
Peripheral Inflammatory Markers TNF-α and CCL2 Revisited: Association with Parkinson’s Disease Severity
 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Demographic and Clinical Characteristics
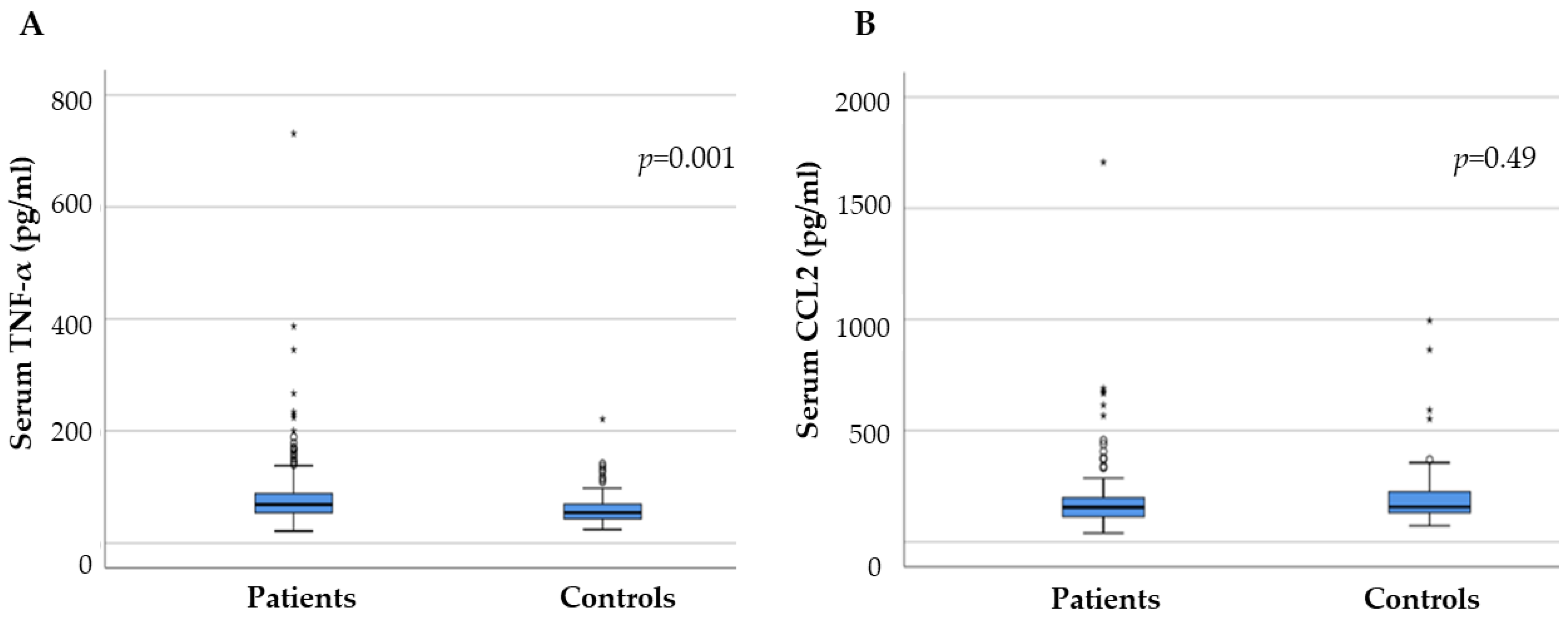
2.2. Serum Inflammatory Factors in PD and Control Groups
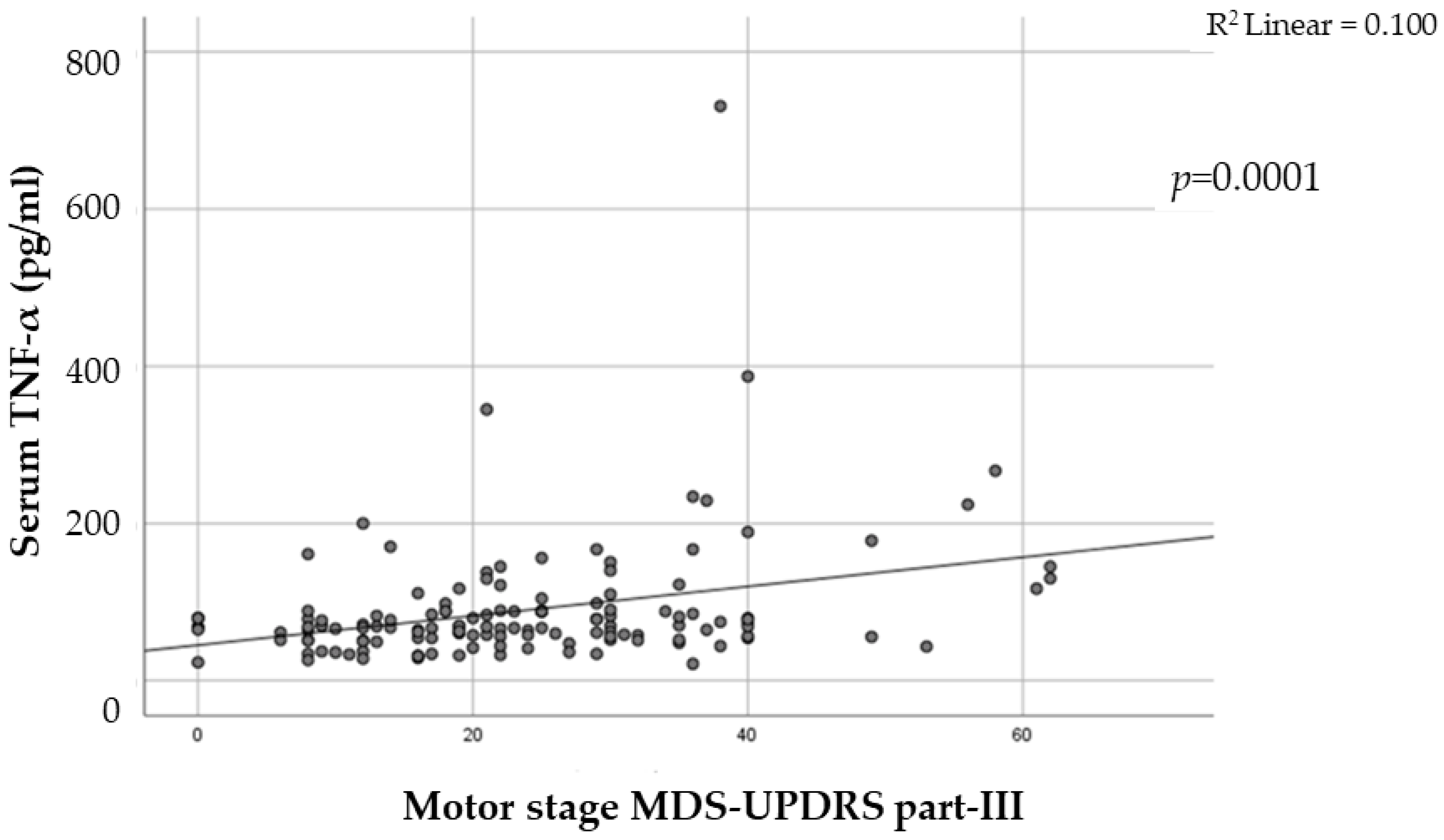
2.3. The Link between Inflammatory Factors and PD Severity
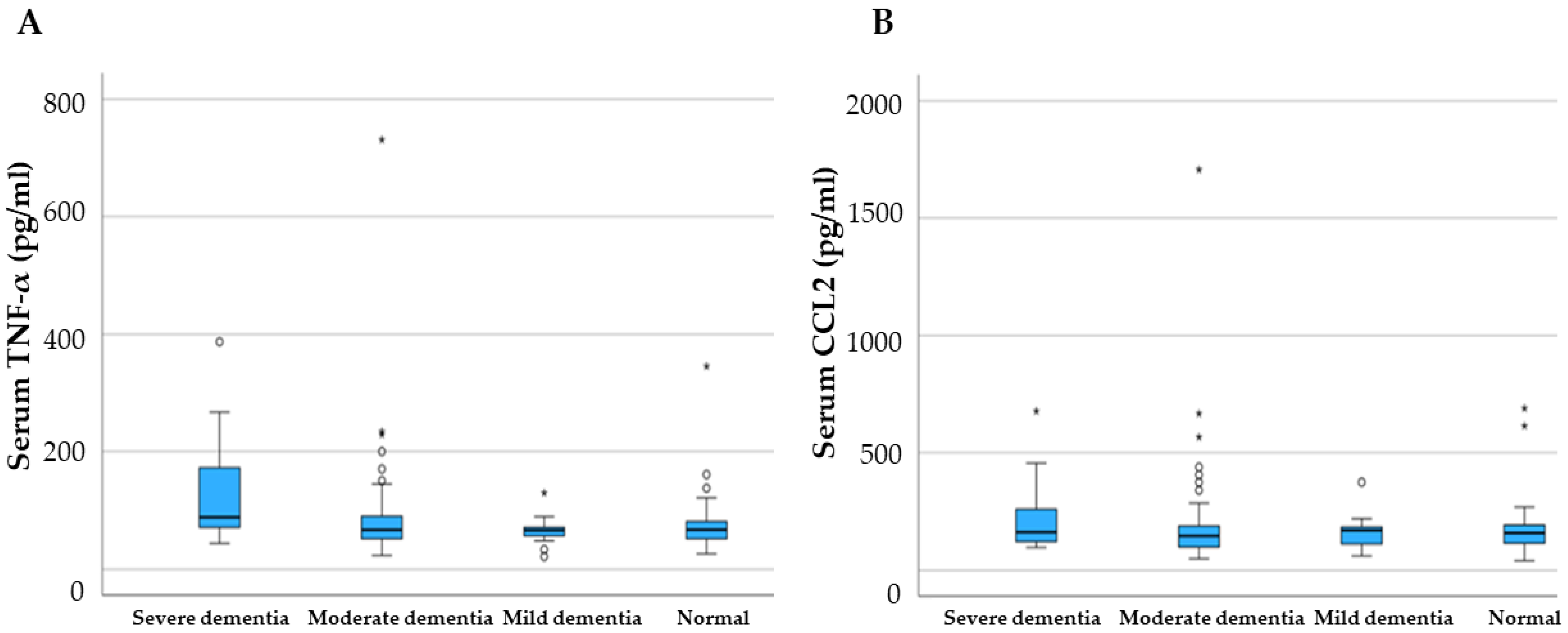
2.4. Cognitive Decline and Motor Phenotypes in PD and Inflammatory Factors
2.5. Main Association of PD with Cytokine Levels from Previous Analysis
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.2. Blood Sample and ELISA
4.3. Statistical Analysis
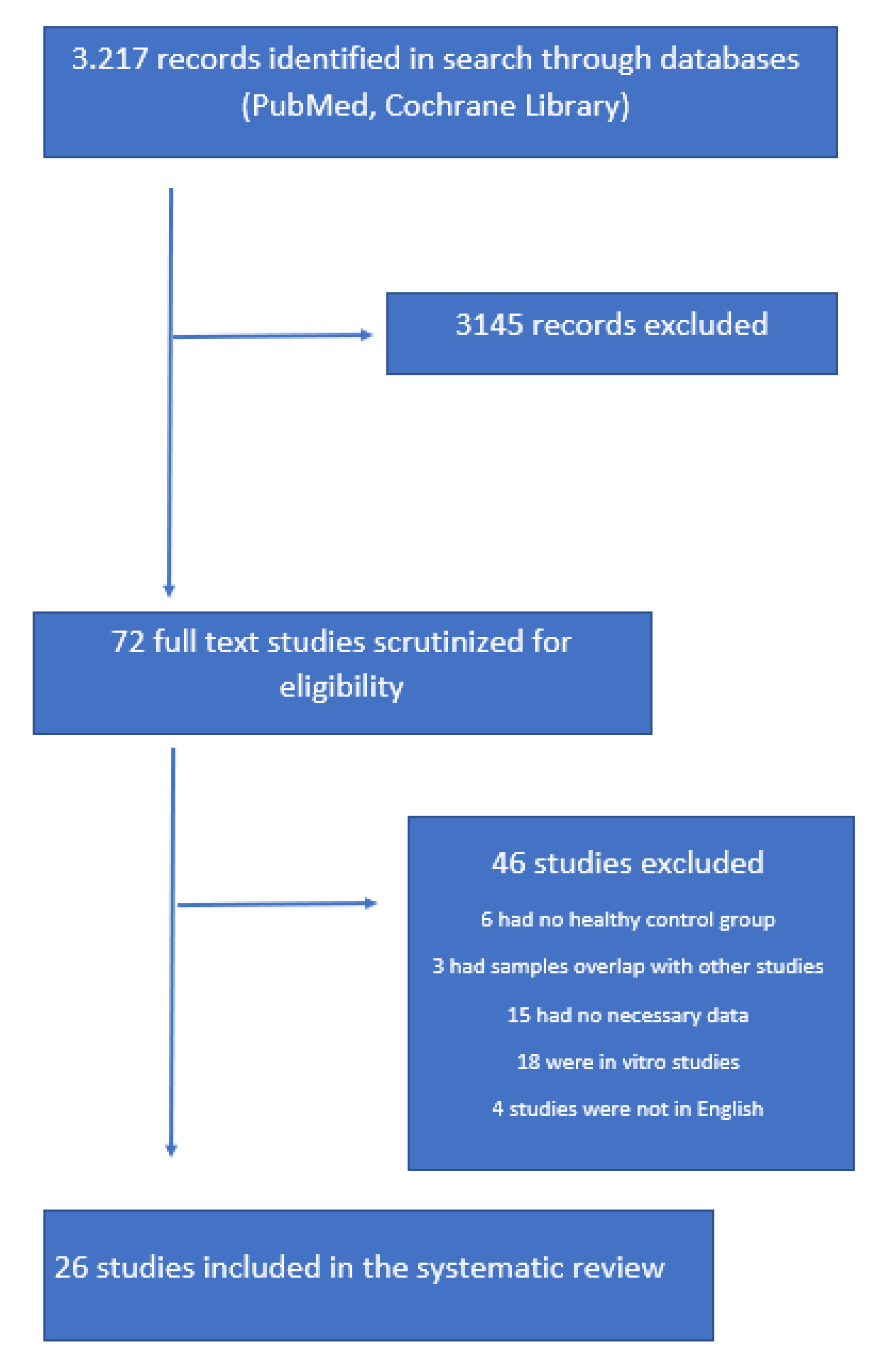
4.4. Search Strategy
4.5. Data Collection and Eligibility Criteria
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zesiewicz, T.A. Parkinson Disease. Contin. Minneap. Minn 2019, 25, 896–918. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Wang, J.; Zhao, Y.; Feng, Y.; Han, S.; Dong, Q.; Cui, M.; Tieu, K. Microglial Exosomes Facilitate α-Synuclein Transmission in Parkinson’s Disease. Brain J. Neurol. 2020, 143, 1476–1497. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.S. Microglia in Parkinson’s Disease. Adv. Exp. Med. Biol. 2019, 1175, 335–353. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.T.; Howell, J.C.; Ozturk, T.; Gangishetti, U.; Kollhoff, A.L.; Hatcher-Martin, J.M.; Anderson, A.M.; Tyor, W.R. CSF Cytokines in Aging, Multiple Sclerosis, and Dementia. Front. Immunol. 2019, 10, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Hu, Y.; Cao, Z.; Liu, Q.; Cheng, Y. Cerebrospinal Fluid Inflammatory Cytokine Aberrations in Alzheimer’s Disease, Parkinson’s Disease and Amyotrophic Lateral Sclerosis: A Systematic Review and Meta-Analysis. Front. Immunol. 2018, 9, 2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Esparcia, P.; Llorens, F.; Carmona, M.; Ferrer, I. Complex Deregulation and Expression of Cytokines and Mediators of the Immune Response in Parkinson’s Disease Brain Is Region Dependent. Brain Pathol. Zurich Switz. 2014, 24, 584–598. [Google Scholar] [CrossRef] [PubMed]
