
Autoantibodies against PIP4K2B and AKT3 Are Associated with Skin and Lung Fibrosis in Patients with Systemic Sclerosis
 , ,
, ,
Abstract
:1. Introduction
2. Results
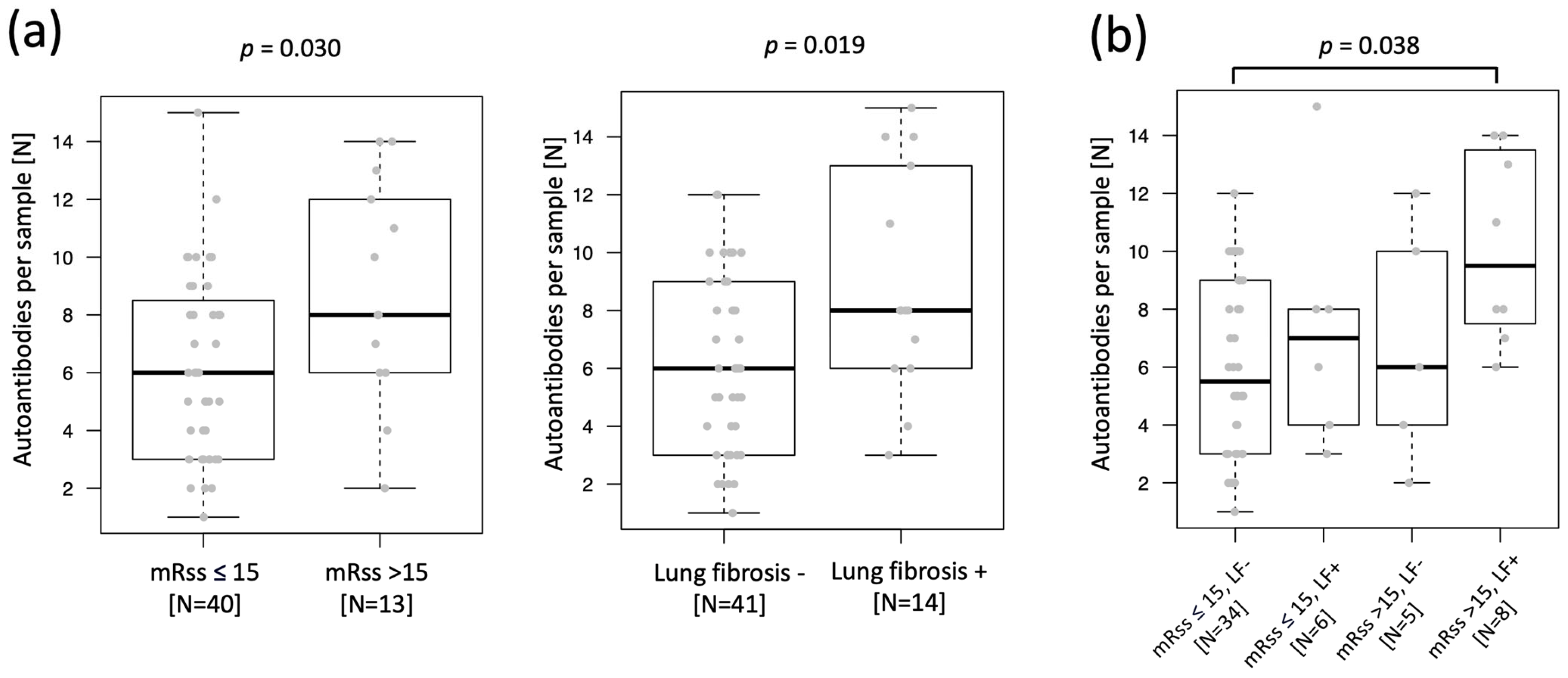
2.1. Increased Autoantibody Load in SSc Patients with Skin and Lung Fibrosis
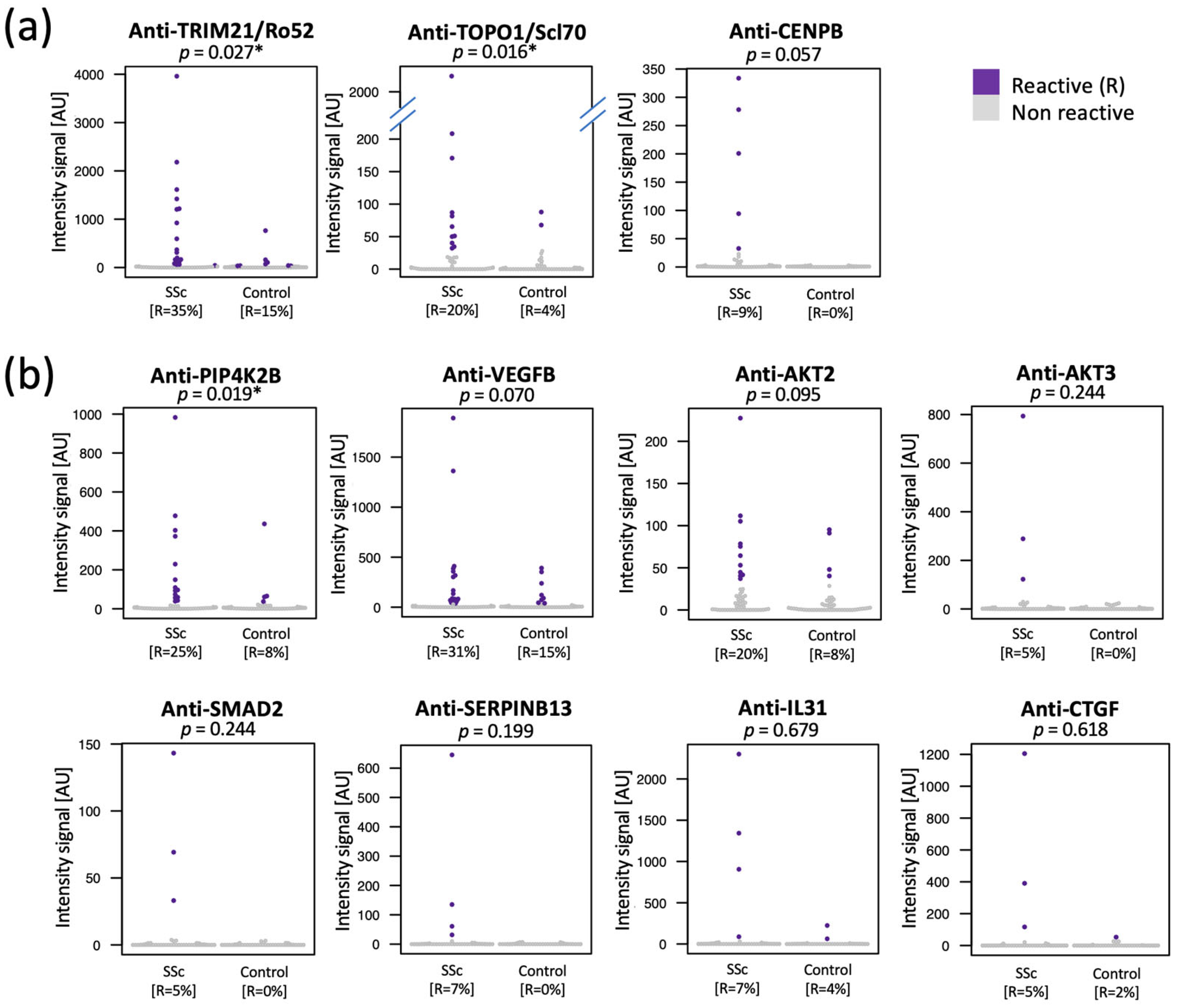
2.2. Selection of 11 Autoantibodies with Higher Prevalence in Plasma of SSc Patients and Reactive toward Fibrosis-Related Proteins
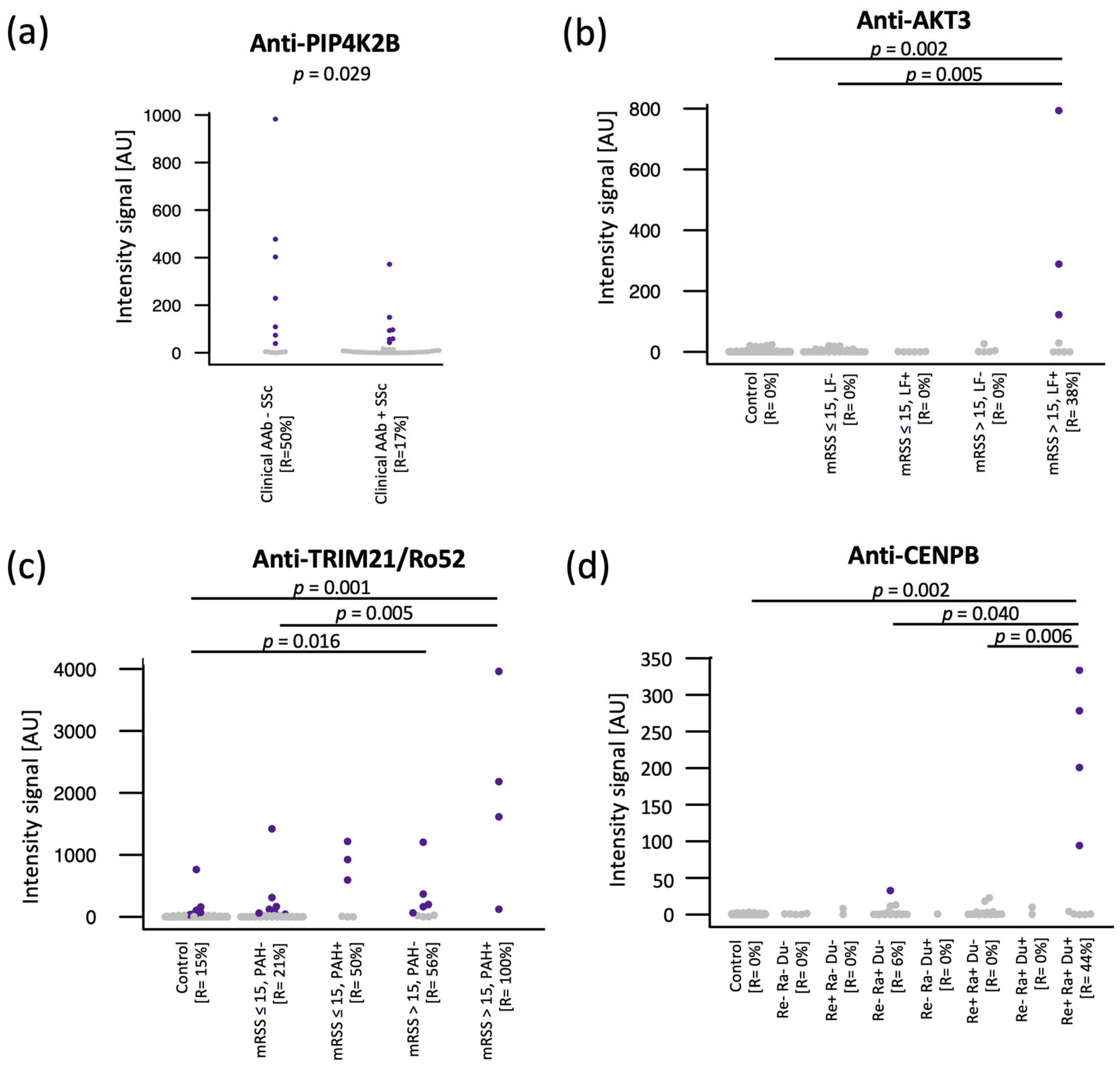
2.3. High Prevalence of Anti-PIP4K2B, Anti-AKT3, Anti-TRIM21/Ro52, and Anti-CENPB in Subgroups of SSc Patients
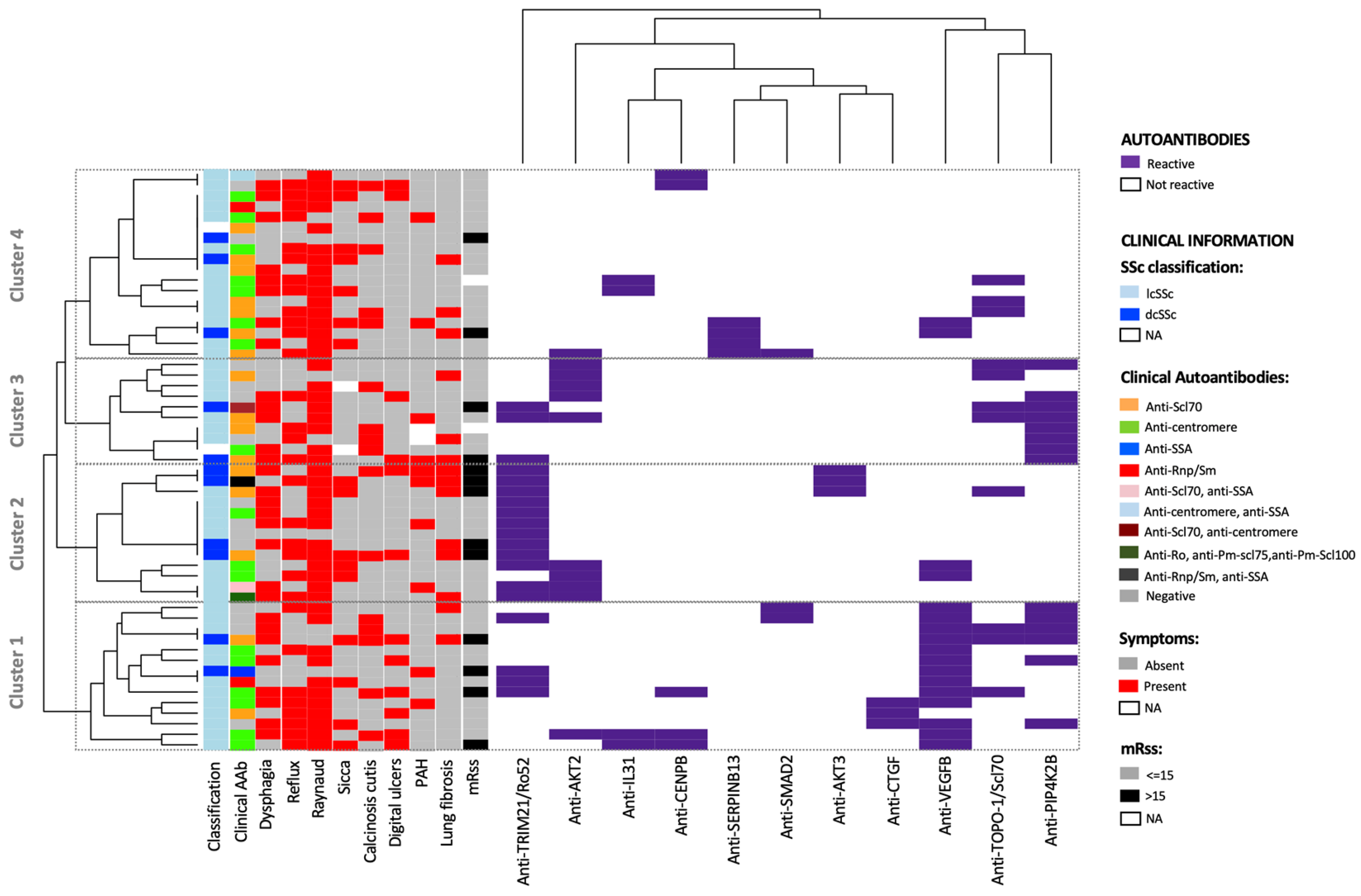
2.4. Autoantibody Combination and Cluster Analysis Separate Subgroups of SSc Patients with Skin and Lung Fibrosis
3. Discussion
4. Materials and Methods
4.1. Study Group
4.2. Study Design
4.3. Untargeted Autoantibody Screening by Proteome-Wide Planar Antigen Array
4.4. Targeted Autoantibody Screening Using Antigen Bead Array
4.5. Antigens
4.6. Data Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ingegnoli, F.; Ughi, N.; Mihai, C. Update on the epidemiology, risk factors, and disease outcomes of systemic sclerosis. Best Pract. Res. Clin. Rheumatol. 2018, 32, 223–240. [Google Scholar] [CrossRef] [PubMed]
- Elhai, M.; Meune, C.; Boubaya, M.; Avouac, J.; Hachulla, E.; Balbir-Gurman, A.; Riemekasten, G.; Airò, P.; Joven, B.; Vettori, S.; et al. Mapping and predicting mortality from systemic sclerosis. Ann. Rheum. Dis. 2017, 76, 1897–1905. [Google Scholar] [CrossRef]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steen, V.D. Autoantibodies in systemic sclerosis. Semin. Arthritis Rheum. 2005, 35, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Salazar, G.A.; Assassi, S.; Wigley, F.; Hummers, L.; Varga, J.; Hinchcliff, M.; Khanna, D.; Schiopu, E.; Phillips, K.; Furst, D.E.; et al. Antinuclear antibody-negative systemic sclerosis. Semin. Arthritis Rheum. 2015, 44, 680–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikpour, M.; Hissaria, P.; Byron, J.; Sahhar, J.; Micallef, M.; Paspaliaris, W.; Roddy, J.; Nash, P.; Sturgess, A.; Proudman, S.; et al. Prevalence, correlates and clinical usefulness of antibodies to RNA polymerase III in systemic sclerosis: A cross-sectional analysis of data from an Australian cohort. Arthritis Res. Ther. 2011, 13, R211. [Google Scholar] [CrossRef] [Green Version]
