
Appropriateness of Proton Pump Inhibitor Prescription Evaluated by Using Serological Markers
 ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Inclusion Criteria
- -
- Age > 18 years.
- -
- Determination of gastric function using serological testing.
- -
- PPI use for at least 3 months prior to evaluation. Therapy with PPI included the following generic and brand drugs: Omeprazole (Antra®, Omeprazen®, Mepral®, and Losec®), Esomeprazole (Nexium®, Lucen®, Axagon®, and Esopral®, Pantoprazole (Pantorc®, Pantopan®, Pantecta®, Peptazol®), Rabeprazole (Pariet®), and Lansoprazole (Zoton®, Limpidex®, and Lansox®).
- -
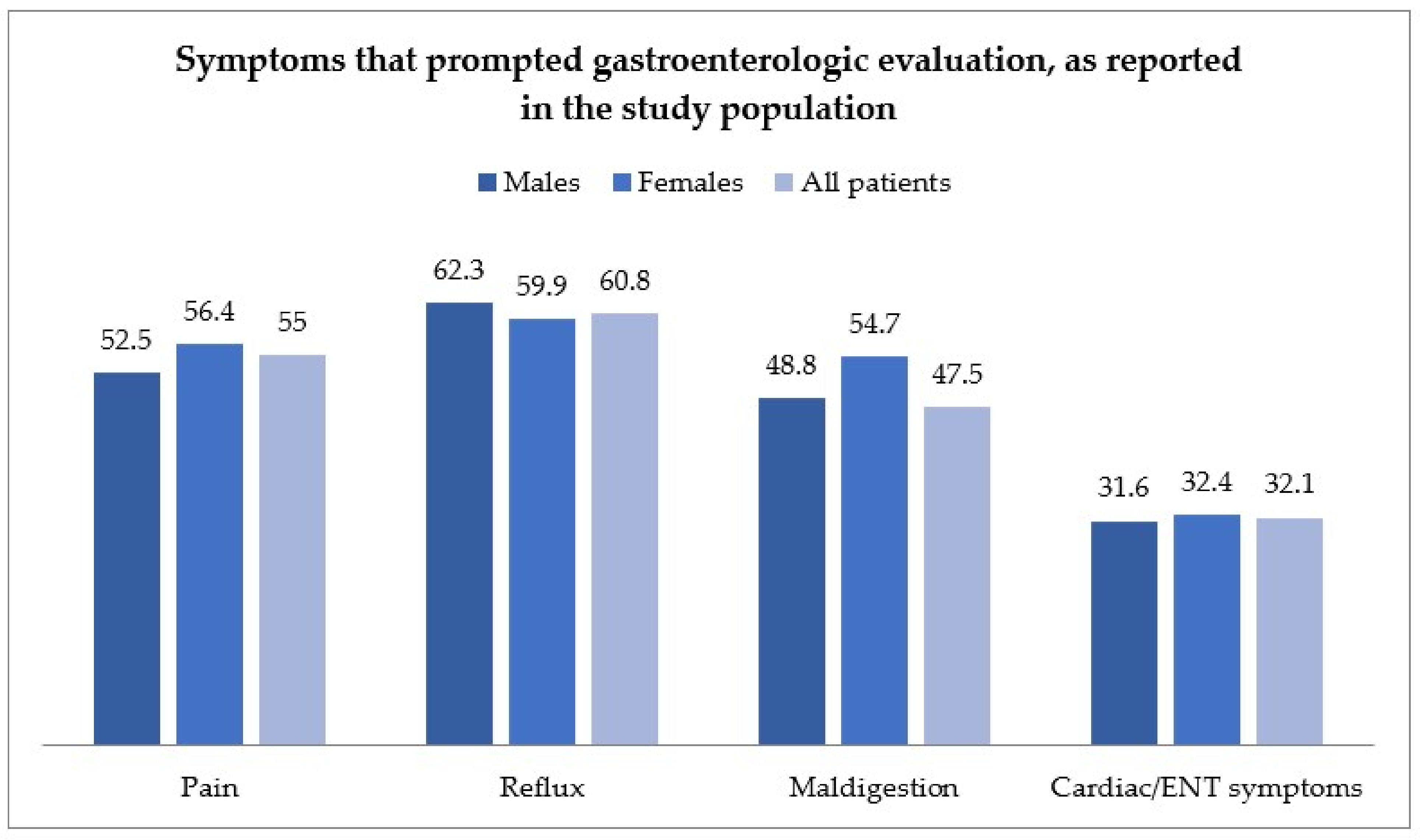
- The presence of symptoms attributed to gastroesophageal acid-related disease, for which patients were on PPI therapy; symptoms were assigned to the following categories: pain symptoms (including epigastric and abdominal pain); reflux symptoms (including heartburn, acid regurgitation, persistent hiccup, belching, sialorrhea, and globus pharynges); maldigestion symptoms (including nausea, bloating, flatulence, rumbling abdomen, bitter taste in the mouth, and aerophagia); otorhinolaryngological symptoms (including hoarseness, chronic laryngitis, coughing, glossitis, and pharyngitis); and chest/cardiac symptoms (including thoracic pain, tachycardia, extrasystoles, and dyspnea).
4.2. Exclusion Criteria
- -
- Alarm symptoms or signs as an indication for upper endoscopic and/or gastric functional evaluation, such as weight loss, anemia, presence of bright red blood per rectum, coffee-ground stools, ematochezia, dysphagia, persistent vomiting or vomiting of coffee-ground material or hematemesis, and persistent diarrhea.
- -
- History of Zollinger-Ellison syndrome.
- -
- Pyloric stenosis.
- -
- Previous surgery of the esophagus and/or gastrointestinal tract (except for appendectomy and cholecystectomy).
- -
- Malignant gastrointestinal tumors.
- -
- Therapy with H2-blockers.
4.3. Serological Evaluation of Gastric Function
4.4. Endoscopic and Histological Evaluation
4.5. PPI Therapy Therapeutic Response
4.6. Statistical Analysis
4.7. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CAG | chronic atrophic gastritis |
| PG-I | Pepsinogen I |
| PG-II | Pepsinogen II |
| G17 | gastrin 17 |
| HP | Helicobacter pylori |
| NSAIDs | Non-Steroidal Anti-inflammatory Drugs |
| PPIs | proton pump inhibitors |
| µg | micrograms |
| pmol | picomoles |
| U/L | Unit/liter |
References
