
Antioxidant Genetic Variants Modify Echocardiography Indices in Long COVID
 , , , , , ,
, , , , , ,  , and
, and
Abstract
:1. Introduction
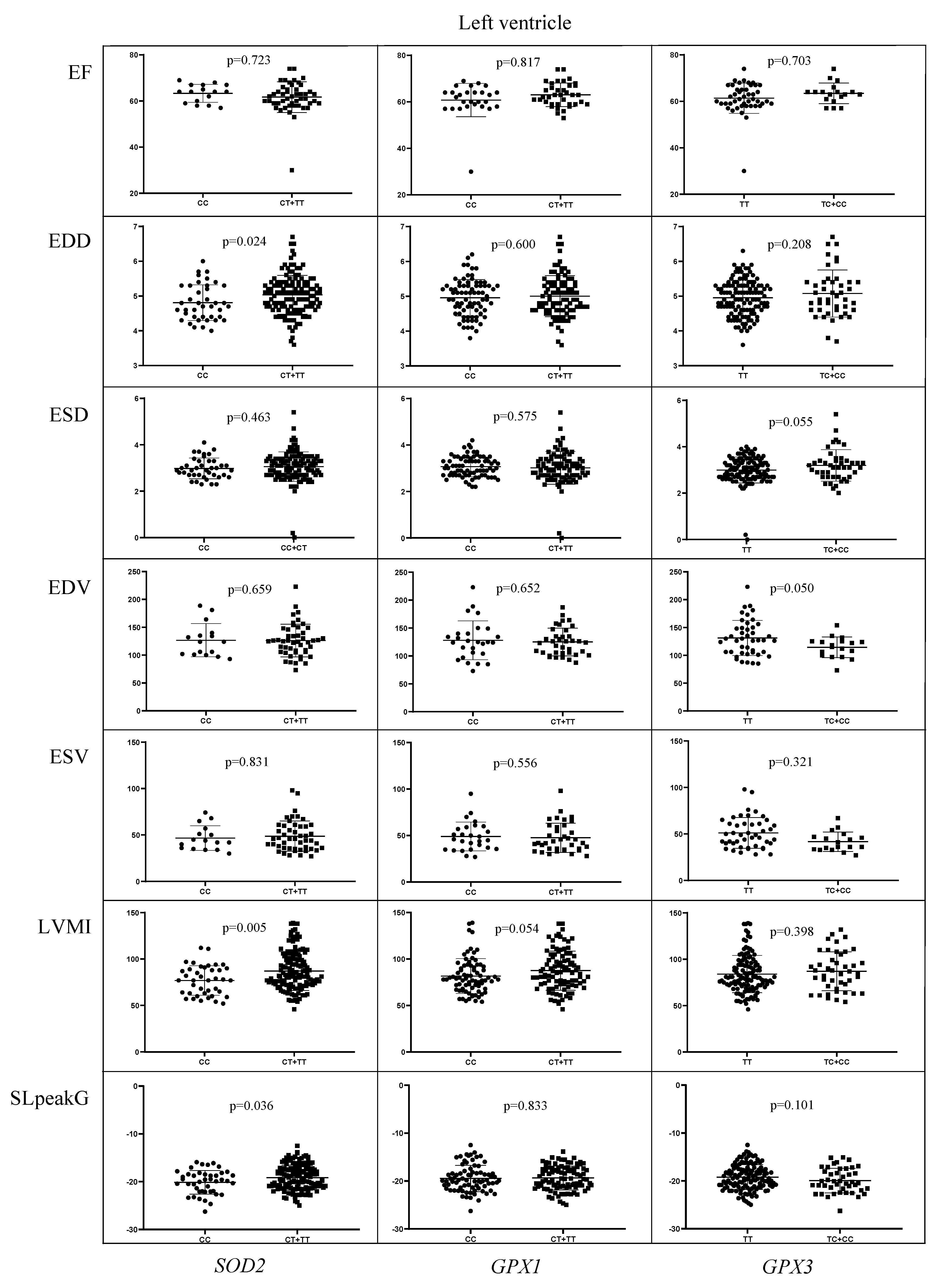
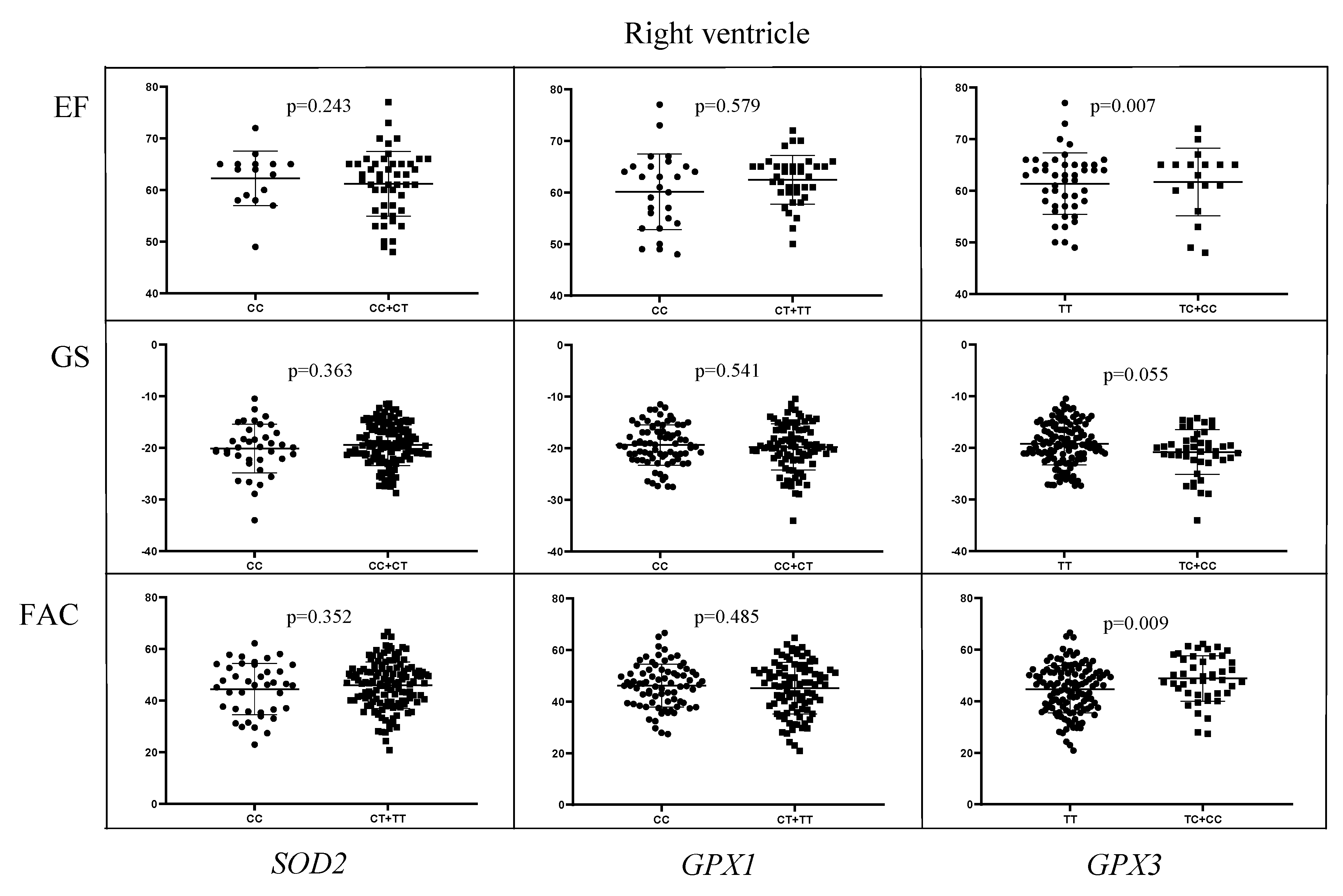
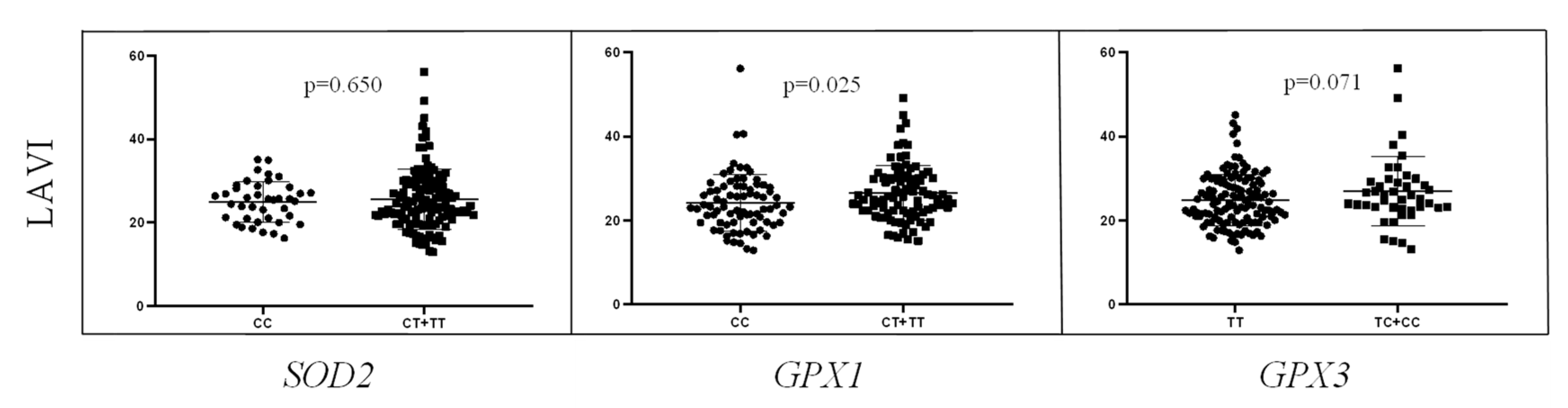
2. Results
3. Discussion
4. Materials and Methods
4.1. Patients and Study Design
4.2. Echocardiographic Examination
4.3. Cardiac Magnetic Resonance Data Acquisition and Postprocessing
4.4. Genotyping
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Basso, C.; Leone, O.; Rizzo, S.; De Gaspari, M.; Van Der Wal, A.C.; Aubry, M.-C.; Bois, M.C.; Lin, P.T.; Maleszewski, J.J.; Stone, J.R. Pathological features of COVID-19-associated myocardial injury: A multicentre cardiovascular pathology study. Eur. Heart J. 2020, 41, 3827–3835. [Google Scholar] [CrossRef] [PubMed]
