
Carbonic Anhydrase IX in Tumor Tissue and Plasma of Breast Cancer Patients: Reliable Biomarker of Hypoxia and Prognosis
 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
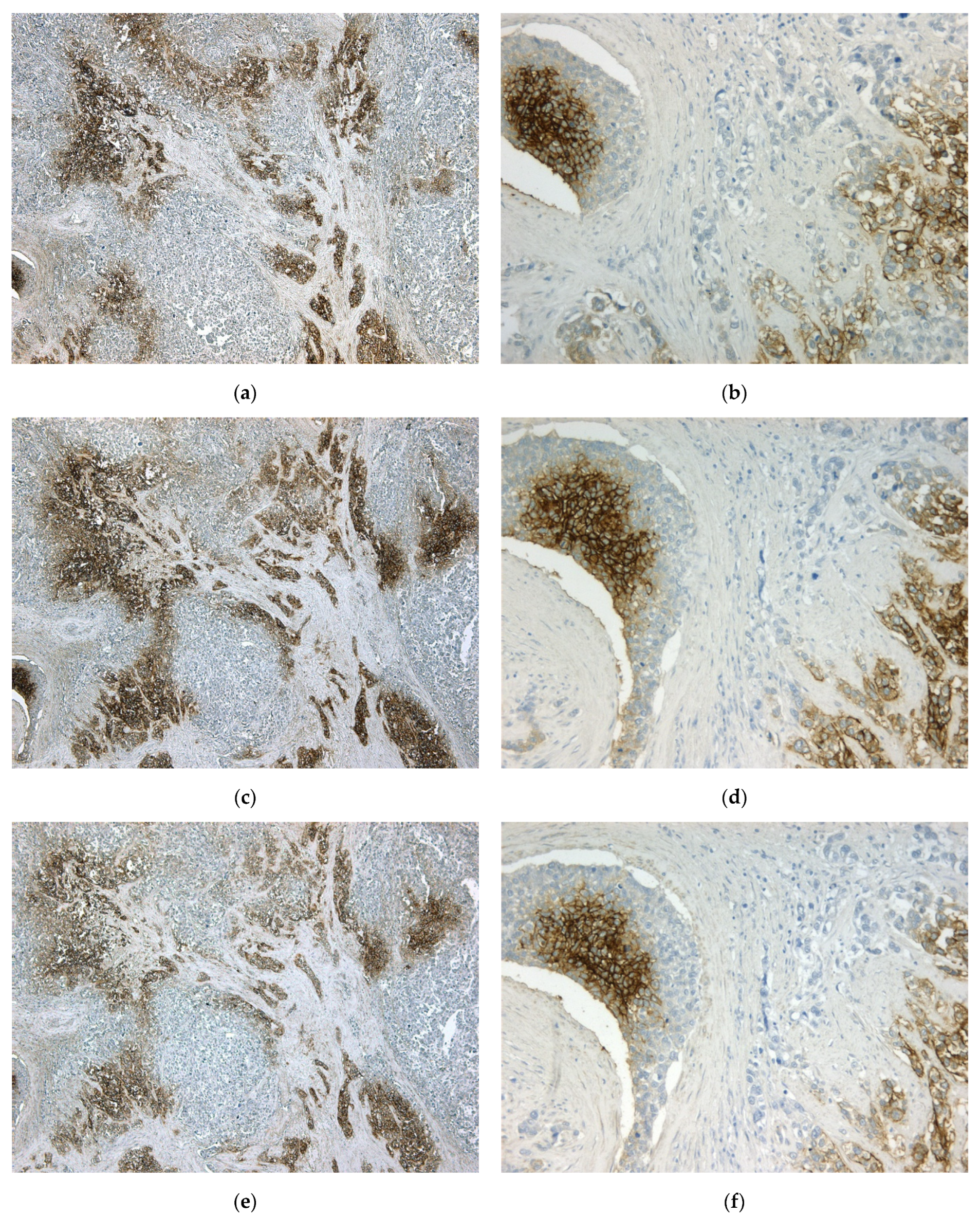
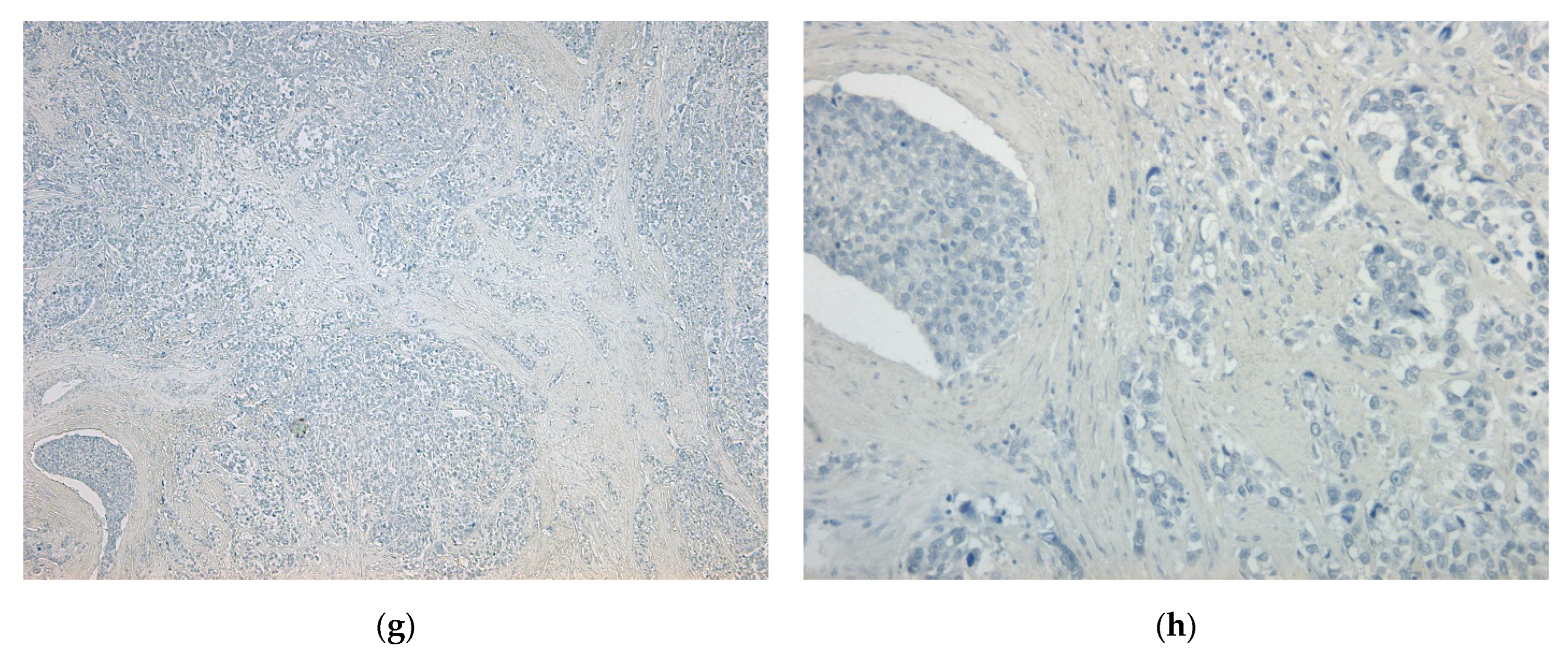
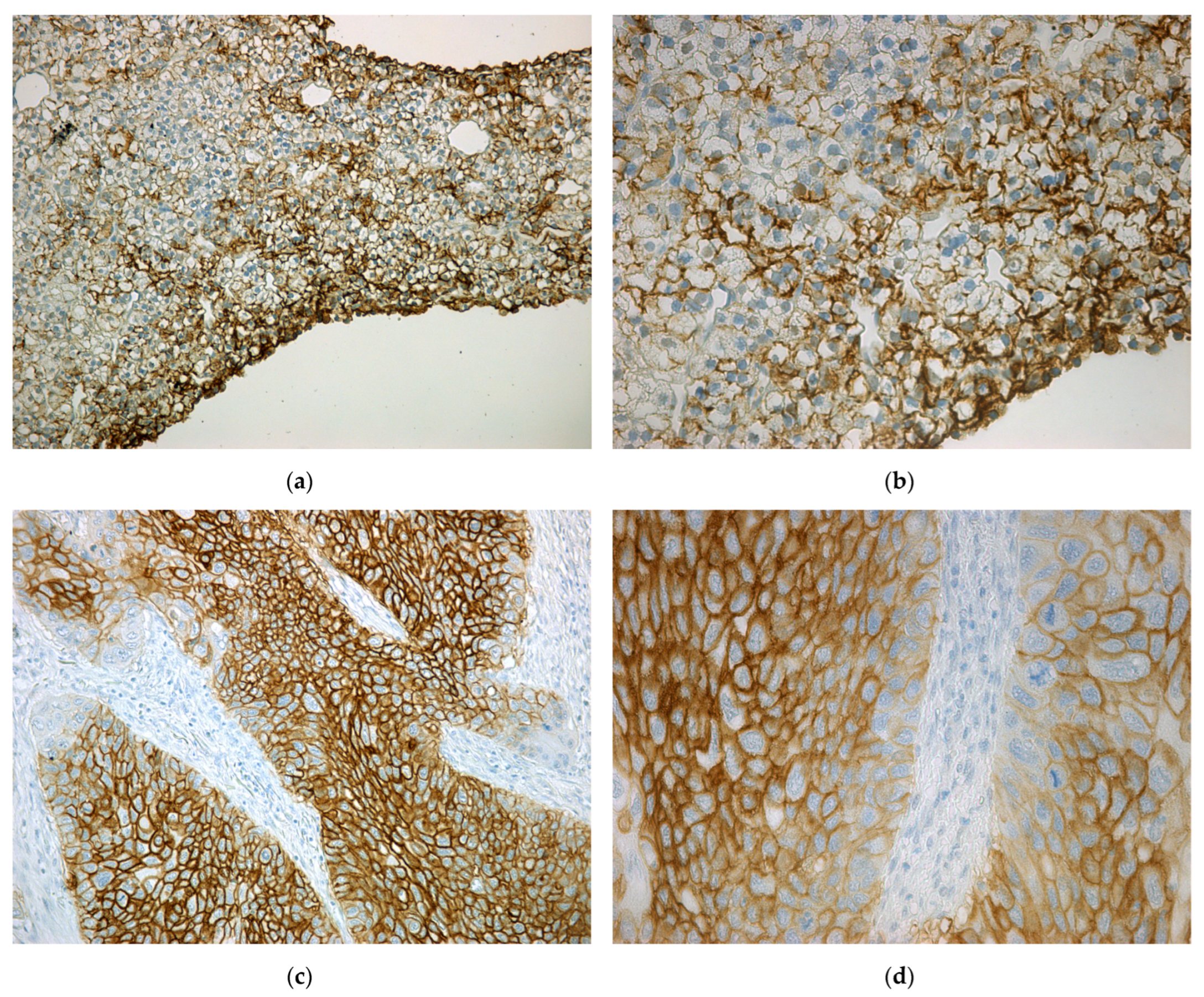
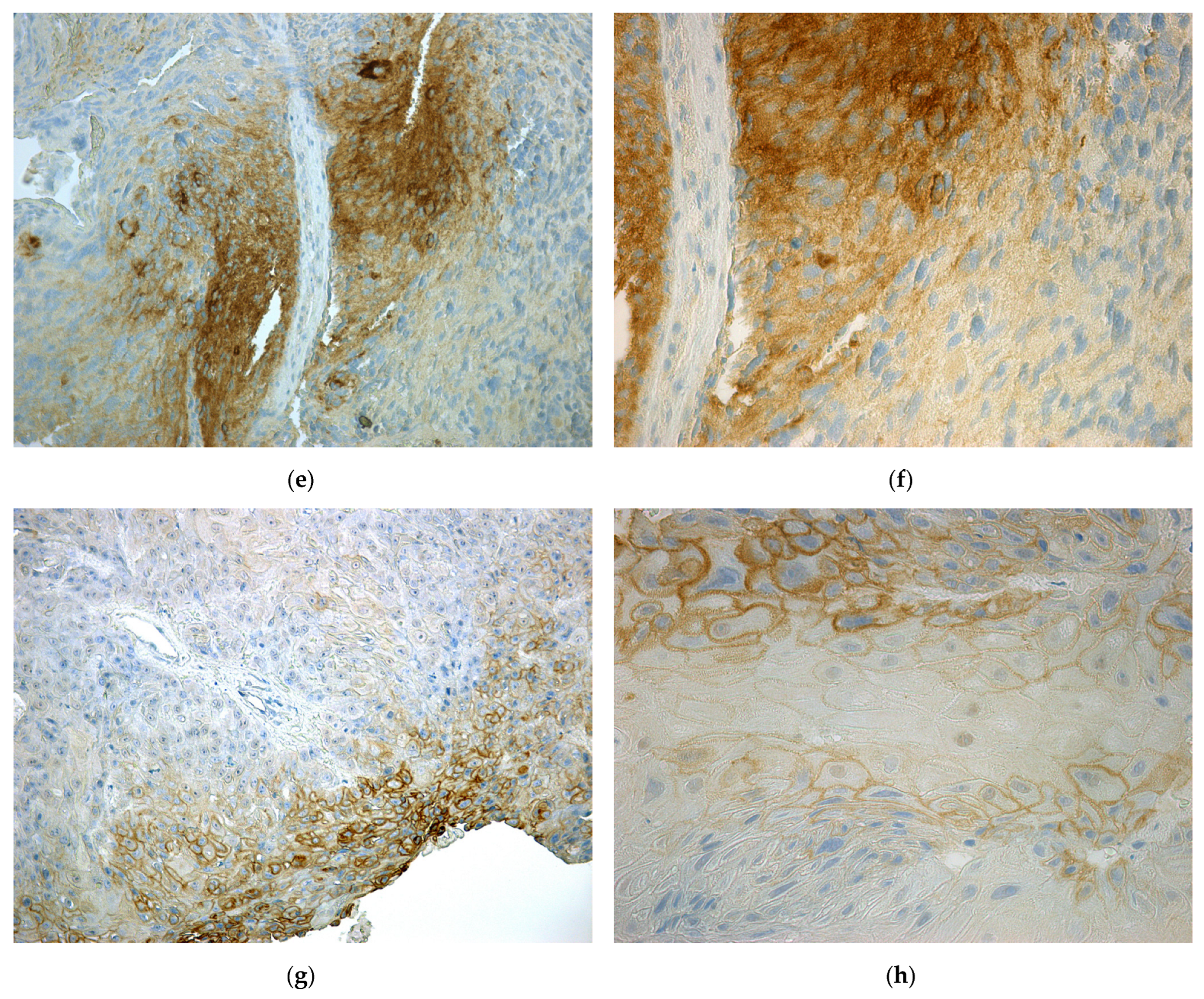
2.2. Immunohistochemical Detection of CA IX in Tumor Tissues
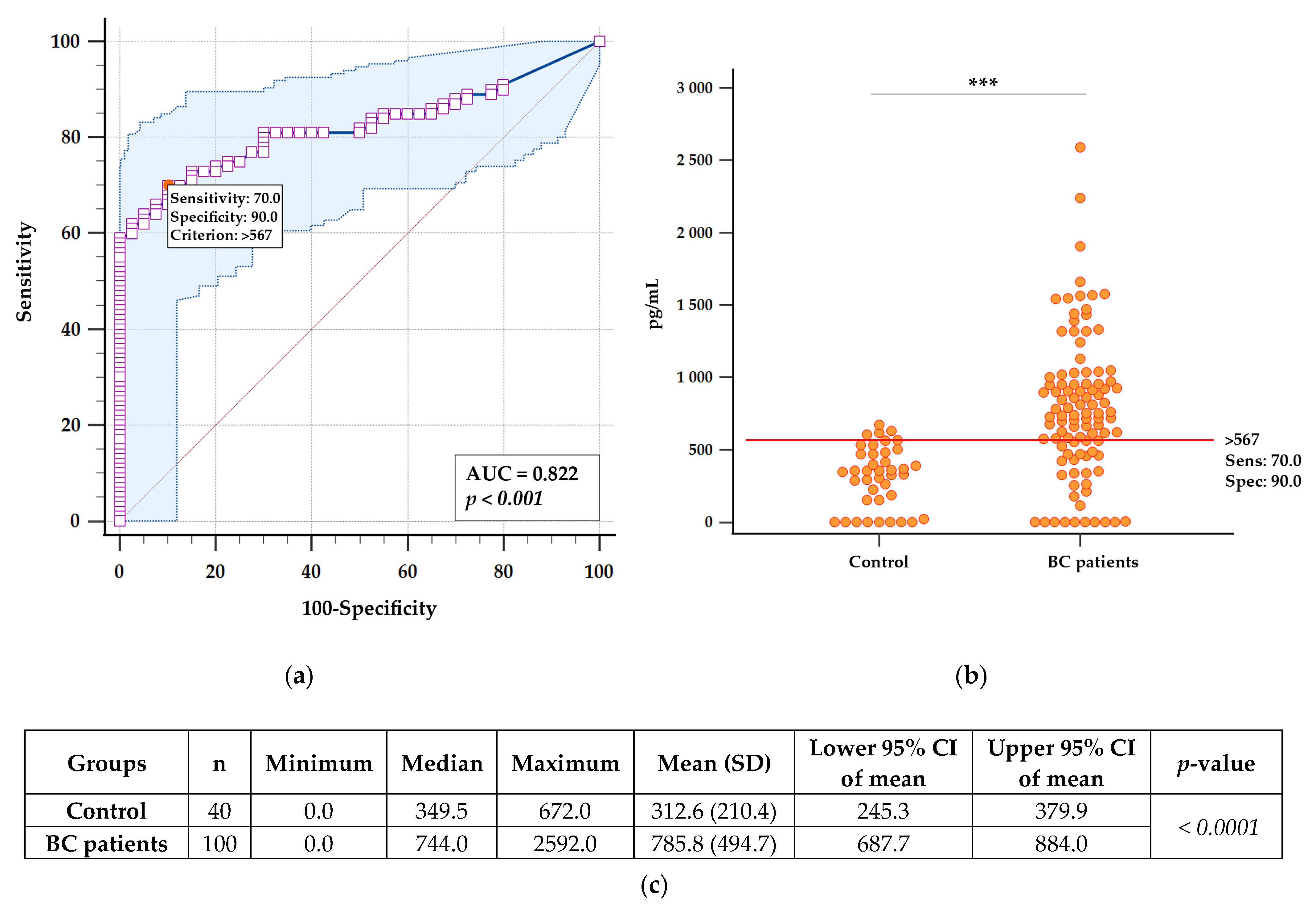
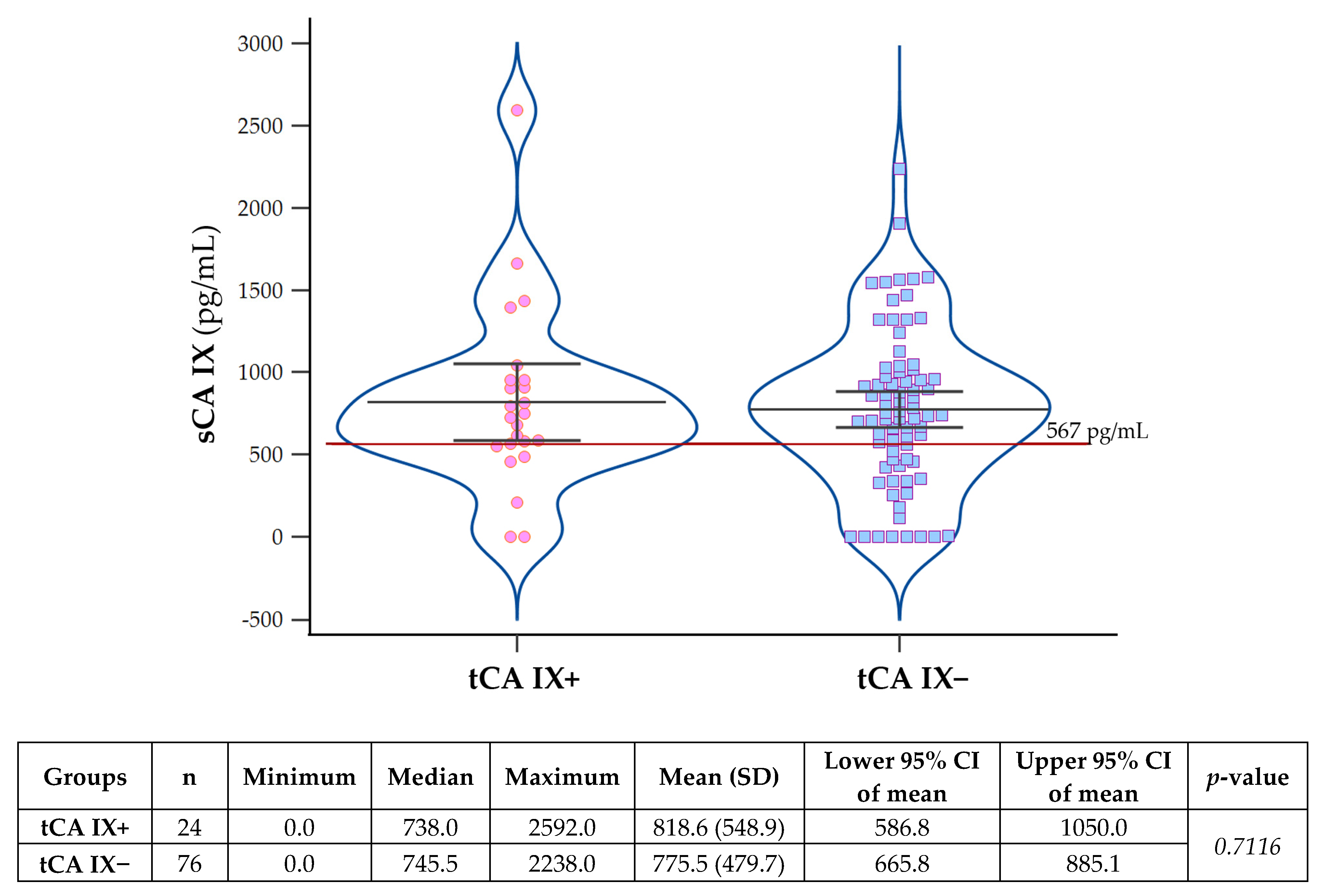
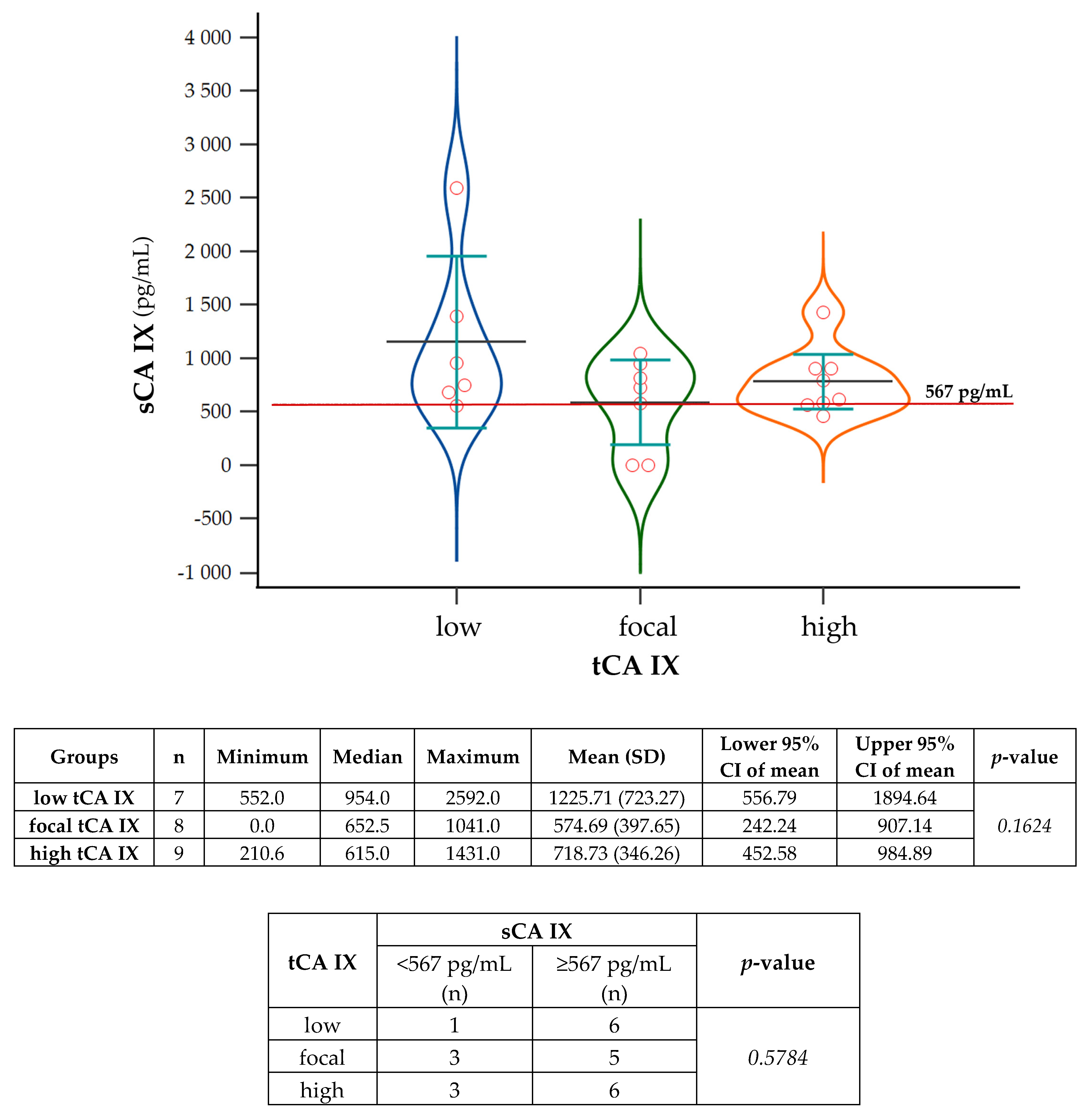
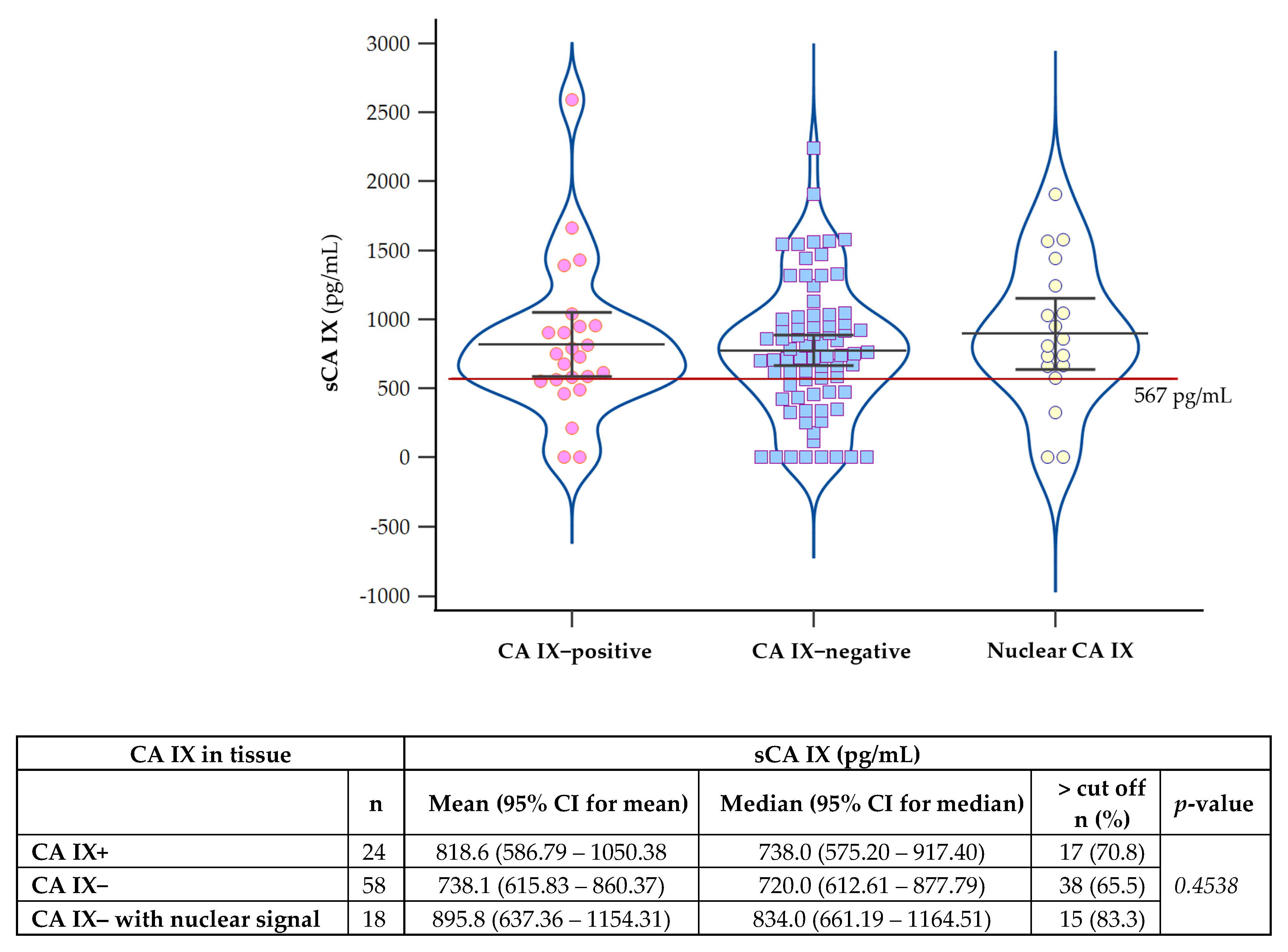
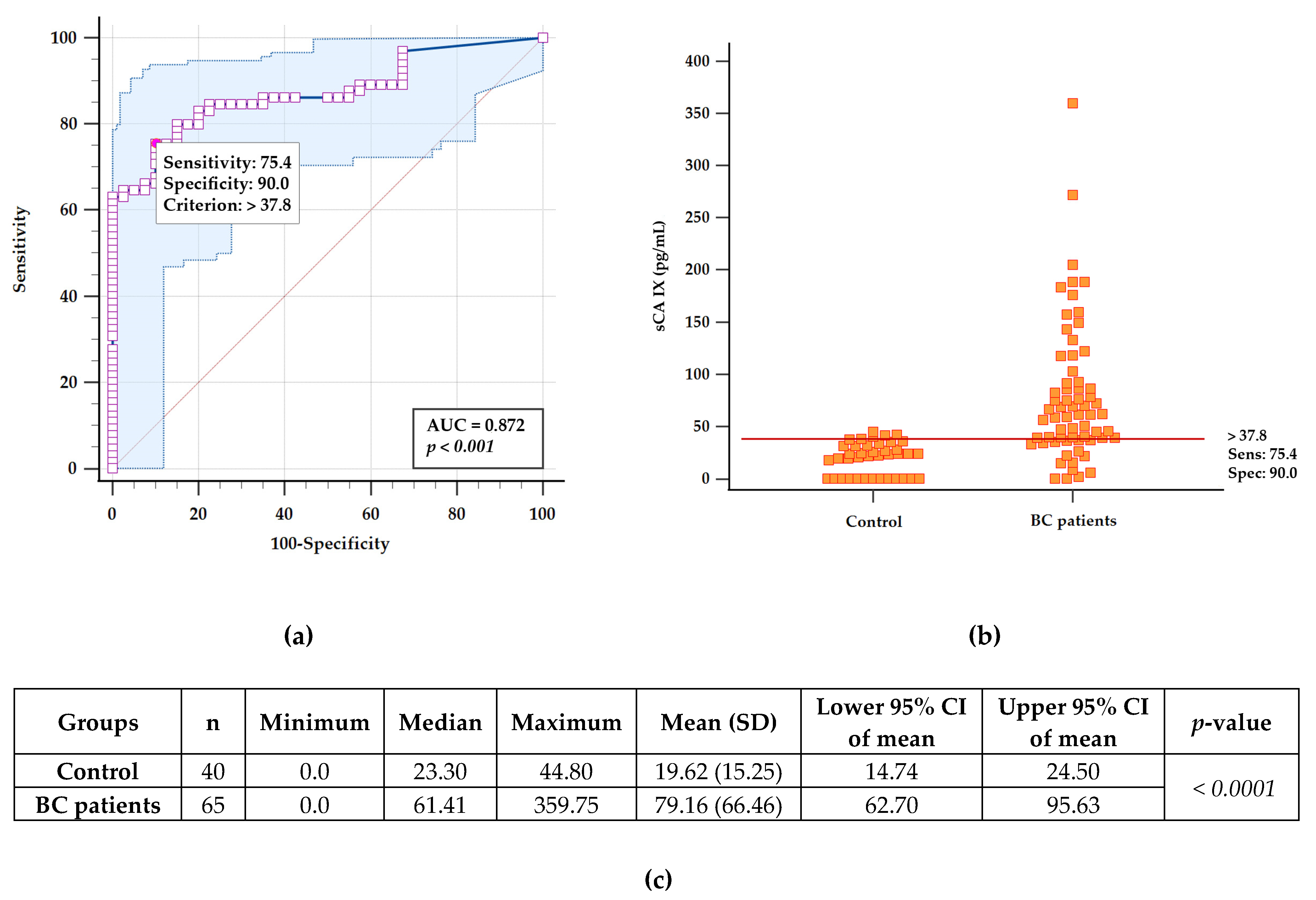
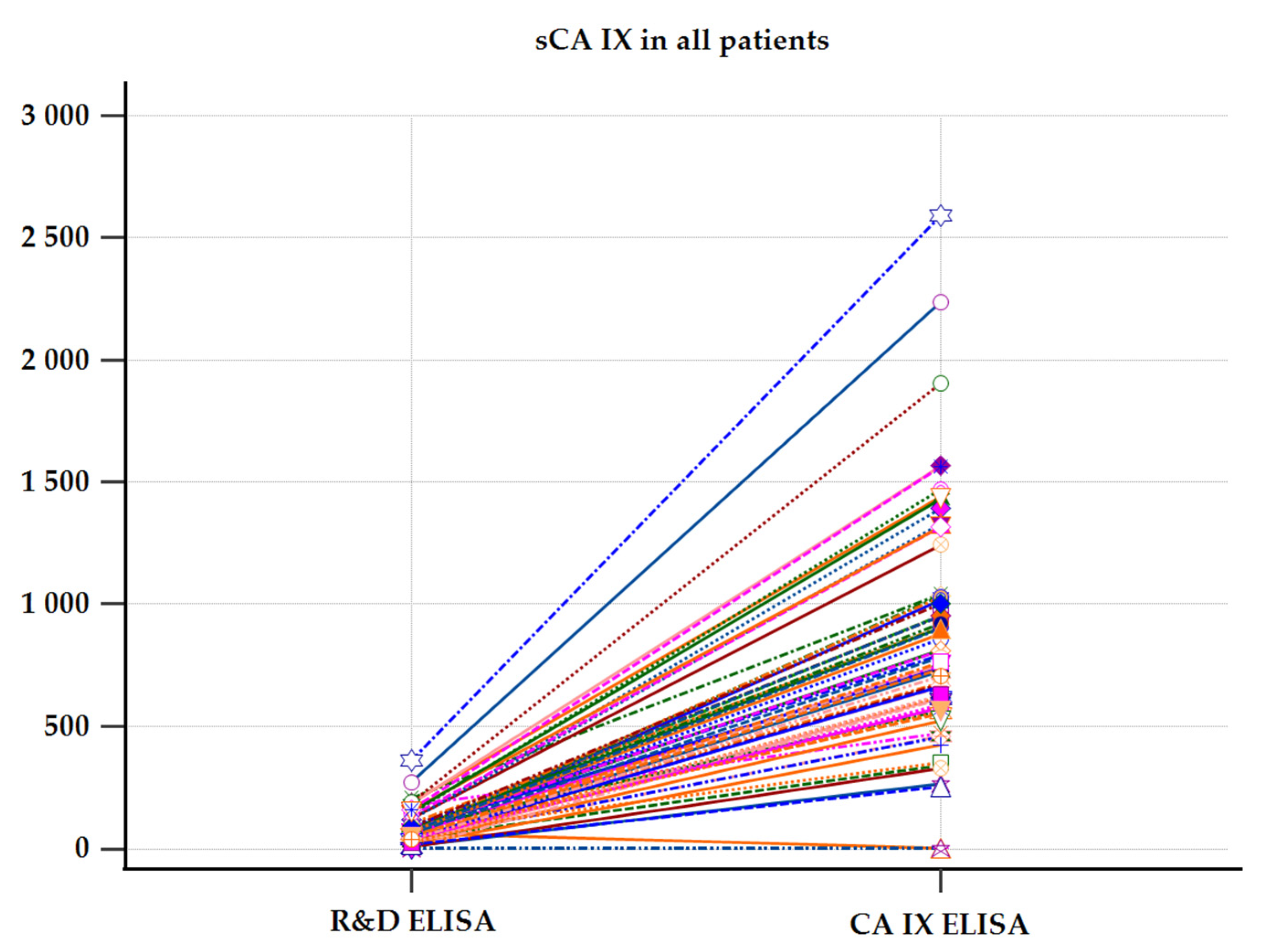
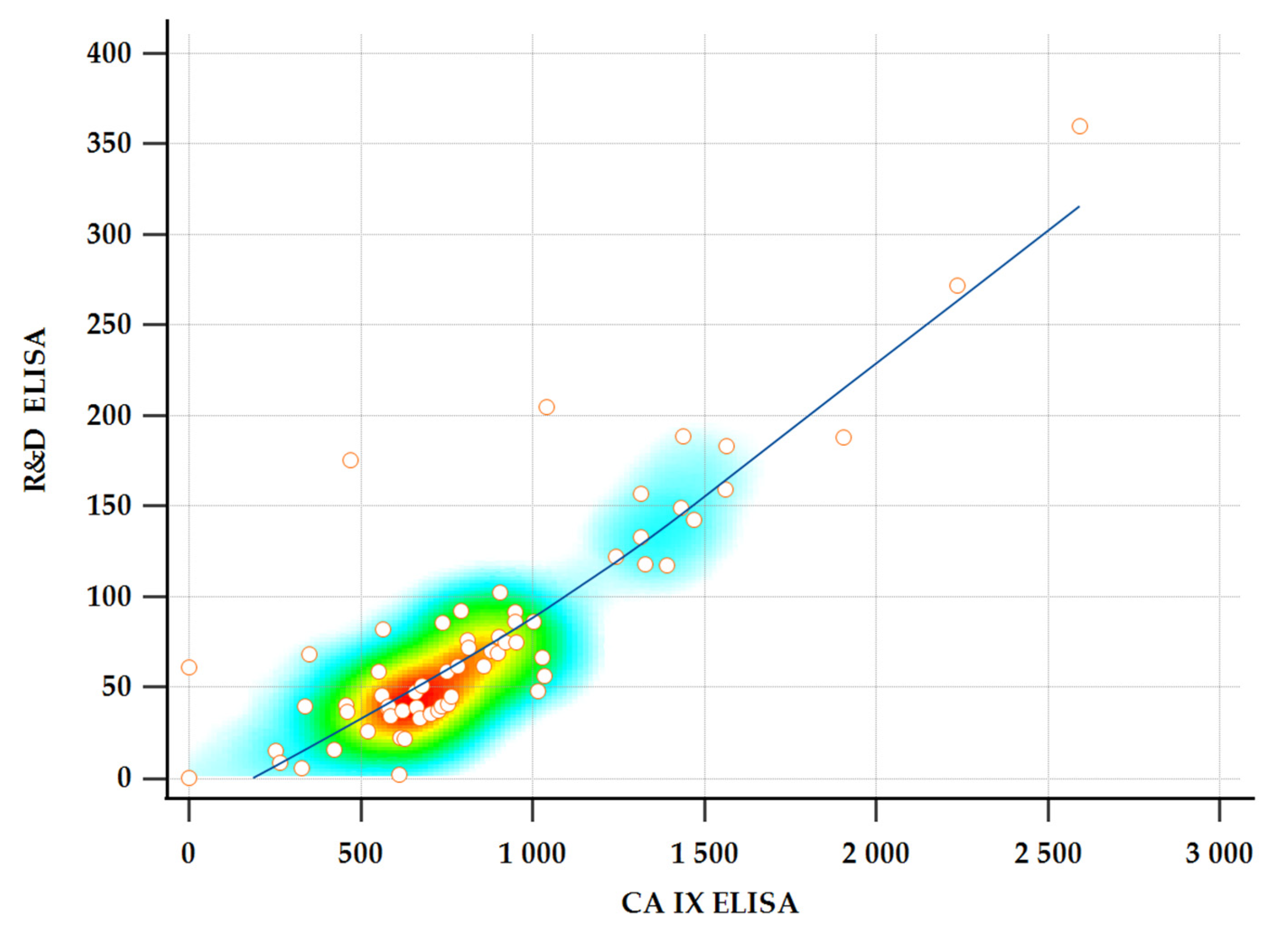
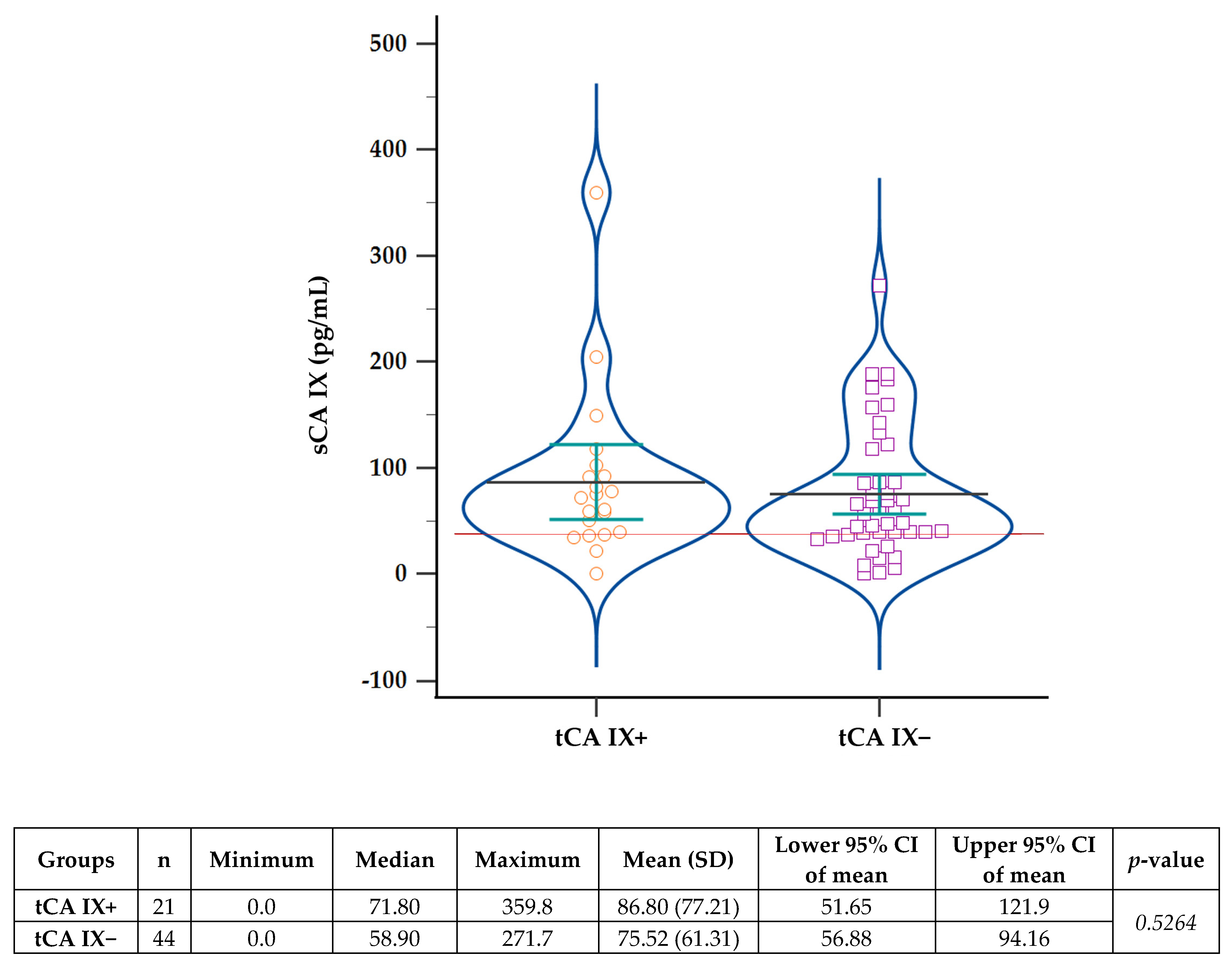
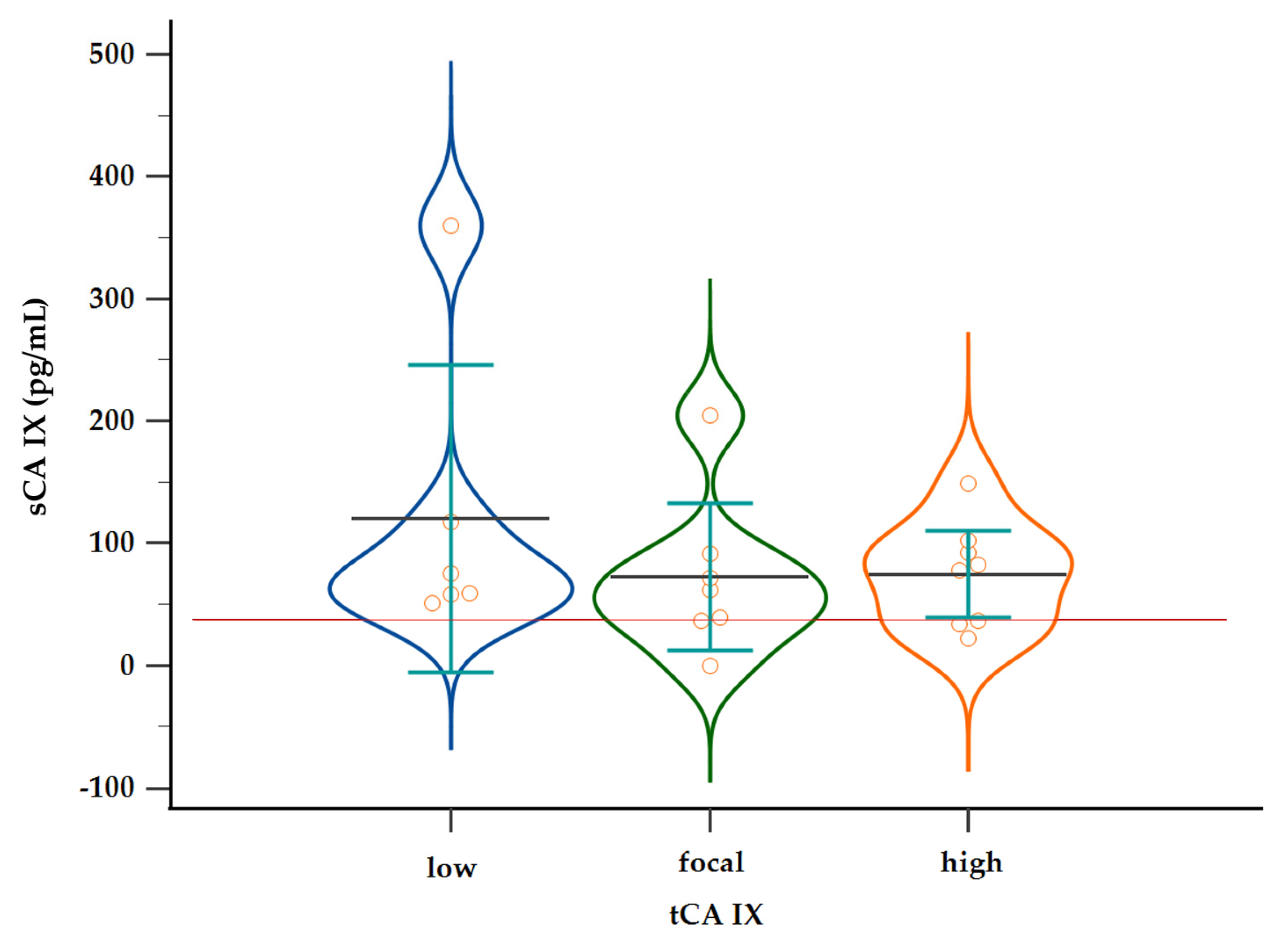
2.3. Evaluation of Soluble CA IX in Patient Plasma
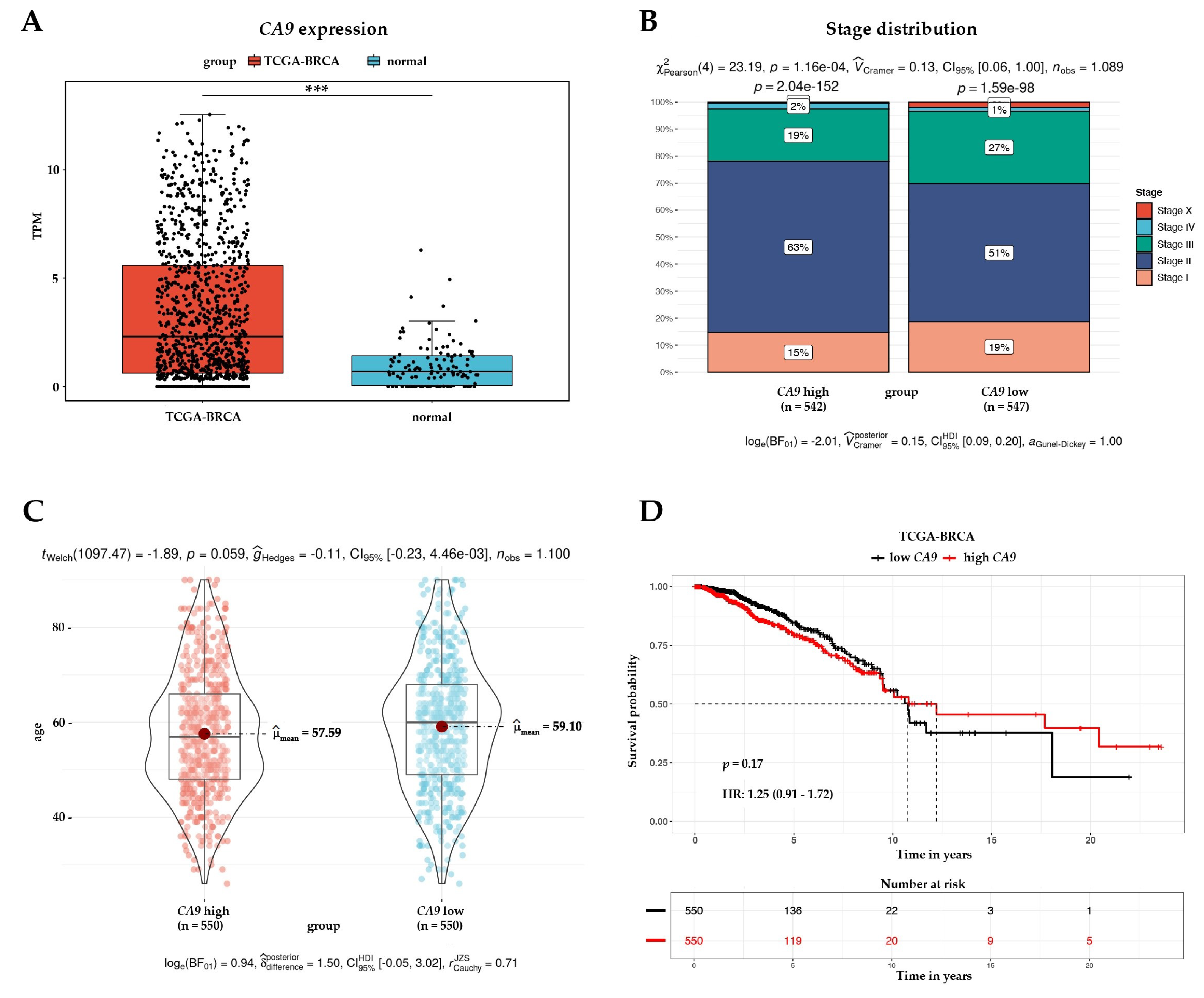
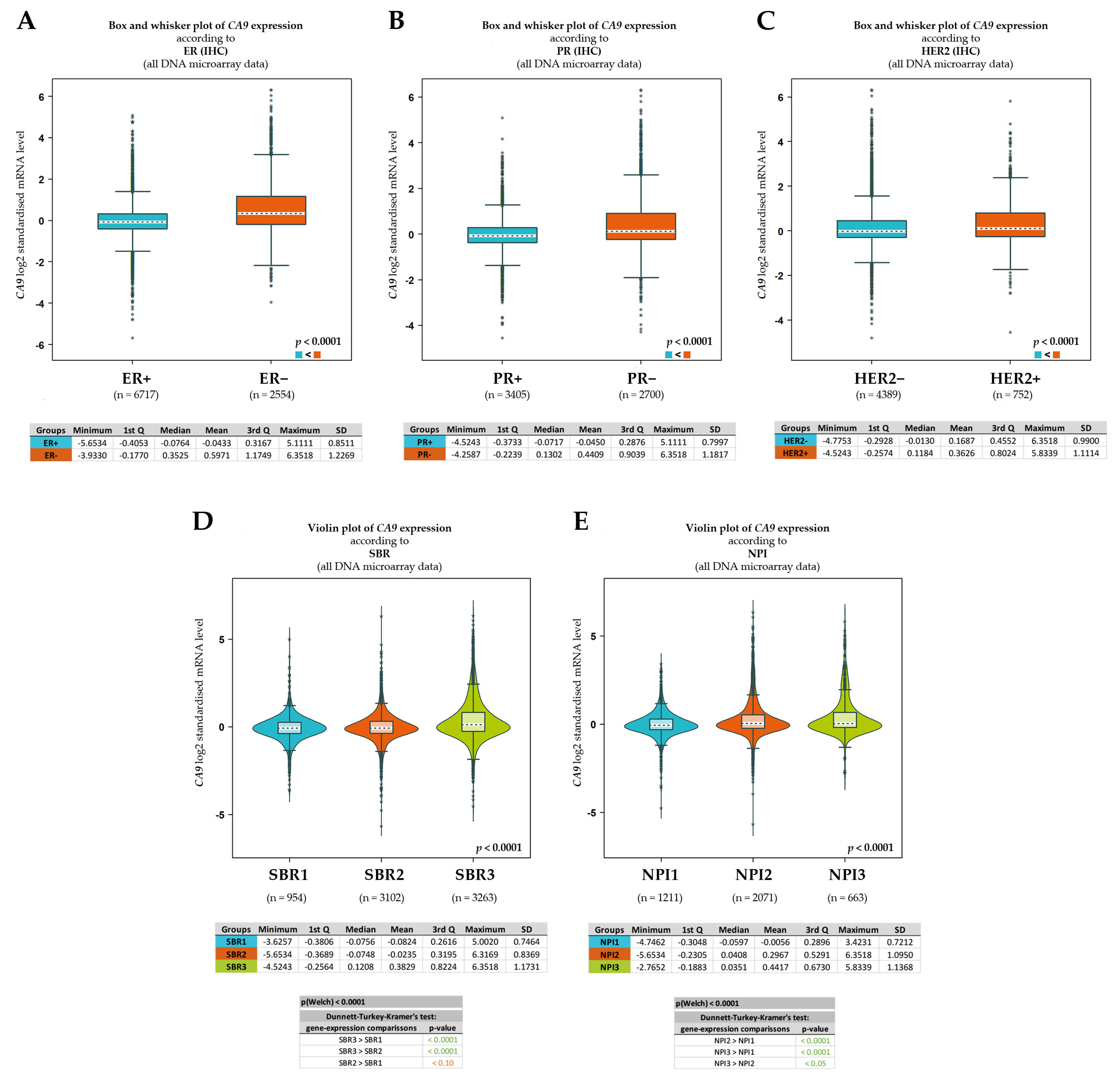
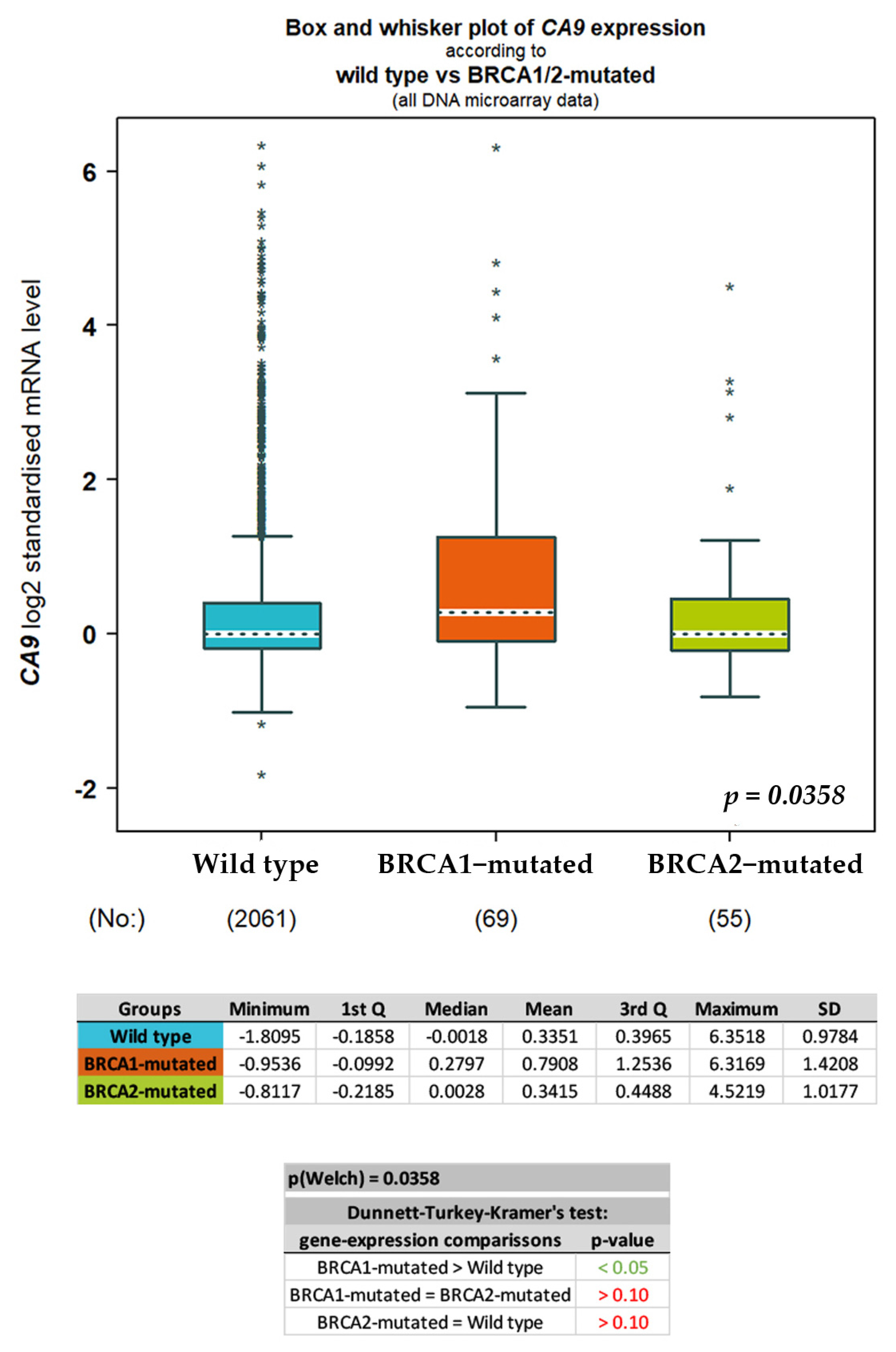
2.4. In Silico Analysis of CA IX Expression in Breast Cancer
3. Discussion
4. Materials and Methods
4.1. Study Design and Patient Population
4.2. Ethics Statement
4.3. Surgical Procedures and Plasma Sample Collection
4.4. Pathology
4.5. Preparation of Monoclonal Antibody for Immunohistochemistry
4.6. CA IX Immunohistochemistry
- Intensity of CA IX staining scored as (+), (++), and (+++);
- Relative number of CA IX positively stained cells: less than 10%, 11–50%, and more than 50% per field of view;
- Subcellular localization of CA IX antigen: membrane, mixed membrane/cytoplasmic, cytoplasmic, or nuclear.
- Low—membrane or mixed membrane/cytoplasmic or cytoplasmic subcellular localization, percentage of positive cells less than 10%, and at the same time, intensity of staining (+);
- Focal—membrane or mixed membrane/cytoplasmic or cytoplasmic subcellular localization, percentage of positive cells 11–50%, and at the same time, intensity of staining (+/++) or (++);
- High—membrane or mixed membrane/cytoplasmic subcellular localization, percentage of positive cells more than 50%, and intensity of staining (+++);
- Negat—nuclear subcellular localization regardless of the percentage of positive cells and staining intensity, and negative CA IX staining.
4.7. CA IX ELISA
4.8. In Silico Analysis
4.9. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASCO | American Society of Clinical Oncology |
| AUC | An area under the curve |
| BC | Breast cancer |
| BCI | Breast Cancer Index |
| BRCA | Breast invasive carcinoma |
| BRCA 1/2 | Breast cancer gene 1/2 |
| CA IX | Carbonic anhydrase IX |
| CA9 | Carbonic anhydrase 9 gene or transcript |
| ccRCC | Clear cell renal cell carcinoma |
| CI | Confidence interval |
| DCIS | Ductal carcinoma in situ |
| DSF | Disease-free survival |
| DSS | Disease-specific survival |
| ECD | Ectodomain of CA IX |
| ELISA | An enzyme-linked immuno-sorbent assay |
| ER | Estrogen receptor |
| FBS | Fetal bovine serum |
| FFPE | Formalin-fixed paraffin-embedded tissues |
| HELLP | Hemolysis, elevated liver enzymes and low platelets syndrome |
| HER2 | Human epidermal growth factor 2 receptor |
| HR | Hazard ratio |
| IHC | Immunohistochemistry |
| IVD | In vitro diagnostics |
| KM | Kaplan–Meier |
| MAb | Monoclonal antibody |
| MSF | Metastasis-free survival |
| NPI | Nottingham prognostic index |
| ns | Non-significant |
| NTA | Nanoparticle tracking analysis |
| OS | Overall survival |
| PBS | Phosphate-buffered saline |
| PFS | Progression-free survival |
| PG | Proteoglycan |
| PR | Progesterone receptor |
| ROC | A receiver operating characteristic curve |
| SBR | Scarff–Bloom–Richardson |
| sCA IX | Soluble form of CA IX |
| SLNs | Sentinel lymph nodes |
| tCA IX | Tissue CA IX |
