

Preliminary Study on the Effect of a Night Shift on Blood Pressure and Clock Gene Expression
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Population Characteristics
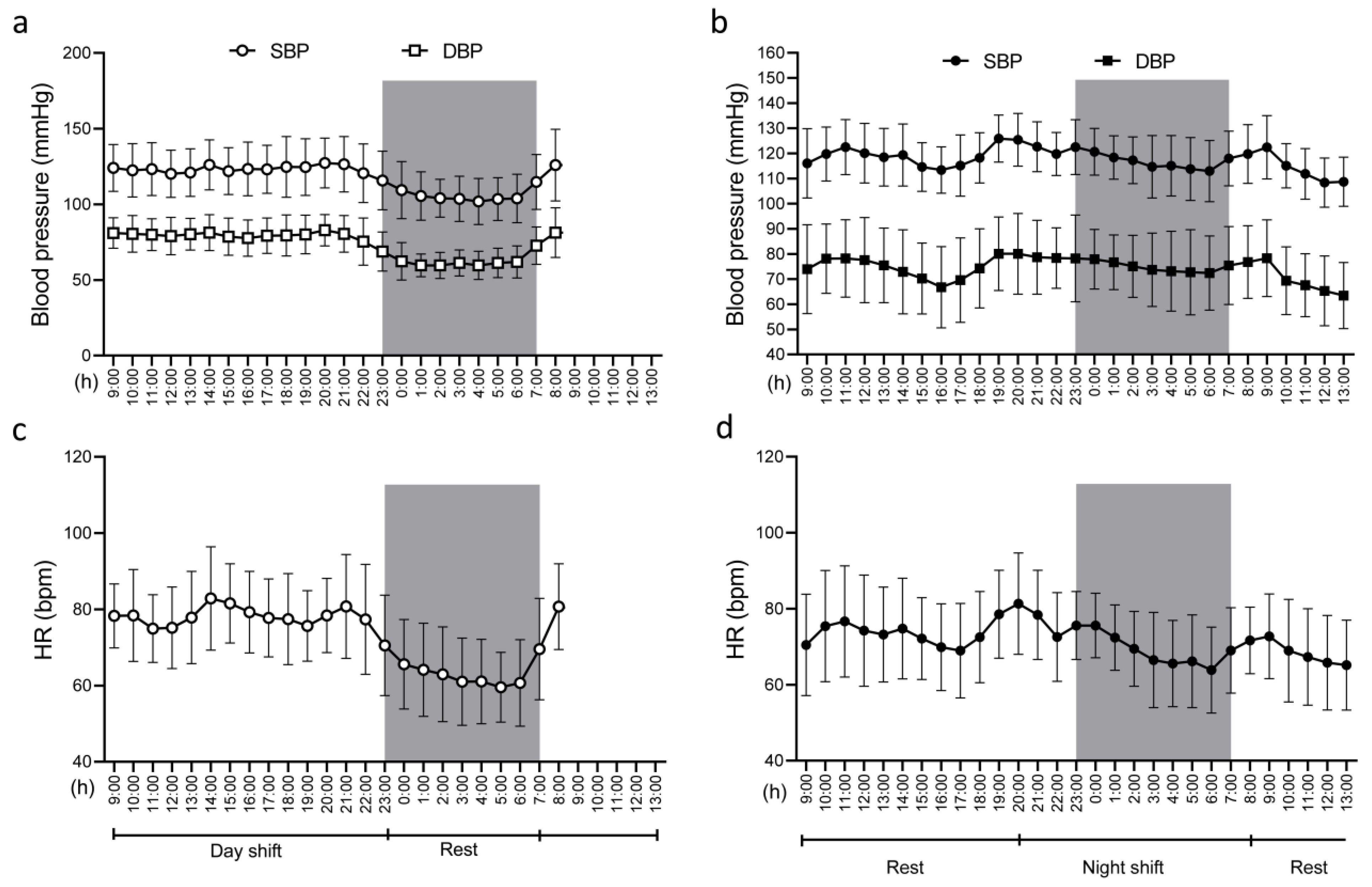
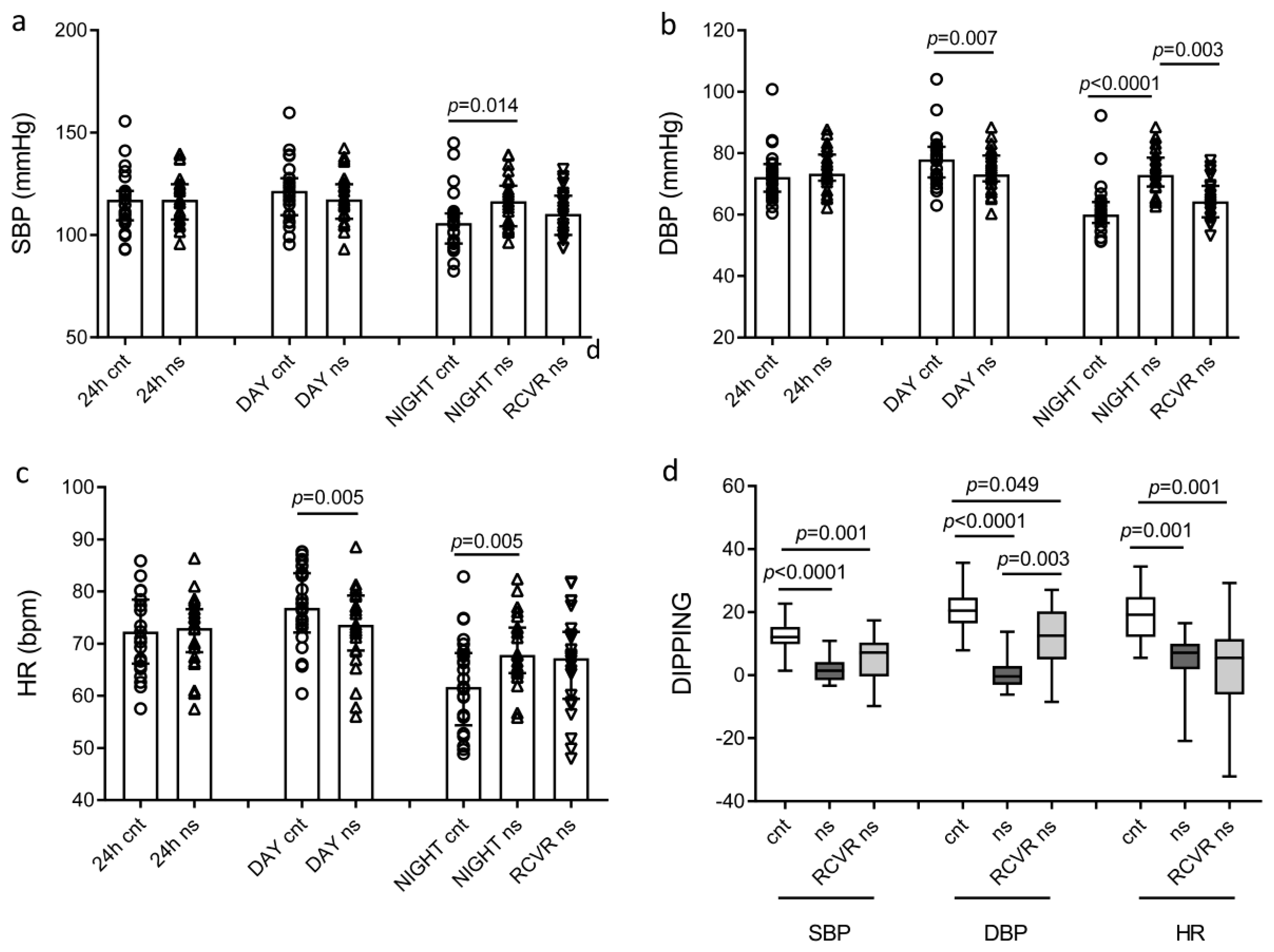
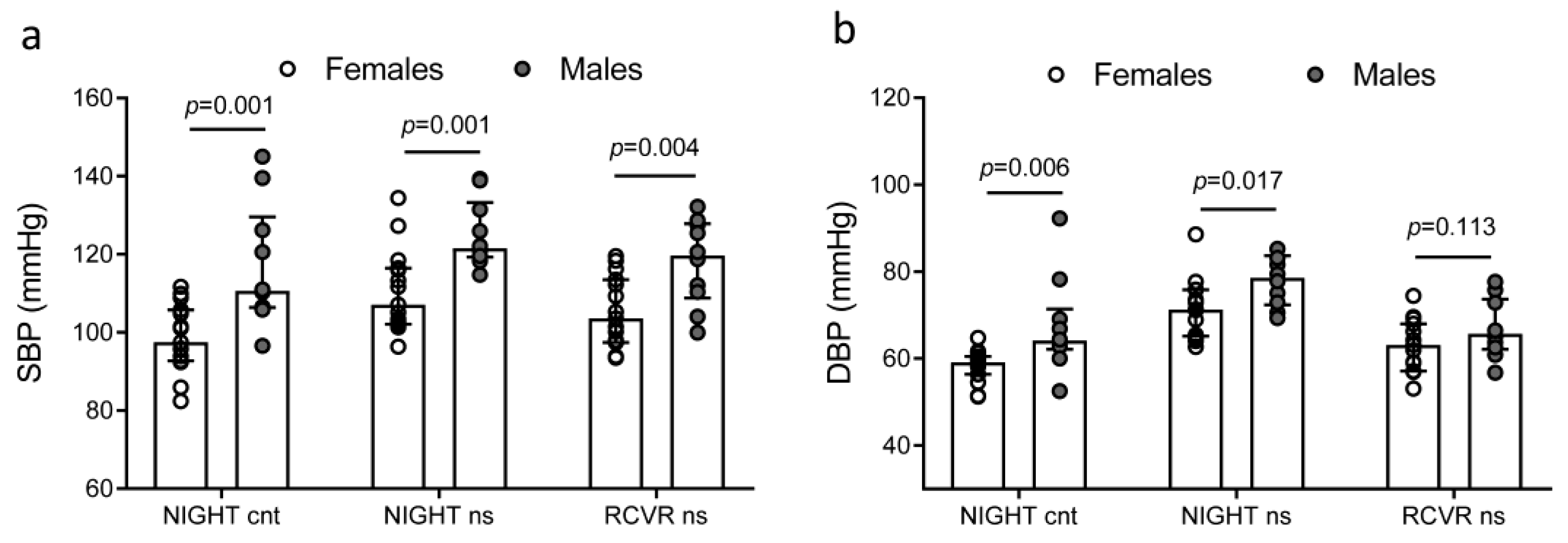
2.2. 24 h Ambulatory Blood Pressure Measurements
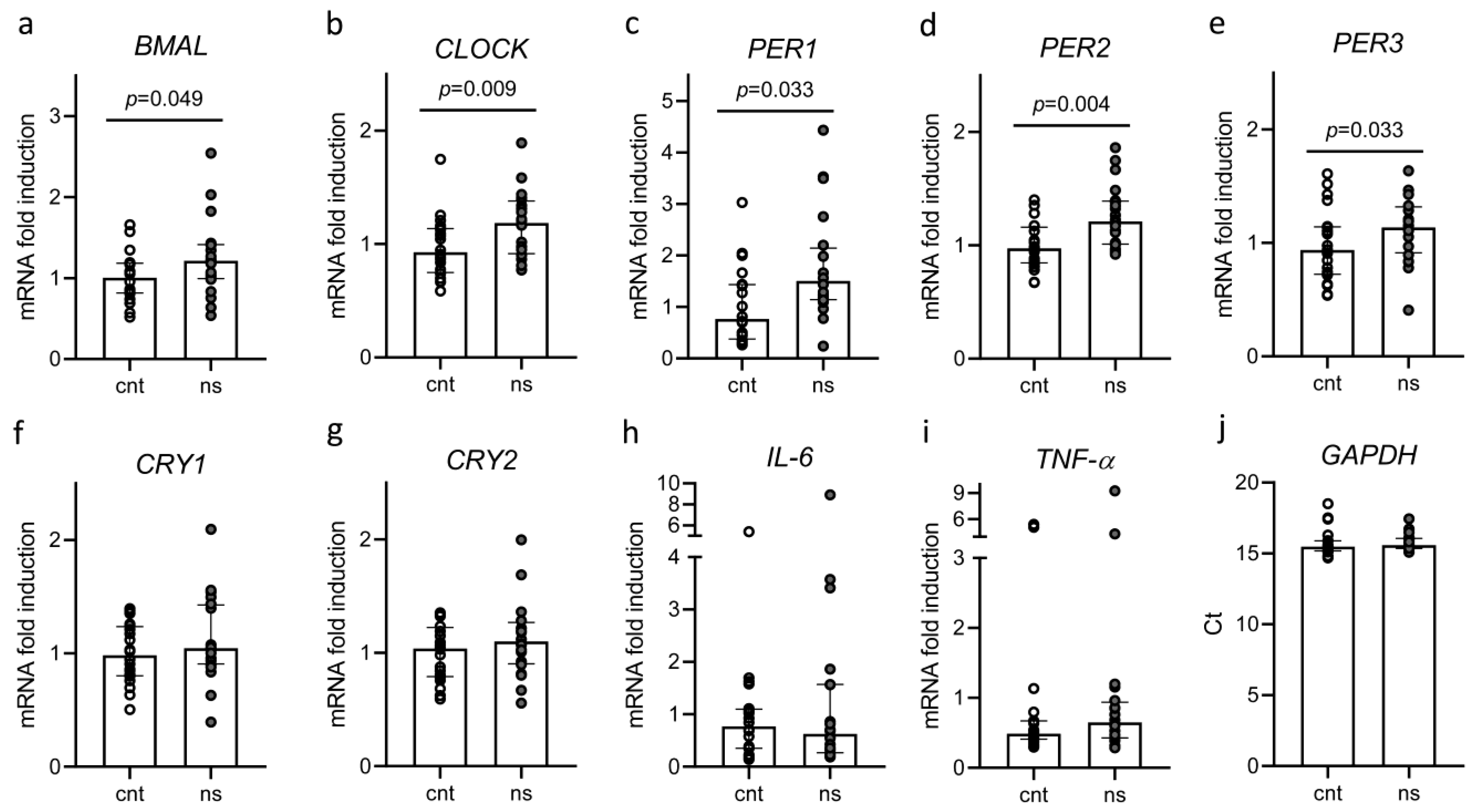
2.3. Biochemical Parameters and Circadian Rhythm Gene Expression
2.4. Correlation Coefficients and Linear Regression Analysis
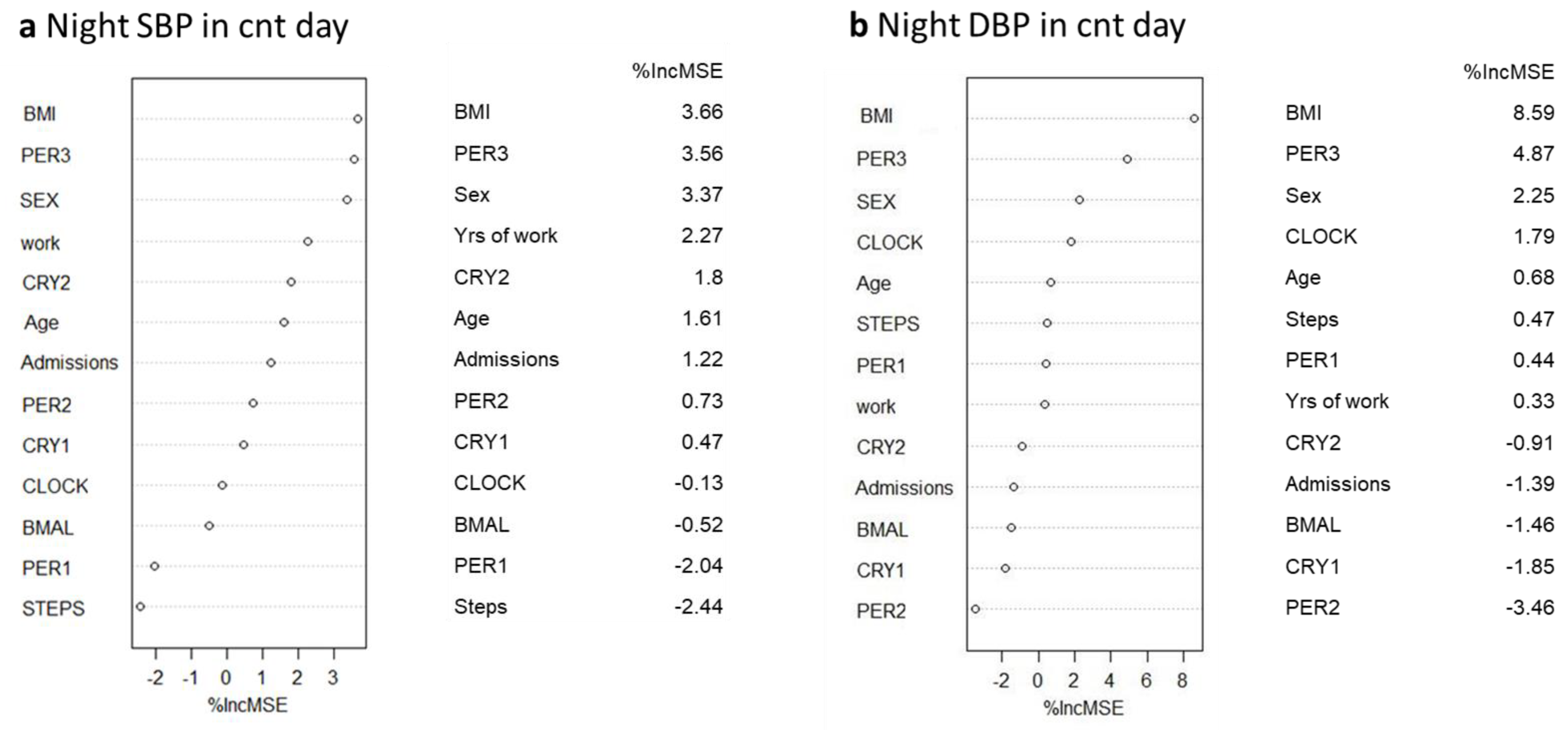
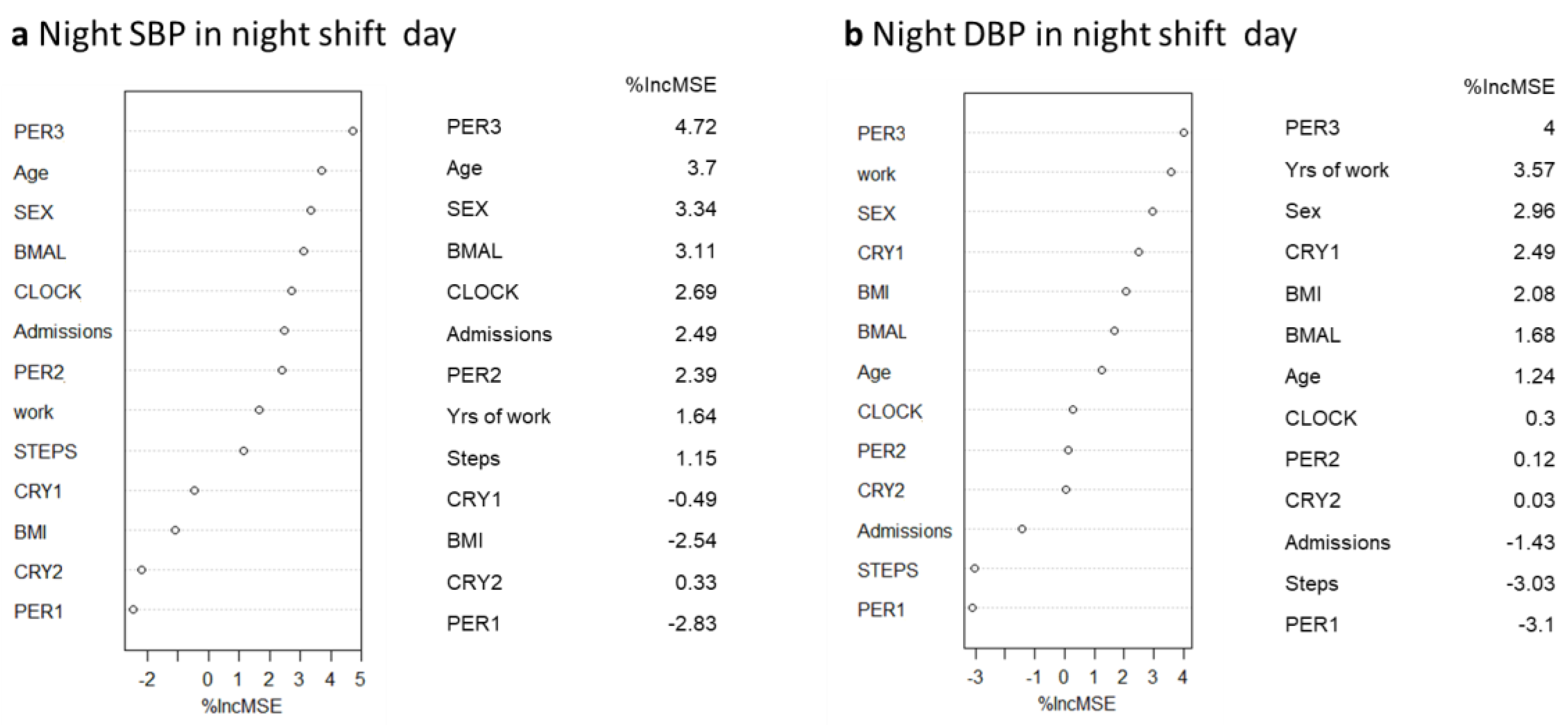
2.5. Random Forest and Linear Regression Analysis
3. Discussion
4. Materials and Methods
4.1. Study Design and Population
4.2. Biochemical Parameters and ELISA
4.3. Peripheral Blood Mononuclear Cell Isolation and Gene Expression Analysis
4.4. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kawachi, I.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C.; Manson, J.E.; Speizer, F.E.; Hennekens, C.H. Prospective study of shift work and risk of coronary heart disease in women. Circulation 1995, 92, 3178–3182. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.L.; Feskanich, D.; Sanchez, B.N.; Rexrode, K.M.; Schernhammer, E.S.; Lisabeth, L.D. Rotating night shift work and the risk of ischemic stroke. Am. J. Epidemiol. 2009, 169, 1370–1377. [Google Scholar] [CrossRef]
- Hemmer, A.; Mareschal, J.; Dibner, C.; Pralong, J.A.; Dorribo, V.; Perrig, S.; Genton, L.; Pichard, C.; Collet, T.H. The Effects of Shift Work on Cardio-Metabolic Diseases and Eating Patterns. Nutrients 2021, 13, 4178. [Google Scholar] [CrossRef]
- Dunlap, J.C. Molecular bases for circadian clocks. Cell 1999, 96, 271–290. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, J.S.; Hong, H.K.; Ko, C.H.; McDearmon, E.L. The genetics of mammalian circadian order and disorder: Implications for physiology and disease. Nat. Rev. Genet. 2008, 9, 764–775. [Google Scholar] [CrossRef] [PubMed]
- Huart, J.; Persu, A.; Lengele, J.P.; Krzesinski, J.M.; Jouret, F.; Stergiou, G.S. Pathophysiology of the Nondipping Blood Pressure Pattern. Hypertension 2023, 80, 719–729. [Google Scholar] [CrossRef] [PubMed]