- Kuck, K.H. Arrhythmias and sudden cardiac death in the COVID-19 pandemic. Herz 2020, 45, 325–326. [Google Scholar] [CrossRef]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.C.; et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat. Med. 2022, 28, 410–422. [Google Scholar] [CrossRef]
- Bhatla, A.; Mayer, M.M.; Adusumalli, S.; Hyman, M.C.; Oh, E.; Tierney, A.; Moss, J.; Chahal, A.A.; Anesi, G.; Denduluri, S.; et al. COVID-19 and cardiac arrhythmias. Heart Rhythm. 2020, 17, 1439–1444. [Google Scholar] [CrossRef]
- Muhamad, S.A.; Ugusman, A.; Kumar, J.; Skiba, D.; Hamid, A.A.; Aminuddin, A. COVID-19 and Hypertension: The What, the Why, and the How. Front. Physiol. 2021, 12, 665064. [Google Scholar] [CrossRef]
- Argenziano, M.G.; Bruce, S.L.; Slater, C.L.; Tiao, J.R.; Baldwin, M.R.; Barr, R.G.; Chang, B.P.; Chau, K.H.; Choi, J.J.; Gavin, N.; et al. Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: Retrospective case series. BMJ 2020, 369, m1996. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 26, m1091. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.H.; Zhao, L.; Yang, X.C.; Wang, P. Cardiovascular complications of SARS-CoV-2 infection (COVID-19): A systematic review and meta-analysis. Rev. Cardiovasc. Med. 2021, 22, 159–165. [Google Scholar] [CrossRef]
- Roh, J.D.; Kitchen, R.R.; Guseh, J.S.; McNeill, J.N.; Aid, M.; Martinot, A.J.; Yu, A.; Platt, C.; Rhee, J.; Weber, B.; et al. Plasma Proteomics of COVID-19–Associated Cardiovascular Complications. JACC Basic Transl. Sci. 2022, 7, 425–441. [Google Scholar] [CrossRef] [PubMed]
- Lala, A.; Johnson, K.W.; Januzzi, J.L.; Russak, A.J.; Paranjpe, I.; Richter, F.; Zhao, S.; Somani, S.; Van Vleck, T.; Vaid, A.; et al. Prevalence and Impact of Myocardial Injury in Patients Hospitalized With COVID-19 Infection. J. Am. Coll. Cardiol. 2020, 76, 533–546. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus Disease (COVID-19) Dashboard [Internet]. Available online: https://covid19.who.int/ (accessed on 13 June 2023).
