
Pre-Emptive Use of Rituximab in Epstein–Barr Virus Reactivation: Incidence, Predictive Factors, Monitoring, and Outcomes
 , , , and
, , , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Conditioning Regimens—Monitoring
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heslop, H.E. How I treat EBV lymphoproliferation. Blood 2009, 114, 4002–4008. [Google Scholar] [CrossRef]
- Sundin, M.; Le Blanc, K.; Ringdén, O.; Barkholt, L.; Omazic, B.; Lergin, C.; Levitsky, V.; Remberger, M. The role of HLA mismatch, splenectomy and recipient Epstein-Barr virus seronegativity as risk factors in post-transplant lymphoproliferative disorder following allogeneic hematopoietic stem cell transplantation. Haematologica 2006, 91, 1059–1067. [Google Scholar] [PubMed]
- Cohen, J.I. Epstein–Barr Virus Infection. N. Engl. J. Med. 2000, 343, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Balfour, H.H.; Dunmire, S.K.; Hogquist, K.A. Infectious mononucleosis. Clin. Transl. Immunol. 2015, 4, e33. [Google Scholar] [CrossRef] [PubMed]
- Young, L.S.; Rickinson, A.B. Epstein–Barr virus: 40 years on. Nat. Rev. Cancer 2004, 4, 757–768. [Google Scholar] [CrossRef]
- Kieff, E.; Rickinson, A.B. Epstein-Barr Virus and Its Replication. In Fields Virology; Knipe, D.M., Howley, P.M., Eds.; Lippinkott-Williams & Wilkins: Philadelphia, PA, USA, 2007; Volume 2, pp. 2603–2654. [Google Scholar]
- Vereide, D.T.; Sugden, B. Lymphomas differ in their dependence on Epstein-Barr virus. Blood 2011, 117, 1977–1985. [Google Scholar] [CrossRef] [PubMed]
- Burns, D.M.; Tierney, R.; Shannon-Lowe, C.; Croudace, J.; Inman, C.; Abbotts, B.; Nagra, S.; Fox, C.P.; Chaganti, S.; Craddock, C.F.; et al. Memory B-cell reconstitution following allogeneic hematopoietic stem cell transplantation is an EBV-associated transformation event. Blood 2015, 126, 2665–2675. [Google Scholar] [CrossRef]
- Krams, S.M.; Martinez, O.M. Epstein–Barr virus, rapamycin, and host immune responses. Curr. Opin. Organ Transplant. 2008, 13, 563–568. [Google Scholar] [CrossRef]
- Capello, D.; Rossi, D.; Gaidano, G. Post-transplant lymphoproliferative disorders: Molecular basis of disease histogenesis and pathogenesis. Hematol. Oncol. 2005, 23, 61–67. [Google Scholar] [CrossRef]
- Henderson, S.; Rowe, M.; Gregory, C.; Croom-Carter, D.; Wang, F.; Longnecker, R.; Kieff, E.; Rickinson, A. Induction of bcl-2 expression by epstein-barr virus latent membrane protein 1 protects infected B cells from programmed cell death. Cell 1991, 65, 1107–1115. [Google Scholar] [CrossRef]
- Swerdlow, S.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.T.J. Post-transplant Lymphoproliferative Disorders. In WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; Swerdlow, S.H., Webber, S.A., Ferry, J.A., Eds.; AARC: Lyon, France, 2017; pp. 453–464. [Google Scholar]
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, A.D.; Araujo, I.B.O.; Berti, E.; Bhagat, G.; Borges, A.M.; Boyer, D.; Calaminici, M.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022, 36, 1720–1748. [Google Scholar] [CrossRef] [PubMed]
- Landgren, O.; Gilbert, E.S.; Rizzo, J.D.; Socié, G.; Banks, P.M.; Sobocinski, K.A.; Horowitz, M.M.; Jaffe, E.S.; Kingma, D.W.; Travis, L.B.; et al. Risk factors for lymphoproliferative disorders after allogeneic hematopoietic cell transplantation. Blood 2009, 113, 4992–5001. [Google Scholar] [CrossRef] [PubMed]
