
Limited Accuracy of Pan-Trk Immunohistochemistry Screening for NTRK Rearrangements in Follicular-Derived Thyroid Carcinoma

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
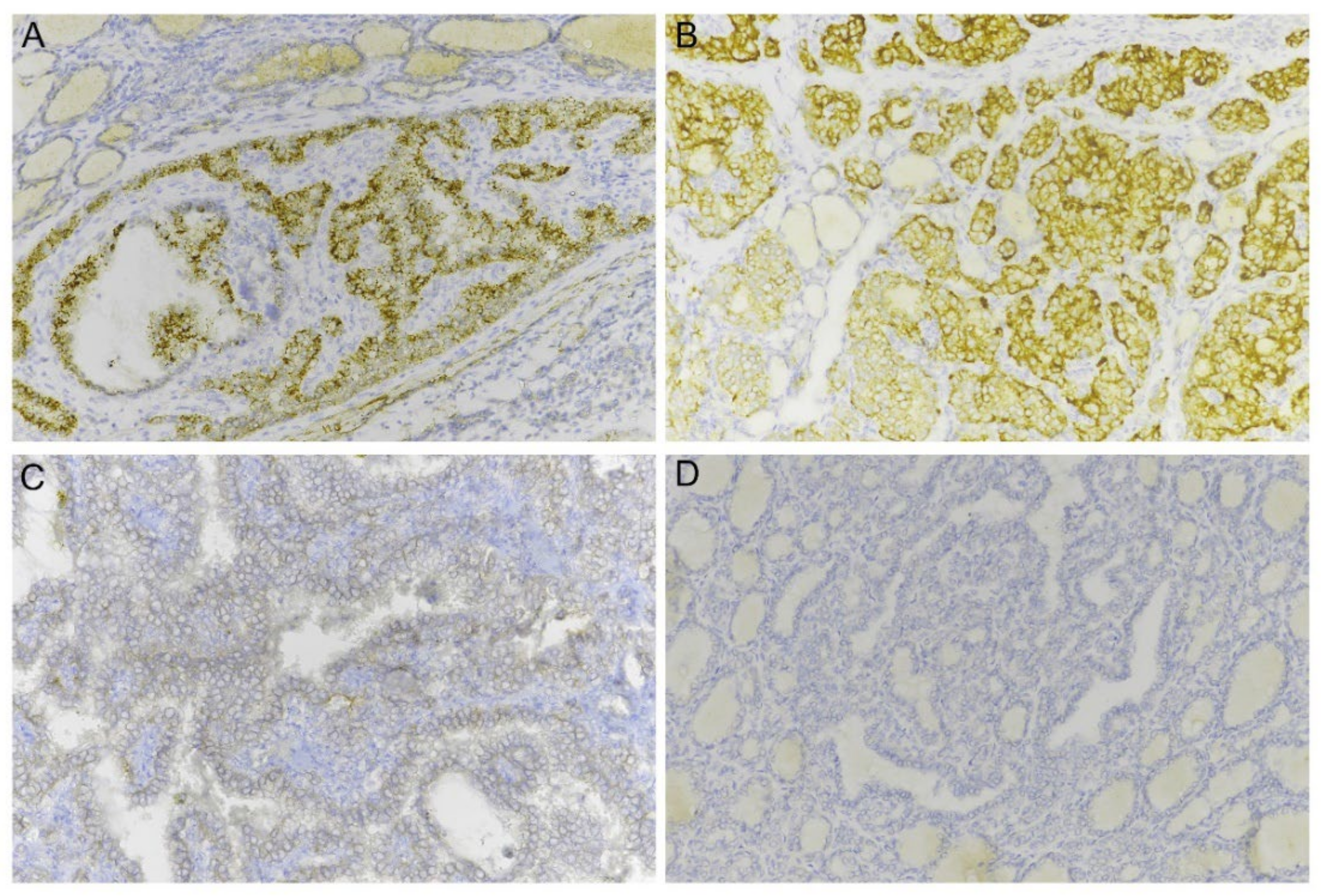
2.1. Pan-Trk Immunohistochemistry in Thyroid Cancer
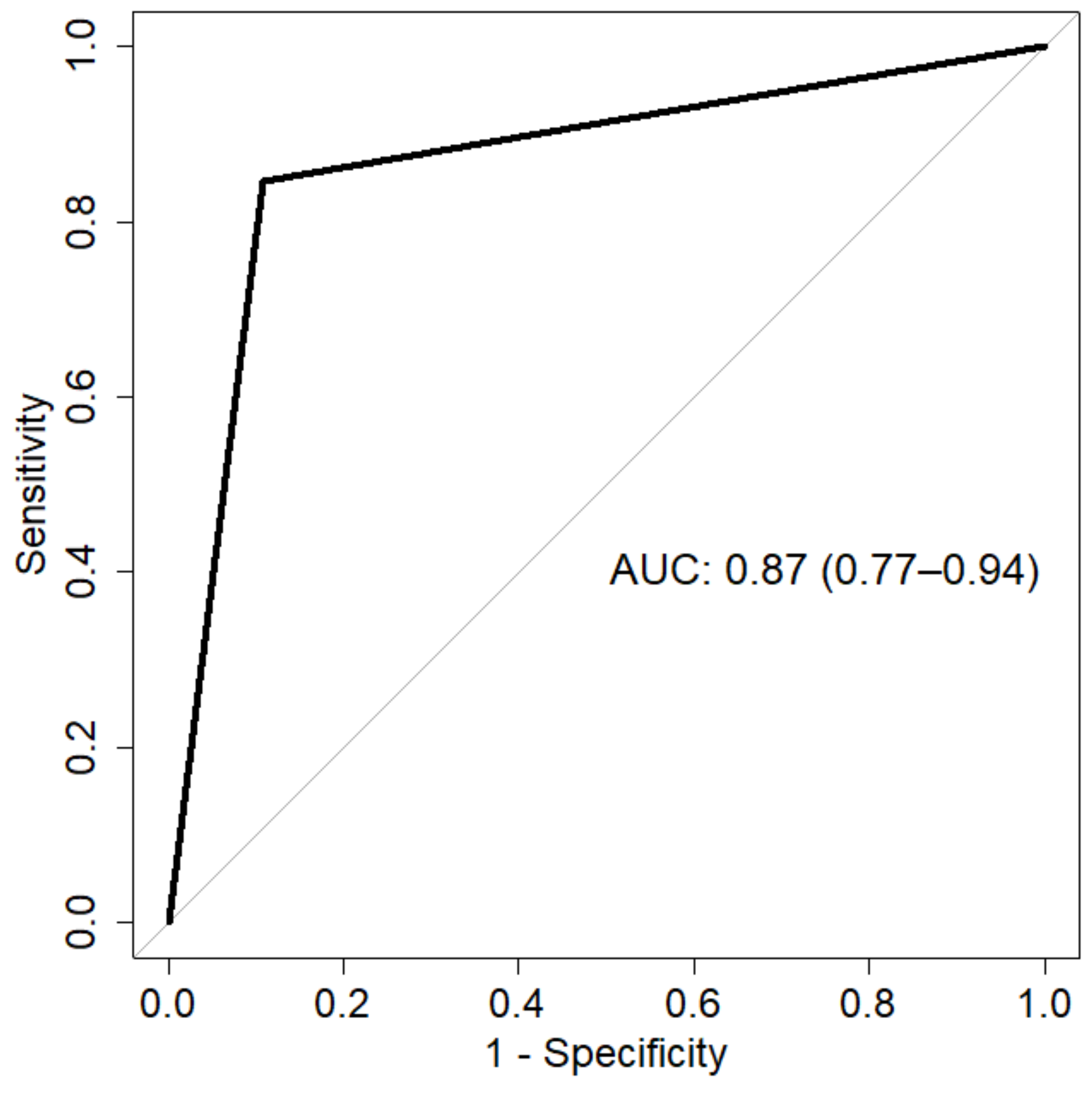
2.2. Pan-Trk Immunohistochemistry Test Performance
3. Discussion
4. Materials and Methods
4.1. Samples
4.2. IHC Analysis
4.3. Data Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Belli, C.; Penault-Llorca, F.; Ladanyi, M.; Normanno, N.; Scoazec, J.-Y.; Lacroix, L.; Reis-Filho, J.S.; Subbiah, V.; Gainor, J.F.; Endris, V.; et al. ESMO Recommendations on the Standard Methods to Detect RET Fusions and Mutations in Daily Practice and Clinical Research. Ann. Oncol. 2021, 32, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Integrated Genomic Characterization of Papillary Thyroid Carcinoma. Cell 2014, 159, 676–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastos, A.U.; de Jesus, A.C.; Cerutti, J.M. ETV6-NTRK3 and STRN-ALK Kinase Fusions Are Recurrent Events in Papillary Thyroid Cancer of Adult Population. Eur. J. Endocrinol. 2018, 178, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Van der Tuin, K.; Ventayol Garcia, M.; Corver, W.E.; Khalifa, M.N.; Ruano Neto, D.; Corssmit, E.P.M.; Hes, F.J.; Links, T.P.; Smit, J.W.A.; Plantinga, T.S.; et al. Targetable Gene Fusions Identified in Radioactive Iodine Refractory Advanced Thyroid Carcinoma. Eur. J. Endocrinol. 2019, 180, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Solomon, J.P.; Linkov, I.; Rosado, A.; Mullaney, K.; Rosen, E.Y.; Frosina, D.; Jungbluth, A.A.; Zehir, A.; Benayed, R.; Drilon, A.; et al. NTRK Fusion Detection across Multiple Assays and 33,997 Cases: Diagnostic Implications and Pitfalls. Mod. Pathol. 2020, 33, 38–46. [Google Scholar] [CrossRef]
- Pozdeyev, N.; Gay, L.M.; Sokol, E.S.; Hartmaier, R.; Deaver, K.E.; Davis, S.; French, J.D.; Borre, P.V.; LaBarbera, D.V.; Tan, A.-C.; et al. Genetic Analysis of 779 Advanced Differentiated and Anaplastic Thyroid Cancers. Clin. Cancer Res. 2018, 24, 3059–3068. [Google Scholar] [CrossRef] [Green Version]
