
One Third of Malignant Pleural Mesothelioma Shows High Immunohistochemical Expression of MSLN or CXCR4 Which Indicates Potent Candidates for Endo-Radiotherapy

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
2.1. Clinicopathological Data of Patients
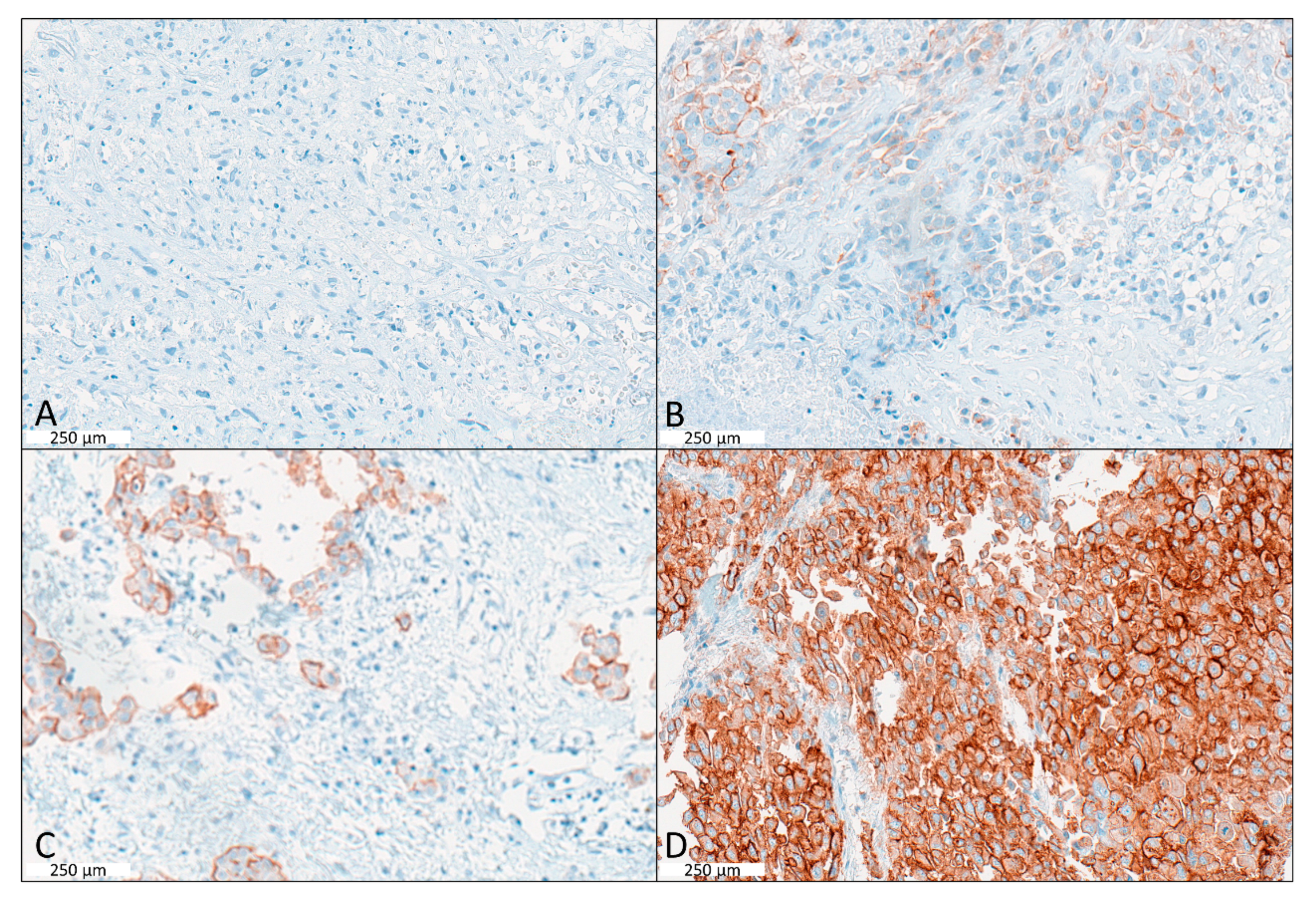
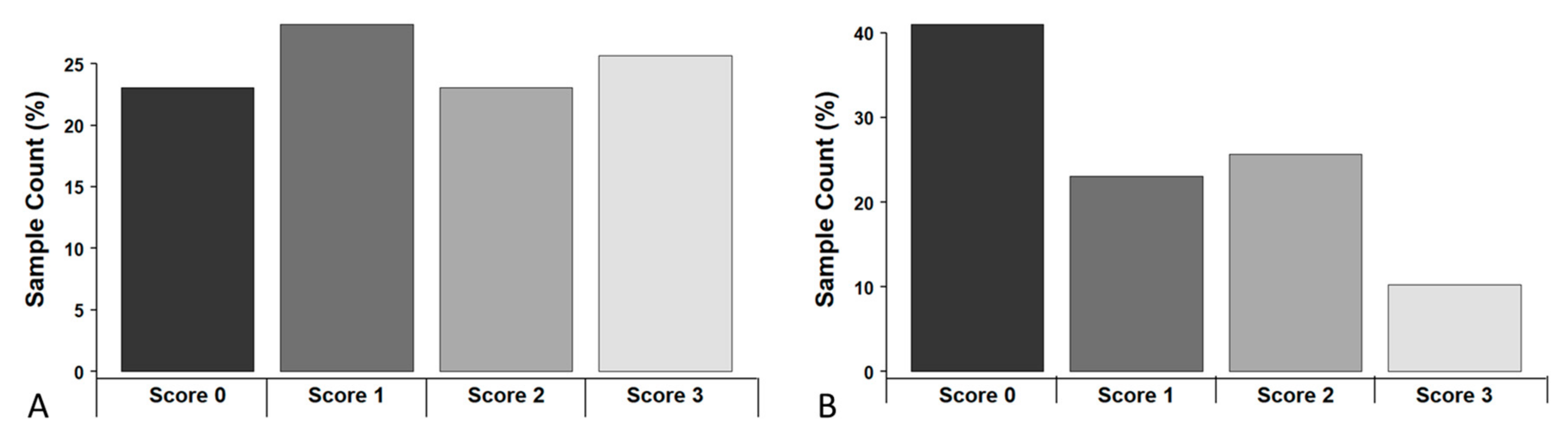
2.2. CXCR4 Expression in Human MPM Is Associated with Clinical Factors
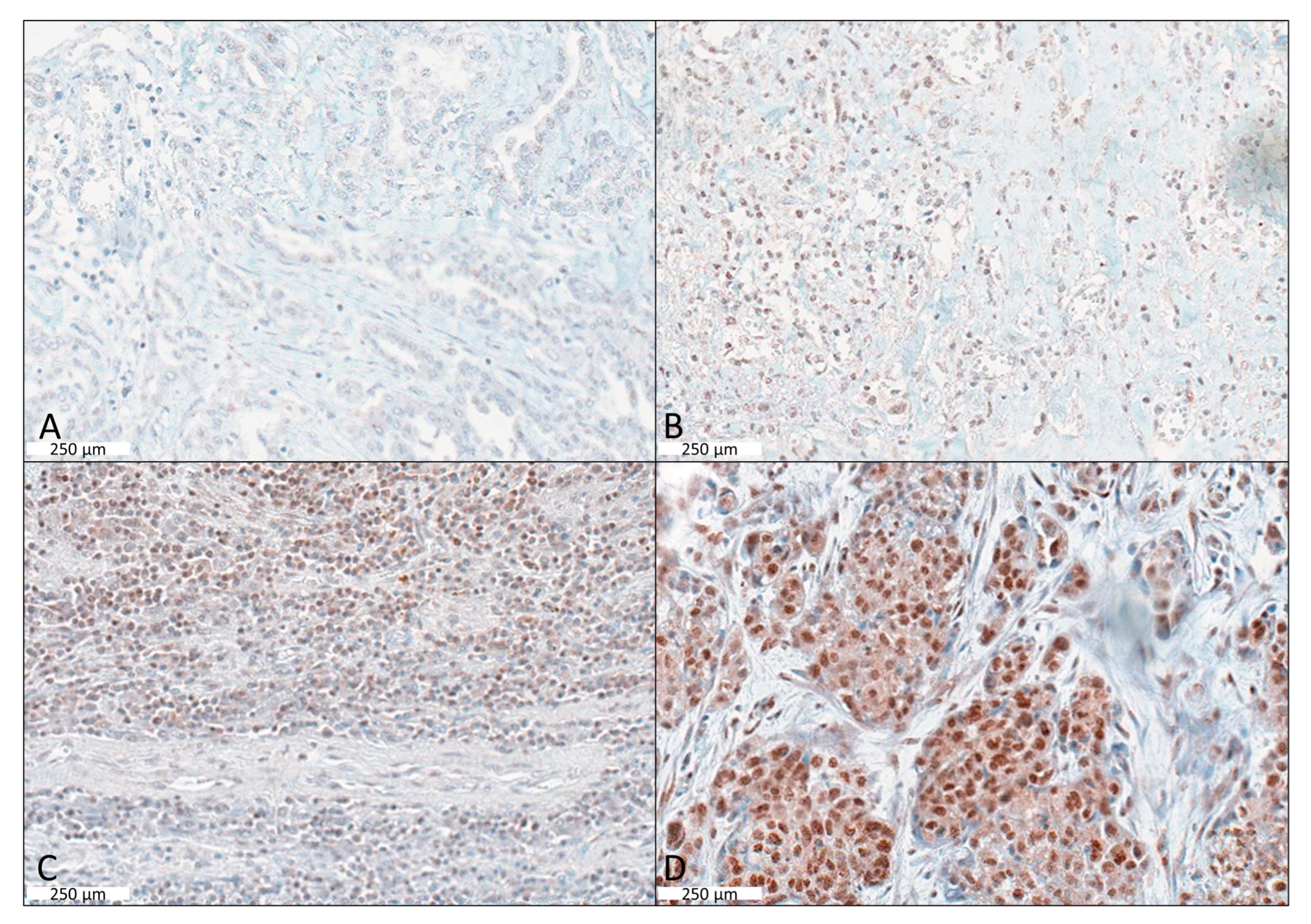
2.3. MSLN Expression in Human MPM Is Associated with Clinical Factors
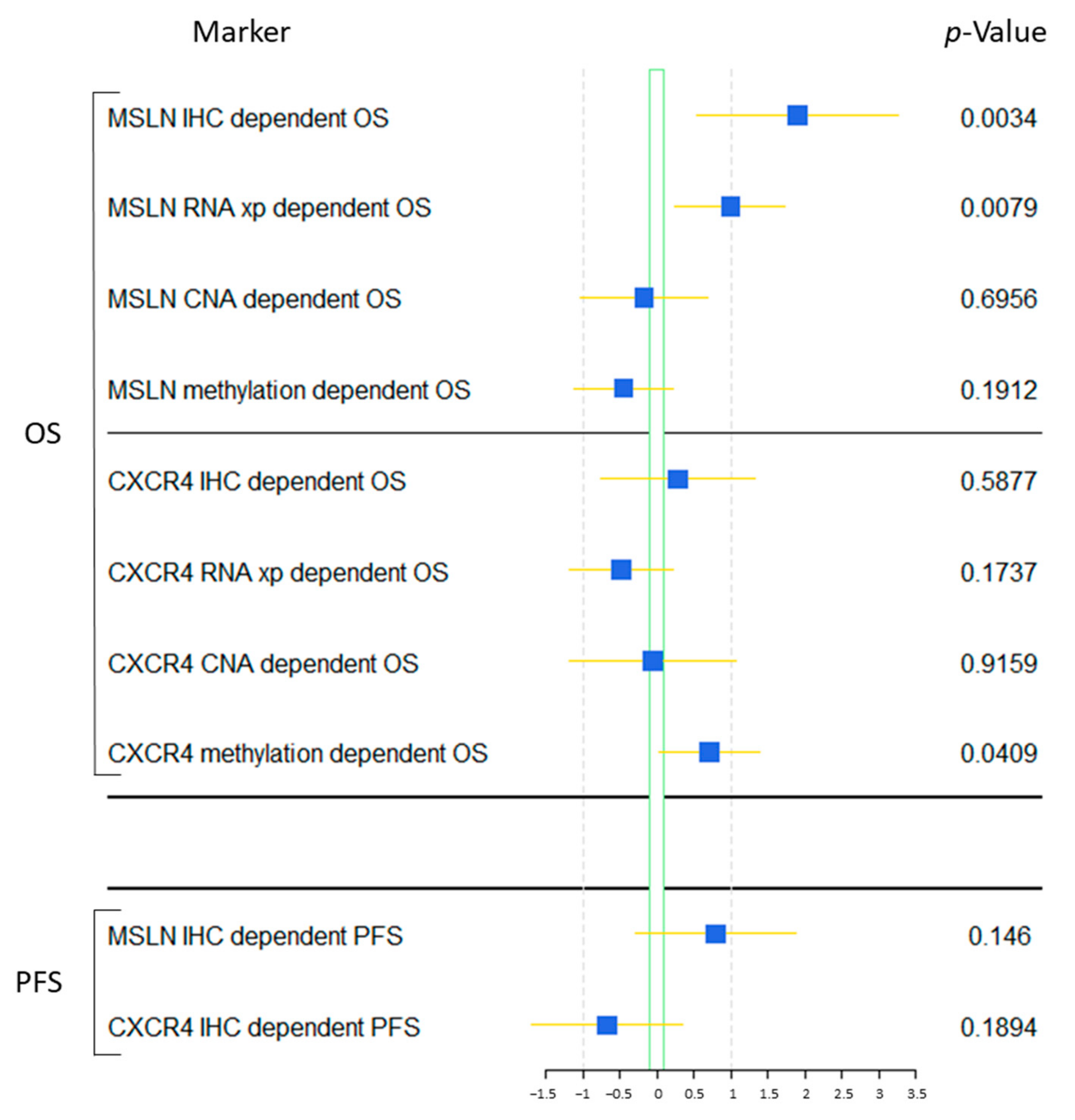
2.4. Survival Analysis
2.5. Validation of the Results and Biological Regulation Using the TCGA Data Set
3. Discussion
4. Materials and Methods
4.1. The Demographic Data
4.2. Clinicopathological Data
4.3. Immunohistochemistry
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goudar, R.K. Review of pemetrexed in combination with cisplatin for the treatment of malignant pleural mesothelioma. Ther. Clin. Risk Manag. 2008, 4, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Klominek, J. Regulation of matrix metalloprotease activity in malignant mesothelioma cell lines by growth factors. Thorax 2003, 58, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramalingam, S.S.; Belani, C.P. Recent advances in the treatment of malignant pleural mesothelioma. J. Thorac. Oncol. 2008, 3, 1056–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vorobiof, D.A.; Mafafo, K. Malignant pleural mesothelioma: Medical treatment update. Clin. Lung Cancer 2009, 10, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Ceresoli, G.L.; Castagneto, B.; Zucali, P.A.; Favaretto, A.; Mencoboni, M.; Grossi, F.; Cortinovis, D.; Del