- Al Hamed, R.; Bazarbachi, A.H.; Mohty, M. Epstein-Barr virus-related post-transplant lymphoproliferative disease (EBV-PTLD) in the setting of allogeneic stem cell transplantation: A comprehensive review from pathogenesis to forthcoming treatment modalities. Bone Marrow Transplant. 2020, 55, 25–39. [Google Scholar] [CrossRef]
- Juvonen, E.; Aalto, S.M.; Tarkkanen, J.; Volin, L.; Mattila, P.S.; Knuutila, S.; Ruutu, T.; Hedman, K. High incidence of PTLD after non-T-cell-depleted allogeneic haematopoietic stem cell transplantation as a consequence of intensive immunosuppressive treatment. Bone Marrow Transplant. 2003, 32, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Uhlin, M.; Wikell, H.; Sundin, M.; Blennow, O.; Maeurer, M.; Ringden, O.; Winiarski, J.; Ljungman, P.; Remberger, M.; Mattsson, J. Risk factors for Epstein-Barr virus-related post-transplant lymphoproliferative disease after allogeneic hematopoietic stem cell transplantation. Haematologica 2013, 99, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.M.; Cooper, N.; Chakrabarti, S.; Thomson, K.; Samarasinghe, S.; Cubitt, D.; Lloyd, C.; Woolfrey, A.; Veys, P.; Amrolia, P.J. EBV-related disease following haematopoietic stem cell transplantation with reduced intensity conditioning. Leuk. Lymphoma 2007, 48, 256–269. [Google Scholar] [CrossRef]
- Cockfield, S.M. Identifying the patient at risk for post-transplant lymphoproliferative disorder. Transpl. Infect. Dis. 2001, 3, 70–78. [Google Scholar] [CrossRef]
- San-Juan, R.; Manuel, O.; Hirsch, H.H.; Fernández-Ruiz, M.; López-Medrano, F.; Comoli, P.; Caillard, S.; Grossi, P.A.; Aguado, J.M.; Alamo-Martinez, J.M.; et al. Current preventive strategies and management of Epstein–Barr virus-related post-transplant lymphoproliferative disease in solid organ transplantation in Europe. Results of the ESGICH Questionnaire-based Cross-sectional Survey. Clin. Microbiol. Infect. 2015, 21, 604.e1–604.e9. [Google Scholar] [CrossRef]
- Gross, T.G.; Steinbuch, M.; DeFor, T.; Shapiro, R.S.; McGlave, P.; Ramsay, N.K.C.; Wagner, J.E.; Filipovich, A.H. B cell lymphoproliferative disorders following hematopoietic stem cell transplantation: Risk factors, treatment and outcome. Bone Marrow Transplant. 1999, 23, 251–258. [Google Scholar] [CrossRef]
- Kinch, A.; Öberg, G.; Arvidson, J.; Falk, K.I.; Linde, A.; Pauksens, K. Post-transplant lymphoproliferative disease and other Epstein-Barr virus diseases in allogeneic haematopoietic stem cell transplantation after introduction of monitoring of viral load by polymerase chain reaction. Scand. J. Infect. Dis. 2007, 39, 235–244. [Google Scholar] [CrossRef]
- Brunstein, C.G.; Weisdorf, D.J.; DeFor, T.; Barker, J.N.; Tolar, J.; van Burik, J.-A.H.; Wagner, J.E. Marked increased risk of Epstein-Barr virus-related complications with the addition of antithymocyte globulin to a nonmyeloablative conditioning prior to unrelated umbilical cord blood transplantation. Blood 2006, 108, 2874–2880. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, M.S.; Cho, Y.W.; Shah, T.; Bunnapradist, S.; Hutchinson, I.V. Impact of Epstein-Barr virus donor and recipient serostatus on the incidence of post-transplant lymphoproliferative disorder in kidney transplant recipients. Nephrol. Dial. Transplant. 2012, 27, 2971–2979. [Google Scholar] [CrossRef] [PubMed]
