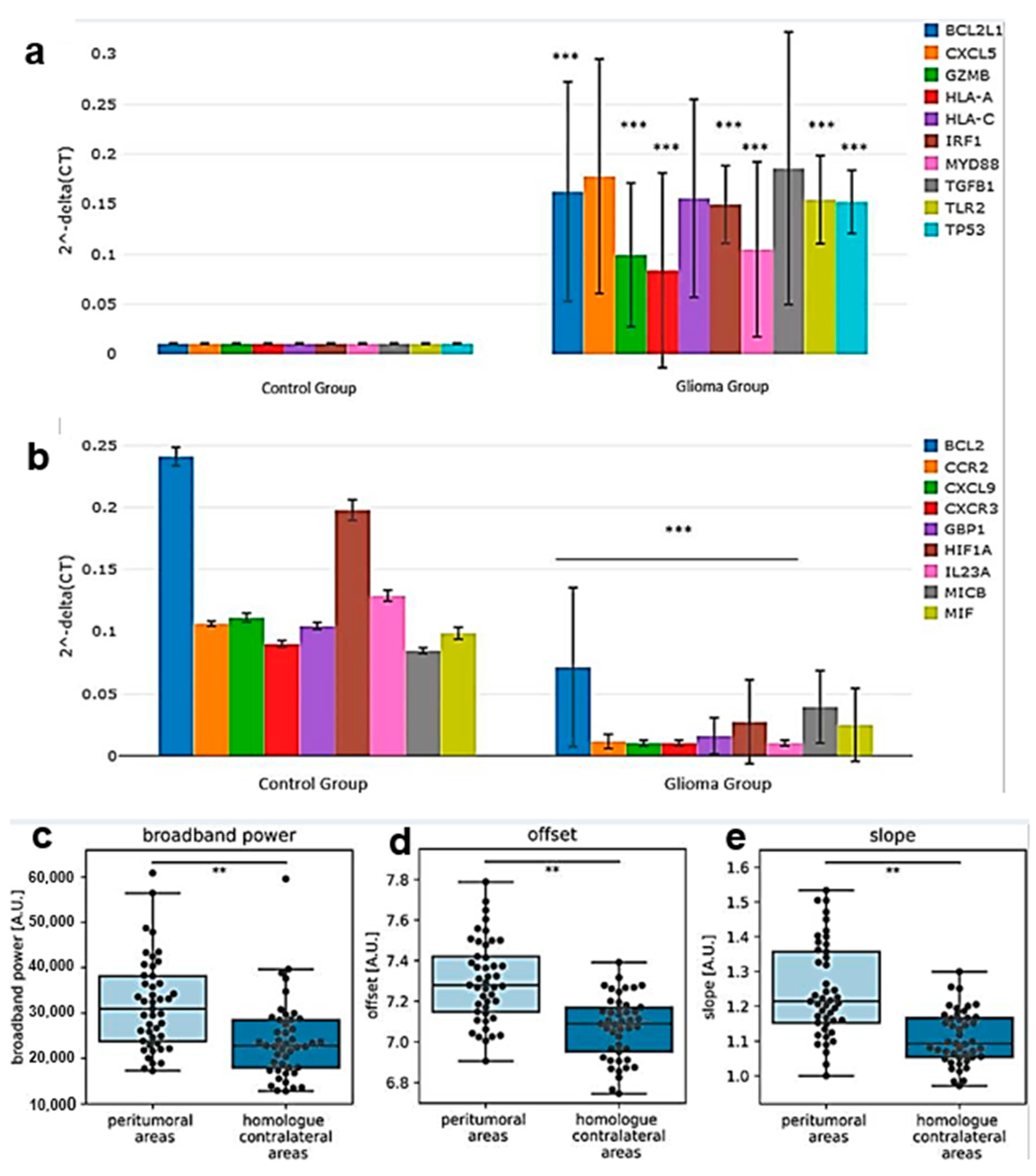
| Significant differential expression of genes involved in cancer inflammation and immunity crosstalk were found among patients with different glioma grades, and there was positive correlation between their transcriptomic profiles in the plasma and tumor samples and with the cancer genome atlas (TCGA) glioma-derived RNA. | Blood samples were collected from twenty glioma patients prior to tumor resection. Plasma circulating cell-free messenger ribonucleic acids (ccfm-RNAs) and glioma-derived RNA were extracted and profiled. | VIII | [36] |
| Brain activity was significantly increased in the tumor hemisphere in general and in peritumoral regions specifically. However, none of the measures and spatial levels of brain activity correlated with changes in tumor volume, nor did they differ between patients with increasing versus stable tumor volumes. | The relationship between brain activity and increasing tumor volumes on routine clinical MRI in glioma patients was assessed. Postoperative magnetoencephalography (MEG) was recorded in 45 diffuse glioma patients. | VIII | [37] |
| The combination of a HGG, multiple development venous anomalies (DVAs) and malformations of cortical development (MCD) in a paediatric or young adult patient should prompt the neuroradiologist to hypothesize an underlying diagnosis of constitutional mismatch repair deficiency (CMMRD). | Case report: an 8-year-old boy with acute headache, vomiting, and an episode of unconsciousness in whom brain imaging revealed an HGG. | VIII | [38] |
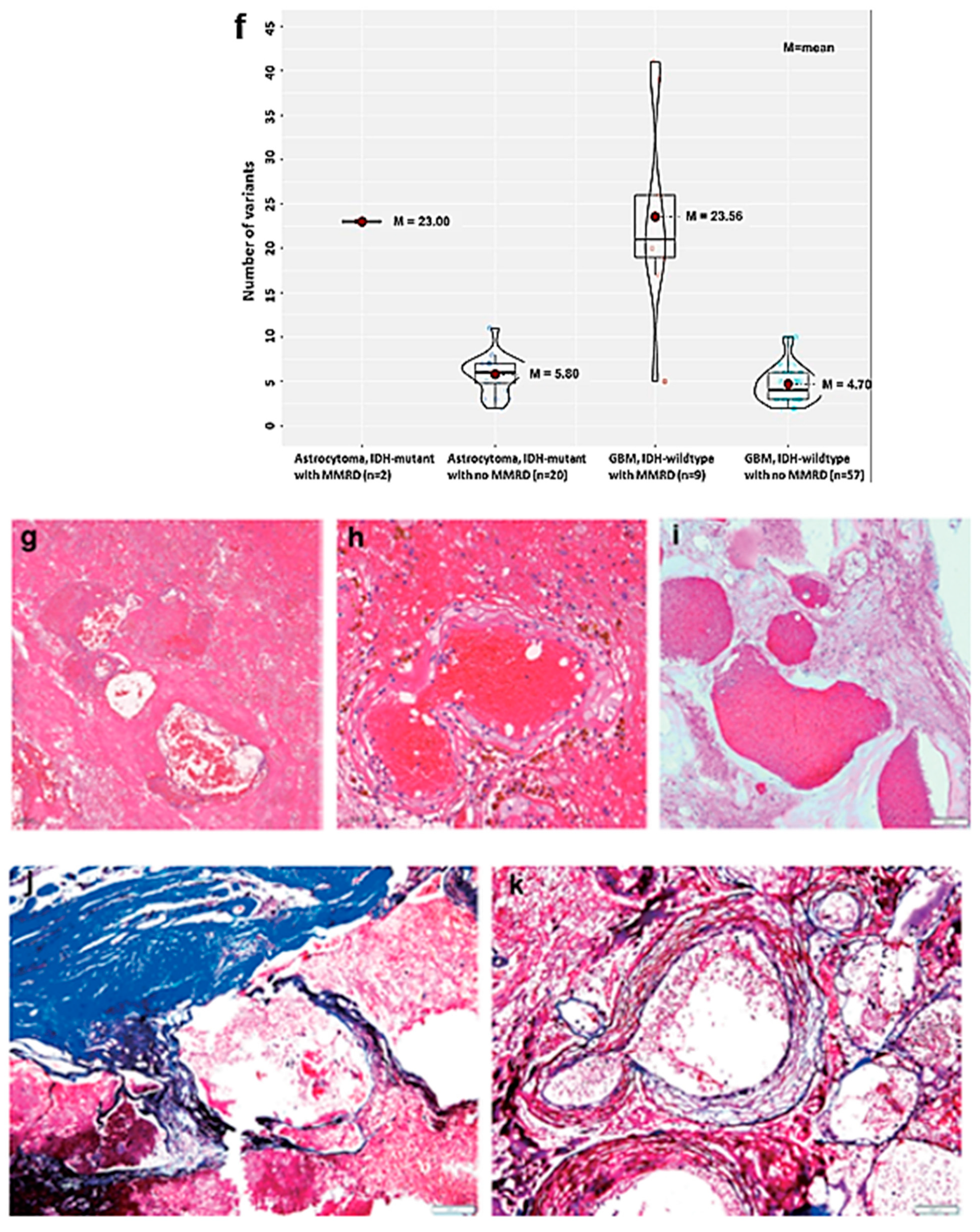
| The most common mismatch repair deficiency (MMRD) primary brain tumor was GB IDH wild-type. The genetic profile of MMRD GB was different from that of conventional GB. | Thirteen MMRD-associated (nine sporadic and four Lynch syndrome) primary HGGs were analyzed to determine their clinicopathological, molecular characteristics, and biological behavior. | VIII | [39] |
| A pathological diagnosis can be made safely and efficiently in brainstem lesions using stereotactic biopsy. | The medical records of 42 adult patients who underwent stereotactic biopsy on brainstem lesions were retrospectively analyzed. | VIII | [40] |
| Radiation-induced organizing hematoma (RIOH) is more likely to occur earlier with thick tumor wall in subjects who underwent gamma knife surgery (GKS) than it is in patients who underwent conventional radiotherapy (RT). These results indicate the clinical course of RIOH differs based on type of treatment and might help determine the duration of follow-up. | Thirty-seven RIOHs confirmed by surgical excision were divided into subgroups based on type of radiation treatment and pathology of the original lesion. The clinicopathological results were compared between the groups. | VIII | [41] |
3.2. Advances in MRI
3.3. Advances in PET
3.4. Advances in Non-Imaging Diagnosis
4. Advances in Prognosis
| Major Finding | Experimental System | LE 1 | Ref |
|---|---|---|---|
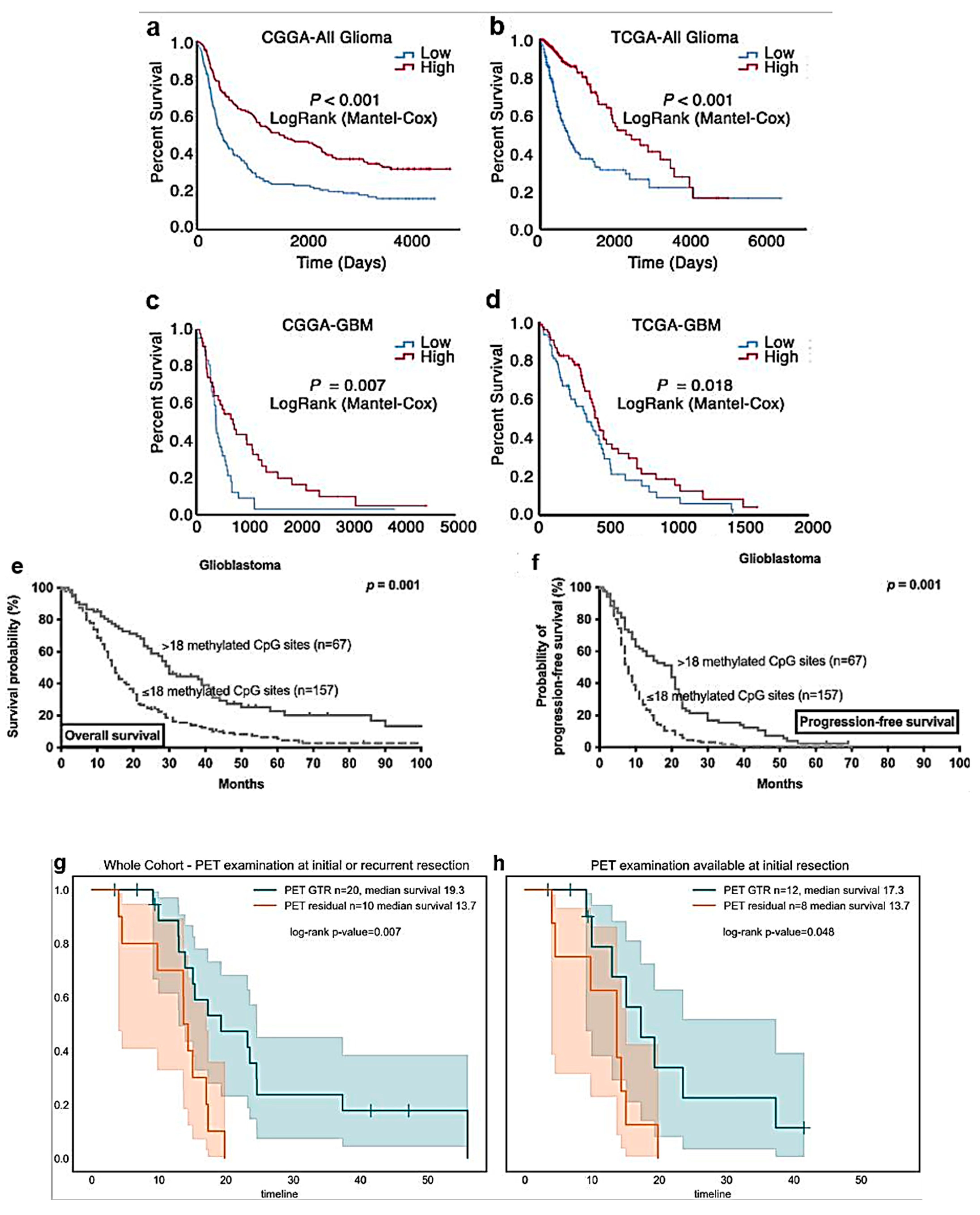
| A grade-dependent reduction on storkhead box 1 (STOX1) expression in glioma was revealed. STOX1 may be used as a novel predictive molecular biomarker for glioma grading and patients’ OS. | STOX1 expression in glioma was analyzed using three publicly available datasets, including CGGA, TCGA, and Rembrandt. | VIII | [52] |
| Extent and patterns of methylated CpG sites are similar in GB and IDH wild-type astrocytoma with ptert mutations. In both tumor entities, higher numbers of methylated CpG sites appear to be associated with a more favorable outcome. | An institutional database was searched for patients with GB defined by histopathology and IDH wild-type astrocytoma with promoter of telomerase reverse transcriptase (ptert) mutations. O6-methylguanine-DNA methyltransferase (MGMT) promotor methylation was analyzed using methylation-specific PCR and Sanger sequencing of CpG sites within the MGMT promotor region. | VIII | [54] |
| Positron emission tomography (PET)-guided gross total resection (GTR) improves the OS in patients with HGG. A multimodal imaging approach including FET-PET for surgical planning in newly diagnosed and recurrent tumors may improve the oncological outcome in HGG patients. | Imaging and survival data from patients with primary and recurrent HGGs who underwent FET-PET before surgical resection were retrospectively analyzed. | VIII | [55] |
