
The Impact of Abnormal Lipid Metabolism on the Occurrence Risk of Idiopathic Pulmonary Arterial Hypertension
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Population Characteristics
2.2. Differences in Lipid Content between IPAH Patients and Healthy Controls
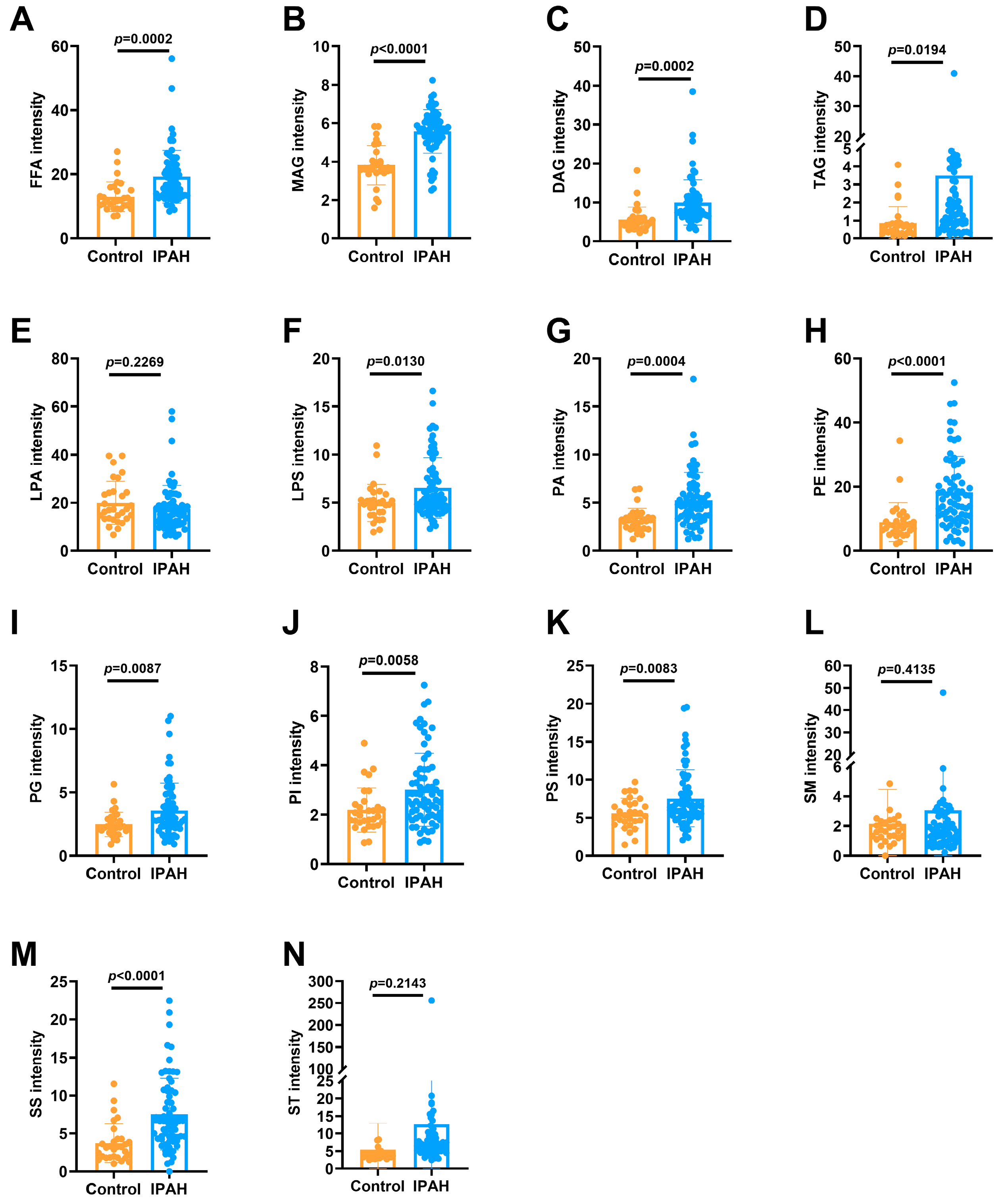
2.2.1. The 14 Lipid Subclasses in IPAH Patients and Healthy Controls
2.2.2. Levels of the 14 Lipid Subclasses in IPAH Patients and Healthy Controls
2.3. Levels of Lipid Subclasses and FFA between Males and Females
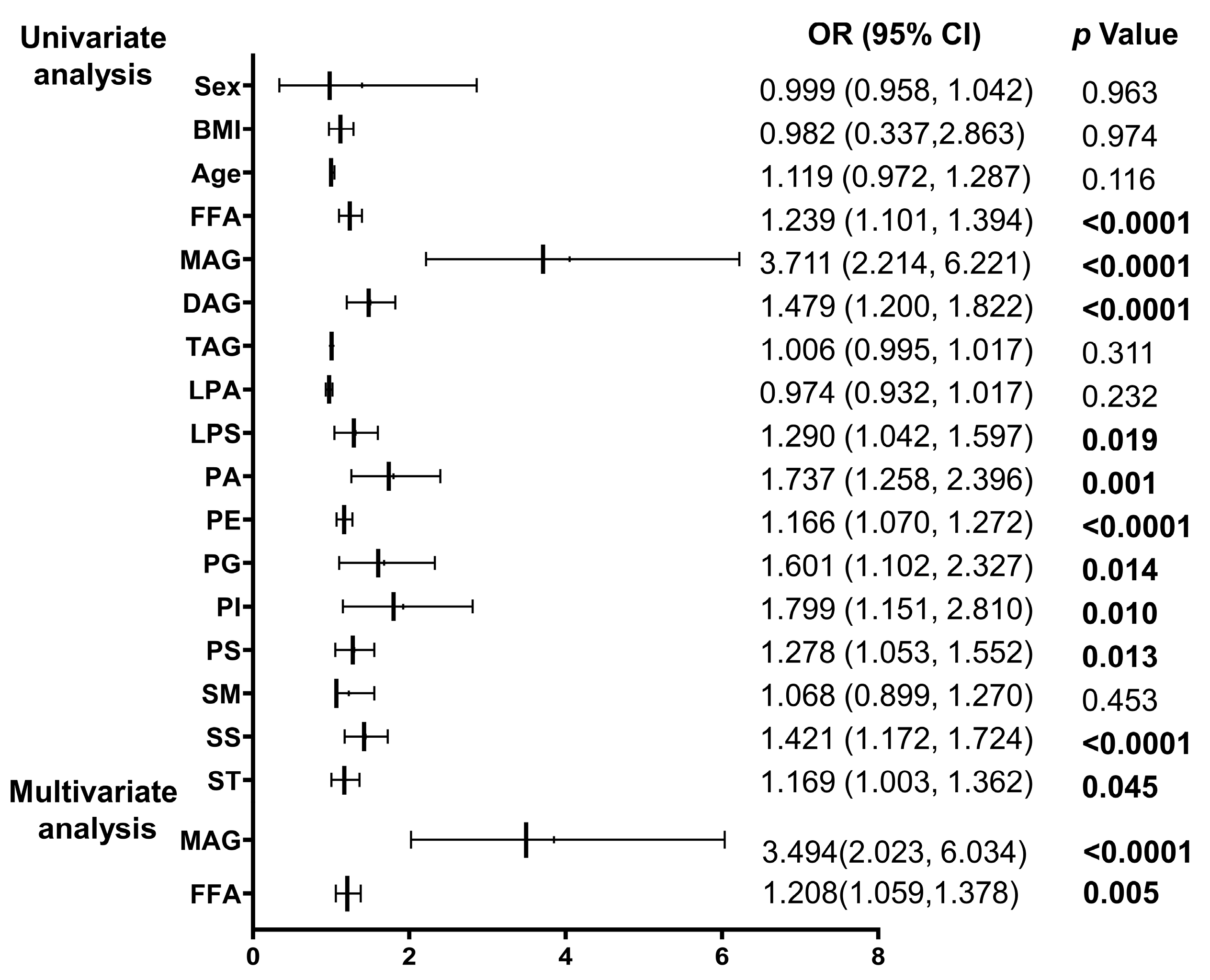
2.4. Logistic Regression Analysis of IPAH Occurrence of Different Types of Lipids
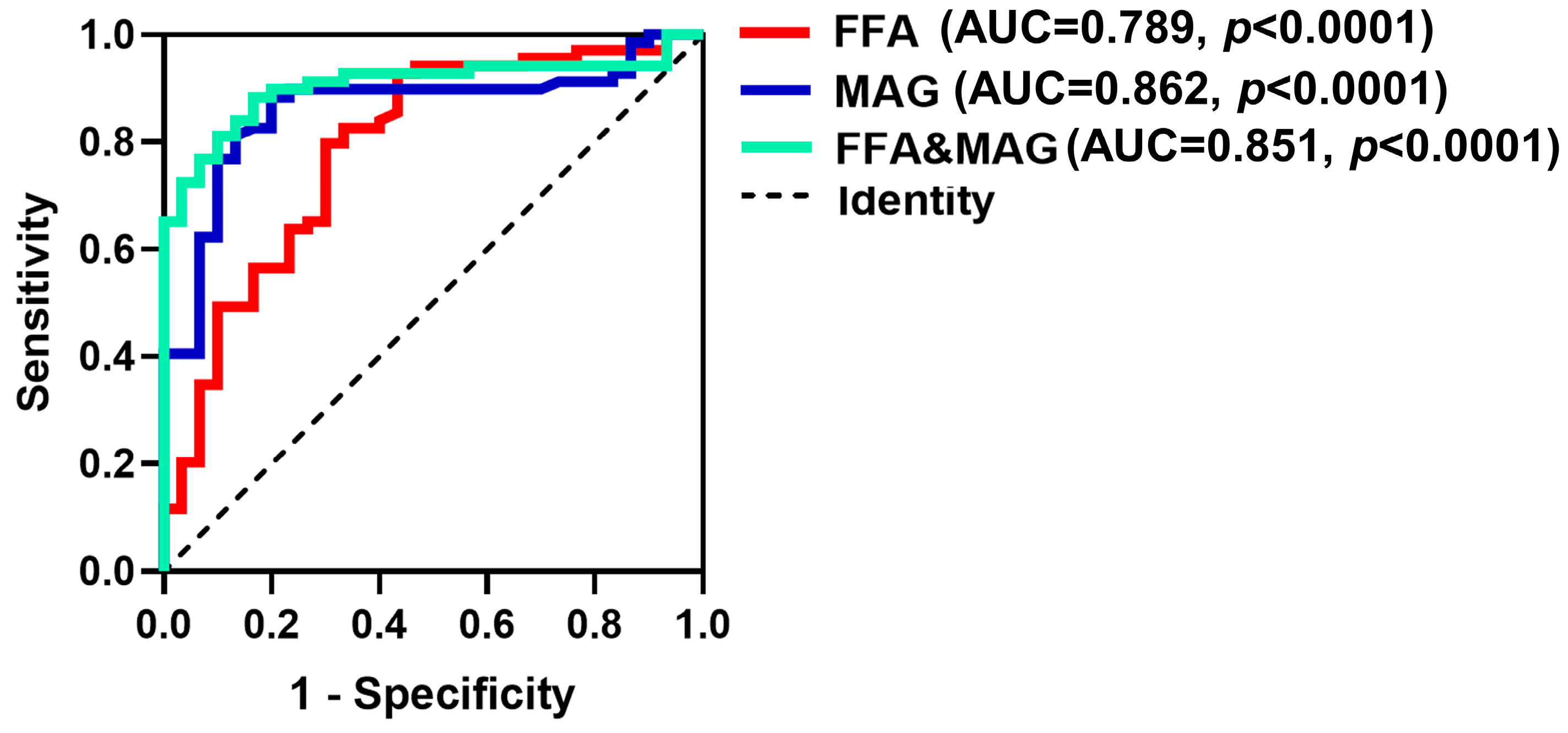
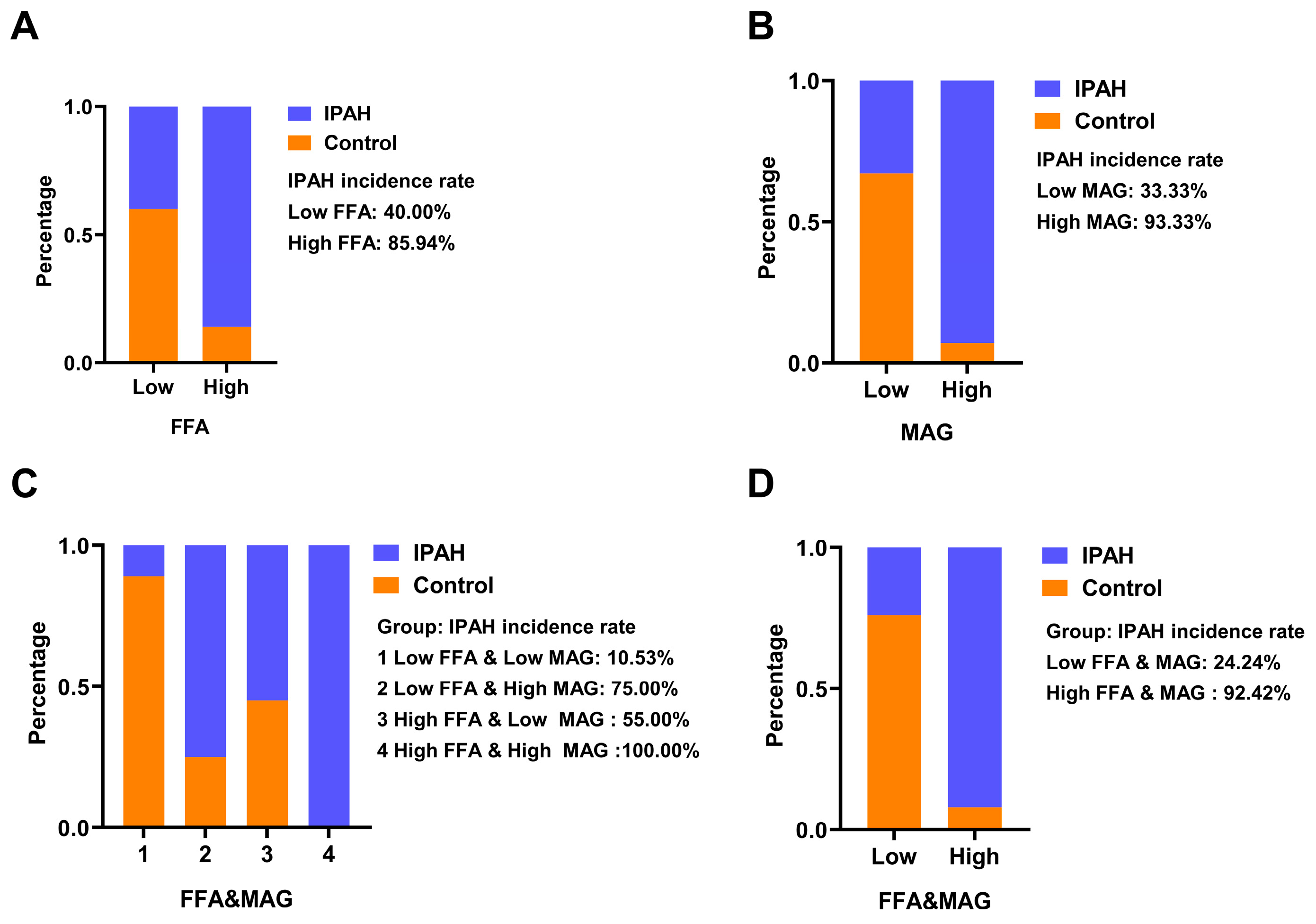
2.5. ROC Analysis of FFA, MAG and Their Combined Detection to Predict IPAH
3. Discussion
4. Materials and Methods
4.1. Study Design and Subjects
4.2. Clinical Data Collection
4.3. Blood Sample Collection
4.4. GC–MS Analysis
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef] [PubMed]
- Ruaro, B.; Salton, F.; Baratella, E.; Confalonieri, P.; Geri, P.; Pozzan, R.; Torregiani, C.; Bulla, R.; Confalonieri, M.; Matucci-Cerinic, M.; et al. An Overview of Different Techniques for Improving the Treatment of Pulmonary Hypertension Secondary in Systemic Sclerosis Patients. Diagnostics 2022, 12, 616. [Google Scholar] [CrossRef]
- Novoyatleva, T. Pulmonary Hypertension: New Insights and Recent Advances from Basic Science to Translational Approaches. Int. J. Mol. Sci. 2023, 24, 8462. [Google Scholar] [CrossRef] [PubMed]
