
Psycho-Neuro-Endocrine-Immunological Basis of the Placebo Effect: Potential Applications beyond Pain Therapy

 , , , , ,
, , , , ,
Abstract
:1. Introduction
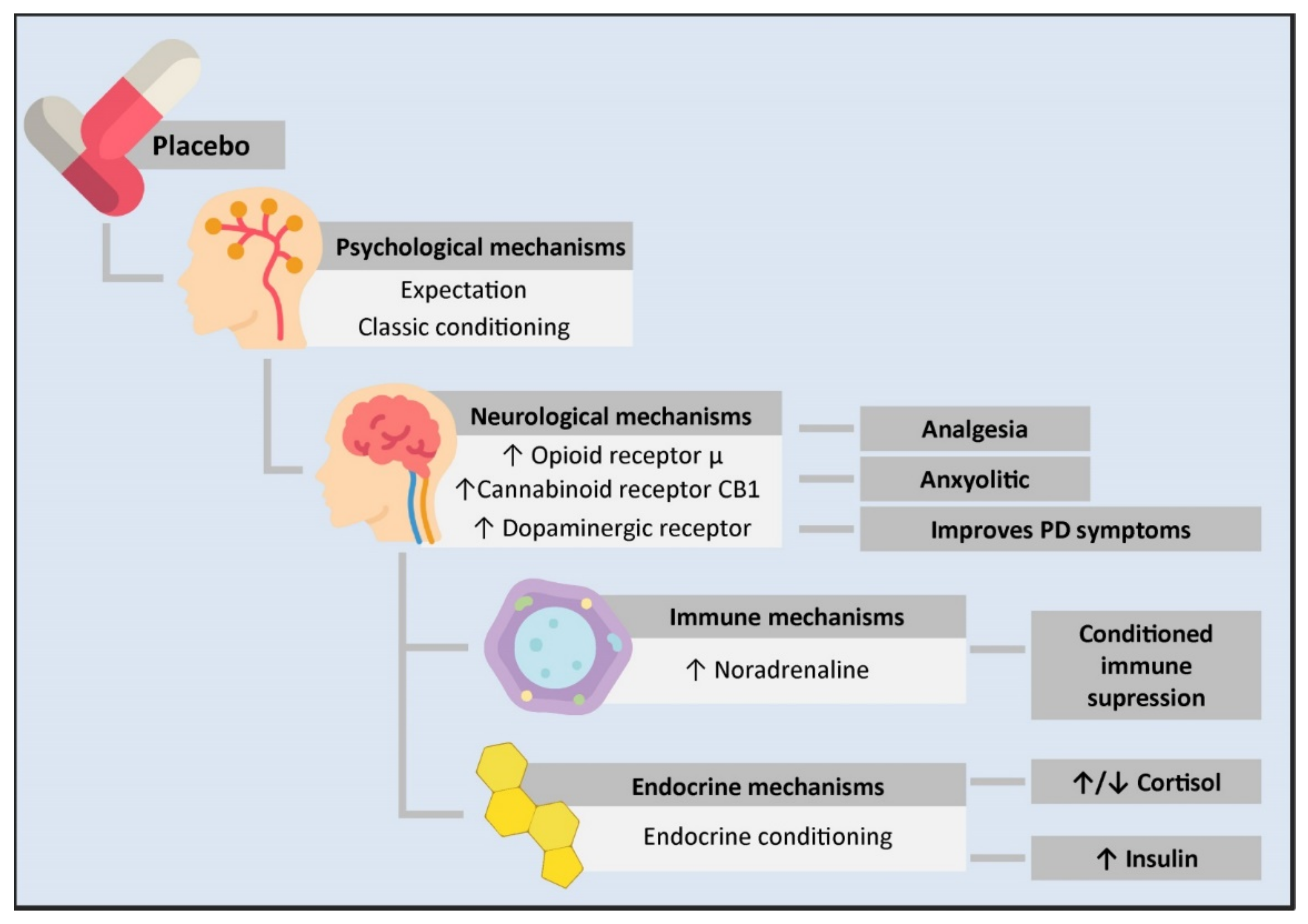
2. Psycho-Neuro-Endocrine-Immune Basis of the Placebo Effect
2.1. Psychological Mechanisms: The Power of the Mind
2.2. Neurobiological Mechanisms Underlying Placebo Effects
2.2.1. Role of Opioids
2.2.2. Endocannabinoid System
2.2.3. Dopaminergic System
2.2.4. Other Neurotransmitters
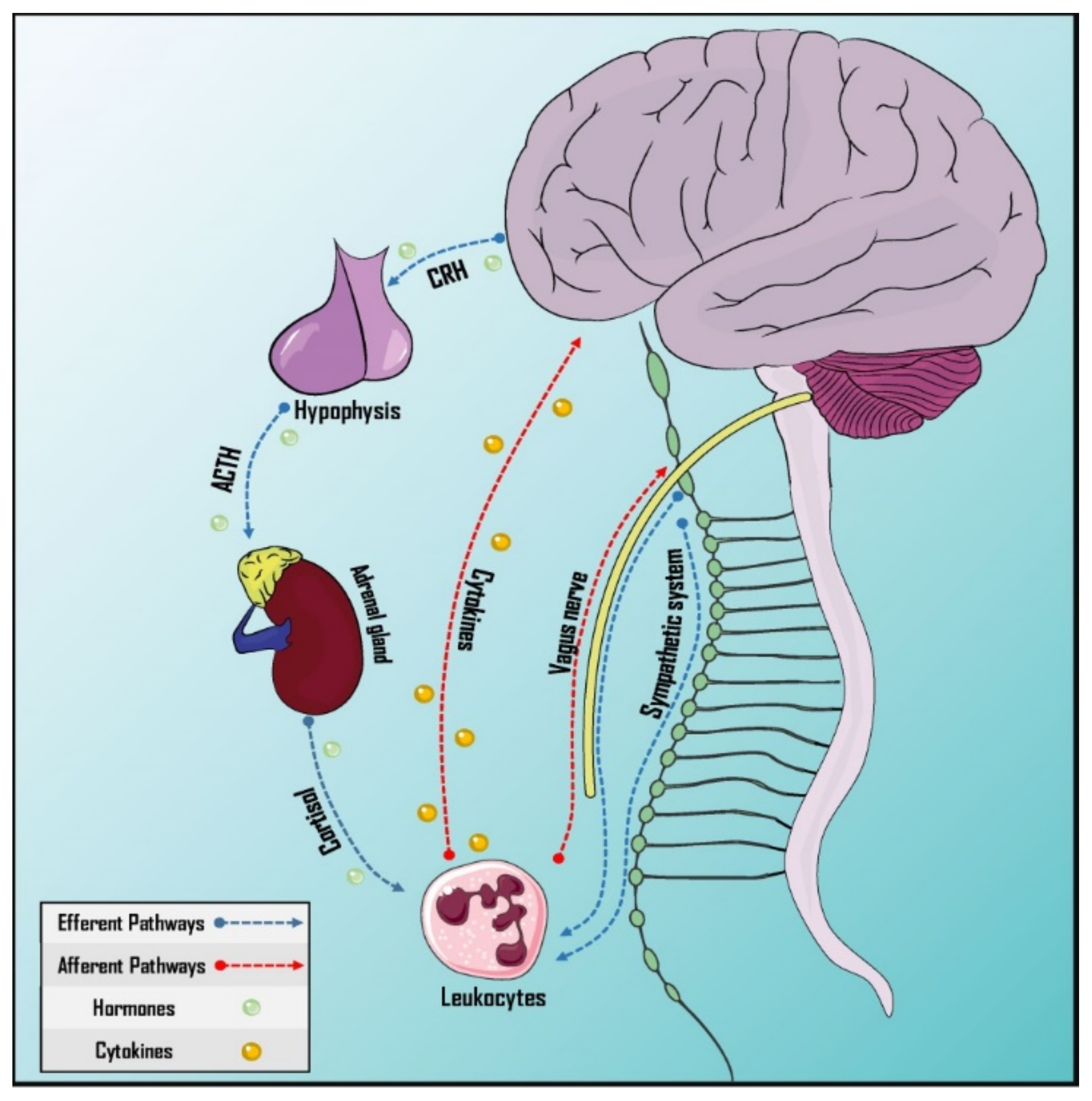
2.3. Immunological Mechanisms
2.4. Endocrine Mechanisms: Placebo Effect on Hormone Secretion
3. Preclinical and Clinical Implications of the Placebo Effect
3.1. Neurological Disorders
3.2. Psychiatric Disorders
3.3. Immunological Disorders
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jütte, R. The Early History of the Placebo. Complement. Ther. Med. 2013, 21, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Kerr, C.E.; Milne, I.; Kaptchuk, T.J. William Cullen and a Missing Mind-Body Link in the Early History of Placebos. J. R. Soc. Med. 2008, 101, 89–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavel, M.E. The Placebo Effect: The Good, the Bad, and the Ugly. Am. J. Med. 2014, 127, 484–488. [Google Scholar] [CrossRef] [PubMed]
- Colagiuri, B.; Schenk, L.A.; Kessler, M.D.; Dorsey, S.G.; Colloca, L. The Placebo Effect: From Concepts to Genes. Neuroscience 2015, 307, 171–190. [Google Scholar] [CrossRef] [Green Version]
- Wager, T.D.; Atlas, L.Y. The Neuroscience of Placebo Effects: Connecting Context, Learning and Health. Nat. Rev. Neurosci. 2015, 16, 403–418. [Google Scholar] [CrossRef]
- Klinger, R.; Colloca, L.; Bingel, U.; Flor, H. Placebo Analgesia: Clinical Applications. Pain 2014, 155, 1055–1058. [Google Scholar] [CrossRef]
- Meyer, B.; Yuen, K.S.L.; Ertl, M.; Polomac, N.; Mulert, C.; Büchel, C.; Kalisch, R. Neural Mechanisms of Placebo Anxiolysis. J. Neurosci. 2015, 35, 7365–7373. [Google Scholar] [CrossRef] [Green Version]
- Frisaldi, E.; Carlino, E.; Zibetti, M.; Barbiani, D.; Dematteis, F.; Lanotte, M.; Lopiano, L.; Benedetti, F. The Placebo Effect on Bradykinesia in Parkinson’s Disease with and without Prior Drug Conditioning. Mov. Disord. 2017, 32, 1474–1478. [Google Scholar] [CrossRef]
- Tolusso, D.V.; Laurent, C.M.; Fullenkamp, A.M.; Tobar, D.A. Placebo Effect: Influence on Repeated Intermittent Sprint Performance on Consecutive Days. J. Strength Cond. Res. 2015, 29, 1915–1924. [Google Scholar] [CrossRef]
- Turi, Z.; Bjørkedal, E.; Gunkel, L.; Antal, A.; Paulus, W.; Mittner, M. Evidence for Cognitive Placebo and Nocebo Effects in Healthy Individuals. Sci. Rep. 2018, 8, 17443. [Google Scholar] [CrossRef]
- Benedetti, F. Placebo-Induced Improvements: How Therapeutic Rituals Affect the Patient’s Brain. J. Acupunct. Meridian Stud. 2012, 5, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Kong, J.; Spaeth, R.; Cook, A.; Kirsch, I.; Claggett, B.; Vangel, M.; Gollub, R.L.; Smoller, J.W.; Kaptchuk, T.J. Are All Placebo Effects Equal? Placebo Pills, Sham Acupuncture, Cue Conditioning and Their Association. PLoS ONE 2013, 8, e67485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.-C.; Yuan, T.-T.; Liu, T. Is Acupuncture a Placebo Therapy? Complement. Ther. Med. 2014, 22, 724–730. [Google Scholar] [CrossRef]
- Geuter, S.; Koban, L.; Wager, T.D. The Cognitive Neuroscience of Placebo Effects: Concepts, Predictions, and Physiology. Annu. Rev. Neurosci. 2017, 40, 167–188. [Google Scholar] [CrossRef] [PubMed]
- Eelen, P. Classical Conditioning: Classical Yet Modern. Psychol. Belg. 2018, 58, 196–211. [Google Scholar] [CrossRef] [Green Version]
- Frisaldi, E.; Piedimonte, A.; Benedetti, F. Placebo and Nocebo Effects: A Complex Interplay Between Psychological Factors and Neurochemical Networks. Am. J. Clin. Hypn. 2015, 57, 267–284. [Google Scholar] [CrossRef] [PubMed]
- Colloca, L.; Miller, F.G. How Placebo Responses Are Formed: A Learning Perspective. Philos. Trans. R. Soc. B 2011, 366, 1859–1869. [Google Scholar] [CrossRef] [Green Version]
- Carlino, E.; Torta, D.M.E.; Piedimonte, A.; Frisaldi, E.; Vighetti, S.; Benedetti, F. Role of Explicit Verbal Information in Conditioned Analgesia: Explicit Verbal Information in Conditioned Analgesia. Eur. J. Pain 2015, 19, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Ursano, A.M.; Sonnenberg, S.M.; Ursano, R.J. Physician-Patient Relationship. In Psychiatry; Tasman, A., Kay, J., Lieberman, J.A., First, M.B., Riba, M.B., Eds.; John Wiley & Sons, Ltd.: Chichester, UK, 2015; pp. 20–33. ISBN 978-1-118-75337-8. [Google Scholar]
- Rabinovich, M.; Kacen, L. Transference in View of a Classical Conditioning Model. Am. J. Psychol. 2012, 125, 209–223. [Google Scholar] [CrossRef]
- Carlino, E.; Benedetti, F. Placebo and Nocebo Effects. In The Handbook of Behavioral Medicine; Mostofsky, D.I., Ed.; John Wiley & Sons, Ltd.: Oxford, UK, 2014; pp. 36–57. ISBN 978-1-118-45394-0. [Google Scholar]
- Brown, W.A. Expectation, the Placebo Effect and the Response to Treatment. R. I. Med. J. 2015, 98, 19–21. [Google Scholar]
- Price, D.D.; Finniss, D.G.; Benedetti, F. A Comprehensive Review of the Placebo Effect: Recent Advances and Current Thought. Annu. Rev. Psychol. 2008, 59, 565–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, J.N.; Meyer, R.A. Mechanisms of Neuropathic Pain. Neuron 2006, 52, 77–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vachon-Presseau, E.; Berger, S.E.; Abdullah, T.B.; Huang, L.; Cecchi, G.; Griffith, J.W.; Schnitzer, T.J.; Apkarian, A.V. Brain and Psychological Determinants of Placebo Pill Response in Chronic Pain Patients. Neuroscience 2017, 9, 3397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wanigasekera, V.; Wartolowska, K.; Huggins, J.P.; Duff, E.P.; Vennart, W.; Whitlock, M.; Massat, N.; Pauer, L.; Rogers, P.; Hoggart, B.; et al. Disambiguating Pharmacological Mechanisms from Placebo in Neuropathic Pain Using Functional Neuroimaging. Br. J. Anaesth. 2018, 120, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Wager, T.D.; Atlas, L.Y.; Leotti, L.A.; Rilling, J.K. Predicting Individual Differences in Placebo Analgesia: Contributions of Brain Activity during Anticipation and Pain Experience. J. Neurosci. 2011, 31, 439–452. [Google Scholar] [CrossRef]
- Xu, L.; Wan, Y.; Ma, L.; Zheng, J.; Han, B.; Liu, F.-Y.; Yi, M.; Wan, Y. A Context-Based Analgesia Model in Rats: Involvement of Prefrontal Cortex. Neurosci. Bull. 2018, 34, 1047–1057. [Google Scholar] [CrossRef] [Green Version]
- Hikida, T.; Morita, M.; Macpherson, T. Neural Mechanisms of the Nucleus Accumbens Circuit in Reward and Aversive Learning. Neurosci. Res. 2016, 108, 1–5. [Google Scholar] [CrossRef]
