
Prognostic Value of Galectin-3 after Left Atrial Appendage Occlusion for Predicting Peri-Device Leakage
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patient Cohort
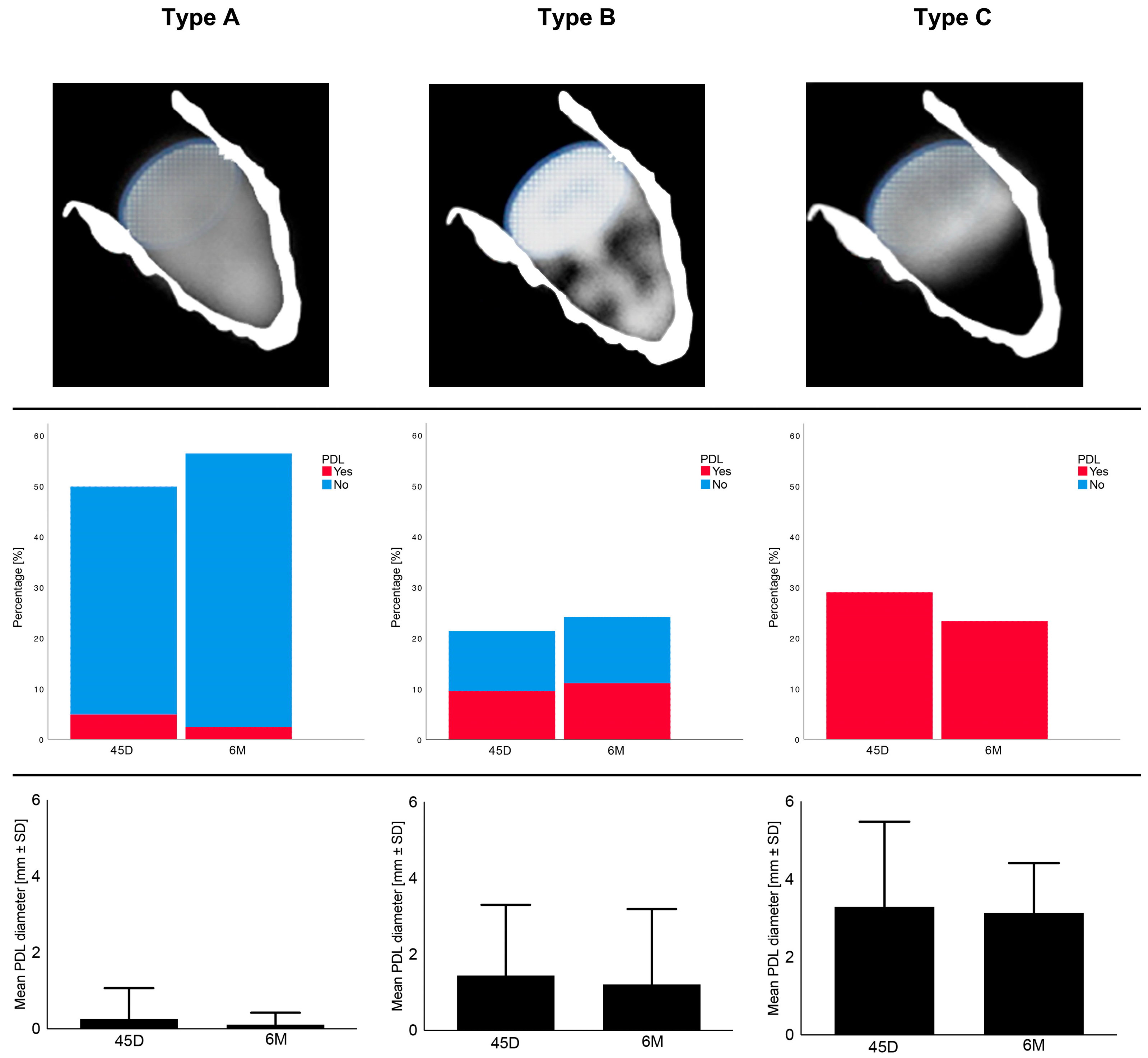
2.2. Echocardiographic Morphology after LAAO
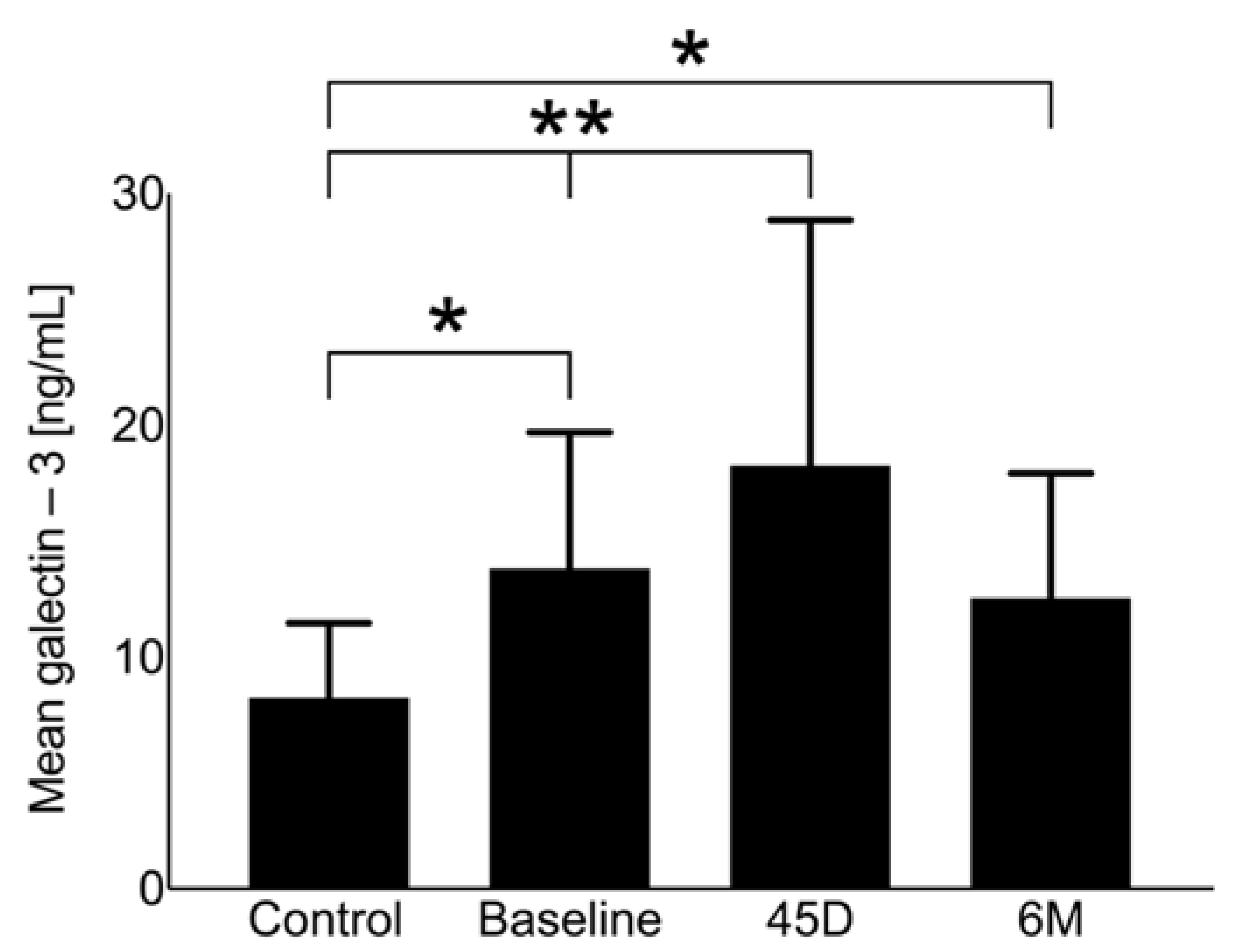
2.3. Dynamics of Galectin-3
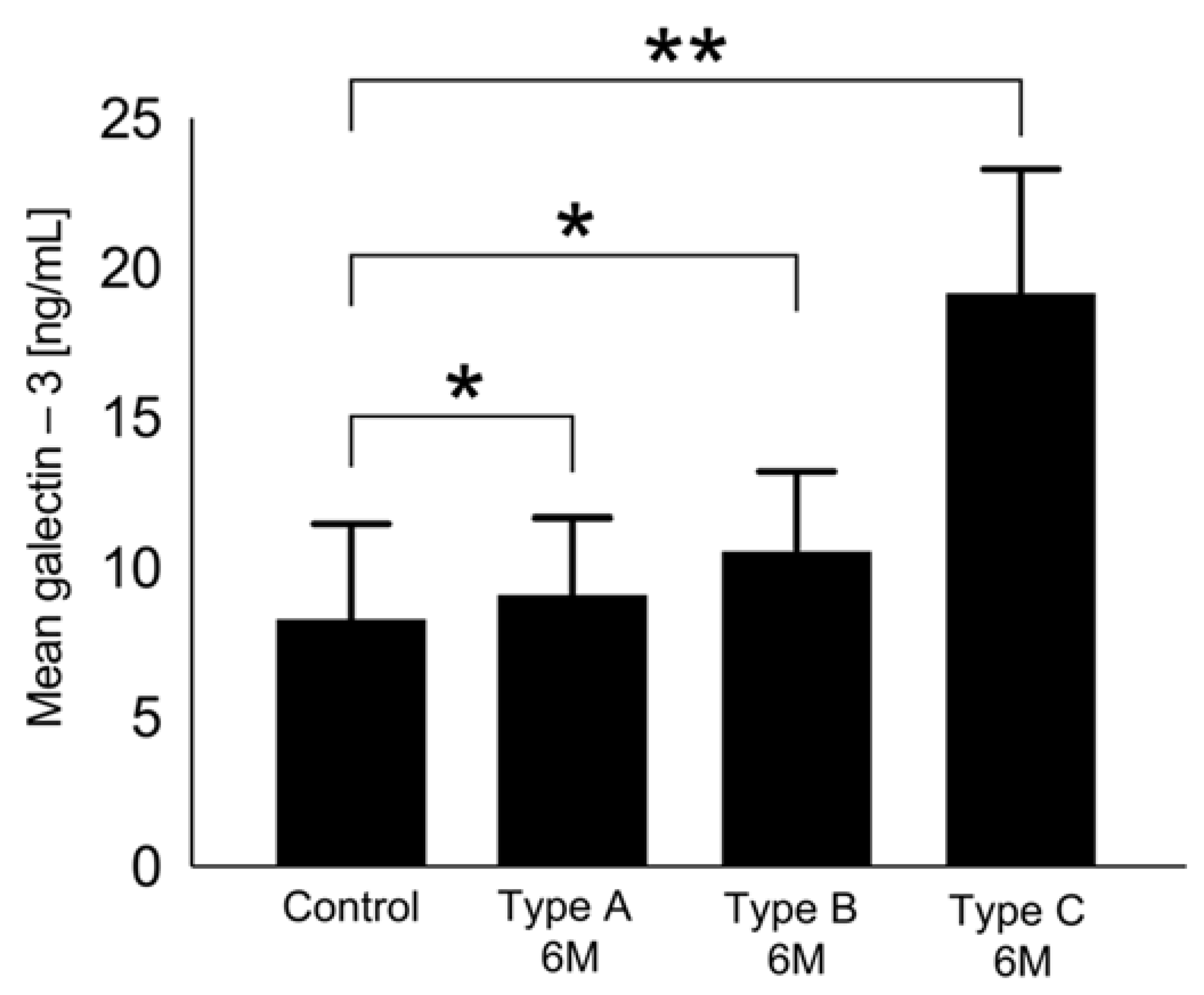
2.4. Association of Galectin-3 with Echocardiographic Morphology
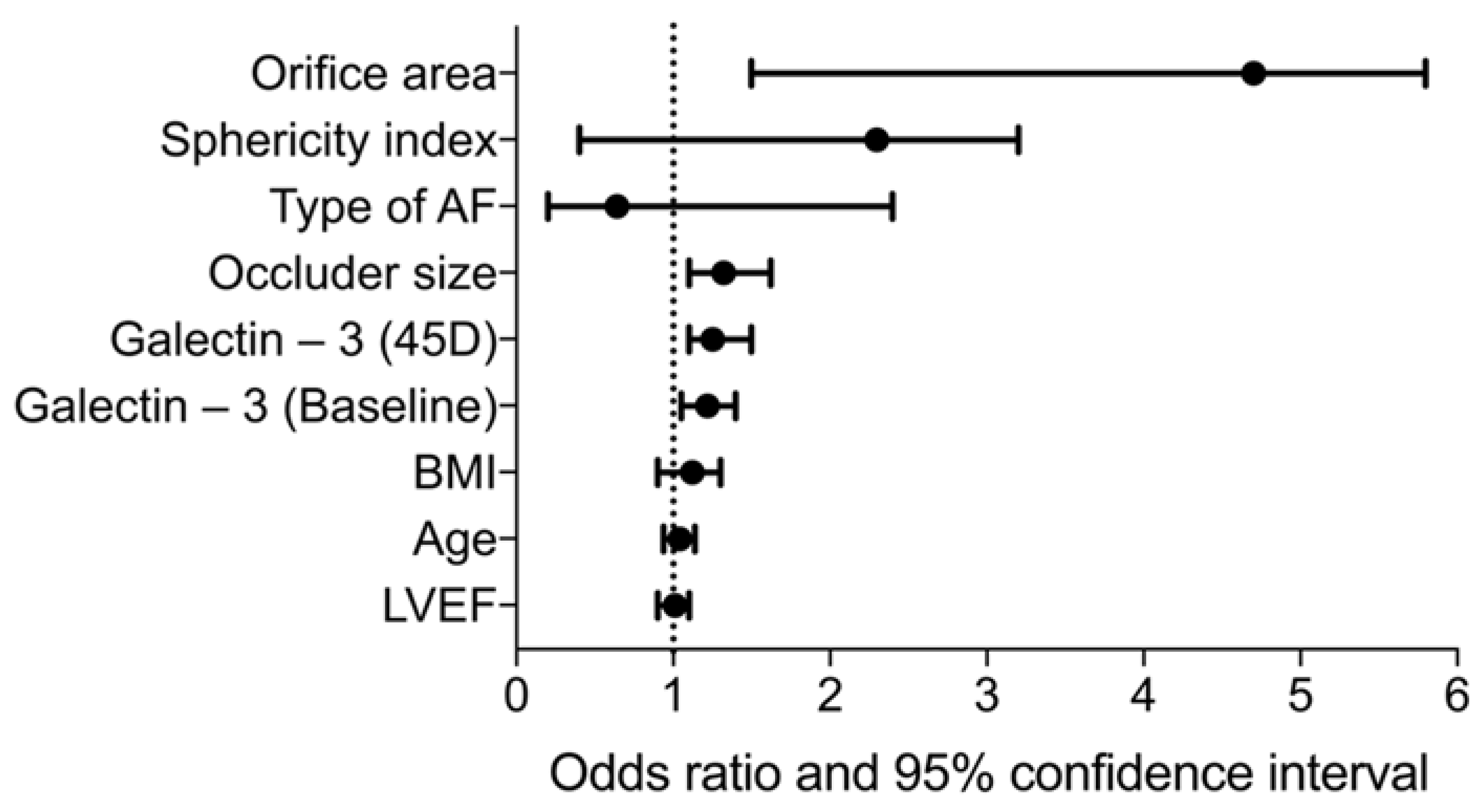
2.5. Prognostic Value of Galectin-3 for Type C
2.6. Cut-Off Values for Galectin-3 Predicting Type C
3. Discussion
Clinical Application of Galectin-3 for Detection of Unsuccessful LAAO
4. Materials and Methods
4.1. Patients
4.2. LAAO Procedure and Peri-Device Leak Assessment
4.3. Transesophageal Echocardiography (TEE)
4.4. Serum Quantification of Galectin-3 Using ELISA Technique
4.5. Control Group
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamberts, M.; Staerk, L.; Olesen, J.B.; Fosbol, E.L.; Hansen, M.L.; Harboe, L.; Lefevre, C.; Evans, D.; Gislason, G.H. Major Bleeding Complications and Persistence With Oral Anticoagulation in Non-Valvular Atrial Fibrillation: Contemporary Findings in Real-Life Danish Patients. J. Am. Heart Assoc. 2017, 6, e004517. [Google Scholar] [CrossRef] [PubMed]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Accetta, G.; Ambrosio, G.; Atar, D.; Bassand, J.P.; Berge, E.; Cools, F.; Fitzmaurice, D.A.; Goldhaber, S.Z.; Goto, S.; et al. Evolving antithrombotic treatment patterns for patients with newly diagnosed atrial fibrillation. Heart 2017, 103, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.R., Jr.; Kar, S.; Price, M.J.; Whisenant, B.; Sievert, H.; Doshi, S.K.; Huber, K.; Reddy, V.Y. Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: The PREVAIL trial. J. Am. Coll. Cardiol. 