- Ceribelli, A.; Isailovic, N.; De Santis, M.; Gorlino, C.; Satoh, M.; Selmi, C. Autoantibodies as biomarkers for interstitial lung disease in idiopathic inflammatory myositis and systemic sclerosis: The case of anti-eIF2B antibodies. J. Transl. Autoimmun. 2020, 3, 100049. [Google Scholar] [CrossRef]
- Kuwana, M.; Allanore, Y.; Denton, C.P.; Distler, J.H.; Steen, V.; Khanna, D.; Matucci-Cerinic, M.; Mayes, M.D.; Volkmann, E.R.; Miede, C.; et al. Nintedanib in patients with systemic sclerosis-associated interstitial lung disease: Subgroup analyses by autoantibody status and skin score. Arthritis Rheumatol. 2022, 74, 518–526. [Google Scholar] [CrossRef]
- Kayser, C.; Fritzler, M.J. Autoantibodies in systemic sclerosis: Unanswered questions. Front. Immunol. 2015, 6, 167. [Google Scholar] [CrossRef]
- Assassi, S.; Sharif, R.; Lasky, R.E.; McNearney, T.A.; Estrada-Y-Martin, R.M.; Draeger, H.; Nair, D.K.; Fritzler, M.J.; Reveille, J.D.; Arnett, F.C.; et al. Predictors of interstitial lung disease in early systemic sclerosis: A prospective longitudinal study of the GENISOS cohort. Arthritis Res. Ther. 2010, 12, R166. [Google Scholar] [CrossRef] [Green Version]
- Uhlén, M.; Fagerberg, L.; Hallström, B.M.; Lindskog, C.; Oksvold, P.; Mardinoglu, A.; Sivertsson, Å.; Kampf, C.; Sjöstedt, E.; Asplund, A.; et al. Proteomics. Tissue-based map of the human proteome. Science 2015, 347, 1260419. [Google Scholar] [CrossRef] [PubMed]
- Ayoglu, B.; Mitsios, N.; Kockum, I.; Khademi, M.; Zandian, A.; Sjöberg, R.; Forsström, B.; Bredenberg, J.; Lima Bomfim, I.; Holmgren, E.; et al. Anoctamin 2 identified as an autoimmune target in multiple sclerosis. Proc. Natl. Acad. Sci. USA 2016, 113, 2188–2193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pin, E.; Petricoin, E.F.; Cortes, N.; Bowman, T.G.; Andersson, E.; Uhlén, M.; Nilsson, P.; Caswell, S.V. Immunoglobulin A Autoreactivity toward Brain Enriched and Apoptosis-Regulating Proteins in Saliva of Athletes after Acute Concussion and Subconcussive Impacts. J. Neurotrauma 2021, 38, 2373–2383. [Google Scholar] [CrossRef]
