
Markers of Restenosis after Percutaneous Transluminal Balloon Angioplasty in Patients with Critical Limb Ischemia
 , , and
, , and
Abstract
:1. Introduction
1.1. The Collection of Materials for the Review
1.2. The Role of Atherosclerosis and Diabetes Mellitus in the Development of Restenosis
1.3. General Mechanism of Restenosis after Endovascular Revascularization
2. Key Pathogenetic Mechanisms of Restenosis Development
2.1. The Role of Inflammation in the Development of Restenosis
2.2. The Ratio of Neutrophils to Lymphocytes as a Predictor of Restenosis
2.3. Markers of Oxidative Stress
2.4. Hemostasis Factors
2.5. MicroRNA
2.6. The Kinin–Kallikrein System
2.7. Metalloproteinases
2.8. The Role of Osteopontin and Osteoprotegrin
3. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE | angiotensin-converting enzyme |
| APOA | apolipoprotein E is encoded by the APOA gene |
| bFGF | basic fibroblast growth factor |
| CLI | critical limb ischemia |
| CLTI | chronic limb-threatening ischemia |
| CRP | C-reactive protein |
| DCB | drug-coated balloon |
| DES | drug-eluting stent |
| DM | diabetes mellitus |
| eNOS | endothelial nitric oxide synthase |
| GPx | glutathione peroxidase |
| GSH | thiol groups |
| HIF | hypoxia-inducible factors |
| HMGB-1 | highly mobile group box-1 |
| IL | interleukin |
| IPOD | infrapopliteal arterial occlusive disease |
| ISR | in-stent restenosis |
| KKS | kinin–kallikrein system |
| LDL | low-density lipoprotein |
| LEA | limb extremity amputation |
| MACE | major adverse cardiovascular events |
| miRNAs | microRNAs |
| MDA | malondialdehyde |
| MMPs | matrix metalloproteinases |
| NLR | neutrophil to lymphocyte ratio |
| NO | nitric oxide |
| OPG | osteoprotegerin |
| OPN | osteopontin |
| PAI-1 | plasminogen activator inhibitor |
| PAD | peripheral arterial disease |
| SOD | superoxide dismutase |
| TAT | thrombin–antithrombin complex |
| TF | tissue factor |
| TFPI | tissue factor pathway inhibitor |
| TGF-b1 | transforming growth factor beta1 |
| TIMPs | metalloproteinase inhibitors |
| TLR | target lesion revascularization |
| TNF-α | tumor necrosis factor alpha |
| T2D | type 2 diabetes |
| VSMCs | vascular smooth muscle cells |
References
- Malysheva, A.V.; Kosyakov, D.V.; Guskov, A.E. Methodology for selecting publications for scientific reviews. Sci. Tech. Libr. 2022, 11, 56–81. [Google Scholar] [CrossRef]
- Signorelli, S.S.; Marino, E.; Scuto, S.; Di Raimondo, D. Pathophysiology of Peripheral Arterial Disease (PAD): A Review on Oxidative Disorders. Int. J. Mol. Sci. 2020, 21, 4393. [Google Scholar] [CrossRef] [PubMed]
- Abramson, B.L.; Al-Omran, M.; Anand, S.S.; Albalawi, Z.; Coutinho, T.; de Mestral, C.; Dubois, L.; Gill, H.L.; Greco, E.; Guzman, R.; et al. Canadian Cardiovascular Society 2022 Guidelines for Peripheral Arterial Disease. Can. J. Cardiol. 2022, 38, 560–587. [Google Scholar] [CrossRef] [PubMed]
- Barnes, J.A.; Eid, M.A.; Creager, M.A.; Goodney, P.P. Epidemiology and Risk of Amputation in Patients with Diabetes Mellitus and Peripheral Artery Disease. Arter. Thromb. Vasc. Biol. 2020, 40, 1808–1817. [Google Scholar] [CrossRef]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.-B.; Suresh, K.R.; Murad, M.H.; et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. Eur. J. Vasc. Endovasc. Surg. 2019, 58, S1–S109.e133. [Google Scholar] [CrossRef]
- Vrsalovic, M.; Vucur, K.; Vrsalovic Presecki, A.; Fabijanic, D.; Milosevic, M. Impact of diabetes on mortality in peripheral artery disease: A meta-analysis. Clin. Cardiol. 2017, 40, 287–291. [Google Scholar] [CrossRef]
- Glovaci, D.; Fan, W.; Wong, N.D. Epidemiology of Diabetes Mellitus and Cardiovascular Disease. Curr. Cardiol. Rep. 2019, 21, 21. [Google Scholar] [CrossRef]
- Beckman, J.A.; Schneider, P.A.; Conte, M.S. Advances in Revascularization for Peripheral Artery Disease: Revascularization in PAD. Circ. Res. 2021, 128, 1885–1912. [Google Scholar] [CrossRef]
- Varela, D.L.; Armstrong, E.J. Endovascular Management of Femoropopliteal In-Stent Restenosis: A Systematic Review. Cardiovasc. Revasc. Med. 2019, 20, 915–925. [Google Scholar] [CrossRef]
- Donners, M.M.P.C.; Daemen, M.J.A.P.; Cleutjens, K.B.J.M.; Heeneman, S. Inflammation and restenosis: Implications for therapy. Ann. Med. 2003, 35, 523–531. [Google Scholar] [CrossRef]
- Anantha-Narayanan, M.; Love, K.; Nagpal, S.; Sheikh, A.B.; Regan, C.J.; Mena-Hurtado, C. Safety and efficacy of paclitaxel drug-coated balloon in femoropopliteal in-stent restenosis. Expert Rev. Med. Devices 2020, 17, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Lucas, A.; Liu, L.-Y.; Macen, J.; Nash, P.; Dai, E.; Stewart, M.; Graham, K.; Etches, W.; Boshkov, L.; Nation, P.N.; et al. Virus-Encoded Serine Proteinase Inhibitor SERP-1 Inhibits Atherosclerotic Plaque Development After Balloon Angioplasty. Circulation 1996, 94, 2890–2900. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.S.; Murphy, J.G.; Edwards, W.D.; Camrud, A.R.; Vliestra, R.E.; Holmes, D.R. Restenosis after balloon angioplasty. A practical proliferative model in the porcine coronary arteries. Circulation 1990, 82, 2190–2200. [Google Scholar] [CrossRef] [PubMed]