- Bilo, G.; Grillo, A.; Guida, V.; Parati, G. Morning blood pressure surge: Pathophysiology, clinical relevance and therapeutic aspects. Integr. Blood Press. Control 2018, 11, 47–56. [Google Scholar] [CrossRef]
- Boivin, D.B.; Tremblay, G.M.; James, F.O. Working on atypical schedules. Sleep Med. 2007, 8, 578–589. [Google Scholar] [CrossRef]
- Yamasaki, F.; Schwartz, J.E.; Gerber, L.M.; Warren, K.; Pickering, T.G. Impact of shift work and race/ethnicity on the diurnal rhythm of blood pressure and catecholamines. Hypertension 1998, 32, 417–423. [Google Scholar] [CrossRef]
- Martino, T.A.; Tata, N.; Belsham, D.D.; Chalmers, J.; Straume, M.; Lee, P.; Pribiag, H.; Khaper, N.; Liu, P.P.; Dawood, F.; et al. Disturbed diurnal rhythm alters gene expression and exacerbates cardiovascular disease with rescue by resynchronization. Hypertension 2007, 49, 1104–1113. [Google Scholar] [CrossRef]
- Ohkubo, T.; Imai, Y.; Tsuji, I.; Nagai, K.; Watanabe, N.; Minami, N.; Kato, J.; Kikuchi, N.; Nishiyama, A.; Aihara, A.; et al. Relation between nocturnal decline in blood pressure and mortality. The Ohasama Study. Am. J. Hypertens. 1997, 10, 1201–1207. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.W.; Jen, S.L.; Lee, W.L.; Hsu, N.W.; Lin, S.J.; Ting, C.T.; Chang, M.S.; Wang, P.H. Differential glucose tolerance in dipper and nondipper essential hypertension: The implications of circadian blood pressure regulation on glucose tolerance in hypertension. Diabetes Care 1998, 21, 1743–1748. [Google Scholar] [CrossRef] [PubMed]
- Davidson, M.B.; Hix, J.K.; Vidt, D.G.; Brotman, D.J. Association of impaired diurnal blood pressure variation with a subsequent decline in glomerular filtration rate. Arch. Intern. Med. 2006, 166, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Salles, G.F.; Reboldi, G.; Fagard, R.H.; Cardoso, C.R.; Pierdomenico, S.D.; Verdecchia, P.; Eguchi, K.; Kario, K.; Hoshide, S.; Polonia, J.; et al. Prognostic Effect of the Nocturnal Blood Pressure Fall in Hypertensive Patients: The Ambulatory Blood Pressure Collaboration in Patients With Hypertension (ABC-H) Meta-Analysis. Hypertension 2016, 67, 693–700. [Google Scholar] [CrossRef]
- Torquati, L.; Mielke, G.I.; Brown, W.J.; Kolbe-Alexander, T. Shift work and the risk of cardiovascular disease. A systematic review and meta-analysis including dose-response relationship. Scand. J. Work Environ. Health 2018, 44, 229–238. [Google Scholar] [CrossRef]
