
Splanchnic Vein Thrombosis in Myelofibrosis—An Underappreciated Hallmark of Disease Phenotype

Abstract
:1. Introduction
2. Splanchnic Vein Thrombosis—General Considerations
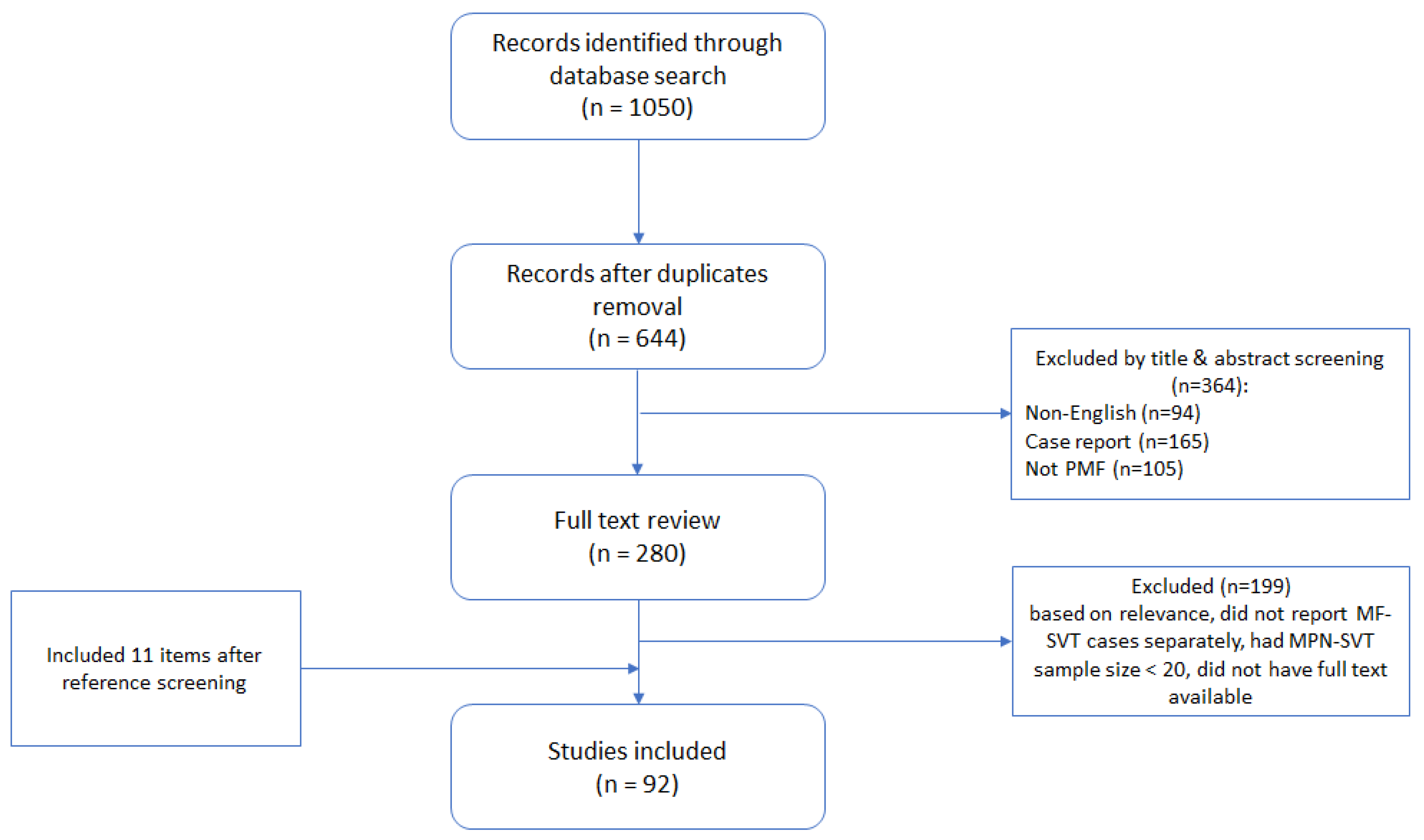
3. Methods
4. Epidemiology of SVT in Myelofibrosis
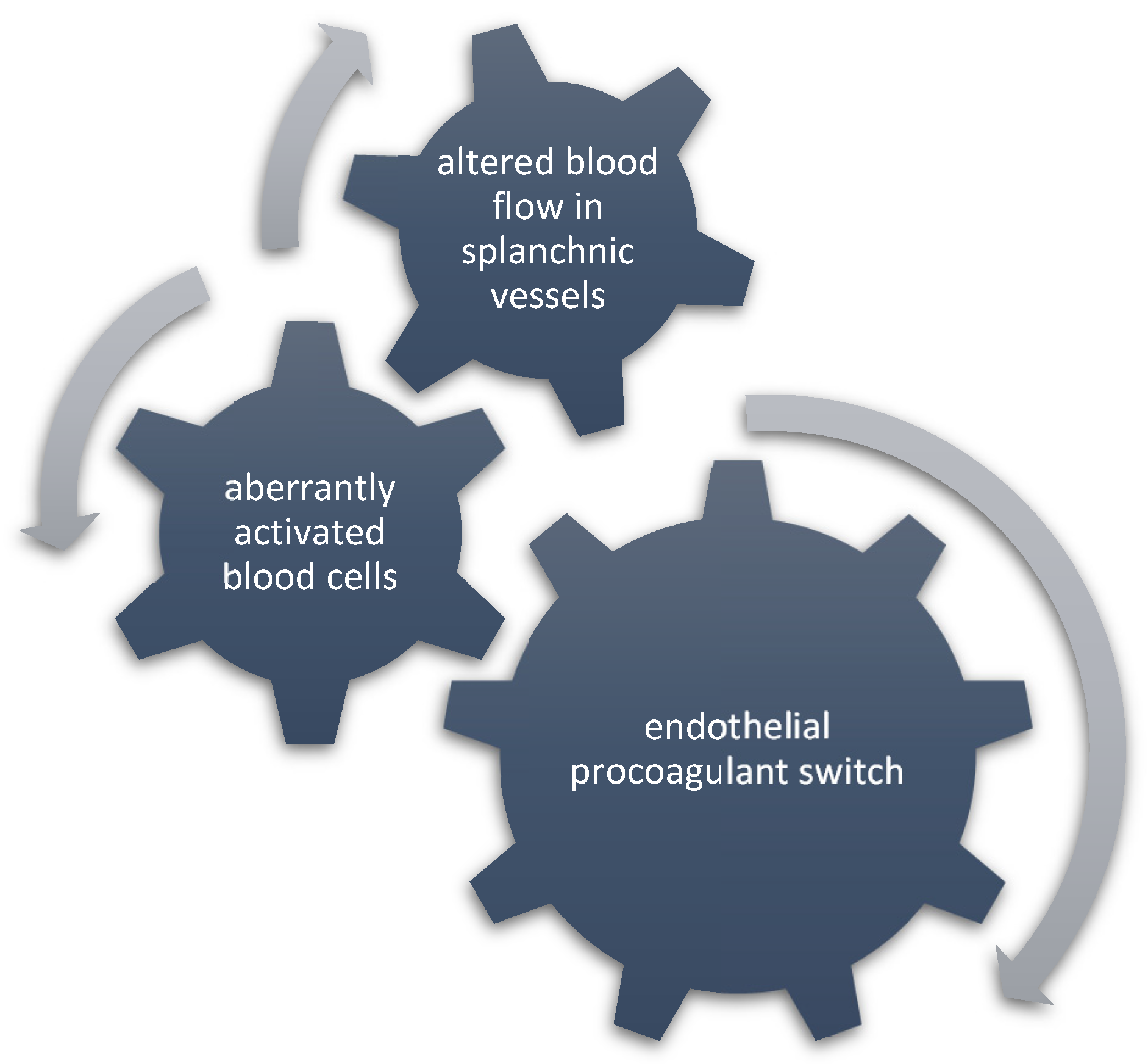
5. Pathogenesis of SVT in Myelofibrosis
6. Predictive Risk Factors and Clinical Outcomes of SVT in Myelofibrosis
7. Molecular Profiling and Thrombotic Risk in Myelofibrosis
8. Treatment of SVT in Myelofibrosis
8.1. Role of Non-MF Directed Therapy
8.1.1. Medical Treatment
8.1.2. Interventional Treatment
8.2. Role of MF Directed Therapy
9. Future Directions and Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| BCS | Budd–Chiari syndrome |
| CHIP | clonal hematopoiesis of indeterminate potential |
| CI | confidence interval |
| DOACs | direct oral anticoagulants |
| E-CFC | endothelial colony-forming cells |
| EDA-FN | extra-domain A fibronectin |
| ET | essential thrombocythemia |
| HMR | high molecular risk |
| HR | hazard ratio |
| ICAM-1 | Intercellular Adhesion Molecule 1 |
| IPSET | International Prognostic Score of Thrombosis in Essential Thrombocythemia |
| IPSS | International Prognostic Scoring System |
| LMWH | low-molecular weight heparin |
| MF | myelofibrosis |
| MPNs | myeloproliferative neoplasms |
| MF | myelofibrosis |
| MVT | mesenteric vein thrombosis |
| NET | neutrophil extracellular traps |
| NGS | next generation sequencing |
| OLT | orthotopic liver transplantation |
| OS | overall survival |
| prePMF | prefibrotic primary myelofibrosis |
| PMF | primary myelofibrosis (PV—polycythemia vera) |
| PVT | portal vein thrombosis |
| SVT | splanchnic vein thrombosis |
| TIPS | transjugular intrahepatic portosystemic shunt |
| TFS | thrombosis free survival |
| TNF | tumor necrotizing factor |
| VCAM-1 | vascular cell adhesion protein 1 |
| VEGF | vascular endothelial growth factor |
| vWF | von Willebrand Factors |
References
- Moulard, O.; Mehta, J.; Fryzek, J.; Olivares, R.; Iqbal, U.; Mesa, R.A. Epidemiology of Myelofibrosis, Essential Thrombocythemia, and Polycythemia Vera in the European Union. Eur. J. Haematol. 2014, 92, 289–297. [Google Scholar] [CrossRef]
- Barosi, G.; Rosti, V.; Bonetti, E.; Campanelli, R.; Carolei, A.; Catarsi, P.; Isgrò, A.M.; Lupo, L.; Massa, M.; Poletto, V.; et al. Evidence That Prefibrotic Myelofibrosis Is Aligned along a Clinical and Biological Continuum Featuring Primary Myelofibrosis. PLoS ONE 2012, 7, e35631. [Google Scholar] [CrossRef] [PubMed]
- Tefferi, A. Primary Myelofibrosis: 2021 Update on Diagnosis, Risk-Stratification and Management. Am. J. Hematol. 2021, 96, 145–162. [Google Scholar] [CrossRef]
- Emanuel, R.M.; Dueck, A.C.; Geyer, H.L.; Kiladjian, J.-J.; Slot, S.; Zweegman, S.; te Boekhorst, P.A.W.; Commandeur, S.; Schouten, H.C.; Sackmann, F.; et al. Myeloproliferative Neoplasm (MPN) Symptom Assessment Form Total Symptom Score: Prospective International Assessment of an Abbreviated Symptom Burden Scoring System among Patients with MPNs. J. Clin. Oncol. 2012, 30, 4098–4103. [Google Scholar] [CrossRef] [PubMed]
- Rungjirajittranon, T.; Owattanapanich, W.; Ungprasert, P.; Siritanaratkul, N.; Ruchutrakool, T. A Systematic Review and Meta-Analysis of the Prevalence of Thrombosis and Bleeding at Diagnosis of Philadelphia-Negative Myeloproliferative Neoplasms. BMC Cancer 2019, 19, 184. [Google Scholar] [CrossRef] [PubMed]
- Guglielmelli, P.; Carobbio, A.; Rumi, E.; De Stefano, V.; Mannelli, L.; Mannelli, F.; Rotunno, G.; Coltro, G.; Betti, S.; Cavalloni, C.; et al. Validation of the IPSET Score for Thrombosis in Patients with Prefibrotic Myelofibrosis. Blood Cancer J. 2020, 10, 21. [Google Scholar] [CrossRef]
- Ageno, W.; Squizzato, A.; Togna, A.; Magistrali, F.; Mangini, M.; Fugazzola, C.; Dentali, F. Incidental Diagnosis of a Deep Vein Thrombosis in Consecutive Patients Undergoing a Computed Tomography Scan of the Abdomen: A Retrospective Cohort Study. J. Thromb. Haemost. 2012, 10, 158–160. [Google Scholar] [CrossRef]