| Similar results for the differentiation of HGG progression from treatment-related changes were obtained using different machine learning models. Further, an additional advantage based on TBR values only was found for tumor-to-background ratio (TBR) static and TTP dynamic radiomics over those of the classical analysis. | Eighty-five patients with histologically confirmed HGG who were investigated by dynamic 18F-FDOPA PET in two institutions were retrospectively analyzed. | VIII | [56] |
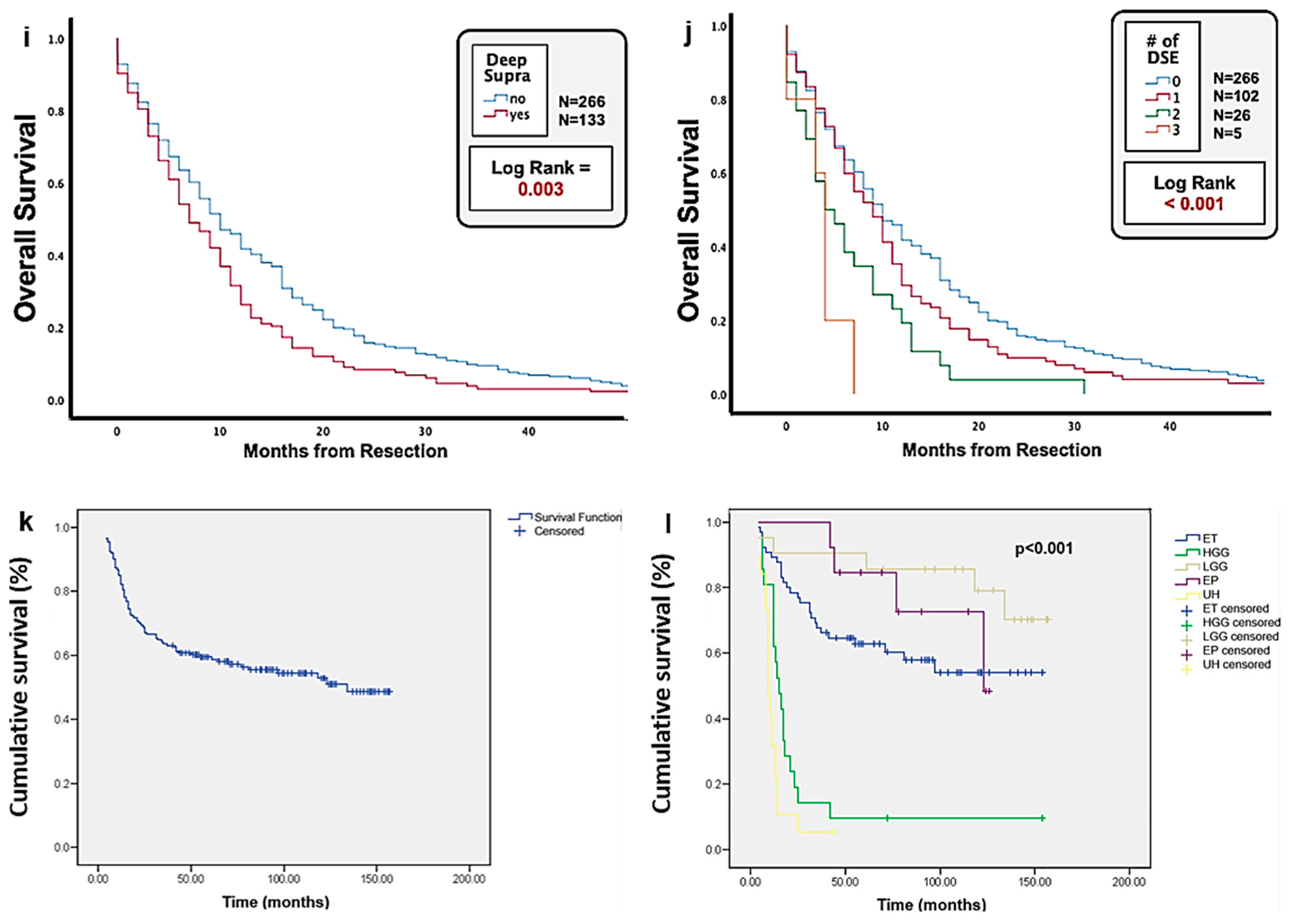
| GB patients with deep supratentorial extension (DSE) have a lower OS compared to those without DSE. This survival difference appears to be primarily related to the limited surgical extent of resection, owing to the neurological deficits that may be incurred with involvement of eloquent deep brain structures. | The MRI scans of 419 HGG patients who underwent tumor resection were retrospectively analyzed. | VIII | [57] |
| Quantitative analysis of conventional MRI sequences can demarcate HGG peritumoral region (PTR) from LGG, which is otherwise indistinguishable by visual estimation. | A total of 74 patients were included in the analysis: 42 patients affected by HGG with preoperative scans of tumors, and 32 patients affected by LGG without high-grade features on imaging. | VIII | [58] |
| Baseline mean K(ep) may be a useful biomarker for predicting the response and stratifying patient outcomes following bevacizumab treatment in patients with recurrent HGG. | Fifty-three patients with recurrent HGG underwent baseline MRI including diffusion tensor imaging (DTI), dynamic contrast enhancement (DCE), and dynamic susceptibility contrast (DSC) before bevacizumab treatment. | VIII | [59] |
| This is a precious dataset that can be used to relate the visual appearance of the tumor on the scan with the genetic and histological features and to develop automatic segmentation methods. | The Erasmus Glioma Database (EGD) contains structural MRI scans, genetic and histological features (specifying the WHO 2016 subtype), and whole tumor segmentations of patients with glioma. | VIII | [60] |
| Even after adjusting for known confounders, married patients with HGG and LGG have a higher possibility of having a better outcome. This study highlights the potential significance that intimate support from spouse may improve glioma patients’ survival. | The Surveillance, Epidemiology, and End Results program was used to identify 81,277 patients diagnosed with the most common primary malignant brain tumors, including glioma, ependymoma, and medulloblastoma. | VIII | [61] |
| With an organized and dedicated multidisciplinary team, adequate outcomes for pediatric brain tumor patients can be achieved in a middle-income country setting. The presence of local residual disease after surgery and disseminated disease has a strong negative effect on OS. | A series of 173 pediatric patients treated in a Serbian referral oncology institution were analyzed based on their clinical, histological, treatment, and follow-up data. | VIII | [62] |
| The rs7853346 polymorphism in long non coding (lnc) RNA-PTENP1 and the rs1799864 polymorphism in chemokine receptor (CCR)2 could independently affect cognitive impairment after RT, while a more significant combined effect on cognitive impairment was exerted in glioma patients via the signaling pathway of PTENP1/miR-19b/CCR2. | Two hundred and seventy-nine glioma patients were recruited and grouped according to their genotypes of rs7853346 in PTENP1 and rs1799864 in CCR1. | VIII | [63] |
| A high incidence of early-onset endocrine disorders was found in examined brain tumor pediatric patients. An endocrine consultation and nutritional evaluation should be mandatory for all patients with a brain tumor, especially when the tumor is suprasellar or after hypothalamus/pituitary irradiation. | This is a noninterventional observational study based on data collection from medical records of 221 brain tumor pediatric patients. The main tumor types were medulloblastoma (37.6%), craniopharyngioma (29.0%), and glioma (20.4%). | VIII | [64] |
5. Concluding Remarks and Future Perspectives
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADC | apparent diffusion coefficient |
| AI | artificial intelligence |