- Manohar, S.; Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Herrmann, S.M. Associations of rotational shift work and night shift status with hypertension: A systematic review and meta-analysis. J. Hypertens. 2017, 35, 1929–1937. [Google Scholar] [CrossRef]
- Riegel, B.; Daus, M.; Lozano, A.J.; Malone, S.K.; Patterson, F.; Hanlon, A.L. Shift Workers Have Higher Blood Pressure Medicine Use, But Only When They Are Short Sleepers: A Longitudinal UK Biobank Study. J. Am. Heart Assoc. 2019, 8, e013269. [Google Scholar] [CrossRef]
- Matre, D.; Sirnes, P.A.; Goffeng, E.; Skare, O.; Skogstad, M. Sleep Duration, Number of Awakenings and Arterial Stiffness in Industrial Shift Workers: A Five-Week Follow-Up Study. Int. J. Environ. Res. Public Health 2022, 19, 1964. [Google Scholar] [CrossRef]
- Adams, S.L.; Roxe, D.M.; Weiss, J.; Zhang, F.; Rosenthal, J.E. Ambulatory blood pressure and Holter monitoring of emergency physicians before, during, and after a night shift. Acad. Emerg. Med. 1998, 5, 871–877. [Google Scholar] [CrossRef]
- Zhao, B.; Li, J.; Li, Y.; Liu, J.; Feng, D.; Hao, Y.; Zhen, Y.; Hao, X.; Xu, M.; Chen, X.; et al. A cross-sectional study of the interaction between night shift frequency and age on hypertension prevalence among female nurses. J. Clin. Hypertens. 2022, 24, 598–608. [Google Scholar] [CrossRef]
- Moller-Levet, C.S.; Archer, S.N.; Bucca, G.; Laing, E.E.; Slak, A.; Kabiljo, R.; Lo, J.C.; Santhi, N.; von Schantz, M.; Smith, C.P.; et al. Effects of insufficient sleep on circadian rhythmicity and expression amplitude of the human blood transcriptome. Proc. Natl. Acad. Sci. USA 2013, 110, E1132–E1141. [Google Scholar] [CrossRef]
- Barclay, J.L.; Husse, J.; Bode, B.; Naujokat, N.; Meyer-Kovac, J.; Schmid, S.M.; Lehnert, H.; Oster, H. Circadian desynchrony promotes metabolic disruption in a mouse model of shiftwork. PLoS ONE 2012, 7, e37150. [Google Scholar] [CrossRef] [PubMed]
- Depres-Brummer, P.; Levi, F.; Metzger, G.; Touitou, Y. Light-induced suppression of the rat circadian system. Am. J. Physiol. 1995, 268, R1111–R1116. [Google Scholar] [CrossRef] [PubMed]