- Jernbom Falk, A.; Galletly, C.; Just, D.; Toben, C.; Baune, B.T.; Clark, S.R.; Liu, D.; Nilsson, P.; Månberg, A.; Schubert, K.O. Autoantibody profiles associated with clinical features in psychotic disorders. Transl. Psychiatry 2021, 11, 474. [Google Scholar] [CrossRef] [PubMed]
- Häggmark, A.; Hamsten, C.; Wiklundh, E.; Lindskog, C.; Mattsson, C.; Andersson, E.; Lundberg, I.E.; Grönlund, H.; Schwenk, J.M.; Eklund, A.; et al. Proteomic profiling reveals autoimmune targets in sarcoidosis. Am. J. Respir. Crit. Care Med. 2015, 191, 574–583. [Google Scholar] [CrossRef] [PubMed]
- Lourido, L.; Ruiz-Romero, C.; Picchi, F.; Diz-Rosales, N.; Vilaboa-Galán, S.; Fernández-López, C.; Pinto Tasende, J.A.; Pérez-Pampin, E.; Regueiro, C.; Mera-Varela, A.; et al. Association of serum anti-centromere protein F antibodies with clinical response to infliximab in patients with rheumatoid arthritis: A prospective study. Semin. Arthritis Rheum. 2020, 50, 1101–1108. [Google Scholar] [CrossRef]
- Neiman, M.; Hellström, C.; Just, D.; Mattsson, C.; Fagerberg, L.; Schuppe-Koistinen, I.; Gummesson, A.; Bergström, G.; Kallioniemi, O.; Achour, A.; et al. Individual and stable autoantibody repertoires in healthy individuals. Autoimmunity 2019, 52, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Shome, M.; Chung, Y.; Chavan, R.; Park, J.G.; Qiu, J.; LaBaer, J. Serum autoantibodyome reveals that healthy individuals share common autoantibodies. Cell Rep. 2022, 39, 110873. [Google Scholar] [CrossRef]
- Van Willis, C.; Demoruelle, M.K.; Derber, L.A.; Chartier-Logan, C.J.; Parish, M.C.; Pedraza, I.F.; Weisman, M.H.; Norris, J.M.; Holers, V.M.; Deane, K.D. Sputum autoantibodies in patients with established rheumatoid arthritis and subjects at risk of future clinically apparent disease. Arthritis Rheum. 2013, 65, 2545–2554. [Google Scholar] [CrossRef]
- Pisetsky, D.S.; Lipsky, P.E. New insights into the role of antinuclear antibodies in systemic lupus erythematosus. Nat. Rev. Rheumatol. 2020, 16, 565–579. [Google Scholar] [CrossRef]