- Villa, A.E.; Guzman, L.A.; Chen, W.; Golomb, G.; Levy, R.J.; Topol, E.J. Local delivery of dexamethasone for prevention of neointimal proliferation in a rat model of balloon angioplasty. J. Clin. Investig. 1994, 93, 1243–1249. [Google Scholar] [CrossRef] [PubMed]
- Scott, N.A.; Cipolla, G.D.; Ross, C.E.; Dunn, B.; Martin, F.H.; Simonet, L.; Wilcox, J.N. Identification of a Potential Role for the Adventitia in Vascular Lesion Formation After Balloon Overstretch Injury of Porcine Coronary Arteries. Circulation 1996, 93, 2178–2187. [Google Scholar] [CrossRef] [PubMed]
- Vrsalovic, M. Diabetes and peripheral artery disease: A bad combination. Am. J. Surg. 2017, 216, 182–183. [Google Scholar] [CrossRef]
- Joosten, M.M.; Pai, J.K.; Bertoia, M.L.; Rimm, E.B.; Spiegelman, D.; Mittleman, M.; Mukamal, K.J. Associations Between Conventional Cardiovascular Risk Factors and Risk of Peripheral Artery Disease in Men. JAMA 2012, 308, 1660–1667. [Google Scholar] [CrossRef]
- Domingueti, C.P.; Dusse, L.M.S.; Carvalho, M.D.G.; de Sousa, L.P.; Gomes, K.B.; Fernandes, A.P. Diabetes mellitus: The linkage between oxidative stress, inflammation, hypercoagulability and vascular complications. J. Diabetes Its Complicat. 2016, 30, 738–745. [Google Scholar] [CrossRef]
- Thiruvoipati, T.; Kielhorn, C.E.; Armstrong, E.J. Peripheral Artery Disease in Patients with Diabetes: Epidemiology, Mechanisms, and Outcomes. World J. Diabetes 2015, 6, 961–969. [Google Scholar] [CrossRef]
- American Diabetes Association Peripheral Arterial Disease in People with Diabetes. Diabetes Care 2003, 26, 3333–3341. [CrossRef]
- Fowkes, F.; Aboyans, V.; McDermott, M.M.; Sampson, U.K.A.; Criqui, M.H. Peripheral artery disease: Epidemiology and global perspectives. Nat. Rev. Cardiol. 2017, 14, 156–170. [Google Scholar] [CrossRef]
- Cavender, M.A.; Scirica, B.M.; Raz, I.; Steg, P.G.; McGuire, D.K.; Leiter, L.A.; Hirshberg, B.; Davidson, J.; Cahn, A.; Mosenzon, O.; et al. Cardiovascular Outcomes of Patients in SAVOR-TIMI 53 by Baseline Hemoglobin A1c. Am. J. Med. 2016, 129, 340.e1–340.e8. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.L.; Blomster, J.I.; Heizer, G.; Berger, J.S.; Baumgartner, I.; Fowkes, F.G.R.; Held, P.; Katona, B.G.; Norgren, L.; Jones, W.S.; et al. Cardiovascular and Limb Outcomes in Patients with Diabetes and Peripheral Artery Disease: The EUCLID Trial. J. Am. Coll. Cardiol. 2018, 72, 3274–3284. [Google Scholar] [CrossRef] [PubMed]
- Treat-Jacobson, D. Review of article: Goldman M.P., Clark C.J., Craven T.E., Davis R.P., Williams T.K., Velazquez-Ramirez G., Hurie J.B., Edwards M.S. Effect of intensive glycemic control on risk of lower extremity amputation. J Am Coll Surg 2018; 227: 596–604. J. Vasc. Nurs. 2019, 37, 272–273. [Google Scholar] [CrossRef]
- Takahara, M.; Kaneto, H.; Iida, O.; Gorogawa, S.-I.; Katakami, N.; Matsuoka, T.-A.; Ikeda, M.; Shimomura, I. The Influence of Glycemic Control on the Prognosis of Japanese Patients Undergoing Percutaneous Transluminal Angioplasty for Critical Limb Ischemia. Diabetes Care 2010, 33, 2538–2542. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Armstrong, E.J.; Sherif, W.; Alvandi, B.; Westin, G.G.; Singh, G.D.A.; Amsterdam, E.; Laird, J.R. Association of Elevated Fasting Glucose with Lower Patency and Increased Major Adverse Limb Events among Patients with DI-Abetes Undergoing Infrapopliteal Balloon Angioplasty. Vasc. Med. 2014, 19, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Shumkov, O.A.; Lyubarkiy, M.S.; Altukhov, I.A.; Soluyanov, M.Y.; Smagin, M.A. The role of vascular surgery in the multidisciplinary approach to the diabetic foot syndrome. Khirurgiia 2013, 11, 9–15. [Google Scholar]
- Smagin, M.; Shumkov, O.; Khapaev, R.; Surovtseva, M.; Nimaev, V. The combined approach to treatment of patients witn chronic ischemia and diabetic foot syndrome. In Proceedings of the 2020 Cognitive Sciences, Genomics and Bioinformatics (CSGB), Novosibirsk, Russia, 6–10 July 2020; pp. 236–239. [Google Scholar]
- Lee, S.-Y.; Hong, M.-K.; Jang, Y. Formation and Transformation of Neointima after Drug-eluting Stent Implantation: Insights from Optical Coherence Tomographic Studies. Korean Circ. J. 2017, 47, 823–832. [Google Scholar] [CrossRef]
- Aoki, J.; Tanabe, K. Mechanisms of drug-eluting stent restenosis. Cardiovasc. Interv. Ther. 2021, 36, 23–29. [Google Scholar] [CrossRef]
- Tummala, S.; Amin, A.; Mehta, A. Infrapopliteal Artery Occlusive Disease: An Overview of Vessel Preparation and Treatment Options. J. Clin. Med. 2020, 9, 3321. [Google Scholar] [CrossRef]
- Calle, M.C.; Fernandez, M.L. Inflammation and type 2 diabetes. Diabetes Metab. 2012, 38, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Saik, O.; Sobolevskaya, E.; Khapaev, R.; Shumkov, O.; Smagin, M.; Nimaev, V. Revealing the Molecular Basis of Vascular Restenosis by Gene Network Analysis. In Proceedings of the 2022 IEEE International Multi-Conference on Engineering, Computer and Information Sciences (SIBIRCON 2022), Yekaterinburg, Russia, 11–13 November 2022; pp. 350–353. [Google Scholar] [CrossRef]