- Ogren, M.; Bergqvist, D.; Björck, M.; Acosta, S.; Eriksson, H.; Sternby, N.H. Portal Vein Thrombosis: Prevalence, Patient Characteristics and Lifetime Risk: A Population Study Based on 23,796 Consecutive Autopsies. World J. Gastroenterol. 2006, 12, 2115–2119. [Google Scholar] [CrossRef] [PubMed]
- Pantic, N.; Pantic, I.; Jevtic, D.; Mogulla, V.; Oluic, S.; Durdevic, M.; Nordin, T.; Jecmenica, M.; Milovanovic, T.; Gavrancic, T.; et al. Celiac Disease and Thrombotic Events: Systematic Review of Published Cases. Nutrients 2022, 14, 2162. [Google Scholar] [CrossRef]
- Thatipelli, M.R.; McBane, R.D.; Hodge, D.O.; Wysokinski, W.E. Survival and Recurrence in Patients With Splanchnic Vein Thromboses. Clin. Gastroenterol. Hepatol. 2010, 8, 200–205. [Google Scholar] [CrossRef]
- Ageno, W.; Dentali, F.; Squizzato, A. How I Treat Splanchnic Vein Thrombosis. Blood 2014, 124, 3685–3691. [Google Scholar] [CrossRef]
- Darwish Murad, S.; Valla, D.-C.; de Groen, P.C.; Zeitoun, G.; Hopmans, J.A.M.; Haagsma, E.B.; van Hoek, B.; Hansen, B.E.; Rosendaal, F.R.; Janssen, H.L.A. Determinants of Survival and the Effect of Portosystemic Shunting in Patients with Budd-Chiari Syndrome. Hepatology 2004, 39, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Senzolo, M.; Cholongitas, E.C.; Patch, D.; Burroughs, A.K. Update on the Classification, Assessment of Prognosis and Therapy of Budd-Chiari Syndrome. Nat. Clin. Pr. Gastroenterol. Hepatol. 2005, 2, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.E.; Wadhera, R.K.; Piazza, G. Mesenteric Venous Thrombosis. Circulation 2015, 131, 1599–1603. [Google Scholar] [CrossRef] [PubMed]
- Benjilali, L.; Essaadouni, L. Les thromboses veineuses splanchniques: Étude monocentrique de 31 cas. J. Mal. Vasc. 2016, 41, 26–35. [Google Scholar] [CrossRef]
- Al Hashmi, K.; Al Aamri, L.; Al Lamki, S.; Pathare, A. Portal Vein Thrombosis in Adult Omani Patients: A Retrospective Cohort Study. Oman Med. J. 2017, 32, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Rajani, R.; Björnsson, E.; Bergquist, A.; Danielsson, A.; Gustavsson, A.; Grip, O.; Melin, T.; Sangfelt, P.; Wallerstedt, S.; Almer, S. The Epidemiology and Clinical Features of Portal Vein Thrombosis: A Multicentre Study. Aliment. Pharmacol. Ther. 2010, 32, 1154–1162. [Google Scholar] [CrossRef] [PubMed]
- Acosta, S.; Alhadad, A.; Svensson, P.; Ekberg, O. Epidemiology, Risk and Prognostic Factors in Mesenteric Venous Thrombosis. Br. J. Surg. 2008, 95, 1245–1251. [Google Scholar] [CrossRef]
- Riva, N.; Ageno, W.; Schulman, S.; Beyer-Westendorf, J.; Duce, R.; Malato, A.; Santoro, R.; Poli, D.; Verhamme, P.; Martinelli, I.; et al. Clinical History and Antithrombotic Treatment of Incidentally Detected Splanchnic Vein Thrombosis: A Multicentre, International Prospective Registry. Lancet Haematol. 2016, 3, e267–e275. [Google Scholar] [CrossRef]
- Martin, K. Risk Factors for and Management of MPN-Associated Bleeding and Thrombosis. Curr. Hematol. Malig. Rep. 2017, 12, 389–396. [Google Scholar] [CrossRef] [PubMed]
- De Stefano, V.; Ruggeri, M.; Cervantes, F.; Alvarez-Larrán, A.; Iurlo, A.; Randi, M.L.; Elli, E.; Finazzi, M.C.; Finazzi, G.; Zetterberg, E.; et al. High Rate of Recurrent Venous Thromboembolism in Patients with Myeloproliferative Neoplasms and Effect of Prophylaxis with Vitamin K Antagonists. Leukemia 2016, 30, 2032–2038. [Google Scholar] [CrossRef]
- Smalberg, J.H.; Arends, L.R.; Valla, D.C.; Kiladjian, J.-J.; Janssen, H.L.A.; Leebeek, F.W.G. Myeloproliferative Neoplasms in Budd-Chiari Syndrome and Portal Vein Thrombosis: A Meta-Analysis. Blood 2012, 120, 4921–4928. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Wang, Q.; Luo, B.; Chen, H.; Wang, Z.; Niu, J.; Yuan, J.; Yuan, X.; Bai, W.; He, C.; et al. Prevalence of Prothrombotic Factors in Patients with Budd–Chiari Syndrome or Non-cirrhotic Nonmalignant Portal Vein Thrombosis: A Hospital-based Observational Study. J. Gastroenterol. Hepatol. 2020, 35, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Ageno, W.; Riva, N.; Schulman, S.; Beyer-Westendorf, J.; Bang, S.M.; Senzolo, M.; Grandone, E.; Pasca, S.; Di Minno, M.N.D.; Duce, R.; et al. Long-Term Clinical Outcomes of Splanchnic Vein Thrombosis: Results of an International Registry. JAMA Intern. Med. 2015, 175, 1474–1480. [Google Scholar] [CrossRef] [PubMed]