- Tynan, T.; Hird, K.; Hannon, T.; Gabbay, E. Pulmonary arterial hypertension outcomes upon endothelin-1 receptor antagonist switch to macitentan. J. Int. Med. Res. 2019, 47, 2177–2186. [Google Scholar] [CrossRef]
- Pahal, P.; Sharma, S. Idiopathic Pulmonary Artery Hypertension; StatPearls Publishing LLC: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Omura, J.; Habbout, K.; Shimauchi, T.; Wu, W.H.; Breuils-Bonnet, S.; Tremblay, E.; Martineau, S.; Nadeau, V.; Gagnon, K.; Mazoyer, F.; et al. Identification of Long Noncoding RNA H19 as a New Biomarker and Therapeutic Target in Right Ventricular Failure in Pulmonary Arterial Hypertension. Circulation 2020, 142, 1464–1484. [Google Scholar] [CrossRef]
- Mahley, R.W.; Innerarity, T.L.; Rall, S.C.; Weisgraber, K.H. Plasma lipoproteins: Apolipoprotein structure and function. J. Lipid. Res. 1984, 25, 1277–1294. [Google Scholar] [CrossRef] [PubMed]
- Gallart-Ayala, H.; Teav, T.; Ivanisevic, J. Metabolomics meets lipidomics: Assessing the small molecule component of metabolism. BioEssays 2020, 42, e2000052. [Google Scholar] [CrossRef]
- Han, X. Lipidomics for studying metabolism. Nat. Rev. Endocrinol. 2016, 12, 668–679. [Google Scholar] [CrossRef]
- Illingworth, D.R. Lipoprotein Metabolism. Am. J. Kidney Dis. 1993, 22, 90–97. [Google Scholar] [CrossRef]
- Busatto, S.; Walker, S.A.; Grayson, W.; Pham, A.; Tian, M.; Nesto, N.; Barklund, J.; Wolfram, J. Lipoprotein-based drug delivery. Adv. Drug Deliv. Rev. 2020, 159, 377–390. [Google Scholar] [CrossRef]