- Mondello, S.; Constantinescu, R.; Zetterberg, H.; Andreasson, U.; Holmberg, B.; Jeromin, A. CSF α-Synuclein and UCH-L1 Levels in Parkinson’s Disease and Atypical Parkinsonian Disorders. Parkinsonism Relat. Disord. 2014, 20, 382–387. [Google Scholar] [CrossRef]
- Zhao, Y.; Yang, G. Potential of Extracellular Vesicles in the Parkinson’s Disease-Pathological Mediators and Biomarkers. Neurochem. Int. 2021, 144, 104974. [Google Scholar] [CrossRef] [PubMed]
- Sampson, T.R.; Debelius, J.W.; Thron, T.; Janssen, S.; Shastri, G.G.; Ilhan, Z.E.; Challis, C.; Schretter, C.E.; Rocha, S.; Gradinaru, V.; et al. Gut Microbiota Regulate Motor Deficits and Neuroinflammation in a Model of Parkinson’s Disease. Cell 2016, 167, 1469–1480.e12. [Google Scholar] [CrossRef] [Green Version]
- Joers, V.; Masilamoni, G.; Kempf, D.; Weiss, A.R.; Rotterman, T.M.; Murray, B.; Yalcin-Cakmakli, G.; Voll, R.J.; Goodman, M.M.; Howell, L.; et al. Microglia, Inflammation and Gut Microbiota Responses in a Progressive Monkey Model of Parkinson’s Disease: A Case Series. Neurobiol. Dis. 2020, 144, 105027. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-J.; Chen, C.-C.; Liao, H.-Y.; Wu, Y.-W.; Liou, J.-M.; Wu, M.-S.; Kuo, C.-H.; Lin, C.-H. Alteration of Gut Microbial Metabolites in the Systemic Circulation of Patients with Parkinson’s Disease. J. Park. Dis. 2022, 12, 1219–1230. [Google Scholar] [CrossRef] [PubMed]
- Amin, R.; Quispe, C.; Docea, A.O.; Ydyrys, A.; Kulbayeva, M.; Durna Daştan, S.; Calina, D.; Sharifi-Rad, J. The Role of Tumour Necrosis Factor in Neuroinflammation Associated with Parkinson’s Disease and Targeted Therapies. Neurochem. Int. 2022, 158, 105376. [Google Scholar] [CrossRef] [PubMed]
- Shastri, A.; Bonifati, D.M.; Kishore, U. Innate Immunity and Neuroinflammation. Mediators Inflamm. 2013, 2013, 342931. [Google Scholar] [CrossRef]
- Harms, A.S.; Ferreira, S.A.; Romero-Ramos, M. Periphery and Brain, Innate and Adaptive Immunity in Parkinson’s Disease. Acta Neuropathol. 2021, 141, 527–545. [Google Scholar] [CrossRef]
