
Plasma Fibulin-5 Levels as an Independent Predictor of a Poor Outcome after an Aneurysmal Subarachnoid Hemorrhage
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Results
2.1. Clinical Variables Related to a Poor Outcome
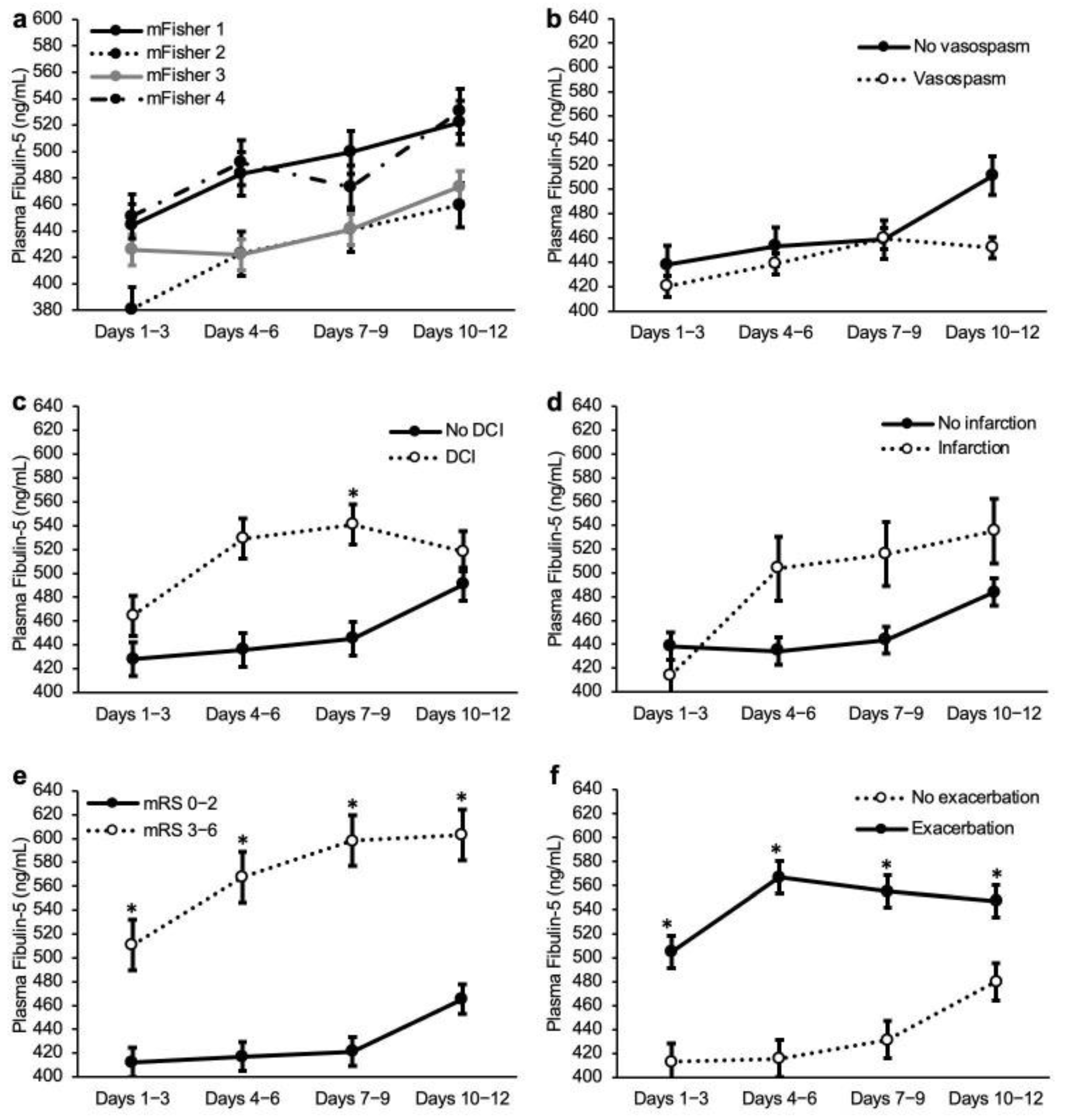
2.2. Plasma FBLN5 Levels
2.3. Receiver-Operating Characteristic (ROC) Curve Analyses for the Performance of Plasma FBLN5, to Differentiate the Poor Outcomes
2.4. Independent Determinants for a 90-Day Poor Outcome
2.5. Analyses in Non-Severe SAH Cases
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Clinical Variables
4.3. Measurement of Plasma FBLN5
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A
References
- Van Gijn, J.; Rinkel, G.J. Subarachnoid haemorrhage: Diagnosis, causes and management. Brain 2001, 124 Pt 2, 249–278. [Google Scholar] [CrossRef] [PubMed]
- Vergouwen, M.D.; Vermeulen, M.; van Gijn, J.; Rinkel, G.J.; Wijdicks, E.F.; Muizelaar, J.P.; Mendelow, A.D.; Juvela, S.; Yonas, H.; Terbrugge, K.G.; et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: Proposal of a multidisciplinary research group. Stroke 2010, 41, 2391–2395. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H. What is early brain injury? Transl. Stroke Res. 2015, 6, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Luo, J.; Reis, C.; Manaenko, A.; Zhang, J. Hydrocephalus after Subarachnoid Hemorrhage: Pathophysiology, Diagnosis, and Treatment. Biomed. Res. Int. 2017, 2017, 8584753. [Google Scholar] [CrossRef] [Green Version]
- Rush, B.; Wiskar, K.; Fruhstorfer, C.; Hertz, P. Association between seizures and mortality in patients with aneurysmal subarachnoid hemorrhage: A nationwide retrospective cohort analysis. Seizure 2016, 41, 66–69. [Google Scholar] [CrossRef] [Green Version]
- Taki, W.; Sakai, N.; Suzuki, H. Determinants of poor outcome after aneurysmal subarachnoid hemorrhage when both clipping and coiling are available: Prospective Registry of Subarachnoid Aneurysms Treatment (PRESAT) in Japan. World Neurosurg. 2011, 76, 437–445. [Google Scholar] [CrossRef]
- Buce-Satoba, I.; Rozkalne, D.; Stepanovs, J.; Mamaja, B.; Krumina, G.; Ozolina, A. Literature Review of Aneurysmal Subarachnoid Hemorrhage from Incidence to Treatment Options. Acta Chir. Latv. 2020, 18, 70–78. [Google Scholar] [CrossRef]
- Suzuki, H.; Kanamaru, H.; Kawakita, F.; Asada, R.; Fujimoto, M.; Shiba, M. Cerebrovascular pathophysiology of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. Histol. Histopathol. 2021, 36, 143–158. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Suzuki, H.; Uekawa, K.; Kawano, T.; Kim-Mitsuyama, S. Characteristics of Cerebrovascular Injury in the Hyperacute Phase after Induced Severe Subarachnoid Hemorrhage. Transl. Stroke Res. 2015, 6, 458–466. [Google Scholar] [CrossRef]