- Mause, S.F.; Ritzel, E.; Deck, A.; Vogt, F.; Liehn, E.A. Endothelial progenitor cells modulate the phenotype of smooth muscle cells and increase their neointimal accumulation following vascular injury. Thromb. Haemost. 2022, 122, 456–469. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, J.C.; di Lugano, O.R. The Biology of In-Stent Restenosis and the Rationale for Debulking. Vasc. Dis. Manag. 2016, 13, E198–E208. [Google Scholar]
- Inoue, S.; Koyama, H.; Miyata, T.; Shigematsu, H. Pathogenetic heterogeneity of in-stent lesion formation in human peripheral arterial disease. J. Vasc. Surg. 2002, 35, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Iida, O.; Uematsu, M.; Soga, Y.; Hirano, K.; Suzuki, K.; Yokoi, H.; Muramatsu, T.; Inoue, N.; Nanto, S.; Nagata, S. Timing of the restenosis following nitinol stenting in the superficial femoral artery and the factors associated with early and late restenoses. Catheter. Cardiovasc. Interv. 2011, 78, 611–617. [Google Scholar] [CrossRef]
- Kornowski, R.; Hong, M.K.; Tio, F.O.; Bramwell, O.; Wu, H.; Leon, M.B. In-Stent Restenosis: Contributions of Inflammatory Responses and Arterial Injury to Neointimal Hyperplasia. J. Am. Coll. Cardiol. 1998, 31, 224–230. [Google Scholar] [CrossRef]
- Romero, M.E.; Yahagi, K.; Kolodgie, F.D.; Virmani, R. Neoatherosclerosis from a Pathologist’s Point of View. Arter. Thromb. Vasc. Biol. 2015, 35, e43–e49. [Google Scholar] [CrossRef]
- Sage, A.P.; Tsiantoulas, D.; Binder, C.J.; Mallat, Z. The role of B cells in atherosclerosis. Nat. Rev. Cardiol. 2019, 16, 180–196. [Google Scholar] [CrossRef]
- Martinet, W.; Schrijvers, D.M.; De Meyer, G.R.Y. Necrotic cell death in atherosclerosis. Basic Res. Cardiol. 2011, 106, 749–760. [Google Scholar] [CrossRef]
- Vesnina, A.; Prosekov, A.; Atuchin, V.; Minina, V.; Ponasenko, A. Tackling Atherosclerosis via Selected Nutrition. Int. J. Mol. Sci. 2022, 23, 8233. [Google Scholar] [CrossRef]
- Mazin, I.; Paul, G.; Asher, E. Neoatherosclerosis—From basic concept to clinical implication. Thromb. Res. 2019, 178, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Christoph, M.; Pfluecke, C.; Mensch, M.; Augstein, A.; Jellinghaus, S.; Ende, G.; Mierke, J.; Franke, K.; Wielockx, B.; Ibrahim, K.; et al. Myeloid PHD2 deficiency accelerates neointima formation via Hif-1α. Mol. Immunol. 2022, 149, 48–58. [Google Scholar] [CrossRef]
- Ullah, K.; Wu, R. Hypoxia-Inducible Factor Regulates Endothelial Metabolism in Cardiovascular Disease. Front. Physiol. 2021, 12, 670653. [Google Scholar] [CrossRef] [PubMed]
- Miroshnichenko, S.; Usynin, I.; Dudarev, A.; Nimaev, V.; Solovieva, A. Apolipoprotein A-I supports MSCS survival under stress conditions. Int. J. Mol. Sci. 2020, 21, 4062. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, F.; Sakakura, K.; Yahagi, K.; Joner, M.; Virmani, R. Has our understanding of calcification in human coronary atherosclerosis progressed? Arterioscler. Thromb. Vasc. Biol. 2014, 34, 724–736. [Google Scholar] [CrossRef]
- Virmani, R.; Joner, M.; Sakakura, K. Recent highlights of ATVB: Calcification. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1329–1332. [Google Scholar] [CrossRef]
- Yahagi, K.; Kolodgie, F.D.; Otsuka, F.; Finn, A.V.; Davis, H.R.; Joner, M.; Virmani, R. Pathophysiology of native coronary, vein graft, and in-stent atherosclerosis. Nat. Rev. Cardiol. 2016, 13, 79–98. [Google Scholar] [CrossRef]
- Maguire, E.M.; Pearce, S.W.A.; Xiao, Q. Foam cell formation: A new target for fighting atherosclerosis and cardiovascular disease. Vasc. Pharmacol. 2019, 112, 54–71. [Google Scholar] [CrossRef]
- Lundberg, A.M.; Hansson, G.K. Innate immune signals in atherosclerosis. Clin. Immunol. 2010, 134, 5–24. [Google Scholar] [CrossRef]
- Nakazawa, G.; Otsuka, F.; Nakano, M.; Vorpahl, M.; Yazdani, S.K.; Ladich, E.; Kolodgie, F.D.; Finn, A.V.; Virmani, R. The Pathology of Neoatherosclerosis in Human Coronary Implants: Bare-Metal and Drug-Eluting Stents. J. Am. Coll. Cardiol. 2011, 57, 1314–1322. [Google Scholar] [CrossRef]
- Farb, A.; Kolodgie, F.D.; Hwang, J.-Y.; Burke, A.P.; Tefera, K.; Weber, D.K.; Wight, T.N.; Virmani, R. Extracellular Matrix Changes in Stented Human Coronary Arteries. Circulation 2004, 110, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Paneni, F.; Beckman, J.; Creager, M.A.; Cosentino, F. Diabetes and vascular disease: Pathophysiology, clinical consequences, and medical therapy: Part I. Eur. Hear. J. 2013, 34, 2436–2443. [Google Scholar] [CrossRef]
- Chahil, T.J.; Ginsberg, H.N. Diabetic dyslipidemia. Endocrinol. Metab. Clin. N. Am. 2006, 35, 491–510, vii–viii. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M. Hypertriglyceridemia, insulin resistance, and the metabolic syndrome. Am. J. Cardiol. 1999, 83, 25F–29F. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Cushman, M.; Stampfer, M.J.; Tracy, R.P.; Hennekens, C.H. Plasma Concentration of C-Reactive Protein and Risk of Developing Peripheral Vascular Disease. Circulation 1998, 97, 425–428. [Google Scholar] [CrossRef]
- Kawashima, S.; Yokoyama, M. Dysfunction of Endothelial Nitric Oxide Synthase and Atherosclerosis. Arter. Thromb. Vasc. Biol. 2004, 24, 998–1005. [Google Scholar] [CrossRef]
- Vinik, A.I.; Erbas, T.; Park, T.S.; Nolan, R.; Pittenger, G.L. Platelet Dysfunction in Type 2 Diabetes. Diabetes Care 2001, 24, 1476–1485. [Google Scholar] [CrossRef]