- Debureaux, P.-E.; Cassinat, B.; Soret-Dulphy, J.; Mora, B.; Verger, E.; Maslah, N.; Plessier, A.; Rautou, P.-E.; Ollivier-Hourman, I.; De Ledinghen, V.; et al. Molecular Profiling and Risk Classification of Patients with Myeloproliferative Neoplasms and Splanchnic Vein Thromboses. Blood Adv. 2020, 4, 3708–3715. [Google Scholar] [CrossRef]
- Lavu, S.; Gangat, N.; Pardanani, A.; Hanson, C.A.; Ketterling, R.P.; Ashrani, A.A.; Kamath, P.S.; Tefferi, A. Splanchnic Vein Thrombosis in Overt Myeloproliferative Neoplasms: The Mayo Clinic Experience with 107 Unselected Consecutive Cases. Blood 2017, 130, 2925. [Google Scholar]
- Kaifie, A.; Kirschner, M.; Wolf, D.; Maintz, C.; Hänel, M.; Gattermann, N.; Gökkurt, E.; Platzbecker, U.; Hollburg, W.; Göthert, J.R.; et al. Bleeding, Thrombosis, and Anticoagulation in Myeloproliferative Neoplasms (MPN): Analysis from the German SAL-MPN-Registry. J. Hematol. Oncol. 2016, 9, 18. [Google Scholar] [CrossRef]
- Lavu, S.; Szuber, N.; Mudireddy, M.; Yogarajah, M.; Gangat, N.; Pardanani, A.; Hanson, C.A.; Ketterling, R.P.; Ashrani, A.A.; Kamath, P.S.; et al. Splanchnic Vein Thrombosis in Patients with Myeloproliferative Neoplasms: The Mayo Clinic Experience with 84 Consecutive Cases. Am. J. Hematol. 2018, 93, E61–E64. [Google Scholar] [CrossRef]
- Vannucchi, A.M.; Barbui, T.; Cervantes, F.; Harrison, C.; Kiladjian, J.-J.; Kröger, N.; Thiele, J.; Buske, C. Philadelphia Chromosome-Negative Chronic Myeloproliferative Neoplasms: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2015, 26, v85–v99. [Google Scholar] [CrossRef] [PubMed]
- De Stefano, V.; Vannucchi, A.M.; Ruggeri, M.; Cervantes, F.; Alvarez-Larrán, A.; Iurlo, A.; Randi, M.L.; Pieri, L.; Rossi, E.; Guglielmelli, P.; et al. Splanchnic Vein Thrombosis in Myeloproliferative Neoplasms: Risk Factors for Recurrences in a Cohort of 181 Patients. Blood Cancer J. 2016, 6, e493. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, D.; Bucelli, C.; Marchetti, A.; Lionetti, M.; Fermo, E.; Bellani, V.; De Magistris, C.; Maeda, A.; Marella, A.; Primignani, M.; et al. Pathological and Genomic Features of Myeloproliferative Neoplasms Associated with Splanchnic Vein Thrombosis in a Single-Center Cohort. Ann. Hematol. 2023, 102, 1409–1420. [Google Scholar] [CrossRef] [PubMed]
- Gianelli, U.; Iurlo, A.; Cattaneo, D.; Bossi, A.; Cortinovis, I.; Augello, C.; Moro, A.; Savi, F.; Castelli, R.; Brambilla, C.; et al. Discrepancies between Bone Marrow Histopathology and Clinical Phenotype in BCR-ABL1-Negative Myeloproliferative Neoplasms Associated with Splanchnic Vein Thrombosis. Leuk. Res. 2015, 39, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Pieri, L.; Paoli, C.; Arena, U.; Marra, F.; Mori, F.; Zucchini, M.; Colagrande, S.; Castellani, A.; Masciulli, A.; Rosti, V.; et al. Safety and Efficacy of Ruxolitinib in Splanchnic Vein Thrombosis Associated with Myeloproliferative Neoplasms. Am. J. Hematol. 2017, 92, 187–195. [Google Scholar] [CrossRef]
- How, J.; Trinkaus, K.M.; Oh, S.T. Distinct Clinical, Laboratory and Molecular Features of Myeloproliferative Neoplasm Patients with Splanchnic Vein Thrombosis. Br. J. Haematol. 2018, 183, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Sant’Antonio, E.; Guglielmelli, P.; Pieri, L.; Primignani, M.; Randi, M.L.; Santarossa, C.; Rumi, E.; Cervantes, F.; Delaini, F.; Carobbio, A.; et al. Splanchnic Vein Thromboses Associated with Myeloproliferative Neoplasms: An International, Retrospective Study on 518 Cases. Am. J. Hematol. 2020, 95, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, D.; Vogel, A.S.; Moshier, E.; Hoffman, R.; Kremyanskaya, M.; Zhou, S.; Schiano, T.; Mascarenhas, J. Outcomes of Splanchnic Vein Thrombosis in Patients with Myeloproliferative Neoplasms in a Single Center Experience. Eur. J. Haematol. 2020, 104, 72–73. [Google Scholar] [CrossRef] [PubMed]