- Bilaloglu, S.; Aphinyanaphongs, Y.; Jones, S.; Iturrate, E.; Hochman, J.; Berger, J.S. Thrombosis in Hospitalized Patients With COVID-19 in a New York City Health System. JAMA 2020, 324, 799. [Google Scholar] [CrossRef]
- McKee, C.M.; Coll, R.C. NLRP3 inflammasome priming: A riddle wrapped in a mystery inside an enigma. J. Leukoc. Biol. 2020, 108, 937–952. [Google Scholar] [CrossRef]
- Magadum, A.; Kishore, R. Cardiovascular Manifestations of COVID-19 Infection. Cells 2020, 9, 2508. [Google Scholar] [CrossRef]
- Iqubal, A.; Iqubal, M.K.; Hoda, F.; Najmi, A.K.; Haque, S.E. COVID-19 and cardiovascular complications: An update from the underlying mechanism to consequences and possible clinical intervention. Expert Rev. Anti-Infect. Ther. 2021, 19, 1083–1092. [Google Scholar] [CrossRef] [PubMed]
- Mullard, A. NLRP3 inhibitors stoke anti-inflammatory ambitions. Nat. Rev. Drug Discov. 2019, 18, 405–407. [Google Scholar] [CrossRef] [PubMed]
- Zaccone, G.; Tomasoni, D.; Italia, L.; Lombardi, C.M.; Metra, M. Myocardial Involvement in COVID-19: An Interaction Between Comorbidities and Heart Failure with Preserved Ejection Fraction. A Further Indication of the Role of Inflammation. Curr. Heart Fail. Rep. 2021, 18, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Ercegovac, M.; Asanin, M.; Savic-Radojevic, A.; Ranin, J.; Matic, M.; Djukic, T.; Coric, V.; Jerotic, D.; Todorovic, N.; Milosevic, I.; et al. Antioxidant Genetic Profile Modifies Probability of Developing Neurological Sequelae in Long-COVID. Antioxidants 2022, 11, 954. [Google Scholar] [CrossRef] [PubMed]
- Marzec, J.M.; Christie, J.D.; Reddy, S.P.; Jedlicka, A.E.; Vuong, H.; Lanken, P.N.; Aplenc, R.; Yamamoto, T.; Yamamoto, M.; Cho, H.-Y.; et al. Functional polymorphisms in the transcription factor NRF2 in humans increase the risk of acute lung injury. FASEB J. 2007, 21, 2237–2246. [Google Scholar] [CrossRef]
- Sutton, A.; Khoury, H.; Prip-Buus, C.; Cepanec, C.; Pessayre, D.; Degoul, F. The Ala16Val genetic dimorphism modulates the import of human manganese superoxide dismutase into rat liver mitochondria. Pharmacogenetics 2003, 13, 145–157. [Google Scholar] [CrossRef]
- Sutton, A.; Imbert, A.; Igoudjil, A.; Descatoire, V.; Cazanave, S.; Pessayre, D.; Degoul, F. The manganese superoxide dismutase Ala16Val dimorphism modulates both mitochondrial import and mRNA stability. Pharm. Genom. 2005, 15, 311–319. [Google Scholar] [CrossRef]
- Crawford, A.; Fassett, R.G.; Geraghty, D.P.; Kunde, D.A.; Ball, M.J.; Robertson, I.K.; Coombes, J.S. Relationships between single nucleotide polymorphisms of antioxidant enzymes and disease. Gene 2012, 501, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Voetsch, B.; Jin, R.C.; Bierl, C.; Benke, K.S.; Kenet, G.; Simioni, P.; Ottaviano, F.; Damasceno, B.P.; Annichino-Bizacchi, J.M.; Handy, D.E.; et al. Promoter Polymorphisms in the Plasma Glutathione Peroxidase (GPx-3) Gene: A Novel Risk Factor for Arterial Ischemic Stroke Among Young Adults and Children. Stroke 2007, 38, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Jerotic, D.; Ranin, J.; Bukumiric, Z.; Djukic, T.; Coric, V.; Savic-Radojevic, A.; Todorovic, N.; Asanin, M.; Ercegovac, M.; Milosevic, I.; et al. SOD2 rs4880 and GPX1 rs1050450 polymorphisms do not confer risk of COVID-19, but influence inflammation or coagulation parameters in Serbian cohort. Redox Rep. 2022, 27, 85–91. [Google Scholar] [CrossRef]