| TCGA | The Cancer Genome Atlas |
| TNBC | Triple-negative breast cancer |
| TNM | Tumor, node and metastasis staging |
| ToPP | Tumor online Prognostic analysis Platform |
Appendix A


Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables (n) | CA IX+ (n = 24) | CA IX- (n = 76) | p-Value | |
|---|---|---|---|---|
| WS (n = 58) | NS (n = 18) | |||
| Subtype | ||||
| Luminal A (54) | 9 | 32 | 13 | 0.0142 |
| Luminal B-like (18) | 5 | 13 | 0 | |
| HER2-enriched (16) | 3 | 9 | 4 | |
| Triple-negative (9) | 6 | 2 | 1 | |
| DCIS (3) | 1 | 2 | 0 | |
| Grade | ||||
| I/II (63) | 10 | 40 | 13 | 0.0363 |
| III (36) | 14 | 17 | 5 | |
| pT | ||||
| pT1 (56) | 9 | 34 | 13 | ns |
| pT2-4 (41) | 14 | 22 | 5 | |
| pN | ||||
| pN0 (64) | 14 | 39 | 11 | ns |
| pN1-3 (36) | 10 | 19 | 7 | |
| ER | ||||
| Positive (86) | 17 | 54 | 15 | 0.0023 |
| Negative (14) | 7 | 4 | 3 | |
| PR | ||||
| Positive (81) | 17 | 49 | 15 | ns |
| Negative (19) | 7 | 9 | 3 | |
| HER2 | ||||
| Positive (16) | 3 | 9 | 4 | ns |
| Negative (84) | 21 | 49 | 14 | |
| Tumor necrosis | ||||
| Positive (21) | 11 | 6 | 4 | 0.0018 |
| Negative (78) | 13 | 51 | 14 | |

Appendix C
Appendix C.1. Materials and Methods
Appendix C.1.1. Isolation of Exosomes
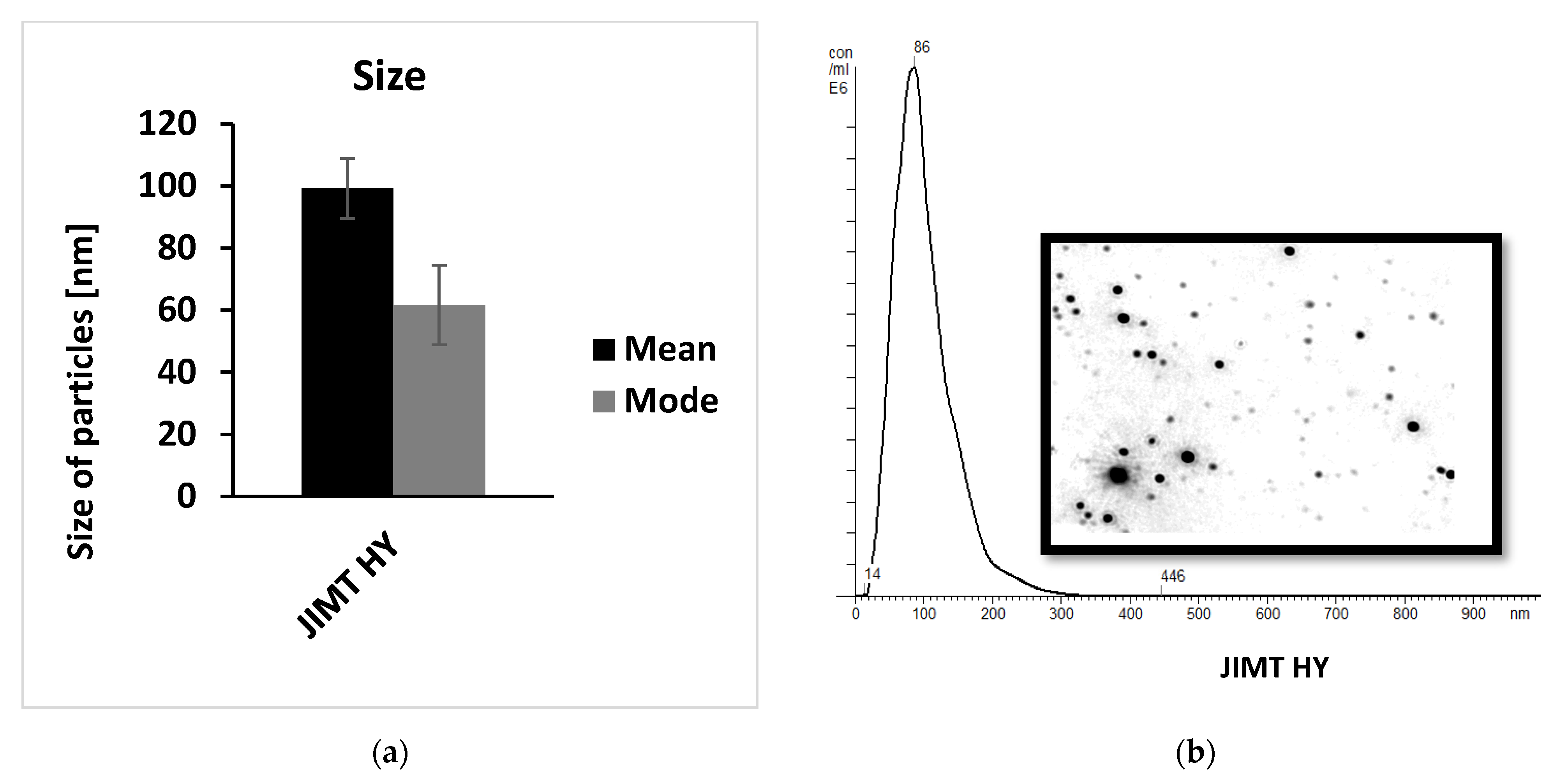
Appendix C.1.2. Nanoparticle Tracking Analysis
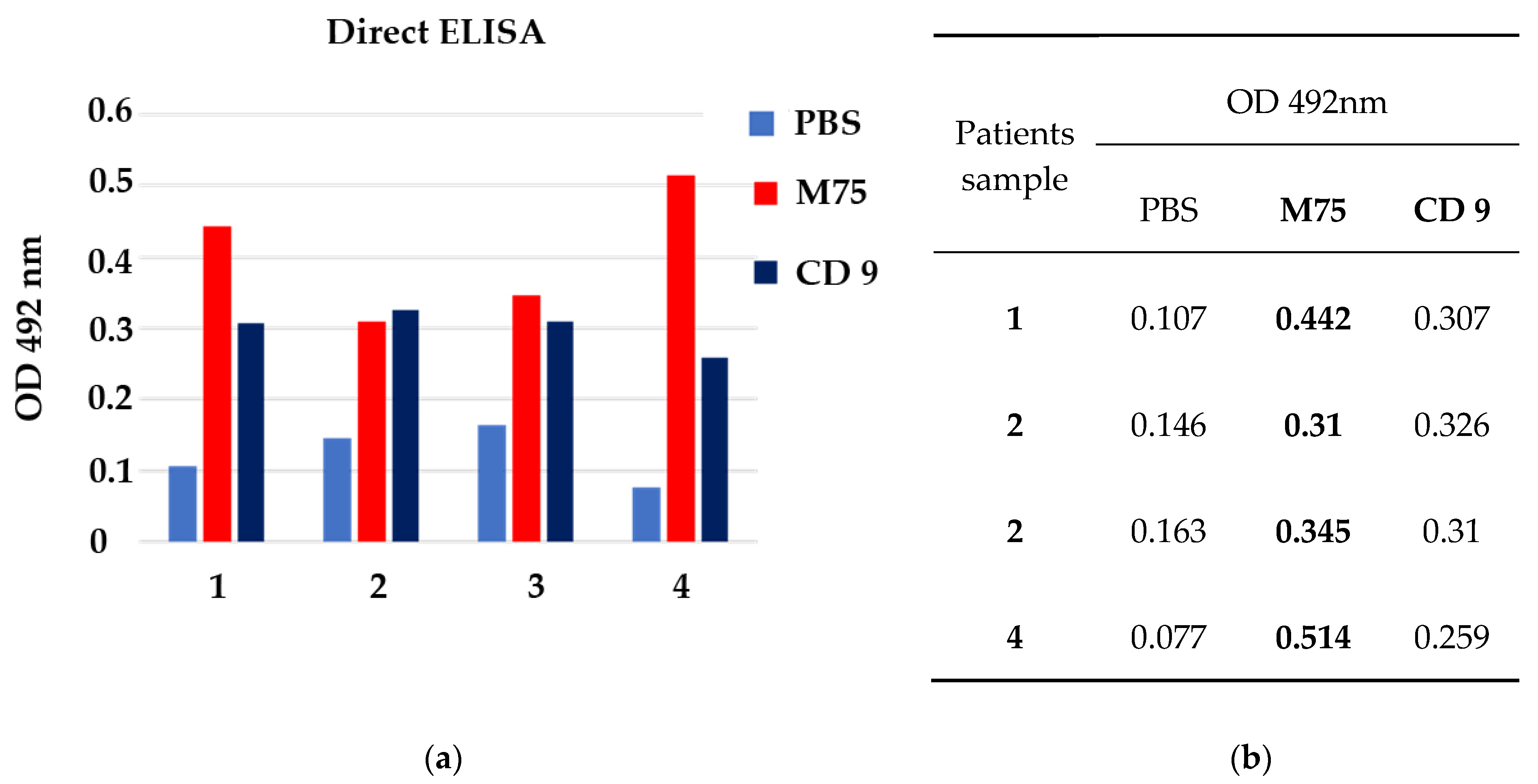
Appendix C.1.3. CA IX and CD9 direct ELISA
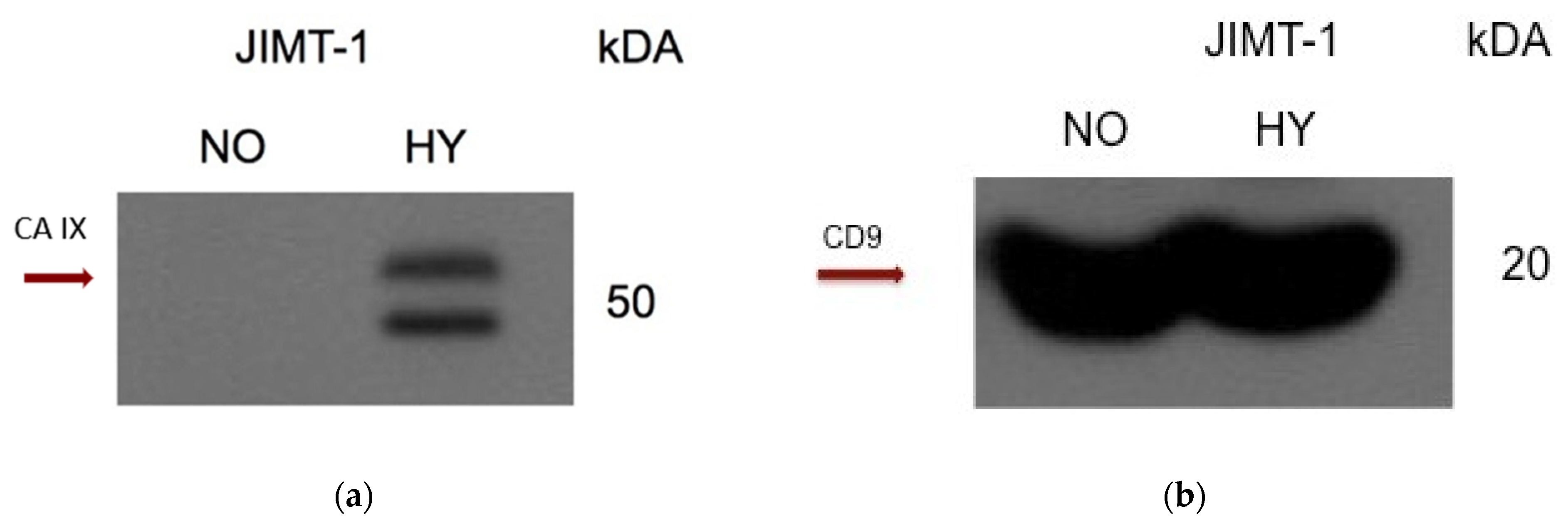
Appendix C.1.4. Western blot
Appendix C.2. Results



Appendix D

Appendix E





References
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Vignat, J.; Gralow, J.R.; Cardoso, F.; Siesling, S.; et al. Current and future burden of breast cancer: Global statistics for 2020 and 2040. Breast 2022, 66, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Mmanual, 8th ed.; American Joint Committee on Cancer; Springer: Chicago, IL, USA, 2017; ISBN 978-3-319-40617-6. [Google Scholar]
- Varga, Z.; Sinn, P.; Seidman, A.D. Summary of head-to-head comparisons of patient risk classifications by the 21-gene Recurrence Score® (RS) assay and other genomic assays for early breast cancer. Int. J. Cancer 2019, 145, 882–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andre, F.; Ismaila, N.; Allison, K.H.; Barlow, W.E.; Collyar, D.E.; Damodaran, S.; Henry, N.L.; Jhaveri, K.; Kalinsky, K.; Kuderer, N.M.; et al. Biomarkers for Adjuvant Endocrine and Chemotherapy in Early-Stage Breast Cancer: ASCO Guideline Update. J. Clin. Oncol. 2022, 40, 1816–1837. [Google Scholar] [CrossRef] [PubMed]
- Wykoff, C.C.; Beasley, N.J.P.; Watson, P.H.; Turner, K.J.; Pastorek, J.; Sibtain, A.; Wilson, G.D.; Turley, H.; Talks, K.L.; Maxwell, P.H.; et al. Hypoxia-inducible Expression of Tumor-associated Carbonic Anhydrases. Cancer Res. 2000, 60, 7075–7083. [Google Scholar] [PubMed]
- Pastorek, J.; Pastorekova, S. Hypoxia-induced carbonic anhydrase IX as a target for cancer therapy: From biology to clinical use. Semin. Cancer Biol. 2015, 31, 52–64. [Google Scholar] [CrossRef]
- Pastorekova, S.; Gillies, R.J. The role of carbonic anhydrase IX in cancer development: Links to hypoxia, acidosis, and beyond. Cancer Metastasis Rev. 2019, 38, 65–77. [Google Scholar] [CrossRef]
- van Kuijk, S.J.A.; Yaromina, A.; Houben, R.; Niemans, R.; Lambin, P.; Dubois, L.J. Prognostic Significance of Carbonic Anhydrase IX Expression in Cancer Patients: A Meta-Analysis. Front. Oncol. 2016, 6, 69. [Google Scholar] [CrossRef] [Green Version]
- Brennan, D.J.; Jirstrom, K.; Kronblad, A.; Millikan, R.C.; Landberg, G.; Duffy, M.J.; Rydén, L.; Gallagher, W.M.; O’Brien, S.L. CA IX is an independent prognostic marker in premenopausal breast cancer patients with one to three positive lymph nodes and a putative marker of radiation resistance. Clin. Cancer Res. 2006, 12, 6421–6431. [Google Scholar] [CrossRef] [Green Version]