- Görtzen, J.; Hunka, L.M.; Vonnahme, M.; Praktiknjo, M.; Kaifie, A.; Fimmers, R.; Jansen, C.; Heine, A.; Lehmann, J.; Goethert, J.R.; et al. γ-Glutamyl Transferase Is an Independent Biomarker of Splanchnic Thrombosis in Patients With Myeloproliferative Neoplasm. Medicine 2016, 95, e3355. [Google Scholar] [CrossRef] [PubMed]
- Rosti, V.; Bonetti, E.; Bergamaschi, G.; Campanelli, R.; Gattoni, E.; Po, S.L.; Magrini, U.; Massa, M.; Vannucchi, A.; Viarengo, G.; et al. High Frequency of Circulating Endothelial Colony Forming Cells (ECFCs) in Myeloproliferative Neoplasms (MPNs) Is Associated with Diagnosis of Prefibrotic Myelofibrosis, History of Splanchnic Vein Thrombosis, and Vascular Splenomegaly. Blood 2009, 114, 309. [Google Scholar] [CrossRef]
- González-Montero, J.; Del Valle-Batalla, L.; Castillo-Astorga, R.; Marín Valdés, A.; Conte Lanza, G. JAK2V617F Mutation Prevalence on Chilean Adults Suffering from Primary Mesenteric and Portal Venous Thromboses. Int. J. Lab. Hematol. 2020, 42, 331–334. [Google Scholar] [CrossRef]
- Naymagon, L.; Tremblay, D.; Zubizarreta, N.; Moshier, E.; Schiano, T.; Mascarenhas, J. Portal Vein Thrombosis Patients Harboring JAK2V617F Have Poor Long-Term Outcomes despite Anticoagulation. J. Thromb. Thrombolysis 2020, 50, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Ho, W.K.; Hong, F.S. CALR Exon 9 Mutations in Idiopathic Splanchnic Vein Thrombosis in an Australian Cohort. Thromb. Res. 2017, 150, 51–52. [Google Scholar] [CrossRef] [PubMed]
- Poisson, J.; Plessier, A.; Kiladjian, J.-J.; Turon, F.; Cassinat, B.; Andreoli, A.; De Raucourt, E.; Goria, O.; Zekrini, K.; Bureau, C.; et al. Selective Testing for Calreticulin Gene Mutations in Patients with Splanchnic Vein Thrombosis: A Prospective Cohort Study. J. Hepatol. 2017, 67, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Yan, M.; Geyer, H.; Mesa, R.; Atallah, E.; Callum, J.; Bartoszko, J.; Yee, K.; Maganti, M.; Wong, F.; Gupta, V. Clinical Features of Patients with Philadelphia-Negative Myeloproliferative Neoplasms Complicated by Portal Hypertension. Clin. Lymphoma Myeloma Leuk. 2015, 15, e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Colaizzo, D.; Amitrano, L.; Guardascione, M.A.; Tiscia, G.L.; D’Andrea, G.; Longo, V.A.C.; Grandone, E.; Margaglione, M. Outcome of Patients with Splanchnic Venous Thrombosis Presenting without Overt MPN: A Role for the JAK2 V617F Mutation Re-Evaluation. Thromb. Res. 2013, 132, e99–e104. [Google Scholar] [CrossRef] [PubMed]
- Villani, L.; Bergamaschi, G.; Primignani, M.; Rosti, V.; Carolei, A.; Poletto, V.; Catarsi, P.; Spolverini, A.; Vannucchi, A.M.; Barosi, G. JAK2 46/1 Haplotype Predisposes to Splanchnic Vein Thrombosis-Associated BCR-ABL Negative Classic Myeloproliferative Neoplasms. Leuk. Res. 2012, 36, e7–e9. [Google Scholar] [CrossRef]
- Smalberg, J.H.; Koehler, E.; Murad, S.D.; Plessier, A.; Seijo, S.; Trebicka, J.; Primignani, M.; de Maat, M.P.M.; Garcia-Pagan, J.-C.; Valla, D.C.; et al. The JAK2 46/1 Haplotype in Budd-Chiari Syndrome and Portal Vein Thrombosis. Blood 2011, 117, 3968–3973. [Google Scholar] [CrossRef]
- Janssen, H.L.; Wijnhoud, A.; Haagsma, E.B.; van Uum, S.H.; van Nieuwkerk, C.M.; Adang, R.P.; Chamuleau, R.A.; van Hattum, J.; Vleggaar, F.P.; Hansen, B.E.; et al. Extrahepatic Portal Vein Thrombosis: Aetiology and Determinants of Survival. Gut 2001, 49, 720–724. [Google Scholar] [CrossRef] [PubMed]
- Ollivier-Hourmand, I.; Allaire, M.; Goutte, N.; Morello, R.; Chagneau-Derrode, C.; Goria, O.; Dumortier, J.; Cervoni, J.P.; Dharancy, S.; Ganne-Carrié, N.; et al. The Epidemiology of Budd-Chiari Syndrome in France. Dig. Liver Dis. 2018, 50, 931–937. [Google Scholar] [CrossRef]
- Darwish Murad, S.; Plessier, A.; Hernandez-Guerra, M.; Fabris, F.; Eapen, C.E.; Bahr, M.J.; Trebicka, J.; Morard, I.; Lasser, L.; Heller, J.; et al. Etiology, Management, and Outcome of the Budd-Chiari Syndrome. Ann. Intern. Med. 2009, 151, 167–175. [Google Scholar] [CrossRef]
