
Prevalence of Neutralizing Antibodies against Adeno-Associated Virus Serotypes 1, 2, and 9 in Non-Injected Latin American Patients with Heart Failure—ANVIAS Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. NAbs Prevalence and Differences between the Analyzed Groups
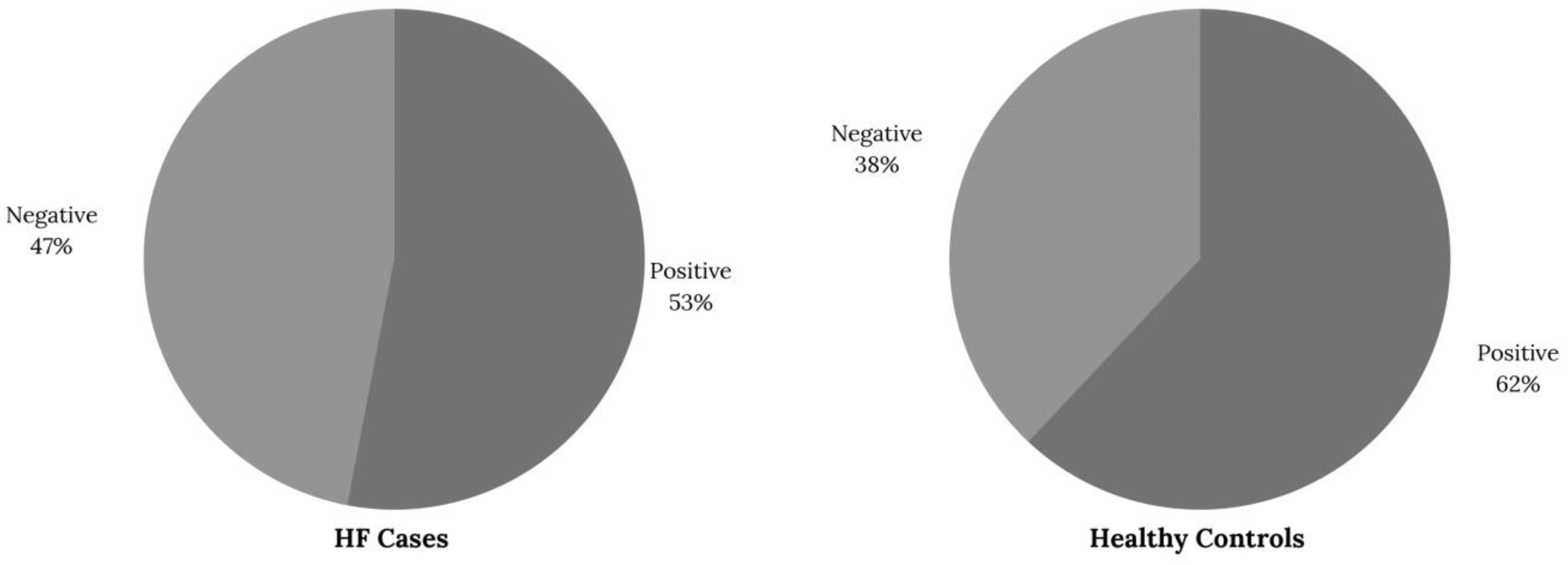
2.2. The Combined Prevalence of NAbs Anti-AAV in HF Patients
2.3. Socioeconomic Factors Related to the Prevalence of NAbs Anti-AAV
3. Discussion
Study Strengths and Limitations
4. Materials and Methods
4.1. Patients and Samples
4.2. Cell Culture and Neutralizing Antibody Assay
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rincon, M.Y.; VandenDriessche, T.; Chuah, M.K. Gene therapy for cardiovascular disease: Advances in vector development, targeting, and delivery for clinical translation. Cardiovasc. Res. 2015, 108, 4–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calcedo, R.; Vandenberghe, L.H.; Gao, G.; Lin, J.; Wilson, J.M. Worldwide epidemiology of neutralizing antibodies to adeno-associated viruses. J. Infect. Dis. 2009, 199, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Jungmann, A.; Müller, O.; Rapti, K. Cell-Based Measurement of Neutralizing Antibodies Against Adeno-Associated Virus (AAV). Methods Mol. Biol. 2017, 1521, 109–126. [Google Scholar] [CrossRef] [PubMed]
- Mingozzi, F.; High, K.A. Immune responses to AAV vectors: Overcoming barriers to successful gene therapy. Blood 2013, 122, 23–36. [Google Scholar] [CrossRef]
- Halbert, C.L.; Miller, A.D.; McNamara, S.; Emerson, J.; Gibson, R.L.; Ramsey, B.; Aitken, M.L. Prevalence of neutralizing antibodies against adeno-associated virus (AAV) types 2, 5, and 6 in cystic fibrosis and normal populations: Implications for gene therapy using AAV vectors. Hum. Gene Ther. 2006, 17, 440–447. [Google Scholar] [CrossRef] [Green Version]