- Sowa, T.; Menju, T.; Chen-Yoshikawa, T.F.; Takahashi, K.; Nishikawa, S.; Nakanishi, T.; Shikuma, K.; Motoyama, H.; Hijiya, K.; Aoyama, A.; et al. Hypoxia-inducible factor 1 promotes chemoresistance of lung cancer by inducing carbonic anhydrase IX expression. Cancer Med. 2017, 6, 288–297. [Google Scholar] [CrossRef]
- Moreno-Acosta, P.; Vallard, A.; Carrillo, S.; Gamboa, O.; Romero-Rojas, A.; Molano, M.; Acosta, J.; Mayorga, D.; Rancoule, C.; Garcia, M.A.; et al. Biomarkers of resistance to radiation therapy: A prospective study in cervical carcinoma. Radiat. Oncol. 2017, 12, 120. [Google Scholar] [CrossRef]
- Ward, C.; Meehan, J.; Gray, M.; Kunkler, I.; Langdon, S.; Argyle, D. Carbonic Anhydrase IX (CAIX), Cancer, and Radiation Responsiveness. Metabolites 2018, 8, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilardi, G.; Zambrano, N.; Merolla, F.; Siano, M.; Varricchio, S.; Vecchione, M.; Rosa, G.; Mascolo, M.; Staibano, S. Histopathological Determinants of Tumor Resistance: A Special Look to the Immunohistochemical Expression of Carbonic Anhydrase IX in Human Cancers. Curr. Med. Chem. 2014, 21, 1569–1582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zatovicova, M.; Sedlakova, O.; Svastova, E.; Ohradanova, A.; Ciampor, F.; Arribas, J.; Pastorek, J.; Pastorekova, S. Ectodomain shedding of the hypoxia-induced carbonic anhydrase IX is a metalloprotease-dependent process regulated by TACE/ADAM17. Br. J. Cancer 2005, 93, 1267–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidlickova, I.; Dequiedt, F.; Jelenska, L.; Sedlakova, O.; Pastorek, M.; Stuchlik, S.; Pastorek, J.; Zatovicova, M.; Pastorekova, S. Apoptosis-induced ectodomain shedding of hypoxia-regulated carbonic anhydrase IX from tumor cells: A double-edged response to chemotherapy. BMC Cancer 2016, 16, 239. [Google Scholar] [CrossRef] [Green Version]
- Zatovicova, M.; Kajanova, I.; Takacova, M.; Jelenska, L.; Sedlakova, O.; Labudova, M.; Pastorekova, S. ADAM10 mediates shedding of carbonic anhydrase IX ectodomain non-redundantly to ADAM17. Oncol. Rep. 2022, 49, 27. [Google Scholar] [CrossRef]
- Horie, K.; Kawakami, K.; Fujita, Y.; Sugaya, M.; Kameyama, K.; Mizutani, K.; Deguchi, T.; Ito, M. Exosomes expressing carbonic anhydrase 9 promote angiogenesis. Biochem. Biophys. Res. Commun. 2017, 492, 356–361. [Google Scholar] [CrossRef]
- Logozzi, M.; Capasso, C.; Di Raimo, R.; Del Prete, S.; Mizzoni, D.; Falchi, M.; Supuran, C.T.; Fais, S. Prostate cancer cells and exosomes in acidic condition show increased carbonic anhydrase IX expression and activity. J. Enzym. Inhib. Med. Chem. 2019, 34, 272–278. [Google Scholar] [CrossRef] [Green Version]
- Wind, T.C.; Messenger, M.P.; Thompson, D.; Selby, P.J.; Banks, R.E. Measuring carbonic anhydrase IX as a hypoxia biomarker: Differences in concentrations in serum and plasma using a commercial enzyme-linked immunosorbent assay due to influences of metal ions. Ann. Clin. Biochem. Int. J. Lab. Med. 2011, 48, 112–120. [Google Scholar] [CrossRef] [Green Version]
- Ho, D.; Huang, J.; Chapman, J.-A.W.; Leitzel, K.; Ali, S.M.; Shepherd, L.; Parulekar, W.R.; Ellis, C.E.; Crescnzo, R.J.; Zhu, L.; et al. Impact of serum HER2, TIMP-1, and CAIX on outcome for HER2+ metastatic breast cancer patients: CCTG MA.31 (lapatinib vs. trastuzumab). Breast Cancer Res. Treat. 2017, 164, 571–580. [Google Scholar] [CrossRef]