- Ibach, M.; Eurich, D.; Dobrindt, E.; Lurje, G.; Schöning, W.; Öllinger, R.; Pratschke, J.; Globke, B. Orthotopic Liver Transplantation for Budd-Chiari Syndrome: Observations from a 30-Year Liver Transplant Program. Medicina 2021, 57, 821. [Google Scholar] [CrossRef]
- Hoekstra, J.; Bresser, E.L.; Smalberg, J.H.; Spaander, M.C.W.; Leebeek, F.W.G.; Janssen, H.L.A. Long-term Follow-up of Patients with Portal Vein Thrombosis and Myeloproliferative Neoplasms. J. Thromb. Haemost. 2011, 9, 2208–2214. [Google Scholar] [CrossRef] [PubMed]
- Primignani, M.; Martinelli, I.; Bucciarelli, P.; Battaglioli, T.; Reati, R.; Fabris, F.; Dell’Era, A.; Pappalardo, E.; Mannucci, P.M. Risk Factors for Thrombophilia in Extrahepatic Portal Vein Obstruction. Hepatology 2005, 41, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Şahin, E.; Yönal-Hindilerden, İ.; Hindilerden, F.; Aday, A.; Nalçacı, M. The Impact of JAK2V617F Mutation on Philadelphia-Negative Myeloproliferative Neoplasms. Turk. J. Med. Sci. 2022, 52, 150–165. [Google Scholar] [CrossRef]
- Marin Oyarzún, C.P.; Heller, P.G. Platelets as Mediators of Thromboinflammation in Chronic Myeloproliferative Neoplasms. Front. Immunol. 2019, 10, 1373. [Google Scholar] [CrossRef] [PubMed]
- Marin Oyarzún, C.P.; Carestia, A.; Lev, P.R.; Glembotsky, A.C.; Castro Ríos, M.A.; Moiraghi, B.; Molinas, F.C.; Marta, R.F.; Schattner, M.; Heller, P.G. Neutrophil Extracellular Trap Formation and Circulating Nucleosomes in Patients with Chronic Myeloproliferative Neoplasms. Sci. Rep. 2016, 6, 38738. [Google Scholar] [CrossRef]
- Wolach, O.; Sellar, R.S.; Martinod, K.; Cherpokova, D.; McConkey, M.; Chappell, R.J.; Silver, A.J.; Adams, D.; Castellano, C.A.; Schneider, R.K.; et al. Increased Neutrophil Extracellular Trap Formation Promotes Thrombosis in Myeloproliferative Neoplasms. Sci. Transl. Med. 2018, 10, eaan8292. [Google Scholar] [CrossRef] [PubMed]
- Edelmann, B.; Gupta, N.; Schnoeder, T.M.; Oelschlegel, A.M.; Shahzad, K.; Goldschmidt, J.; Philipsen, L.; Weinert, S.; Ghosh, A.; Saalfeld, F.C.; et al. JAK2-V617F Promotes Venous Thrombosis through Β1/Β2 Integrin Activation. J. Clin. Invest. 2018, 128, 4359–4371. [Google Scholar] [CrossRef]
- Gupta, N.; Edelmann, B.; Schnoeder, T.M.; Saalfeld, F.C.; Wolleschak, D.; Kliche, S.; Schraven, B.; Heidel, F.H.; Fischer, T. JAK2-V617F Activates Β1-Integrin-Mediated Adhesion of Granulocytes to Vascular Cell Adhesion Molecule 1. Leukemia 2017, 31, 1223–1226. [Google Scholar] [CrossRef]
- Guadall, A.; Lesteven, E.; Letort, G.; Awan Toor, S.; Delord, M.; Pognant, D.; Brusson, M.; Verger, E.; Maslah, N.; Giraudier, S.; et al. Endothelial Cells Harbouring the JAK2V617F Mutation Display Pro-Adherent and Pro-Thrombotic Features. Thromb. Haemost. 2018, 118, 1586–1599. [Google Scholar] [CrossRef]
- Matsuura, S.; Thompson, C.R.; Belghasem, M.E.; Bekendam, R.H.; Piasecki, A.; Leiva, O.; Ray, A.; Italiano, J.; Yang, M.; Merill-Skoloff, G.; et al. Platelet Dysfunction and Thrombosis in JAK2V617F-Mutated Primary Myelofibrotic Mice. Arter. Thromb. Vasc. Biol. 2020, 40, e262–e272. [Google Scholar] [CrossRef]
- Li, J.; Spensberger, D.; Ahn, J.S.; Anand, S.; Beer, P.A.; Ghevaert, C.; Chen, E.; Forrai, A.; Scott, L.M.; Ferreira, R.; et al. JAK2 V617F Impairs Hematopoietic Stem Cell Function in a Conditional Knock-in Mouse Model of JAK2 V617F-Positive Essential Thrombocythemia. Blood 2010, 116, 1528–1538. [Google Scholar] [CrossRef] [PubMed]
- Malara, A.; Gruppi, C.; Massa, M.; Tira, M.E.; Rosti, V.; Balduini, A.; Barosi, G. Elevated Plasma EDA Fibronectin in Primary Myelofibrosis Is Determined by High Allele Burden of JAK2V617F Mutation and Strongly Predicts Splenomegaly Progression. Front. Oncol. 2022, 12, 987643. [Google Scholar] [CrossRef]