- Veysey-Smith, R.; Moore, A.R.; Murugesan, S.V.; Tiszlavicz, L.; Dockray, G.J.; Varro, A.; Pritchard, D.M. Effects of Proton Pump Inhibitor Therapy, H. pylori Infection and Gastric Preneoplastic Pathology on Fasting Serum gastrin Concentrations. Front. Endocrinol. 2021, 12, 741887. [Google Scholar] [CrossRef]
- Shaheen, N.J.; Hansen, R.A.; Morgan, D.R.; Gangarosa, L.M.; Ringel, Y.; Thiny, M.T.; Russo, M.W.; Sandler, R.S. The Burden of Gastrointestinal and Liver Diseases, 2006. Am. J. Gastroenterol. 2006, 101, 2128–2138. [Google Scholar] [CrossRef] [PubMed]
- Heidelbaugh, J.J.; Kim, A.H.; Chang, R.; Walker, P.C. Overutilization of proton pump inhibitors: What the clinician needs to know. Ther. Adv. Gastroenterol. 2012, 5, 219–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inadomi, J.M.; McIntyre, L.; Bernard, L.; Fendrick, A.M. Step-down from multiple- to single-dose proton pump inhibitors (PPIs): A prospective study of patients with heartburn or acid regurgitation completely relieved with PPIs. Am. J. Gastroenterol. 2003, 98, 1940–1944. [Google Scholar] [CrossRef] [PubMed]
- Inadomi, J.M.; Jamal, R.; Murata, G.H.; Hoffman, R.M.; Lavezo, L.A.; Vigil, J.M.; Swanson, K.M.; Sonnenberg, A. Step-down management of gastroesophageal reflux disease. Gastroenterology 2001, 121, 1095–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, P.O.; Gerson, L.B.; Vela, M.F. Guidelines for the Diagnosis and Management of Gastroesophageal Reflux Disease. Off. J. Am. Coll. Gastroenterol. ACG 2013, 108, 308–328. [Google Scholar] [CrossRef]
- Schwartz, S.R.; Cohen, S.M.; Dailey, S.H.; Rosenfeld, R.M.; Deutsch, E.S.; Gillespie, M.B.; Granieri, E.; Hapner, E.R.; Kimball, C.E.; Krouse, H.J.; et al. Clinical Practice Guideline: Hoarseness (Dysphonia). Otolaryngol. Head Neck Surg. 2009, 141 (Suppl. 1), 1–31. [Google Scholar] [CrossRef]
- Bruno, C.; Pearson, S.A.; Daniels, B.; Buckley, N.A.; Schaffer, A.; Zoega, H. Passing the acid test? Evaluating the impact of national education initiatives to reduce proton pump inhibitor use in Australia. BMJ Qual Saf. 2020, 29, 365–373. [Google Scholar] [CrossRef]
- Scarpignato, C.; Gatta, L.; Zullo, A.; Blandizzi, C.; Zullo, A.; Kohn, A.; Leandro, G.; Balzano, A.; Chiriatti, A.; Marocco, W.; et al. Effective and safe proton pump inhibitor therapy in acid-related diseases—A position paper addressing benefits and potential harms of acid suppression. BMC Med. 2016, 14, 179. [Google Scholar] [CrossRef]
- Lahner, E.; Annibale, B.; Fave, G.D. Systematic review: Impaired drug absorption related to the co-administration of antisecretory therapy. Aliment. Pharmacol. Ther. 2009, 29, 1219–1229. [Google Scholar] [CrossRef]