- Müller, V.; Riethdorf, S.; Rack, B.; Janni, W.; Fasching, P.A.; Solomayer, E.; Aktas, B.; Kasimir-Bauer, S.; Zeitz, J.; Pantel, K.; et al. Prospective evaluation of serum tissue inhibitor of metalloproteinase 1 and carbonic anhydrase IX in correlation to circulating tumor cells in patients with metastatic breast cancer. Breast Cancer Res. BCR 2011, 13, R71. [Google Scholar] [CrossRef] [Green Version]
- Brown-Glaberman, U.; Marron, M.; Chalasani, P.; Livingston, R.; Iannone, M.; Specht, J.; Stopeck, A.T. Circulating Carbonic Anhydrase IX and Antiangiogenic Therapy in Breast Cancer. Dis. Markers 2016, 2016, 9810383. [Google Scholar] [CrossRef] [Green Version]
- Janning, M.; Müller, V.; Vettorazzi, E.; Cubas-Cordova, M.; Gensch, V.; Ben-Batalla, I.; Zu Eulenburg, C.; Schem, C.; Fasching, P.A.; Schnappauf, B.; et al. Evaluation of soluble carbonic anhydrase IX as predictive marker for efficacy of bevacizumab: A biomarker analysis from the geparquinto phase III neoadjuvant breast cancer trial. Int. J. Cancer 2019, 145, 857–868. [Google Scholar] [CrossRef]
- Takacova, M.; Kajanova, I.; Kolarcikova, M.; Lapinova, J.; Zatovicova, M.; Pastorekova, S. Understanding metabolic alterations and heterogeneity in cancer progression through validated immunodetection of key molecular components: A case of carbonic anhydrase IX. Cancer Metastasis Rev. 2021, 40, 1035–1053. [Google Scholar] [CrossRef]
- Zatovicova, M.; Tarabkova, K.; Svastova, E.; Gibadulinova, A.; Mucha, V.; Jakubicková, L.; Biesová, Z.; Rafajová, M.; Ortova Gut, M.; Parkkila, S.; et al. Monoclonal antibodies generated in carbonic anhydrase IX-deficient mice recognize different domains of tumour-associated hypoxia-induced carbonic anhydrase IX. J. Immunol. Methods 2003, 282, 117–134. [Google Scholar] [CrossRef]
- Pastoreková, S.; Závadová, Z.; Košťál, M.; Babušíková, O.; Závada, J. A novel quasi-viral agent, MaTu, is a two-component system. Virology 1992, 187, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Bartošová, M.; Parkkila, S.; Pohlodek, K.; Karttunen, T.J.; Galbavý, Š.; Mucha, V.; Harris, A.L.; Pastorek, J.; Pastoreková, S. Expression of carbonic anhydrase IX in breast is associated with malignant tissues and is related to overexpression of c-erbB2: Carbonic anhydrase IX and c-erbB2 in breast cancer. J. Pathol. 2002, 197, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Chia, S.K.; Wykoff, C.C.; Watson, P.H.; Han, C.; Leek, R.D.; Pastorek, J.; Gatter, K.C.; Ratcliffe, P.; Harris, A.L. Prognostic significance of a novel hypoxia-regulated marker, carbonic anhydrase IX, in invasive breast carcinoma. J. Clin. Oncol. 2001, 19, 3660–3668. [Google Scholar] [CrossRef] [PubMed]
- Kalavska, K.; Chovanec, M.; Zatovicova, M.; Takacova, M.; Gronesova, P.; Svetlovska, D.; Baratova, M.; Miskovska, V.; Obertova, J.; Palacka, P.; et al. Prognostic value of serum carbonic anhydrase IX in testicular germ cell tumor patients. Oncol. Lett. 2016, 12, 2590–2598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouyang, J.; Qin, G.; Liu, Z.; Jian, X.; Shi, T.; Xie, L. ToPP: Tumor online prognostic analysis platform for prognostic feature selection and clinical patient subgroup selection. iScience 2022, 25, 104190. [Google Scholar] [CrossRef]
- Jézéquel, P.; Gouraud, W.; Ben Azzouz, F.; Guérin-Charbonnel, C.; Juin, P.P.; Lasla, H.; Campone, M. bc-GenExMiner 4.5: New mining module computes breast cancer differential gene expression analyses. Database 2021, 2021, baab007. [Google Scholar] [CrossRef]
- Amat, S.; Penault-Llorca, F.; Cure, H.; Le Bouedëc, G.; Achard, J.-L.; Van Praagh, I.; Feillel, V.; Mouret-Reynier, M.-A.; Dauplat, J.; Chollet, P. Scarff-Bloom-Richardson (SBR) grading: A pleiotropic marker of chemosensitivity in invasive ductal breast carcinomas treated by neoadjuvant chemotherapy. Int. J. Oncol. 2002, 20, 791–796. [Google Scholar] [CrossRef]