- Duan, H.; Li, Y.; Hu, P.; Gao, J.; Ying, J.; Xu, W.; Zhao, D.; Wang, Z.; Ye, J.; Lizaso, A.; et al. Mutational Profiling of Poorly Differentiated and Anaplastic Thyroid Carcinoma by the Use of Targeted Next-generation Sequencing. Histopathology 2019, 75, 890–899. [Google Scholar] [CrossRef]
- Xu, B.; Fuchs, T.; Dogan, S.; Landa, I.; Katabi, N.; Fagin, J.A.; Tuttle, R.M.; Sherman, E.; Gill, A.J.; Ghossein, R. Dissecting Anaplastic Thyroid Carcinoma: A Comprehensive Clinical, Histologic, Immunophenotypic, and Molecular Study of 360 Cases. Thyroid 2020, 30, 1505–1517. [Google Scholar] [CrossRef]
- Cordioli, M.I.C.V.; Moraes, L.; Bastos, A.U.; Besson, P.; de Seixas Alves, M.T.; Delcelo, R.; Monte, O.; Longui, C.; Cury, A.N.; Cerutti, J.M. Fusion Oncogenes Are the Main Genetic Events Found in Sporadic Papillary Thyroid Carcinomas from Children. Thyroid 2017, 27, 182–188. [Google Scholar] [CrossRef]
- Pekova, B.; Sykorova, V.; Dvorakova, S.; Vaclavikova, E.; Moravcova, J.; Katra, R.; Astl, J.; Vlcek, P.; Kodetova, D.; Vcelak, J.; et al. RET, NTRK, ALK, BRAF, and MET Fusions in a Large Cohort of Pediatric Papillary Thyroid Carcinomas. Thyroid 2020, 30, 1771–1780. [Google Scholar] [CrossRef]
- Alzahrani, A.S.; Alswailem, M.; Alswailem, A.A.; Al-Hindi, H.; Goljan, E.; Alsudairy, N.; Abouelhoda, M. Genetic Alterations in Pediatric Thyroid Cancer Using a Comprehensive Childhood Cancer Gene Panel. J. Clin. Endocrinol. Metab. 2020, 105, 3324–3334. [Google Scholar] [CrossRef] [PubMed]
- Macerola, E.; Proietti, A.; Poma, A.M.; Ugolini, C.; Torregrossa, L.; Vignali, P.; Basolo, A.; Materazzi, G.; Elisei, R.; Santini, F.; et al. Molecular Alterations in Relation to Histopathological Characteristics in a Large Series of Pediatric Papillary Thyroid Carcinoma from a Single Institution. Cancers 2021, 13, 3123. [Google Scholar] [CrossRef] [PubMed]
- Marchiò, C.; Scaltriti, M.; Ladanyi, M.; Iafrate, A.J.; Bibeau, F.; Dietel, M.; Hechtman, J.F.; Troiani, T.; López-Rios, F.; Douillard, J.-Y.; et al. ESMO Recommendations on the Standard Methods to Detect NTRK Fusions in Daily Practice and Clinical Research. Ann. Oncol. 2019, 30, 1417–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zito Marino, F.; Pagliuca, F.; Ronchi, A.; Cozzolino, I.; Montella, M.; Berretta, M.; Errico, M.E.; Donofrio, V.; Bianco, R.; Franco, R. NTRK Fusions, from the Diagnostic Algorithm to Innovative Treatment in the Era of Precision Medicine. Int. J. Mol. Sci 2021, 21, 3718. [Google Scholar] [CrossRef] [PubMed]