2014, 64, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Nieuwlaat, R.; Capucci, A.; Camm, A.J.; Olsson, S.B.; Andresen, D.; Davies, D.W.; Cobbe, S.; Breithardt, G.; Le Heuzey, J.Y.; Prins, M.H.; et al. Atrial fibrillation management: A prospective survey in ESC member countries: The Euro Heart Survey on Atrial Fibrillation. Eur. Heart J. 2005, 26, 2422–2434. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.P.; Park, P.; Lakkireddy, D. Left Atrial Appendages Occlusion: Current Status and Prospective. Korean Circ. J. 2018, 48, 692–704. [Google Scholar] [CrossRef] [PubMed]
- Lakkireddy, D.; Thaler, D.; Ellis, C.R.; Swarup, V.; Sondergaard, L.; Carroll, J.; Gold, M.R.; Hermiller, J.; Diener, H.C.; Schmidt, B.; et al. Amplatzer Amulet Left Atrial Appendage Occluder Versus Watchman Device for Stroke Prophylaxis (Amulet IDE): A Randomized, Controlled Trial. Circulation 2021, 144, 1543–1552. [Google Scholar] [CrossRef]
- Holmes, D.R.; Reddy, V.Y.; Turi, Z.G.; Doshi, S.K.; Sievert, H.; Buchbinder, M.; Mullin, C.M.; Sick, P. Investigators, Protect Af Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: A randomised non-inferiority trial. Lancet 2009, 374, 534–542. [Google Scholar] [CrossRef]
- Bai, R.; Horton, R.P.; Di Biase, L.; Mohanty, P.; Pump, A.; Cardinal, D.; Scallon, C.; Mohanty, S.; Santangeli, P.; Brantes, M.C.; et al. Intraprocedural and long-term incomplete occlusion of the left atrial appendage following placement of the WATCHMAN device: A single center experience. J. Cardiovasc. Electrophysiol. 2012, 23, 455–461. [Google Scholar] [CrossRef]
- Jaguszewski, M.; Manes, C.; Puippe, G.; Salzberg, S.; Muller, M.; Falk, V.; Luscher, T.; Luft, A.; Alkadhi, H.; Landmesser, U. Cardiac CT and echocardiographic evaluation of peri-device flow after percutaneous left atrial appendage closure using the AMPLATZER cardiac plug device. Catheter. Cardiovasc. Interv. 2015, 85, 306–312. [Google Scholar] [CrossRef]