- D’Eredita’, G.; Giardina, C.; Martellotta, M.; Natale, T.; Ferrarese, F. Prognostic factors in breast cancer: The predictive value of the Nottingham Prognostic Index in patients with a long-term follow-up that were treated in a single institution. Eur. J. Cancer 2001, 37, 591–596. [Google Scholar] [CrossRef]
- Fong, Y.; Evans, J.; Brook, D.; Kenkre, J.; Jarvis, P.; Gower-Thomas, K. The Nottingham Prognostic Index: Five- and ten-year data for all-cause Survival within a Screened Population. Ann. R. Coll. Surg. Engl. 2015, 97, 137–139. [Google Scholar] [CrossRef] [Green Version]
- Hussain, S.A.; Ganesan, R.; Reynolds, G.; Gross, L.; Stevens, A.; Pastorek, J.; Murray, P.G.; Perunovic, B.; Anwar, M.S.; Billingham, L.; et al. Hypoxia-regulated carbonic anhydrase IX expression is associated with poor survival in patients with invasive breast cancer. Br. J. Cancer 2007, 96, 104–109. [Google Scholar] [CrossRef]
- Generali, D.; Fox, S.B.; Berruti, A.; Brizzi, M.P.; Campo, L.; Bonardi, S.; Wigfield, S.M.; Bruzzi, P.; Bersiga, A.; Allevi, G.; et al. Role of carbonic anhydrase IX expression in prediction of the efficacy and outcome of primary epirubicin/tamoxifen therapy for breast cancer. Endocr. Relat. Cancer 2006, 13, 921–930. [Google Scholar] [CrossRef] [Green Version]
- Tomes, L.; Emberley, E.; Niu, Y.; Troup, S.; Pastorek, J.; Strange, K.; Harris, A.; Watson, P.H. Necrosis and hypoxia in invasive breast carcinoma. Breast Cancer Res. Treat. 2003, 81, 61–69. [Google Scholar] [CrossRef]
- Neumeister, V.M.; Sullivan, C.A.; Lindner, R.; Lezon-Geyda, K.; Li, J.; Zavada, J.; Martel, M.; Glazer, P.M.; Tuck, D.P.; Rimm, D.L.; et al. Hypoxia-induced protein CAIX is associated with somatic loss of BRCA1 protein and pathway activity in triple negative breast cancer. Breast Cancer Res. Treat. 2012, 136, 67–75. [Google Scholar] [CrossRef]
- Krieg, A.; Mwahech-Fauceglia, P.; Lim, J.; Pejovic, T. Co-expression of the Hypoxic Marker Carbonic Anhydrase 9 (CA-IX) with Breast Cancer Associated 1 (BRCA1) is associated with faster recurrence in High Grade Serous Adenocarcinoma. Gynecol. Oncol. 2017, 147, 199. [Google Scholar] [CrossRef]
- Rafajová, M.; Zatovicová, M.; Kettmann, R.; Pastorek, J.; Pastoreková, S. Induction by hypoxia combined with low glucose or low bicarbonate and high posttranslational stability upon reoxygenation contribute to carbonic anhydrase IX expression in cancer cells. Int. J. Oncol. 2004, 24, 995–1004. [Google Scholar] [CrossRef]
- Olive, P.L.; Aquino-Parsons, C.; MacPhail, S.H.; Liao, S.Y.; Raleigh, J.A.; Lerman, M.I.; Stanbridge, E.J. Carbonic anhydrase 9 as an endogenous marker for hypoxic cells in cervical cancer. Cancer Res. 2001, 61, 8924–8929. [Google Scholar]
- Barathova, M.; Takacova, M.; Holotnakova, T.; Gibadulinova, A.; Ohradanova, A.; Zatovicova, M.; Hulikova, A.; Kopacek, J.; Parkkila, S.; Supuran, C.T.; et al. Alternative splicing variant of the hypoxia marker carbonic anhydrase IX expressed independently of hypoxia and tumour phenotype. Br. J. Cancer 2008, 98, 129–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Švastová, E.; Žilka, N.; Zat’ovičová, M.; Gibadulinová, A.; Čiampor, F.; Pastorek, J.; Pastoreková, S. Carbonic anhydrase IX reduces E-cadherin-mediated adhesion of MDCK cells via interaction with β-catenin. Exp. Cell Res. 2003, 290, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Zatovicova, M.; Jelenska, L.; Hulikova, A.; Csaderova, L.; Ditte, Z.; Ditte, P.; Goliasova, T.; Pastorek, J.; Pastorekova, S. Carbonic Anhydrase IX as an Anticancer Therapy Target: Preclinical Evaluation of Internalizing Monoclonal Antibody Directed to Catalytic Domain. Curr. Pharm. Des. 2010, 16, 3255–3263. [Google Scholar] [CrossRef]