Conte, G.; Ceribelli, A.; Bearz, A.; et al. Pemetrexed plus carboplatin in elderly patients with malignant pleural mesothelioma: Combined analysis of two phase II trials. Br. J. Cancer 2008, 99, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Ceresoli, G.L.; Zucali, P.A.; Favaretto, A.; Grossi, F.; Bidoli, P.; Del Conte, G.; Ceribelli, A.; Bearz, A.; Morenghi, E.; Cavina, R.; et al. Phase II study of pemetrexed plus carboplatin in malignant pleural mesothelioma. J. Clin. Oncol. 2006, 24, 1443–1448. [Google Scholar] [CrossRef] [PubMed]
- Kindler, H.L. Systemic treatments for mesothelioma: Standard and novel. Curr. Treat. Options Oncol. 2008, 9, 171–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, N.S.; Gupta, V. Repurposing therapeutics for malignant pleural mesothelioma (MPM)—Updates on clinical translations and future outlook. Life Sci. 2022, 304, 120716. [Google Scholar] [CrossRef] [PubMed]
- Tomek, S.; Manegold, C. Chemotherapy for malignant pleural mesothelioma: Past results and recent developments. Lung Cancer 2004, 45 (Suppl. 1), S103–S119. [Google Scholar] [CrossRef] [Green Version]
- Mairinger, F.; Vollbrecht, C.; Halbwedl, I.; Hatz, M.; Stacher, E.; Gülly, C.; Quehenberger, F.; Stephan-Falkenau, S.; Kollmeier, J.; Roth, A.; et al. Reduced folate carrier and folylpolyglutamate synthetase, but not thymidylate synthase predict survival in pemetrexed-treated patients suffering from malignant pleural mesothelioma. J. Thorac. Oncol. 2013, 8, 644–653. [Google Scholar] [CrossRef] [Green Version]