- Watanabe, M. Emotional and Motivational Functions of the Prefrontal Cortex. Brain Nerve 2016, 68, 1291–1299. [Google Scholar] [CrossRef]
- Krummenacher, P.; Candia, V.; Folkers, G.; Schedlowski, M.; Schönbächler, G. Prefrontal Cortex Modulates Placebo Analgesia. Pain 2010, 148, 368–374. [Google Scholar] [CrossRef]
- Peciña, M.; Bohnert, A.S.B.; Sikora, M.; Avery, E.T.; Langenecker, S.A.; Mickey, B.J.; Zubieta, J.-K. Association between Placebo-Activated Neural Systems and Antidepressant Responses: Neurochemistry of Placebo Effects in Major Depression. JAMA Psychiatry 2015, 72, 1087–1094. [Google Scholar] [CrossRef]
- Petrovic, P.; Dietrich, T.; Fransson, P.; Andersson, J.; Carlsson, K.; Ingvar, M. Placebo in Emotional Processing—Induced Expectations of Anxiety Relief Activate a Generalized Modulatory Network. Neuron 2005, 46, 957–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte, D.F. Uma Breve História Do Ópio e Dos Opióides. Rev. Bras. Anestesiol. 2005, 55, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, A.; Marsch, L.A.; Joseph, H.; Portenoy, R.K. Opioids and the Treatment of Chronic Pain: Controversies, Current Status, and Future Directions. Exp. Clin. Psychopharmacol. 2008, 16, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.; Smith, T.W.; Kosterlitz, H.W.; Fothergill, L.A.; Morgan, B.A.; Morris, H.R. Identification of Two Related Pentapeptides from the Brain with Potent Opiate Agonist Activity. Nature 1975, 258, 577–580. [Google Scholar] [CrossRef] [PubMed]
- Grossman, A.; Clement-Jones, V. Opiate Receptors: Enkephalins and Endorphins. Clin. Endocrinol. Metab. 1983, 12, 31–56. [Google Scholar] [CrossRef]
- Gu, Z.-H.; Wang, B.; Kou, Z.-Z.; Bai, Y.; Chen, T.; Dong, Y.-L.; Li, H.; Li, Y.-Q. Endomorphins: Promising Endogenous Opioid Peptides for the Development of Novel Analgesics. Neurosignals 2017, 25, 98–116. [Google Scholar] [CrossRef] [Green Version]
- Schwarzer, C. 30 Years of Dynorphins—New Insights on Their Functions in Neuropsychiatric Diseases. Pharmacol. Ther. 2009, 123, 353–370. [Google Scholar] [CrossRef] [Green Version]
- Manglik, A.; Kruse, A.C.; Kobilka, T.S.; Thian, F.S.; Mathiesen, J.M.; Sunahara, R.K.; Pardo, L.; Weis, W.I.; Kobilka, B.K.; Granier, S. Crystal Structure of the Μ-Opioid Receptor Bound to a Morphinan Antagonist. Nature 2012, 485, 321–326. [Google Scholar] [CrossRef] [Green Version]
- Granier, S.; Manglik, A.; Kruse, A.C.; Kobilka, T.S.; Thian, F.S.; Weis, W.I.; Kobilka, B.K. Structure of the δ-Opioid Receptor Bound to Naltrindole. Nature 2012, 485, 400–404. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Wacker, D.; Mileni, M.; Katritch, V.; Han, G.W.; Vardy, E.; Liu, W.; Thompson, A.A.; Huang, X.-P.; Carroll, F.I.; et al. Structure of the Human κ-Opioid Receptor in Complex with JDTic. Nature 2012, 485, 327–332. [Google Scholar] [CrossRef]
- Peng, J.; Sarkar, S.; Chang, S.L. Opioid Receptor Expression in Human Brain and Peripheral Tissues Using Absolute Quantitative Real-Time RT-PCR. Drug Alcohol Depend. 2012, 124, 223–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pathan, H.; Williams, J. Basic Opioid Pharmacology: An Update. Br. J. Pain 2012, 6, 11–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, C. Opioid Receptors. Annu. Rev. Med. 2016, 67, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.D.; Gordon, N.C.; Fields, H.L. The Mechanism of Placebo Analgesia. Lancet 1978, 2, 654–657. [Google Scholar] [CrossRef]
- Eippert, F.; Bingel, U.; Schoell, E.D.; Yacubian, J.; Klinger, R.; Lorenz, J.; Büchel, C. Activation of the Opioidergic Descending Pain Control System Underlies Placebo Analgesia. Neuron 2009, 63, 533–543. [Google Scholar] [CrossRef] [Green Version]
- Lipman, J.J.; Miller, B.E.; Mays, K.S.; Miller, M.N.; North, W.C.; Byrne, W.L. Peak B Endorphin Concentration in Cerebrospinal Fluid: Reduced in Chronic Pain Patients and Increased during the Placebo Response. Psychopharmacology 1990, 102, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.-R.; Zhang, W.-C.; Wang, J.-Y.; Guo, J.-Y. The Opioid Placebo Analgesia Is Mediated Exclusively through μ-Opioid Receptor in Rat. Int. J. Neuropsychopharmacol. 2013, 16, 849–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peciña, M.; Love, T.; Stohler, C.S.; Goldman, D.; Zubieta, J.-K. Effects of the Mu Opioid Receptor Polymorphism (OPRM1 A118G) on Pain Regulation, Placebo Effects and Associated Personality Trait Measures. Neuropsychopharmacology 2015, 40, 957–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zubieta, J.-K. Placebo Effects Mediated by Endogenous Opioid Activity on-Opioid Receptors. J. Neurosci. 2005, 25, 7754–7762. [Google Scholar] [CrossRef] [Green Version]
- Scott, D.J.; Stohler, C.S.; Egnatuk, C.M.; Wang, H.; Koeppe, R.A.; Zubieta, J.-K. Placebo and Nocebo Effects Are Defined by Opposite Opioid and Dopaminergic Responses. Arch. Gen. Psychiatry 2008, 65, 220. [Google Scholar] [CrossRef] [Green Version]
- Zubieta, J.-K.; Stohler, C.S. Neurobiological Mechanisms of Placebo Responses. Ann. N. Y. Acad. Sci. 2009, 1156, 198–210. [Google Scholar] [CrossRef] [Green Version]
- Atlas, L.Y.; Wager, T.D. A Meta-Analysis of Brain Mechanisms of Placebo Analgesia: Consistent Findings and Unanswered Questions. In Placebo Handbook of Experimental Pharmacology; Benedetti, F., Enck, P., Frisaldi, E., Schedlowski, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; Volume 225, pp. 37–69. ISBN 978-3-662-44518-1. [Google Scholar]
- Eippert, F.; Finsterbusch, J.; Bingel, U.; Büchel, C. Direct Evidence for Spinal Cord Involvement in Placebo Analgesia. Science 2009, 326, 404. [Google Scholar] [CrossRef]
- Amanzio, M.; Benedetti, F. Neuropharmacological Dissection of Placebo Analgesia: Expectation-Activated Opioid Systems versus Conditioning-Activated Specific Subsystems. J. Neurosci. 1999, 19, 484–494. [Google Scholar] [CrossRef] [PubMed]
- Vase, L.; Robinson, M.E.; Verne, N.G.; Price, D.D. Increased Placebo Analgesia over Time in Irritable Bowel Syndrome (IBS) Patients Is Associated with Desire and Expectation but Not Endogenous Opioid Mechanisms. Pain 2005, 115, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.-Y.; Wang, J.-Y.; Luo, F. Dissection of Placebo Analgesia in Mice: The Conditions for Activation of Opioid and Non-Opioid Systems. J. Psychopharmacol. 2010, 24, 1561–1567. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.-S.; Lee, B.; Park, H.-J.; Olausson, H.; Enck, P.; Chae, Y. A New Animal Model of Placebo Analgesia: Involvement of the Dopaminergic System in Reward Learning. Sci. Rep. 2015, 5, 17140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackie, K. Distribution of Cannabinoid Receptors in the Central and Peripheral Nervous System. Handb. Exp. Pharmacol. 2005, 168, 299–325. [Google Scholar] [CrossRef]