- Bavishi, C.; DuPont, H.L. Systematic review: The use of proton pump inhibitors and increased susceptibility to enteric infection. Aliment. Pharmacol. Ther. 2011, 34, 1269–1281. [Google Scholar] [CrossRef]
- Zacharioudakis, I.M.; Zervou, F.N.; Pliakos, E.E.; Ziakas, P.D.; Mylonakis, E. Colonization With Toxinogenic C. difficile Upon Hospital Admission, and Risk of Infection: A Systematic Review and Meta-Analysis. Off. J. Am. Coll. Gastroenterol. ACG 2015, 110, 381–390. [Google Scholar] [CrossRef]
- Tleyjeh, I.M.; Abdulhak, A.A.B.; Riaz, M.; Alasmari, F.A.; Garbati, M.A.; AlGhamdi, M.; Khan, A.R.; Tannir, M.A.; Erwin, P.J.; Ibrahim, T.; et al. Association between Proton Pump Inhibitor Therapy and Clostridium difficile Infection: A Contemporary Systematic Review and Meta-Analysis. PLoS ONE 2012, 7, e50836. [Google Scholar] [CrossRef] [Green Version]
- Agréus, L.; Kuipers, E.J.; Kupcinskas, L.; Malfertheiner, P.; Di Mario, F.; Leja, M.; Mahachai, V.; Yaron, N.; van Oijen, M.; Perez, G.P.; et al. Rationale in diagnosis and screening of atrophic gastritis with stomach-specific plasma biomarkers. Scand. J. Gastroenterol. 2012, 47, 136–147. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of helicobacter pylori infection-the Maastricht V/Florence consensus report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Germaná, B.; Di Mario, F.; Cavallaro, L.G.; Moussa, A.M.; Lecis, P.; Liatoupolou, S.; Comparato, G.; Carloni, C.; Bertiato, G.; Battiestel, M.; et al. Clinical usefulness of serum pepsinogens I and II, gastrin-17 and anti-Helicobacterpylori antibodies in the management of dyspeptic patients in primary care. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2005, 37, 501–508. [Google Scholar] [CrossRef]
- Bornschein, J.; Selgrad, M.; Wex, T.; Kuester, D.; Malfertheiner, P. Serological assessment of gastric mucosal atrophy in gastric cancer. BMC Gastroenterol. 2012, 12, 10. [Google Scholar] [CrossRef] [Green Version]
- Väänänen, H.; Vauhkonen, M.; Helske, T.; Kääriäinen, I.; Rasmussen, M.; Tunturi-Hihnala, H.; Koskenpato, J.; Sotka, M.; Turunen, M.; Sandström, R.; et al. Non-endoscopic diagnosis of atrophic gastritis with a blood test. Correlation between gastric histology and serum levels of gastrin-17 and pepsinogen I: A multicentre study. Eur. J. Gastroenterol. Hepatol. 2003, 15, 885–891. [Google Scholar] [CrossRef]
- Samloff, I.M.; Varis, K.; Ihamaki, T.; Siurala, M.; Rotter, J.I. Relationships Among Serum Pepsinogen I, Serum Pepsinogen II, and Gastric Mucosal Histology: A Study in Relatives of Patients with Pernicious Anemia. Gastroenterology 1982, 83, 204–209. [Google Scholar] [CrossRef]
