
Investigating Biomarkers for USH2A Retinopathy Using Multimodal Retinal Imaging

 , and
, and 
Abstract
:1. Introduction
2. Results
2.1. Subject Demographics and Genetic Results
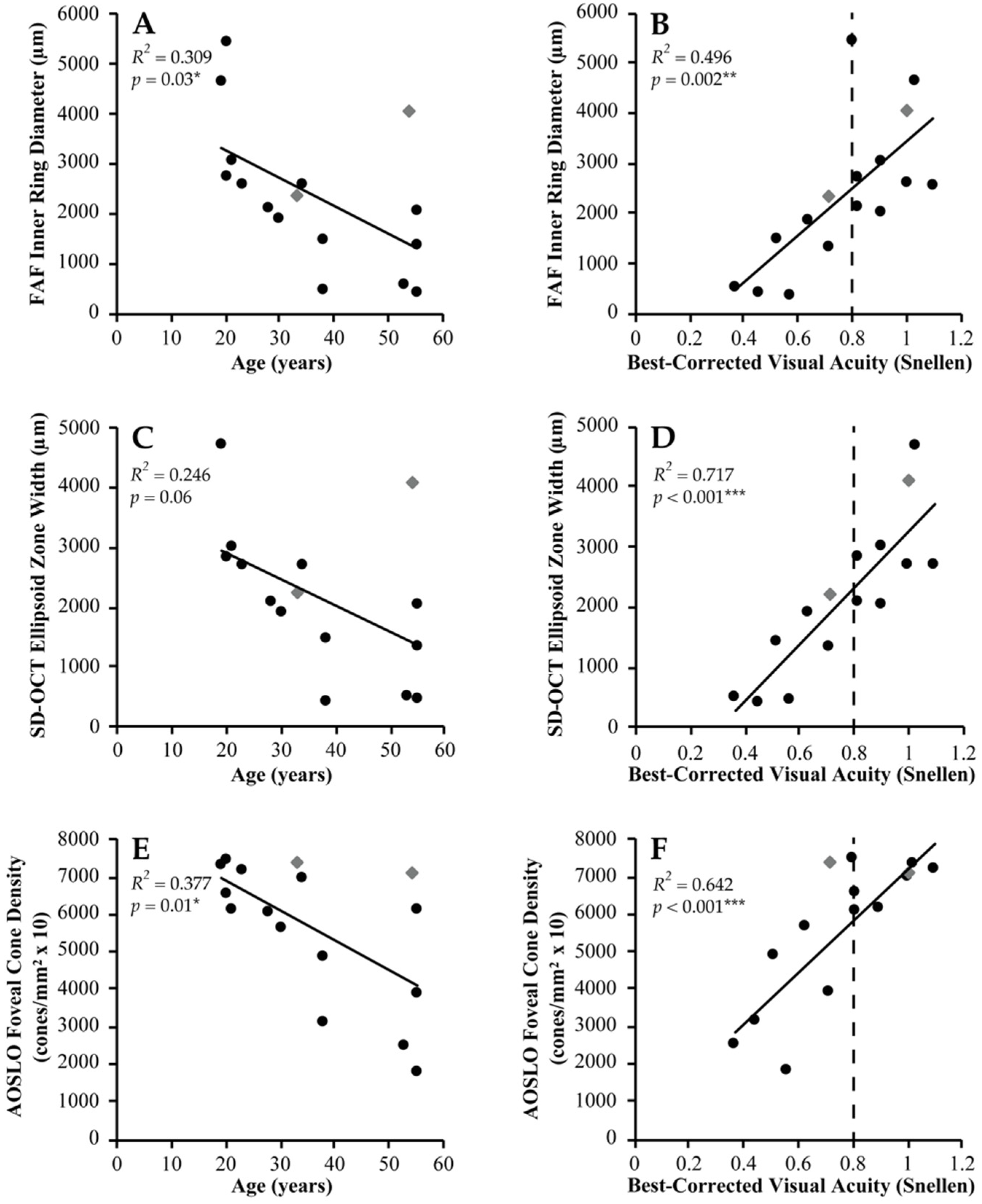
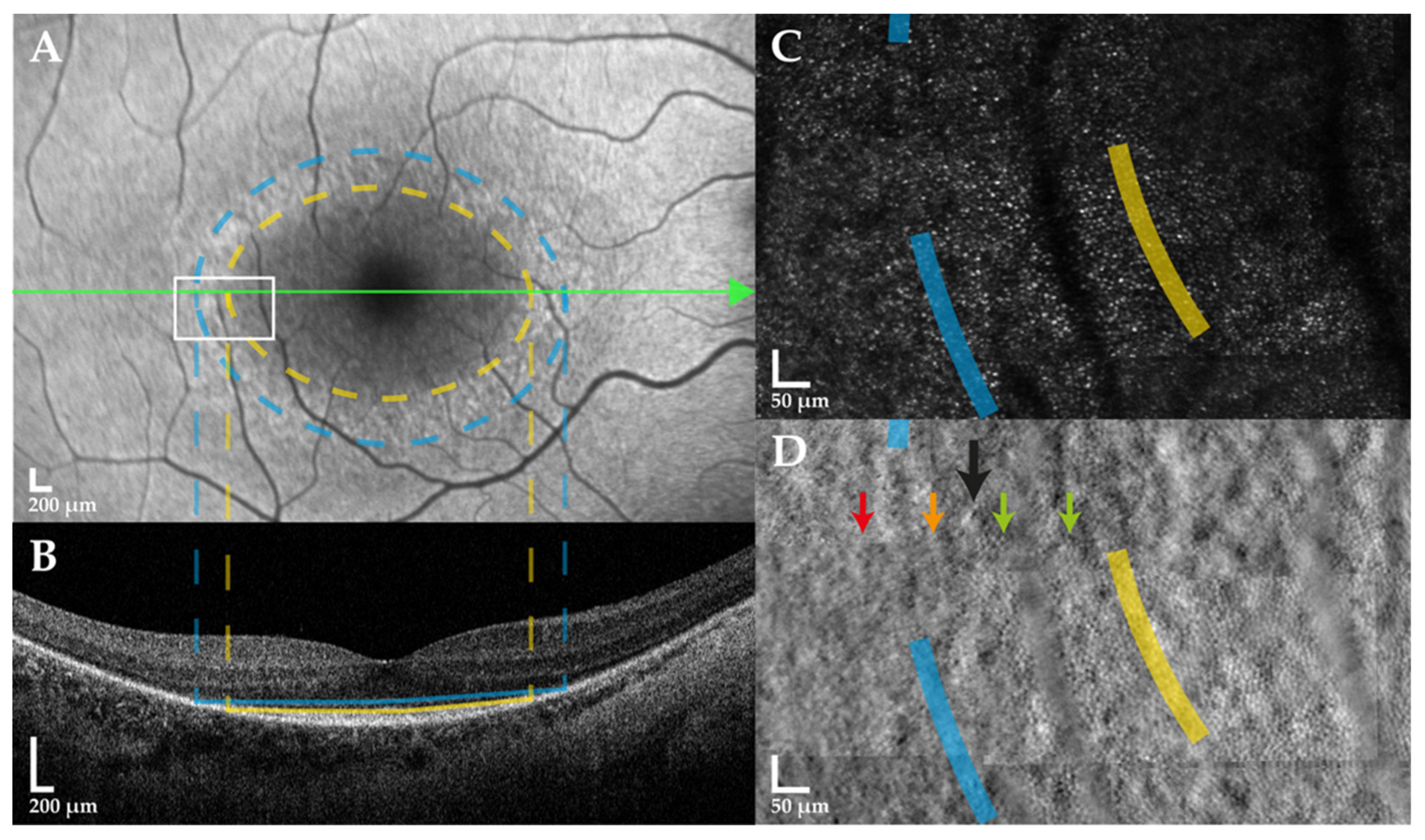
2.2. Clinical Imaging Analysis
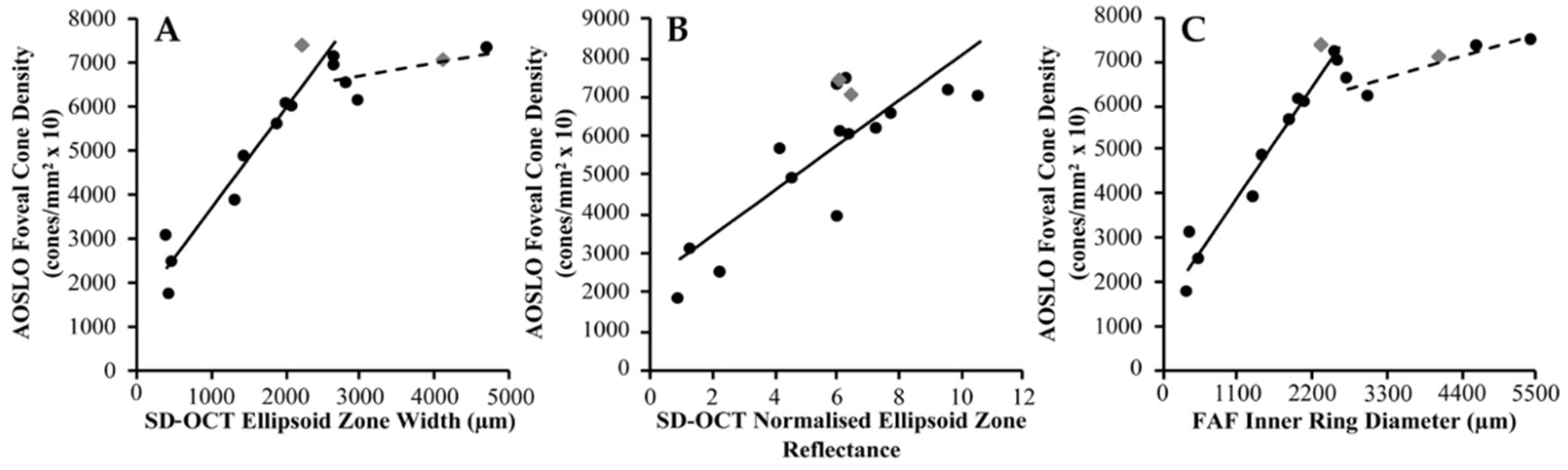
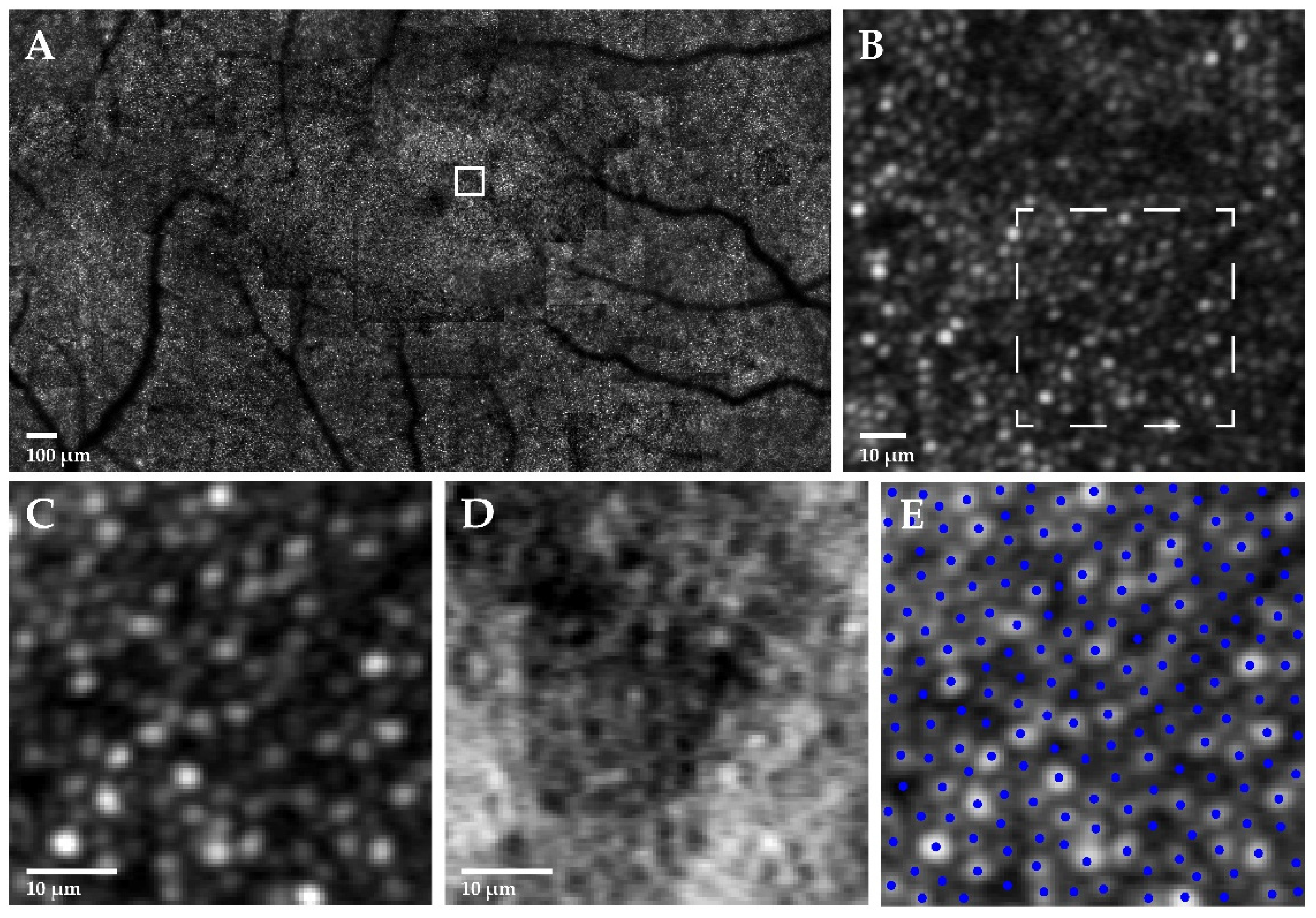
2.3. Photoreceptor Mosaic Analysis
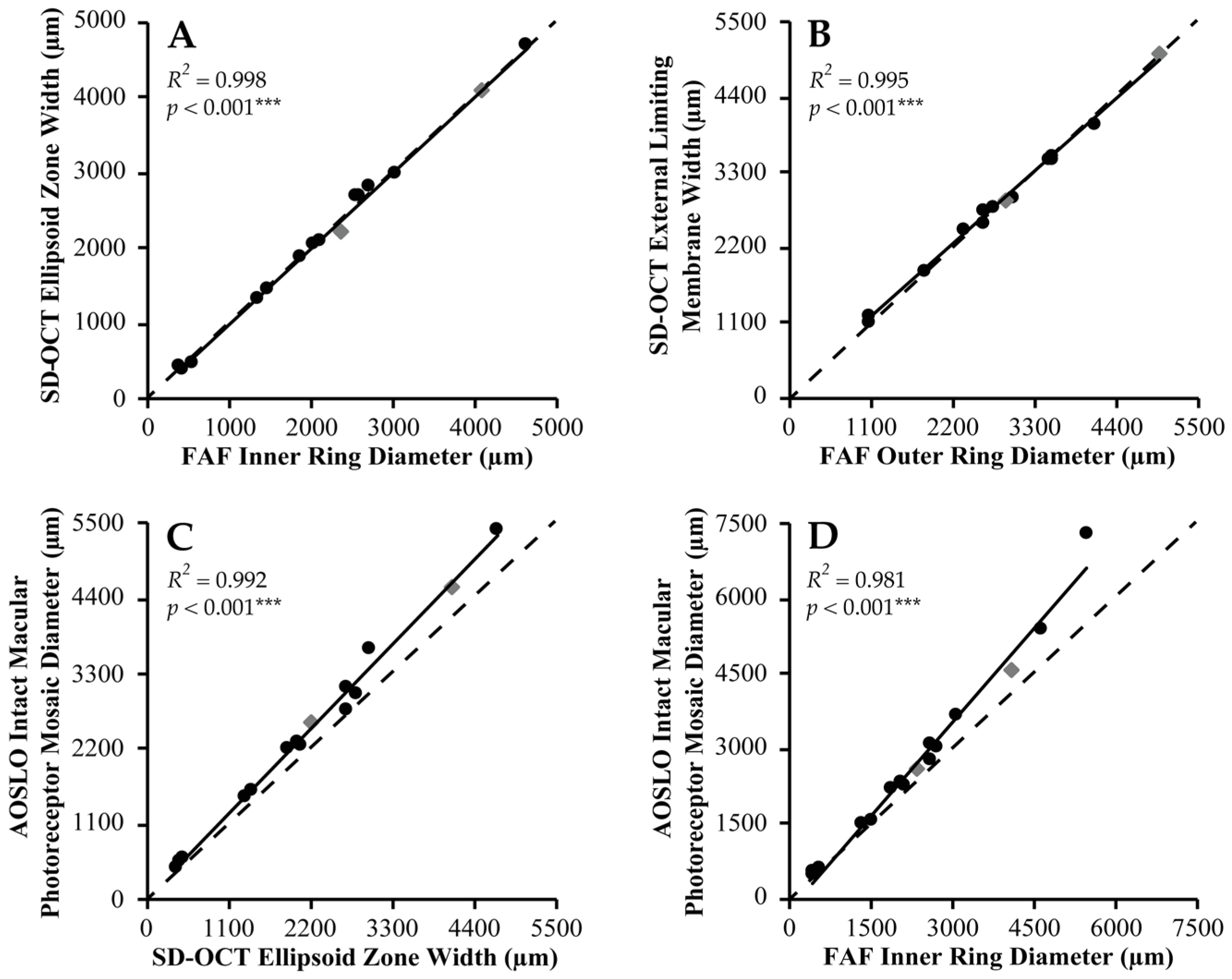
2.4. Multimodal Imaging Correlations
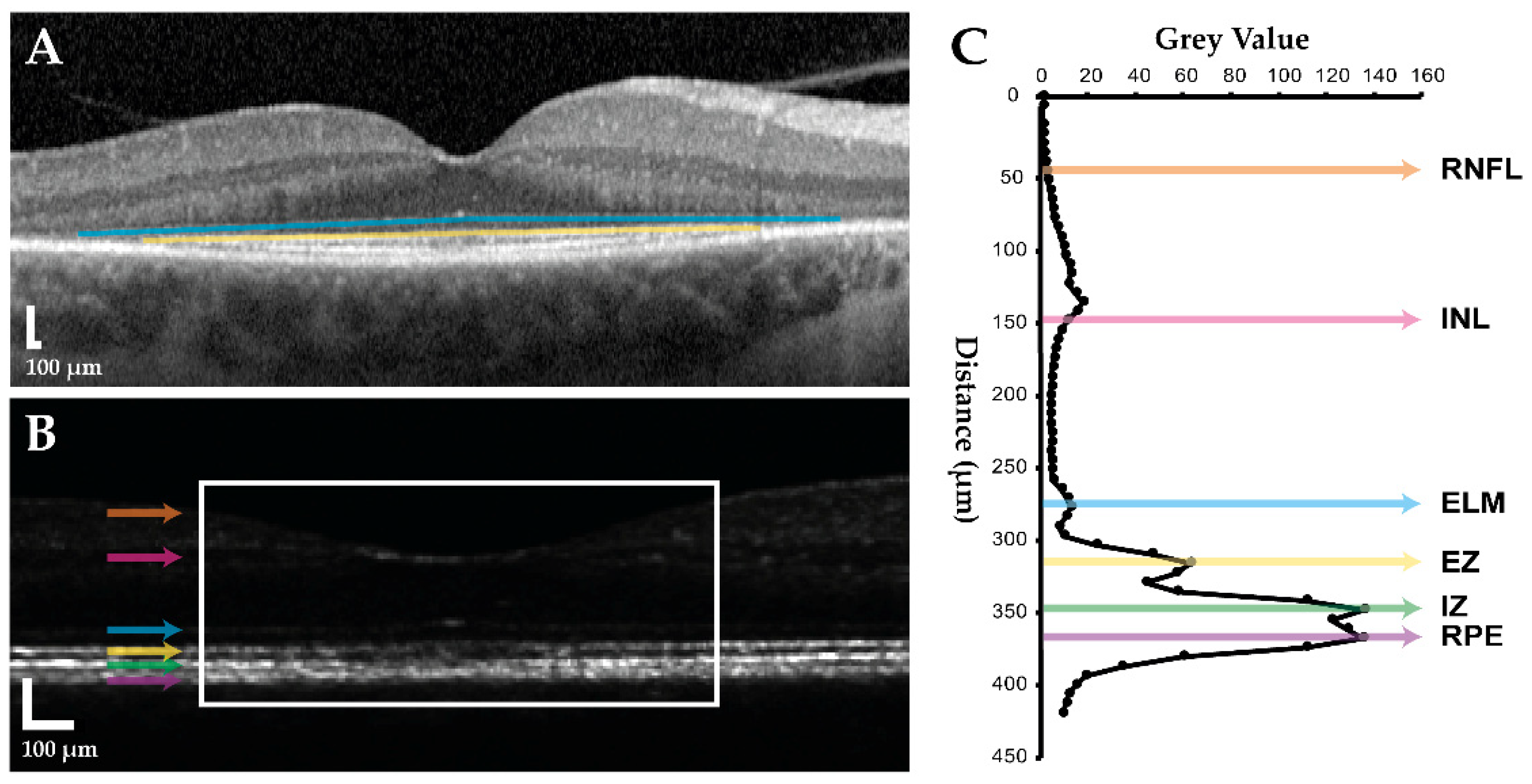