- Kruzik, A.; Fetahagic, D.; Hartlieb, B.; Dorn, S.; Koppensteiner, H.; Horling, F.M.; Scheiflinger, F.; Reipert, B.M.; de la Rosa, M. Prevalence of Anti-Adeno-Associated Virus Immune Responses in International Cohorts of Healthy Donors. Mol. Ther. Methods Clin. Dev. 2019, 14, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Louis Jeune, V.; Joergensen, J.A.; Hajjar, R.J.; Weber, T. Pre-existing anti-adeno-associated virus antibodies as a challenge in AAV gene therapy. Hum. Gene Ther. Methods 2013, 24, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Calcedo, R.; Morizono, H.; Wang, L.; McCarter, R.; He, J.; Jones, D.; Batshaw, M.L.; Wilson, J.M. Adeno-associated virus antibody profiles in newborns, children, and adolescents. Clin. Vaccine Immunol. 2011, 18, 1586–1588. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, B.; Butler, J.; Felker, G.M.; Ponikowski, P.; Voors, A.A.; Pogoda, J.M.; Provost, R.; Guerrero, J.; Hajjar, R.J.; Zsebo, K.M. Prevalence of AAV1 neutralizing antibodies and consequences for a clinical trial of gene transfer for advanced heart failure. Gene Ther. 2016, 23, 313–319. [Google Scholar] [CrossRef]
- Klamroth, R.; Hayes, G.; Andreeva, T.; Gregg, K.; Suzuki, T.; Mitha, I.H.; Hardesty, B.; Shima, M.; Pollock, T.; Slev, P.; et al. Global Seroprevalence of Pre-existing Immunity Against AAV5 and Other AAV Serotypes in People with Hemophilia A. Hum. Gene Ther. 2022, 33, 432–441. [Google Scholar] [CrossRef]
- Rincon, M.Y.; Prada, C.E.; Lopez, M.; Castillo, V.; Echeverria, L.E.; Serrano, N. Determination of Anti-Adeno-Associated Viral Vector Neutralizing Antibodies in Patients with Heart Failure in the Cardiovascular Foundation of Colombia (ANVIAS): Study Protocol. JMIR Res. Protoc. 2016, 5, e102. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- Bocchi, E.A. Heart failure in South America. Curr. Cardiol. Rev. 2013, 9, 147–156. [Google Scholar]
- SISPRO, Integral system of social information, Ministry of Social Protection, Mortality due to Heart Failure and in Colombia in 2016. Available online: http://www.sispro.gov.co/Pages/TC_PDSP.aspx (accessed on 23 August 2020).