- Dierickx, D.; Habermann, T.M. Post-Transplantation Lymphoproliferative Disorders in Adults. N. Engl. J. Med. 2018, 378, 549–562. [Google Scholar] [CrossRef]
- Allen, U.D.; Preiksaitis, J.K. Post-transplant lymphoproliferative disorders, Epstein-Barr virus infection, and disease in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13652. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, F.; Yazbeck, V.; Raptis, A.; Felgar, R.; Boyiadzis, M. Primary central nervous system post-transplant lymphoproliferative disorders following allogeneic hematopoietic stem cell transplantation. J. Neuro-Oncol. 2011, 107, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Preiksaitis, J.K.; Pang, X.L.; Fox, J.D.; Fenton, J.M.; Caliendo, A.M.; Miller, G.G. Interlaboratory Comparison of Epstein-Barr Virus Viral Load Assays. Am. J. Transplant. 2009, 9, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Preiksaitis, J.K. Epstein—Barr Viral Load Testing: Role in the Prevention, Diagnosis and Management of Posttransplant Lymphoproliferative Disorders. In Post-Transplant Lymphoproliferative Disorders; Dharnidharka, V.R., Green, M., Webber, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; pp. 45–67. [Google Scholar] [CrossRef]
- Gärtner, B.; Preiksaitis, J.K. EBV viral load detection in clinical virology. J. Clin. Virol. 2010, 48, 82–90. [Google Scholar] [CrossRef]
- Styczynski, J.; Van Der Velden, W.; Fox, C.P.; Engelhard, D.; de la Camara, R.; Cordonnier, C.; Ljungman, P. Management of Epstein-Barr Virus infections and post-transplant lymphoproliferative disorders in patients after allogeneic hematopoietic stem cell transplantation: Sixth European Conference on Infections in Leukemia (ECIL-6) guidelines. Haematologica 2016, 101, 803–811. [Google Scholar] [CrossRef]
- Tang, L.; Su, Y.; Pounds, S.; Hayden, R.T. Quantitative Inference of Commutability for Clinical Viral Load Testing. J. Clin. Microbiol. 2018, 56, e00146-18. [Google Scholar] [CrossRef]
- Buelow, D.; Sun, Y.; Tang, L.; Gu, Z.; Pounds, S.; Hayden, R. Comparative Evaluation of Four Real-Time PCR Methods for the Quantitative Detection of Epstein-Barr Virus from Whole Blood Specimens. J. Mol. Diagn. 2016, 18, 527–534. [Google Scholar] [CrossRef]
- Rychert, J.; Danziger-Isakov, L.; Yen-Lieberman, B.; Storch, G.; Buller, R.; Sweet, S.C.; Mehta, A.K.; Cheeseman, J.A.; Heeger, P.; Rosenberg, E.S.; et al. Multicenter comparison of laboratory performance in cytomegalovirus and Epstein-Barr virus viral load testing using international standards. Clin. Transplant. 2014, 28, 1416–1423. [Google Scholar] [CrossRef] [PubMed]
- van Esser, J.W.J.; van der Holt, B.; Meijer, E.; Niesters, H.G.M.; Trenschel, R.; Thijsen, S.F.T.; van Loon, A.M.; Frassoni, F.; Bacigalupo, A.; Schaefer, U.W.; et al. Epstein-Barr virus (EBV) reactivation is a frequent event after allogeneic stem cell transplantation (SCT) and quantitatively predicts EBV-lymphoproliferative disease following T-cell–depleted SCT. Blood 2001, 98, 972–978. [Google Scholar] [CrossRef]