- Lundquist, M.R.; Goncalves, M.D.; Loughran, R.M.; Possik, E.; Vijayaraghavan, T.; Yang, A.; Pauli, C.; Ravi, A.; Verma, A.; Yang, Z.; et al. Phosphatidylinositol-5-Phosphate 4-Kinases Regulate Cellular Lipid Metabolism By Facilitating Autophagy. Mol. Cell 2018, 70, 531–544.e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keune, W.-J.; Sims, A.H.; Jones, D.R.; Bultsma, Y.; Lynch, J.T.; Jirström, K.; Landberg, G. Low PIP4K2B expression in human breast tumors correlates with reduced patient survival: A role for PIP4K2B in the regulation of E-cadherin expression. Cancer Res. 2013, 73, 6913–6925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanjore, H.; Xu, X.C.; Polosukhin, V.V.; Degryse, A.L.; Li, B.; Han, W.; Sherrill, T.P.; Plieth, D.; Neilson, E.G.; Blackwell, T.S.; et al. Contribution of epithelial-derived fibroblasts to bleomycin-induced lung fibrosis. Am. J. Respir. Crit. Care Med. 2009, 180, 657–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Lamouille, S.; Derynck, R. TGF-beta-induced epithelial to mesenchymal transition. Cell Res. 2009, 19, 156–172. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Tang, Z.; Hou, X.; Lennartsson, J.; Li, Y.; Koch, A.W.; Scotney, P.; Lee, C.; Arjunan, P.; Dong, L.; et al. VEGF-B is dispensable for blood vessel growth but critical for their survival, and VEGF-B targeting inhibits pathological angiogenesis. Proc. Natl. Acad. Sci. USA 2009, 106, 6152–6157. [Google Scholar] [CrossRef] [Green Version]
- Falkevall, A.; Mehlem, A.; Palombo, I.; Heller Sahlgren, B.; Ebarasi, L.; He, L.; Ytterberg, A.J.; Olauson, H.; Axelsson, J.; Sundelin, B.; et al. Reducing VEGF-B Signaling Ameliorates Renal Lipotoxicity and Protects against Diabetic Kidney Disease. Cell Metab. 2017, 25, 713–726. [Google Scholar] [CrossRef] [Green Version]
- Muoio, D.M. Metabolism and vascular fatty acid transport. N. Engl. J. Med. 2010, 363, 291–293. [Google Scholar] [CrossRef]
- Louzier, V.; Raffestin, B.; Leroux, A.; Branellec, D.; Caillaud, J.M.; Levame, M.; Eddahibi, S.; Adnot, S. Role of VEGF-B in the lung during development of chronic hypoxic pulmonary hypertension. Am. J. Physiol. Lung Cell Mol. Physiol. 2003, 284, L926–L937. [Google Scholar] [CrossRef] [Green Version]