| ALA | 5-aminolevulinic acid |
| APT | amide proton transfer |
| BSG | brainstem glioma |
| CBF | cerebral blood flow |
| ccfm-RNAs | circulating cell-free messenger ribonucleic acids |
| CCR2 | chemokine receptor-2 |
| CGGA | Chinese glioma genome atlas |
| CH | cavernous hemangioma |
| CMMRD | constitutional mismatch repair deficiency |
| CNS | central nervous system |
| CT | computed tomography |
| DCE | dynamic contrast-enhanced |
| DIPG | diffuse intrinsic pontine glioma |
| DIVIDE | diffusion variance decomposition |
| DMG | diffuse midline glioma |
| DMT | disease management team |
| DNP | dynamic nuclear polarization |
| DSC | dynamic susceptibility contrast |
| DSE | deep supratentorial extension |
| DTI | diffusion tensor imaging |
| DVA | developmental venous anomaly |
| DWI | diffusion-weighted imaging |
| EGD | Erasmus glioma database |
| EGFR | epidermal growth factor receptor |
| FAC | ferric ammonium citrate |
| FDG | fluorodeoxyglucose |
| 18FDOPA | 3,4-dihydroxy-6-18F-fluoro-L-phenylalanine |
| 18F-FET | O- (2-18F-fluoroethyl) -L-tyrosine |
| FLAIR | fluid attenuated inversion recovery |
| GB | glioblastoma |
| GFAP | glial fibrillary acidic protein |
| GKS | gamma knife surgery |
| HE | hematoxylin and eosin |
| GTR | gross total resection |
| HGG | high-grade glioma |
| IDH | isocitrate dehydrogenase |
| K(ep) | mean rate transfer coefficient |
| LAT1 | L1 amino acid transporter |
| LE | level of evidence according to https://guides.library.stonybrook.edu/evidence-based-medicine/levels_of_evidence (accessed on 14 March 2023) |
| LGG | low-grade glioma |
| lncRNA | long non-coding RNA |
| MCD | malformations of cortical development |
| MEG | magnetoencephalography |
| MET | methionine |
| MGMT | O6-methylguanine-DNA methyltransferase |
| MMRD | mismatch repair deficiency |
| MP | multiparametric |
| MRI | magnetic resonance imaging |
| OS | overall survival |
| PCNSL | primary central nervous system lymphoma |
| PET | positron emission tomography |
| PFS | progression-free survival |
| PSR | percentage signal recovery |
| PTR | peritumoral region |
| qPCR | quantitative polymerase chain reaction |
| qSM | quantitative susceptibility mapping |
| rCBV | relative cerebral blood volume |
| RECIST | response evaluation criteria in solid tumors |
| RIOH | radiation-induced organizing hematoma |
| ROI | region of interest |
| RT | radiotherapy |
| SGS | secondary gliosarcoma |
| STOX1 | storkhead box 1 |
| SWI | susceptibility-weighted imaging |
| TBR | tumor-to-background ratio |
| TCGA | the cancer genome atlas |
| pTERT | promoter of telomerase reverse transcriptase |
| TMZ | temozolomide |
| TTP | time-to-peak |
| WHO | World Health Organization |
References
- Crocetti, E.; Trama, A.; Stiller, C.; Caldarella, A.; Soffietti, R.; Jaal, J.; Weber, D.C.; Ricardi, U.; Slowinski, J.; Brandes, A. Epidemiology of glial and non-glial brain tumours in Europe. Eur. J. Cancer 2012, 48, 1532–1542. [Google Scholar] [CrossRef] [PubMed]
- Sandler, A.; Reilly, K.; Widemann, B. Editorial: Special issue on rare cancers. Curr. Probl. Cancer 2021, 45, 100774. [Google Scholar] [CrossRef]
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omuro, A.; DeAngelis, L.M. Glioblastoma and Other Malignant Gliomas: A Clinical Review. JAMA 2013, 310, 1842–1850. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Antonelli, M.; Poliani, P.L. Adult type diffuse gliomas in the new 2021 WHO Classification. Pathologica 2022, 114, 397–409. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Śledzińska, P.; Bebyn, M.; Szczerba, E.; Furtak, J.; Harat, M.; Olszewska, N.; Kamińska, K.; Kowalewski, J.; Lewandowska, M.A. Glioma 2021 WHO Classification: The Superiority of NGS Over IHC in Routine Diagnostics. Mol. Diagn. Ther. 2022, 26, 699–713. [Google Scholar] [CrossRef]
- Halasz, L.M.; Attia, A.; Bradfield, L.; Brat, D.J.; Kirkpatrick, J.P.; Laack, N.N.; Lalani, N.; Lebow, E.S.; Liu, A.K.; Niemeier, H.M.; et al. Radiation Therapy for IDH-Mutant Grade 2 and Grade 3 Diffuse Glioma: An ASTRO Clinical Practice Guideline. Pract. Radiat. Oncol. 2022, 12, 370–386. [Google Scholar] [CrossRef] [PubMed]
- Kresbach, C.; Neyazi, S.; Schüller, U. Updates in the classification of ependymal neoplasms: The 2021 WHO Classification and beyond. Brain Pathol. 2022, 32, e13068. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, P.; Brat, D.J. The 2021 WHO classification of central nervous system tumors: What neurologists need to know. Curr. Opin. Neurol. 2022, 35, 764–771. [Google Scholar] [CrossRef]
