
Pyrroles as a Potential Biomarker for Oxidative Stress Disorders


Abstract
:1. Pyrroles
2. Previous Clinical Studies with Pyrroles
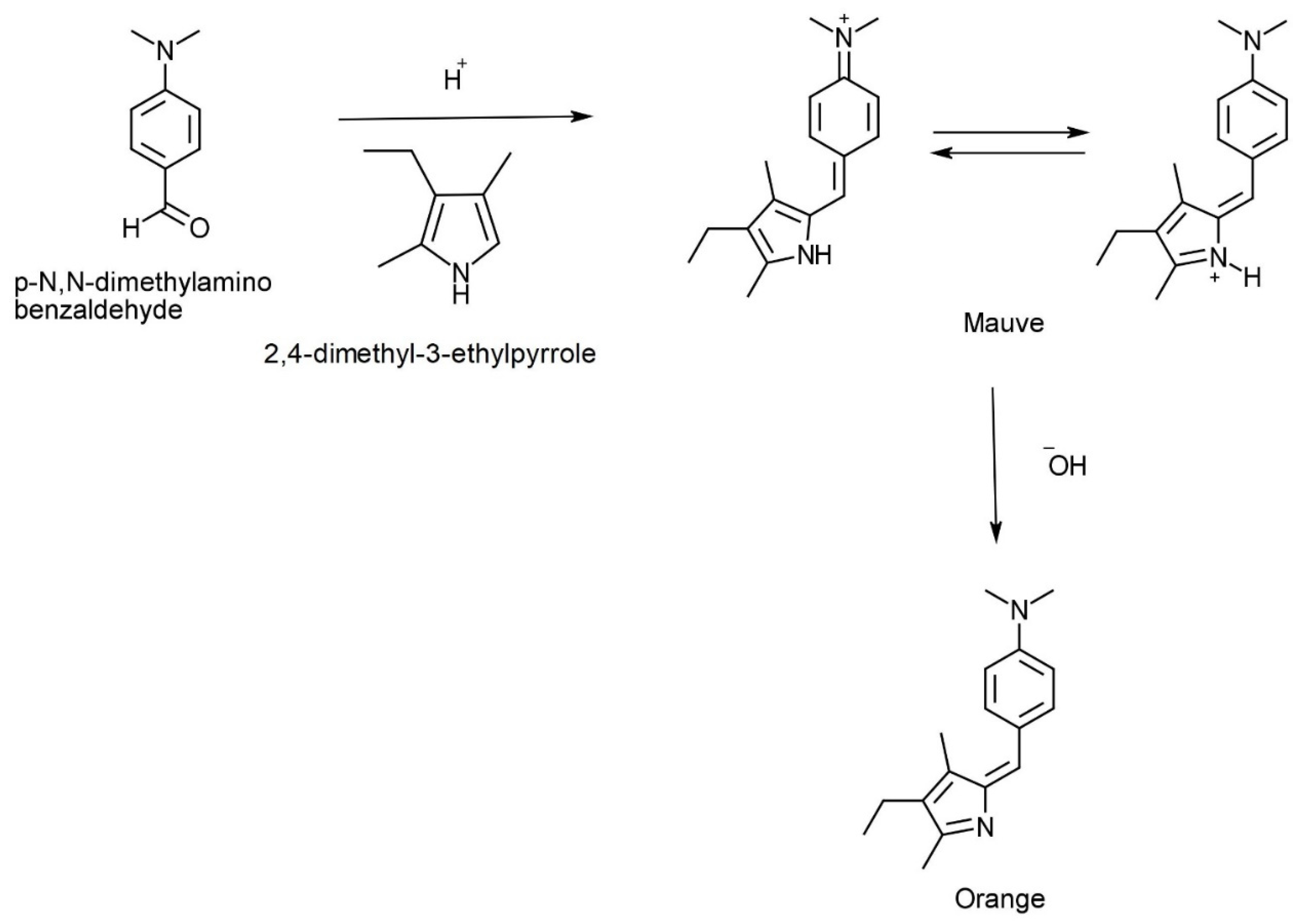
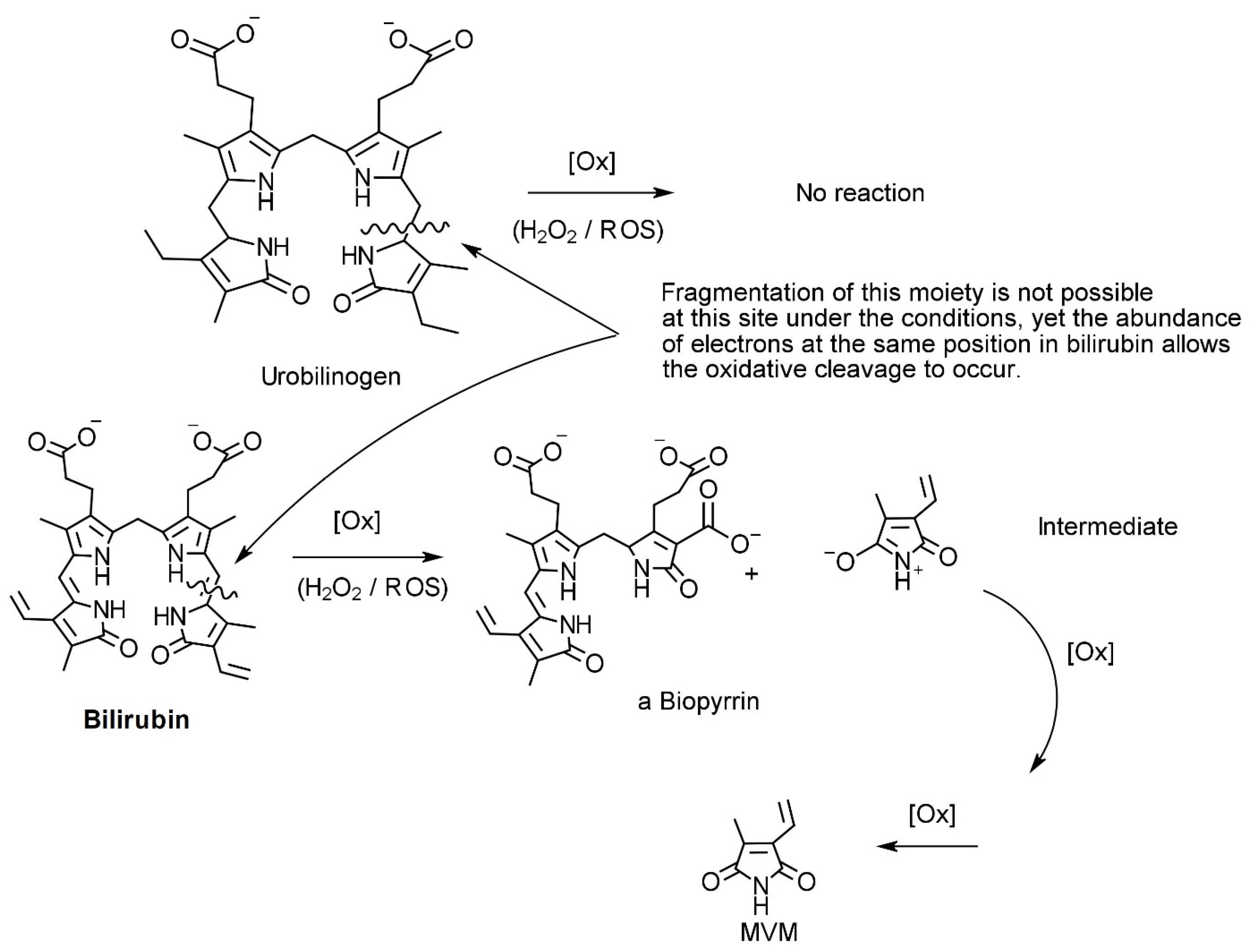
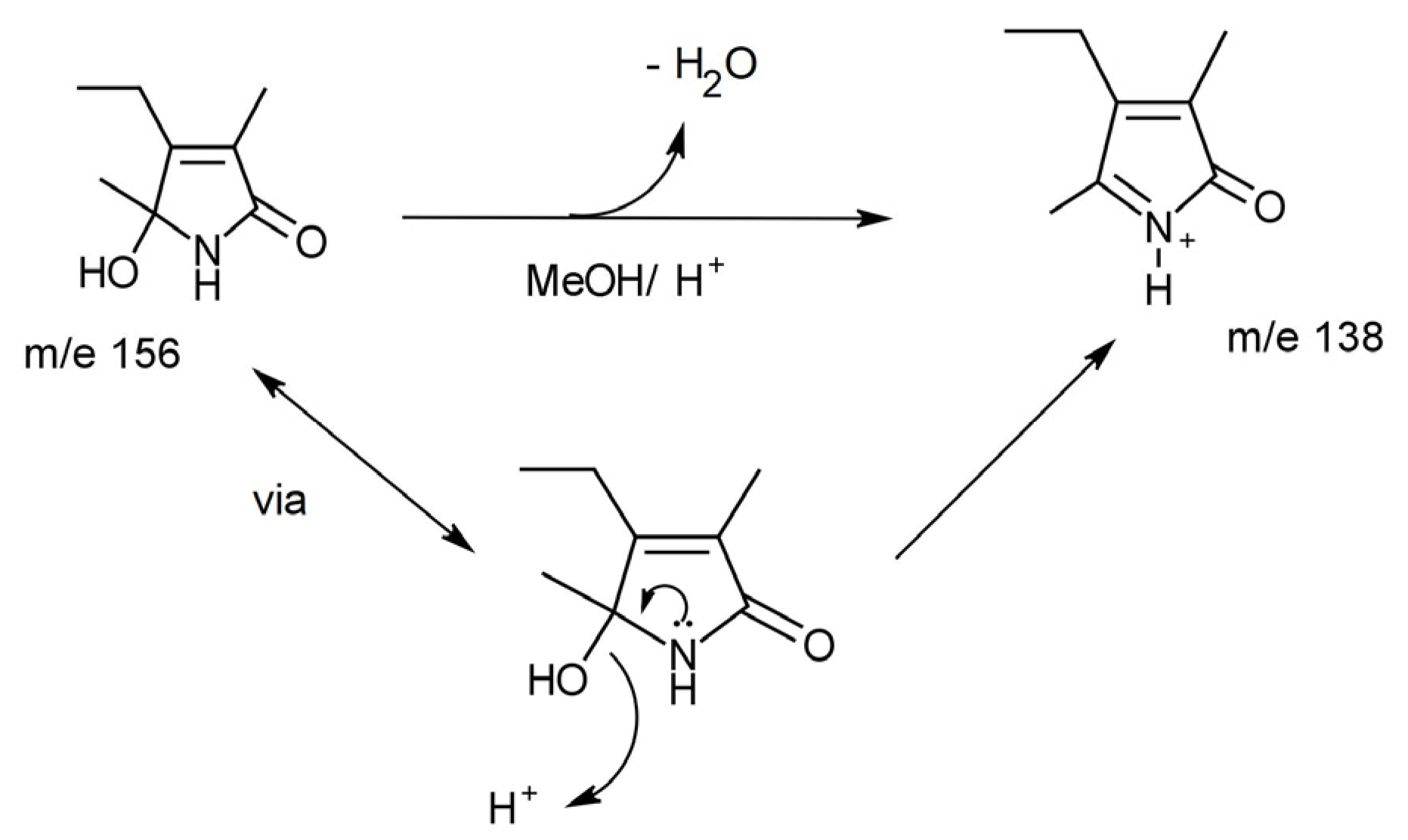
3. Chemistry of HPL, DMAB, and Pyrroles
4. Treatment of Elevated Pyrroles
5. Limitations of the Assay
6. Recommendations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guest, G.H. A Study of Pyrroles in Biological Materials McGill University Libraries; McGill University: Montreal, QC, Canada, 1938. [Google Scholar]
- Reichstein, T. The Pine-Splinter Reaction of Furan Compounds. Helv. Chim. Acta 1932, 15, 1110–1112. [Google Scholar] [CrossRef]
- Runge, F.F. Ueber einige Produkte der Steinkohlendestillation. Ann. Physik. 1834, 107, 65–78. [Google Scholar] [CrossRef]
- Irvine, D.G. Hydroxy-hemopyrrolenone, not kryptopyrrole, in the urine of schizophrenics and porphyrics. Clin. Chem. 1978, 24, 2069–2070. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, A. Malvaria, schizophrenia and the HOD test. Int. J. Neuropsychiatr. 1966, 2, 175–178. [Google Scholar]
- Hoffer, A.; Mahon, M. The presence of unidentified substances in the urine of psychiatric patients. J. Neuropsychiatr. 1961, 2, 331–362. [Google Scholar]
- Voisey, J.; Swagell, C.D.; Hughes, I.P.; Connor, J.P.; Lawford, B.R.; Young, R.M.; Morris, C.P. A polymorphism in the dysbindin gene (DTNBP1) associated with multiple psychiatric disorders including schizophrenia. Behav. Brain Funct. 2010, 6, 41. [Google Scholar] [CrossRef]