- Dhopeshwarkar, A.; Mackie, K. Cannabinoid Receptors as a Therapeutic Target—What Does the Future Hold? Mol. Pharmacol. 2014, 86, 430–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodhams, S.G.; Chapman, V.; Finn, D.P.; Hohmann, A.G.; Neugebauer, V. The Cannabinoid System and Pain. Neuropharmacology 2017, 124, 105–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedetti, F.; Amanzio, M.; Rosato, R.; Blanchard, C. Nonopioid Placebo Analgesia Is Mediated by CB1 Cannabinoid Receptors. Nat. Med. 2011, 17, 1228–1230. [Google Scholar] [CrossRef]
- Peciña, M.; Martínez-Jauand, M.; Hodgkinson, C.; Stohler, C.S.; Goldman, D.; Zubieta, J.K. FAAH Selectively Influences Placebo Effects. Mol. Psychiatry 2014, 19, 385–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brodermann, H.M. Pain, Pleasure and Placebo: The Cannabinoids in Reward Processing and the Perception of Pain. Ment. Health Addict. Res. 2016, 1, 59–63. [Google Scholar] [CrossRef] [Green Version]
- Klein, M.O.; Battagello, D.S.; Cardoso, A.R.; Hauser, D.N.; Bittencourt, J.C.; Correa, R.G. Dopamine: Functions, Signaling, and Association with Neurological Diseases. Cell Mol. Neurobiol. 2019, 39, 31–59. [Google Scholar] [CrossRef]
- Beaulieu, J.-M.; Gainetdinov, R.R. The Physiology, Signaling, and Pharmacology of Dopamine Receptors. Pharmacol. Rev. 2011, 63, 182–217. [Google Scholar] [CrossRef] [Green Version]
- Beaulieu, J.-M.; Espinoza, S.; Gainetdinov, R.R. Dopamine Receptors—IUPHAR Review 13: Dopamine Receptors. Br. J. Pharmacol. 2015, 172, 1–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irizarry, K.J.L.; Licinio, J. An Explanation for the Placebo Effect? Science 2005, 307, 1411–1412. [Google Scholar] [CrossRef] [PubMed]
- Peciña, M.; Zubieta, J.-K. Molecular Mechanisms of Placebo Responses in Humans. Mol. Psychiatry 2015, 20, 416–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarcho, J.M.; Feier, N.A.; Labus, J.S.; Naliboff, B.; Smith, S.R.; Hong, J.-Y.; Colloca, L.; Tillisch, K.; Mandelkern, M.A.; Mayer, E.A.; et al. Placebo Analgesia: Self-Report Measures and Preliminary Evidence of Cortical Dopamine Release Associated with Placebo Response. NeuroImage Clin. 2016, 10, 107–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaasinen, V.; Aalto, S.; Nagren, K.; Rinne, J.O. Expectation of Caffeine Induces Dopaminergic Responses in Humans. Eur. J. Neurosci. 2004, 19, 2352–2356. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Schaeffer, W. Is Cell Death Primary or Secondary in the Pathophysiology of Idiopathic Parkinson’s Disease? Biomolecules 2015, 5, 1467–1479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Fuente-Fernández, R.; Ruth, T.J.; Sossi, V.; Schulzer, M.; Calne, D.B.; Stoessl, A.J. Expectation and Dopamine Release: Mechanism of the Placebo Effect in Parkinson’s Disease. Science 2001, 293, 1164–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Fuente-Fernández, R.; Phillips, A.G.; Zamburlini, M.; Sossi, V.; Calne, D.B.; Ruth, T.J.; Stoessl, A.J. Dopamine Release in Human Ventral Striatum and Expectation of Reward. Behav. Brain Res. 2002, 136, 359–363. [Google Scholar] [CrossRef]
- Strafella, A.P.; Ko, J.H.; Monchi, O. Therapeutic Application of Transcranial Magnetic Stimulation in Parkinson’s Disease: The Contribution of Expectation. NeuroImage 2006, 31, 1666–1672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lidstone, S.C.; Schulzer, M.; Dinelle, K.; Mak, E.; Sossi, V.; Ruth, T.J.; de la Fuente-Fernández, R.; Phillips, A.G.; Stoessl, A.J. Effects of Expectation on Placebo-Induced Dopamine Release in Parkinson Disease. Arch. Gen. Psychiatry 2010, 67, 857. [Google Scholar] [CrossRef] [Green Version]
- Quattrone, A.; Barbagallo, G.; Cerasa, A.; Stoessl, A.J. Neurobiology of Placebo Effect in Parkinson’s Disease: What We Have Learned and Where We Are Going: Placebo Effect in PD. Mov. Disord. 2018, 33, 1213–1227. [Google Scholar] [CrossRef] [PubMed]
- Haour, F. Mechanisms of the Placebo Effect and of Conditioning. Neuroimmunomodulation 2005, 12, 195–200. [Google Scholar] [CrossRef]
- Vinar, O. Addiction to Placebo. Am. J. Psychiatry 1978, 135, 1000. [Google Scholar] [CrossRef]
- Kessner, S.; Sprenger, C.; Wrobel, N.; Wiech, K.; Bingel, U. Effect of Oxytocin on Placebo Analgesia: A Randomized Study. JAMA 2013, 310, 1733–1735. [Google Scholar] [CrossRef] [PubMed]
- Skvortsova, A.; Veldhuijzen, D.S.; Van Middendorp, H.; Van den Bergh, O.; Evers, A.W.M. Enhancing Placebo Effects in Somatic Symptoms Through Oxytocin. Psychosom. Med. 2018, 80, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colloca, L.; Pine, D.S.; Ernst, M.; Miller, F.G.; Grillon, C. Vasopressin Boosts Placebo Analgesic Effects in Women: A Randomized Trial. Biol. Psychiatry 2016, 79, 794–802. [Google Scholar] [CrossRef] [PubMed]
- Boggero, I.A.; Segerstrom, S.C. Human Psychoneuroimmunology. In Encyclopedia of Mental Health; Elsevier: Amsterdam, The Netherlands, 2016; pp. 343–349. ISBN 978-0-12-397753-3. [Google Scholar]
- Dhabhar, F.S.; Malarkey, W.B.; Neri, E.; McEwen, B.S. Stress-Induced Redistribution of Immune Cells—From Barracks to Boulevards to Battlefields: A Tale of Three Hormones—Curt Richter Award Winner. Psychoneuroendocrinology 2012, 37, 1345–1368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohleder, N. Acute and Chronic Stress Induced Changes in Sensitivity of Peripheral Inflammatory Pathways to the Signals of Multiple Stress Systems—2011 Curt Richter Award Winner. Psychoneuroendocrinology 2012, 37, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Morey, J.N.; Boggero, I.A.; Scott, A.B.; Segerstrom, S.C. Current Directions in Stress and Human Immune Function. Curr. Opin. Psychol. 2015, 5, 13–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herkenham, M.; Kigar, S.L. Contributions of the Adaptive Immune System to Mood Regulation: Mechanisms and Pathways of Neuroimmune Interactions. Prog. Neuropsychopharmacol. Biol. Psychiatry 2017, 79, 49–57. [Google Scholar] [CrossRef]
- Bonaz, B.; Sinniger, V.; Pellissier, S. Anti-Inflammatory Properties of the Vagus Nerve: Potential Therapeutic Implications of Vagus Nerve Stimulation: Anti-Inflammatory Effect of Vagus Nerve Stimulation. J. Physiol. 2016, 594, 5781–5790. [Google Scholar] [CrossRef] [Green Version]
- Madden, K.S. Sympathetic Neural-Immune Interactions Regulate Hematopoiesis, Thermoregulation and Inflammation in Mammals. Dev. Comp. Immunol. 2017, 66, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Bonaz, B.; Sinniger, V.; Pellissier, S. The Vagus Nerve in the Neuro-Immune Axis: Implications in the Pathology of the Gastrointestinal Tract. Front. Immunol. 2017, 8, 1452. [Google Scholar] [CrossRef]