- Chen, J.; Rathinasabapathy, A.; Luo, J.; Yang, X.; Luo, P.; Chen, Y.; Li, Z.; Li, J. Differential serum lipid distribution in IPAH and CHD-PAH patients. Respir. Med. 2021, 191, 106711. [Google Scholar] [CrossRef] [PubMed]
- Jonas, K.; Waligóra, M.; Magoń, W.; Zdrojewski, T.; Stokwiszewski, J.; Płazak, W.; Podolec, P.; Kopeć, G. Prognostic role of traditional cardiovascular risk factors in patients with idiopathic pulmonary arterial hypertension. Arch. Med. Sci. 2019, 15, 1397–1406. [Google Scholar] [CrossRef] [PubMed]
- Jonas, K.; Kurzyna, M.; Mroczek, E.; Chrzanowski, Ł.; Mularek-Kubzdela, T.; Skoczylas, I.; Błaszczak, P.; Grześk, G.; Mizia-Stec, K.; Kuśmierczyk, B.; et al. Impact of diabetes mellitus on disease severity and patient survival in idiopathic pulmonary arterial hypertension: Data from the Polish multicentre registry (BNP-PL). Cardiovasc. Diabetol. 2023, 22, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.H.; Peng, F.H.; Wei, H.; He, J.; Chen, F.D.; Di, R.M.; Jiang, X.; Jiang, R.; Chen, Y.J.; Heresi, G.A.; et al. Serum High-Density Lipoprotein Cholesterol Levels as a Prognostic Indicator in Patients with Idiopathic Pulmonary Arterial Hypertension. Am. J. Cardiol. 2012, 110, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Wu, J.H.Y. Omega-3 Fatty Acids and Cardiovascular Disease: Effects on risk factors, molecular pathways, and clinical events. J. Am. Coll. Cardiol. 2011, 58, 2047–2067. [Google Scholar] [CrossRef]
- Liu, J.; Zhao, M.; Zhu, Y.; Wang, X.; Zheng, L.; Yin, Y. LC–MS-Based Metabolomics and Lipidomics Study of High-Density-Lipoprotein-Modulated Glucose Metabolism with an apoA-I Knockout Mouse Model. J. Proteome Res. 2018, 18, 48–56. [Google Scholar] [CrossRef]