- Mairinger, F.; Vollbrecht, C.; Mairinger, T.; Popper, H. The issue of studies evaluating biomarkers which predict outcome after pemetrexed-based chemotherapy in malignant pleural mesothelioma. J. Thorac. Oncol. 2013, 8, e80–e82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomek, S.; Emri, S.; Krejcy, K.; Manegold, C. Chemotherapy for malignant pleural mesothelioma: Past results and recent developments. Br. J. Cancer 2003, 88, 167–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satapathy, S.; Singh, H.; Kumar, R.; Mittal, B.R. Diagnostic Accuracy of (68)Ga-PSMA PET/CT for Initial Detection in Patients With Suspected Prostate Cancer: A Systematic Review and Meta-Analysis. AJR Am. J. Roentgenol. 2021, 216, 599–607. [Google Scholar] [CrossRef] [PubMed]
- FDA Approves First PSMA-Targeted PET Drug. J. Nucl. Med. 2021, 62, 11n.
- Gupta, M.; Karthikeyan, G.; Choudhury, P.S.; Babu Koyyala, V.P.; Sharma, M.; Jain, P.; Talwar, V.; Singh, A.; Rawal, S. A Walk with Lu-177 PSMA: How Close we Have Reached from Bench to Bedside? Cancer Investig. 2020, 38, 486–492. [Google Scholar] [CrossRef]
- Hayrapetian, A.; Girgis, M.D.; Yanagawa, J.; French, S.W.M.; Schelbert, H.R.M.; Auerbach, M.S.; Czernin, J.; Calais, J.M. Incidental Detection of Elastofibroma Dorsi With 68Ga-FAPI-46 and 18F-FDG PET/CT in a Patient With Esophageal Cancer. Clin. Nucl. Med. 2021, 46, e86–e87. [Google Scholar] [CrossRef]
- Pang, Y.; Wei, J.; Shang, Q.; Zhao, L.; Chen, H. 68Ga-Fibroblast Activation Protein Inhibitor, a Promising Radiopharmaceutical in PET/CT to Detect the Primary and Metastatic Lesions of Chromophobe Renal Cell Carcinoma. Clin. Nucl. Med. 2021, 46, 177–179. [Google Scholar] [CrossRef]