- Luchian, M.L.; Motoc, A.; Lochy, S.; Magne, J.; Belsack, D.; De Mey, J.; Roosens, B.; Van den Bussche, K.; Boeckstaens, S.; Chameleva, H.; et al. Subclinical Myocardial Dysfunction in Patients with Persistent Dyspnea One Year after COVID-19. Diagnostics 2021, 12, 57. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Xu, E.; Benjamin, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]
- Crudo, V.L.; Ahmed, A.I.; Cowan, E.L.; Shah, D.J.; Al-Mallah, M.H.; Malahfji, M. Acute and Subclinical Myocardial Injury in COVID-19. Methodist DeBakey Cardiovasc. J. 2021, 217, 22–30. [Google Scholar] [CrossRef]
- Krishna, H.; Ryu, A.J.; Scott, C.G.; Mandale, D.R.; Naqvi, T.Z.; Pellikka, P.A. Cardiac Abnormalities in COVID-19 and Relationship to Outcome. Mayo Clin. Proc. 2021, 96, 932–942. [Google Scholar] [CrossRef]
- Rahman, I. Antioxidant therapeutic advances in COPD. Ther. Adv. Respir. Dis. 2008, 2, 351–374. [Google Scholar] [CrossRef] [Green Version]
- Montano, M.A.E.; da Cruz, I.; Duarte, M.M.M.F.; Krewer, C.D.C.; Rocha, M.I.D.U.M.D.; Mânica-Cattani, M.F.; Soares, F.; Rosa, G.; Maris, A.F.; Battiston, F.G.; et al. Inflammatory cytokines in vitro production are associated with Ala16Val superoxide dismutase gene polymorphism of peripheral blood mononuclear cells. Cytokine 2012, 60, 30–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte, T.; da Cruz, I.B.M.; Barbisan, F.; Capelleto, D.; Moresco, R.N.; Duarte, M.M.M.F. The effects of rosuvastatin on lipid-lowering, inflammatory, antioxidant and fibrinolytics blood biomarkers are influenced by Val16Ala superoxide dismutase manganese-dependent gene polymorphism. Pharm. J. 2016, 16, 501–506. [Google Scholar] [CrossRef]
- Shuvalova, Y.A.; Kaminnyi, A.I.; Meshkov, A.N.; Shirokov, R.O.; Samko, A.N. Association between polymorphisms of eNOS and GPx-1 genes, activity of free-radical processes and in-stent restenosis. Mol. Cell Biochem. 2012, 370, 241–249. [Google Scholar] [CrossRef]
- Karlsson, J.O.G.; Jynge, P.; Ignarro, L.J. May Mangafodipir or Other SOD Mimetics Contribute to Better Care in COVID-19 Patients? Antioxidants 2020, 9, 971. [Google Scholar] [CrossRef]
- Lee, S.; Lee, E.-K.; Kang, D.H.; Lee, J.; Hong, S.H.; Jeong, W.; Kang, S.W. Glutathione peroxidase-1 regulates ASK1-dependent apoptosis via interaction with TRAF2 in RIPK3-negative cancer cells. Exp. Mol. Med. 2021, 53, 1080–1091. [Google Scholar] [CrossRef]
- Baroncini, L.A.V.; Borges, L.J.L.; Camarozano, A.C.; De Carmo, D.C.; Darwich, R.Z.; Fortunato Junior, J.A. Echocardiographic Correlation between Right Ventricular Function and Left Atrial Volume. Arquivos Brasileiros de Cardiologia [Internet]. 2019. [cited 11 July 2022]. Available online: https://www.scielo.br/scielo.php?script=sci_arttext&pid=S0066-782X2019000300249 (accessed on 13 June 2023).