- Greenberg, B. Gene therapy for heart failure. Trends Cardiovasc. Med. 2017, 27, 216–222. [Google Scholar] [CrossRef]
- Blacklow, N.R.; Hoggan, M.D.; Kapikian, A.Z.; Austin, J.B.; Rowe, W.P. Epidemiology of adenovirus-associated virus infection in a nursery population. Am. J. Epidemiol. 1968, 88, 368–378. [Google Scholar] [CrossRef]
- Blacklow, N.R.; Hoggan, M.D.; Rowe, W.P. Serologic evidence for human infection with adenovirus-associated viruses. J. Natl. Cancer Inst. 1968, 40, 319–327. [Google Scholar]
- Lugin, M.L.; Lee, R.T.; Kwon, Y.J. Synthetically Engineered Adeno-Associated Virus for Efficient, Safe, and Versatile Gene Therapy Applications. ACS Nano 2020, 14, 14262–14283. [Google Scholar] [CrossRef]
- Harbison, C.E.; Weichert, W.S.; Gurda, B.L.; Chiorini, J.A.; Agbandje-McKenna, M.; Parrish, C.R. Examining the cross-reactivity and neutralization mechanisms of a panel of mAbs against adeno-associated virus serotypes 1 and 5. J. Gen. Virol. 2012, 93, 347–355. [Google Scholar] [CrossRef]
- Moskalenko, M.; Chen, L.; van Roey, M.; Donahue, B.A.; Snyder, R.O.; McArthur, J.G.; Patel, S.D. Epitope mapping of human anti-adeno-associated virus type 2 neutralizing antibodies: Implications for gene therapy and virus structure. J. Virol. 2000, 74, 1761–1766. [Google Scholar] [CrossRef] [Green Version]
- Kashiwakura, Y.; Baatartsogt, N.; Yamazaki, S.; Nagao, A.; Amano, K.; Suzuki, N.; Matsushita, T.; Sawada, A.; Higasa, S.; Yamasaki, N.; et al. The seroprevalence of neutralizing antibodies against the adeno-associated virus capsids in Japanese hemophiliacs. Mol. Ther. Methods Clin. Dev. 2022, 27, 404–414. [Google Scholar] [CrossRef]
- Khatri, A.; Shelke, R.; Guan, S.; Somanathan, S. Higher Seroprevalence of Anti-Adeno-Associated Viral Vector Neutralizing Antibodies among Racial Minorities in the United States. Hum. Gene Ther. 2022, 33, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Mendell, J.R.; Connolly, A.M.; Lehman, K.J.; Griffin, D.A.; Khan, S.Z.; Dharia, S.D.; Quintana-Gallardo, L.; Rodino-Klapac, L.R. Testing preexisting antibodies prior to AAV gene transfer therapy: Rationale, lessons and future considerations. Mol. Ther. Methods Clin. Dev. 2022, 25, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Aronson, S.J.; Veron, P.; Collaud, F.; Hubert, A.; Delahais, V.; Honnet, G.; de Knegt, R.J.; Junge, N.; Baumann, U.; Di Giorgio, A.; et al. Prevalence and Relevance of Pre-Existing Anti-Adeno-Associated Virus Immunity in the Context of Gene Therapy for Crigler-Najjar Syndrome. Hum. Gene Ther. 2019, 30, 1297–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniel, H.D.-J.; Kumar, S.; Kannangai, R.; Lakshmi, K.M.; Agbandje-Mckenna, M.; Coleman, K.; Srivastava, A.; Srivastava, A.; Abraham, A.M. Prevalence of Adeno-Associated Virus 3 Capsid Binding and Neutralizing Antibodies in Healthy and Hemophilia B Individuals from India. Hum. Gene Ther. 2021, 32, 451–457. [Google Scholar] [CrossRef]
- Stolte, B.; Schreiber-Katz, O.; Günther, R.; Wurster, C.D.; Petri, S.; Osmanovic, A.; Freigang, M.; Uzelac, Z.; Leo, M.; von Velsen, O.; et al. Prevalence of Anti-Adeno-Associated Virus Serotype 9 Antibodies in Adult Patients with Spinal Muscular Atrophy. Hum. Gene Ther. 2022, 33, 968–976. [Google Scholar] [CrossRef]