- Watabe, T.; Liu, Y.; Kaneda-Nakashima, K.; Shirakami, Y.; Lindner, T.; Ooe, K.; Toyoshima, A.; Nagata, K.; Shimosegawa, E.; Haberkorn, U.; et al. Theranostics Targeting Fibroblast Activation Protein in the Tumor Stroma: (64)Cu- and (225)Ac-Labeled FAPI-04 in Pancreatic Cancer Xenograft Mouse Models. J. Nucl. Med. 2020, 61, 563–569. [Google Scholar] [CrossRef]
- Baldo, P.; Cecco, S. Amatuximab and novel agents targeting mesothelin for solid tumors. Onco Targets Ther. 2017, 10, 5337–5353. [Google Scholar] [CrossRef] [Green Version]
- Hatterer, E.; Chauchet, X.; Richard, F.; Barba, L.; Moine, V.; Chatel, L.; Broyer, L.; Pontini, G.; Bautzova, T.; Juan, F.; et al. Targeting a membrane-proximal epitope on mesothelin increases the tumoricidal activity of a bispecific antibody blocking CD47 on mesothelin-positive tumors. MAbs 2020, 12, 1739408. [Google Scholar] [CrossRef] [Green Version]
- Lamberts, L.E.; Menke-van der Houven, C.W.; ter Weele, E.J.; Bensch, F.; Smeenk, M.M.; Voortman, J.; Hoekstra, O.S.; Williams, S.P.; Fine, B.M.; Maslyar, D.; et al. ImmunoPET with Anti-Mesothelin Antibody in Patients with Pancreatic and Ovarian Cancer before Anti-Mesothelin Antibody-Drug Conjugate Treatment. Clin. Cancer Res. 2016, 22, 1642–1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, K.; Sasaki, T.; Takenaka, F.; Yakushiji, H.; Fujii, Y.; Kishi, Y.; Kita, S.; Shen, L.; Kumon, H.; Matsuura, E. A novel PET imaging using ⁶⁴Cu-labeled monoclonal antibody against mesothelin commonly expressed on cancer cells. J. Immunol. Res. 2015, 2015, 268172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caruz, A.; Samsom, M.; Alonso, J.; Alcami, J.; Baleux, F.; Virelizier, J.; Parmentier, M.; Arenzana-Seisdedos, F. Genomic organization and promoter characterization of human CXCR4 gene. FEBS