- Perreault, S.; Chami, R.; Deyell, R.J.; El Demellawy, D.; Ellezam, B.; Jabado, N.; Morgenstern, D.A.; Narendran, A.; Sorensen, P.H.B.; Wasserman, J.D.; et al. Canadian Consensus for Biomarker Testing and Treatment of TRK Fusion Cancer in Pediatric Patients. Curr. Oncol. 2021, 28, 346–366. [Google Scholar] [CrossRef] [PubMed]
- Bruno, R.; Fontanini, G. Next Generation Sequencing for Gene Fusion Analysis in Lung Cancer: A Literature Review. Diagnostics 2020, 10, 521. [Google Scholar] [CrossRef]
- Hsiao, S.J.; Zehir, A.; Sireci, A.N.; Aisner, D.L. Detection of Tumor NTRK Gene Fusions to Identify Patients Who May Benefit from Tyrosine Kinase (TRK) Inhibitor Therapy. J. Mol. Diag. 2019, 21, 553–571. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-C.; Chen, J.-Y.; Huang, C.-J.; Chen, H.-S.; Yang, A.-H.; Hang, J.-F. Detection of NTRK1/3 Rearrangements in Papillary Thyroid Carcinoma Using Immunohistochemistry, Fluorescent In Situ Hybridization, and Next-Generation Sequencing. Endocr. Pathol. 2020, 31, 348–358. [Google Scholar] [CrossRef]
- Penault-Llorca, F.; Rudzinski, E.R.; Sepulveda, A.R. Testing Algorithm for Identification of Patients with TRK Fusion Cancer. J. Clin. Pathol. 2019, 72, 460–467. [Google Scholar] [CrossRef]
- Kim, S.-W.; Roh, J.; Park, C.-S. Immunohistochemistry for Pathologists: Protocols, Pitfalls, and Tips. J. Pathol. Transl. Med. 2016, 50, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Macerola, E.; Poma, A.M.; Vignali, P.; Basolo, A.; Ugolini, C.; Torregrossa, L.; Santini, F.; Basolo, F. Molecular Genetics of Follicular-Derived Thyroid Cancer. Cancers 2021, 13, 1139. [Google Scholar] [CrossRef] [PubMed]
- Hechtman, J.F.; Benayed, R.; Hyman, D.M.; Drilon, A.; Zehir, A.; Frosina, D.; Arcila, M.E.; Dogan, S.; Klimstra, D.S.; Ladanyi, M.; et al. Pan-Trk Immunohistochemistry Is an Efficient and Reliable Screen for the Detection of NTRK Fusions. Am. J. Surg. Pathol. 2017, 41, 1547–1551. [Google Scholar] [CrossRef] [PubMed]