- Ahmad, I.; Cau, N.V.; Kwan, J.; Maaroufi, Y.; Meuleman, N.; Aoun, M.; Lewalle, P.; Martiat, P.; Crokaert, F.; Bron, D. Preemptive Management of Epstein-Barr Virus Reactivation After Hematopoietic Stem-Cell Transplantation. Transplantation 2009, 87, 1240–1245. [Google Scholar] [CrossRef] [PubMed]
- Worth, A.; Conyers, R.; Cohen, J.; Jagani, M.; Chiesa, R.; Rao, K.; Goulden, N.; Veys, P.; Amrolia, P.J. Pre-emptive rituximab based on viraemia and T cell reconstitution: A highly effective strategy for the prevention of Epstein–Barr virus-associated lymphoproliferative disease following stem cell transplantation. Br. J. Haematol. 2011, 155, 377–385. [Google Scholar] [CrossRef] [PubMed]
- DeStefano, C.B.; Desai, S.H.; Shenoy, A.G.; Catlett, J.P. Management of post-transplant lymphoproliferative disorders. Br. J. Haematol. 2018, 182, 330–343. [Google Scholar] [CrossRef]
- Kullberg-Lindh, C.; Olofsson, S.; Brune, M.; Lindh, M. Comparison of serum and whole blood levels of cytomegalovirus and Epstein-Barr virus DNA. Transpl. Infect. Dis. 2008, 10, 308–315. [Google Scholar] [CrossRef]
- Reshef, R.; Vardhanabhuti, S.; Luskin, M.R.; Heitjan, D.F.; Hadjiliadis, D.; Goral, S.; Krok, K.L.; Goldberg, L.R.; Porter, D.L.; Stadtmauer, E.A.; et al. Reduction of Immunosuppression as Initial Therapy for Posttransplantation Lymphoproliferative Disorder★. Am. J. Transplant. 2011, 11, 336–347. [Google Scholar] [CrossRef]
- Styczynski, J.; Einsele, H.; Gil, L.; Ljungman, P. Outcome of treatment of Epstein-Barr virus-related post-transplant lymphoproliferative disorder in hematopoietic stem cell recipients: A comprehensive review of reported cases. Transpl. Infect. Dis. 2009, 11, 383–392. [Google Scholar] [CrossRef]
- Raberahona, M.; Wackenheim, C.; Carré, M.; Thiébaut, A.; Lupo, J.; Semenova, T.; Morand, P.; Bulabois, C.-E.; Cahn, J.-Y.; Germi, R.; et al. Dynamics of Epstein-Barr viral load after hematopoietic stem cell transplantation and effect of preemptive rituximab therapy. Transpl. Infect. Dis. 2016, 18, 889–895. [Google Scholar] [CrossRef]
- Chang, Y.-J.; Xu, L.-P.; Wang, Y.; Zhang, X.-H.; Chen, H.; Chen, Y.-H.; Wang, F.-R.; Han, W.; Sun, Y.-Q.; Yan, C.-H.; et al. Rituximab for desensitization during HLA-mismatched stem cell transplantation in patients with a positive donor-specific anti-HLA antibody. Bone Marrow Transplant. 2020, 55, 1326–1336. [Google Scholar] [CrossRef]
- Coppoletta, S.; Tedone, E.; Galano, B.; Soracco, M.; Raiola, A.M.; Lamparelli, T.; Gualandi, F.; Bregante, S.; Ibatici, A.; di Grazia, C.; et al. Rituximab Treatment for Epstein-Barr Virus DNAemia after Alternative-Donor Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2011, 17, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Patriarca, F.; Medeot, M.; Isola, M.; Battista, M.L.; Sperotto, A.; Pipan, C.; Toffoletti, E.; Dozzo, M.; Michelutti, A.; Gregoraci, G.; et al. Prognostic factors and outcome of Epstein-Barr virus DNAemia in high-risk recipients of allogeneic stem cell transplantation treated with preemptive rituximab. Transpl. Infect. Dis. 2013, 15, 259–267. [Google Scholar] [CrossRef]
- Messahel, B.; Taj, M.M.; Hobson, R.; Hadzic, N.; Ramsay, A.; Hann, I.; Pinkerton, R. Single agent efficacy of rituximab in childhood immunosuppression related lymphoproliferative disease: A United Kingdom Children’s Cancer Study Group (UKCCSG) retrospective review. Leuk. Lymphoma 2006, 47, 2584–2589. [Google Scholar] [CrossRef] [PubMed]