- Malhotra, A.K.; Karthikeyan, V.; Zabih, V.; Landry, A.; Bennett, J.; Bartels, U.; Nathan, P.C.; Tabori, U.; Hawkins, C.; Das, S.; et al. Adolescent and young adult glioma: Systematic review of demographic, disease, and treatment influences on survival. Neuro-Oncol. Adv. 2022, 4, vdac168. [Google Scholar] [CrossRef]
- Chaganti, J.; Taylor, M.; Woodford, H.; Steel, T. Differentiation of Primary Central Nervous System Lymphoma and High-Grade Glioma with Dynamic Susceptibility Contrast−Derived Metrics: Pilot Study. World Neurosurg. 2021, 151, e979–e987. [Google Scholar] [CrossRef] [PubMed]
- Hohm, A.; Karremann, M.; Gielen, G.H.; Pietsch, T.; Warmuth-Metz, M.; Vandergrift, L.A.; Bison, B.; Stock, A.; Hoffmann, M.; Pham, M.; et al. Magnetic Resonance Imaging Characteristics of Molecular Subgroups in Pediatric H3 K27M Mutant Diffuse Midline Glioma. Clin. Neuroradiol. 2021, 32, 249–258. [Google Scholar] [CrossRef]
- Li, J.; Zhao, Y.H.; Tian, S.F.; Xu, C.S.; Cai, Y.X.; Li, K.; Cheng, Y.B.; Wang, Z.F.; Li, Z.Q. Genetic alteration and clonal evolution of primary glioblastoma into secondary gliosarcoma. CNS Neurosci. Ther. 2021, 27, 1483–1492. [Google Scholar] [CrossRef]
- Ozturk, K.; Soylu, E.; Cayci, Z. Differentiation between primary CNS lymphoma and atypical glioblastoma according to major genomic alterations using diffusion and susceptibility-weighted MR imaging. Eur. J. Radiol. 2021, 141, 109784. [Google Scholar] [CrossRef]
- McAvoy, M.; Prieto, P.C.; Kaczmarzyk, J.R.; Fernández, I.S.; McNulty, J.; Smith, T.; Yu, K.-H.; Gormley, W.B.; Arnaout, O. Classification of glioblastoma versus primary central nervous system lymphoma using convolutional neural networks. Sci. Rep. 2021, 11, 15219. [Google Scholar] [CrossRef]
- Siakallis, L.; Sudre, C.H.; Mulholland, P.; Fersht, N.; Rees, J.; Topff, L.; Thust, S.; Jager, R.; Cardoso, M.J.; Panovska-Griffiths, J.; et al. Longitudinal structural and perfusion MRI enhanced by machine learning outperforms standalone modalities and radiological expertise in high-grade glioma surveillance. Neuroradiology 2021, 63, 2047–2056. [Google Scholar] [CrossRef]
- Manikis, G.; Ioannidis, G.; Siakallis, L.; Nikiforaki, K.; Iv, M.; Vozlic, D.; Surlan-Popovic, K.; Wintermark, M.; Bisdas, S.; Marias, K. Multicenter DSC–MRI-Based Radiomics Predict IDH Mutation in Gliomas. Cancers 2021, 13, 3965. [Google Scholar] [CrossRef]
- Strasser, B.; Arango, N.S.; Stockmann, J.P.; Gagoski, B.; Thapa, B.; Li, X.; Bogner, W.; Moser, P.; Small, J.; Cahill, D.P.; et al. Improving D-2-Hydroxyglutarate MR Spectroscopic Imaging in Mutant Isocitrate Dehydrogenase Glioma Patients with Multiplexed RF-Receive/B(0)-Shim Array Coils at 3 T. NMR Biomed. 2021, 35, e4621. [Google Scholar] [CrossRef]
- Li, S.; Zheng, Y.; Sun, W.; Lasič, S.; Szczepankiewicz, F.; Wei, Q.; Han, S.; Zhang, S.; Zhong, X.; Wang, L.; et al. Glioma grading, molecular feature classification, and microstructural characterization using MR diffusional variance decomposition (DIVIDE) imaging. Eur. Radiol. 2021, 31, 8197–8207. [Google Scholar] [CrossRef] [PubMed]
- Cluceru, J.; Interian, Y.; Phillips, J.J.; Molinaro, A.M.; Luks, T.L.; Alcaide-Leon, P.; Olson, M.P.; Nair, D.; LaFontaine, M.; Shai, A.; et al. Improving the noninvasive classification of glioma genetic subtype with deep learning and diffusion-weighted imaging. Neuro-Oncology 2022, 24, 639–652. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Yong, X.; Ma, X.; Zhao, J.; Shen, Z.; Chen, X.; Tian, F.; Chen, W.; Wu, D.; Zhang, Y. Differentiation of low- and high-grade pediatric gliomas with amide proton transfer imaging: Added value beyond quantitative relaxation times. Eur. Radiol. 2021, 31, 9110–9119. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, Z.; Qu, L.; Zhang, P.; Duan, Y.; Cheng, D.; Xu, X.; Sun, T.; Ding, J.; Xie, C.; Liu, X.; et al. Prediction of H3K27M-mutant brainstem glioma by amide proton transfer–weighted imaging and its derived radiomics. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4426–4436. [Google Scholar] [CrossRef]