- Wood, G.; Kirkevang, T.S.; Agergaard, J.; Leth, S.; Hansen, E.S.S.; Laustsen, C.; Larsen, A.H.; Jensen, H.K.; Østergaard, L.J.; Bøtker, H.E.; et al. Cardiac Performance and Cardiopulmonary Fitness After Infection With SARS-CoV-2. Front. Cardiovasc. Med. 2022, 9, 871603. [Google Scholar] [CrossRef]
- Muhammad, Y.; Kani, Y.A.; Iliya, S.; Muhammad, J.B.; Binji, A.; Ahmad, A.E.-F.; Kabir, M.B.; Bindawa, K.U.; Ahmed, A. Deficiency of antioxidants and increased oxidative stress in COVID-19 patients: A cross-sectional comparative study in Jigawa, Northwestern Nigeria. SAGE Open Med. 2021, 9, 205031212199124. [Google Scholar] [CrossRef] [PubMed]
- Seale, L.A.; Torres, D.J.; Berry, M.J.; Pitts, M.W. A role for selenium-dependent GPX1 in SARS-CoV-2 virulence. Am. J. Clin. Nutr. 2020, 112, 447–448. [Google Scholar] [CrossRef] [PubMed]
- Anttila, S.; Hirvonen, A.; Vainio, H.; Husgafvel-Pursiainen, K.; Hayes, J.D.; Ketterer, B. Immunohistochemical localization of glutathione S-transferases in human lung. Cancer Res. 1993, 53, 5643–5648. [Google Scholar] [PubMed]
- Rowe, J.D.; Nieves, E.; Listowsky, I. Subunit diversity and tissue distribution of human glutathione S-transferases: Interpretations based on electrospray ionization-MS and peptide sequence-specific antisera. Biochem. J. 1997, 325 Pt 2, 481–486. [Google Scholar] [CrossRef] [Green Version]
- Saha, S.; Buttari, B.; Panieri, E.; Profumo, E.; Saso, L. An Overview of Nrf2 Signaling Pathway and Its Role in Inflammation. Molecules 2020, 25, 5474. [Google Scholar] [CrossRef]
- Thimmulappa, R.K.; Mai, K.H.; Srisuma, S.; Kensler, T.W.; Yamamoto, M.; Biswal, S. Identification of Nrf2-regulated genes induced by the chemopreventive agent sulforaphane by oligonucleotide microarray. Cancer Res. 2002, 62, 5196–5203. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Multimodality imaging in patients with heart failure and preserved ejection fraction: An expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2022, 23, e34–e61. [Google Scholar]
- Voigt, J.U.; Mălăescu, G.G.; Haugaa, K.; Badano, L. How to do LA strain. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265. [Google Scholar] [CrossRef]
- Chen, B.-H.; Shi, N.-N.; Wu, C.-W.; An, D.-A.; Shi, Y.-X.; Wesemann, L.D.; Hu, J.; Xu, J.-R.; Shan, F.; Wu, L.-M. Early cardiac involvement in patients with acute COVID-19 infection identified by multiparametric cardiovascular magnetic resonance imaging. Eur. Heart J.—Cardiovasc. Imaging 2021, 22, 844–851. [Google Scholar] [CrossRef]
- Kotecha, T.; Knight, D.S.; Razvi, Y.; Kumar, K.; Vimalesvaran, K.; Thornton, G.; Patel, R.; Chacko, L.; Brown, J.T.; Coyle, C.; et al. Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur. Heart J. 2021, 42, 1866–1878. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Characteristics | Cardiac Characteristics | ||
|---|---|---|---|
| Age (years) a | 55.65 ± 12.33 | ||
| Gender, n (%) | Arrhythmia, n (%) b | ||
| Male | 103 (59.2) | No | 153 (87.9) |
| Female | 71 (40.8) | Yes | 21 (12.1) |
| Hypertension, n (%) b | Dyspnea, n (%) b | ||
| No | 95 (54.5) | No | 128 (73.6) |
| Yes | 79 (45.5) | Yes | 46 (26.4) |
| Obesity, n (%) b | Blood pressure (mmHg) a | ||