- Yanagisawa, H.; Schluterman, M.K.; Brekken, R.A. Fibulin-5, an integrin-binding matricellular protein: Its function in development and disease. J. Cell Commun. Signal 2009, 3, 337–347. [Google Scholar] [CrossRef]
- Nakamura, T.; Lozano, P.R.; Ikeda, Y.; Iwanaga, Y.; Hinek, A.; Minamisawa, S.; Cheng, C.F.; Kobuke, K.; Dalton, N.; Takada, Y.; et al. Fibulin-5/DANCE is essential for elastogenesis in vivo. Nature 2002, 415, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, H.; Davis, E.C.; Starcher, B.C.; Ouchi, T.; Yanagisawa, M.; Richardson, J.A.; Olson, E.N. Fibulin-5 is an elastin-binding protein essential for elastic fibre development in vivo. Nature 2002, 415, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Nonaka, R.; Onoue, S.; Wachi, H.; Sato, F.; Urban, Z.; Starcher, B.C.; Seyama, Y. DANCE/fibulin-5 promotes elastic fiber formation in a tropoelastin isoform-dependent manner. Clin. Biochem. 2009, 42, 713–721. [Google Scholar] [CrossRef]
- Guo, J.; Cheng, C.; Chen, C.S.; Xing, X.; Xu, G.; Feng, J.; Qin, X. Overexpression of Fibulin-5 Attenuates Ischemia/Reperfusion Injury after Middle Cerebral Artery Occlusion in Rats. Mol. Neurobiol. 2016, 53, 3154–3167. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wang, Y.; Bi, G. Limb remote ischaemic postconditioning-induced elevation of fibulin-5 confers neuroprotection to rats with cerebral ischaemia/reperfusion injury: Activation of the AKT pathway. Clin. Exp. Pharmacol. Physiol. 2017, 44, 656–663. [Google Scholar] [CrossRef]
- Hu, L.; Dong, M.X.; Zhao, H.; Xu, G.H.; Qin, X.Y. Fibulin-5: A novel biomarker for evaluating severity and predicting prognosis in patients with acute intracerebral haemorrhage. Eur. J. Neurol. 2016, 23, 1195–1201. [Google Scholar] [CrossRef]
- Elshony, H.S.; Okda, M.A.; El-Kabany, R.A. Ischemia-modified albumin and fibulin-5 as diagnostic and prognostic markers for acute cerebrovascular disease. Egypt. J. Neurol. Psychiatr. Neurosurg. 2021, 57, 12. [Google Scholar] [CrossRef]
- Papke, C.L.; Yanagisawa, H. Fibulin-4 and fibulin-5 in elastogenesis and beyond: Insights from mouse and human studies. Matrix Biol. 2014, 37, 142–149. [Google Scholar] [CrossRef]
- Kowal, R.C.; Richardson, J.A.; Miano, J.M.; Olson, E.N. EVEC, a novel epidermal growth factor-like repeat-containing protein upregulated in embryonic and diseased adult vasculature. Circ. Res. 1999, 84, 1166–1176. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, T.; Ruiz-Lozano, P.; Lindner, V.; Yabe, D.; Taniwaki, M.; Furukawa, Y.; Kobuke, K.; Tashiro, K.; Lu, Z.; Andon, N.L.; et al. DANCE, a novel secreted RGD protein expressed in developing, atherosclerotic, and balloon-injured arteries. J. Biol. Chem. 1999, 274, 22476–22483. [Google Scholar] [CrossRef]