Lett. 1998, 426, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruizinga, R.C.; Bestebroer, J.; Berghuis, P.; de Haas, C.J.C.; Links, T.P.; de Vries, E.G.E.; Walenkamp, A.M.E. Role of Chemokines and Their Receptors in Cancer. Curr. Pharm. Des. 2009, 15, 3396–3416. [Google Scholar] [CrossRef]
- Loetscher, P.; Moser, B.; Baggiolini, M. Chemokines and their receptors in lymphocyte traffic and HIV infection. Adv. Immunol. 2000, 74, 127–180. [Google Scholar]
- Balkwill, F. Cancer and the chemokine network. Nat. Rev. Cancer 2004, 4, 540–550. [Google Scholar] [CrossRef]
- Sun, X.; Cheng, G.; Hao, M.; Zheng, J.; Zhou, X.; Zhang, J.; Taichman, R.S.; Pienta, K.J.; Wang, J. CXCL12/CXCR4/CXCR7 chemokine axis and cancer progression. Cancer Metastasis Rev. 2010, 29, 709–722. [Google Scholar] [CrossRef] [Green Version]
- Guo, F.; Wang, Y.; Liu, J.; Mok, S.C.; Xue, F.; Zhang, W. CXCL12/CXCR4: A symbiotic bridge linking cancer cells and their stromal neighbors in oncogenic communication networks. Oncogene 2016, 35, 816–826. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Raderer, M.; Lamm, W.; Pichler, V.; Pfaff, S.; Weber, M.; Kiesewetter, B.; Hacker, M.; Kazianka, L.; Staber, P.B.; et al. CXCR4 PET imaging of mantle cell lymphoma using [(68)Ga]Pentixafor: Comparison with [(18)F]FDG-PET. Theranostics 2021, 11, 567–578. [Google Scholar] [CrossRef]
- Walenkamp, A.M.; Lapa, C.; Herrmann, K.; Wester, H.J. CXCR4 Ligands: The Next Big Hit? J. Nucl. Med. 2017, 58 (Suppl. 2), 77S–82S. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Brambilla, E.; Müller-Hermelink, H.K.; Harris, C.C. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. In WHO Classification of Tumours, 3rd ed; IARC Press: Lyon, France; Oxford University Press: Oxford, UK, 2004; Volume 10, 344p. [Google Scholar]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; Wiley-Blackwell: Chichester, UK; Hoboken, NJ, USA, 2010; 309p. [Google Scholar]
- Byrne, M.J.; Nowak, A.K. Modified RECIST criteria for assessment of response in malignant pleural mesothelioma. Ann. Oncol. 2004, 15, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Mairinger, F.D.; Vollbrecht, C.; Flom, E.; Christoph, D.C.; Schmid, K.-W.; Kollmeier, J.; Popper, H.H.; Mairinger, T.; Walter, R.F.H. Folic acid phenotype (FAP) is a superior biomarker predicting response to pemetrexed-based chemotherapy in malignant pleural mesothelioma. Oncotarget 2017, 8, 37502–37510. [Google Scholar] [CrossRef] [PubMed]
- Schmid, K.W.; Ellis, I.; Gee, J.M.W.; Darke, B.M.; Lees, W.E.; Kay, J.; Cryer, A.; Stark, J.M.; Hittmair, A.; Öfner, D.; et al. Presence and possible significance of immunocytochemically demonstrable metallothionein over-expression in primary invasive ductal carcinoma of the breast. Virchows Arch. A Pathol. Anat. Histopathol. 1993, 422, 153–159. [Google Scholar] [CrossRef]
- Goulding, H.; Jasani, B.; Pereira, H.; Reid, A.; Galea, M.; Bell, J.A.; Elston, C.W.; Robertson, J.F.; Blamey, R.W.; Nicholson, R.A.; et al. Metallothionein expression in human breast cancer. Br. J. Cancer 1995, 72, 968–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | 105 |
|---|---|
| Gender | |
| male | 84 |
| female | 21 |
| unknown Gender | 0 |
| Histological subtype | |
| epithelioid | 96 |
| biphasic | 5 |
| sarcomatoid | 4 |
| Age | |
| Mean|Median age at diagnosis (years) | 65|65 |