2.4.1. FAF versus SD-OCT
2.4.2. SD-OCT versus AOSLO
2.4.3. FAF versus AOSLO
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Fundus Autofluorescence and Spectral-Domain Optical Coherence Tomography
4.3. Adaptive Optics Scanning Laser Ophthalmoscopy
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hartong, D.T.; Berson, E.L.; Dryja, T.P. Retinitis pigmentosa. Lancet 2006, 368, 1795–1809. [Google Scholar] [CrossRef]
- Boughman, J.A.; Vernon, M.; Shaver, K.A. Usher syndrome: Definition and estimate of prevalence from two high-risk populations. J. Chronic Dis. 1983, 36, 595–603. [Google Scholar] [CrossRef]
- Usher, C. On the inheritance of retinitis pigmentosa, with notes of cases. R. Lond. Ophthalmol. Hosp. Rep. 1914, 19, 130–236. [Google Scholar]
- Vernon, M. Usher’s syndrome—Deafness and progressive blindness. Clinical cases, prevention, theory and literature survey. J. Chronic Dis. 1969, 22, 133–151. [Google Scholar] [CrossRef]
- Kimberling, W.J.; Hildebrand, M.S.; Shearer, A.E.; Jensen, M.L.; Halder, J.A.; Trzupek, K.; Cohn, E.S.; Weleber, R.G.; Stone, E.M.; Smith, R.J. Frequency of Usher syndrome in two pediatric populations: Implications for genetic screening of deaf and hard of hearing children. Genet. Med. 2010, 12, 512–516. [Google Scholar] [CrossRef] [Green Version]
- Toms, M.; Pagarkar, W.; Moosajee, M. Usher syndrome: Clinical features, molecular genetics and advancing therapeutics. Ther. Adv. Ophthalmol. 2020, 12, 1–19. [Google Scholar] [CrossRef]
- RetNet. Available online: https://sph.uth.edu/RetNet/ (accessed on 14 February 2022).