- McLeay, S.C.; Harvey, W.M.; Romaniuk, M.N.; Crawford, D.H.; Colquhoun, D.M.; Young, R.M.; Dwyer, M.; Gibson, J.; O’Sullivan, R.A.; Cooksley, G.; et al. Physical comorbidities of post-traumatic stress disorder in Australian Vietnam War veterans. Med. J. Aust. 2017, 206, 251–257. [Google Scholar] [CrossRef]
- Warren, B.; Sarris, J.; Mulder, R.T.; Rucklidge, J.J. Pyroluria: Fact or Fiction? J. Altern. Complement. Med. 2021, 27, 407–415. [Google Scholar] [CrossRef]
- O’Reilly, P.O.; Hughes, G.; Russell, R.T.; Ernest, M. The mauve factor: An evaluation. Dis. Nerv. Syst. 1965, 26, 562–568. [Google Scholar]
- Sohler, A.; Beck, R.; Noval, J.J. Mauve factor re-identified as 2,4-dimethyl-3-ethylpyrrole and its sedative effect on the CNS. Nature 1970, 228, 1318–1320. [Google Scholar] [CrossRef]
- Pfeiffer, C.C.; Sohler, A. Treatment of Pyroluric Schizophrenia with Large Doses of Pyridoxine and a dietry Supplement of Zinc. J. Orthomol. Med. 1974, 3, 292–300. [Google Scholar]
- Walsh, W.J.; Glab, L.B.; Haakenson, M.L. Reduced violent behavior following biochemical therapy. Physiol. Behav. 2004, 82, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Stuckey, R.; Walsh, W.; Lambert, B. The Effectiveness of Targeted Nutrient Therapy in Treatment of Mental Illness. J. Australas. Coll. Nutr. Environ. Med. 2010, 29, 3. [Google Scholar]
- Cruz, R.; Vogel, W.H. Pyroluria: A poor marker in chronic schizophrenia. Am. J. Psychiatry 1978, 135, 1239–1240. [Google Scholar]
- Gorchein, A. Urine concentration of 3-ethyl-5-hydroxy-4,5-dimethyl-delta 3-pyrrolin-2-one (‘mauve factor’) is not causally related to schizophrenia or to acute intermittent porphyria. Clin. Sci. (Lond. Engl. 1979) 1980, 58, 469–476. [Google Scholar] [CrossRef]