- Jiang, S.; Gao, H.; Luo, Q.; Wang, P.; Yang, X. The Correlation of Lymphocyte Subsets, Natural Killer Cell, and Parkinson’s Disease: A Meta-Analysis. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2017, 38, 1373–1380. [Google Scholar] [CrossRef] [PubMed]
- Huerta, C.; Alvarez, V.; Mata, I.F.; Coto, E.; Ribacoba, R.; Martínez, C.; Blázquez, M.; Guisasola, L.M.; Salvador, C.; Lahoz, C.H.; et al. Chemokines (RANTES and MCP-1) and Chemokine-Receptors (CCR2 and CCR5) Gene Polymorphisms in Alzheimer’s and Parkinson’s Disease. Neurosci. Lett. 2004, 370, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Kalkonde, Y.V.; Morgan, W.W.; Sigala, J.; Maffi, S.K.; Condello, C.; Kuziel, W.; Ahuja, S.S.; Ahuja, S.K. Chemokines in the MPTP Model of Parkinson’s Disease: Absence of CCL2 and Its Receptor CCR2 Does Not Protect against Striatal Neurodegeneration. Brain Res. 2007, 1128, 1–11. [Google Scholar] [CrossRef]
- Kempuraj, D.; Thangavel, R.; Fattal, R.; Pattani, S.; Yang, E.; Zaheer, S.; Santillan, D.A.; Santillan, M.K.; Zaheer, A. Mast Cells Release Chemokine CCL2 in Response to Parkinsonian Toxin 1-Methyl-4-Phenyl-Pyridinium (MPP(+)). Neurochem. Res. 2016, 41, 1042–1049. [Google Scholar] [CrossRef] [Green Version]
- Reale, M.; Iarlori, C.; Thomas, A.; Gambi, D.; Perfetti, B.; Di Nicola, M.; Onofrj, M. Peripheral Cytokines Profile in Parkinson’s Disease. Brain. Behav. Immun. 2009, 23, 55–63. [Google Scholar] [CrossRef]
- Rajput, A.H.; Rajput, M.L.; Ferguson, L.W.; Rajput, A. Baseline Motor Findings and Parkinson Disease Prognostic Subtypes. Neurology 2017, 89, 138–143. [Google Scholar] [CrossRef]
- Lindqvist, D.; Kaufman, E.; Brundin, L.; Hall, S.; Surova, Y.; Hansson, O. Non-Motor Symptoms in Patients with Parkinson’s Disease-Correlations with Inflammatory Cytokines in Serum. PLoS ONE 2012, 7, e47387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, V.; Garg, R.K.; Khattri, S. Levels of IL-8 and TNF-α Decrease in Parkinson’s Disease. Neurol. Res. 2016, 38, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Eidson, L.N.; Kannarkat, G.T.; Barnum, C.J.; Chang, J.; Chung, J.; Caspell-Garcia, C.; Taylor, P.; Mollenhauer, B.; Schlossmacher, M.G.; Ereshefsky, L.; et