- Hirai, M.; Ohbayashi, T.; Horiguchi, M.; Okawa, K.; Hagiwara, A.; Chien, K.R.; Kita, T.; Nakamura, T. Fibulin-5/DANCE has an elastogenic organizer activity that is abrogated by proteolytic cleavage in vivo. J. Cell Biol. 2007, 176, 1061–1071. [Google Scholar] [CrossRef] [Green Version]
- Chailley-Heu, B.; Boucherat, O.; Barlier-Mur, A.M.; Bourbon, J.R. FGF-18 is upregulated in the postnatal rat lung and enhances elastogenesis in myofibroblasts. Am. J. Physiol. Lung Cell Mol. Physiol. 2005, 288, L43–L51. [Google Scholar] [CrossRef]
- Fujimoto, M.; Shiba, M.; Kawakita, F.; Liu, L.; Shimojo, N.; Imanaka-Yoshida, K.; Yoshida, T.; Suzuki, H. Deficiency of tenascin-C and attenuation of blood-brain barrier disruption following experimental subarachnoid hemorrhage in mice. J. Neurosurg. 2016, 124, 1693–1702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Fujimoto, M.; Nakano, F.; Nishikawa, H.; Okada, T.; Kawakita, F.; Imanaka-Yoshida, K.; Yoshida, T.; Suzuki, H. Deficiency of Tenascin-C Alleviates Neuronal Apoptosis and Neuroinflammation after Experimental Subarachnoid Hemorrhage in Mice. Mol. Neurobiol. 2018, 55, 8346–8354. [Google Scholar] [CrossRef]
- Suzuki, H.; Fujimoto, M.; Kawakita, F.; Liu, L.; Nakatsuka, Y.; Nakano, F.; Nishikawa, H.; Okada, T.; Kanamaru, H.; Imanaka-Yoshida, K.; et al. Tenascin-C in brain injuries and edema after subarachnoid hemorrhage: Findings from basic and clinical studies. J. Neurosci. Res. 2020, 98, 42–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, T.; Suzuki, H.; Travis, Z.D.; Altay, O.; Tang, J.; Zhang, J.H. SPARC Aggravates Blood-Brain Barrier Disruption via Integrin alphaVbeta3/MAPKs/MMP-9 Signaling Pathway after Subarachnoid Hemorrhage. Oxid. Med. Cell Longev. 2021, 2021, 9739977. [Google Scholar] [CrossRef] [PubMed]
- Kawakita, F.; Kanamaru, H.; Asada, R.; Suzuki, H. Potential roles of matricellular proteins in stroke. Exp. Neurol. 2019, 322, 113057. [Google Scholar] [CrossRef]
- Suzuki, H.; Hasegawa, Y.; Chen, W.; Kanamaru, K.; Zhang, J.H. Recombinant osteopontin in cerebral vasospasm after subarachnoid hemorrhage. Ann. Neurol. 2010, 68, 650–660. [Google Scholar] [CrossRef] [Green Version]
- Fujimoto, M.; Shiba, M.; Kawakita, F.; Liu, L.; Shimojo, N.; Imanaka-Yoshida, K.; Yoshida, T.; Suzuki, H. Effects of Tenascin-C Knockout on Cerebral Vasospasm after Experimental Subarachnoid Hemorrhage in Mice. Mol. Neurobiol. 2018, 55, 1951–1958. [Google Scholar] [CrossRef]