- Pradhan, A.D.; Manson, J.E.; Rifai, N.; Buring, J.E.; Ridker, P.M. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA 2001, 286, 327–334. [Google Scholar] [CrossRef]
- Pickup, J.C.; Chusney, G.D.; Thomas, S.M.; Burt, D. Plasma interleukin-6, tumour necrosis factor alpha and blood cytokine production in type 2 diabetes. Life Sci. 2000, 67, 291–300. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis is an inflammatory disease. Am. Heart J. 1999, 138, S419–S420. [Google Scholar] [CrossRef]
- Beckman, J.A.; Creager, M.A.; Libby, P. Diabetes and atherosclerosis: Epidemiology, pathophysiology, and management. JAMA 2002, 287, 2570–2581. [Google Scholar] [CrossRef] [PubMed]
- De Vriese, A.S.; Verbeuren, T.J.; Van de Voorde, J.; Lameire, N.H.; Vanhoutte, P.M. Endothelial dysfunction in diabetes. Br. J. Pharmacol. 2000, 130, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Troidl, K.; Schaper, W. Arteriogenesis versus angiogenesis in peripheral artery disease. Diabetes/Metab. Res. Rev. 2012, 28, 27–29. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, L.A.; Poot, M.; Gerrity, R.G.; Bornfeldt, K.E. Diabetes accelerates smooth muscle accumulation in lesions of atherosclerosis: Lack of direct growth-promoting effects of high glucose levels. Diabetes 2001, 50, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Radomski, M.W.; Palmer, R.M.; Moncada, S. The role of nitric oxide and cGMP inplatelet adhesion to vascular endothelium. Biochem. Biophys. Res. Commun. 1987, 148, 1482–1489. [Google Scholar] [CrossRef]
- Steinberg, H.O.; Baron, A.D. Vascular function, insulin resistance and fatty acids. Diabetologia 2002, 45, 623–634. [Google Scholar] [CrossRef]
- Sarkar, R.; Meinberg, E.G.; Stanley, J.C.; Gordon, D.; Webb, R.C. Nitric Oxide Reversibly Inhibits the Migration of Cultured Vascular Smooth Muscle Cells. Circ. Res. 1996, 78, 225–230. [Google Scholar] [CrossRef]
- Uemura, S.; Matsushita, H.; Li, W.; Glassford, A.J.; Asagami, T.; Lee, K.H.; Harrison, D.G.; Tsao, P.S. Diabetes mellitus enhances vascular matrix metalloproteinase activity: Role of oxidative stress. Circ Res. 2001, 88, 1291–1298. [Google Scholar] [CrossRef]
- Johnstone, M.T.; Creager, S.J.; Scales, K.M.; Cusco, J.A.; Lee, B.K.; Creager, M.A. Impaired endothelium-dependent vasodilation in patients with insulin-dependent diabetes mellitus. Circulation 1993, 88, 2510–2516. [Google Scholar] [CrossRef]
- Inoue, T.; Croce, K.; Morooka, T.; Sakuma, M.; Node, K.; Simon, D.I. Vascular Inflammation and Repair: Implications for Re-Endothelialization, Restenosis, and Stent Thrombosis. JACC Cardiovasc. Interv. 2011, 4, 1057–1066. [Google Scholar] [CrossRef]
- Simon, D.I. Inflammation and Vascular Injury. Circ. J. 2012, 76, 1811–1818. [Google Scholar] [CrossRef] [PubMed]
- Demyanets, S.; Tentzeris, I.; Jarai, R.; Katsaros, K.M.; Farhan, S.; Wonnerth, A.; Weiss, T.W.; Wojta, J.; Speidl, W.S.; Huber, K. An increase of interleukin-33 serum levels after coronary stent implantation is associated with coronary in-stent restenosis. Cytokine 2014, 67, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Schillinger, M.; Minar, E. Restenosis after percutaneous angioplasty: The role of vascular inflammation. Vasc. Risk. Manag. 2005, 1, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Schwartz, D.; Brogi, E.; Tanaka, H.; Clinton, S.K. A cascade model for restenosis. A special case of atherosclerosisprogression. Circulation 1992, 86 (Suppl. S6), III47–52. [Google Scholar]
- Guimaraes, T.S.; da Rocha, L.A.; Becari, C.; Piccinato, C.E.; Joviliano, R.D.; Ribeiro, M.; Joviliano, E.E. The Role of Interleukins and Inflammatory Markers in the Early Restenosis of Covered Stents in the Femoropopliteal Arterial Segment. Ann. Vasc. Surg. 2018, 50, 88–95. [Google Scholar] [CrossRef]
- Araújo, P.V.; Ribeiro, M.S.; Dalio, M.B.; Rocha, L.A.; Viaro, F.; Joviliano, R.D.; Piccinato, C.E.; Évora, P.R.B.; Joviliano, E.E. Interleukins and Inflammatory Markers in In-Stent Restenosis after Femoral Percutaneous Transluminal Angioplasty. Ann. Vasc. Surg. 2015, 29, 731–737. [Google Scholar] [CrossRef]
- Jiang, Z.; Tao, M.; Omalley, K.A.; Wang, D.; Ozaki, C.K.; Berceli, S.A. Established neointimal hyperplasia in vein grafts expands via TGF-β-mediated progressive fibrosis. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, H1200–H1207. [Google Scholar] [CrossRef]
- Signorelli, S.S.; Anzaldi, M.; Libra, M.; Navolanic, P.M.; Malaponte, G.; Mangano, K.; Quattrocchi, C.; Marco, D.R.; Fiore, V.; Neri, S. Plasma Levels of Inflammatory Biomarkers in Peripheral Arterial Disease: Results of a Cohort Study. Angiology 2016, 67, 870–874. [Google Scholar] [CrossRef]
- Barani, J.; Nilsson, J.; Mattiasson, I.; Lindblad, B.; Gottsäter, A. Inflammatory mediators are associated with 1-year mortality in critical limb ischemia. J. Vasc. Surg. 2005, 42, 75–80. [Google Scholar] [CrossRef]
- Di, X.; Han, W.; Liu, C.-W.; Ni, L.; Zhang, R. A systematic review and meta-analysis on the association between C-reactive protein levels and adverse limb events after revascularization in patients with peripheral arterial disease. J. Vasc. Surg. 2021, 74, 317–326. [Google Scholar] [CrossRef]