- Ge, X.; Zhu, T.; Zhang, X.; Liu, Y.; Wang, Y.; Zhang, W. Gender differences in pulmonary arterial hypertension patients with BMPR2 mutation: A meta-analysis. Respir. Res. 2020, 21, 1–10. [Google Scholar] [CrossRef]
- Umar, S.; Cunningham, C.M.; Itoh, Y.; Moazeni, S.; Vaillancourt, M.; Sarji, S.; Centala, A.; Arnold, A.P.; Eghbali, M. The Y Chromosome Plays a Protective Role in Experimental Hypoxic Pulmonary Hypertension. Am. J. Respir. Crit. Care Med. 2018, 197, 952–955. [Google Scholar] [CrossRef]
- Cunningham, C.M.; Li, M.; Ruffenach, G.; Doshi, M.; Aryan, L.; Hong, J.; Park, J.; Hrncir, H.; Medzikovic, L.; Umar, S.; et al. Y-Chromosome Gene, Uty, Protects Against Pulmonary Hypertension by Reducing Proinflammatory Chemokines. Am. J. Respir. Crit. Care Med. 2022, 206, 186–196. [Google Scholar] [CrossRef]
- Jia, W.B.; Jiang, X.; Zuo, X.R.; He, J.; Zhao, Q.H.; Jiang, R.; Jing, Z.C. Clinical characteristics of 161 Chinese patients with idiopathic pulmonary arterial. Zhonghua Xin Xue Guan Bing Za Zhi 2012, 40, 652–656. [Google Scholar]
- Strange, G.; Gabbay, E.; Kermeen, F.; Williams, T.; Carrington, M.; Stewart, S.; Keogh, A. Time from Symptoms to Definitive Diagnosis of Idiopathic Pulmonary Arterial Hypertension: The Delay Study. Pulm. Circ. 2013, 3, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.; Crowley, J.; O’Shea, P.; McEvoy, J.W.; Griffin, D.G. Lipid reference values in an Irish population. Ir. J. Med. Sci. 2021, 190, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Magkos, F.; Mittendorfer, B. Sex Differences in Lipid and Lipoprotein Metabolism: It’s Not Just about Sex Hormones. J. Clin. Endocrinol. Metab. 2011, 96, 885–893. [Google Scholar] [CrossRef]
