
Advances in Boron Neutron Capture Therapy (BNCT) for Recurrent Intracranial Meningioma
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
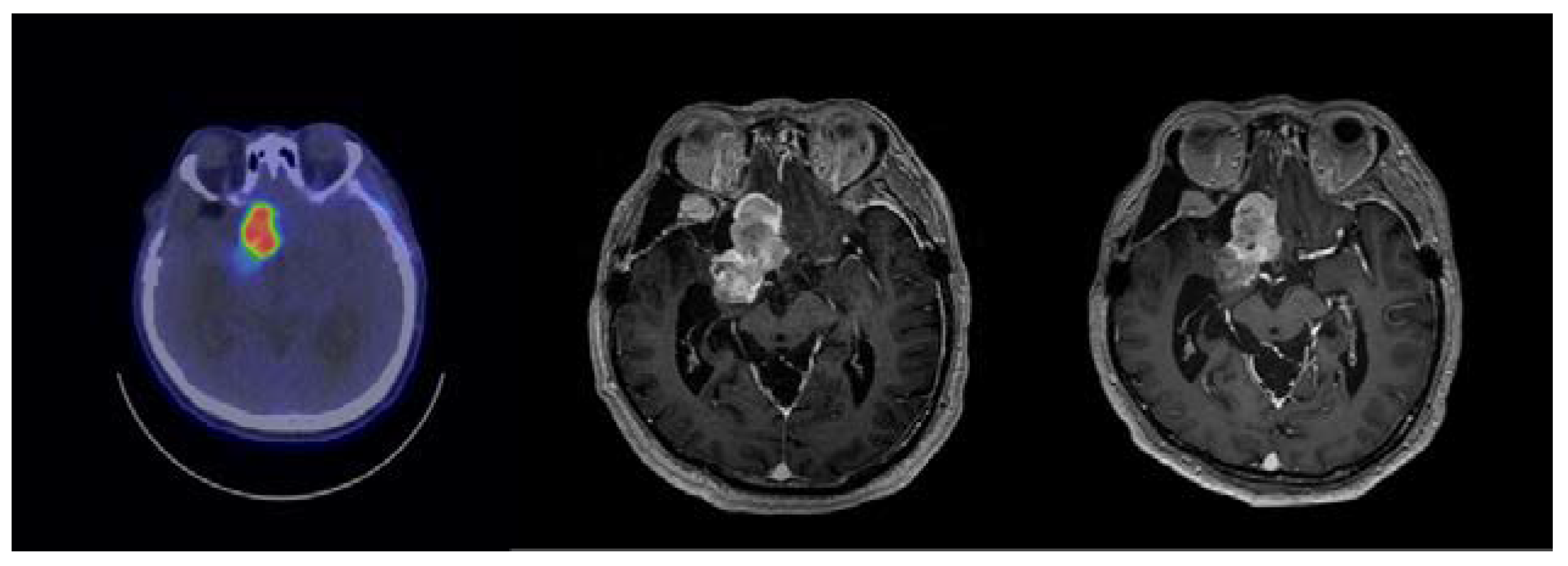
2.1. Case 115
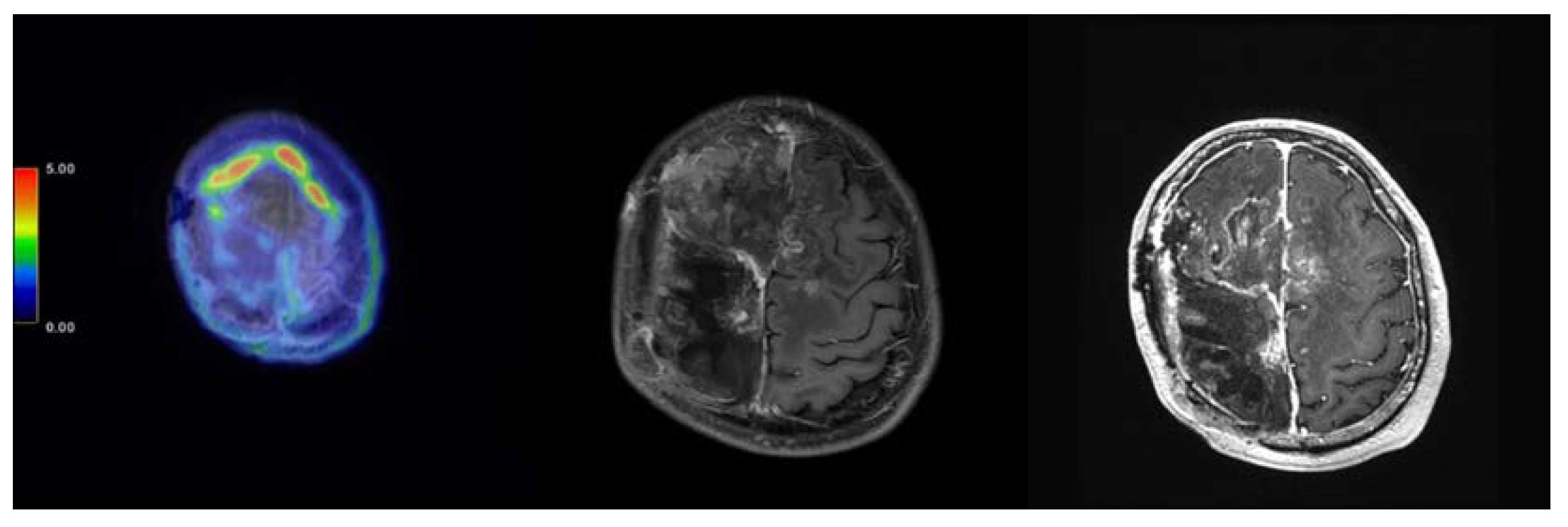
2.2. Case 191
2.3. Case 197
2.4. Case 284
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Treatment Protocol
4.3. Response Evaluation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wiemels, J.; Wrensch, M.; Claus, E.B. Epidemiology and etiology of meningioma. J. Neurooncol. 2010, 99, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO classification of tumors of the central nervous system: A summary. Neuro. Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Buerki, R.A.; Horbinski, C.M.; Kruser, T.; Horowitz, P.M.; James, C.D.; Lukas, R.V. An overview of meningiomas. Future Oncol. 2018, 14, 2161–2177. [Google Scholar] [CrossRef] [PubMed]
- Paldor, I.; Awad, M.; Sufaro, Y.Z.; Kaye, A.H.; Shoshan, Y. Review of controversies in management of non-benign meningioma. J. Clin. Neurosci. 2016, 31, 37–46. [Google Scholar] [CrossRef]
- Quddusi, A.; Shamim, M.S. Simpson grading as predictor of meningioma recurrence. J. Pak. Med. Assoc. 2018, 68, 819–821. [Google Scholar]
- Pereira, B.J.A.; de Almeida, A.N.; Paiva, W.S.; Teixeira, M.J.; Marie, S.K.N. Impact of radiotherapy in atypical meningioma recurrence: Literature review. Neurosurg. Rev. 2019, 42, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M. Boron neutron capture therapy (BNCT): A unique role in radiotherapy with a view to entering the accelerator based BNCT era. Int. J. Clin. Oncol. 2020, 25, 43–50. [Google Scholar] [CrossRef]
- Chen, Y.W.; Lee, Y.Y.; Lin, C.F.; Pan, P.S.; Chen, J.K.; Wang, C.W.; Hsu, S.M.; Kuo, Y.C.; Lan, T.L.; Hsu, S.P.C.; et al. Salvage boron neutron capture therapy for malignant brain tumor patients in compliance with emergency and compassionate use: Evaluation of 34 cases in Taiwan. Biology 2021, 10, 334. [Google Scholar] [CrossRef]
- Lan, T.L.; Chou, F.I.; Lin, K.H.; Pan, P.S.; Lee, J.C.; Huang, W.S.; Liu, Y.M.; Chao, Y.; Chen, Y.W. Using salvage boron neutron capture therapy (BNCT) for recurrent malignant brain tumors in Taiwan. Appl. Radiat. Isot. 2020, 160, 109105. [Google Scholar] [CrossRef]