- Erickson, M.A.; Banks, W.A. Neuroimmune Axes of the Blood–Brain Barriers and Blood–Brain Interfaces: Bases for Physiological Regulation, Disease States, and Pharmacological Interventions. Pharmacol. Rev. 2018, 70, 278–314. [Google Scholar] [CrossRef]
- Quan, N. In-Depth Conversation: Spectrum and Kinetics of Neuroimmune Afferent Pathways. Brain Behav. Immun. 2014, 40, 1–8. [Google Scholar] [CrossRef]
- Prossin, A.; Koch, A.; Campbell, P.; Laumet, G.; Stohler, C.S.; Dantzer, R.; Zubieta, J.-K. Effects of Placebo Administration on Immune Mechanisms and Relationships with Central Endogenous Opioid Neurotransmission. Mol. Psychiatry 2021, in press. [Google Scholar] [CrossRef]
- Albring, A.; Wendt, L.; Benson, S.; Witzke, O.; Kribben, A.; Engler, H.; Schedlowski, M. Placebo Effects on the Immune Response in Humans: The Role of Learning and Expectation. PLoS ONE 2012, 7, e49477. [Google Scholar] [CrossRef] [Green Version]
- Hadamitzky, M.; Sondermann, W.; Benson, S.; Schedlowski, M. Placebo Effects in the Immune System. In International Review of Neurobiology; Elsevier: Amsterdam, The Netherlands, 2018; Volume 138, pp. 39–59. ISBN 978-0-12-814325-4. [Google Scholar]
- Exton, M.S.; von Hörsten, S.; Schult, M.; Vöge, J.; Strubel, T.; Donath, S.; Steinmüller, C.; Seeliger, H.; Nagel, E.; Westermann, J.; et al. Behaviorally Conditioned Immunosuppression Using Cyclosporine A: Central Nervous System Reduces IL-2 Production via Splenic Innervation. J. Neuroimmunol. 1998, 88, 182–191. [Google Scholar] [CrossRef]
- Exton, M.S.; Schult, M.; Donath, S.; Strubel, T.; Bode, U.; del Rey, A.; Westermann, J.; Schedlowski, M. Conditioned Immunosuppression Makes Subtherapeutic Cyclosporin Effective via Splenic Innervation. Am. J. Physiol. 1999, 276, R1710–R1717. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Frede, S.; Harnish, M.J.; Exton, M.S.; Schedlowski, M. Beta-Adrenoceptor-Induced Inhibition of Rat Splenocyte Proliferation: Cytokine Gene Transcription as the Target of Action. Immunobiology 2002, 206, 345–353. [Google Scholar] [CrossRef]
- Exton, M.S.; Gierse, C.; Meier, B.; Mosen, M.; Xie, Y.; Frede, S.; Goebel, M.U.; Limmroth, V.; Schedlowski, M. Behaviorally Conditioned Immunosuppression in the Rat Is Regulated via Noradrenaline and Beta-Adrenoceptors. J. Neuroimmunol. 2002, 131, 21–30. [Google Scholar] [CrossRef]
- Pacheco-López, G.; Doenlen, R.; Krügel, U.; Arnold, M.; Wirth, T.; Riether, C.; Engler, A.; Niemi, M.-B.; Christians, U.; Engler, H.; et al. Neurobehavioural Activation during Peripheral Immunosuppression. Int. J. Neuropsychopharmacol. 2013, 16, 137–149. [Google Scholar] [CrossRef] [Green Version]
- Hörbelt, T.; Hetze, S.; Schedlowski, M.; Lückemann, L. Die gelernte Placeboantwort im Immunsystem. Nervenarzt 2020, 91, 667–674. [Google Scholar] [CrossRef]
- Wirth, T.; Ober, K.; Prager, G.; Vogelsang, M.; Benson, S.; Witzke, O.; Kribben, A.; Engler, H.; Schedlowski, M. Repeated Recall of Learned Immunosuppression: Evidence from Rats and Men. Brain Behav. Immun. 2011, 25, 1444–1451. [Google Scholar] [CrossRef]
- Kirchhof, J.; Petrakova, L.; Brinkhoff, A.; Benson, S.; Schmidt, J.; Unteroberdörster, M.; Wilde, B.; Kaptchuk, T.J.; Witzke, O.; Schedlowski, M. Learned Immunosuppressive Placebo Responses in Renal Transplant Patients. Proc. Natl. Acad. Sci. USA 2018, 115, 4223–4227. [Google Scholar] [CrossRef] [Green Version]
- Lueckemann, L.; Bösche, K.; Engler, H.; Schwitalla, J.-C.; Hadamitzky, M.; Schedlowski, M. Pre-Exposure to the Unconditioned or Conditioned Stimulus Does Not Affect Learned Immunosuppression in Rats. Brain Behav. Immun. 2016, 51, 252–257. [Google Scholar] [CrossRef]
- Buske-Kirschbaum, A.; Kirschbaum, C.; Stierle, H.; Lehnert, H.; Hellhammer, D. Conditioned Increase of Natural Killer Cell Activity (NKCA) in Humans. Psychosom. Med. 1992, 54, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Buske-Kirschbaum, A.; Kirschbaum, C.; Stierle, H.; Jabaij, L.; Hellhammer, D. Conditioned Manipulation of Natural Killer (NK) Cells in Humans Using a Discriminative Learning Protocol. Biol. Psychol. 1994, 38, 143–155. [Google Scholar] [CrossRef]
- Grigoleit, J.-S.; Kullmann, J.S.; Winkelhaus, A.; Engler, H.; Wegner, A.; Hammes, F.; Oberbeck, R.; Schedlowski, M. Single-Trial Conditioning in a Human Taste-Endotoxin Paradigm Induces Conditioned Odor Aversion but Not Cytokine Responses. Brain Behav. Immun. 2012, 26, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Coover, G.D.; Sutton, B.R.; Heybach, J.P. Conditioning Decreases in Plasma Corticosterone Level in Rats by Paring Stimuli with Daily Feedings. J. Comp. Physiol. Psychol. 1977, 91, 716–726. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, F.; Pollo, A.; Lopiano, L.; Lanotte, M.; Vighetti, S.; Rainero, I. Conscious Expectation and Unconscious Conditioning in Analgesic, Motor, and Hormonal Placebo/Nocebo Responses. J. Neurosci. 2003, 23, 4315–4323. [Google Scholar] [CrossRef] [PubMed]
- Barreto, R.E.; Volpato, G.L. Evaluating Feeding as Unconditioned Stimulus for Conditioning of an Endocrine Effect in Nile Tilapia. Physiol. Behav. 2007, 92, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Ader, R. Conditioned Adrenocortical Steroid Elevations in the Rat. J. Comp. Physiol. Psychol. 1976, 90, 1156–1163. [Google Scholar] [CrossRef]
- Hall, G.; Stockhorst, U.; Enck, P.; Klosterhalfen, S. Overshadowing and Latent Inhibition in Nausea-Based Context Conditioning in Humans: Theoretical and Practical Implications. Q. J. Exp. Psychol. 2016, 69, 1227–1238. [Google Scholar] [CrossRef]
- Sabbioni, M.E.; Bovbjerg, D.H.; Mathew, S.; Sikes, C.; Lasley, B.; Stokes, P.E. Classically Conditioned Changes in Plasma Cortisol Levels Induced by Dexamethasone in Healthy Men. FASEB J. 1997, 11, 1291–1296. [Google Scholar] [CrossRef]
- Davis, K.W.; Cepeda-Benito, A.; Harraid, J.H.; Wellman, P.J. Plasma Corticosterone in the Rat in Response to Nicotine and Saline Injections in a Context Previously Paired or Unpaired with Nicotine. Psychopharmacology 2005, 180, 466–472. [Google Scholar] [CrossRef]
- Stockhorst, U.; Gritzmann, E.; Klopp, K.; Schottenfeld-Naor, Y.; Hubinger, A.; Berresheim, H.-W.; Steingruber, H.-J.; Gries, F.A. Classical Conditioning of Insulin Effects in Healthy Humans. Psychosom. Med. 1999, 61, 424–435. [Google Scholar] [CrossRef] [PubMed]
- Detke, M.J.; Brandon, S.E.; Weingarten, H.P.; Rodin, J.; Wagner, A.R. Modulation of Behavioral and Insulin Responses by Contextual Stimuli Paired with Food. Physiol. Behav. 1989, 45, 845–851. [Google Scholar] [CrossRef]
- Roozendaal, B.; Oldenburger, W.P.; Strubbe, J.H.; Koolhaas, J.M.; Bohus, B. The Central Amygdala Is Involved in the Conditioned but Not in the Meal-Induced Cephalic Insulin Response in the Rat. Neurosci. Lett. 1990, 116, 210–215. [Google Scholar] [CrossRef]