- Ren, J.-S.; Kamangar, F.; Qiao, Y.-L.; Taylor, P.R.; Liang, H.; Dawsey, S.M.; Liu, B.; Fan, J.-H.; Abnet, C.C. Serum pepsinogens and risk of gastric and oesophageal cancers in the General Population Nutrition Intervention Trial cohort. Gut 2009, 58, 636–642. [Google Scholar] [CrossRef]
- Korstanje, A.; den Hartog, G.; Biemond, I.; Lamers, C.B.H.W. The Serological Gastric Biopsy: A Non-Endoscopical Diagnostic Approach in Management of the Dyspeptic Patient Significance for Primary Care Based on a Survey of the Literature. Scand. J. Gastroenterol. 2002, 37, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Oksanen, A.; Sipponen, P.; Miettinen, A.; Sarna, S.; Rautelin, H. Evaluation of blood tests to predict normal gastric mucosa. Scand. J. Gastroenterol. 2000, 35, 791–795. [Google Scholar] [CrossRef] [PubMed]
- Lundell, L.; Vieth, M.; Gibson, F.; Nagy, P.; Kahrilas, P.J. Systematic review: The effects of long-term proton pump inhibitor use on serum gastrin levels and gastric histology. Aliment. Pharmacol. Ther. 2015, 42, 649–663. [Google Scholar] [CrossRef] [PubMed]
- Raines, D.; Chester, M.; Diebold, A.E.; Mamikunian, P.; Anthony, C.T.; Mamikunian, G.; Woltering, E.A. A Prospective Evaluation of the Effect of Chronic Proton Pump Inhibitor Use on Plasma Biomarker Levels in Humans. Pancreas 2012, 41, 508. [Google Scholar] [CrossRef] [Green Version]
- Sipponen, P.; Valle, J.; Varis, K.; Kekki, M.; Ihamäki, T.; Siurala, M. Fasting Levels of Serum Gastrin in Different Functional and Morphologic States of the Antrofundal Mucosa: An Analysis of 860 Subjects. Scand. J. Gastroenterol. 1990, 255, 513–519. [Google Scholar] [CrossRef]
- Di Mario, F.; Cavallaro, L.G.; Moussa, A.M.; Caruana, P.; Merli, R.; Maini, A.; Bertolini, S.; Dal Bó, N.; Rugge, M.; Cavestro, G.M.; et al. Usefulness of Serum Pepsinogens in Helicobacter pylori Chronic Gastritis: Relationship With Inflammation, Activity, and Density of the Bacterium. Dig. Dis. Sci. 2006, 51, 1791–1795. [Google Scholar] [CrossRef]
- Kekki, M.; Samloff, I.M.; Varis, K.; Ihamäki, T. Serum Pepsinogen I and Serum gastrin in the Screening of Severe Atrophic Corpus Gastritis. Scand. J. Gastroenterol. 1991, 26 (Suppl. 186), 109–116. [Google Scholar] [CrossRef]
- Tosetti, C.; Nanni, I. Use of proton pump inhibitors in general practice. World J. Gastrointest. Pharmacol. Ther. 2017, 8, 180–185. [Google Scholar] [CrossRef]