| BMI < 30 | 114 (65.5) | Systolic | 128.32 ± 19.47 |
| BMI > 30 | 60 (34.5) | Diastolic | 78.52 ± 11.15 |
| Smoking, n (%) b | hs-cTnT (ng/L) c | 7 (3–130) | |
| Never | 86 (48.9) | ||
| Former | 60 (34.1) | ||
| Ever | 17 (9.7) | ||
| Diabetes, n (%) b | |||
| No | 147 (84.5) | BNP (pg/mL) c | 18 (0–358) |
| Yes | 27 (15.5) | ||
| Hospitalization, n (%) b | |||
| No | 31 (17.8) | ||
| Yes | 143 (82.2) | ||
| Pneumonia, n (%) b | D-dimer (mg/L) c | 0.34 (0.17–3.39) | |
| No | 24 (13.8) | ||
| Yes | 150 (86.2) | ||
| O2 support, n (%) b | CRP (mg/L) c | 1.55 (0.6–44.6) | |
| No | 110 (63.2) | ||
| Yes | 64 (36.8) | ||
| Genotypes | |||
| SOD2 rs4880, n (%) b | |||
| CC | 40 (23.1) | ||
| CT + TT | 133 (76.9) | ||
| GPX1 rs1050450, n (%) b | |||
| CC | 77 (44.8) | ||
| CT + TT | 95 (55.2) | ||
| GPX3 rs8177412, n (%) b | |||
| TT | 128 (74.4) | ||
| TC + CC | 44 (25.6) | ||
| Nrf2 rs6721961, n (%) b | |||
| CC | 128 (74.9) | ||
| CA + AA | 43 (25.1) | ||
| Left Ventricle | |
| End-diastolic volume (EDV, mL) a | 126.34 ± 28.93 |
| End-diastolic volume index (EDVI, mL/m2) a | 64.15 ± 12.94 |
| End-systolic volume (ESV, mL) a | 48.38 ± 15.45 |
| End-systolic volume index (ESVI, mL/m2) a | 24.08 ± 6.57 |
| EF (%) a | 61.98 ± 6.07 |
| Right ventricle | |
| End-diastolic volume (EDV, mL) a | 125.30 ± 33.20 |
| End-diastolic volume index (EDVI, mL/m2) a | 63.00 ± 14.47 |
| End-systolic volume (ESV, mL) a | 49.03 ± 16.92 |
| End-systolic volume index (ESVI, mL/m2) a | 25.05 ± 7.07 |
| EF (%) a | 61.57 ± 6.03 |
| T1 mapping | |
| Pre-contrast (ms) a | 1028.28 ± 108.58 |
| Increased T1 pre-contrast values (%) | 20.0 |
| Postcontrast (ms) a | 452.59 ± 96.69 |
| Increased T1 postcontrast values (%) | 23.1 |
| ECV (%) a | 22.9 ± 4.9 |
| T2 mapping | |
| Pre-contrast (ms) a | 48.08 ± 7.00 |
| Increased T2 pre-contrast values (%) b | 18.8 |
| Postcontrast (ms) a | 54.59 ± 6.66 |
| Increased T2 postcontrast values (%) b | 14.3 |
| LGE | |
| Pathological findings (%) b | 44.4 |
| T2w | |
| Pathological findings (%) b | 5.7 |
| Pericardial | |
| Pathological findings (%) b | 12.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asanin, M.; Ercegovac, M.; Krljanac, G.; Djukic, T.; Coric, V.; Jerotic, D.; Pljesa-Ercegovac, M.; Matic, M.; Milosevic, I.; Viduljevic, M.; et al. Antioxidant Genetic Variants Modify Echocardiography Indices in Long COVID. Int. J. Mol. Sci. 2023, 24, 10234. https://doi.org/10.3390/ijms241210234
Asanin M, Ercegovac M, Krljanac G, Djukic T, Coric V, Jerotic D, Pljesa-Ercegovac M, Matic M, Milosevic I, Viduljevic M, et al. Antioxidant Genetic Variants Modify Echocardiography Indices in Long COVID. International Journal of Molecular Sciences. 2023; 24(12):10234. https://doi.org/10.3390/ijms241210234
Chicago/Turabian StyleAsanin, Milika, Marko Ercegovac, Gordana Krljanac, Tatjana Djukic, Vesna Coric, Djurdja Jerotic, Marija Pljesa-Ercegovac, Marija Matic, Ivana Milosevic, Mihajlo Viduljevic, and et al. 2023. "Antioxidant Genetic Variants Modify Echocardiography Indices in Long COVID" International Journal of Molecular Sciences 24, no. 12: 10234. https://doi.org/10.3390/ijms241210234