- Nishikawa, H.; Liu, L.; Nakano, F.; Kawakita, F.; Kanamaru, H.; Nakatsuka, Y.; Okada, T.; Suzuki, H. Modified Citrus Pectin Prevents Blood-Brain Barrier Disruption in Mouse Subarachnoid Hemorrhage by Inhibiting Galectin-3. Stroke 2018, 49, 2743–2751. [Google Scholar] [CrossRef]
- Liu, L.; Kawakita, F.; Fujimoto, M.; Nakano, F.; Imanaka-Yoshida, K.; Yoshida, T.; Suzuki, H. Role of Periostin in Early Brain Injury after Subarachnoid Hemorrhage in Mice. Stroke 2017, 48, 1108–1111. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Hasegawa, Y.; Kanamaru, K.; Zhang, J.H. Mechanisms of osteopontin-induced stabilization of blood-brain barrier disruption after subarachnoid hemorrhage in rats. Stroke 2010, 41, 1783–1790. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H.; Ayer, R.; Sugawara, T.; Chen, W.; Sozen, T.; Hasegawa, Y.; Kanamaru, K.; Zhang, J.H. Protective effects of recombinant osteopontin on early brain injury after subarachnoid hemorrhage in rats. Crit. Care Med. 2010, 38, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Topkoru, B.C.; Altay, O.; Duris, K.; Krafft, P.R.; Yan, J.; Zhang, J.H. Nasal administration of recombinant osteopontin attenuates early brain injury after subarachnoid hemorrhage. Stroke 2013, 44, 3189–3194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakatsuka, Y.; Shiba, M.; Nishikawa, H.; Terashima, M.; Kawakita, F.; Fujimoto, M.; Suzuki, H.; pSEED Group. Acute-Phase Plasma Osteopontin as an Independent Predictor for Poor Outcome After Aneurysmal Subarachnoid Hemorrhage. Mol. Neurobiol. 2018, 55, 6841–6849. [Google Scholar] [CrossRef]
- Asada, R.; Suzuki, H. Osteopontin in post-subarachnoid hemorrhage pathologies. J. Integr. Neurosci. 2022, 21, 62. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.H.; Macdonald, R.L.; Keller, E. Biospecimens and molecular and cellular biomarkers in aneurysmal subarachnoid hemorrhage studies: Common data elements and standard reporting recommendations. Neurocrit. Care 2019, 30, S46–S59. [Google Scholar] [CrossRef]
- Nakatsuka, Y.; Kawakita, F.; Yasuda, R.; Umeda, Y.; Toma, N.; Sakaida, H.; Suzuki, H. Preventive effects of cilostazol against the development of shunt-dependent hydrocephalus after subarachnoid hemorrhage. J. Neurosurg. 2017, 127, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Nakatsuka, Y.; Terashima, M.; Nishikawa, H.; Kawakita, F.; Fujimoto, M.; Shiba, M.; Yasuda, R.; Toma, N.; Sakaida, H.; Suzuki, H. Current Status of Ruptured Cerebral Aneurysm Treatment in Regional Hospitals and Results of Coil Embolization. J. Neuroendovascular. Ther. 2018, 12, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, H.; Nakatsuka, Y.; Shiba, M.; Kawakita, F.; Fujimoto, M.; Suzuki, H.; pSEED Group. Increased Plasma Galectin-3 Preceding the Development of Delayed Cerebral Infarction and Eventual Poor Outcome in Non-Severe Aneurysmal Subarachnoid Hemorrhage. Transl. Stroke Res. 2018, 9, 110–119. [Google Scholar] [CrossRef]