- Bourseau-Guilmain, E.; Menard, J.A.; Lindqvist, E.; Indira Chandran, V.; Christianson, H.C.; Cerezo Magaña, M.; Lidfeldt, J.; Marko-Varga, G.; Welinder, C.; Belting, M. Hypoxia regulates global membrane protein endocytosis through caveolin-1 in cancer cells. Nat. Commun. 2016, 7, 11371. [Google Scholar] [CrossRef] [Green Version]
- Zaťovičová, M.; Pastoreková, S. Modulation of cell surface density of carbonic anhydrase IX by shedding of the ectodomain and endocytosis. Acta Virol. 2013, 57, 257–264. [Google Scholar] [CrossRef] [Green Version]
- Famta, P.; Shah, S.; Khatri, D.K.; Guru, S.K.; Singh, S.B.; Srivastava, S. Enigmatic role of exosomes in breast cancer progression and therapy. Life Sci. 2022, 289, 120210. [Google Scholar] [CrossRef]
- Buanne, P.; Renzone, G.; Monteleone, F.; Vitale, M.; Monti, S.M.; Sandomenico, A.; Garbi, C.; Montanaro, D.; Accardo, M.; Troncone, G.; et al. Characterization of Carbonic Anhydrase IX Interactome Reveals Proteins Assisting Its Nuclear Localization in Hypoxic Cells. J. Proteome Res. 2013, 12, 282–292. [Google Scholar] [CrossRef] [Green Version]
- Barsoum, I.B.; Hamilton, T.K.; Li, X.; Cotechini, T.; Miles, E.A.; Siemens, D.R.; Graham, C.H. Hypoxia Induces Escape from Innate Immunity in Cancer Cells via Increased Expression of ADAM10: Role of Nitric Oxide. Cancer Res. 2011, 71, 7433–7441. [Google Scholar] [CrossRef] [Green Version]
- Rzymski, T.; Petry, A.; Kračun, D.; Rieß, F.; Pike, L.; Harris, A.L.; Görlach, A. The unfolded protein response controls induction and activation of ADAM17/TACE by severe hypoxia and ER stress. Oncogene 2012, 31, 3621–3634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGowan, P.M.; McKiernan, E.; Bolster, F.; Ryan, B.M.; Hill, A.D.K.; McDermott, E.W.; Evoy, D.; O’Higgins, N.; Crown, J.; Duffy, M.J. ADAM-17 predicts adverse outcome in patients with breast cancer. Ann. Oncol. 2008, 19, 1075–1081. [Google Scholar] [CrossRef]
- Mullooly, M.; McGowan, P.M.; Kennedy, S.A.; Madden, S.F.; Crown, J.; O’ Donovan, N.; Duffy, M.J. ADAM10: A new player in breast cancer progression? Br. J. Cancer 2015, 113, 945–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, H.W.; Defamie, V.; Waterhouse, P.; Khokha, R. TIMPs: Versatile extracellular regulators in cancer. Nat. Rev. Cancer 2017, 17, 38–53. [Google Scholar] [CrossRef] [PubMed]
- Cheng, G.; Fan, X.; Hao, M.; Wang, J.; Zhou, X.; Sun, X. Higher levels of TIMP-1 expression are associated with a poor prognosis in triple-negative breast cancer. Mol. Cancer 2016, 15, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajanova, I.; Zatovicova, M.; Jelenska, L.; Sedlakova, O.; Barathova, M.; Csaderova, L.; Debreova, M.; Lukacikova, L.; Grossmannova, K.; Labudova, M.; et al. Impairment of carbonic anhydrase IX ectodomain cleavage reinforces tumorigenic and metastatic phenotype of cancer cells. Br. J. Cancer 2020, 122, 1590–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Della Rocca, Y.; Fonticoli, L.; Rajan, T.S.; Trubiani, O.; Caputi, S.; Diomede, F.; Pizzicannella, J.; Marconi, G.D. Hypoxia: Molecular pathophysiological mechanisms in human diseases. J. Physiol. Biochem. 2022, 78, 739–752. [Google Scholar] [CrossRef] [PubMed]
- Tal, R. The Role of Hypoxia and Hypoxia-Inducible Factor-1Alpha in Preeclampsia Pathogenesis. Biol. Reprod. 2012, 87, 134. [Google Scholar] [CrossRef]
- Galbiati, S.; Gabellini, D.; Ambrosi, A.; Soriani, N.; Pasi, F.; Locatelli, M.; Lucianò, R.; Candiani, M.; Valsecchi, L.; Zerbini, G.; et al. Early increase in circulating carbonic anhydrase IX: A potential new predictive biomarker of preeclampsia. Front. Mol. Biosci. 2023, 10, 1075604. [Google Scholar] [CrossRef]