- Laddha, A.P.; Kulkarni, Y.A. VEGF and FGF-2: Promising targets for the treatment of respiratory disorders. Respir. Med. 2019, 156, 33–46. [Google Scholar] [CrossRef]
- Zanin-Silva, D.C.; Santana-Gonçalves, M.; Kawashima-Vasconcelos, M.Y.; Oliveira, M.C. Management of Endothelial Dysfunction in Systemic Sclerosis: Current and Developing Strategies. Front. Med. 2021, 8, 788250. [Google Scholar] [CrossRef]
- Distler, O.; Highland, K.B.; Gahlemann, M.; Azuma, A.; Fischer, A.; Mayes, M.D.; Raghu, G.; Sauter, W.; Girard, M.; Alves, M.; et al. Nintedanib for Systemic Sclerosis-Associated Interstitial Lung Disease. N. Engl. J. Med. 2019, 380, 2518–2528. [Google Scholar] [CrossRef] [PubMed]
- Jun, J.-B.; Kuechle, M.; Min, J.; Shim, S.C.; Kim, G.; Montenegro, V.; Korn, J.H.; Elkon, K.B. Scleroderma fibroblasts demonstrate enhanced activation of Akt (protein kinase B) in situ. J. Investig. Dermatol. 2005, 124, 298–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nie, Y.; Sun, L.; Wu, Y.; Yang, Y.; Wang, J.; He, H.; Hu, Y.; Chang, Y.; Liang, Q.; Zhu, J.; et al. AKT2 Regulates Pulmonary Inflammation and Fibrosis via Modulating Macrophage Activation. J. Immunol. 2017, 198, 4470–4480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revathidevi, S.; Munirajan, A.K. Akt in cancer: Mediator and more. Semin. Cancer Biol. 2019, 59, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Morrisroe, K.; Hansen, D.; Huq, M.; Stevens, W.; Sahhar, J.; Ngian, G.-S.; Ferdowsi, N.; Hill, C.; Roddy, J.; Walker, J.; et al. Incidence, Risk Factors, and Outcomes of Cancer in Systemic Sclerosis. Arthritis Care Res. 2020, 72, 1625–1635. [Google Scholar] [CrossRef]
- Morrisroe, K.; Nikpour, M. Cancer and scleroderma: Recent insights. Curr. Opin. Rheumatol. 2020, 32, 479–487. [Google Scholar] [CrossRef]
- Bonifazi, M.; Tramacere, I.; Pomponio, G.; Gabrielli, B.; Avvedimento, E.V.; La Vecchia, C.; Negri, E.; Gabrielli, A. Systemic sclerosis (scleroderma) and cancer risk: Systematic review and meta-analysis of observational studies. Rheumatology 2013, 52, 143–154. [Google Scholar] [CrossRef] [Green Version]