- Barth, R.F.; Mi, P.; Yang, W. Boron delivery agents for neutron capture therapy of cancer. Cancer Commun. 2018, 38, 35. [Google Scholar] [CrossRef] [Green Version]
- Morita, T.; Kurihara, H.; Hiroi, K.; Honda, N.; Igaki, H.; Hatazawa, J.; Arai, Y.; Itami, J. Dynamic changes in 18F-borono-L-phenylalanine uptake in unresectable, advanced, or recurrent squamous cell carcinoma of the head and neck and malignant melanoma during boron neutron capture therapy patient selection. Radiat. Oncol. 2018, 13, 4. [Google Scholar] [CrossRef] [Green Version]
- Miyatake, S.; Kawabata, S.; Yokoyama, K.; Kuroiwa, T.; Michiue, H.; Sakurai, Y.; Kumada, H.; Suzuki, M.; Maruhashi, A.; Kirihata, M.; et al. Survival benefit of boron neutron capture therapy for recurrent malignant gliomas. J. Neurooncol. 2009, 91, 199–206. [Google Scholar] [CrossRef]
- Miyatake, S.; Wanibuchi, M.; Hu, N.; Ono, K. Boron neutron capture therapy for malignant brain tumors. J. Neurooncol. 2020, 149, 1–11. [Google Scholar] [CrossRef]
- Wang, Y.C.; Chuang, C.C.; Wei, K.C.; Chang, C.N.; Lee, S.T.; Wu, C.T.; Hsu, Y.H.; Lin, T.K.; Hsu, P.W.; Huang, Y.C.; et al. Long term surgical outcome and prognostic factors of atypical and malignant meningiomas. Sci. Rep. 2016, 6, 35743. [Google Scholar] [CrossRef] [Green Version]
- Fabi, A.; Nuzzo, C.; Vidiri, A.; Ciccarese, M.; Felici, A.; Cattani, F.; Cognetti, F. Bone and lung metastases from intracranial meningioma. Anticancer Res. 2006, 26, 3835–3837. [Google Scholar]
- McCarthy, B.J.; Davis, F.G.; Freels, S.; Surawicz, T.S.; Damek, D.M.; Grutsch, J.; Menck, H.R.; Laws, E.R., Jr. Factors associated with survival in patients with meningioma. J. Neurosurg. 1998, 88, 831–839. [Google Scholar] [CrossRef]
- Magill, S.T.; Young, J.S.; Chae, R.; Aghi, M.K.; Theodosopoulos, P.V.; McDermott, M.W. Relationship between tumor location, size, and WHO grade in meningioma. Neurosurg. Focus 2018, 44, E4. [Google Scholar] [CrossRef] [Green Version]