- Wu, R.R.; Zhao, J.P.; Zhai, J.G.; Guo, X.F.; Guo, W.B. Sex difference in effects of typical and atypical anti-psychotics on glucose-insulin homeostasis and lipid metabolism in first-episode schizophrenia. J. Clin. Psychopharmacol. 2007, 27, 374–379. [Google Scholar] [CrossRef]
- Ambrož, M.; de Vries, S.T.; Vart, P.; Dullaart, R.P.F.; van Lennep, J.R.; Denig, P.; Hoogenberg, K. Sex Differences in Lipid Profile across the Life Span in Patients with Type 2 Diabetes: A Primary Care-Based Study. J. Clin. Med. 2021, 10, 1775. [Google Scholar] [CrossRef] [PubMed]
- Zelt, J.G.; Chaudhary, K.R.; Cadete, V.J.; Mielniczuk, L.M.; Stewart, D.J. Medical Therapy for Heart Failure Associated with Pulmonary Hypertension. Circ. Res. 2019, 124, 1551–1567. [Google Scholar] [CrossRef]
- Duflot, T.; Tu, L.; Leuillier, M.; Messaoudi, H.; Groussard, D.; Feugray, G.; Azhar, S.; Thuillet, R.; Bauer, F.; Humbert, M. Preventing the Increase in Lysophosphatidic Acids: A New Therapeutic Target in Pulmonary Hypertension? Metabolites 2021, 11, 784. [Google Scholar] [CrossRef]
- Brittain, E.L.; Talati, M.; Fessel, J.P.; Zhu, H.; Penner, N.; Calcutt, M.W.; West, J.D.; Funke, M.; Lewis, G.D.; Gerszten, R.E.; et al. Fatty Acid Metabolic Defects and Right Ventricular Lipotoxicity in Human Pulmonary Arterial Hypertension. Circulation 2016, 133, 1936–1944. [Google Scholar] [CrossRef]