- Bleda, S.; de Haro, J.; Varela, C.; Acin, F. C-reactive protein and endovascular treatment of lower limb peripheral artery disease: An independent prognostic factor. J. Endovasc. Ther. 2015, 22, 233–239. [Google Scholar] [CrossRef]
- Singh, T.; Morris, D.; Smith, S.; Moxon, J.; Golledge, J. Systematic Review and Meta-Analysis of the Association Between C-Reactive Protein and Major Cardiovascular Events in Patients with Peripheral Artery Disease. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Schillinger, M.; Exner, M.; Mlekusch, W.; Haumer, M.; Rumpold, H.; Ahmadi, R.; Sabeti, S.; Wagner, O.; Minar, E. Endovascular Revascularization Below the Knee: 6-month Results and Predictive Value of C-reactive Protein Level. Radiology 2003, 227, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-W.; Hsu, L.-A.; Chen, C.-C.; Yeh, J.-T.; Sun, J.-H.; Lin, C.-H.; Chen, S.-T.; Hsu, B.R.-S.; Huang, Y.-Y. C-reactive protein as an outcome predictor for percutaneous transluminal angioplasty in diabetic patients with peripheral arterial disease and infected foot ulcers. Diabetes Res. Clin. Pract. 2010, 90, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Bleda, S.; De Haro, J.; Acin, F.; Varela, C.; Esparza, L.; de Maturana, I.L. Inflammatory Burden Predicts Long-Term Outcomes in Endovascular Therapy in Peripheral Arterial Disease. Ann. Vasc. Surg. 2013, 27, 459–466. [Google Scholar] [CrossRef]
- Kotschy, D.; Kotschy, M.; Masłowski, L.; Socha, P.; Kwapisz, J.; Czyżewska-Buczyńska, A.; Witkiewicz, W. Inflammatory markers in peripheral arterial disease patients after endovascular revascularization with new restenosis. Acta Angiol. 2014, 20, 47–59. [Google Scholar]
- Biscetti, F.; Ferraro, P.M.; Hiatt, W.R.; Angelini, F.; Nardella, E.; Cecchini, A.L.; Santoliquido, A.; Pitocco, D.; Landolfi, R.; Flex, A. Inflammatory Cytokines Associated with Failure of Lower-Extremity Endovascular Revascularization (LER): A Prospective Study of a Population with Diabetes. Diabetes Care 2019, 42, 1939–1945. [Google Scholar] [CrossRef]
- Straface, G.; Biscetti, F.; Pitocco, D.; Bertoletti, G.; Misuraca, M.; Vincenzoni, C.; Snider, F.; Arena, V.; Stigliano, E.; Angelini, F.; et al. Assessment of the Genetic Effects of Polymorphisms in the Osteoprotegerin Gene, TNFRSF11B, on Serum Osteoprotegerin Levels and Carotid Plaque Vulnerability. Stroke 2011, 42, 3022–3028. [Google Scholar] [CrossRef]
- Augoulea, A.; Vrachnis, N.; Lambrinoudaki, I.; Dafopoulos, K.; Iliodromiti, Z.; Daniilidis, A.; Varras, M.; Alexandrou, A.; Deligeoroglou, E.; Creatsas, G. Osteoprotegerin as a Marker of Atherosclerosis in Diabetic Patients. Int. J. Endocrinol. 2013, 2013, 182060. [Google Scholar] [CrossRef]
- Biscetti, F.; Porreca, C.F.; Bertucci, F.; Straface, G.; Santoliquido, A.; Tondi, P.; Angelini, F.; Pitocco, D.; Santoro, L.; Gasbarrini, A.; et al. TNFRSF11B gene polymorphisms increased risk of peripheral arterial occlusive disease and critical limb ischemia in patients with type 2 diabetes. Acta Diabetol. 2014, 51, 1025–1032. [Google Scholar] [CrossRef]
- Giovannini, S.; Tinelli, G.; Biscetti, F.; Straface, G.; Angelini, F.; Pitocco, D.; Mucci, L.; Landolfi, R.; Flex, A. Serum high mobility group box-1 and osteoprotegerin levels are associated with peripheral arterial disease and critical limb ischemia in type 2 diabetic subjects. Cardiovasc. Diabetol. 2017, 16, 99. [Google Scholar] [CrossRef] [PubMed]
- Protogerou, A.; Zampeli, E.; Fragiadaki, K.; Stamatelopoulos, K.; Papamichael, C.; Sfikakis, P. A pilot study of endothelial dysfunction and aortic stiffness after interleukin-6 receptor inhibition in rheumatoid arthritis. Atherosclerosis 2011, 219, 734–736. [Google Scholar] [CrossRef]
- Li, L.; Renier, G. The Connection between C-Reactive Protein (CRP) and Diabetic Vasculopathy. Focus on Preclinical Findings. Curr. Diabetes Rev. 2010, 6, 27–34. [Google Scholar] [CrossRef]
- Mai, J.; Virtue, A.; Shen, J.; Wang, H.; Yang, X.-F. An evolving new paradigm: Endothelial cells—Conditional innate immune cells. J. Hematol. Oncol. 2013, 6, 61. [Google Scholar] [CrossRef] [PubMed]
- Erlandsson, H.H.; Andersson, U. Mini-Review: The Nuclear Protein hmgb1 as a Proinflammatory Mediator. Eur. J. Immunol. 2004, 34, 1503–1512. [Google Scholar] [CrossRef]
- Kalinina, N.; Agrotis, A.; Tararak, E.; Antropova, Y.; Kanellakis, P.; Ilyinskaya, O.; Bobik, A. Increased Expression of the Dna-Binding Cytokine HMBG1 in Human Atherosclerotic Lesions: Role of Activated Macrophages and Cytokines. Cardiovasc. Pathol. 2004, 13, 97–98. [Google Scholar] [CrossRef]
- Biscetti, F.; Straface, G.; De Cristofaro, R.; Lancellotti, S.; Rizzo, P.; Arena, V.; Stigliano, E.; Pecorini, G.; Egashira, K.; De Angelis, G.; et al. High-Mobility Group Box-1 Protein Promotes Angiogenesis After Peripheral Ischemia in Diabetic Mice Through a VEGF-Dependent Mechanism. Diabetes 2010, 59, 1496–1505. [Google Scholar] [CrossRef]
- Oozawa, S.; Sano, S.; Nishibori, M. Usefulness of high mobility group box 1 protein as a plasma biomarker in patient with peripheral artery disease. Acta Med. Okayama 2014, 68, 157–162. [Google Scholar]