- Zattra, C.M.; Zhang, D.Y.; Broggi, M.; Velz, J.; Vasella, F.; Seggewiss, D.; Schiavolin, S.; Bozinov, O.; Krayenbühl, N.; Sarnthein, J.; et al. Repeated craniotomies for intracranial tumors: Is the risk increased? Pooled analysis of two prospective, institutional registries of complications and outcomes. J. Neurooncol. 2019, 142, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Patibandla, M.R.; Lee, C.C.; Sheehan, J. Stereotactic radiosurgery of central skull base meningioma’s—Volumetric evaluation and longterm outcomes. World Neurosurg. 2017, 108, 176–184. [Google Scholar] [CrossRef]
- Ishiwata, K. 4-Borono-2-18F-fluoro-L-phenylalanine PET for boron neutron capture therapy-oriented diagnosis: Overview of a quarter century of research. Ann. Nucl. Med. 2019, 33, 223–236. [Google Scholar] [CrossRef]
- Shimosegawa, E.; Isohashi, K.; Naka, S.; Horitsugi, G.; Hatazawa, J. Assessment of 10B concentration in boron neutron capture therapy: Potential of image-guided therapy using 18FBPA PET. Ann. Nucl. Med. 2016, 30, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Kanai, Y. Amino acid transporter LAT1 (SLC7A5) as a molecular target for cancer diagnosis and therapeutics. Pharmacol. Ther. 2022, 230, 107964. [Google Scholar] [CrossRef]
- Nakahara, Y.; Ito, H.; Masuoka, J.; Abe, T. Boron neutron capture therapy and photodynamic therapy for high-grade meningiomas. Cancers 2020, 12, 1334. [Google Scholar] [CrossRef]
- Miyatake, S.; Tamura, Y.; Kawabata, S.; Iida, K.; Kuroiwa, T.; Ono, K. Boron neutron capture therapy for malignant tumors related to meningiomas. Neurosurgery 2007, 61, 82–90; discussion 90–91. [Google Scholar] [CrossRef]
- Saarinen, I.; Jambor, I.; Kim, M.; Kuisma, A.; Kemppainen, J.; Merisaari, H.; Eskola, O.; Koskenniemi, A.R.; Perez, I.M.; Boström, P.; et al. Correlation between 18F-1-amino-3-fluorocyclobutane-1-carboxylic acid (18F-fluciclovine) uptake and expression of alanine-serine-cysteine-transporter 2 (ASCT2) and L-type amino acid transporter 1 (LAT1) in primary prostate cancer. EJNMMI Res. 2019, 9, 50. [Google Scholar] [CrossRef]
- Takeuchi, K.; Kawabata, S.; Hiramatsu, R.; Matsushita, Y.; Tanaka, H.; Sakurai, Y.; Suzuki, M.; Ono, K.; Miyatake, S.I.; Kuroiwa, T. Boron Neutron Capture Therapy for High-Grade Skull-Base Meningioma. J. Neurol. Surg. B Skull. Base 2018, 79 (Suppl. 4), S322–S327. [Google Scholar] [CrossRef]
- Hawthorne, M.F. New horizons for therapy based on the boron neutron capture reaction. Mol. Med. Today 1998, 4, 174–181. [Google Scholar] [CrossRef]