- Briaud, S.A.; Zhang, B.L.; Sannajust, F. Continuous light exposure and sympathectomy suppress circadian rhythm of blood pressure in rats. J. Cardiovasc. Pharmacol. Ther. 2004, 9, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Douma, L.G.; Gumz, M.L. Circadian clock-mediated regulation of blood pressure. Free Radic. Biol. Med. 2018, 119, 108–114. [Google Scholar] [CrossRef]
- Stow, L.R.; Richards, J.; Cheng, K.Y.; Lynch, I.J.; Jeffers, L.A.; Greenlee, M.M.; Cain, B.D.; Wingo, C.S.; Gumz, M.L. The circadian protein period 1 contributes to blood pressure control and coordinately regulates renal sodium transport genes. Hypertension 2012, 59, 1151–1156. [Google Scholar] [CrossRef]
- Gumz, M.L.; Stow, L.R.; Lynch, I.J.; Greenlee, M.M.; Rudin, A.; Cain, B.D.; Weaver, D.R.; Wingo, C.S. The circadian clock protein Period 1 regulates expression of the renal epithelial sodium channel in mice. J. Clin. Investig. 2009, 119, 2423–2434. [Google Scholar] [CrossRef]
- Gumz, M.L.; Cheng, K.Y.; Lynch, I.J.; Stow, L.R.; Greenlee, M.M.; Cain, B.D.; Wingo, C.S. Regulation of alphaENaC expression by the circadian clock protein Period 1 in mpkCCD(c14) cells. Biochim. Biophys. Acta 2010, 1799, 622–629. [Google Scholar] [CrossRef]
- Marques, F.Z.; Campain, A.E.; Tomaszewski, M.; Zukowska-Szczechowska, E.; Yang, Y.H.; Charchar, F.J.; Morris, B.J. Gene expression profiling reveals renin mRNA overexpression in human hypertensive kidneys and a role for microRNAs. Hypertension 2011, 58, 1093–1098. [Google Scholar] [CrossRef]
- Dashti, H.S.; Aslibekyan, S.; Scheer, F.A.; Smith, C.E.; Lamon-Fava, S.; Jacques, P.; Lai, C.Q.; Tucker, K.L.; Arnett, D.K.; Ordovas, J.M. Clock Genes Explain a Large Proportion of Phenotypic Variance in Systolic Blood Pressure and This Control Is Not Modified by Environmental Temperature. Am. J. Hypertens. 2016, 29, 132–140. [Google Scholar] [CrossRef]
- Kovanen, L.; Donner, K.; Kaunisto, M.; Partonen, T. CRY1, CRY2 and PRKCDBP genetic variants in metabolic syndrome. Hypertens. Res. 2015, 38, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Leu, H.B.; Chung, C.M.; Lin, S.J.; Chiang, K.M.; Yang, H.C.; Ho, H.Y.; Ting, C.T.; Lin, T.H.; Sheu, S.H.; Tsai, W.C.; et al. Association of circadian genes with diurnal blood pressure changes and non-dipper essential hypertension: A genetic association