- Hemnes, A.R.; Luther, J.M.; Rhodes, C.J.; Burgess, J.P.; Carlson, J.; Fan, R.; Fessel, J.P.; Fortune, N.; Gerszten, R.E.; Halliday, S.J.; et al. Human PAH is characterized by a pattern of lipid-related insulin resistance. J. Clin. Investig. 2019, 4, e123611. [Google Scholar] [CrossRef]
- Huai, X.; Sun, Y.; Sun, X.; Wu, W.; Wang, L.; Jiang, R.; Gong, S.; Li, J.; Miao, Y.; Yuan, P.; et al. The effect of docosahexaenoic acid on predicting the survival of patients with idiopathic pulmonary arterial hypertension. Ann. Transl. Med. 2021, 9, 995. [Google Scholar] [CrossRef]
- Cnop, M.; Hannaert, J.C.; Hoorens, A.; Eizirik, D.L.; Pipeleers, D.G. Inverse Relationship Between Cytotoxicity of Free Fatty Acids in Pancreatic Islet Cells and Cellular Triglyceride Accumulation. Diabetes 2001, 50, 1771–1777. [Google Scholar] [CrossRef] [PubMed]
- Nickel, N.P.; Yuan, K.; Dorfmuller, P.; Provencher, S.; Lai, Y.C.; Bonnet, S.; Austin, E.D.; Koch, C.D.; Morris, A.; Perros, F.; et al. Beyond the Lungs: Systemic Manifestations of Pulmonary Arterial Hypertension. Am. J. Respir. Crit. Care Med. 2020, 201, 148–157. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Control (n = 30) | IPAH (n = 69) | p Value |
|---|---|---|---|
| Age, years | 36.5 ± 10.7 | 36.4 ± 10.0 | 0.149 |
| Female, n (%) | 24 (80.0) | 55 (79.7) | 0.611 |
| BMI, kg/m2 | 21.6 ± 2.7 | 22.8 ± 3.4 | 0.458 |
| WHO-FC III/IV (%) | N/A | 41 (59.4) | N/A |
| 6MWD, m | N/A | 393.9 ± 104.8 | N/A |
| Death, n (%) | N/A | 9 (13) | N/A |
| Hemodynamics | |||
| mRAP, mmHg | N/A | 3.5 (1.0–6.0) | N/A |
| mPAP, mmHg | N/A | 55.0 (49.0–62.5) | N/A |
| mPAWP, mmHg | N/A | 6.0 (3.0–8.0) | N/A |