- Pan, Y.Y.; Yao, S.F.; Lin, K.H.; Chou, F.I.; Lee, J.C.; Tai, S.K.; Huang, W.S.; Lan, K.L.; Chao, Y.; Chen, Y.W. Boron neutron capture therapy as salvage treatment for recurrent papillary thyroid carcinoma—A case report. Ther. Radiol. Oncol. 2020, 4, 21. [Google Scholar] [CrossRef]
- Fukuda, H.; Hiratsuka, J. Pharmacokinetics of 10B-p-boronophenylalanine (BPA) in the blood and tumors in human patients: A critical review with special reference to tumor-to-blood (T/B) ratios using resected tumor samples. Appl. Radiat. Isot. 2020, 166, 109308. [Google Scholar] [CrossRef]
- Seki, R.; Wakisaka, Y.; Morimoto, N.; Takashina, M.; Koizumi, M.; Toki, H.; Fukuda, M. Physics of epi-thermal boron neutron capture therapy (epi-thermal BNCT). Radiol. Phys. Technol. 2017, 10, 387–408. [Google Scholar] [CrossRef]
- Farhood, B.; Samadian, H.; Ghorbani, M.; Zakariaee, S.S.; Knaup, C. Physical, dosimetric and clinical aspects and delivery systems in neutron capture therapy. Rep. Pract. Oncol. Radiother. 2018, 23, 462–473. [Google Scholar] [CrossRef]
- Lee, J.C.; Chuang, K.S.; Chen, Y.W.; Hsu, F.Y.; Chou, F.I.; Yen, S.H.; Wu, Y.H. Preliminary dosimetric study on feasibility of multi-beam boron neutron capture therapy in patients with diffuse intrinsic pontine glioma without craniotomy. PLoS ONE 2017, 12, e0180461. [Google Scholar] [CrossRef] [Green Version]
- Ono, K.; Masunaga, S.I.; Kinashi, Y.; Nagata, K.; Suzuki, M.; Sakurai, Y.; Maruhashi, A.; Kato, I.; Nakazawa, M.; Ariyoshi, Y.; et al. Neutron Irradiation under Continuous BPA Injection for Solving the Problem of Heterogeneous Distribution of BPA. In Proceedings of the 12th International Congress on Neutron Capture Therapy—From the Past to the Future, Takamatsu, Japan, 9–13 October 2006. [Google Scholar]
- Kawabata, S.; Miyatake, S.; Nonoguchi, N.; Hiramatsu, R.; Iida, K.; Miyata, S.; Yokoyama, K.; Doi, A.; Kuroda, Y.; Kuroiwa, T.; et al. Survival benefit from boron neutron capture therapy for the newly diagnosed glioblastoma patients. Appl. Radiat. Isot. 2009, 67 (Suppl. 7–8), S15–S18. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | BNCT Date | Irradiation Time (Sec) | Tumor Average Dose (GyE) | Tumor Minimum Dose (GyE) | Brain Maximum Dose (GyE) | Tumor Response | Last Follow-Up | PFS (Months) |