- Mikirova, N. Clinical Test of Pyrroles: Usefulness and Association with Other Biochemical Markers. Clin. Med. Rev. Case Rep. 2015, 2, 27. [Google Scholar] [CrossRef]
- Fryar-Williams, S.; Strobel, J.E. Biomarker Case-Detection and Prediction with Potential for Functional Psychosis Screening: Development and Validation of a Model Related to Biochemistry, Sensory Neural Timing and End Organ Performance. Front. Psychiatry 2016, 7, 48. [Google Scholar] [CrossRef]
- Gonzalez-Liencres, C.; Tas, C.; Brown, E.C.; Erdin, S.; Onur, E.; Cubukcoglu, Z.; Aydemir, O.; Esen-Danaci, A.; Brüne, M. Oxidative stress in schizophrenia: A case-control study on the effects on social cognition and neurocognition. BMC Psychiatry 2014, 14, 268. [Google Scholar] [CrossRef]
- Pistis, G.; Vazquez-Bourgon, J.; Fournier, M.; Jenni, R.; Cleusix, M.; Papiol, S.; Smart, S.E.; Pardiñas, A.F.; Walters, J.T.R.; MacCabe, J.H.; et al. Gene set enrichment analysis of pathophysiological pathways highlights oxidative stress in psychosis. Mol. Psychiatry 2022, 27, 5135–5143. [Google Scholar] [CrossRef]
- Rambaud, V.; Marzo, A.; Chaumette, B. Oxidative Stress and Emergence of Psychosis. Antioxidants 2022, 11, 1870. [Google Scholar] [CrossRef]
- Hambly, J.L.; Francis, K.; Khan, S.; Gibbons, K.S.; Walsh, W.J.; Lambert, B.; Testa, C.; Haywood, A. Micronutrient Therapy for Violent and Aggressive Male Youth: An Open-Label Trial. J. Child. Adolesc. Psychopharmacol. 