- Raphael, C.E.; Friedman, P.A.; Saw, J.; Pislaru, S.V.; Munger, T.M.; Holmes, D.R., Jr. Residual leaks following percutaneous left atrial appendage occlusion: Assessment and management implications. EuroIntervention 2017, 13, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Viles-Gonzalez, J.F.; Kar, S.; Douglas, P.; Dukkipati, S.; Feldman, T.; Horton, R.; Holmes, D.; Reddy, V.Y. The clinical impact of incomplete left atrial appendage closure with the Watchman Device in patients with atrial fibrillation: A PROTECT AF (Percutaneous Closure of the Left Atrial Appendage Versus Warfarin Therapy for Prevention of Stroke in Patients With Atrial Fibrillation) substudy. J. Am. Coll. Cardiol. 2012, 59, 923–929. [Google Scholar] [PubMed]
- Mugge, A.; Kuhn, H.; Nikutta, P.; Grote, J.; Lopez, J.A.; Daniel, W.G. Assessment of left atrial appendage function by biplane transesophageal echocardiography in patients with nonrheumatic atrial fibrillation: Identification of a subgroup of patients at increased embolic risk. J. Am. Coll. Cardiol. 1994, 23, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Pollick, C.; Taylor, D. Assessment of left atrial appendage function by transesophageal echocardiography. Implications for the development of thrombus. Circulation 1991, 84, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Alkhouli, M.; Du, C.; Killu, A.; Simard, T.; Noseworthy, P.A.; Friedman, P.A.; Curtis, J.P.; Freeman, J.V.; Holmes, D.R. Clinical Impact of Residual Leaks Following Left Atrial Appendage Occlusion: Insights From the NCDR LAAO Registry. JACC Clin. Electrophysiol. 2022, 8, 766–778. [Google Scholar] [CrossRef]