- Alvarez-Larrán, A.; Arellano-Rodrigo, E.; Reverter, J.C.; Domingo, A.; Villamor, N.; Colomer, D.; Cervantes, F. Increased Platelet, Leukocyte, and Coagulation Activation in Primary Myelofibrosis. Ann. Hematol. 2008, 87, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Qi, J.; Zhao, S.; Shen, W.; Dai, L.; Han, W.; Huang, M.; Wang, Z.; Ruan, C.; Wu, D.; et al. Clinical Significance of Circulating Microparticles in Ph− Myeloproliferative Neoplasms. Oncol. Lett. 2017, 14, 2531–2536. [Google Scholar] [CrossRef]
- Giordano, G.; Napolitano, M.; Cellurale, M.; Di Carlo, P.; Musuraca, G.; Micucci, G.; Lucchesi, A. Circulating Endothelial Cell Levels Correlate with Treatment Outcomes of Splanchnic Vein Thrombosis in Patients with Chronic Myeloproliferative Neoplasms. J. Pers. Med. 2022, 12, 364. [Google Scholar] [CrossRef] [PubMed]
- Teofili, L.; Martini, M.; Iachininoto, M.G.; Capodimonti, S.; Nuzzolo, E.R.; Torti, L.; Cenci, T.; Larocca, L.M.; Leone, G. Endothelial Progenitor Cells Are Clonal and Exhibit the JAK2V617F Mutation in a Subset of Thrombotic Patients with Ph-Negative Myeloproliferative Neoplasms. Blood 2011, 117, 2700–2707. [Google Scholar] [CrossRef]
- How, J.; Zhou, A.; Oh, S.T. Splanchnic Vein Thrombosis in Myeloproliferative Neoplasms: Pathophysiology and Molecular Mechanisms of Disease. Ther. Adv. Hematol. 2017, 8, 107–118. [Google Scholar] [CrossRef]
- Barbui, T.; Finazzi, G.; Carobbio, A.; Thiele, J.; Passamonti, F.; Rumi, E.; Ruggeri, M.; Rodeghiero, F.; Randi, M.L.; Bertozzi, I.; et al. Development and Validation of an International Prognostic Score of Thrombosis in World Health Organization-Essential Thrombocythemia (IPSET-Thrombosis). Blood 2012, 120, 5128–5133, quiz 5252. [Google Scholar] [CrossRef]
- Hernández-Boluda, J.-C.; Pastor-Galán, I.; Arellano-Rodrigo, E.; Raya, J.-M.; Pérez-Encinas, M.; Ayala, R.; Ferrer-Marín, F.; Velez, P.; Mora, E.; Fox, M.-L.; et al. Predictors of Thrombosis and Bleeding in 1613 Myelofibrosis Patients from the Spanish Registry of Myelofibrosis. Br. J. Haematol. 2022, 199, 529–538. [Google Scholar] [CrossRef]
- Lindgren, M.; Andréasson, B.; Samuelsson, J.; Pettersson, H.; Enblom-Larsson, A.; Ravn-Landtblom, A.; Scheding, S.; Bentham, C.; Ahlstrand, E. Survival and Risk of Vascular Complications in Myelofibrosis—A Population-Based Study from the Swedish MPN Group. Eur. J. Haematol. 2022, 109, 336–342. [Google Scholar] [CrossRef]
- Barbui, T.; Ghirardi, A.; Carobbio, A.; Masciulli, A.; Carioli, G.; Rambaldi, A.; Finazzi, M.C.; Bellini, M.; Rumi, E.; Vanni, D.; et al. Increased Risk of Thrombosis in JAK2 V617F-Positive Patients with Primary Myelofibrosis and Interaction of the Mutation with the IPSS Score. Blood Cancer J. 2022, 12, 156. [Google Scholar] [CrossRef] [PubMed]
- Barbui, T.; De Stefano, V.; Falanga, A.; Finazzi, G.; Martinelli, I.; Rodeghiero, F.; Vannucchi, A.M.; Barosi, G. Addressing and Proposing Solutions for Unmet Clinical Needs in the Management of Myeloproliferative Neoplasm-Associated Thrombosis: A Consensus-Based Position Paper. Blood Cancer J. 2019, 9, 61. [Google Scholar] [CrossRef] [PubMed]
- Kuo, M.-C.; Chuang, W.-Y.; Chang, H.; Lin, T.-H.; Wu, J.-H.; Lin, T.-L.; Ou, C.-W.; Hung, Y.-S.; Huang, T.-Y.; Huang, Y.-J.; et al. Comparison of Clinical and Molecular Features Between Patients With Essential Thrombocythemia and Early/Prefibrotic Primary Myelofibrosis Presenting With Thrombocytosis in Taiwan. Am. J. Clin. Pathol. 2023, 159, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Baiges, A.; Procopet, B.; Silva-Junior, G.; Llop, E.; Tellez, L.; Darnell, A.; Garcia-Criado, Á.; Turon, F.; Nicoara-Farcau, O.; González-Alayón, C.; et al. Incidence and Factors Predictive of Recurrent Thrombosis in People with Non-Cirrhotic Portal Vein Thrombosis. J. Hepatol. 2023, 78, 114–122. [Google Scholar] [CrossRef]
- Levraut, M.; Legros, L.; Drappier, C.; Béné, M.C.; Queyrel, V.; Raynaud, S.; Martis, N. Low Prevalence of JAK2 V617F Mutation in Patients with Thrombosis and Normal Blood Counts: A Retrospective Impact Study. J. Thromb. Thrombolysis 2020, 50, 995–1003. [Google Scholar] [CrossRef]