- Li, C.; Narkbunnam, N.; Samulski, R.J.; Asokan, A.; Hu, G.; Jacobson, L.J.; Manco-Johnson, M.J.; Monahan, P.E. Joint Outcome Study Investigators Neutralizing antibodies against adeno-associated virus examined prospectively in pediatric patients with hemophilia. Gene Ther. 2012, 19, 288–294. [Google Scholar] [CrossRef] [Green Version]
- Leborgne, C.; Latournerie, V.; Boutin, S.; Desgue, D.; Quéré, A.; Pignot, E.; Collaud, F.; Charles, S.; Simon Sola, M.; Masat, E.; et al. Prevalence and long-term monitoring of humoral immunity against adeno-associated virus in Duchenne Muscular Dystrophy patients. Cell. Immunol. 2019, 342, 103780. [Google Scholar] [CrossRef]
- Ling, C.; Wang, Y.; Feng, Y.; Zhang, Y.; Li, J.; Hu, X.; Wang, L.; Zhong, M.; Zhai, X.; Zolotukhin, I.; et al. Prevalence of neutralizing antibodies against liver-tropic adeno-associated virus serotype vectors in 100 healthy Chinese and its potential relation to body constitutions. J. Integr. Med. 2015, 13, 341–346. [Google Scholar] [CrossRef]
- Kononenko, V.; Narat, M.; Drobne, D. Nanoparticle interaction with the immune system. Arh. Hig. Rada Toksikol. 2015, 66, 97–108. [Google Scholar] [CrossRef] [Green Version]
- Erles, K.; Sebökovà, P.; Schlehofer, J.R. Update on the prevalence of serum antibodies (IgG and IgM) to adeno-associated virus (AAV). J. Med. Virol. 1999, 59, 406–411. [Google Scholar] [CrossRef]
- Chirmule, N.; Propert, K.; Magosin, S.; Qian, Y.; Qian, R.; Wilson, J. Immune responses to adenovirus and adeno-associated virus in humans. Gene Ther. 1999, 6, 1574–1583. [Google Scholar] [CrossRef] [Green Version]
- Wagner, J.A.; Nepomuceno, I.B.; Messner, A.H.; Moran, M.L.; Batson, E.P.; Dimiceli, S.; Brown, B.W.; Desch, J.K.; Norbash, A.M.; Conrad, C.K.; et al. A phase II, double-blind, randomized, placebo-controlled clinical trial of tgAAVCF using maxillary sinus delivery in patients with cystic fibrosis with antrostomies. Hum. Gene Ther. 2002, 13, 1349–1359. [Google Scholar] [CrossRef]
- Murphy, S.L.; Li, H.; Mingozzi, F.; Sabatino, D.E.; Hui, D.J.; Edmonson, S.A.; High, K.A. Diverse IgG subclass responses to adeno-associated virus infection and vector administration. J. Med. Virol. 2009, 81, 65–74. [Google Scholar] [CrossRef] [Green Version]
- Boutin, S.; Monteilhet, V.; Veron, P.; Leborgne, C.; Benveniste, O.; Montus, M.F.; Masurier, C. Prevalence of serum IgG and neutralizing factors against adeno associated virus (AAV) types 1, 2, 5, 6, 8, and 9 in the healthy population: Implications for gene therapy using AAV vectors. Hum. Gene Ther. 2010, 21, 704–712. [Google Scholar] [CrossRef]
- Van der Marel, S.; Comijn, E.M.; Verspaget, H.W.; van Deventer, S.; van den Brink, G.R.; Petry, H.; Hommes, D.W.; Ferreira, V. Neutralizing antibodies against adeno-associated viruses in inflammatory bowel disease patients: Implications for gene therapy. Inflamm. Bowel Dis. 2011, 17, 2436–2442. [Google Scholar] [CrossRef]
- Veron, P.; Leborgne, C.; Monteilhet, V.; van Deventer, S.; van den Brink, G.R.; Petry, H.; Hommes, D.W.; Ferreira, V. Humoral and cellular capsid-specific immune responses to adenoassociated virus type 1 in randomized healthy donors. J. Immunol. 2012, 188, 6418–6424. [Google Scholar] [CrossRef] [Green Version]
- Gray, S.J.; Nagabhushan Kalburgi, S.; McCown, T.J.; Jude Samulski, R. Global CNS gene delivery and evasion of anti-AAV-neutralizing antibodies by intrathecal AAV administration in non-human primates. Gene Ther. 2013, 20, 450–459. [Google Scholar]