- Rouce, R.H.; Louis, C.U.; Heslop, H.E. Epstein–Barr virus lymphoproliferative disease after hematopoietic stem cell transplant. Curr. Opin. Hematol. 2014, 21, 476–481. [Google Scholar] [CrossRef]
- Reddy, N.; Rezvani, K.; Barrett, A.J.; Savani, B.N. Strategies to Prevent EBV Reactivation and Posttransplant Lymphoproliferative Disorders (PTLD) after Allogeneic Stem Cell Transplantation in High-Risk Patients. Biol. Blood Marrow Transplant. 2011, 17, 591–597. [Google Scholar] [CrossRef]
- Chiereghin, A.; Bertuzzi, C.; Piccirilli, G.; Gabrielli, L.; Squarzoni, D.; Turello, G.; Ferioli, M.; Sessa, M.; Bonifazi, F.; Zanoni, L.; et al. Successful management of EBV-PTLD in allogeneic bone marrow transplant recipient by virological–immunological monitoring of EBV infection, prompt diagnosis and early treatment. Transpl. Immunol. 2016, 34, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Stocker, N.; Labopin, M.; Boussen, I.; Paccoud, O.; Bonnin, A.; Malard, F.; Amiel, C.; Gozlan, J.; Battipaglia, G.; Duléry, R.; et al. Pre-emptive rituximab treatment for Epstein–Barr virus reactivation after allogeneic hematopoietic stem cell transplantation is a worthwhile strategy in high-risk recipients: A comparative study for immune recovery and clinical outcomes. Bone Marrow Transplant. 2019, 55, 586–594. [Google Scholar] [CrossRef]
- Avivi, I.; Stroopinsky, D.; Katz, T. Anti-CD20 monoclonal antibodies: Beyond B-cells. Blood Rev. 2013, 27, 217–223. [Google Scholar] [CrossRef]
- Kinch, A.; Hallböök, H.; Arvidson, J.; Sällström, K.; Bondeson, K.; Pauksens, K. Long-term outcome of Epstein–Barr virus DNAemia and PTLD with the use of preemptive rituximab following allogeneic HSCT. Leuk. Lymphoma 2017, 59, 1172–1179. [Google Scholar] [CrossRef]
- Luterbacher, F.; Bernard, F.; Baleydier, F.; Ranza, E.; Jandus, P.; Blanchard-Rohner, G. Case Report: Persistent Hypogammaglobulinemia More Than 10 Years After Rituximab Given Post-HSCT. Front. Immunol. 2021, 12, 773853. [Google Scholar] [CrossRef]
- Petropoulou, A.D.; Porcher, R.; de Latour, R.P.; Xhaard, A.; Weisdorf, D.; Ribaud, P.; Rodriguez-Otero, P.; Agbalika, F.; Talbot, A.; Toubert, A.; et al. Increased Infection Rate After Preemptive Rituximab Treatment for Epstein-Barr Virus Reactivation After Allogeneic Hematopoietic Stem-Cell Transplantation. Transplantation 2012, 94, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Comoli, P.; Basso, S.; Zecca, M.; Pagliara, D.; Baldanti, F.; Bernardo, M.E.; Barberi, W.; Moretta, A.; Labirio, M.; Paulli, M.; et al. Preemptive Therapy of EBV-Related Lymphoproliferative Disease after Pediatric Haploidentical Stem Cell Transplantation. Am. J. Transplant. 2007, 7, 1648–1655. [Google Scholar] [CrossRef]