- Grossmannova, K.; Barathova, M.; Belvoncikova, P.; Lauko, V.; Csaderova, L.; Tomka, J.; Dulka, T.; Pastorek, J.; Madaric, J. Hypoxia Marker Carbonic Anhydrase IX Is Present in Abdominal Aortic Aneurysm Tissue and Plasma. Int. J. Mol. Sci. 2022, 23, 879. [Google Scholar] [CrossRef]
- Geçkil, A.A.; Kıran, T.R.; Berber, N.K.; Otlu, Ö.; Erdem, M.; İn, E. Carbonic Anhydrase IX as a Marker of Disease Severity in Obstructive Sleep Apnea. Medicina 2022, 58, 1643. [Google Scholar] [CrossRef]
- Merkx, R.I.J.; Lobeek, D.; Konijnenberg, M.; Jiménez-Franco, L.D.; Kluge, A.; Oosterwijk, E.; Mulders, P.F.A.; Rijpkema, M. Phase I study to assess safety, biodistribution and radiation dosimetry for 89Zr-girentuximab in patients with renal cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3277–3285. [Google Scholar] [CrossRef]
- Verhoeff, S.R.; van Es, S.C.; Boon, E.; van Helden, E.; Angus, L.; Elias, S.G.; Oosting, S.F.; Aarntzen, E.H.; Brouwers, A.H.; Kwee, T.C.; et al. Lesion detection by [89Zr]Zr-DFO-girentuximab and [18F]FDG-PET/CT in patients with newly diagnosed metastatic renal cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1931–1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zatovicova, M.; Kajanova, I.; Barathova, M.; Takacova, M.; Labudova, M.; Csaderova, L.; Jelenska, L.; Svastova, E.; Pastorekova, S.; Harris, A.L.; et al. Novel humanized monoclonal antibodies for targeting hypoxic human tumors via two distinct extracellular domains of carbonic anhydrase IX. Cancer Metab. 2022, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Schütze, D.; Milde-Langosch, K.; Witzel, I.; Rody, A.; Karn, T.; Schmidt, M.; Choschzick, M.; Jänicke, F.; Müller, V. Relevance of cellular and serum carbonic anhydrase IX in primary breast cancer. J. Cancer Res. Clin. Oncol. 2013, 139, 747–754. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; Dang, C.; et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2022, 20, 691–722. [Google Scholar] [CrossRef] [PubMed]
- Ellis, I.O.; Rakha, E.A.; Tse, G.M.; Tan, P.H. An international unified approach to reporting and grading invasive breast cancer. An overview of the International Collaboration on Cancer Reporting (ICCR) initiative. Histopathology 2023, 82, 189–197. [Google Scholar] [CrossRef] [PubMed]







| No. of Evaluated Patients | 100 | |
|---|---|---|
| Age–median (range) | 57.5 (34–85) | |
| Menopausal status | ||
| Pre-menopause | 26 | 26% |
| Post-menopause | 73 | 73% |
| Not applicable—male | 1 | 1% |
| Grade | ||
| I | 6 | 6% |
| II | 57 | 57% |
| III | 36 | 36% |
| DCIS | 1 | 1% |
| T stage | ||
| pTis | 3 | 3% |
| pT1 | 56 | 56% |
| pT2 | 37 | 37% |
| pT3 | 3 | 3% |
| pT4 | 1 | 1% |
| N status | ||
| pN0 | 64 | 64% |
| pN1 | 21 | 21% |
| pN2 | 12 | 12% |
| pN3 | 3 | 3% |
| ER | ||
| Positive | 86 | 86% |
| Negative | 14 | 14% |
| PR | ||
| Positive | 81 | 81% |
| Negative | 19 | 19% |
| HER2 | ||
| Positive | 16 | 16% |
| Negative | 84 | 84% |
| Tumor necrosis | ||
| Negative | 78 | 78% |
| Positive (+) | 14 | 14% |
| Positive (+++) | 1 | 1% |
| Micro | 6 | 6% |
| Comedo necrosis | 1 | 1% |
| Variables (n) | CA IX+ (n = 24) | CA IX- (n = 76) | p-Value | CA IX Score | p-Value | ||
|---|---|---|---|---|---|---|---|
| Low | Focal | High | |||||
| Subtype | |||||||
| Luminal A (54) | 9 | 45 | 0.0115 | 3 | 4 | 2 | ns |
| Luminal B-like (18) | 5 | 13 | 0 | 2 | 3 | ||
| HER2-enriched (16) | 3 | 13 | 1 | 1 | 1 | ||
| TNBC (9) | 6 | 3 | 2 | 1 | 3 | ||
| DCIS (3) | 1 | 2 | 1 | 0 | 0 | ||
| Grade | |||||||
| I/II (63) | 10 | 53 | 0.0146 | 4 | 5 | 1 | 0.0060 |
| III (36) | 14 | 22 | 3 | 3 | 8 | ||
| pT | |||||||
| pT1 (56) | 9 | 47 | ns | 2 | 4 | 3 | ns |