al. Candidate Inflammatory Biomarkers Display Unique Relationships with Alpha-Synuclein and Correlate with Measures of Disease Severity in Subjects with Parkinson’s Disease. J. Neuroinflammation 2017, 14, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, Progression and Mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale Presentation and Clinimetric Testing Results: MDS-UPDRS: Clinimetric Assessment. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N.; Tsolaki, M.; Chantzi, H.; Kazis, A. Mini Mental State Examination (MMSE): A Validation Study in Greece. Am. J. Alzheimer’s Dis. Dementias 2000, 15, 342–345. [Google Scholar] [CrossRef]
- Konstantinopoulou, E.; Kosmidis, M.H.; Ioannidis, P.; Kiosseoglou, G.; Karacostas, D.; Taskos, N. Adaptation of Addenbrooke’s Cognitive Examination-Revised for the Greek Population. Eur. J. Neurol. 2011, 18, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Menza, M.; DeFronzo Dobkin, R.; Marin, H.; Mark, M.H.; Gara, M.; Bienfait, K.; Dicke, A.; Kusnekov, A. The Role of Inflammatory Cytokines in Cognition and Other Non-Motor Symptoms of Parkinson’s Disease. Psychosomatics 2010, 51, 474–479. [Google Scholar] [CrossRef] [Green Version]
- Ren, T.; Gao, Y.; Qiu, Y.; Jiang, S.; Zhang, Q.; Zhang, J.; Wang, L.; Zhang, Y.; Wang, L.; Nie, K. Gut Microbiota Altered in Mild Cognitive Impairment Compared with Normal Cognition in Sporadic Parkinson’s Disease. Front. Neurol. 2020, 11, 137. [Google Scholar] [CrossRef]
- Qin, X.-Y.; Zhang, S.-P.; Cao, C.; Loh, Y.P.; Cheng, Y. Aberrations in Peripheral Inflammatory Cytokine Levels in Parkinson Disease: A Systematic Review and Meta-Analysis. JAMA Neurol. 2016, 73, 1316–1324. [Google Scholar] [CrossRef]
- Wang, X.-M.; Zhang, Y.-G.; Li, A.-L.; Long, Z.-H.; Wang, D.; Li, X.-X.; Xia, J.-H.; Luo, S.-Y.; Shan, Y.-H. Relationship between Levels of Inflammatory Cytokines in the Peripheral Blood and the Severity of Depression and Anxiety in Patients with Parkinson’s Disease. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 3853–3856. [Google Scholar] [PubMed]