- Papa, A.; Emdin, M.; Passino, C.; Michelassi, C.; Battaglia, D.; Cocci, F. Predictive value of elevated neutrophil–lymphocyte ratio on cardiac mortality in patients with stable coronary artery disease. Clin. Chim. Acta 2008, 395, 27–31. [Google Scholar] [CrossRef]
- Ferrante, G.; Niccoli, G.; Biasucci, L.M.; Liuzzo, G.; Burzotta, F.; Galiuto, L.; Trani, C.; Rebuzzi, A.G.; Crea, F. Association between C-reactive protein and angiographic restenosis after bare metal stents: An updated and comprehensive meta-analysis of 2747 patients. Cardiovasc. Revasc. Med. 2008, 9, 156–165. [Google Scholar] [CrossRef]
- Rahel, B.M.; Visseren, F.L.; Suttorp, M.J.; Plokker, T.H.; Kelder, J.C.; de Jongh, B.M.; Bouter, K.P.; Diepersloot, R.J. Preprocedural serum levels of acute phase reactants and prognosis after percutaneous coronary intervention. Cardiovasc. Res. 2003, 60, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Turak, O.; Ozcan, F.; Isleyen, A.; Tok, D.; Sokmen, E.; Buyukkaya, E.; Aydogdu, S.; Akpek, M.; Kaya, M.G. Usefulness of the Neutrophil-to-Lymphocyte Ratio to Predict Bare-Metal Stent Restenosis. Am. J. Cardiol. 2012, 110, 1405–1410. [Google Scholar] [CrossRef] [PubMed]
- Chang, Z.; Zheng, J.; Liu, Z.; Guo, Q. The Relationship Between the Neutrophil-Lymphocyte Ratio and In-Stent Restenosis in Patients with Femoropopliteal Chronic Total Occlusions. Angiology 2018, 69, 177–182. [Google Scholar] [CrossRef]
- Yang, Y.; Ge, F.; Shen, J.; Song, J.; Xie, J.; Qu, J.; Mao, X.; Kuang, Z.; Wang, X.; Wu, Y.; et al. The relationship between neutrophil–lymphocyte ratio and in-stent restenosis in superficial femoral artery. Biosci. Rep. 2020, 40, BSR20193448. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Puckridge, P.; Ullah, S.; Delaney, C.; Spark, J.I. Neutrophil-lymphocyte ratio as a prognostic marker of outcome in infrapopliteal percutaneous interventions for critical limb ischemia. J. Vasc. Surg. 2014, 60, 661–668. [Google Scholar] [CrossRef]
- Lee, S.; Hoberstorfer, T.; Wadowski, P.P.; Kopp, C.W.; Panzer, S.; Gremmel, T. Platelet-to-lymphocyte and Neutrophil-to-lymphocyte ratios predict target vessel restenosis after infrainguinal angioplasty with stent implantation. J. Clin. Med. 2020, 9, 1729. [Google Scholar] [CrossRef]
- Schwarzwalder, U.; Zeller, T. Below-the-knee revascularization. Advanced techniques. J. Cardiovasc. Surg. 2009, 50, 627–634. [Google Scholar]
- Ganjali, S.; Mansouri, A.; Abbasifard, M.; Moallem, S.A.; Tayarani-Najaran, Z.; Sahebkar, A. Association between Oxidative Burden and Restenosis: A Case-Control Study. Oxidative Med. Cell. Longev. 2022, 2022, 3577761. [Google Scholar] [CrossRef]
- Migdalski, A.; Jawień, A.; Kotschy, M.; Knapik-Bieniek, A. Selected haemostatic factors in carotid bifurcation plaques of patients undergoing carotid endarterectomy. Eur. J. Vasc. Endovasc. Surg. 2004, 27, 172–179. [Google Scholar] [CrossRef]
- Migdalski, A.; Kotschy, M.; Jawien, A. Tissue Factor, Tissue Factor Pathway Inhibitor and Vascular Endothelial Growth Factor-A in Carotid Atherosclerotic Plaques. Eur. J. Vasc. Endovasc. Surg. 2005, 30, 41–47. [Google Scholar] [CrossRef]
- Ross, R. The pathogenesis of atherosclerosis: A perspective for the 1990s. Nature 1993, 362, 801–809. [Google Scholar] [CrossRef]
- Kotschy, M.; Kotschy, D.; Witkiewicz, W. Rola czynnika tkankowego i jego inhibitora w procesie krzepnięcia krwioraz w powikłaniach zakrzepowych. Kardiol. Pol. 2010, 10, 1158–1162. [Google Scholar]
- Strano, A.; Hoppensteadt, D.; Walenga, J.M.; Fareed, J.; Sabbá, C.; Berardi, E.; Allegra, C.; Carlizza, A.; Binaghi, F.; Fronteddu, F.; et al. Plasma levels of the molecular markers of coagulation and fibrinolysis inpatients with peripheral arterial disease. Semin. Thromb. Hemost. 1996, 22 (Suppl. S1), 35–40. [Google Scholar] [PubMed]
- Grinnel, B.W.; Berg, D.T. Surface thrombomodulin modulatestrombin receptor responses on vascular smooth muscle cells. Am. J. Physiol. 1996, 270, H603–H609. [Google Scholar]
- Blann, A.D.; Naqvi, T.; Waite, M.; McCollum, C.N. Von Willebrandfactor and endothelial damage in essential hypertension. J. Hum. Hypertens. 1993, 7, 107–111. [Google Scholar]
- Steffel, J.; Lüscher, T.F.; Tanner, F.C. Tissue factor in cardiovasculardiseases: Molecular mechanisms and clinical implications. Circulation 2006, 113, 722–731. [Google Scholar] [CrossRef]
- Monaco, M.; Di Tommaso, L.; Stassano, P.; Smimmo, R.; De, A.V.; Pantaleo, A.; Pinna, G.B.; Iannelli, G. Impact of blood coagulationand fibrinolytic system changes on early and mid term clinical outcomein patients undergoing stent endografting surgery. Interact. Cardiovasc. Thorac. Surg. 2006, 5, 724–728. [Google Scholar] [CrossRef]
- Kotschy, D.; Kotschy, M.; Socha, P.; Masłowski, L.; Kwapisz, J.; Żuk, N.; Dubis, J.; Karczewski, M.; Witkiewicz, W. Tissue Factor and Other Hemostatic Parameters in Patients with Advanced Peripheral Artery Disease After Endovascular Revascularization—Search for Hemostatic Factors which Indicate Restenosis. Adv. Clin. Exp. Med. 2015, 24, 93–98. [Google Scholar] [CrossRef]
- Kalinin, R.E.; Suchkov, I.A.; Mzhavanadze, N.D.; Zhurina, O.N.; Klimentova, E.A.; Povarov, V.O. Coagulation Factor Activity and Hemostatic Markers of Endothelial Dysfunction in Patients with Peripheral Arterial Disease. Vasc. Speéc. Int. 2021, 37, 26. [Google Scholar] [CrossRef]