- Stockhorst, U.; Mahl, N.; Krueger, M.; Huenig, A.; Schottenfeld-Naor, Y.; Huebinger, A.; Berresheim, H.-W.; Steingrueber, H.-J.; Scherbaum, W.A. Classical Conditioning and Conditionability of Insulin and Glucose Effects in Healthy Humans. Physiol. Behav. 2004, 81, 375–388. [Google Scholar] [CrossRef]
- Stockhorst, U.; de Fries, D.; Steingrueber, H.-J.; Scherbaum, W.A. Unconditioned and Conditioned Effects of Intranasally Administered Insulin vs. Placebo in Healthy Men: A Randomised Controlled Trial. Diabetologia 2011, 54, 1502–1506. [Google Scholar] [CrossRef] [Green Version]
- Overduin, J.; Jansen, A. Conditioned Insulin and Blood Sugar Responses in Humans in Relation to Binge Eating. Physiol. Behav. 1997, 61, 569–575. [Google Scholar] [CrossRef]
- Onaka, T.; Yagi, K. Oxytocin Release from the Neurohypophysis after the Taste Stimuli Previously Paired with Intravenous Cholecystokinin in Anaesthetized Rats. J. Neuroendocrinol. 1998, 10, 309–316. [Google Scholar] [CrossRef]
- Tancin, V.; Kraetzl, W.-D.; Schams, D.; Bruckmaier, R.M. The Effects of Conditioning to Suckling, Milking and of Calf Presence on the Release of Oxytocin in Dairy Cows. Appl. Anim. Behav. Sci. 2001, 72, 235–246. [Google Scholar] [CrossRef]
- Graham, J.M.; Desjardins, C. Classical Conditioning: Induction of Luteinizing Hormone and Testosterone Secretion in Anticipation of Sexual Activity. Science 1980, 210, 1039–1041. [Google Scholar] [CrossRef]
- Golombek, D.A.; Chuluyan, H.E.; Kanterewicz, B.I.; Cardinali, D.P. Increased Pineal Melatonin Content Coupled to Restricted Water Availability in a Pavlovian Conditioning Paradigm in Rats. J. Neural Transm. 1994, 98, 237–246. [Google Scholar] [CrossRef]
- Keller, A.; Akintola, T.; Colloca, L. Placebo Analgesia in Rodents: Current and Future Research. Int. Rev. Neurobiol. 2018, 138, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annoni, M.; Miller, F.G. Placebos in Clinical Practice: An Ethical Overview. Douleur Analg. 2014, 27, 215–220. [Google Scholar] [CrossRef]
- American Medical Association. American Medical Association Code of Ethics Opinion 8.083 (2006) Placebo Use in Clinical Practice; American Medical Association: Chicago, IL, USA, 2006. [Google Scholar]
- Charlesworth, J.E.G.; Petkovic, G.; Kelley, J.M.; Hunter, M.; Onakpoya, I.; Roberts, N.; Miller, F.G.; Howick, J. Effects of Placebos without Deception Compared with No Treatment: A Systematic Review and Meta-Analysis. J. Evid. Based Med. 2017, 10, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho, C.; Caetano, J.M.; Cunha, L.; Rebouta, P.; Kaptchuk, T.J.; Kirsch, I. Open-Label Placebo Treatment in Chronic Low Back Pain: A Randomized Controlled Trial. Pain 2016, 157, 2766–2772. [Google Scholar] [CrossRef]
- Kaptchuk, T.J.; Friedlander, E.; Kelley, J.M.; Sanchez, M.N.; Kokkotou, E.; Singer, J.P.; Kowalczykowski, M.; Miller, F.G.; Kirsch, I.; Lembo, A.J. Placebos without Deception: A Randomized Controlled Trial in Irritable Bowel Syndrome. PLoS ONE 2010, 5, e15591. [Google Scholar] [CrossRef] [PubMed]
- Kelley, J.M.; Kaptchuk, T.J.; Cusin, C.; Lipkin, S.; Fava, M. Open-Label Placebo for Major Depressive Disorder: A Pilot Randomized Controlled Trial. Psychother. Psychosom. 2012, 81, 312–314. [Google Scholar] [CrossRef] [Green Version]
- Kam-Hansen, S.; Jakubowski, M.; Kelley, J.M.; Kirsch, I.; Hoaglin, D.C.; Kaptchuk, T.J.; Burstein, R. Altered Placebo and Drug Labeling Changes the Outcome of Episodic Migraine Attacks. Sci. Transl. Med. 2014, 6, 218ra5. [Google Scholar] [CrossRef] [Green Version]
- Krueger, G.G.; Elewski, B.; Papp, K.; Wang, A.; Zitnik, R.; Jahreis, A. Patients with Psoriasis Respond to Continuous Open-Label Etanercept Treatment after Initial Incomplete Response in a Randomized, Placebo-Controlled Trial. J. Am. Acad. Dermatol. 2006, 54, S112–S119. [Google Scholar] [CrossRef]
- Sandler, A.D.; Bodfish, J.W. Open-Label Use of Placebos in the Treatment of ADHD: A Pilot Study. Child Care Health Dev. 2008, 34, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, L.D.; Cookfair, D.L.; Rudick, R.A.; Herndon, R.M.; Richert, J.R.; Salazar, A.M.; Fischer, J.S.; Goodkin, D.E.; Granger, C.V.; Simon, J.H.; et al. Intramuscular Interferon Beta-1a for Disease Progression in Relapsing Multiple Sclerosis. The Multiple Sclerosis Collaborative Research Group (MSCRG). Ann. Neurol. 1996, 39, 285–294. [Google Scholar] [CrossRef]
- Faria, V.; Gingnell, M.; Hoppe, J.M.; Hjorth, O.; Alaie, I.; Frick, A.; Hultberg, S.; Wahlstedt, K.; Engman, J.; Månsson, K.N.T.; et al. Do You Believe It? Verbal Suggestions Influence the Clinical and Neural Effects of Escitalopram in Social Anxiety Disorder: A Randomized Trial. EBio Med. 2017, 24, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goebel, M.U.; Meykadeh, N.; Kou, W.; Schedlowski, M.; Hengge, U.R. Behavioral Conditioning of Antihistamine Effects in Patients with Allergic Rhinitis. Psychother. Psychosom. 2008, 77, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Bardo, M.T.; Valone, J.M. Morphine-Conditioned Analgesia Using a Taste Cue: Dissociation of Taste Aversion and Analgesia. Psychopharmacology 1994, 114, 269–274. [Google Scholar] [CrossRef]
- Miller, J.S.; Kelly, K.S.; Neisewander, J.L.; McCoy, D.F.; Bardo, M.T. Conditioning of Morphine-Induced Taste Aversion and Analgesia. Psychopharmacology 1990, 101, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Valone, J.M.; Randall, C.K.; Kraemer, P.J.; Bardo, M.T. Olfactory Cues and Morphine-Induced Conditioned Analgesia in Rats. Pharmacol. Biochem. Behav. 1998, 60, 115–118. [Google Scholar] [CrossRef]
- Akintola, T.; Tricou, C.; Raver, C.; Castro, A.; Colloca, L.; Keller, A. In Search of a Rodent Model of Placebo Analgesia in Chronic Orofacial Neuropathic Pain. Neurobiol. Pain 2019, 6, 100033. [Google Scholar] [CrossRef] [PubMed]
- McNabb, C.T.; White, M.M.; Harris, A.L.; Fuchs, P.N. The Elusive Rat Model of Conditioned Placebo Analgesia. Pain 2014, 155, 2022–2032. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Hu, D.; Yang, W.; Hayashinaka, E.; Wada, Y.; Watanabe, Y.; Zeng, Q.; Cui, Y. A Voxel-Based Analysis of Neurobiological Mechanisms in Placebo Analgesia in Rats. Neuroimage 2018, 178, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Mbizvo, G.K.; Nolan, S.J.; Nurmikko, T.J.; Goebel, A. Placebo Responses in Long-Standing Complex Regional Pain Syndrome: A Systematic Review and Meta-Analysis. J. Pain 2015, 16, 99–115. [Google Scholar] [CrossRef] [PubMed]