- Williams-Gray, C.H.; Wijeyekoon, R.; Yarnall, A.J.; Lawson, R.A.; Breen, D.P.; Evans, J.R.; Cummins, G.A.; Duncan, G.W.; Khoo, T.K.; Burn, D.J.; et al. Serum Immune Markers and Disease Progression in an Incident Parkinson’s Disease Cohort (ICICLE-PD). Mov. Disord. Off. J. Mov. Disord. Soc. 2016, 31, 995–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Usenko, T.S.; Nikolaev, M.A.; Miliukhina, I.V.; Bezrukova, A.I.; Senkevich, K.A.; Gomzyakova, N.A.; Beltceva, Y.A.; Zalutskaya, N.M.; Gracheva, E.V.; Timofeeva, A.A.; et al. Plasma Cytokine Profile in Synucleinophaties with Dementia. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2020, 78, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Csencsits-Smith, K.; Suescun, J.; Li, K.; Luo, S.; Bick, D.L.; Schiess, M. Serum Lymphocyte-Associated Cytokine Concentrations Change More Rapidly over Time in Multiple System Atrophy Compared to Parkinson Disease. Neuroimmunomodulation 2016, 23, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Schröder, J.B.; Pawlowski, M.; Meyer zu Hörste, G.; Gross, C.C.; Wiendl, H.; Meuth, S.G.; Ruck, T.; Warnecke, T. Immune Cell Activation in the Cerebrospinal Fluid of Patients with Parkinson’s Disease. Front. Neurol. 2018, 9, 1081. [Google Scholar] [CrossRef] [Green Version]
- Miliukhina, I.V.; Usenko, T.S.; Senkevich, K.A.; Nikolaev, M.A.; Timofeeva, A.A.; Agapova, E.A.; Semenov, A.V.; Lubimova, N.E.; Totolyan, A.A.; Pchelina, S.N. Plasma Cytokines Profile in Patients with Parkinson’s Disease Associated with Mutations in GBA Gene. Bull. Exp. Biol. Med. 2020, 168, 423–426. [Google Scholar] [CrossRef]
- Qin, L.; Wu, X.; Block, M.L.; Liu, Y.; Breese, G.R.; Hong, J.-S.; Knapp, D.J.; Crews, F.T. Systemic LPS Causes Chronic Neuroinflammation and Progressive Neurodegeneration. Glia 2007, 55, 453–462. [Google Scholar] [CrossRef] [Green Version]
- Harry, G.J.; Kraft, A.D. Neuroinflammation and Microglia: Considerations and Approaches for Neurotoxicity Assessment. Expert Opin. Drug Metab. Toxicol. 2008, 4, 1265–1277. [Google Scholar] [CrossRef]