|---|---|---|---|---|---|---|---|---|
| 115 | 21 August 2020 | 1893 | 14.91 | 11.53 | 8.34 | SD | 28 June 2022, SD | 23 |
| 191 | 12 January 2022 15 June 2022 | 910 1055 | 39.15 35.34 | 18.99 18.96 | 11.59 12.48 | PR SD | 13 December 2022, PR | 11 |
| 197 | 11 February 2022 | 1428 | 40.84 | 17.62 | 13.00 | CR | 20 December 2022, CR | 10 |
| 284 | 28 December 2022 | 2369 | 16.83 | 9.61 | 11.29 | SD | 10 January 2023 | 2 |
| All Patients (n = 4) | |
|---|---|
| Age (years) | 61.75 |
| Gender (M, F) | 3, 1 |
| Mean T/N ratio | 4.125 |
| Mean irradiation time (sec) | 1531 |
| Mean blood boron conc. (ppm) | 32.23 |
| Mean tumor average dose (GyE) | 29.414 |
| Mean tumor BED6 | 194.58 |
| Mean tumor minimum dose (GyE) | 15.342 |
| Mean brain max dose (GyE) | 11.11 |
| Case | Age/Gender | Initial Pathology | Site | TN Ratio | Previous Treatment |
|---|---|---|---|---|---|
| 115 | 74/Male | Meningioma | Skull base | 2.89 | RT + ChemoT |
| 191 | 45/Male | Atypical meningioma | Right high frontal | 3.9 | RT + OP + ChemoT |
| 197 | 59/Female | Atypical meningioma | Right high frontal | 2.64 | RT + OP + ChemoT |
| 284 | 69/Male | Atypical meningioma | Right SC sinus | 7.07 | RT + OP + ChemoT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lan, T.-L.; Lin, C.-F.; Lee, Y.-Y.; Lin, K.-H.; Chang, F.-C.; Lin, S.-C.; Lee, J.-C.; Chou, F.-I.; Peir, J.-J.; Liu, H.-M.; et al. Advances in Boron Neutron Capture Therapy (BNCT) for Recurrent Intracranial Meningioma. Int. J. Mol. Sci. 2023, 24, 4978. https://doi.org/10.3390/ijms24054978
Lan T-L, Lin C-F, Lee Y-Y, Lin K-H, Chang F-C, Lin S-C, Lee J-C, Chou F-I, Peir J-J, Liu H-M, et al. Advances in Boron Neutron Capture Therapy (BNCT) for Recurrent Intracranial Meningioma. International Journal of Molecular Sciences. 2023; 24(5):4978. https://doi.org/10.3390/ijms24054978
Chicago/Turabian StyleLan, Tien-Li, Chun-Fu Lin, Yi-Yen Lee, Ko-Han Lin, Feng-Chi Chang, Shih-Chieh Lin, Jia-Cheng Lee, Fong-In Chou, Jinn-Jer Peir, Hong-Ming Liu, and et al. 2023. "Advances in Boron Neutron Capture Therapy (BNCT) for Recurrent Intracranial Meningioma" International Journal of Molecular Sciences 24, no. 5: 4978. https://doi.org/10.3390/ijms24054978