- Mimuro, J.; Mizukami, H.; Shima, M.; Matsushita, T.; Taki, M.; Muto, S.; Higasa, S.; Sakai, M.; Ohmori, T.; Madoiwa, S.; et al. The prevalence of neutralizing antibodies against adeno-associated virus capsids is reduced in young Japanese individuals. J. Med. Virol. 2014, 86, 1990–1997. [Google Scholar] [CrossRef]
- Ferla, R.; Claudiani, P.; Savarese, M.; Kozarsky, K.; Parini, R.; Scarpa, M.; Donati, M.A.; Sorge, G.; Hopwood, J.J.; Parenti, G.; et al. Prevalence of anti-adeno-associated virus serotype 8 neutralizing antibodies and arylsulfatase B cross-reactive immunologic material in mucopolysaccharidosis VI patient candidates for a gene therapy trial. Hum. Gene Ther. 2015, 26, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Harrington, E.A.; Sloan, J.L.; Manoli, I.; Chandler, R.J.; Schneider, M.; McGuire, P.J.; Calcedo, R.; Wilson, J.M.; Venditti, C.P. Neutralizing antibodies against adeno-associated viral capsids in patientswith mut methylmalonic acidemia. Hum. Gene Ther. 2016, 27, 345–353. [Google Scholar] [CrossRef] [Green Version]
- Ellsworth, J.L.; OCallaghan, M.; Rubin, H.; Seymour, A. Low seroprevalence of neutralizing antibodies targeting two Clade F AAV in humans. Hum. Gene Ther. Clin. Dev. 2018, 29, 60–67. [Google Scholar] [PubMed]
- Liu, Q.; Huang, W.; Zhao, C.; Zhang, L.; Meng, S.; Gao, D.; Wang, Y. The prevalence of neutralizing antibodies against AAV serotype 1 in healthy subjects in China: Implications for gene therapy and vaccines using AAV1 vector. J. Med. Virol. 2013, 85, 1550–1556. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| HF Cases (N = 60) | Healthy Controls (N = 60) | p-Value | |
|---|---|---|---|
| Age | 62 (51.8, 72) | 61 (52, 71) | 0.655 |
| Male sex | 46 (76.7%) | 46 (76.7%) | 1.000 |
| Race | 0.074 | ||
| Hispanic | 55 (91.7%) | 60 (100.0%) | |
| African-American | 4 (6.7%) | 0 (0.0%) | |
| White | 1 (1.7%) | 0 (0.0%) | |
| Origin | 0.032 | ||
| Rural Area | 36 (57,9%) | 30(50%) | |
| Urban Area | 24 (42,1%) | 30(50%) | |
| T2DM | 12 (20.0%) | 9 (15.0%) | 0.471 |
| Hypertension | 35 (58.3%) | 24 (40.0%) | 0.045 |
| Dyslipidemia | 21 (35.0%) | 8 (13.3%) | 0.015 |
| Renal Disease | 16 (26.7%) | 5 (8.3%) | 0.008 |
| Obesity/Overweight | 29 (48.3%) | 37 (61.7%) | 0.142 |
| AMI | 26 (43.3%) | 2 (3.3%) | <0.001 |
| Years with HF | 4 (2, 7) | NA | |
| HF Stage | NA | ||
| A | 1 (1.7%) | - | |
| B | 49 (81.7%) | - | |
| C | 10 (16.7%) | - | |
| Hospitalized during the last year | 40 (66.7%) | 0 (0%) | NA |
| Physical activity | 43 (71.7%) | 42 (70.0%) | 0.841 |
| Minutes of exercise per day | 30 (0, 60) | 30 (0, 60) | 0.603 |
| Exercise days per week | 5 (0, 7) | 2 (0, 6) | 0.047 |
| Surgery during the last year | 46 (76.7%) | 38 (63.3%) | 0.111 |
| Toxic exposure during the last year | 16 (26.7%) | 21 (35.0%) | 0.323 |
| Allergies | 11 (18.3%) | 8 (13.3%) | 0.453 |
| Hemoglobin | 13.3 (12.2, 14.2) | - | NA |
| Leukocytes | 6.9 (5.6, 8.2) | - | NA |
| Platelets | 213 (178.5, 250.5) | - | NA |
| LVEF | 30 (20, 45) | - | NA |
| Garbage disposal | 52 (86.7%) | 60 (100.0%) | 0.003 |
| Sewage system | 51 (85.0%) | 60 (100.0%) | 0.002 |
| Traveling during the last year | 29 (48.3%) | 8 (13.3%) | <0.001 |