- Karakose, S.; Oruc, N.; Zengin, M.; Akarca, U.S.; Ersoz, G. Diagnostic Value of the JAK2 V617F Mutation for Latent Chronic Myeloproliferative Disorders in Patients with Budd-Chiari Syndrome and/or Portal Vein Thrombosis. Turk. J. Gastroenterol. 2015, 26, 42–48. [Google Scholar] [CrossRef]
- Barbui, T.; Carobbio, A.; Cervantes, F.; Vannucchi, A.M.; Guglielmelli, P.; Antonioli, E.; Alvarez-Larrán, A.; Rambaldi, A.; Finazzi, G.; Barosi, G. Thrombosis in Primary Myelofibrosis: Incidence and Risk Factors. Blood 2010, 115, 778–782. [Google Scholar] [CrossRef]
- Magaz, M.; Alvarez-Larrán, A.; Colomer, D.; López-Guerra, M.; García-Criado, M.Á.; Mezzano, G.; Belmonte, E.; Olivas, P.; Soy, G.; Cervantes, F.; et al. Next-Generation Sequencing in the Diagnosis of Non-Cirrhotic Splanchnic Vein Thrombosis. J. Hepatol. 2021, 74, 89–95. [Google Scholar] [CrossRef]
- Tremblay, D.; Winters, A.; Beckman, J.D.; Naymagon, L.; Patel, R.; Mascarenhas, J.; Schiano, T.D. Splanchnic Vein Thrombosis Associated with Myeloproliferative Neoplasms. Thromb. Res. 2022, 218, 8–16. [Google Scholar] [CrossRef]
- Carrà, G.; Giugliano, E.; Camerlo, S.; Rosati, G.; Branca, E.; Maffeo, B.; Russo, I.; Piazza, R.; Cilloni, D.; Morotti, A. Clonal Hematopoiesis by DNMT3A Mutations as a Common Finding in Idiopathic Splanchnic Vein Thrombosis. Haematologica 2023, 108, 1447–1449. [Google Scholar] [CrossRef]
- Finazzi, G.; De Stefano, V.; Barbui, T. Splanchnic Vein Thrombosis in Myeloproliferative Neoplasms: Treatment Algorithm 2018. Blood Cancer J. 2018, 8, 64. [Google Scholar] [CrossRef] [PubMed]
- Franchis, R.d.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Abraldes, J.G.; Albillos, A.; Baiges, A.; Bajaj, J.; Bañares, R.; et al. Baveno VII—Renewing Consensus in Portal Hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef]
- Shukla, A.; Shreshtha, A.; Mukund, A.; Bihari, C.; Eapen, C.E.; Han, G.; Deshmukh, H.; Cua, I.H.Y.; Lesmana, C.R.A.; Al Meshtab, M.; et al. Budd-Chiari Syndrome: Consensus Guidance of the Asian Pacific Association for the Study of the Liver (APASL). Hepatol. Int. 2021, 15, 531–567. [Google Scholar] [CrossRef]
- Rössle, M.; Bettinger, D.; Trebicka, J.; Klinger, C.; Praktiknjo, M.; Sturm, L.; Caca, K.; Mücke, V.T.; Radecke, K.; Engelmann, C.; et al. A Prospective, Multicentre Study in Acute Non-Cirrhotic, Non-Malignant Portal Vein Thrombosis: Comparison of Medical and Interventional Treatment. Aliment. Pharmacol. Ther. 2020, 52, 329–339. [Google Scholar] [CrossRef]
- Barbui, T.; De Stefano, V.; Carobbio, A.; Iurlo, A.; Alvarez-Larran, A.; Cuevas, B.; Ferrer Marín, F.; Vannucchi, A.M.; Palandri, F.; Harrison, C.; et al. Direct Oral Anticoagulants for Myeloproliferative Neoplasms: Results from an International Study on 442 Patients. Leukemia 2021, 35, 2989–2993. [Google Scholar] [CrossRef]
- Sekhar, M. Prevention and Management of Thrombosis in Myeloproliferative Neoplasms. Clin. Adv. Hematol. Oncol. 2017, 15, 178–181. [Google Scholar] [PubMed]
- Tefferi, A.; Barrett, S.M.; Silverstein, M.N.; Nagorney, D.M. Outcome of Portal-Systemic Shunt Surgery for Portal Hypertension Associated with Intrahepatic Obstruction in Patients with Agnogenic Myeloid Metaplasia. Am. J. Hematol. 1994, 46, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Potthoff, A.; Attia, D.; Pischke, S.; Mederacke, I.; Beutel, G.; Rifai, K.; Deterding, K.; Heiringhoff, K.; Klempnauer, J.; Strassburg, C.P.; et al. Long-Term Outcome of Liver Transplant Patients with Budd-Chiari Syndrome Secondary to Myeloproliferative Neoplasms. Liver Int. 2015, 35, 2042–2049. [Google Scholar] [CrossRef]
- Guy, A.; Gourdou-Latyszenok, V.; Lay, N.L.; Peghaire, C.; Kilani, B.; Dias, J.V.; Duplaa, C.; Renault, M.-A.; Denis, C.; Villeval, J.L.; et al. Vascular Endothelial Cell Expression of JAK2V617F Is Sufficient to Promote a Pro-Thrombotic State Due to Increased P-Selectin Expression. Haematologica 2019, 104, 70–81. [Google Scholar] [CrossRef]
- Mora, B.; Guglielmelli, P.; Kuykendall, A.; Rumi, E.; Maffioli, M.; Palandri, F.; De Stefano, V.; Caramella, M.; Salmoiraghi, S.; Kiladjian, J.-J.; et al. Prediction of Thrombosis in Post-Polycythemia Vera and Post-Essential Thrombocythemia Myelofibrosis: A Study on 1258 Patients. Leukemia 2022, 36, 2453–2460. [Google Scholar] [CrossRef]