- Park, J.-Y.; Paik, S.R.; Jou, I.; Park, S.M. Microglial Phagocytosis Is Enhanced by Monomeric Alpha-Synuclein, Not Aggregated Alpha-Synuclein: Implications for Parkinson’s Disease. Glia 2008, 56, 1215–1223. [Google Scholar] [CrossRef]
- Ma, Y.; Li, R.; Zhan, W.; Huang, X.; Zhang, Z.; Lv, S.; Wang, J.; Liang, L.; Jia, X. Role of BMI in the Relationship Between Dietary Inflammatory Index and Depression: An Intermediary Analysis. Front. Med. 2021, 8, 748788. [Google Scholar] [CrossRef]
- Liu, Y.; Li, H.; Wang, J.; Xue, Q.; Yang, X.; Kang, Y.; Li, M.; Xu, J.; Li, G.; Li, C.; et al. Association of Cigarette Smoking with Cerebrospinal Fluid Biomarkers of Neurodegeneration, Neuroinflammation, and Oxidation. JAMA Netw. Open 2020, 3, e2018777. [Google Scholar] [CrossRef] [PubMed]
- Diaz, K.; Kohut, M.L.; Russell, D.W.; Stegemöller, E.L. Peripheral Inflammatory Cytokines and Motor Symptoms in Persons with Parkinson’s Disease. Brain Behav. Immun.-Health 2022, 21, 100442. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, R.; Strafella, A.P.; Bernard, A.; Schulte, C.; van den Heuvel, L.; Schneiderhan-Marra, N.; Knorpp, T.; Joos, T.O.; Leypoldt, F.; Geritz, J.; et al. Serum Inflammatory Profile for the Discrimination of Clinical Subtypes in Parkinson’s Disease. Front. Neurol. 2018, 9, 1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, E.; O’Brien, J.T.; Donaghy, P.; Morris, C.; Barnett, N.; Olsen, K.; Martin-Ruiz, C.; Taylor, J.-P.; Thomas, A.J. Peripheral Inflammation in Prodromal Alzheimer’s and Lewy Body Dementias. J. Neurol. Neurosurg. Psychiatry 2018, 89, 339–345. [Google Scholar] [CrossRef]
- Zhang, T.; Wang, T.; Chen, X.; Zhao, Z.; Chen, Z. Gut Microbiota Relieves Inflammation in the Substantia Nigra of Chronic Parkinson’s Disease by Protecting the Function of Dopamine Neurons. Exp. Ther. Med. 2022, 23, 52. [Google Scholar] [CrossRef]
- Pinna, A.; Costa, G.; Serra, M.; Contu, L.; Morelli, M. Neuroinflammation and L-Dopa-Induced Abnormal Involuntary Movements in 6-Hydroxydopamine-Lesioned Rat Model of Parkinson’s Disease Are Counteracted by Combined Administration of a 5-HT1A/1B Receptor Agonist and A2A Receptor Antagonist. Neuropharmacology 2021, 196, 108693. [Google Scholar] [CrossRef]