- Kotschy, D.; Kotschy, M.; Socha, P.; Masłowski, L.; Kwapisz, J.; Żuk, N.; Dubis, J.; Karczewski, M.; Witkiewicz, W. Wybrane śródbłonkowe markery hemostazy u pacjentów z miażdżycą tętnic kończyn dolnych po wewnątrznaczyniowej rewaskularyzacji i po powstaniu restenoz [Selected endothelial hemostatic markers in patients with peripheral arterial disease after endovascular revascularization and restenosis formation]. Postępy Hig. Med. Dosw. 2015, 69, 905–912. [Google Scholar] [CrossRef]
- Baek, D.; Villén, J.; Shin, C.; Camargo, F.D.; Gygi, S.P.; Bartel, D.P. The impact of microRNAs on protein output. Nature 2008, 455, 64–71. [Google Scholar] [CrossRef]
- Chen, L.J.; Lim, S.H.; Yeh, Y.T.; Lien, S.C.; Chiu, J.J. Roles of microRNAs in atherosclerosis and restenosis. J. Biomed. Sci. 2012, 19, 79. [Google Scholar] [CrossRef]
- Yamakuchi, M. MicroRNAs in Vascular Biology. Int. J. Vasc. Med. 2012, 2012, 794898. [Google Scholar] [CrossRef] [PubMed]
- Gareri, C.; De Rosa, S.; Indolfi, C. MicroRNAs for Restenosis and Thrombosis after Vascular Injury. Circ. Res. 2016, 118, 1170–1184. [Google Scholar] [CrossRef] [PubMed]
- Polimeni, A.; De Rosa, S.; Indolfi, C. Vascular miRNAs After Balloon Angioplasty. Trends Cardiovasc. Med. 2013, 23, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Stojkovic, S.; Jurisic, M.; Kopp, C.W.; Koppensteiner, R.; Huber, K.; Wojta, J.; Gremmel, T. Circulating microRNAs identify patients at increased risk of in-stent restenosis after peripheral angioplasty with stent implantation. Atherosclerosis 2018, 269, 197–203. [Google Scholar] [CrossRef]
- Moreau, M.E.; Garbacki, N.; Molinaro, G.; Brown, N.J.; Marceau, F.; Adam, A. The Kallikrein-Kinin System: Current and Future Pharmacological Targets. J. Pharmacol. Sci. 2005, 99, 6–38. [Google Scholar] [CrossRef]
- De Gasparo, M. Angiotensin II and nitric oxide interaction. Heart Fail. Rev. 2002, 7, 347–358. [Google Scholar] [CrossRef]
- Rocha, L.A.; Piccinato, C.E.; Ribiero, M.S.; Becari, C.; Joviliano, R.D.; Joviliano, E.E. The role of the kallikrein-kinin system, matrix metalloproteinases, and tissue inhibitors of metalloproteinases in the early restenosis of covered stents in the femoropopliteal arterial segment. J. Vasc. Surg. 2017, 65, 119–127. [Google Scholar] [CrossRef]
- Nagase, H.; Visse, R.; Murphy, G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc. Res. 2006, 69, 562–573. [Google Scholar] [CrossRef]
- Galis, Z.S.; Khatri, J.J. Matrix metalloproteinases in vascular remodeling and atherogenesis: The good, the bad, and the ugly. Circ. Res. 2002, 90, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Newby, A.C. Matrix metalloproteinases regulate migration, proliferation, and death of vascular smooth muscle cells by degrading matrix and non-matrix substrates. Cardiovasc. Res. 2006, 69, 614–624. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.M.; Kandasamy, A.D.; Youssef, N.; Schulz, R. Matrix metalloproteinase inhibitor properties of tetracyclines: Therapeutic potential in cardiovascular diseases. Pharmacol. Res. 2011, 64, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.M.; Tanus-Santos, J.E.; Gerlach, R.F. Matrix metal- loproteinases: Targets for doxycycline to prevent the vascular alterations of hypertension. Pharmacol. Res. 2011, 64, 567–572. [Google Scholar] [CrossRef]
- Chen, Q.; Jin, M.; Yang, F.; Zhu, J.; Xiao, Q.; Zhang, L. Matrix Metalloproteinases: Inflammatory Regulators of Cell Behaviors in Vascular Formation and Remodeling. Mediat. Inflamm. 2013, 2013, 928315. [Google Scholar] [CrossRef]
- Poulsen, M.K.; Nybo, M.; Dahl, J.; Hosbond, S.; Poulsen, T.S.; Johansen, A.; Høilund-Carlsen, P.F.; Beck-Nielsen, H.; Rasmussen, L.M.; Henriksen, J.E. Plasma osteoprotegerin is related to carotid and peripheral arterial disease, but not to myocardial ischemia in type 2 diabetes mellitus. Cardiovasc. Diabetol. 2011, 10, 76. [Google Scholar] [CrossRef]
- Hosbond, S.E.; Poulsen, T.S.; Diederichsen, A.C.P.; Nybo, M.; Rasmussen, L.M.; Mickley, H. Osteoprotegerin as a marker of atherosclerosis: A systematic update. Scand. Cardiovasc. J. 2012, 46, 203–211. [Google Scholar] [CrossRef]
- Venuraju, S.M.; Yerramasu, A.; Corder, R.; Lahiri, A. Osteoprotegerin as a Predictor of Coronary Artery Disease and Cardiovascular Mortality and Morbidity. J. Am. Coll. Cardiol. 2010, 55, 2049–2061. [Google Scholar] [CrossRef]
- Bucay, N.; Sarosi, I.; Dunstan, C.; Morony, S.; Tarpley, J.; Capparelli, C.; Scully, S.; Tan, H.L.; Xu, W.; Lacey, D.L.; et al. osteoprotegerin-deficient mice develop early onset osteoporosis and arterial calcification. Genes Dev. 1998, 12, 1260–1268. [Google Scholar] [CrossRef]
- Kadoglou, N.P.E.; Kapetanios, D.; Korakas, E.; Valsami, G.; Tentolouris, N.; Papanas, N.; Lambadiari, V.; Karkos, C. Association of serum levels of osteopontin and osteoprotegerin with adverse outcomes after endovascular revascularisation in peripheral artery disease. Cardiovasc. Diabetol. 2022, 21, 171. [Google Scholar] [CrossRef]