- Gatalica, Z.; Xiu, J.; Swensen, J.; Vranic, S. Molecular Characterization of Cancers with NTRK Gene Fusions. Mod. Pathol. 2019, 32, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Nozaki, Y.; Yamamoto, H.; Iwasaki, T.; Sato, M.; Jiromaru, R.; Hongo, T.; Yasumatsu, R.; Oda, Y. Clinicopathological Features and Immunohistochemical Utility of NTRK-, ALK-, and ROS1-Rearranged Papillary Thyroid Carcinomas and Anaplastic Thyroid Carcinomas. Hum. Pathol. 2020, 106, 82–92. [Google Scholar] [CrossRef]
- Murphy, D.A.; Ely, H.A.; Shoemaker, R.; Boomer, A.; Culver, B.P.; Hoskins, I.; Haimes, J.D.; Walters, R.D.; Fernandez, D.; Stahl, J.A.; et al. Detecting Gene Rearrangements in Patient Populations Through a 2-Step Diagnostic Test Comprised of Rapid IHC Enrichment Followed by Sensitive Next-Generation Sequencing. Appl. Immunohistochem. Mol. Morphol. 2017, 25, 513–523. [Google Scholar] [CrossRef] [Green Version]
- Rudzinski, E.R.; Lockwood, C.M.; Stohr, B.A.; Vargas, S.O.; Sheridan, R.; Black, J.O.; Rajaram, V.; Laetsch, T.W.; Davis, J.L. Pan-Trk Immunohistochemistry Identifies NTRK Rearrangements in Pediatric Mesenchymal Tumors. Am. J. Surg. Pathol. 2018, 42, 927–935. [Google Scholar] [CrossRef]
- Harrison, B.T.; Fowler, E.; Krings, G.; Chen, Y.-Y.; Bean, G.R.; Vincent-Salomon, A.; Fuhrmann, L.; Barnick, S.E.; Chen, B.; Hosfield, E.M.; et al. Pan-TRK Immunohistochemistry: A Useful Diagnostic Adjunct For Secretory Carcinoma of the Breast. Am. J. Surg. Pathol. 2019, 43, 1693–1700. [Google Scholar] [CrossRef]
- Bell, D.; Ferrarotto, R.; Liang, L.; Goepfert, R.P.; Li, J.; Ning, J.; Broaddus, R.; Weber, R.S.; El-Naggar, A.K. Pan-Trk immunohistochemistry reliably identifies ETV6-NTRK3 fusion in secretory carcinoma of the salivary gland. Virchows Arch. 2020, 476, 295–305. [Google Scholar] [CrossRef]
- Strohmeier, S.; Brcic, I.; Popper, H.; Liegl-Atzwanger, B.; Lindenmann, J.; Brcic, L. Applicability of Pan-TRK Immunohistochemistry for Identification of NTRK Fusions in Lung Carcinoma. Sci. Rep. 2021, 11, 9785. [Google Scholar] [CrossRef]
- Koopman, B.; Kuijpers, C.; Groen, H.; Timens, W.; Schuuring, E.; Willems, S.M.; van Kempen, L.C. Detection of NTRK Fusions and TRK Expression and Performance of pan-TRK Immunohistochemistry in Routine Diagnostics: Results from a Nationwide Community-Based Cohort. Diagnostics 2022, 12, 668. [Google Scholar] [CrossRef]