with young-onset hypertension. Hypertens. Res. 2015, 38, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Woon, P.Y.; Kaisaki, P.J.; Braganca, J.; Bihoreau, M.T.; Levy, J.C.; Farrall, M.; Gauguier, D. Aryl hydrocarbon receptor nuclear translocator-like (BMAL1) is associated with susceptibility to hypertension and type 2 diabetes. Proc. Natl. Acad. Sci. USA 2007, 104, 14412–14417. [Google Scholar] [CrossRef] [PubMed]
- van Elk, F.; Robroek, S.J.W.; Smits-de Boer, S.; Kouwenhoven-Pasmooij, T.A.; Burdorf, A.; Oude Hengel, K.M. Study design of PerfectFit@Night, a workplace health promotion program to improve sleep, fatigue, and recovery of night shift workers in the healthcare sector. BMC Public Health 2022, 22, 779. [Google Scholar] [CrossRef]
- Patterson, P.D.; Weiss, L.S.; Weaver, M.D.; Salcido, D.D.; Opitz, S.E.; Okerman, T.S.; Smida, T.T.; Martin, S.E.; Guyette, F.X.; Martin-Gill, C.; et al. Napping on the night shift and its impact on blood pressure and heart rate variability among emergency medical services workers: Study protocol for a randomized crossover trial. Trials 2021, 22, 212. [Google Scholar] [CrossRef]
- Bernardi, S.; Toffoli, B.; Tonon, F.; Francica, M.; Campagnolo, E.; Ferretti, T.; Comar, S.; Giudici, F.; Stenner, E.; Fabris, B. Sex Differences in Proatherogenic Cytokine Levels. Int. J. Mol. Sci. 2020, 21, 3861. [Google Scholar] [CrossRef]
- Tonon, F.; Di Bella, S.; Giudici, F.; Zerbato, V.; Segat, L.; Koncan, R.; Misin, A.; Toffoli, B.; D’Agaro, P.; Luzzati, R.; et al. Discriminatory Value of Adiponectin to Leptin Ratio for COVID-19 Pneumonia. Int. J. Endocrinol. 2022, 2022, 9908450. [Google Scholar] [CrossRef]
- Tonon, F.; Candido, R.; Toffoli, B.; Tommasi, E.; Cortello, T.; Fabris, B.; Bernardi, S. Type 1 diabetes is associated with significant changes of ACE and ACE2 expression in peripheral blood mononuclear cells. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1275–1282. [Google Scholar] [CrossRef]
- Tonon, F.; Tornese, G.; Giudici, F.; Nicolardi, F.; Toffoli, B.; Barbi, E.; Fabris, B.; Bernardi, S. Children With Short Stature Display Reduced ACE2 Expression in Peripheral Blood Mononuclear Cells. Front. Endocrinol. 2022, 13, 912064. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n = 25 | |