- Gianni, C.; Di Biase, L.; Trivedi, C.; Mohanty, S.; Gokoglan, Y.; Gunes, M.F.; Bai, R.; Al-Ahmad, A.; Burkhardt, J.D.; Horton, R.P.; et al. Clinical Implications of Leaks Following Left Atrial Appendage Ligation With the LARIAT Device. JACC Cardiovasc. Interv. 2016, 9, 1051–1057. [Google Scholar] [CrossRef]
- Hamadanchi, A.; Ijuin, S.; Haertel, F.; Bekfani, T.; Westphal, J.; Franz, M.; Moebius-Winkler, S.; Schulze, P.C. A Novel Echocardiographic-Based Classification for the Prediction of Peri-Device Leakage following Left Atrial Appendage Occluder Implantation. J. Clin. Med. 2022, 11, 1059. [Google Scholar] [CrossRef]
- Sygitowicz, G.; Maciejak-Jastrzebska, A.; Sitkiewicz, D. The Diagnostic and Therapeutic Potential of Galectin-3 in Cardiovascular Diseases. Biomolecules 2021, 12, 46. [Google Scholar] [CrossRef]
- Cha, J.H.; Wee, H.J.; Seo, J.H.; Ahn, B.J.; Park, J.H.; Yang, J.M.; Lee, S.W.; Kim, E.H.; Lee, O.H.; Heo, J.H.; et al. AKAP12 mediates barrier functions of fibrotic scars during CNS repair. PLoS ONE 2014, 9, e94695. [Google Scholar] [CrossRef]
- Sharma, U.C.; Pokharel, S.; Van Brakel, T.J.; Van Berlo, J.H.; Cleutjens, J.P.; Schroen, B.; Andre, S.; Crijns, H.J.; Gabius, H.J.; Maessen, J.; et al. Galectin-3 marks activated macrophages in failure-prone hypertrophied hearts and contributes to cardiac dysfunction. Circulation 2004, 110, 3121–3128. [Google Scholar] [CrossRef]
- Sonmez, O.; Ertem, F.U.; Vatankulu, M.A.; Erdogan, E.; Tasal, A.; Kucukbuzcu, S.; Goktekin, O. Novel fibro-inflammation markers in assessing left atrial remodeling in non-valvular atrial fibrillation. Med. Sci. Monit. 2014, 20, 463–470. [Google Scholar] [PubMed]