- Kanamaru, H.; Kawakita, F.; Nakano, F.; Miura, Y.; Shiba, M.; Yasuda, R.; Toma, N.; Suzuki, H.; pSEED Group. Plasma Periostin and Delayed Cerebral Ischemia after Aneurysmal Subarachnoid Hemorrhage. Neurotherapeutics 2019, 16, 480–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanamaru, H.; Kawakita, F.; Asada, R.; Miura, Y.; Shiba, M.; Toma, N.; Suzuki, H.; pSEED Group. Prognostic factors varying with age in patients with aneurysmal subarachnoid hemorrhage. J. Clin. Neurosci. 2020, 76, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Claassen, J.; Bernardini, G.L.; Kreiter, K.; Bates, J.; Du, Y.E.; Copeland, D.; Connolly, E.S.; Mayer, S.A. Effect of cisternal and ventricular blood on risk of delayed cerebral ischemia after subarachnoid hemorrhage: The Fisher scale revisited. Stroke 2001, 32, 2012–2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 204) | mRS 0–2 (n = 127) | mRS 3–6 (n = 77) | p Value | |
|---|---|---|---|---|
| Age | ||||
| Median (IQR), years | 66.0 (51.8–74.3) | 60.0 (48.0–69.0) | 74.0 (66.0–82.0) | <0.001 a |
| ≥75 years old | 51 (25.0) | 14 (11.0) | 37 (48.1) | <0.001 b |
| Female | 149 (73.0) | 86 (67.7) | 63 (81.8) | 0.028 b |
| Past history | ||||
| SAH | 10 (4.9) | 5 (3.9) | 5 (6.5) | 0.308 c |
| Cerebral infarction | 9 (4.4) | 2 (1.6) | 7 (9.1) | 0.016 c |
| Hypertension | 90 (44.1) | 56 (44.1) | 34 (44.2) | 0.993 b |
| Dyslipidemia | 23 (11.3) | 12 (9.4) | 11 (14.3) | 0.290 b |
| Diabetes mellitus | 15 (7.4) | 8 (6.3) | 7 (9.1) | 0.459 b |
| Family history of SAH | 21 (10.3) | 16 (12.6) | 5 (6.5) | 0.164 b |
| Current smoking | 45 (22.1) | 33 (26.0) | 12 (15.6) | 0.082 b |
| Pre-onset mRS | ||||
| 0 | 188 (92.2) | 123 (96.9) | 65 (84.4) | 0.002 c |
| 1 | 13 (6.4) | 4 (3.1) | 9 (11.7) | 0.018 c |
| 2 | 3 (1.5) | 0 (0.0) | 3 (3.9) | 0.052 c |
| Admission WFNS grade | ||||
| I-III | 127 (62.3) | 100 (78.7) | 27 (35.1) | <0.001 b |
| IV-V | 77 (37.7) | 27 (21.3) | 50 (64.9) | <0.001 b |
| Modified Fisher grade | ||||
| 1 | 25 (12.3) | 22 (17.3) | 3 (3.9) | 0.003 c |
| 2 | 8 (3.9) | 7 (5.5) | 1 (1.3) | 0.127 c |
| 3 | 99 (48.5) | 74 (58.3) | 25 (32.5) | <0.001 b |
| 4 | 72 (35.3) | 24 (18.9) | 48 (62.3) | <0.001 b |
| Acute hydrocephalus | 67 (32.8) | 25 (19.7) | 42 (54.5) | <0.001 b |
| Ruptured AN location | ||||