2017, 27, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Voisey, J.; Swagell, C.D.; Hughes, I.P.; Lawford, B.R.; Young, R.M.; Morris, C.P. Analysis of HapMap tag-SNPs in dysbindin (DTNBP1) reveals evidence of consistent association with schizophrenia. Eur. Psychiatry 2010, 25, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Wockner, L.F.; Noble, E.P.; Lawford, B.R.; Young, R.M.; Morris, C.P.; Whitehall, V.L.J.; Voisey, J. Genome-wide DNA methylation analysis of human brain tissue from schizophrenia patients. Transl. Psychiatry 2014, 4, e339. [Google Scholar] [CrossRef] [PubMed]
- Wockner, L.F.; Morris, C.P.; Noble, E.P.; Lawford, B.R.; Whitehall, V.L.J.; Young, R.; Voisey, J. Brain-specific epigenetic markers of schizophrenia. Transl. Psychiatry 2015, 5, e680. [Google Scholar] [CrossRef] [PubMed]
- Van Urk, H.W. p-Dimethylamino benzaldehyde as a Reagent for Organic Drugs. Pharm. Weekbl. 1929, 66, 101–108. [Google Scholar]
- Clark, J.F.; Reilly, M.; Sharp, F.R. Oxidation of bilirubin produces compounds that cause prolonged vasospasm of rat cerebral vessels: A contributor to subarachnoid hemorrhage-induced vasospasm. J. Cereb. Blood Flow Metab. 2002, 22, 472–478. [Google Scholar] [CrossRef]
- Clark, J.F.; Sharp, F.R. Bilirubin oxidation products (BOXes) and their role in cerebral vasospasm after subarachnoid hemorrhage. J. Cereb. Blood Flow Metab. 2006, 26, 1223–1233. [Google Scholar] [CrossRef] [Green Version]
- Joerk, A.; Seidel, R.A.; Walter, S.G.; Wiegand, A.; Kahnes, M.; Klopfleisch, M.; Kirmse, K.; Pohnert, G.; Westerhausen, M.; Witte, O.W.; et al. Impact of heme and heme degradation products on vascular diameter in mouse visual cortex. J. Am. Heart Assoc. 2014, 3, e001220. [Google Scholar] [CrossRef]
- McGinnis, W.R.; Audhya, T.; Walsh, W.J.; Jackson, J.A.; McLaren-Howard, J.; Lewis, A.; Lauda, P.H.; Bibus, D.M.; Jurnak, F.; Lietha, R.; et al. Discerning the Mauve Factor, Part 1. Altern. Ther. Health Med. 2008, 14, 40–50. Available online: https://pubmed.ncbi.nlm.nih.gov/18383989/ (accessed on 29 January 2023).