- Maria, A.T.; Partouche, L.; Goulabchand, R.; Rivière, S.; Rozier, P.; Bourgier, C.; Le Quellec, A.; Morel, J.; Noël, D.; Guilpain, P. Intriguing Relationships Between Cancer and Systemic Sclerosis: Role of the Immune System and Other Contributors. Front. Immunol. 2018, 9, 3112. [Google Scholar] [CrossRef] [Green Version]
- Takagi, K.; Kawaguchi, Y.; Kawamoto, M.; Ota, Y.; Tochimoto, A.; Gono, T.; Katsumata, Y.; Takagi, M.; Hra, M.; Yamanaka, H. Activation of the activin A-ALK-Smad pathway in systemic sclerosis. J. Autoimmun. 2011, 36, 181–188. [Google Scholar] [CrossRef]
- Lunardi, F.; Villano, G.; Perissinotto, E.; Agostini, C.; Rea, F.; Gnoato, M.; Bradaschia, A.; Valente, M.; Pontisso, P.; Calabrese, F. Overexpression of SERPIN B3 promotes epithelial proliferation and lung fibrosis in mice. Lab. Investig. 2011, 91, 945–954. [Google Scholar] [CrossRef] [Green Version]
- Makino, K.; Makino, T.; Stawski, L.; Lipson, K.E.; Leask, A.; Trojanowska, M. Anti-connective tissue growth factor (CTGF/CCN2) monoclonal antibody attenuates skin fibrosis in mice models of systemic sclerosis. Arthritis Res. Ther. 2017, 19, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldzizhar, R.; Fedorchuk, C.; Jha, M.; Rathinam, C.; Henegariu, O.; Czyzyk, J. Anti-serpin antibody-mediated regulation of proteases in autoimmune diabetes. J. Biol. Chem. 2013, 288, 1612–1619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaseen, B.; Lopez, H.; Taki, Z.; Zafar, S.; Rosario, H.; Abdi, B.A.; Vigneswaran, S.; Xing, F.; Arumalla, N.; Black, S.; et al. Interleukin-31 promotes pathogenic mechanisms underlying skin and lung fibrosis in scleroderma. Rheumatology 2020, 59, 2625–2636. [Google Scholar] [CrossRef] [PubMed]
- Kuzumi, A.; Yoshizaki, A.; Matsuda, K.M.; Kotani, H.; Norimatsu, Y.; Fukayama, M.; Ebata, S.; Fukasawa, T.; Yoshizaki-Ogawa, A.; Asano, Y.; et al. Interleukin-31 promotes fibrosis and T helper 2 polarization in systemic sclerosis. Nat. Commun. 2021, 12, 5947. [Google Scholar] [CrossRef]