| ACA | 70 (34.3) | 48 (37.8) | 22 (28.6) | 0.179 b |
| ICA | 76 (37.3) | 45 (35.4) | 31 (40.3) | 0.489 b |
| MCA | 40 (19.6) | 23 (18.1) | 17 (22.1) | 0.489 b |
| VA-BA | 18 (8.8) | 11 (8.7) | 7 (9.1) | 0.917 b |
| Anterior circulation | 186 (91.2) | 116 (91.3) | 70 (90.9) | 0.917 b |
| Multiple Aneurysms | 56 (27.5) | 34 (26.8) | 22 (28.6) | 0.780 b |
| Treatment modality | ||||
| Clipping | 161 (78.9) | 96 (75.6) | 65 (84.4) | 0.134 b |
| Coiling | 43 (21.1) | 31 (24.4) | 12 (15.6) | 0.134 b |
| CSF drainage | 69 (33.8) | 35 (27.6) | 34 (44.2) | 0.015 b |
| Prophylactic drug for DCI | ||||
| Fasudil hydrochloride | 201 (98.5) | 126 (99.2) | 75 (97.4) | 0.319 c |
| Cilostazol | 166 (81.4) | 105 (82.7) | 61 (79.2) | 0.539 b |
| Ethyl icosapentate | 103 (50.5) | 68 (53.5) | 35 (45.5) | 0.263 b |
| Statin | 50 (24.5) | 35 (27.6) | 15 (19.5) | 0.193 b |
| Angiographic vasospasm | 62 (30.4) | 33 (26.0) | 29 (37.7) | 0.068 b |
| DCI | 29 (14.2) | 11 (8.7) | 18 (23.4) | 0.004 b |
| Delayed cerebral infarction | 45 (22.1) | 15 (11.8) | 30 (39.0) | <0.001 b |
| Variables | Odds Ratio | 95% CI | p Value |
|---|---|---|---|
| Age ≥ 75 years old | 3.31 | 1.38–7.93 | 0.007 |
| Delayed cerebral infarction | 12.64 | 4.48–35.68 | <0.001 |
| Fibulin-5 at days 4–6 ≥ 487.2 ng/mL | 2.55 | 1.10–5.88 | 0.029 |
| Pre-onset mRS 0 | 0.10 | 0.02–0.62 | 0.013 |
| Acute hydrocephalus | 4.84 | 2.03–11.54 | <0.001 |
| Modified Fisher grade 3 | 0.30 | 0.13–0.71 | 0.006 |
| Admission WFNS grades IV-V | 5.93 | 2.61–13.47 | <0.001 |
| Female | 0.887 | ||
| Past history of a cerebral infarction | 0.120 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, Y.; Oinaka, H.; Nakajima, H.; Nampei, M.; Kawakita, F.; Miura, Y.; Yasuda, R.; Toma, N.; Suzuki, H.; pSEED Group. Plasma Fibulin-5 Levels as an Independent Predictor of a Poor Outcome after an Aneurysmal Subarachnoid Hemorrhage. Int. J. Mol. Sci. 2022, 23, 15184. https://doi.org/10.3390/ijms232315184
Suzuki Y, Oinaka H, Nakajima H, Nampei M, Kawakita F, Miura Y, Yasuda R, Toma N, Suzuki H, pSEED Group. Plasma Fibulin-5 Levels as an Independent Predictor of a Poor Outcome after an Aneurysmal Subarachnoid Hemorrhage. International Journal of Molecular Sciences. 2022; 23(23):15184. https://doi.org/10.3390/ijms232315184
Chicago/Turabian StyleSuzuki, Yume, Hiroki Oinaka, Hideki Nakajima, Mai Nampei, Fumihiro Kawakita, Yoichi Miura, Ryuta Yasuda, Naoki Toma, Hidenori Suzuki, and pSEED Group. 2022. "Plasma Fibulin-5 Levels as an Independent Predictor of a Poor Outcome after an Aneurysmal Subarachnoid Hemorrhage" International Journal of Molecular Sciences 23, no. 23: 15184. https://doi.org/10.3390/ijms232315184