- De Stefano, V.; Rossi, E.; Carobbio, A.; Ghirardi, A.; Betti, S.; Finazzi, G.; Vannucchi, A.M.; Barbui, T. Hydroxyurea Prevents Arterial and Late Venous Thrombotic Recurrences in Patients with Myeloproliferative Neoplasms but Fails in the Splanchnic Venous District. Pooled Analysis of 1500 Cases. Blood Cancer J. 2018, 8, 112. [Google Scholar] [CrossRef] [PubMed]
- Samuelson, B.T.; Vesely, S.K.; Chai-Adisaksopha, C.; Scott, B.L.; Crowther, M.; Garcia, D. The Impact of Ruxolitinib on Thrombosis in Patients with Polycythemia Vera and Myelofibrosis: A Meta-Analysis. Blood Coagul. Fibrinolysis 2016, 27, 648–652. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | All MPN-SVT, n (100%) | PV, n (%) | ET, n (%) | MF, n (%) | MPNu, n (%) | |
|---|---|---|---|---|---|---|
| De Stefano et al. [30] | 181 | 67 (37) | 67 (37) | 47 (26) | NA | |
| Kaifie et al. [27] | 22 | 3 (13.63) | 6 (27.3) | 6 (27.3) | primary | 3 |
| 4 (18.2) | post-PV | |||||
| Lavu et al. [28] | 84 | 29 (35) | 26 (30) | 29 (35) | NA | |
| How et al. [34] | 52 | 21 (41) | 17 (33) | 7 (13) | 7 (13) | |
| Sant’Antonio et al. [35] | 518 | 192 (37) | 178 (34.3) | 68 (13) | primary | 55 (11) |
| 20 (3.9) | prePMF | |||||
| 4 (0.7) | post-PV | |||||
| 1 (0.1) | post-ET | |||||
| Tremblay et al. [36] | 64 | 29 (45) | 14 (22) | 8 (13) | primary | 6 (9) |
| 2 (3) | prePMF | |||||
| 5 (8) | post-ET/PV | |||||
| Debureaux et al. [25] | 80 | 52 (65) | 23 (29) | 5 (6) | NA | |
| Görtzen et al. [37] | 33 | 7 (21) | 6 (18) | 13 (40) | 7 (21) | |
| Gianelli et al. [32] | 29 | 11 (37.9) | 6 (20.6) | 11 (37.9) | 1 (3.4) | |
| Cattaneo et al. [31] | 58 | 9 (15.5) | 8 (13.8) | 4 (6.9) | primary | |
| 16 (27.6) | prePMF | 16 (27.5) | ||||
| 5 (8.6) | secondary | |||||
| Rosti et al. [38] | 214 | 38 (17.7) | 21 (9.8) | 106 (49.5) | primary | NA |
| 49 (22.8) | prePMF | |||||
| Gonzales-Montero et al. [39] | 26 | 5 (19.2) | 12 (46.1) | 4 (15.3) | ||
| Naymagon et al. [40] | 23 | 8 (34.7) | 11 (47.8) | 2 (8.7) | 2 (8.7) | |
| Fan et al. [23] | 126 | 23 (18.2) | 50 (39.6) | 15 (12) | 38 (30) | |
| Ho et al. [41] | 26 | 11 (42) | 8 (30.7) | 2 (7.7) | primary | 3 (11.5) |
| 2 (7.7) | prePMF | |||||
| Pieri et al. [33] | 21 | 5 (23.8) | 4 (19) | 8 (38.1) | primary | NA |
| 3 (14.3) | post-PV | |||||
| 1 (4.8) | post-ET | |||||
| Poisson et al. [42] | 74 | 32 (43.2) | 23 (31) | 6 (8.1) | 13 (17.5) | |
| Yan et al. [43] | 28 | 17 (60.7) | 2 (7) | 9 (32.1) | NA | |
| Colaizzo et al. [44] | 28 | 9 (32.1) | 7 (25) | 12 (42.8) | NA | |
| Villani et al. [45] | 108 | NA | 32 (29.6) | 29 (26.8) | primary | 21 (19.4) |
| 26 (24) | prePMF | |||||
| Smalberg et al. [46] | 66 | 27 (41) | 17 (25.8) | 6 (9) | 16 (24.2) | |
| Janssen et al. [47] | 23 | 12 (52.1) | 3 (13) | 6 (26) | 2 (8.6) | |
| Ollivier-Hourmand et al. [48] ω | 72 | 44 (61) | 20 (27.7) | 1 (1.3) | 7 (9.7) | |
| Darwish Murad et al. [49] ω | 49 (100) | 27 (55) | 9 (18.3) | 2 (4) | 11 (22.4) | |
| Ibach et al. [50] ω | 22 (100) | 5 (22) | 9 (46) | 1 (5) | 7 (31) | |
| Hoekstra et al. [51] Δ | 44 (100) | 14 (31.8) | 12 (27.2) | 7 (15.9) | 11 (25) | |
| Primignani et al. [52] Δ | 23 (100) | 3 (13) | 14 (60.8) | 2 (8.7) | 4 (17.3) | |
| Sahin et al. [53] | 32 (100) | 11 (34.3) | 12 (37.5) | 9 (28.1) | NA | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beleva, E.A. Splanchnic Vein Thrombosis in Myelofibrosis—An Underappreciated Hallmark of Disease Phenotype. Int. J. Mol. Sci. 2023, 24, 15717. https://doi.org/10.3390/ijms242115717
Beleva EA. Splanchnic Vein Thrombosis in Myelofibrosis—An Underappreciated Hallmark of Disease Phenotype. International Journal of Molecular Sciences. 2023; 24(21):15717. https://doi.org/10.3390/ijms242115717
Chicago/Turabian StyleBeleva, Elina A. 2023. "Splanchnic Vein Thrombosis in Myelofibrosis—An Underappreciated Hallmark of Disease Phenotype" International Journal of Molecular Sciences 24, no. 21: 15717. https://doi.org/10.3390/ijms242115717