- Bağci, I.S.; Ruzicka, T. IL-31: A new key player in dermatology and beyond. J. Allergy Clin. Immunol. 2018, 141, 858–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ständer, S.; Yosipovitch, G.; Legat, F.J.; Lacour, J.-P.; Paul, C.; Narbutt, J.; Bieber, T.; Misery, L.; Wollenberg, A.; Reich, A.; et al. Trial of Nemolizumab in Moderate-to-Severe Prurigo Nodularis. N. Engl. J. Med. 2020, 382, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.; Almeida, C.; Teixeira, A.; Oliveira, J.; Vasconcelos, C. Impaired angiogenesis as a feature of digital ulcers in systemic sclerosis. Clin. Rheumatol. 2016, 35, 1743–1751. [Google Scholar] [CrossRef]
- Hudson, M.; Pope, J.; Mahler, M.; Tatibouet, S.; Steele, R.; Baron, M.; Canadian Scleroderma Research Group (CSRG); Fritzer, M.J. Clinical significance of antibodies to Ro52/TRIM21 in systemic sclerosis. Arthritis Res. Ther. 2012, 14, R50. [Google Scholar] [CrossRef] [Green Version]
- Sobanski, V.; Giovannelli, J.; Allanore, Y.; Riemekasten, G.; Airò, P.; Vettori, S.; Cozzi, F.; Distler, O.; Matucci-Cerinic, M.; Denton, C.; et al. Phenotypes Determined by Cluster Analysis and Their Survival in the Prospective European Scleroderma Trials and Research Cohort of Patients With Systemic Sclerosis. Arthritis Rheumatol. 2019, 71, 1553–1570. [Google Scholar] [CrossRef] [Green Version]
- Cozzani, E.; Muracchioli, A.; Murdaca, G.; Beccalli, M.; Caprioli, S.; Zentilin, P.; Ameri, P.; Grosso, M.; Russo, R.; Carmisciano, L.; et al. Correlation Between Skin and Affected Organs in 52 Sclerodermic Patients Followed in a Diseases Management Team: Development of a Risk Prediction Model of Organ-Specific Complications. Front. Immunol. 2021, 12, 588753. [Google Scholar] [CrossRef]
- Becker, M.; Graf, N.; Sauter, R.; Allanore, Y.; Curram, J.; Denton, C.P.; Khanna, D.; Matucci-Cerinic, M.; de Oliveira Pena, J.; Pope, J.E.; et al. Predictors of disease worsening defined by progression of organ damage in diffuse systemic sclerosis: A European Scleroderma Trials and Research (EUSTAR) analysis. Ann. Rheum. Dis. 2019, 78, 1242–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ledoult, E.; Launay, D.; Béhal, H.; Mouthon, L.; Pugnet, G.; Lega, J.-C.; Agard, C.; Allanore, Y.; Jego, P.; Fauchais, A.-L.; et al. Early trajectories of skin thickening are associated with severity and mortality in systemic sclerosis. Arthritis Res. Ther. 2020, 22, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Galdo, F.; Hartley, C.; Allanore, Y. Randomised controlled trials in systemic sclerosis: Patient selection and endpoints for next generation trials. Lancet Rheumatol. 2020, 2, e173–e184. [Google Scholar] [CrossRef]