- Lassalle, M.; Le Tri, T.; Bardou, M.; Biour, M.; Kirchgesner, J.; Rouby, F.; Dumarcet, N.; Zureik, M.; Dray-Spira, R. Use of proton pump inhibitors in adults in France: A nationwide drug utilization study. Eur. J. Clin. Pharmacol. 2020, 76, 449–457. [Google Scholar] [CrossRef] [Green Version]
- Mishuk, A.U.; Chen, L.; Gaillard, P.; Westrick, S.; Hansen, R.A.; Qian, J. National trends in prescription proton pump inhibitor use and expenditure in the United States in 2002–2017. J. Am. Pharm. Assoc. 2021, 61, 87–94.e7. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans Biological Agents. Volume 100 B. A review of human carcinogens. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100, 1–441. [Google Scholar]
- Watabe, H.; Mitsushima, T.; Yamaji, Y.; Okamoto, M.; Wada, R.; Kokubo, T.; Doi, H.; Yoshida, H.; Kawabe, T.; Omata, M. Predicting the development of gastric cancer from combining Helicobacter pylori antibodies and serum pepsinogen status: A prospective endoscopic cohort study. Gut 2005, 54, 764–768. [Google Scholar] [CrossRef] [Green Version]
- Asaka, M.; Kimura, T.; Kudo, M.; Takeda, H.; Mitani, S.; Miyazaki, T.; Miki, K.; Graham, D.Y. Relationship of Helicobacter pylori to serum pepsinogens in an asymptomatic Japanese population. Gastroenterology 1992, 102, 760–766. [Google Scholar] [CrossRef]
- Robinson, M. Review article: The pharmacodynamics and pharmacokinetics of proton pump inhibitors--overview and clinical implications. Aliment. Pharmacol. Ther. 2004, 20 (Suppl. 6), 1–10. [Google Scholar] [CrossRef]
- Graham, D.Y.; Tansel, A. Interchangeable Use of Proton Pump Inhibitors Based on Relative Potency. Clin. Gastroenterol. Hepatol. 2018, 16, 800–808. [Google Scholar] [CrossRef]
- Ottenm, M.H.; Lekkerkerker, J.F.F.F.; Mulder, C.J.J. [Why some proton pump inhibitors are more equal than others]. Ned. Tijdschr. Geneeskd. 2009, 153, B414. [Google Scholar]
- Hussain, Z.H.; Henderson, E.E.; Maradey-Romerao, C.; George, N.; Fass, R.; Lacy, B.E. The Proton Pump Inhibitor Non-Responder: A Clinical Conundrum. Clin. Transl. Gastroenterol. 2015, 6, e106. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Males | Females | p | Total | |
|---|---|---|---|---|
| Patients (n, %) | 377 (37.1) | 638 (62.9) | 1015 (100) | |
| Mean age ±SD (years) | 45.0 ± 14.8 | 47.9 ± 15.7 | 0.003 | 46.8 ± 15.4 |
| Range age (years) | 18–84 | 18–95 | 18–95 | |
| Body mass index (kg/m2) | 24.9 ± 3.6 | 23.9 ± 4.7 | 0.004 | 24.3 ± 4.4 |
| Cigarette smoking (%) | 18.6 | 17.9 | 0.061 | 18.2 |
| Daily alcohol intake (%) | 64.3 | 37.7 | 0.0001 | 47.5 |
| Autoimmune thyroiditis (%) | 3.4 | 19.3 | 0.0001 | 13.4 |
| HP eradication (%) | 15.6 | 23.2 | 0.002 | 20.4 |