- Calmon, R.; Dangouloff-Ros, V.; Varlet, P.; Deroulers, C.; Philippe, C.; Debily, M.-A.; Castel, D.; Beccaria, K.; Blauwblomme, T.; Grevent, D.; et al. Radiogenomics of diffuse intrinsic pontine gliomas (DIPGs): Correlation of histological and biological characteristics with multimodal MRI features. Eur. Radiol. 2021, 31, 8913–8924. [Google Scholar] [CrossRef]
- Kawai, T.; Brender, J.R.; Lee, J.A.; Kramp, T.; Kishimoto, S.; Krishna, M.C.; Tofilon, P.; Camphausen, K.A. Detection of metabolic change in glioblastoma cells after radiotherapy using hyperpolarized 13 C-MRI. NMR Biomed. 2021, 34, e4514. [Google Scholar] [CrossRef]
- Ebrahimpour, A.; Tirgar, F.; Hajipour-Verdom, B.; Abbasi, A.; Hadjighassem, M.; Abdolmaleki, P.; Hosseindoost, S.; Javadi, S.A.H.; Hashemi, H.; Foroushani, A.R.; et al. Detection of glioblastoma multiforme using quantitative molecular magnetic resonance imaging based on 5-aminolevulinic acid: In vitro and in vivo studies. Magn. Reson. Mater. Phys. Biol. Med. 2021, 35, 3–15. [Google Scholar] [CrossRef]
- Vettermann, F.J.; Diekmann, C.; Weidner, L.; Unterrainer, M.; Suchorska, B.; Ruf, V.; Dorostkar, M.; Wenter, V.; Herms, J.; Tonn, J.-C.; et al. L-type amino acid transporter (LAT) 1 expression in 18F-FET-negative gliomas. EJNMMI Res. 2021, 11, 124. [Google Scholar] [CrossRef]
- Tatekawa, H.; Uetani, H.; Hagiwara, A.; Bahri, S.; Raymond, C.; Lai, A.; Cloughesy, T.F.; Nghiemphu, P.L.; Liau, L.M.; Pope, W.B.; et al. Worse prognosis for IDH wild-type diffuse gliomas with larger residual biological tumor burden. Ann. Nucl. Med. 2021, 35, 1022–1029. [Google Scholar] [CrossRef]
- Li, Z.; Kaiser, L.; Holzgreve, A.; Ruf, V.C.; Suchorska, B.; Wenter, V.; Quach, S.; Herms, J.; Bartenstein, P.; Tonn, J.-C.; et al. Prediction of TERTp-Mutation Status in IDH-Wildtype High-Grade Gliomas using Pre-Treatment Dynamic [(18)F]FET PET Radiomics. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4415–4425. [Google Scholar] [CrossRef] [PubMed]
- Pellerin, A.; Khalifé, M.; Sanson, M.; Rozenblum-Beddok, L.; Bertaux, M.; Soret, M.; Galanaud, D.; Dormont, D.; Kas, A.; Pyatigorskaya, N. Simultaneously acquired PET and ASL imaging biomarkers may be helpful in differentiating progression from pseudo-progression in treated gliomas. Eur. Radiol. 2021, 31, 7395–7405. [Google Scholar] [CrossRef]
- Tomura, N.; Saginoya, T.; Goto, H. PET findings in lymphomatosis and gliomatosis of the brain: A comparison of C-11 methionine PET/CT and F-18 FDG PET/CT. Acta Radiol. 2021, 62, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Nobashi, T.W.; Mayer, A.T.; Xiao, Z.; Chan, C.T.; Chaney, A.M.; James, M.L.; Gambhir, S.S. Whole-body PET Imaging of T-cell Response to Glioblastoma. Clin. Cancer Res. 2021, 27, 6445–6456. [Google Scholar] [CrossRef] [PubMed]
- Ita, M.I.; Wang, J.H.; Toulouse, A.; Lim, C.; Fanning, N.; O’Sullivan, M.; Nolan, Y.; Kaar, G.F.; Redmond, H.P. The Utility of Plasma Circulating Cell-Free Messenger RNA as a Biomarker of Glioma: A Pilot Study. Acta Neurochir. 2021, 164, 723–735. [Google Scholar] [CrossRef]
- Numan, T.; Kulik, S.D.; Moraal, B.; Reijneveld, J.C.; Stam, C.J.; Hamer, P.C.D.W.; Derks, J.; Bruynzeel, A.M.E.; van Linde, M.E.; Wesseling, P.; et al. Non-invasively measured brain activity and radiological progression in diffuse glioma. Sci. Rep. 2021, 11, 18990. [Google Scholar] [CrossRef]
- Chhabda, S.; Sudhakar, S.; Mankad, K.; Jorgensen, M.; Carceller, F.; Jacques, T.S.; Merve, A.; Aizpurua, M.; Chalker, J.; Garimberti, E.; et al. Constitutional Mismatch Repair Deficiency (CMMRD) Presenting with High-Grade Glioma, Multiple Developmental Venous Anomalies and Malformations of Cortical Development-a Multidisciplinary/Multicentre Approach and Neuroimaging Clues to Clinching the Diagnosis. Childs Nerv. Syst. 2021, 37, 2375–2379. [Google Scholar]
- Kim, H.; Lim, K.Y.; Park, J.W.; Kang, J.; Won, J.K.; Lee, K.; Shim, Y.; Park, C.-K.; Kim, S.-K.; Choi, S.-H.; et al. Sporadic and Lynch syndrome-associated mismatch repair-deficient brain tumors. Lab. Investig. 2022, 102, 160–171. [Google Scholar] [CrossRef]
- Jung, I.; Chang, K.W.; Park, S.H.; Moon, J.H.; Kim, E.H.; Jung, H.H.; Kang, S.; Chang, J.H.; Chang, J.W.; Chang, W.S. Stereotactic biopsy for adult brainstem lesions: A surgical approach and its diagnostic value according to the 2016 World Health Organization Classification. Cancer Med. 2021, 10, 7514–7524. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, S.H.; Chang, J.-H.; Park, M.; Cha, Y.J. Clinicopathological differences in radiation-induced organizing hematomas of the brain based on type of radiation treatment and primary lesions. J. Pathol. Transl. Med. 2022, 56, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Smits, M. Update on neuroimaging in brain tumours. Curr. Opin. Neurol. 2021, 34, 497–504. [Google Scholar] [CrossRef]