- Heslop, H.E.; Sharma, S.; Rooney, C.M. Adoptive T-Cell Therapy for Epstein-Barr Virus–Related Lymphomas. J. Clin. Oncol. 2021, 39, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Heslop, H.E.; Slobod, K.S.; Pule, M.A.; Hale, G.A.; Rousseau, A.; Smith, C.A.; Bollard, C.M.; Liu, H.; Wu, M.-F.; Rochester, R.J.; et al. Long-term outcome of EBV-specific T-cell infusions to prevent or treat EBV-related lymphoproliferative disease in transplant recipients. Blood 2010, 115, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Saglio, F.; Hanley, P.J.; Bollard, C.M. The time is now: Moving toward virus-specific T cells after allogeneic hematopoietic stem cell transplantation as the standard of care. Cytotherapy 2014, 16, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Moosmann, A.; Bigalke, I.; Tischer, J.; Schirrmann, L.; Kasten, J.; Tippmer, S.; Leeping, M.; Prevalšek, D.; Jaeger, G.; Ledderose, G.; et al. Effective and long-term control of EBV PTLD after transfer of peptide-selected T cells. Blood 2010, 115, 2960–2970. [Google Scholar] [CrossRef]
- Keller, M.D.; Darko, S.; Lang, H.; Ransier, A.; Lazarski, C.A.; Wang, Y.; Hanley, P.J.; Davila, B.J.; Heimall, J.R.; Ambinder, R.F.; et al. T-cell receptor sequencing demonstrates persistence of virus-specific T cells after antiviral immunotherapy. Br. J. Haematol. 2019, 187, 206–218. [Google Scholar] [CrossRef]
- Papadopoulou, A.; Alvanou, M.; Karavalakis, G.; Tzannou, I.; Yannaki, E. Pathogen-specific T Cells: Targeting Old Enemies and New Invaders in Transplantation and Beyond. Hemasphere 2023, 7, e809. [Google Scholar] [CrossRef]
- Luttwak, E.; Hagin, D.; Perry, C.; Wolach, O.; Itchaki, G.; Amit, O.; Bar-On, Y.; Freund, T.; Kay, S.; Eshel, R.; et al. Anti-CD19 CAR-T therapy for EBV-negative posttransplantation lymphoproliferative disease—A single center case series. Bone Marrow Transplant. 2020, 56, 1031–1037. [Google Scholar] [CrossRef]
- Dang, B.N.; Ch’ng, J.; Russell, M.; Cheng, J.C.; Moore, T.B.; Alejos, J.C. Treatment of post-transplant lymphoproliferative disorder (PTLD) in a heart transplant recipient with chimeric antigen receptor T-cell therapy. Pediatr. Transplant. 2020, 25, e13861. [Google Scholar] [CrossRef]
- Krishnamoorthy, S.; Ghobadi, A.; Santos, R.D.; Schilling, J.D.; Malone, A.F.; Murad, H.; Bartlett, N.L.; Alhamad, T. CAR-T therapy in solid organ transplant recipients with treatment refractory posttransplant lymphoproliferative disorder. Am. J. Transplant. 2020, 21, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Mamlouk, O.; Nair, R.; Iyer, S.P.; Edwards, A.; Neelapu, S.S.; Steiner, R.E.; Adkins, S.A.; Hawkins, M.; Saini, N.Y.; Devashish, K.; et al. Safety of CAR T-cell therapy in kidney transplant recipients. Blood 2021, 137, 2558–2562. [Google Scholar] [CrossRef] [PubMed]
- Yan, N.; Wang, N.; Zhang, P.; Wang, G.; Mao, X.; Peng, D.; Kuang, D.; Chen, L.; Zhu, L.; Zhou, J.; et al. Case Report: Successful Chimeric Antigen Receptor T Cell Therapy in Haploidentical-Allogeneic Stem Cell Transplant Patients with Post-Transplant Lymphoproliferative Disorder. Front. Oncol. 2021, 11, 709370. [Google Scholar] [CrossRef] [PubMed]
- Portell, C.; Nand, S. Single agent lenalidomide induces a response in refractory T-cell posttransplantation lymphoproliferative disorder. Blood 2008, 111, 4416–4417. [Google Scholar] [CrossRef] [PubMed]
- Läubli, H.; Tzankov, A.; Juskevicius, D.; Degen, L.; Rochlitz, C.; Stenner-Liewen, F. Lenalidomide monotherapy leads to a complete remission in refractory B-cell post-transplant lymphoproliferative disorder. Leuk. Lymphoma 2015, 57, 945–948. [Google Scholar] [CrossRef]
- Blaes, A.H.; Hammerschmidt, D.E.; Peterson, B.A. Bortezomib and Rituximab in the Treatment of Post-Transplant Lymphoproliferative Disorders. Blood 2011, 118, 4947. [Google Scholar] [CrossRef]