- Loder, E.; Goldstein, R.; Biondi, D. Placebo Effects in Oral Triptan Trials: The Scientific and Ethical Rationale for Continued Use of Placebo Controls. Cephalalgia 2005, 25, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Meissner, K.; Fässler, M.; Rücker, G.; Kleijnen, J.; Hróbjartsson, A.; Schneider, A.; Antes, G.; Linde, K. Differential Effectiveness of Placebo Treatments: A Systematic Review of Migraine Prophylaxis. JAMA Intern. Med. 2013, 173, 1941–1951. [Google Scholar] [CrossRef] [PubMed]
- Cragg, J.J.; Warner, F.M.; Finnerup, N.B.; Jensen, M.P.; Mercier, C.; Richards, J.S.; Wrigley, P.; Soler, D.; Kramer, J.L.K. Meta-Analysis of Placebo Responses in Central Neuropathic Pain: Impact of Subject, Study, and Pain Characteristics. Pain 2016, 157, 530–540. [Google Scholar] [CrossRef] [PubMed]
- Castelnuovo, G.; Giusti, E.M.; Manzoni, G.M.; Saviola, D.; Gabrielli, S.; Lacerenza, M.; Pietrabissa, G.; Cattivelli, R.; Spatola, C.A.M.; Rossi, A.; et al. What Is the Role of the Placebo Effect for Pain Relief in Neurorehabilitation? Clinical Implications from the Italian Consensus Conference on Pain in Neurorehabilitation. Front. Neurol. 2018, 9, 310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cepeda, M.S.; Berlin, J.A.; Gao, C.Y.; Wiegand, F.; Wada, D.R. Placebo Response Changes Depending on the Neuropathic Pain Syndrome: Results of a Systematic Review and Meta-Analysis. Pain Med. 2012, 13, 575–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Häuser, W.; Sarzi-Puttini, P.; Tölle, T.R.; Wolfe, F. Placebo and Nocebo Responses in Randomised Controlled Trials of Drugs Applying for Approval for Fibromyalgia Syndrome Treatment: Systematic Review and Meta-Analysis. Clin. Exp. Rheumatol. 2012, 30, 78–87. [Google Scholar] [PubMed]
- Macedo, A.; Baños, J.-E.; Farré, M. Placebo Response in the Prophylaxis of Migraine: A Meta-Analysis. Eur. J. Pain 2008, 12, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Schneider, T.; Luethi, J.; Mauermann, E.; Bandschapp, O.; Ruppen, W. Pain Response to Open Label Placebo in Induced Acute Pain in Healthy Adult Males. Anesthesiology 2020, 132, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Damien, J.; Colloca, L.; Bellei-Rodriguez, C.-É.; Marchand, S. Pain Modulation: From Conditioned Pain Modulation to Placebo and Nocebo Effects in Experimental and Clinical Pain. Int. Rev. Neurobiol. 2018, 139, 255–296. [Google Scholar] [CrossRef]
- Klinger, R.; Stuhlreyer, J.; Schwartz, M.; Schmitz, J.; Colloca, L. Clinical Use of Placebo Effects in Patients with Pain Disorders. Int. Rev. Neurobiol. 2018, 139, 107–128. [Google Scholar] [CrossRef] [PubMed]
- Darnall, B.D.; Colloca, L. Optimizing Placebo and Minimizing Nocebo to Reduce Pain, Catastrophizing, and Opioid Use: A Review of the Science and an Evidence-Informed Clinical Toolkit. In International Review of Neurobiology; Elsevier: Amsterdam, The Netherlands, 2018; Volume 139, pp. 129–157. ISBN 978-0-12-815416-8. [Google Scholar]
- Diederich, N.J.; Goetz, C.G. The Placebo Treatments in Neurosciences: New Insights from Clinical and Neuroimaging Studies. Neurology 2008, 71, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Chung, E.J.; Lee, W.Y.; Shin, H.Y.; Lee, G.H.; Choe, Y.-S.; Choi, Y.; Kim, B.J. Therapeutic Effect of Repetitive Transcranial Magnetic Stimulation in Parkinson’s Disease: Analysis of [11C] Raclopride PET Study. Mov. Disord. 2008, 23, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.H.; Feigin, A.; Mattis, P.J.; Tang, C.C.; Ma, Y.; Dhawan, V.; During, M.J.; Kaplitt, M.G.; Eidelberg, D. Network Modulation Following Sham Surgery in Parkinson’s Disease. J. Clin. Investig. 2014, 124, 3656–3666. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, L.; Braun, E.K.; Wager, T.D.; Shohamy, D. Mind Matters: Placebo Enhances Reward Learning in Parkinson’s Disease. Nat. Neurosci. 2014, 17, 1793–1797. [Google Scholar] [CrossRef] [Green Version]
- Espay, A.J.; Norris, M.M.; Eliassen, J.C.; Dwivedi, A.; Smith, M.S.; Banks, C.; Allendorfer, J.B.; Lang, A.E.; Fleck, D.E.; Linke, M.J.; et al. Placebo Effect of Medication Cost in Parkinson Disease: A Randomized Double-Blind Study. Neurology 2015, 84, 794–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shetty, N.; Friedman, J.H.; Kieburtz, K.; Marshall, F.J.; Oakes, D. The Placebo Response in Parkinson’s Disease. Parkinson Study Group. Clin. Neuropharmacol. 1999, 22, 207–212. [Google Scholar] [PubMed]
- Diamond, S.G.; Markham, C.H.; Treciokas, L.J. Double-Blind Trial of Pergolide for Parkinson’s Disease. Neurology 1985, 35, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Leurgans, S.; Raman, R.; Stebbins, G.T. Objective Changes in Motor Function during Placebo Treatment in PD. Neurology 2000, 54, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Wuu, J.; McDermott, M.P.; Adler, C.H.; Fahn, S.; Freed, C.R.; Hauser, R.A.; Olanow, W.C.; Shoulson, I.; Tandon, P.K.; et al. Placebo Response in Parkinson’s Disease: Comparisons among 11 Trials Covering Medical and Surgical Interventions. Mov. Disord. 2008, 23, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Leurgans, S.; Raman, R. Parkinson Study Group Placebo-Associated Improvements in Motor Function: Comparison of Subjective and Objective Sections of the UPDRS in Early Parkinson’s Disease. Mov. Disord. 2002, 17, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, F.; Frisaldi, E.; Carlino, E.; Giudetti, L.; Pampallona, A.; Zibetti, M.; Lanotte, M.; Lopiano, L. Teaching Neurons to Respond to Placebos. J. Physiol. 2016, 594, 5647–5660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumitriu, A.; Popescu, B.O. Placebo Effects in Neurological Diseases. J. Med. Life 2010, 3, 114–121. [Google Scholar]
- Oken, B.S. Placebo Effects: Clinical Aspects and Neurobiology. Brain 2008, 131, 2812–2823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beyenburg, S.; Stavem, K.; Schmidt, D. Placebo-Corrected Efficacy of Modern Antiepileptic Drugs for Refractory Epilepsy: Systematic Review and Meta-Analysis. Epilepsia 2010, 51, 7–26. [Google Scholar] [CrossRef] [PubMed]
- Marson, A.G.; Kadir, Z.A.; Chadwick, D.W. New Antiepileptic Drugs: A Systematic Review of Their Efficacy and Tolerability. BMJ 1996, 313, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Guekht, A.B.; Korczyn, A.D.; Bondareva, I.B.; Gusev, E.I. Placebo Responses in Randomized Trials of Antiepileptic Drugs. Epilepsy Behav. 2010, 17, 64–69. [Google Scholar] [CrossRef]
- Brown, W.A. Placebo as a Treatment for Depression. Neuropsychopharmacology 1994, 10, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, L.A.; Berman, J.S.; Neimeyer, R.A. Psychotherapy for the Treatment of Depression: A Comprehensive Review of Controlled Outcome Research. Psychol. Bull. 1990, 108, 30–49. [Google Scholar] [CrossRef]
- Rief, W.; Nestoriuc, Y.; Weiss, S.; Welzel, E.; Barsky, A.J.; Hofmann, S.G. Meta-Analysis of the Placebo Response in Antidepressant Trials. J. Affect. Disord. 2009, 118, 1–8. [Google Scholar] [CrossRef]