- Jouret, G.; Poirsier, C.; Spodenkiewicz, M.; Jaquin, C.; Gouy, E.; Arndt, C.; Labrousse, M.; Gaillard, D.; Doco-Fenzy, M.; Lebre, A.S. Genetics of Usher syndrome: New insights from a meta-analysis. Otol. Neurotol. 2019, 40, 121–129. [Google Scholar] [CrossRef]
- Gao, F.J.; Wang, D.D.; Chen, F.; Sun, H.X.; Hu, F.Y.; Xu, P.; Li, J.; Liu, W.; Qi, Y.H.; Li, W.; et al. Prevalence and genetic-phenotypic characteristics of patients with USH2A mutations in a large cohort of Chinese patients with inherited retinal disease. Br. J. Ophthalmol. 2021, 105, 87–92. [Google Scholar] [CrossRef]
- Liu, X.; Bulgakov, O.V.; Darrow, K.N.; Pawlyk, B.; Adamian, M.; Liberman, M.C.; Li, T. Usherin is required for maintenance of retinal photoreceptors and normal development of cochlear hair cells. Proc. Natl. Acad. Sci. USA 2007, 104, 4413–4418. [Google Scholar] [CrossRef] [Green Version]
- Schwaller, F.; Begay, V.; Garcia-Garcia, G.; Taberner, F.J.; Moshourab, R.; McDonald, B.; Docter, T.; Kuhnemund, J.; Ojeda-Alonso, J.; Paricio-Montesinos, R.; et al. USH2A is a Meissner’s corpuscle protein necessary for normal vibration sensing in mice and humans. Nat. Neurosci. 2021, 24, 74–81. [Google Scholar] [CrossRef]
- Lenassi, E.; Vincent, A.; Li, Z.; Saihan, Z.; Coffey, A.J.; Steele-Stallard, H.B.; Moore, A.T.; Steel, K.P.; Luxon, L.M.; Heon, E.; et al. A detailed clinical and molecular survey of subjects with nonsyndromic USH2A retinopathy reveals an allelic hierarchy of disease-causing variants. Eur. J. Hum. Genet. 2015, 23, 1318–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, L.; Maltese, P.E.; Romano, D.; Fogagnolo, P.; Castori, M.; Marceddu, G.; Cristofoli, F.; Percio, M.; Pitekova, B.; Modarelli, A.M.; et al. SD-OCT analysis in syndromic and non-syndromic forms of retinitis pigmentosa due to USH2A gene mutations. Ophthalmic Res. 2021; published online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Liu, X.; Li, Y.; Guo, T.; Yang, L. Correlation between genotype and phenotype in 69 Chinese patients with USH2A mutations: A comparative study of the patients with Usher syndrome and nonsyndromic retinitis pigmentosa. Acta Ophthalmol. 2021, 99, e447–e460. [Google Scholar] [CrossRef] [PubMed]
- Pierrache, L.H.; Hartel, B.P.; van Wijk, E.; Meester-Smoor, M.A.; Cremers, F.P.; de Baere, E.; de Zaeytijd, J.; van Schooneveld, M.J.; Cremers, C.W.; Dagnelie, G.; et al. Visual prognosis in USH2A-associated retinitis pigmentosa is worse for patients with Usher syndrome type IIa than for those with nonsyndromic retinitis pigmentosa. Ophthalmology 2016, 123, 1151–1160. [Google Scholar] [CrossRef]
- Birch, D.G.; Cheng, P.; Duncan, J.L.; Ayala, A.R.; Maguire, M.G.; Audo, I.; Cheetham, J.K.; Durham, T.A.; Fahim, A.T.; Ferris, F.L., 3rd; et al. The RUSH2A study: Best-corrected visual acuity, full-field electroretinography amplitudes, and full-field stimulus thresholds at baseline. Transl. Vis. Sci. Technol. 2020, 9, 9. [Google Scholar] [CrossRef]
- Duncan, J.L.; Liang, W.; Maguire, M.G.; Audo, I.; Ayala, A.R.; Birch, D.G.; Carroll, J.; Cheetham, J.K.; Esposti, S.D.; Durham, T.A.; et al. Baseline visual field findings in the RUSH2A study: Associated factors and correlation with other measures of disease severity. Am. J. Ophthalmol. 2020, 219, 87–100. [Google Scholar] [CrossRef]
- Inaba, A.; Maeda, A.; Yoshida, A.; Kawai, K.; Hirami, Y.; Kurimoto, Y.; Kosugi, S.; Takahashi, M. Truncating variants contribute to hearing loss and severe retinopathy in USH2A-associated retinitis pigmentosa in Japanese patients. Int. J. Mol. Sci. 2020, 21, 7817. [Google Scholar]
- Zhu, T.; Chen, D.F.; Wang, L.; Wu, S.; Wei, X.; Li, H.; Jin, Z.B.; Sui, R. USH2A variants in Chinese patients with Usher syndrome type II and non-syndromic retinitis pigmentosa. Br. J. Ophthalmol. 2021, 105, 694–703. [Google Scholar] [CrossRef]
- Fakin, A.; Jarc-Vidmar, M.; Glavac, D.; Bonnet, C.; Petit, C.; Hawlina, M. Fundus autofluorescence and optical coherence tomography in relation to visual function in Usher syndrome type 1 and 2. Vision Res. 2012, 75, 60–70. [Google Scholar] [CrossRef] [Green Version]
- Robson, A.G.; Saihan, Z.; Jenkins, S.A.; Fitzke, F.W.; Bird, A.C.; Webster, A.R.; Holder, G.E. Functional characterisation and serial imaging of abnormal fundus autofluorescence in patients with retinitis pigmentosa and normal visual acuity. Br. J. Ophthalmol. 2006, 90, 472–479. [Google Scholar] [CrossRef] [Green Version]
- Wakabayashi, T.; Sawa, M.; Gomi, F.; Tsujikawa, M. Correlation of fundus autofluorescence with photoreceptor morphology and functional changes in eyes with retinitis pigmentosa. Acta Ophthalmol. 2010, 88, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Robson, A.G.; Tufail, A.; Fitzke, F.; Bird, A.C.; Moore, A.T.; Holder, G.E.; Webster, A.R. Serial imaging and structure-function correlates of high-density rings of fundus autofluorescence in retinitis pigmentosa. Retina 2011, 31, 1670–1679. [Google Scholar] [CrossRef] [PubMed]