- Reid, E.G. Bortezomib-induced Epstein–Barr virus and Kaposi sarcoma herpesvirus lytic gene expression. Curr. Opin. Oncol. 2011, 23, 482–487. [Google Scholar] [CrossRef]
- Kalra, A.; Roessner, C.; Jupp, J.; Williamson, T.; Tellier, R.; Chaudhry, A.; Khan, F.; Taparia, M.; Jimenez-Zepeda, V.H.; Stewart, D.A.; et al. Epstein-barr virus DNAemia monitoring for the management of post-transplant lymphoproliferative disorder. Cytotherapy 2018, 20, 706–714. [Google Scholar] [CrossRef]
- García-Cadenas, I.; Castillo, N.; Martino, R.; Barba, P.; Esquirol, A.; Novelli, S.; Orti, G.; Garrido, A.; Saavedra, S.; Moreno, C.; et al. Impact of Epstein Barr virus-related complications after high-risk allo-SCT in the era of pre-emptive rituximab. Bone Marrow Transplant. 2015, 50, 579–584. [Google Scholar] [CrossRef]
- Chen, J.; Sun, Y.Q.; Xu, L.P.; Zhang, X.H.; Liu, K.Y.; Mo, X.D.; Cheng, Y.F.; Huang, X.J.; Wang, Y. Dynamic monitoring of plasma Epstein-Barr Virus DNA load can predict the occurrence of lymphoproliferative disorders after haploidentical hematopoietic stem cell transplantation. Zhonghua Xue Ye Xue Za Zhi 2023, 44, 284–288. [Google Scholar] [CrossRef]
- Düver, F.; Weißbrich, B.; Eyrich, M.; Wölfl, M.; Schlegel, P.G.; Wiegering, V. Viral reactivations following hematopoietic stem cell transplantation in pediatric patients—A single center 11-year analysis. PLoS ONE 2020, 15, e0228451. [Google Scholar] [CrossRef] [PubMed]
- Solano, C.; Mateo, E.M.; Pérez, A.; Talaya, A.; Terol, M.J.; Albert, E.; Giménez, E.; Vinuesa, V.; Piñana, J.L.; Boluda, J.C.H.; et al. Epstein-Barr virus DNA load kinetics analysis in allogeneic hematopoietic stem cell transplant recipients: Is it of any clinical usefulness? J. Clin. Virol. 2017, 97, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Sakellari, I.; Batsis, I.; Bousiou, Z.; Mallouri, D.; Constantinou, V.; Gavriilaki, E.; Smias, C.; Yannaki, E.; Kaloyannidis, P.; Papaioannou, G.; et al. The Role of Low-dose Anti-thymocyte Globulin as Standard Prophylaxis in Mismatched and Matched Unrelated Hematopoietic Peripheral Stem Cell Transplantation for Hematologic Malignancies. Clin. Lymphoma Myeloma Leuk. 2017, 17, 658–666. [Google Scholar] [CrossRef]
- Gavriilaki, E.; Sakellari, I.; Chatzikonstantinou, T.; Mallouri, D.; Batsis, I.; Vardi, A.; Bousiou, Z.; Koravou, E.-E.; Masmanidou, M.; Touloumenidou, T.; et al. Endothelial and Complement Activation as Predictors of Survival in Adult Allogeneic Hematopoietic Cell Transplantation. Hemasphere 2020, 5, e487. [Google Scholar] [CrossRef] [PubMed]
- Glucksberg, H.; Storb, R.; Fefer, A.; Buckner, C.D.; Neiman, P.E.; Clift, R.A.; Lerner, K.G.; Thomas, E.D. Clinical manifestations of graft-versus-host disease in human recipients of marrow from hl-a-matched sibling donors. Transplantation 1974, 18, 295–304. [Google Scholar] [CrossRef]
- Lee, S.J.; Wolff, D.; Kitko, C.; Koreth, J.; Inamoto, Y.; Jagasia, M.; Pidala, J.; Olivieri, A.; Martin, P.J.; Przepiorka, D.; et al. Measuring Therapeutic Response in Chronic Graft-versus-Host Disease. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: IV. The 2014 Response Criteria Working Group Report. Biol. Blood Marrow Transplant. 2015, 21, 984–999. [Google Scholar] [CrossRef]