| PVR, wood units | N/A | 11.7 ± 6.0 | N/A |
| CO, L/min | N/A | 4.2 (3.5–5.2) | N/A |
| CI, L/min/m2 | N/A | 2.6 (2.2–3.7) | N/A |
| Laboratory | |||
| NT-proBNP, pg/mL | N/A | 1019.9 ± 926.3 | N/A |
| TBIL, µmol/L | N/A | 15.0 (11.0–20.4) | N/A |
| DBIL, µmol/L | N/A | 5.0 (4.0–7.4) | N/A |
| UA, mg/dL | N/A | 410.1 ± 116.8 | N/A |
| CR, µmol/L | N/A | 63.3 ± 13.0 | N/A |
| GLU, mmol/L | N/A | 4.8 (4.4–5.1) | N/A |
| TC, mmol/L | N/A | 4.0 ± 1.0 | N/A |
| TG, mmol/L | N/A | 1.4 ± 0.7 | N/A |
| HDL, mmol/L | N/A | 1.0 ± 0.3 | N/A |
| LDL, mmol/L | N/A | 2.4 (2.0–3.1) | N/A |
| HGB, g/L | N/A | 141.8 ± 18.6 | N/A |
| RBC, 1012/L | N/A | 4.8 ± 0.6 | N/A |
| WBC, 109/L | N/A | 6.2 (5.3–7.7) | N/A |
| Specific therapy | |||
| PDE-5 inhibitors | N/A | 15 (21.7) | N/A |
| ERAs | N/A | 6 (8.7) | N/A |
| Prostacyclin analogs | N/A | 0 (0) | N/A |
| Combination | N/A | 41 (59.4) | N/A |
| Non-specific medication | N/A | 7 (10.1) | N/A |
| Lipid Intensity | Control (n = 30) | p Value | IPAH (n = 69) | p Value | ||
|---|---|---|---|---|---|---|
| Male (n = 6) | Female (n = 24) | Male (n = 14) | Female (n = 55) | |||
| FFA | 12.0 ± 2.3 | 13.3 ± 5.0 | 0.553 | 18.4 ± 7.1 * | 19.5 ± 8.5 # | 0.650 |
| MAG | 4.0 ± 0.8 | 3.8 ± 1.0 | 0.690 | 5.6 ± 0.9 * | 5.6 ± 1.2 # | 0.954 |
| DAG | 4.7 ± 2.6 | 5.8 ± 3.4 | 0.450 | 10.4± 5.9 * | 9.9 ± 5.8 # | 0.766 |
| TAG | 7.6 ± 8.3 | 23.5 ± 72.8 | 0.603 | 25.1 ± 23.7 * | 37.6 ± 66.5 | 0.492 |
| LPA | 21.2 ± 8.2 | 19.7 ± 9.3 | 0.717 | 15.4 ± 6.4 | 18.0 ± 10.4 | 0.381 |
| LPS | 4.8 ± 1.8 | 5.0 ± 2.0 | 0.852 | 7.1 ± 3.7 | 6.4 ± 3.0 # | 0.456 |