- Espinosa-Cárdenas, R.; Arce-Sillas, A.; Álvarez-Luquin, D.; Leyva-Hernández, J.; Montes-Moratilla, E.; González-Saavedra, I.; Boll, M.C.; Garcia-Garcia, E.; Ángeles-Perea, S.; Fragoso, G.; et al. Immunomodulatory Effect and Clinical Outcome in Parkinson’s Disease Patients on Levodopa-Pramipexole Combo Therapy: A Two-Year Prospective Study. J. Neuroimmunol. 2020, 347, 577328. [Google Scholar] [CrossRef]
- Huang, J.; Hong, W.; Yang, Z.; Ding, J.; Ren, Y. Efficacy of Pramipexole Combined with Levodopa for Parkinson’s Disease Treatment and Their Effects on QOL and Serum TNF-α Levels. J. Int. Med. Res. 2020, 48, 300060520922449. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | PD Patients (142) |
|---|---|
| Mean age (range) | 65 (36–83) |
| Disease duration (years) mean (SD) | 7.5 (4) |
| Sex | M. = 87, F. = 55 |
| PD phenotype | Tremor dominant 49%, PIGD 28%, intermediate 23% |
| H and Y Stage * | Mild 49%, moderate 34%, severe 14% |
| Motor stage MDS-UPDRS part-III ** | Mild 49%, moderate 37%, severe 14% |
| Cognitive impairment MMSE *** | Normal 64%, mild 12%, moderate 20%, severe 4% |
| Family history | No 83% |
| Smoking | 19% |
| Other comorbidities: Diabetes | 16% |
| Hypertension | 47% |
| Dyslipidemia | 20% |
| Main Outcome | Studies * | PD Cases/Controls | p-Values |
|---|---|---|---|
| Lower TNF-α in cases versus controls | Choi et al., 2012 [1] | 8/13 | 0.6 |
| Gupta et al., 2016 [2] | 81/83 | <0.001 | |
| Eidson et al., 2017 [3] | 12/6 | <0.001 | |
| Li et al., 2018 [4] | 43/24 | 0.7 | |
| Rocha et al., 2018 [5] | 23/21 | <0.001 | |
| Higher TNF-α in cases versus controls | Brodacki et al., 2008 [6] | 48/20 | <0.005 |
| Gruden et al., 2012 [7] | 32/26 | <0.005 | |
| Koziorowski et al., 2012 [8] | 60/24 | <0.001 | |
| Bu et al., 2015 [9] | 131/141 | 0.002 | |
| Hu et al., 2015 [10] | 152/31 | 0.034 | |
| Csencsits-Smith et al., 2016 [11] | 15/24 | <0.005 | |
| Yang et al., 2018 [12] | 120/100 | <0.05 | |
| Kim et al., 2018 [13] | 58/20 | >0.1 | |
| King et al., 2019 [14] | 156/64 | <0.05 | |
| Alrafiah et al., 2019 [15] | 26/24 | >0.01 | |