- Lima, L.H.; Burke, T.; Greenstein, V.C.; Chou, C.L.; Cella, W.; Yannuzzi, L.A.; Tsang, S.H. Progressive constriction of the hyperautofluorescent ring in retinitis pigmentosa. Am. J. Ophthalmol. 2012, 153, 718–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toms, M.; Dubis, A.M.; de Vrieze, E.; Tracey-White, D.; Mitsios, A.; Hayes, M.; Broekman, S.; Baxendale, S.; Utoomprurkporn, N.; Bamiou, D.; et al. Clinical and preclinical therapeutic outcome metrics for USH2A-related disease. Hum. Mol. Genet. 2020, 29, 1882–1899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aizawa, S.; Mitamura, Y.; Hagiwara, A.; Sugawara, T.; Yamamoto, S. Changes of fundus autofluorescence, photoreceptor inner and outer segment junction line, and visual function in patients with retinitis pigmentosa. Clin. Exp. Ophthalmol. 2010, 38, 597–604. [Google Scholar] [CrossRef]
- Sujirakul, T.; Lin, M.K.; Duong, J.; Wei, Y.; Lopez-Pintado, S.; Tsang, S.H. Multimodal imaging of central retinal disease progression in a 2-year mean follow-up of retinitis pigmentosa. Am. J. Ophthalmol. 2015, 160, 786–798. [Google Scholar] [CrossRef] [Green Version]
- Cabral, T.; Lima de Carvalho, J.R., Jr.; Kim, J.; Oh, J.K.; Levi, S.R.; Park, K.S.; Duong, J.K.; Park, J.; Boudreault, K.; Belfort, R., Jr.; et al. Comparative analysis of functional and structural decline in retinitis pigmentosas. Int. J. Mol. Sci. 2020, 21, 2730. [Google Scholar] [CrossRef] [Green Version]
- Cuenca, N.; Ortuno-Lizaran, I.; Sanchez-Saez, X.; Kutsyr, O.; Albertos-Arranz, H.; Fernandez-Sanchez, L.; Martinez-Gil, N.; Noailles, A.; Lopez-Garrido, J.A.; Lopez-Galvez, M.; et al. Interpretation of OCT and OCTA images from a histological approach: Clinical and experimental implications. Prog. Retin. Eye Res. 2020, 77, 100828. [Google Scholar] [CrossRef] [PubMed]
- Milam, A.H.; Li, Z.Y.; Fariss, R.N. Histopathology of the human retina in retinitis pigmentosa. Prog. Retin. Eye Res. 1998, 17, 175–205. [Google Scholar] [PubMed]
- Liang, J.; Williams, D.R.; Miller, D.T. Supernormal vision and high-resolution retinal imaging through adaptive optics. J. Opt. Soc. Am. A 1997, 14, 2884–2892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, J.L.; Zhang, Y.; Gandhi, J.; Nakanishi, C.; Othman, M.; Branham, K.E.; Swaroop, A.; Roorda, A. High-resolution imaging with adaptive optics in patients with inherited retinal degeneration. Investig. Ophthalmol. Vis. Sci. 2007, 48, 3283–3291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talcott, K.E.; Ratnam, K.; Sundquist, S.M.; Lucero, A.S.; Lujan, B.J.; Tao, W.; Porco, T.C.; Roorda, A.; Duncan, J.L. Longitudinal study of cone photoreceptors during retinal degeneration and in response to ciliary neurotrophic factor treatment. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2219–2226. [Google Scholar] [CrossRef] [PubMed]
- Ratnam, K.; Vastinsalo, H.; Roorda, A.; Sankila, E.M.; Duncan, J.L. Cone structure in patients with usher syndrome type III and mutations in the Clarin 1 gene. JAMA Ophthalmol. 2013, 131, 67–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, L.W.; Johnson, R.D.; Langlo, C.S.; Cooper, R.F.; Razeen, M.M.; Russillo, M.C.; Dubra, A.; Connor, T.B., Jr.; Han, D.P.; Pennesi, M.E.; et al. Assessing photoreceptor structure in retinitis pigmentosa and Usher syndrome. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2428–2442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roorda, A.; Romero-Borja, F.; Donnelly Iii, W.; Queener, H.; Hebert, T.; Campbell, M. Adaptive optics scanning laser ophthalmoscopy. Opt. Express 2002, 10, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Scoles, D.; Sulai, Y.N.; Dubra, A. In vivo dark-field imaging of the retinal pigment epithelium cell mosaic. Biomed. Opt. Express 2013, 4, 1710–1723. [Google Scholar] [CrossRef] [Green Version]
- Scoles, D.; Sulai, Y.N.; Langlo, C.S.; Fishman, G.A.; Curcio, C.A.; Carroll, J.; Dubra, A. In vivo imaging of human cone photoreceptor inner segments. Investig. Ophthalmol. Vis. Sci. 2014, 55, 4244–4251. [Google Scholar] [CrossRef]
- Ratnam, K.; Carroll, J.; Porco, T.C.; Duncan, J.L.; Roorda, A. Relationship between foveal cone structure and clinical measures of visual function in patients with inherited retinal degenerations. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5836–5847. [Google Scholar] [CrossRef]
- Tojo, N.; Nakamura, T.; Fuchizawa, C.; Oiwake, T.; Hayashi, A. Adaptive optics fundus images of cone photoreceptors in the macula of patients with retinitis pigmentosa. Clin. Ophthalmol. 2013, 7, 203–210. [Google Scholar]
- Nakatake, S.; Murakami, Y.; Funatsu, J.; Koyanagi, Y.; Akiyama, M.; Momozawa, Y.; Ishibashi, T.; Sonoda, K.H.; Ikeda, Y. Early detection of cone photoreceptor cell loss in retinitis pigmentosa using adaptive optics scanning laser ophthalmoscopy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 1169–1181. [Google Scholar] [CrossRef]
- Makiyama, Y.; Ooto, S.; Hangai, M.; Takayama, K.; Uji, A.; Oishi, A.; Ogino, K.; Nakagawa, S.; Yoshimura, N. Macular cone abnormalities in retinitis pigmentosa with preserved central vision using adaptive optics scanning laser ophthalmoscopy. PLoS ONE 2013, 8, e79447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gale, M.J.; Feng, S.; Titus, H.E.; Smith, T.B.; Pennesi, M.E. Interpretation of flood-illuminated adaptive optics images in subjects with retinitis pigmentosa. Adv. Exp. Med. Biol. 2016, 854, 291–297. [Google Scholar] [PubMed]