- Eleftheriadou, I.; Tsilingiris, D.; Tentolouris, A.; Mourouzis, I.; Grigoropoulou, P.; Kapelios, C.; Pantos, C.; Makrilakis, K.; Tentolouris, N. Association of Circulating Osteopontin Levels with Lower Extremity Arterial Disease in Subjects With Type 2 Diabetes Mellitus: A Cross-Sectional Observational Study. Int. J. Low. Extremity Wounds 2020, 19, 180–189. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Stage | Inclusion/Exclusion Criteria | Stage Results |
|---|---|---|
| 1. Initial search | Scopus query (November, 2022): TITLE-ABS-KEY (restenosis) AND KEY (markers or «risk factors») AND (PUBYEAR AFT 2017) AND (PUBYEAR BEF 2023) | 1781 publ. |
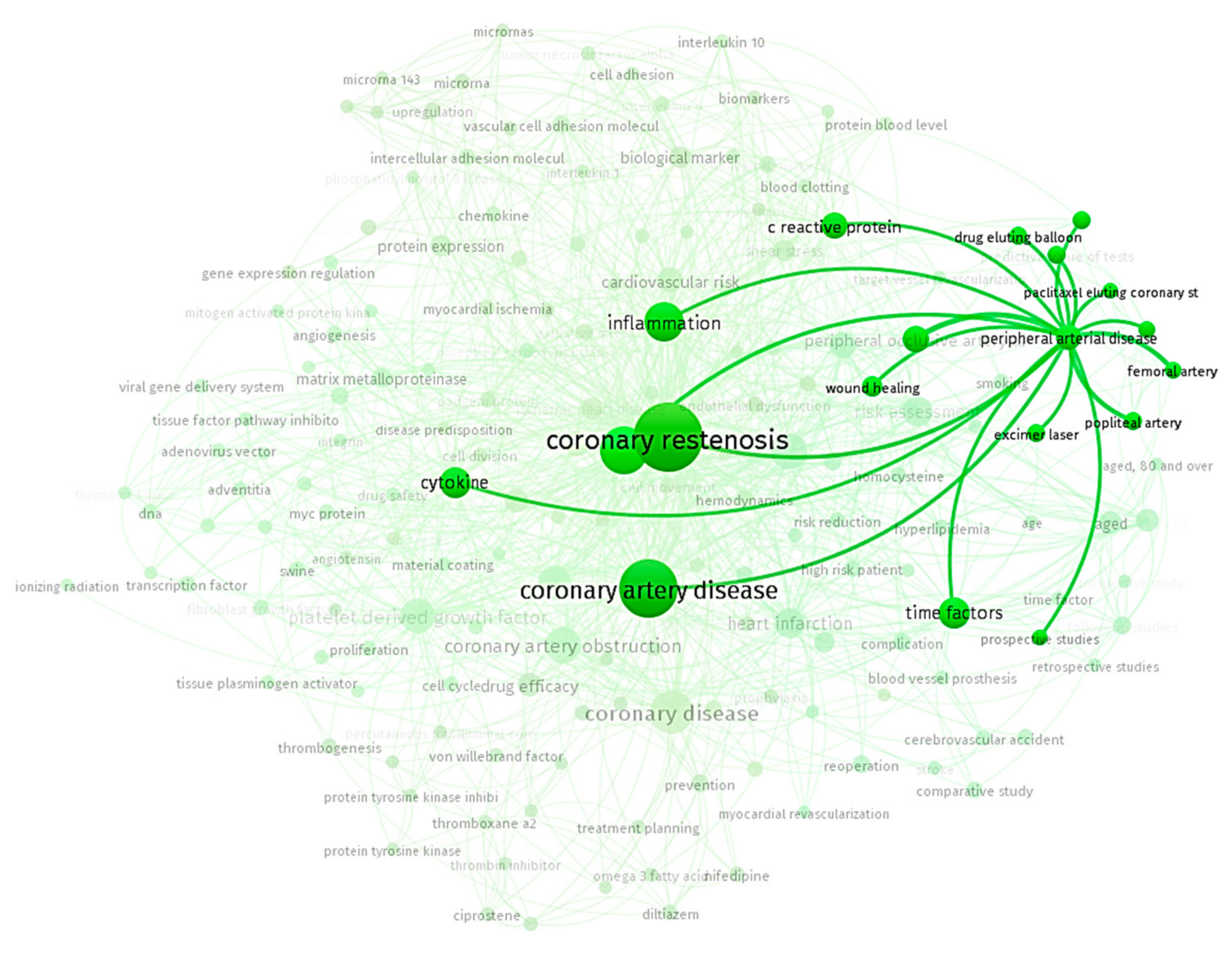
| 2. Analysis | The bibliometric analysis revealed an imbalance in covering the problems of predictors of restenosis in the arteries of lower extremities and coronary arteries | |
| 3. Record exclusion | Excluded publications, which do not contain the keywords “limb ischemia”, “peripheral arteries”, “femoropopliteal arterial” | 48 reviews, 139 articles |
| 4. Sample expansion | All cited documents from the stage 2 sample | 8136 publ. |
| 5. Record exclusion | Exclude publications that do not contain “angioplasty” in TITLE-ABS-KEY | 651 |
| 6. Screening | Examine titles and abstracts by reviewers to exclude articles that do not meet the aims of the paper | 13 reviews, 93 articles |
| Links of Pathogenesis in Restenosis | Basic Mechanisms | Key Markers |
|---|---|---|
| Inflammatory process | 1. Association of C-reactive protein (CRP) and inflammatory responses with both PAD and DM [56,57]. 2. Promotes the production of procoagulant tissue factor, leukocyte adhesion molecules, and chemoattractants [19]. 3. Inhibits endothelial nitric oxide synthase (eNOS), => reducing nitric oxide (NO) [20,58]. 4. Promotes the production of plasminogen activator inhibitor (PAI)-1, thereby blocking the cleavage of plasminogen into plasmin (impairs the process of fibrinolysis) [59]. 5. An elevated level of (TNF)-α and IL-6 in T2D leads to the binding of cytokines to the receptors on the surface of endothelial cells, the synthesis of adhesion molecules of endothelial cells, which leads to an increase in the binding of leukocytes and platelets to the surface of the endothelium, thereby contributing to thrombosis [60,61,62]. | CRP, (eNOS), NO, (TGF-β), IL-6, IL-8, IL-12, (PAI)-1 |
| Endothelial dysfunction | 1. Endothelium is involved in the production of endothelin, NO, and reactive oxygen species [63,64]. 2. Hyperglycemia and insulin resistance: indirect effect of insulin on the NO production and relaxation of VSMCs [65,66]. 3. Insulin resistance leads to accumulation of free fatty acids => increase in free oxygen species and decreasing the NO concentration => cannot inhibit the platelet activation and limit migration, and proliferation of VSMC [66,67,68]; 4. Indirect effect on the transformation of macrophages into foam cells, leading to the onset of atherosclerotic plaque formation [20]. | Endothelin, NO, reactive oxygen species, free fatty acids |
| Migration of the VSMC | 1. Migration of VSMC from the medial layer to the intimal layer as a stabilization of the atherosclerotic plaque; it is not typical of patients with DM [19,69]. 2. Production of metalloproteinases that destroy collagen, thereby leading to plaque destabilization [70]. 3. Activation of the endothelin-A receptor on the surface of VSMCs, followed by the secretion of endothelin-1, causing pathological vasoconstriction [71]. | VSMC, endothelin-1 |
| Platelet dysfunction | 1. Activation of protein kinase C and decrease in NO concentration [48]. 2. Increased adhesion of platelets due to the increased expression of P-selectin on the surface of platelets [19]. 3. Increased expression of platelet receptors, such as glycoprotein Ib (which binds to von Willebrand factor) and IIb/IIIa receptors. These receptors mediate platelet adhesion and aggregation, thereby causing thrombosis [19]. | Protein kinase C, 3-selectin, glycoprotein Ib, IIb/IIIa receptors. |
| Coagulation | Activation of factor VIIa and tissue factor, suppression of anticoagulants such as antithrombin III, protein S and protein C [19]. | Factor VIIa and tissue factor, suppression of antithrombin III, protein S, and protein C |
| Blood rheology | Increased fibrinogen production [50]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobolevskaya, E.V.; Shumkov, O.A.; Smagin, M.A.; Guskov, A.E.; Malysheva, A.V.; Atuchin, V.V.; Nimaev, V.V. Markers of Restenosis after Percutaneous Transluminal Balloon Angioplasty in Patients with Critical Limb Ischemia. Int. J. Mol. Sci. 2023, 24, 9096. https://doi.org/10.3390/ijms24109096
Sobolevskaya EV, Shumkov OA, Smagin MA, Guskov AE, Malysheva AV, Atuchin VV, Nimaev VV. Markers of Restenosis after Percutaneous Transluminal Balloon Angioplasty in Patients with Critical Limb Ischemia. International Journal of Molecular Sciences. 2023; 24(10):9096. https://doi.org/10.3390/ijms24109096
Chicago/Turabian StyleSobolevskaya, Elvira V., Oleg A. Shumkov, Mikhail A. Smagin, Andrey E. Guskov, Alexandra V. Malysheva, Victor V. Atuchin, and Vadim V. Nimaev. 2023. "Markers of Restenosis after Percutaneous Transluminal Balloon Angioplasty in Patients with Critical Limb Ischemia" International Journal of Molecular Sciences 24, no. 10: 9096. https://doi.org/10.3390/ijms24109096