- Mavissakalian, M. The Placebo Effect in Agoraphobia. J. Nerv. Ment. Dis. 1987, 175, 95–99. [Google Scholar] [CrossRef]
- Mellergård, M.; Rosenberg, N.K. Patterns of Response during Placebo Treatment of Panic Disorder. Acta Psychiatry Scand. 1990, 81, 340–344. [Google Scholar] [CrossRef]
- Piercy, M.A.; Sramek, J.J.; Kurtz, N.M.; Cutler, N.R. Placebo Response in Anxiety Disorders. Ann. Pharmacother. 1996, 30, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Huppert, J.D.; Schultz, L.T.; Foa, E.B.; Barlow, D.H.; Davidson, J.R.T.; Gorman, J.M.; Shear, M.K.; Simpson, H.B.; Woods, S.W. Differential Response to Placebo among Patients with Social Phobia, Panic Disorder, and Obsessive-Compulsive Disorder. Am. J. Psychiatry 2004, 161, 1485–1487. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Kolts, R.L.; Rapaport, M.H.; Krishnan, K.R.R.; Brodhead, A.E.; Browns, W.A. Magnitude of Placebo Response and Drug-Placebo Differences across Psychiatric Disorders. Psychol. Med. 2005, 35, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Baldwin, D.S.; Dolberg, O.T.; Despiegel, N.; Bandelow, B. Which Factors Predict Placebo Response in Anxiety Disorders and Major Depression? An Analysis of Placebo-Controlled Studies of Escitalopram. J. Clin. Psychiatry 2006, 67, 1741–1746. [Google Scholar] [CrossRef] [PubMed]
- Pecknold, J.C.; Swinson, R.P.; Kuch, K.; Lewis, C.P. Alprazolam in Panic Disorder and Agoraphobia: Results from a Multicenter Trial. III. Discontinuation Effects. Arch. Gen. Psychiatry 1988, 45, 429–436. [Google Scholar] [CrossRef]
- Ballenger, J.C.; Burrows, G.D.; DuPont, R.L.; Lesser, I.M.; Noyes, R.; Pecknold, J.C.; Rifkin, A.; Swinson, R.P. Alprazolam in Panic Disorder and Agoraphobia: Results from a Multicenter Trial. I. Efficacy in Short-Term Treatment. Arch. Gen. Psychiatry 1988, 45, 413–422. [Google Scholar] [CrossRef]
- Weiss, R.D.; O’malley, S.S.; Hosking, J.D.; Locastro, J.S.; Swift, R.; COMBINE Study Research Group. Do Patients with Alcohol Dependence Respond to Placebo? Results from the COMBINE Study. J. Stud. Alcohol Drugs 2008, 69, 878–884. [Google Scholar] [CrossRef]
- Ader, R.; Cohen, N. Behaviorally Conditioned Immunosuppression and Murine Systemic Lupus Erythematosus. Science 1982, 215, 1534–1536. [Google Scholar] [CrossRef]
- Klosterhalfen, W.; Klosterhalfen, S. Pavlovian Conditioning of Immunosuppression Modifies Adjuvant Arthritis in Rats. Behav. Neurosci. 1983, 97, 663–666. [Google Scholar] [CrossRef]
- Kemeny, M.E.; Rosenwasser, L.J.; Panettieri, R.A.; Rose, R.M.; Berg-Smith, S.M.; Kline, J.N. Placebo Response in Asthma: A Robust and Objective Phenomenon. J. Allergy Clin. Immunol. 2007, 119, 1375–1381. [Google Scholar] [CrossRef] [Green Version]
- Kaptchuk, T.J.; Kelley, J.M.; Deykin, A.; Wayne, P.M.; Lasagna, L.C.; Epstein, I.O.; Kirsch, I.; Wechsler, M.E. Do “Placebo Responders” Exist? Contemp. Clin. Trials 2008, 29, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Olness, K.; Ader, R. Conditioning as an Adjunct in the Pharmacotherapy of Lupus Erythematosus. J. Dev. Behav. Pediatr. 1992, 13, 124–125. [Google Scholar] [CrossRef] [PubMed]
- Vits, S.; Cesko, E.; Benson, S.; Rueckert, A.; Hillen, U.; Schadendorf, D.; Schedlowski, M. Cognitive Factors Mediate Placebo Responses in Patients with House Dust Mite Allergy. PLoS ONE 2013, 8, e79576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meissner, K.; Bingel, U.; Colloca, L.; Wager, T.D.; Watson, A.; Flaten, M.A. The Placebo Effect: Advances from Different Methodological Approaches. J. Neurosci. 2011, 31, 16117–16124. [Google Scholar] [CrossRef]
- Vits, S.; Cesko, E.; Enck, P.; Hillen, U.; Schadendorf, D.; Schedlowski, M. Behavioural Conditioning as the Mediator of Placebo Responses in the Immune System. Philos. Trans. R Soc. Lond. B Biol. Sci. 2011, 366, 1799–1807. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, M.; Harke, R.; Denke, C. Open-Label Placebos Improve Symptoms in Allergic Rhinitis: A Randomized Controlled Trial. Psychother. Psychosom. 2016, 85, 373–374. [Google Scholar] [CrossRef]
- May, O.; Hansen, N.C. Comparison of Terbutaline, Isotonic Saline, Ambient Air and Non-Treatment in Patients with Reversible Chronic Airway Obstruction. Eur. Respir. J. 1988, 1, 527–530. [Google Scholar]
- Isenberg, S.A.; Lehrer, P.M.; Hochron, S. The Effects of Suggestion on Airways of Asthmatic Subjects Breathing Room Air as a Suggested Bronchoconstrictor and Bronchodilator. J. Psychosom. Res. 1992, 36, 769–776. [Google Scholar] [CrossRef]
- Wechsler, M.E.; Kelley, J.M.; Boyd, I.O.E.; Dutile, S.; Marigowda, G.; Kirsch, I.; Israel, E.; Kaptchuk, T.J. Active Albuterol or Placebo, Sham Acupuncture, or No Intervention in Asthma. N. Engl. J. Med. 2011, 365, 119–126. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Authors (REF) | Mechanism | Methodology | Results |
|---|---|---|---|
| Carlino et al. [18] | Psychological | Thirty-four healthy subjects were divided into two groups. Both received stimulation with a CO2 laser and a conditioning procedure through which two visual signals were coupled with increases and decreases in the strength of the stimulus. However, one group was verbally informed about the meaning of the keys and the second group was blinded. The LEP was used as the response index. | A decrease in pain classification (p < 0.05) and the amplitude of LEP (p < 0.01) in response to the signals was reported only in the group that received verbal information. This suggests that the visual–analgesic association does not happen without explicit verbal information. This highlights the importance of cognitive content as context to the keys. |
| Levine et al. [46] | Neurobiological (Opioids) | A double-blind study included 51 patients who underwent extraction of their third molar. The patients were distributed in groups to administer morphine, naloxone, or placebo in a different order. Two pain classification scales were used. One was visual and the second was verbal. | When the placebo group was divided into responsive and non-responsive, it was observed that naloxone administration increased pain scores only in responders. This suggests that the analgesic effect of placebo is reversible with naloxone as this is an antagonist of μ opioid receptors. |
| Benedetti et al. [63] | Neurobiological (Endocannabinoids) | The effects of rimonabant (CB1 receptor antagonist) as an inhibitor of the placebo effect were evaluated in 82 volunteers, who underwent a pain test with a tourniquet for five consecutive dates. Patients were divided into six groups to receive different combinations of placebo, pain killers, and rimonabant. | It was observed that in the group who received initial placebo analgesia, rimonabant blocked the placebo response entirely. Likewise, a statistically significant difference was observed for pain tolerance in the placebo group with rimonabant and the placebo without rimonabant (p < 0.001). |