- Johnson, D.R.; Kaufmann, T.J.; Patel, S.H.; Chi, A.S.; Snuderl, M.; Jain, R. There is an exception to every rule—T2-FLAIR mismatch sign in gliomas. Neuroradiology 2019, 61, 225–227. [Google Scholar] [CrossRef]
- Pinto, C.; Noronha, C.; Taipa, R.; Ramos, C. T2-FLAIR mismatch sign: A roadmap of pearls and pitfalls. Br. J. Radiol. 2021, 95, 20210825. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, R.; Baba, A.; Kurokawa, M.; Pinarbasi, E.S.; Makise, N.; Ota, Y.; Kim, J.; Srinivasan, A.; Moritani, T. Neuroimaging features of diffuse hemispheric glioma, H3 G34-mutant: A case series and systematic review. J. Neuroimaging 2021, 32, 17–27. [Google Scholar] [CrossRef]
- Rykkje, A.; Li, D.; Skjøth-Rasmussen, J.; Larsen, V.; Nielsen, M.; Hansen, A.; Carlsen, J. Surgically Induced Contrast Enhancements on Intraoperative and Early Postoperative MRI Following High-Grade Glioma Surgery: A Systematic Review. Diagnostics 2021, 11, 1344. [Google Scholar] [CrossRef]
- Laudicella, R.; Quartuccio, N.; Argiroffi, G.; Alongi, P.; Baratto, L.; Califaretti, E.; Frantellizzi, V.; De Vincentis, G.; Del Sole, A.; Evangelista, L.; et al. Unconventional non-amino acidic PET radiotracers for molecular imaging in gliomas. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3925–3939. [Google Scholar] [CrossRef] [PubMed]
- Ekici, S.; Nye, J.; Neill, S.; Allen, J.; Shu, H.-K.; Fleischer, C. Glutamine Imaging: A New Avenue for Glioma Management. AJNR Am. J. Neuroradiol. 2021, 43, 11–18. [Google Scholar] [CrossRef]
- Tuleasca, C.; Leroy, H.-A.; Peciu-Florianu, I.; Strachowski, O.; Derre, B.; Levivier, M.; Schulder, M.; Reyns, N. Impact of combined use of intraoperative MRI and awake microsurgical resection on patients with gliomas: A systematic review and meta-analysis. Neurosurg. Rev. 2021, 44, 2977–2990. [Google Scholar] [CrossRef] [PubMed]
- Matsumae, M.; Nishiyama, J.; Kuroda, K. Intraoperative MR Imaging during Glioma Resection. Magn. Reson. Med. Sci. 2021, 21, 148–167. [Google Scholar] [CrossRef]
- Zhang, C.; Ji, Z.; Wang, M.; Zhang, W.; Yang, R.; An, H.; Yang, R.; van Abel, D.; van Dijk, M.; Yang, X.; et al. Stox1 as a novel transcriptional suppressor of Math1 during cerebellar granule neurogenesis and medulloblastoma formation. Cell Death Differ. 2016, 23, 2042–2053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, F.-Q.; Jin, L.; Wang, Y.-L. Downregulation of STOX1 is a novel prognostic biomarker for glioma patients. Open Life Sci. 2021, 16, 1164–1174. [Google Scholar] [CrossRef] [PubMed]
- Brandner, S.; McAleenan, A.; Kelly, C.; Spiga, F.; Cheng, H.Y.; Dawson, S.; Schmidt, L.; Faulkner, C.L.; Wragg, C.; Jefferies, S.; et al. MGMT Promoter Methylation Testing to Predict overall Survival in People with Glioblastoma Treated with Temozolomide: A Comprehensive Meta-Analysis Based on a Cochrane Systematic Review. Neuro-Oncology 2021, 23, 1457–1469. [Google Scholar] [CrossRef]
- Teske, N.; Karschnia, P.; Weller, J.; Siller, S.; Dorostkar, M.M.; Herms, J.; von Baumgarten, L.; Tonn, J.C.; Thon, N. Extent, Pattern, and Prognostic Value of MGMT Promotor Methylation: Does it Differ between Glioblastoma and IDH-Wildtype/TERT-Mutated Astrocytoma? J. Neuro-Oncol. 2021, 156, 317–327. [Google Scholar] [CrossRef]
- Ort, J.; Hamou, H.A.; Kernbach, J.M.; Hakvoort, K.; Blume, C.; Lohmann, P.; Galldiks, N.; Heiland, D.H.; Mottaghy, F.M.; Clusmann, H.; et al. 18F-FET-PET-guided gross total resection improves overall survival in patients with WHO grade III/IV glioma: Moving towards a multimodal imaging-guided resection. J. Neuro-Oncol. 2021, 155, 71–80. [Google Scholar] [CrossRef]
- Ahrari, S.; Zaragori, T.; Rozenblum, L.; Oster, J.; Imbert, L.; Kas, A.; Verger, A. Relevance of Dynamic 18F-DOPA PET Radiomics for Differentiation of High-Grade Glioma Progression from Treatment-Related Changes. Biomedicines 2021, 9, 1924. [Google Scholar] [CrossRef]