|---|---|---|
| Age | 33 (29–37) | |
| Sex | Female (%) | 15 (60%) |
| Male (%) | 10 (40%) | |
| BMI | 22.6 (20.8–24.54) | |
| Physical activity (Recreational activity) | Yes (%) | 12 (48%) |
| No (%) | 13 (52%) | |
| Medical conditions | Yes (%) | 3 (12%) |
| No (%) | 22 (88%) | |
| Medication | Yes (%) | 5 (20%) |
| No (%) | 20 (80%) | |
| Years of work | 7 (2–10) | |
| Working position | Attending physician (%) | 13 (52%) |
| Resident physician (%) | 12 (48%) | |
| Day shift steps | 7720 (6504–11,062) | |
| Night shift calls | 17.5 (13–20) | |
| Night shift admissions | 8.5 (6–10) | |
| Night shift steps | 6660 (5785–7822) |
| NIGHT cnt (t1) | NIGHT ns (t2) | RCVR ns (t3) | ANOVA | t1 vs. t2 | t2 vs. t3 | t1 vs. t3 | |
|---|---|---|---|---|---|---|---|
| SBP (mmHg) | 106.08 ± 14.82 | 116.38 ± 12.15 | 110.24 ± 11.66 | F = 10.98 p < 0.001 ηg2 = 0.1 | p < 0.001 | p = 0.006 | p = 0.28 |
| DBP (mmHg) | 61.85 ± 8.57 | 73.96 ± 7.12 | 64.87 ± 6.64 | F = 30.72 p < 0.001 ηg2 = 0.33 | p < 0.001 | p < 0.001 | p = 0.23 |
| SBP dipping (%) | 12.6 ± 4.82 | 1.49 ± 3.69 | 5.01 ± 7.51 | F = 27.56 p < 0.001 ηg2 = 0.42 | p < 0.001 | p = 0.17 | p < 0.001 |
| DBP dipping (%) | 20.7 ± 6.58 | 0.47 ± 4.67 | 11.7 ± 10.6 | F = 42.42 p < 0.001 ηg2 = 0.55 | p < 0.001 | p < 0.001 | p < 0.001 |
| Variable | After Night of Rest | After a Night Shift | p-Value |
|---|---|---|---|
| Glucose (mg/dL) | 88.5 (80–91) | 86 (80–96) | p = 0.35 |
| Cortisol (nmol/L) | 303 (260.5–362) | 331 (269–413) | p = 0.11 |
| Melatonin (pg/mL) | 108.1 (98–158) | 127.8 (99–138) | p = 0.58 |
| CRP (mg/L) | 0.85 (0.4–1.5) | 0.7 (0.6–1.4) | p = 0.11 |
| IL-1β (pg/mL) | 12.08 (0–69) | 12.89 (0–72) | p = 0.41 |
| IL-6 (pg/mL) | 28.81 (3–117.5) | 30.77 (2–156) | p = 0.15 |
| TNF-α (pg/mL) | 5.13 (0–82.5) | 3.20 (0–76) | p = 1.00 |
| Variable | Cnt Day | Night Shift Day | ||||||
|---|---|---|---|---|---|---|---|---|
| Night SBP | Night DBP | Night SBP | Night DBP | |||||
| rho | p | rho | p | rho | p | rho | p | |
| Age | 0.01 | 0.96 | 0.10 | 0.65 | −0.23 | 0.28 | 0.18 | 0.37 |
| BMI | 0.42 | 0.04 * | 0.49 | 0.01 * | 0.40 | 0.05 * | 0.40 | 0.045 * |
| BMAL | 0.18 | 0.43 | 0.09 | 0.70 | −0.22 | 0.35 | −0.09 | 0.69 |
| CLOCK | 0.30 | 0.20 | 0.05 | 0.83 | 0.36 | 0.12 | 0.33 | 0.15 |