- Ueno, S.; Koyanagi, Y.; Kominami, T.; Ito, Y.; Kawano, K.; Nishiguchi, K.M.; Rivolta, C.; Nakazawa, T.; Sonoda, K.H.; Terasaki, H. Clinical characteristics and high resolution retinal imaging of retinitis pigmentosa caused by RP1 gene variants. Jpn. J. Ophthalmol. 2020, 64, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Menghini, M.; Lujan, B.J.; Zayit-Soudry, S.; Syed, R.; Porco, T.C.; Bayabo, K.; Carroll, J.; Roorda, A.; Duncan, J.L. Correlation of outer nuclear layer thickness with cone density values in patients with retinitis pigmentosa and healthy subjects. Investig. Ophthalmol. Vis. Sci. 2014, 56, 372–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toualbi, L.; Toms, M.; Moosajee, M. USH2A-retinopathy: From genetics to therapeutics. Exp. Eye Res. 2020, 201, 108330. [Google Scholar] [CrossRef]
- Murakami, T.; Akimoto, M.; Ooto, S.; Suzuki, T.; Ikeda, H.; Kawagoe, N.; Takahashi, M.; Yoshimura, N. Association between abnormal autofluorescence and photoreceptor disorganization in retinitis pigmentosa. Am. J. Ophthalmol. 2008, 145, 687–694. [Google Scholar] [CrossRef]
- Robson, A.G.; Egan, C.A.; Luong, V.A.; Bird, A.C.; Holder, G.E.; Fitzke, F.W. Comparison of fundus autofluorescence with photopic and scotopic fine-matrix mapping in patients with retinitis pigmentosa and normal visual acuity. Investig. Ophthalmol. Vis. Sci. 2004, 45, 4119–4125. [Google Scholar] [CrossRef] [Green Version]
- Gill, J.S.; Moosajee, M.; Dubis, A.M. Cellular imaging of inherited retinal diseases using adaptive optics. Eye Lond. 2019, 33, 1683–1698. [Google Scholar] [CrossRef]
- Gale, M.J.; Harman, G.A.; Chen, J.; Pennesi, M.E. Repeatability of adaptive optics automated cone measurements in subjects with retinitis pigmentosa and novel metrics for assessment of image quality. Transl. Vis. Sci. Technol. 2019, 8, 17. [Google Scholar] [CrossRef]
- Litts, K.M.; Cooper, R.F.; Duncan, J.L.; Carroll, J. Photoreceptor-based biomarkers in AOSLO retinal imaging. Investig. Ophthalmol. Vis. Sci. 2017, 58, BIO255–BIO267. [Google Scholar] [CrossRef] [Green Version]
- Curcio Christine, A.; Sloan Kenneth, R.; Kalina Robert, E.; Hendrickson Anita, E. Human photoreceptor topography. J. Comp. Neurol. 1990, 292, 497–523. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Godara, P.; Blanco, E.R.; Griffin, R.L.; Wang, X.; Curcio, C.A.; Zhang, Y. Variability in human cone topography assessed by adaptive optics scanning laser ophthalmoscopy. Am. J. Ophthalmol. 2015, 160, 290–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, K.S.; Harmening, W.M.; Langston, B.R.; Tuten, W.S.; Roorda, A.; Sincich, L.C. Normal perceptual sensitivity arising from weakly reflective cone photoreceptors. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4431–4438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, H.; Chui, T.Y.; Zhong, Z.; Elsner, A.E.; Burns, S.A. Variation of cone photoreceptor packing density with retinal eccentricity and age. Investig. Ophthalmol. Vis. Sci. 2011, 52, 7376–7384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, B.; Xiao, J.; Wang, K.; So, K.F.; Tipoe, G.L.; Lin, B. Suppression of microglial activation is neuroprotective in a mouse model of human retinitis pigmentosa. J. Neurosci. 2014, 34, 8139–8150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leveillard, T.; Mohand-Said, S.; Lorentz, O.; Hicks, D.; Fintz, A.C.; Clerin, E.; Simonutti, M.; Forster, V.; Cavusoglu, N.; Chalmel, F.; et al. Identification and characterization of rod-derived cone viability factor. Nat. Genet. 2004, 36, 755–759. [Google Scholar] [CrossRef] [PubMed]
- Flores, M.; Debellemaniere, G.; Bully, A.; Meillat, M.; Tumahai, P.; Delbosc, B.; Saleh, M. Reflectivity of the outer retina on spectral-domain optical coherence tomography as a predictor of photoreceptor cone density. Am. J. Ophthalmol. 2015, 160, 588–595. [Google Scholar] [CrossRef]
- Saleh, M.; Flores, M.; Gauthier, A.S.; Elphege, E.; Delbosc, B. Quantitative analysis of photoreceptor layer reflectivity on en-face optical coherence tomography as an estimator of cone density. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 2119–2126. [Google Scholar] [CrossRef]
- Csaky, K.; Ferris, F., 3rd; Chew, E.Y.; Nair, P.; Cheetham, J.K.; Duncan, J.L. Report from the NEI/FDA endpoints workshop on age-related macular degeneration and inherited retinal diseases. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3456–3463. [Google Scholar] [CrossRef]
- Grover, S.; Fishman, G.A.; Anderson, R.J.; Alexander, K.R.; Derlacki, D.J. Rate of visual field loss in retinitis pigmentosa. Ophthalmology 1997, 104, 460–465. [Google Scholar] [CrossRef]
- Calzetti, G.; Levy, R.A.; Cideciyan, A.V.; Garafalo, A.V.; Roman, A.J.; Sumaroka, A.; Charng, J.; Heon, E.; Jacobson, S.G. Efficacy outcome measures for clinical trials of USH2A caused by the common c.2299delG mutation. Am. J. Ophthalmol. 2018, 193, 114–129. [Google Scholar] [CrossRef] [PubMed]
- Wynne, N.; Carroll, J.; Duncan, J.L. Promises and pitfalls of evaluating photoreceptor-based retinal disease with adaptive optics scanning light ophthalmoscopy (AOSLO). Prog. Retin. Eye Res. 2021, 83, 100920. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.B.; Parker, M.; Steinkamp, P.N.; Weleber, R.G.; Smith, N.; Wilson, D.J.; VPA Clinical Trial Study Group; EZ Working Group. Structure-function modeling of optical coherence tomography and standard automated perimetry in the retina of patients with autosomal dominant retinitis pigmentosa. PLoS ONE 2016, 11, e0148022. [Google Scholar] [CrossRef] [PubMed]