| Li et al., 2022 [16] | 138/132 | <0.005 | |
| Correlation of TNF-α with disease severity (H and Y, UPDRSIII) | Dobbs et al., 1999 [17] | 78/140 | 0.015 |
| Williams-Gray et al., 2016 [18] | 230/93 | <0.005 | |
| Kouchaki et al., 2018 [19] | 83/83 | <0.0001 | |
| Rathnayake et al., 2019 [24] | 72/30 | <0.001 | |
| Correlation of TNF-α with cognitive decline | Williams-Gray et al., 2016 [18] | 230/93 | <0.007 |
| Karpenko et al., 2018 [25] | 117/60 | <0.05 | |
| Correlation of TNF-α with depression and anxiety | Lindqvist et al., 2012 [26] | 86/40 | <0.001 |
| Wang et al., 2016 [27] | 62/62 | <0.005 | |
| Higher MCP-1 levels in cases versus control | Usenko et al., 2016 [20] | 47/19 | <0.001 |
| Csencsits et al., 2016 [11] | 25/15 | ≤0.05 | |
| Schröder et al., 2018 [28] | 10/13 | <0.05 | |
| Lower MCP-1 levels in cases versus control | Miluikhina et al., 2020 [29] | 28/28 | ≤0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiromerisiou, G.; Marogianni, C.; Lampropoulos, I.C.; Dardiotis, E.; Speletas, M.; Ntavaroukas, P.; Androutsopoulou, A.; Kalala, F.; Grigoriadis, N.; Papoutsopoulou, S. Peripheral Inflammatory Markers TNF-α and CCL2 Revisited: Association with Parkinson’s Disease Severity. Int. J. Mol. Sci. 2023, 24, 264. https://doi.org/10.3390/ijms24010264
Xiromerisiou G, Marogianni C, Lampropoulos IC, Dardiotis E, Speletas M, Ntavaroukas P, Androutsopoulou A, Kalala F, Grigoriadis N, Papoutsopoulou S. Peripheral Inflammatory Markers TNF-α and CCL2 Revisited: Association with Parkinson’s Disease Severity. International Journal of Molecular Sciences. 2023; 24(1):264. https://doi.org/10.3390/ijms24010264
Chicago/Turabian StyleXiromerisiou, Georgia, Chrysoula Marogianni, Ioannis C. Lampropoulos, Efthimios Dardiotis, Matthaios Speletas, Panagiotis Ntavaroukas, Anastasia Androutsopoulou, Fani Kalala, Nikolaos Grigoriadis, and Stamatia Papoutsopoulou. 2023. "Peripheral Inflammatory Markers TNF-α and CCL2 Revisited: Association with Parkinson’s Disease Severity" International Journal of Molecular Sciences 24, no. 1: 264. https://doi.org/10.3390/ijms24010264