| Gastric cancer familiarity (%) | 10.1 | 10.8 | 0.454 | 10.5 |
| NSAIDs use (%) | 15.4 | 21.8 | 0.007 | 19.4 |
| Aspirin use (%) | 8.8 | 6.6 | 0.125 | 7.4 |
| PPI Therapy Dosing | ||||
|---|---|---|---|---|
| N. 1015 | Half 294 | Full 709 | High 12 | |
| Adequate response G17 >7, n., % | 354 (34.9) | 85 (28.9) | 261 (36.8) | 8 (66.7) |
| Low response G17 1-7, n., % | 417 (41.1) | 139 (47.3) | 277 (39.1) | 1 (8.3) |
| No response G17 < 1, n., % | 207 (20.4) | 65 (22.1) | 141 (19.9) | 1 (8.3) |
| CAG, n., % | 37 (3.6) | 5 (1.7) | 30 (4.2) | 2 (16.7) |
| Gastric Functional Status | ||||
|---|---|---|---|---|
| PG-I (μg/L) Mean ± DS | G-17 (pmol/L) Mean ± DS | PG-II (pmol/L) Mean ± DS | PGI/PGII Ratio | |
| Total | 139.1 ± 97.3 | 11.7 ± 21.1 | 12.8 ± 10.7 | 12.4 ± 5.1 |
| Adequate response G-17 > 7 | 193.9 ± 120.8 | 21.8 ± 17.5 | 18.2 ± 13.6 | 12.6 ± 5.5 |
| Low response G-17 1-7 | 127.1 ± 68.5 | 3.1 ± 1.73 | 11.1 ± 8.5 | 12.9 ± 4.6 |
| No response G-17 < 1 | 91.2 ± 40.9 | 0.38 ± 0.29 | 7.52 ± 3.8 | 12.9 ± 3.9 |
| CAG | 17.0 ± 16.7 | 73.7 ± 54.2 | 8.6 ± 4.4 | 1.95 ± 1.8 |
| Therapeutic Response to PPIs | |||
|---|---|---|---|
| OR | (95% CI) | p | |
| Older Age (>60 years) | 1.419 | (1.070–1.882) | 0.002 |
| Gender (F) | 1.015 | (1.006–1.025) | 0.015 |
| Previous HP eradication | 0.896 | (0.628–1.276) | 0.541 |
| Active HP infection | 1.578 | (1.135–2.194) | 0.007 |
| Branded PPIs | 1.407 | (1.067–1.855) | 0.0015 |
| Full Dosage PPIs | 1.712 | (1.276–2.298) | 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, M.; Rodriguez-Castro, K.I.; Franceschi, M.; Ferronato, A.; Panozzo, M.P.; Brozzi, L.; Di Mario, F.; Crafa, P.; Brandimarte, G.; Tursi, A. Appropriateness of Proton Pump Inhibitor Prescription Evaluated by Using Serological Markers. Int. J. Mol. Sci. 2023, 24, 2378. https://doi.org/10.3390/ijms24032378
Russo M, Rodriguez-Castro KI, Franceschi M, Ferronato A, Panozzo MP, Brozzi L, Di Mario F, Crafa P, Brandimarte G, Tursi A. Appropriateness of Proton Pump Inhibitor Prescription Evaluated by Using Serological Markers. International Journal of Molecular Sciences. 2023; 24(3):2378. https://doi.org/10.3390/ijms24032378
Chicago/Turabian StyleRusso, Michele, Kryssia Isabel Rodriguez-Castro, Marilisa Franceschi, Antonio Ferronato, Maria Piera Panozzo, Lorenzo Brozzi, Francesco Di Mario, Pellegrino Crafa, Giovanni Brandimarte, and Antonio Tursi. 2023. "Appropriateness of Proton Pump Inhibitor Prescription Evaluated by Using Serological Markers" International Journal of Molecular Sciences 24, no. 3: 2378. https://doi.org/10.3390/ijms24032378