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar]



{kind=link}
{kind=link}
| Biographical Data | Category | Frequency | Percentage | Mean (Copies/mL) | Median (Copies/mL) | Min (Copies/mL) | Max (Copies/mL) |
|---|---|---|---|---|---|---|---|
| Gender | Male | 56/100 | 56% | 112,944 | 27,950 | 9120 | 2,760,000 |
| Female | 44/100 | 44% | 102,348 | 20,000 | 8690 | 1,150,000 | |
| Age group | 0–18 | 6/100 | 6% | 64,567 | 17,700 | 10,400 | 180,000 |
| 18–44 | 49/100 | 49% | 118,480 | 27,200 | 8700 | 2,760,000 | |
| 44+ | 45/100 | 45% | 103,005 | 21,000 | 8690 | 1,150,000 | |
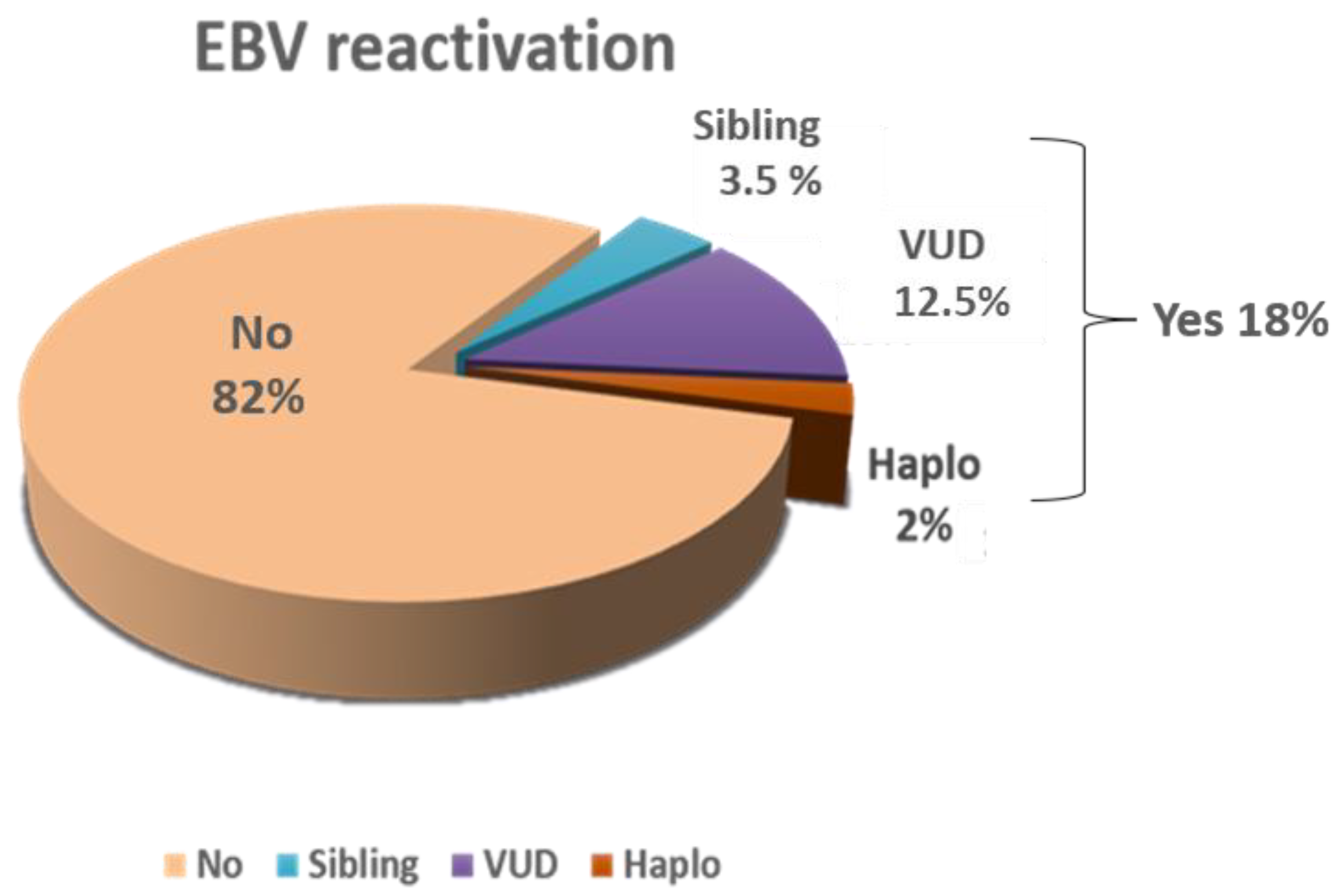
| Type of transplant | Sibling | 20/100 | 20% | 95,622 | 20,500 | 9930 | 1,150,000 |
| VUD | 68/100 | 68% | 74,100 | 22,850 | 8690 | 951,000 | |
| Haplo | 12/100 | 12% | 323,075 | 48,900 | 10,800 | 2,760,000 | |
| Type of conditioning | Myeloablative | 88/100 | 88% | 118,796 | 27,250 | 8690 | 2,760,000 |
| RIC | 12/100 | 12% | 19,225 | 17,250 | 8700 | 47,100 | |
| aGVHD | Yes | 64/100 | 64% | 95,706 | 26,650 | 8690 | 2,760,000 |
| No | 36/100 | 36% | 130,637 | 22,750 | 9930 | 1,150,000 | |
| cGVHD | Yes | 82/100 | 82% | 76,344 | 26,650 | 8690 | 1,150,000 |
| No | 18/100 | 18% | 253,772 | 17,550 | 10,000 | 2,760,000 | |
| Rituximab treatment | Yes | 74/100 | 74% | 135,788 | 30,400 | 8690 | 2,760,000 |
| No | 26/100 | 26% | 29,996 | 16,350 | 10,300 | 148,000 | |
| Rituximab cycles | One | 64/74 | 86.5% | 138,663 | 29,300 | 8690 | 2,760,000 |
| Two | 9/74 | 12.1% | 83,244 | 29,800 | 10,400 | 499,000 | |
| Three | 1/74 | 1.4% | 383,000 | 383,000 | 383,000 | 383,000 | |
| PTLD | Yes | 5/100 | 5% | 684,680 | 78,400 | 31,000 | 2,760,000 |
| No | 95/100 | 95% | 77,495 | 21,000 | 8690 | 1,150,000 | |
| EBV relapse | Yes | 13/100 | 13% | 281,323 | 40,000 | 11,000 | 2,760,000 |
| No | 87/100 | 87% | 76,339 | 20,500 | 8690 | 1,150,000 | |
| CMV reactivation | Yes | 47/100 | 47% | 82,766 | 20,300 | 8690 | 1,150,000 |
| No | 53/100 | 53% | 130,778 | 24,600 | 9120 | 2,760,000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papalexandri, A.; Gavriilaki, E.; Vardi, A.; Kotsiou, N.; Demosthenous, C.; Constantinou, N.; Touloumenidou, T.; Zerva, P.; Kika, F.; Iskas, M.; et al. Pre-Emptive Use of Rituximab in Epstein–Barr Virus Reactivation: Incidence, Predictive Factors, Monitoring, and Outcomes. Int. J. Mol. Sci. 2023, 24, 16029. https://doi.org/10.3390/ijms242216029
Papalexandri A, Gavriilaki E, Vardi A, Kotsiou N, Demosthenous C, Constantinou N, Touloumenidou T, Zerva P, Kika F, Iskas M, et al. Pre-Emptive Use of Rituximab in Epstein–Barr Virus Reactivation: Incidence, Predictive Factors, Monitoring, and Outcomes. International Journal of Molecular Sciences. 2023; 24(22):16029. https://doi.org/10.3390/ijms242216029
Chicago/Turabian StylePapalexandri, Apostolia, Eleni Gavriilaki, Anna Vardi, Nikolaos Kotsiou, Christos Demosthenous, Natassa Constantinou, Tasoula Touloumenidou, Panagiota Zerva, Fotini Kika, Michalis Iskas, and et al. 2023. "Pre-Emptive Use of Rituximab in Epstein–Barr Virus Reactivation: Incidence, Predictive Factors, Monitoring, and Outcomes" International Journal of Molecular Sciences 24, no. 22: 16029. https://doi.org/10.3390/ijms242216029