| Range (years) | 34–82 |
| OS | |
| Deceased | 88 |
| Alive | 14 |
| Lost-of-FU | 3 |
| Median|Mean OS (months) | 18.6|23.4 |
| Range (months) | 1.2–91.3 |
| PFS | |
| Partial remission (initial) | 7 |
| Stable disease (initial) | 42 |
| Progressive disease (initial) | 54 |
| Unknown response | 2 |
| Median|Mean PFS (months) | 7.5|12.2 |
| 95% CI | 5.9–12.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hager, T.; Borchert, S.; Wessolly, M.; Mathilakathu, A.; Mairinger, E.; Kollmeier, J.; Mairinger, T.; Hegedus, B.; Greimelmaier, K.; Wohlschlaeger, J.; et al. One Third of Malignant Pleural Mesothelioma Shows High Immunohistochemical Expression of MSLN or CXCR4 Which Indicates Potent Candidates for Endo-Radiotherapy. Int. J. Mol. Sci. 2023, 24, 6356. https://doi.org/10.3390/ijms24076356
Hager T, Borchert S, Wessolly M, Mathilakathu A, Mairinger E, Kollmeier J, Mairinger T, Hegedus B, Greimelmaier K, Wohlschlaeger J, et al. One Third of Malignant Pleural Mesothelioma Shows High Immunohistochemical Expression of MSLN or CXCR4 Which Indicates Potent Candidates for Endo-Radiotherapy. International Journal of Molecular Sciences. 2023; 24(7):6356. https://doi.org/10.3390/ijms24076356
Chicago/Turabian StyleHager, Thomas, Sabrina Borchert, Michael Wessolly, Alexander Mathilakathu, Elena Mairinger, Jens Kollmeier, Thomas Mairinger, Balazs Hegedus, Kristina Greimelmaier, Jeremias Wohlschlaeger, and et al. 2023. "One Third of Malignant Pleural Mesothelioma Shows High Immunohistochemical Expression of MSLN or CXCR4 Which Indicates Potent Candidates for Endo-Radiotherapy" International Journal of Molecular Sciences 24, no. 7: 6356. https://doi.org/10.3390/ijms24076356