| PA | 2.8 ± 0.7 | 3.3 ± 1.3 | 0.335 | 4.8 ± 2.4 * | 5.4 ± 73.0 # | 0.482 |
| PE | 6.3 ± 2.4 | 9.7 ± 6.6 | 0.223 | 15.9 ± 8.7 * | 18.8 ± 11.8 # | 0.386 |
| PG | 2.4 ± 0.7 | 2.5 ± 1.0 | 0.780 | 2.9 ± 1.5 | 3.7 ± 2.3 # | 0.214 |
| PI | 2.6 ± 1.0 | 2.1 ± 0.9 | 0.272 | 2.4 ± 0.9 | 3.2 ± 1.6 # | 0.089 |
| PS | 6.1 ± 2.0 | 5.5 ± 2.0 | 0.511 | 6.2 ± 2.3 | 7.9 ± 4.0 # | 0.121 |
| SM | 1.6 ± 0.7 | 2.3 ± 2.6 | 0.550 | 1.7 ± 1.1 | 3.4 ± 6.6 | 0.346 |
| SS | 2.2 ± 0.8 | 4.1 ± 2.7 | 0.113 | 7.2 ± 4.3 * | 7.6± 4.8 # | 0.728 |
| St | 3.9 ± 1.3 | 5.8 ± 8.3 | 0.590 | 6.9 ± 2.4 * | 14.1 ± 34.8 | 0.444 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, Y.; Zhao, H.; Kalionis, B.; Huai, X.; Hu, X.; Wu, W.; Jiang, R.; Gong, S.; Wang, L.; Liu, J.; et al. The Impact of Abnormal Lipid Metabolism on the Occurrence Risk of Idiopathic Pulmonary Arterial Hypertension. Int. J. Mol. Sci. 2023, 24, 14280. https://doi.org/10.3390/ijms241814280
Wei Y, Zhao H, Kalionis B, Huai X, Hu X, Wu W, Jiang R, Gong S, Wang L, Liu J, et al. The Impact of Abnormal Lipid Metabolism on the Occurrence Risk of Idiopathic Pulmonary Arterial Hypertension. International Journal of Molecular Sciences. 2023; 24(18):14280. https://doi.org/10.3390/ijms241814280
Chicago/Turabian StyleWei, Yaqin, Hui Zhao, Bill Kalionis, Xu Huai, Xiaoyi Hu, Wenhui Wu, Rong Jiang, Sugang Gong, Lan Wang, Jinming Liu, and et al. 2023. "The Impact of Abnormal Lipid Metabolism on the Occurrence Risk of Idiopathic Pulmonary Arterial Hypertension" International Journal of Molecular Sciences 24, no. 18: 14280. https://doi.org/10.3390/ijms241814280