- Barsouk, A.; Baldassari, M.P.; Khanna, O.; Andrews, C.E.; Ye, D.Y.; Velagapudi, L.; Al Saiegh, F.; Hafazalla, K.; Cunningham, E.; Patel, H.; et al. Glioblastoma with deep supratentorial extension is associated with a worse overall survival. J. Clin. Neurosci. 2021, 93, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Malik, N.; Geraghty, B.; Dasgupta, A.; Maralani, P.J.; Sandhu, M.; Detsky, J.; Tseng, C.-L.; Soliman, H.; Myrehaug, S.; Husain, Z.; et al. MRI radiomics to differentiate between low grade glioma and glioblastoma peritumoral region. J. Neuro-Oncol. 2021, 155, 181–191. [Google Scholar] [CrossRef]
- Park, Y.W.; Ahn, S.S.; Moon, J.H.; Kim, E.H.; Kang, S.-G.; Chang, J.H.; Kim, S.H.; Lee, S.-K. Dynamic contrast-enhanced MRI may be helpful to predict response and prognosis after bevacizumab treatment in patients with recurrent high-grade glioma: Comparison with diffusion tensor and dynamic susceptibility contrast imaging. Neuroradiology 2021, 63, 1811–1822. [Google Scholar] [CrossRef]
- van der Voort, S.R.; Incekara, F.; Wijnenga, M.M.; Kapsas, G.; Gahrmann, R.; Schouten, J.W.; Dubbink, H.J.; Vincent, A.J.P.E.; van den Bent, M.J.; French, P.J.; et al. The Erasmus Glioma Database (EGD): Structural MRI scans, WHO 2016 subtypes, and segmentations of 774 patients with glioma. Data Brief 2021, 37, 107191. [Google Scholar] [CrossRef]
- Deng, Z.; Li, X.; Yang, J.; Yu, H.; Zhang, N. Marital Status Independently Predicts Glioma Patient Mortality: A Surveillance, Epidemiology, and End Results (SEER) Analysis. World Neurosurg. 2021, 152, e302–e312. [Google Scholar] [CrossRef] [PubMed]
- Stanić, D.; Grujičić, D.; Pekmezović, T.; Bokun, J.; Popović-Vuković, M.; Janić, D.; Paripović, L.; Ilić, V.; Slović, M.P.; Ilić, R.; et al. Clinical profile, treatment and outcome of pediatric brain tumors in Serbia in a 10-year period: A national referral institution experience. PLoS ONE 2021, 16, e0259095. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Fu, Z.Z.; Zhang, Y.Q.; Fu, B.H.; Dong, L.X. Rs7853346 Polymorphism in lncRNA-PTENP1 and rs1799864 Polymorphism in CCR2 are Associated with Radiotherapy-Induced Cognitive Impairment in Subjects with Glioma Via Regulating PTENP1/miR-19b/CCR2 Signaling Pathway. Biochem. Genet. 2021, 60, 1159–1176. [Google Scholar] [CrossRef]
- Briceño, L.G.G.; Kariyawasam, D.; Samara-Boustani, D.; Giani, E.; Beltrand, J.; Bolle, S.; Fresneau, B.; Puget, S.; Sainte-Rose, C.; Alapetite, C.; et al. High Prevalence of Early Endocrine Disorders After Childhood Brain Tumors in a Large Cohort. J. Clin. Endocrinol. Metab. 2021, 107, e2156–e2166. [Google Scholar] [CrossRef]
- Ko, C.-C.; Yeh, L.-R.; Kuo, Y.-T.; Chen, J.-H. Imaging biomarkers for evaluating tumor response: RECIST and beyond. Biomark. Res. 2021, 9, 52. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, J.P.; Jayson, G.C. Do Imaging Biomarkers Relate to Outcome in Patients Treated with VEGF Inhibitors? Clin. Cancer Res. 2012, 18, 6588–6598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, S.; Fu, Z.; Zhang, Y.; Fu, B.; Dong, L. The G to A transformation of rs4702 polymorphism in 3’UTR of FURIN reduced the risk of radiotherapy-induced cognitive impairment in glioma patients. J. Cell. Mol. Med. 2021, 26, 684–692. [Google Scholar] [CrossRef]
- Singh, G.; Manjila, S.; Sakla, N.; True, A.; Wardeh, A.H.; Beig, N.; Vaysberg, A.; Matthews, J.; Prasanna, P.; Spektor, V. Radiomics and radiogenomics in gliomas: A contemporary update. Br. J. Cancer 2021, 125, 641–657. [Google Scholar] [CrossRef]
- Daisy, P.S.; Anitha, T.S. Can Artificial Intelligence Overtake Human Intelligence on the Bumpy Road Towards Glioma Therapy? Med. Oncol. 2021, 38, 53. [Google Scholar] [CrossRef]
- Strauss, S.B.; Meng, A.; Ebani, E.J.; Chiang, G.C. Imaging Glioblastoma Posttreatment: Progression, Pseudoprogression, Pseudoresponse, Radiation Necrosis. Neuroimaging Clin. N. Am. 2021, 31, 103–120. [Google Scholar] [CrossRef]
- Alhasan, A.S. Clinical Applications of Artificial Intelligence, Machine Learning, and Deep Learning in the Imaging of Gliomas: A Systematic Review. Cureus 2021, 13, e19580. [Google Scholar] [CrossRef]
- Sharma, A.; Graber, J.J. Overview of prognostic factors in adult gliomas. Ann. Palliat. Med. 2021, 10, 863–874. [Google Scholar] [CrossRef] [PubMed]
- Funakoshi, Y.; Hata, N.; Kuga, D.; Hatae, R.; Sangatsuda, Y.; Fujioka, Y.; Takigawa, K.; Mizoguchi, M. Pediatric Glioma: An Update of Diagnosis, Biology and Treatment. Cancers 2021, 13, 758. [Google Scholar] [CrossRef] [PubMed]