| PER1 | −0.02 | 0.94 | −0.09 | 0.71 | −0.17 | 0.46 | −0.05 | 0.82 |
| PER2 | 0.23 | 0.33 | 0.04 | 0.87 | 0.40 | 0.08 * | 0.45 | 0.04 * |
| PER3 | 0.51 | 0.02 * | 0.27 | 0.25 | 0.37 | 0.11 | 0.35 | 0.13 |
| CRY1 | 0.22 | 0.35 | 0.09 | 0.71 | 0.13 | 0.58 | 0.17 | 0.47 |
| CRY2 | 0.32 | 0.17 | 0.30 | 0.20 | 0.23 | 0.34 | 0.29 | 0.22 |
| Night calls | NA | NA | NA | NA | 0.15 | 0.63 | 0.20 | 0.54 |
| Night admissions | NA | NA | NA | NA | 0.01 | 0.96 | 0.07 | 0.74 |
| Night steps | NA | NA | NA | NA | −0.10 | 0.66 | −0.01 | 0.96 |
| Dependent Variable: Night SBP (cnt Day) | ||||
| Predictive Variable | β-Estimate | SE | p-Value | Multiple R-Squared |
| Sex | 9.33 | 3.96 | 0.03 | |
| BMI | 1.69 | 0.60 | 0.01 | 0.72 |
| PER3 | 18.84 | 5.36 | 0.003 | |
| Dependent Variable: Night SBP (Night Shift Day) | ||||
| Predictive Variable | β-Estimate | SE | p-Value | Multiple R-Squared |
| Sex | 10.52 | 5.15 | 0.06 | |
| BMI | 0.85 | 0.77 | 0.28 | 0.41 |
| PER2 | 17.48 | 8.06 | 0.045 | |
| Dependent Variable: Night DBP (Night Shift Day) | ||||
| Predictive Variable | β-Estimate | SE | p-Value | Multiple R-Squared |
| Sex | 4.34 | 3.19 | 0.19 | |
| BMI | 0.50 | 0.48 | 0.31 | 0.48 |
| PER2 | 11.70 | 4.99 | 0.03 | |
| Dependent Variable: Night SBP (cnt Day) | ||||
| Predictive Variable | β-Estimate | SE | p-Value | Multiple R-Squared |
| Sex | −10.36 | 3.38 | 0.007 | |
| BMI | 1.74 | 0.52 | 0.004 | 0.76 |
| PER3 | 19.08 | 4.93 | 0.001 | |
| Dependent Variable: Night DBP (cnt Day) | ||||
| Predictive Variable | β-Estimate | SE | p-Value | Multiple R-Squared |
| Sex | −3.5 | 2.12 | 0.12 | |
| BMI | 0.99 | 0.33 | 0.008 | 0.61 |
| PER3 | 6.79 | 3.10 | 0.04 | |
| Dependent Variable: Night SBP (Night Shift Day) | ||||
| Predictive Variable | β-Estimate | SE | p-Value | Multiple R-Squared |
| Age | −0.11 | 0.35 | 0.75 | |
| Sex | −18.37 | 4.11 | <0.001 | 0.63 |
| PER3 | 25.34 | 7.23 | 0.003 | |
| Dependent Variable: Night DBP (Night Shift Day) | ||||
| Predictive Variable | β-Estimate | SE | p-Value | Multiple R-Squared |
| Sex | −8.50 | 2.81 | 0.008 | |
| Years of work | −0.23 | 0.25 | 0.37 | 0.51 |
| PER3 | 12.38 | 4.99 | 0.02 | |
| Target (GenBank Accession Number) | Primer Pair | Mature Transcript | Amplicon Size (bp) |
|---|---|---|---|