- Tang, Z.; Zeng, L.; Lin, Y.; Han, Z.; Gu, J.; Wang, C.; Zhang, H. Circulating Galectin-3 is Associated With Left Atrial Appendage Remodelling and Thrombus Formation in Patients With Atrial Fibrillation. Heart Lung Circ. 2019, 28, 923–931. [Google Scholar] [CrossRef]
- Herman, D.; Osmancik, P.; Neuzil, P.; Hala, P.; Lekesova, V.; Benesova, K.; Hozman, M.; Jarkovsky, J.; Novackova, M.; Widimsky, P.; et al. The effect of left atrial appendage closure on heart failure biomarkers: A PRAGUE-17 trial subanalysis. J. Cardiovasc. Electrophysiol. 2021, 32, 2645–2654. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.M. Multinucleated giant cells. Curr. Opin. Hematol. 2000, 7, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Gretzer, C.; Emanuelsson, L.; Liljensten, E.; Thomsen, P. The inflammatory cell influx and cytokines changes during transition from acute inflammation to fibrous repair around implanted materials. J. Biomater. Sci. Polym. Ed. 2006, 17, 669–687. [Google Scholar] [CrossRef] [PubMed]
- Luttikhuizen, D.T.; Harmsen, M.C.; Van Luyn, M.J. Cellular and molecular dynamics in the foreign body reaction. Tissue Eng. 2006, 12, 1955–1970. [Google Scholar] [CrossRef]
- Sieweke, J.T.; Pfeffer, T.J.; Biber, S.; Chatterjee, S.; Weissenborn, K.; Grosse, G.M.; Hagemus, J.; Derda, A.A.; Berliner, D.; Lichtinghagen, R.; et al. miR-21 and NT-proBNP Correlate with Echocardiographic Parameters of Atrial Dysfunction and Predict Atrial Fibrillation. J. Clin. Med. 2020, 9, 1118. [Google Scholar] [CrossRef]
- Chandorkar, Y.; Ravikumar, K.; Basu, B. The Foreign Body Response Demystified. ACS Biomater. Sci. Eng. 2019, 5, 19–44. [Google Scholar] [CrossRef]
- De Boer, R.A.; Yu, L.; Van Veldhuisen, D.J. Galectin-3 in cardiac remodeling and heart failure. Curr. Heart Fail. Rep. 2010, 7, 1–8. [Google Scholar] [CrossRef]