| pT2-4 (41) | 14 | 27 | 4 | 4 | 6 | ||
| pN | |||||||
| pN0 (64) | 14 | 50 | ns | 2 | 6 | 6 | ns |
| pN1-3 (36) | 10 | 26 | 5 | 2 | 3 | ||
| ER | |||||||
| Positive (86) | 17 | 69 | 0.0019 | 4 | 7 | 6 | ns |
| Negative (14) | 7 | 7 | 3 | 1 | 3 | ||
| PR | |||||||
| Positive (81) | 17 | 64 | ns | 4 | 7 | 6 | ns |
| Negative (19) | 7 | 12 | 3 | 1 | 3 | ||
| HER2 | |||||||
| Positive (16) | 3 | 13 | ns | 1 | 1 | 1 | ns |
| Negative (84) | 21 | 63 | 6 | 7 | 8 | ||
| Tumor necrosis | |||||||
| Positive (21) | 11 | 10 | 0.0015 | 4 | 3 | 4 | 0.0062 |
| Negative (78) | 13 | 65 | 3 | 5 | 5 | ||
| CA IX Score | Clinicopathological Variables | tCA IX | sCA IX | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| pT | pN | Grade | ER/PR | HER2 | Molecular Subtype | Necrosis | L | I | % Cells | pg/mL | |
| Low | 2c | 1a | III | -/- | - | TNBC | + | M + C | + | <10% | 954.0 |
| 1c | 2a | III | -/- | - | TNBC | 0 | M + C | + | <10% | 1392.0 | |
| 4b (m) | 3a | II | +/+ | - | Luminal A | + | M + C | + | <10% | 1662.0 | |
| 1b | 0(sn) | I | +/+ | - | Luminal A | 0 | M | + | <10% | 2592.0 | |
| 2 (m) | 1a | II | +/+ | - | Luminal A | 0 | C | + / ++ | <10% | 750.0 | |
| is (m) | 0(sn) | II | +/+ | - | DCIS | + | C | + | <10% | 978.0 | |
| 2 | 1a | III | -/- | 3+ | HER2+ | + | C | + | <10% | 552.0 | |
| Focal | 3 | 0 | III | -/- | - | TNBC | +++ | M+C | ++ | 11–50% | 813.0 |
| 2 | 2a | II | +/+ | - | Luminal B-like | + | M + C | ++ | 11–50% | 951.0 | |
| 1c | 0(sn) | II | +/+ | - | Luminal A | 0 | C | ++ | 11–50% | 726.0 | |
| 1c | 0(sn) | II | +/+ | - | Luminal A | 0 | C | + / ++ | 11–50% | 579.0 | |
| 2 (m) | 0 | III | +/+ | + | HER2+ | + | C | + / ++ | 11–50% | 1041.0 | |
| 2 | 0(sn) | II | +/+ | - | Luminal A | 0 | M | ++ | 11–50% | 487.5 | |
| 1a | 0(sn) | II | +/+ | - | Luminal A | 0 | C | ++ | 11–50% | 0.0 | |
| 1b | 2a | III | +/+ | - | Luminal B-like | 0 | C | ++ | 11–50% | 0.0 | |
| High | 2 | 0 | III | +/+ | - | Luminal B-like | 0 | M | +++ | >50% | 588.0 |
| 2 | 1a | III | +/+ | - | Luminal B-like | 0 | M | +++ | >50% | 906.0 | |
| 1c | 0 (sn) | III | +/+ | - | Luminal B-like | + | M | +++ | >50% | 903.0 | |
| 2 | 2a | III | +/+ | + | HER2+ | + | M | +++ | >50% | 615.0 | |
| 1c | 0 (sn) | III | +/+ | - | Luminal A | 0 | M | +++ | >50% | 1431.0 | |
| 1c | 1a | II | +/+ | - | Luminal A | 0 | M | +++ | >50% | 792.0 | |
| 2 | 0 | III | -/- | - | TNBC | + | M | +++ | >50% | 564.0 | |
| 2 | 0(sn) | III | -/- | - | TNBC | 0 | M | +++ | >50% | 459.0 | |
| 2 (m) | 0 | III | -/- | - | TNBC | + | M | +++ | >50% | 210.6 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rezuchova, I.; Bartosova, M.; Belvoncikova, P.; Takacova, M.; Zatovicova, M.; Jelenska, L.; Csaderova, L.; Meciarova, I.; Pohlodek, K. Carbonic Anhydrase IX in Tumor Tissue and Plasma of Breast Cancer Patients: Reliable Biomarker of Hypoxia and Prognosis. Int. J. Mol. Sci. 2023, 24, 4325. https://doi.org/10.3390/ijms24054325
Rezuchova I, Bartosova M, Belvoncikova P, Takacova M, Zatovicova M, Jelenska L, Csaderova L, Meciarova I, Pohlodek K. Carbonic Anhydrase IX in Tumor Tissue and Plasma of Breast Cancer Patients: Reliable Biomarker of Hypoxia and Prognosis. International Journal of Molecular Sciences. 2023; 24(5):4325. https://doi.org/10.3390/ijms24054325
Chicago/Turabian StyleRezuchova, Ingeborg, Maria Bartosova, Petra Belvoncikova, Martina Takacova, Miriam Zatovicova, Lenka Jelenska, Lucia Csaderova, Iveta Meciarova, and Kamil Pohlodek. 2023. "Carbonic Anhydrase IX in Tumor Tissue and Plasma of Breast Cancer Patients: Reliable Biomarker of Hypoxia and Prognosis" International Journal of Molecular Sciences 24, no. 5: 4325. https://doi.org/10.3390/ijms24054325