- Sjöberg, R.; Andersson, E.; Hellström, C.; Mattsson, C.; Schwenk, J.M.; Nilsson, P.; Ayoglu, B. High-Density Antigen Microarrays for the Assessment of Antibody Selectivity and Off-Target Binding. Methods Mol. Biol. 2018, 1785, 231–238. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group | SSc Patients | Controls |
|---|---|---|
| Number, N | 55 | 52 |
| Female/male, N (%) | 46 (84%)/9 (16%) | 39 (75%)/13 (25%) |
| Age, median (range) | 61 (25–85) | 53 (21–79) |
| Limited SSc/diffuse SSc/no sclerosis, N | 42/11/2 | - |
| Disease duration, Y, median (range) | 7 (0–37) | |
| mRSScore, median (range) | 9 (0–46) | - |
| Autoantibodies, N | ||
| Anti-Scl70 | 18 | - |
| Anti-centromere | 19 | - |
| Anti-SSA/Ro | 4 | - |
| Anti-Rnp/Sm | 3 | - |
| Negative to anti-Scl70 and -centromere | 14 | - |
| Clinical manifestations, N | ||
| Calcinosis cutis | 16 | - |
| Digital ulcers | 12 | - |
| Dysphagia | 29 | - |
| Lung fibrosis | 14 | - |
| PAH | 20 | - |
| Raynaud | 47 | - |
| Reflux | 30 | - |
| Sicca | 16 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geroldinger-Simić, M.; Bayati, S.; Pohjanen, E.; Sepp, N.; Nilsson, P.; Pin, E. Autoantibodies against PIP4K2B and AKT3 Are Associated with Skin and Lung Fibrosis in Patients with Systemic Sclerosis. Int. J. Mol. Sci. 2023, 24, 5629. https://doi.org/10.3390/ijms24065629
Geroldinger-Simić M, Bayati S, Pohjanen E, Sepp N, Nilsson P, Pin E. Autoantibodies against PIP4K2B and AKT3 Are Associated with Skin and Lung Fibrosis in Patients with Systemic Sclerosis. International Journal of Molecular Sciences. 2023; 24(6):5629. https://doi.org/10.3390/ijms24065629
Chicago/Turabian StyleGeroldinger-Simić, Marija, Shaghayegh Bayati, Emmie Pohjanen, Norbert Sepp, Peter Nilsson, and Elisa Pin. 2023. "Autoantibodies against PIP4K2B and AKT3 Are Associated with Skin and Lung Fibrosis in Patients with Systemic Sclerosis" International Journal of Molecular Sciences 24, no. 6: 5629. https://doi.org/10.3390/ijms24065629