| De la Fuente-Fernández et al. [74] | Neurobiological (Dopamine) | The release of endogenous dopamine caused by the placebo effect in patients with PD was measured through PET. It was estimated according to the competition between endogenous dopamine and RAC to couple to D2-D3 receptors. | The results of the patients before and after receiving the placebo were compared. A significant decrease was found in the coupling potential of striatum RAC of 17% in the caudate nucleus and 19% in the putamen (p < 0.005 for both). |
| Kirchhof et al. [104] | Immunological | Immunologic functions and basal neuroendocrine parameters were analyzed in 30 patients. They had all had kidney transplants and had been prescribed immune suppressant drugs. Afterward, the drug was administered together with a gustative CS (acquisitive) and finally, some doses were given with a placebo and the gustative CS (evocative). | On day two of the evocative phase, decreases in the proliferative capacity of T cells (p < 0.001), in the expression of γ-IFN mRNA (p = 0.05) and of cortisol circadian plasma levels (p < 0.05) were reported. However, there were no changes in the number of T cells or in the levels of IL-2 and catecholamines. |
| Sabbioni et al. [114] | Endocrine | In a double-blind study, 25 healthy men were divided into two groups. During the first phase, one group received placebo capsules (control) while the second one received a beverage with a distinct flavor and dexamethasone capsules (experimental). During the second phase, all subjects received a beverage and a placebo capsule every other day. | It was observed that the experimental group had significantly higher cortisol plasma levels when they received the beverage and the placebo capsule (p = 0.015). |
| Stockhorst et al. [120] | Endocrine | A double-blind assay evaluated 32 healthy men who were divided into two groups. On day 1, the first group received intranasal insulin together with an olfactory CS while the second group received a placebo together with the CS. On day 2, both groups received a placebo and CS. The evaluated variables were glycemia and insulin levels. | On day 2, the levels of peripheric insulin increased in group 1 and decreased in group 2 (p = 0.027). While the glycemic levels decreased in group 1 and increased in group 2, there was no statistically significant difference (p = 0.150). |
| Authors (REF) | Disorder | Methodology | Results |
|---|---|---|---|
| Carvalho et al. [130] | Neurological (Pain) | A randomized, controlled, open-label study included 83 patients who had chronic lumbar pain for less than three months. They randomly received either two tablets of placebo a day or their usual treatment for three weeks. The intensity of the pain was measured through three scales and a total score was obtained. | Greater pain reduction was observed in each of the scales in the patients who received a placebo in comparison to those receiving their usual treatment (p < 0.001). Similarly, those treated with a placebo had a reduction in their disability compared to those in their regular treatment (p < 0.001). |
| Jacobs et al. [136] | Neurological (Multiple sclerosis) | A Phase III, randomized, placebo-controlled, double-blind trial evaluating the use of beta-1a interferon included 301 patients with multiple sclerosis. Time to progression of disability was the primary endpoint, measured using the Expanded Disability State Scale from Kurtzke. | The placebo significantly delayed the time to progression (p = 0.02). Likewise, patients had fewer exacerbations (p = 0.03) and fewer and smaller brain lesions in magnetic resonance imaging (MRI) (p = 0.02). |
| Kelley et al. [132] | Psychiatric (Depression) | An open-label, placebo-controlled study included outpatient individuals who were diagnosed with major depressive disorder. They were randomized into a control group and an open-label placebo group. | There were no statistically significant differences between groups (p = 0.26). However, improvement before and after four weeks of receiving the placebo was observed (p = 0.03). |
| Faria et al. [137] | Psychiatric (Anxiety) | A trial evaluated 46 patients diagnosed with social anxiety, randomizing them to receive nine weeks of open or blinded treatment with escitalopram. The efficacy of the treatment was evaluated with the LSAS-SR and brain activity measured through MRI. | The results according to the LSAS-SR were better in the open-label group than the blinded group (p < 0.0001), with a response rate three times higher (50% vs. 14%; p = 0.009). This was correlated with greater activity of the posterior cingulate gyrus (p = 0.0006). |
| Goebel et al. [138] | Immunological (Allergic rhinitis) | Thirty patients with allergic rhinitis received a beverage with a distinct flavor followed by a dose of desloratadine for five consecutive days. Afterward, 10 patients received water together with a placebo pill (water group), 11 patients were exposed again to the beverage and the placebo pill (placebo group) and nine patients received water and desloratadine (drug group). | The water group had a decrease in symptoms and results of the cutaneous test but not in basophil activation. The placebo group had a decrease in basophils, decreased response in the cutaneous test and symptoms similar to those observed in the drug group. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega, Á.; Salazar, J.; Galban, N.; Rojas, M.; Ariza, D.; Chávez-Castillo, M.; Nava, M.; Riaño-Garzón, M.E.; Díaz-Camargo, E.A.; Medina-Ortiz, O.; et al. Psycho-Neuro-Endocrine-Immunological Basis of the Placebo Effect: Potential Applications beyond Pain Therapy. Int. J. Mol. Sci. 2022, 23, 4196. https://doi.org/10.3390/ijms23084196
Ortega Á, Salazar J, Galban N, Rojas M, Ariza D, Chávez-Castillo M, Nava M, Riaño-Garzón ME, Díaz-Camargo EA, Medina-Ortiz O, et al. Psycho-Neuro-Endocrine-Immunological Basis of the Placebo Effect: Potential Applications beyond Pain Therapy. International Journal of Molecular Sciences. 2022; 23(8):4196. https://doi.org/10.3390/ijms23084196
Chicago/Turabian StyleOrtega, Ángel, Juan Salazar, Néstor Galban, Milagros Rojas, Daniela Ariza, Mervin Chávez-Castillo, Manuel Nava, Manuel E. Riaño-Garzón, Edgar Alexis Díaz-Camargo, Oscar Medina-Ortiz, and et al. 2022. "Psycho-Neuro-Endocrine-Immunological Basis of the Placebo Effect: Potential Applications beyond Pain Therapy" International Journal of Molecular Sciences 23, no. 8: 4196. https://doi.org/10.3390/ijms23084196