| BMAL1 (NM_001297719) | (F) 5′-TTACTGTGCTAAGGATGGCTG-3′ (R) 5′-GCCCTGAGAATGAGGTGTTTC-3′ | (F) 731–751 (R) 857–837 | 127 |
| CLOCK (NM_004898) | (F) 5’-CTACATTCACTCAGGACAGGC-3’ (R) 5’-GGCCCATAAGCATAGTACTAGG-3’ | (F) 2495–2515 (R) 2614–2593 | 120 |
| PER1 (NM_002616) | (F) 5′-CCTCCAGTGATAGCAACGG-3′ (R) 5′-ACCAGATGCACATCCTTACAG-3′ | (F) 1784–1802 (R) 1874–1854 | 91 |
| PER2 (NM_022817) | (F) 5′-GCCAGAGTCCAGATACCTTTAG-3′ (R) 5′-TGTGTCCACTTTCGAAGACTG-3′ | (F) 505–526 (R) 602–582 | 98 |
| PER3 (NM_001377275) | (F) 5′-CTGTCTCACTGTGGTTGAAAAG-3′ (R) 5′-TAGGTAACCCAGCAAAGGC-3′ | (F) 1063–1084 (R) 1207–1189 | 145 |
| CRY1 (NM_004075) | (F) 5’-TCCCGTCTGTTTGTGATTCG-3’ (R) 5’-TTAATAGCTGCGTCTCGTTCC-3’ | (F) 799–818 (R) 929–909 | 131 |
| CRY2 (NM_021117) | (F) 5′-TGGATAAGCACTTGGAACGG-3′ (R) 5′-AGAGACAACCAAAGCGCAG-3′ | (F) 735–754 (R) 854–836 | 120 |
| TNF-α (NM_000594) | (F) 5′-ACTTTGGAGTGATCGGCC-3′ (R) 5′-GCTTGAGGGTTTGCTACAAC-3′ | (F) 332–349 (R) 470–451 | 139 |
| IL-6 (NM_000600) | (F) 5′-CCACTCACCTCTTCAGAACG-3′ (R) 5′-CATCTTTGGAAGGTTCAGGTTG-3′ | (F) 199–218 (R) 348–327 | 150 |
| GAPDH (NM_002046) | (F) 5’-CATCCATGACAACTTTGGTATCGT-3’ (R) 5’-CCATCACGCCACAGTTTCC-3’ | (F) 565–588 (R) 672–654 | 108 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toffoli, B.; Tonon, F.; Giudici, F.; Ferretti, T.; Ghirigato, E.; Contessa, M.; Francica, M.; Candido, R.; Puato, M.; Grillo, A.; et al. Preliminary Study on the Effect of a Night Shift on Blood Pressure and Clock Gene Expression. Int. J. Mol. Sci. 2023, 24, 9309. https://doi.org/10.3390/ijms24119309
Toffoli B, Tonon F, Giudici F, Ferretti T, Ghirigato E, Contessa M, Francica M, Candido R, Puato M, Grillo A, et al. Preliminary Study on the Effect of a Night Shift on Blood Pressure and Clock Gene Expression. International Journal of Molecular Sciences. 2023; 24(11):9309. https://doi.org/10.3390/ijms24119309
Chicago/Turabian StyleToffoli, Barbara, Federica Tonon, Fabiola Giudici, Tommaso Ferretti, Elena Ghirigato, Matilde Contessa, Morena Francica, Riccardo Candido, Massimo Puato, Andrea Grillo, and et al. 2023. "Preliminary Study on the Effect of a Night Shift on Blood Pressure and Clock Gene Expression" International Journal of Molecular Sciences 24, no. 11: 9309. https://doi.org/10.3390/ijms24119309