- Baldenhofer, G.; Zhang, K.; Spethmann, S.; Laule, M.; Eilers, B.; Leonhardt, F.; Sanad, W.; Dreger, H.; Sander, M.; Grubitzsch, H.; et al. Galectin-3 predicts short- and long-term outcome in patients undergoing transcatheter aortic valve implantation (TAVI). Int. J. Cardiol. 2014, 177, 912–917. [Google Scholar] [CrossRef]
- Xu, J.; Gong, X.; Chen, C.; Xing, J.; Wang, Q.; Shen, W.; Zhang, Q. Reduced plasma level of basic fibroblast growth factor is associated with incomplete device endothelialization at six months following left atrial appendage closure. BMC Cardiovasc. Disord. 2021, 21, 242. [Google Scholar] [CrossRef] [PubMed]
- Gehlken, C.; Suthahar, N.; Meijers, W.C.; De Boer, R.A. Galectin-3 in Heart Failure: An Update of the Last 3 Years. Heart Fail. Clin. 2018, 14, 75–92. [Google Scholar] [CrossRef] [PubMed]
- Pilette, C.; Colinet, B.; Kiss, R.; Andre, S.; Kaltner, H.; Gabius, H.J.; Delos, M.; Vaerman, J.P.; Decramer, M.; Sibille, Y. Increased galectin-3 expression and intra-epithelial neutrophils in small airways in severe COPD. Eur. Respir. J. 2007, 29, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Kuo, P.L. The Role of Galectin-3 in the Kidneys. Int. J. Mol. Sci. 2016, 17, 565. [Google Scholar] [CrossRef]
- Lindner, S.; Behnes, M.; Wenke, A.; Sartorius, B.; Ansari, U.; Akin, M.; Mashayekhi, K.; Vogler, N.; Haubenreisser, H.; Schoenberg, S.O.; et al. Assessment of peri-device leaks after interventional left atrial appendage closure using standardized imaging by cardiac computed tomography angiography. Int. J. Cardiovasc. Imaging 2019, 35, 725–731. [Google Scholar] [CrossRef]
- Schols, A.M.R.; Stakenborg, J.P.G.; Dinant, G.J.; Willemsen, R.T.A.; Cals, J.W.L. Point-of-care testing in primary care patients with acute cardiopulmonary symptoms: A systematic review. Fam. Pract. 2018, 35, 4–12. [Google Scholar] [CrossRef]