- Strampe, M.R.; Huckenpahler, A.L.; Higgins, B.P.; Tarima, S.; Visotcky, A.; Stepien, K.E.; Kay, C.N.; Carroll, J. Intraobserver repeatability and interobserver reproducibility of ellipsoid zone measurements in retinitis pigmentosa. Transl. Vis. Sci. Technol. 2018, 7, 13. [Google Scholar] [CrossRef]
- Zada, M.; Cornish, E.E.; Fraser, C.L.; Jamieson, R.V.; Grigg, J.R. Natural history and clinical biomarkers of progression in X-linked retinitis pigmentosa: A systematic review. Acta Ophthalmol. 2021, 99, 499–510. [Google Scholar] [CrossRef]
- Lombardo, M.; Serrao, S.; Lombardo, G. Technical factors influencing cone packing density estimates in adaptive optics flood illuminated retinal images. PLoS ONE 2014, 9, e107402. [Google Scholar] [CrossRef]
- Huang, Y.; Cideciyan, A.V.; Papastergiou, G.I.; Banin, E.; Semple-Rowland, S.L.; Milam, A.H.; Jacobson, S.G. Relation of optical coherence tomography to microanatomy in normal and rd chickens. Investig. Ophthalmol. Vis. Sci. 1998, 39, 2405–2416. [Google Scholar]
- Dubis, A.M.; Cooper, R.F.; Aboshiha, J.; Langlo, C.S.; Sundaram, V.; Liu, B.; Collison, F.; Fishman, G.A.; Moore, A.T.; Webster, A.R.; et al. Genotype-dependent variability in residual cone structure in achromatopsia: Toward developing metrics for assessing cone health. Investig. Ophthalmol. Vis. Sci. 2014, 55, 7303–7311. [Google Scholar] [CrossRef]
- Dubra, A.; Sulai, Y. Reflective afocal broadband adaptive optics scanning ophthalmoscope. Biomed. Opt. Express 2011, 2, 1757–1768. [Google Scholar] [CrossRef] [Green Version]
- Dubra, A.; Harvey, Z. Registration of 2D images from fast scanning ophthalmic instruments. In Proceedings of the 4th International Workshop on Biomedical Image Registration, Lübeck, Germany, 11–13 July 2010. [Google Scholar]
- Chen, M.; Cooper, R.F.; Han, G.K.; Gee, J.; Brainard, D.H.; Morgan, J.I.W. Multi-modal automatic montaging of adaptive optics retinal images. Biomed. Opt. Express 2016, 7, 4899–4918. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Gender | Age | Phenotype | Variant 1 cDNA | Variant 2 cDNA | Axial Length | BCVA | ||
|---|---|---|---|---|---|---|---|---|---|
| Variant 1 Protein | Variant 2 Protein | OD | OS | OD | OS | ||||
| S19 | F | 33 | NSRP | c.11864G>A | c.13335_13347delinsCTTG | 23.88 | 23.84 | 0.80 | 0.63 |
| p.Trp3955* | p.Glu4445_Ser4449delinsAspLeu | ||||||||
| S21 | M | 55 | USH2 | c.100C>T | c.926C>T | 24.07 | 23.84 | 0.50 | 0.63 |
| p.Arg34* | p.Pro309Leu | ||||||||
| S23 | M | 55 | USH2 | c.8834G>A | c.2299delG | 24.24 | 24.25 | 0.80 | 0.63 |
| p.Trp2945* | p.Glu767Serfs21* | ||||||||
| S24 | F | 55 | USH2 | c.4821G>A | c.1859G>T | 22.27 | 22.16 | 0.80 | 1.00 |
| p.Trp1607* | p.Cys620Phe | ||||||||
| S31 | M | 53 | USH2 | c.4474G>T | c.11047+1G>A | 23.32 | 23.26 | 0.33 | 0.40 |
| p.Glu1492* | Deep intronic variant | ||||||||
| S33 | F | 38 | USH2 | c.6862G>T | c.7595–2144A>G | 25.36 | 24.98 | 0.40 | 0.63 |
| p.Glu2288* | Deep intronic variant | ||||||||
| S39 | M | 30 | USH2 | c.187C>T | c.4645C>T | 22.12 | 22.20 | 0.63 | 0.63 |
| p.Arg63* | p.Arg1549* | ||||||||
| S40 | F | 54 | NSRP | c.8981G>A | c.13274C>T | 23.37 | 23.21 | 1.00 | 1.00 |
| p.Trp2994* | p.Thr4425Met | ||||||||
| S43 | M | 38 | USH2 | c.1876C>T | c.2299delG | 23.04 | 22.97 | 0.40 | 0.50 |
| p.Arg626* | p.Glu767Serfs21* | ||||||||
| S47 a | M | 19 | USH2 | c.163C>T | c.2299delG | 26.10 | 25.44 | 1.25 | 0.80 |
| p.Gln55* | p.Glu767Serfs21* | ||||||||
| S48 | F | 20 | USH2 | c.3518C>A | c.920_923dupGCCA | 22.12 | 22.10 | 0.80 | 0.80 |
| p.Ser1173* | p.His308Glnfs16* | ||||||||
| S49 a | M | 21 | USH2 | c.163C>T | c.2299delG | 27.09 | 26.77 | 0.80 | 1.00 |
| p.Gln55* | p.Glu767Serfs21* | ||||||||
| S50 b | M | 28 | USH2 | c.12954C>A | c.10488_10490del | 22.35 | 22.04 | 1.00 | 0.63 |
| p.Tyr4318* | p.Glu3496del | ||||||||
| S51 b | F | 34 | USH2 | c.12954C>A | c.10488_10490del | 24.47 | 24.76 | 1.20 | 0.80 |
| p.Tyr4318* | p.Glu3496del | ||||||||
| S52 | M | 23 | USH2 | c.11065C>T | c.7645_7661del | 23.62 | 23.55 | 1.20 | 1.00 |
| p.Arg3689* | p.Met2549Alafs3* | ||||||||
| S55 | F | 20 | USH2 | c.7814C>G | c.2299delG | 23.72 | 23.80 | 0.63 | 1.00 |
| p.Ser2605* | p.Glu767Serfs21* | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gill, J.S.; Theofylaktopoulos, V.; Mitsios, A.; Houston, S.; Hagag, A.M.; Dubis, A.M.; Moosajee, M. Investigating Biomarkers for USH2A Retinopathy Using Multimodal Retinal Imaging. Int. J. Mol. Sci. 2022, 23, 4198. https://doi.org/10.3390/ijms23084198
Gill JS, Theofylaktopoulos V, Mitsios A, Houston S, Hagag AM, Dubis AM, Moosajee M. Investigating Biomarkers for USH2A Retinopathy Using Multimodal Retinal Imaging. International Journal of Molecular Sciences. 2022; 23(8):4198. https://doi.org/10.3390/ijms23084198
Chicago/Turabian StyleGill, Jasdeep S., Vasileios Theofylaktopoulos, Andreas Mitsios, Sarah Houston, Ahmed M. Hagag, Adam M. Dubis, and Mariya Moosajee. 2022. "Investigating Biomarkers for USH2A Retinopathy Using Multimodal Retinal Imaging" International Journal of Molecular Sciences 23, no. 8: 4198. https://doi.org/10.3390/ijms23084198