| AAV1 Seropositivity | 20 (33.3%) | 20 (33.3%) | 1.000 |
| AAV2 Seropositivity | 26 (43.3%) | 27 (45.0%) | 0.854 |
| AAV9 Seropositivity | 12 (20.0%) | 14 (23.3%) | 0.658 |
| AAV1 † | AAV2 † | AAV9 † | |
|---|---|---|---|
| HF cases | |||
| AAV1 † | - | 75% AAV2 † (n = 15/20) | 55% AAV9 † (n = 11/20) |
| AAV2 † | 57.6% AAV1+ (n = 15/26) | - | 42.3% AAV9 † (n = 11/26) |
| AAV9 † | 91.6% AAV1+ (n = 11/12) † | 91.6% AAV2 † (n = 11/12) | - |
| Healthy donors | |||
| AAV1 † | - | 50% AAV2 † (n = 10/20) | 25% AAV9 † (n = 5/20) |
| AAV2 † | 37% AAV1 † (n = 10/27) | - | 44.4% AAV9 † (n = 12/27) |
| AAV9 † | 35.7% AAV1 † (n = 5/14) | 85.8% AAV2 † (n = 12/14) | - |
| OR | CI (95%) | p-Value | |
|---|---|---|---|
| Toxic exposition | 22.72 | [20.42; 25.01] | 0.007 |
| Previous surgery | 14.65 | [12.59; 16.74] | 0.015 |
| Access to potable water | 6.00 × 10−10 | [3.4 × 10−156; 4744] | 0.999 |
| Access to proper garbage disposal | 3.3010−9 | [NA; 3.83 × 10113] | 0.999 |
| Previous hospitalization | 4.44 | [2.89; 5.98] | 0.058 |
| Travel in the last year | 0.29 | [0.85; 15] | 0.093 |
| CATEGORY | Independent Variable | OR | CI (95%) | p-Value |
|---|---|---|---|---|
| “ONE”: Positive for only one serotype evaluated | Toxic exposition | 2.97 | [1.03; 8.56] | 0.001 |
| Allergies | 3.05 | [0.8; 11.3] | 0.43 | |
| Previous hospitalization | 3.58 | [0.8; 15.2] | 0.001 | |
| Sewerage system | 9.48 × 10−10 | [6.6 × 10−122; 1.35 × 10103] | 0.24 | |
| Place of residence | 4.01 × 10−20 | [5.1 × 10−33; 3.15 × 10−7] | 0.95 | |
| Access to potable water | 3.33 × 10−11 | [1.78 × 10−110; 6.22 × 1088] | 0.43 | |
| “MULTIPLE”: Positive for multiple serotypes evaluated | Toxic exposition | 0.55 | [0.1; 1.54] | 0.41 |
| Allergies | 0.87 | [0.2; 3] | 0.41 | |
| Previous hospitalization | 0.5 | [0.07; 3.3] | 0.12 | |
| Sewerage system | 2.93 × 10−15 | [6.27 × 10−179; 1.37 × 10149] | 0.47 | |
| Place of residence | 7.53 × 10−21 | [9.57 × 10−34; 5.9 × 10−8) | 0.97 | |
| Access to potable water | 1.88 × 10−5 | [5.2 × 10−182; 6.7 × 10171] | 0.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sierra-Delgado, J.A.; Likhite, S.; Bautista, P.K.; Gómez-Ochoa, S.A.; Echeverría, L.E.; Guío, E.; Vargas, C.; Serrano, N.C.; Meyer, K.C.; Rincon, M.Y. Prevalence of Neutralizing Antibodies against Adeno-Associated Virus Serotypes 1, 2, and 9 in Non-Injected Latin American Patients with Heart Failure—ANVIAS Study. Int. J. Mol. Sci. 2023, 24, 5579. https://doi.org/10.3390/ijms24065579
Sierra-Delgado JA, Likhite S, Bautista PK, Gómez-Ochoa SA, Echeverría LE, Guío E, Vargas C, Serrano NC, Meyer KC, Rincon MY. Prevalence of Neutralizing Antibodies against Adeno-Associated Virus Serotypes 1, 2, and 9 in Non-Injected Latin American Patients with Heart Failure—ANVIAS Study. International Journal of Molecular Sciences. 2023; 24(6):5579. https://doi.org/10.3390/ijms24065579
Chicago/Turabian StyleSierra-Delgado, Julieth A., Shibi Likhite, Paula K. Bautista, Sergio A. Gómez-Ochoa, Luis E. Echeverría, Elizabeth Guío, Clara Vargas, Norma C. Serrano, Kathrin C. Meyer, and Melvin Y. Rincon. 2023. "Prevalence of Neutralizing Antibodies against Adeno-Associated Virus Serotypes 1, 2, and 9 in Non-Injected Latin American Patients with Heart Failure—ANVIAS Study" International Journal of Molecular Sciences 24, no. 6: 5579. https://doi.org/10.3390/ijms24065579