- Goebel, B.; Wieg, S.; Hamadanchi, A.; Otto, S.; Jung, C.; Kretzschmar, D.; Figulla, H.R.; Christian Schulze, P.; Poerner, T.C. Interventional left atrial appendage occlusion: Added value of 3D transesophageal echocardiography for device sizing. Int. J. Cardiovasc. Imaging 2016, 32, 1363–1370. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Population | |
|---|---|
| (n = 47) | |
| Demographics | |
| Age [years—mean ± SD] | 73.9 ± 7.1 |
| >75 years [n (%)] | 23 (49) |
| Male—[n (%)] | 30 (64) |
| Female—[n (%)] | 17 (36) |
| BMI [kg/m2—mean ± SD] | 29.7 ± 4.9 |
| Systolic blood pressure [mmHg—mean ± SD] | 144.2 ± 22.6 |
| Diastolic blood pressure [mmHg—mean ± SD] | 74.9 ± 14.1 |
| Heart rate [bpm—mean ± SD] | 74.4 ± 14.4 |
| Laboratory data | |
| Hemoglobin [mmol/L—mean ± SD] | 9.1 ± 10.1 |
| eGFR [mL/min/1.73 m2—mean ± SD] | 56.5 ± 23.3 |
| Hematocrit [%—mean ± SD] | 37.8 ± 6.1 |
| Scores | |
| CHA2DS2VASC score [mean ± SD] | 3.9 ± 0.9 |
| HAS-BLED score [mean ± SD] | 5.0 ± 0.9 |
| Atrial Fibrillation | |
| Permanent [n (%)] | 26 (55) |
| SR at baseline and paroxysmal AF in history [n (%)] | 21 (45) |
| Type of anticoagulation | |
| Vitamin K antagonist [n (%)] | 19 (40) |
| Rivaroxaban [n (%)] | 7 (15) |
| Apixaban [n (%)] | 10 (21) |
| Dabigatran [n (%)] | 5 (11) |
| Edoxaban [n (%)] | 6 (13) |
| Major bleeding complication under anticoagulation | |
| Gastrointestinal [n (%)] | 21 (45) |
| Intracranial [n (%)] | 15 (32) |
| ENT [n (%)] | 7 (15) |
| UT [n (%)] | 2 (4) |
| Other [n (%)] | 2 (4) |
| Echocardiographic parameters | |
| Left ventricular ejection fraction [%—mean ± SD] | 59.1 ± 11.9 |
| Orifice area [cm2—mean ± SD] | 3.2 ± 1.1 |
| Sphericity index [mean ± SD] | 1.5 ± 0.21 |
| Procedural data | |
| Occluder size [mm—mean ± SD] | 26.4 ± 3.9 |