- McGinnis, W.R.; Audhya, T.; Walsh, W.J.; Jackson, J.A.; McLaren-Howard, J.; Lewis, A.; Lauda, P.H.; Bibus, D.M.; Jurnak, F.; Lietha, R.; et al. Discerning the Mauve factor, Part 2. Altern. Health Med. 2008, 14, 56–62. Available online: https://pubmed.ncbi.nlm.nih.gov/18517107/ (accessed on 29 January 2023).
- Heitzman, J.; Gosek, P.; Lechowicz, W.; Wardenski, R.; Stepien, T. Elevated hydroxylactam of hemopyrrole level in urine in perpetrators of extremely violent acts diagnosed with psychosis. Psychiatr. Pol. 2017, 51, 413–423. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Compound Reacted with DMAB | Lambda Max (nm) |
|---|---|
2,4-dimethyl pyrrole | 540 |
3-ethyl-2,4-dimethyl pyrrole | 538 |
2,5-dimethyl pyrrole | 525 |
Urobilinogen | 2 peaks: 475 and 560 |
Bilirubin | 2 peaks: 440 and 509 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lambert, B.; Semmler, A.; Beer, C.; Voisey, J. Pyrroles as a Potential Biomarker for Oxidative Stress Disorders. Int. J. Mol. Sci. 2023, 24, 2712. https://doi.org/10.3390/ijms24032712
Lambert B, Semmler A, Beer C, Voisey J. Pyrroles as a Potential Biomarker for Oxidative Stress Disorders. International Journal of Molecular Sciences. 2023; 24(3):2712. https://doi.org/10.3390/ijms24032712
Chicago/Turabian StyleLambert, Brett, Annalese Semmler, Cristina Beer, and Joanne Voisey. 2023. "Pyrroles as a Potential Biomarker for Oxidative Stress Disorders" International Journal of Molecular Sciences 24, no. 3: 2712. https://doi.org/10.3390/ijms24032712