- Lohmann, P.; Galldiks, N.; Kocher, M.; Heinzel, A.; Filss, C.P.; Stegmayr, C.; Mottaghy, F.M.; Fink, G.R.; Shah, N.J.; Langen, K.-J. Radiomics in neuro-oncology: Basics, workflow, and applications. Methods 2021, 188, 112–121. [Google Scholar] [CrossRef]
- Razek, A.A.K.A.; Alksas, A.; Shehata, M.; AbdelKhalek, A.; Baky, K.A.; El-Baz, A.; Helmy, E. Clinical applications of artificial intelligence and radiomics in neuro-oncology imaging. Insights Imaging 2021, 12, 152. [Google Scholar] [CrossRef] [PubMed]
- Pinarbasi, E.M.; Pratt, D. The Evolving Molecular Landscape of High-Grade Gliomas. Cancer J. 2021, 27, 337–343. [Google Scholar] [CrossRef]
- Koh, L.; Novera, W.; Lim, S.W.; Chong, Y.K.; Pang, Q.Y.; Low, D.; Ang, B.T.; Tang, C. Integrative multi-omics approach to targeted therapy for glioblastoma. Pharmacol. Res. 2022, 182, 106308. [Google Scholar] [CrossRef]
- Gritsch, S.; Batchelor, T.T.; Castro, L.N.G. Diagnostic, therapeutic, and prognostic implications of the 2021 World Health Organization classification of tumors of the central nervous system. Cancer 2022, 128, 47–58. [Google Scholar] [CrossRef]
- Perez, A.; Huse, J.T. The Evolving Classification of Diffuse Gliomas: World Health Organization Updates for 2021. Curr. Neurol. Neurosci. Rep. 2021, 21, 67. [Google Scholar] [CrossRef]
- Yuan, F.; Wang, Y.; Ma, C. Current WHO Guidelines and the Critical Role of Genetic Parameters in the Classification of Glioma: Opportunities for Immunotherapy. Curr. Treat. Options Oncol. 2022, 23, 188–198. [Google Scholar] [CrossRef]
- Sejda, A.; Grajkowska, W.; Trubicka, J.; Szutowicz, E.; Wojdacz, T.; Kloc, W.; Iżycka-Świeszewska, E. WHO CNS5 2021 classification of gliomas: A practical review and road signs for diagnosing pathologists and proper patho-clinical and neuro-oncological cooperation. Folia Neuropathol. 2022, 60, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Jelski, W.; Mroczko, B. Molecular and Circulating Biomarkers of Brain Tumors. Int. J. Mol. Sci. 2021, 22, 7039. [Google Scholar] [CrossRef]
- Fazzari, F.G.; Rose, F.; Pauls, M.; Guay, E.; Ibrahim, M.F.; Basulaiman, B.; Tu, M.; Hutton, B.; Nicholas, G.; Ng, T.L. The current landscape of systemic therapy for recurrent glioblastoma: A systematic review of randomized-controlled trials. Crit. Rev. Oncol. 2022, 169, 103540. [Google Scholar] [CrossRef] [PubMed]
- Barthel, L.; Hadamitzky, M.; Dammann, P.; Schedlowski, M.; Sure, U.; Thakur, B.K.; Hetze, S. Glioma: Molecular signature and crossroads with tumor microenvironment. Cancer Metastasis Rev. 2022, 41, 53–75. [Google Scholar] [CrossRef]
- Abadi, B.; Ahmadi-Zeidabadi, M.; Dini, L.; Vergallo, C. Stem Cell-Based Therapy Treating Glioblastoma Multiforme. Hematol. Oncol. Stem Cell. Ther. 2021, 14, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kazerooni, A.F.; Bagley, S.J.; Akbari, H.; Saxena, S.; Bagheri, S.; Guo, J.; Chawla, S.; Nabavizadeh, A.; Mohan, S.; Bakas, S.; et al. Applications of Radiomics and Radiogenomics in High-Grade Gliomas in the Era of Precision Medicine. Cancers 2021, 13, 5921. [Google Scholar] [CrossRef]
- Du, P.; Chen, H.; Lv, K.; Geng, D. A Survey of Radiomics in Precision Diagnosis and Treatment of Adult Gliomas. J. Clin. Med. 2022, 11, 3802. [Google Scholar] [CrossRef]
- Gore, S.; Chougule, T.; Jagtap, J.; Saini, J.; Ingalhalikar, M. A Review of Radiomics and Deep Predictive Modeling in Glioma Characterization. Acad. Radiol. 2021, 28, 1599–1621. [Google Scholar] [CrossRef]
- Tabatabaei, M.; Razaei, A.; Sarrami, A.H.; Saadatpour, Z.; Singhal, A.; Sotoudeh, H. Current Status and Quality of Machine Learning-Based Radiomics Studies for Glioma Grading: A Systematic Review. Oncology 2021, 99, 433–443. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frosina, G. Recapitulating the Key Advances in the Diagnosis and Prognosis of High-Grade Gliomas: Second Half of 2021 Update. Int. J. Mol. Sci. 2023, 24, 6375. https://doi.org/10.3390/ijms24076375
Frosina G. Recapitulating the Key Advances in the Diagnosis and Prognosis of High-Grade Gliomas: Second Half of 2021 Update. International Journal of Molecular Sciences. 2023; 24(7):6375. https://doi.org/10.3390/ijms24076375
Chicago/Turabian StyleFrosina, Guido. 2023. "Recapitulating the Key Advances in the Diagnosis and Prognosis of High-Grade Gliomas: Second Half of 2021 Update" International Journal of Molecular Sciences 24, no. 7: 6375. https://doi.org/10.3390/ijms24076375