| Compression rate [%—mean ± SD] | 42.0 ± 40.9 |
| Type of occluder | |
| WATCHMAN® device [n (%)] | 43 (92) |
| LAmbre device [n (%)] | 4 (8) |
| Comorbidities | |
| Hypertension [n (%)] | 44 (94) |
| Diabetes [n (%)] | 20 (43) |
| Obesity [n (%)] | 28 (60) |
| COPD [n (%)] | 6 (13) |
| Myocardial infarction [n (%)] | 12 (26) |
| CAD [n (%)] | 20 (43) |
| PVD [n (%)] | 9 (19) |
| CKD [n (%)] | 42 (89) |
| RRT [n (%)] | 2 (4) |
| Stroke [n (%)] | 21 (45) |
| Heart failure [n (%)] | 13 (28) |
| Type C Likely Cut-Off Value (Sensitivity [%]) | Type C Unlikely Cut-Off Value (Specificity [%]) | ||
|---|---|---|---|
| 45D | 15.1 ng/mL (88.9) |  | 5.2 ng/mL(94.4) |
| 6M | 17.1 ng/mL (88.9) | 5.2 ng/mL (94.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haertel, F.; Lustermann, P.; Hamadanchi, A.; Gruen, K.; Bogoviku, J.; Aftanski, P.; Westphal, J.; Baez, L.; Franz, M.; Schulze, P.C.; et al. Prognostic Value of Galectin-3 after Left Atrial Appendage Occlusion for Predicting Peri-Device Leakage. Int. J. Mol. Sci. 2023, 24, 16802. https://doi.org/10.3390/ijms242316802
Haertel F, Lustermann P, Hamadanchi A, Gruen K, Bogoviku J, Aftanski P, Westphal J, Baez L, Franz M, Schulze PC, et al. Prognostic Value of Galectin-3 after Left Atrial Appendage Occlusion for Predicting Peri-Device Leakage. International Journal of Molecular Sciences. 2023; 24(23):16802. https://doi.org/10.3390/ijms242316802
Chicago/Turabian StyleHaertel, Franz, Paul Lustermann, Ali Hamadanchi, Katja Gruen, Jurgen Bogoviku, Pawel Aftanski, Julian Westphal, Laura Baez, Marcus Franz, P. Christian Schulze, and et al. 2023. "Prognostic Value of Galectin-3 after Left Atrial Appendage Occlusion for Predicting Peri-Device Leakage" International Journal of Molecular Sciences 24, no. 23: 16802. https://doi.org/10.3390/ijms242316802