- Fedchenko, N.; Reifenrath, J. Different Approaches for Interpretation and Reporting of Immunohistochemistry Analysis Results in the Bone Tissue—A Review. Diagn. Pathol. 2014, 9, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Sample Name | Driver Gene | Fusion Partner | Positive Cells (%) | Localization of Positive Signal | Signal Intensity | Tumor Histotype |
|---|---|---|---|---|---|---|
| P1 | NTRK1 | unknown | 50 | Cytoplasmic (granular) | 2+ | PTC—diffuse sclerosing variant |
| P2 | NTRK1 | unknown | 50 | Cell membrane | 2+ | PTC—classical type |
| P3 | NTRK1 | unknown | 80 | Cytoplasmic (granular) | 3+ | PTC—classical type |
| P4 | NTRK1 | unknown | 60 | Cell membrane | 2+ | PTC—classical type |
| P5 | NTRK1 | unknown | 70 | Cytoplasmic (granular) | 2+ | PTC—classical type |
| P6 | NTRK1 | TPM3 | 70 | Cytoplasmic (granular) | 3+ | PDTC |
| P7 | NTRK3 | ETV6 | 40 | Cytoplasmic (granular) | 2+ | PTC—follicular variant |
| P8 | NTRK3 | unknown | 80 | Cytoplasmic (granular) | 2+ | PTC—classical type |
| P11 | NTRK3 | unknown | 60 | Cell membrane | 3+ | PTC—follicular variant |
| P12 | NTRK3 | unknown | 30 | Cytoplasmic (granular) | 3+ | PTC—classical type |
| P13 | NTRK3 | unknown | 70 | Cytoplasmic | 3+ | PTC—classical type |
| P14 | NTRK3 | ETV6 | 20 | Cytoplasmic (granular) | 1+ | PTC–solid variant |
| P15 | NTRK3 | ETV6 | 10 | Cell membrane | 2+ | PTC—classical type |
| P17 | NTRK3 | ETV6 | 30 | Cytoplasmic (granular) | 3+ | PTC—classical type |
| P18 | NTRK3 | unknown | 30 | Cytoplasmic (granular) | 3+ | PTC—classical type |
| P19 | NTRK3 | ETV6 | 40 | Cytoplasmic (granular) | 3+ | PTC—classical type |
| P20 | NTRK3 | ETV6 | 30 | Cytoplasmic (granular) | 2+ | PTC—classical type |
| P21 | NTRK3 | unknown | 70 | Cytoplasmic (granular) | 3+ | PTC—classical type |
| P22 | NTRK3 | SQSTM1 | 20 | Cytoplasmic (granular) | 3+ | PTC—classical type |
| P24 | NTRK3 | ETV6 | 20 | Cytoplasmic (granular) | 2+ | PTC—classical type |
| P25 | NTRK3 | ETV6 | 30 | Cytoplasmic (granular) | 3+ | PTC—classical type |
| P26 | NTRK3 | ETV6 | 80 | Cytoplasmic (granular) | 3+ | ATC |
| N20 | RET fusion | / | 10 | Cell membrane | 1+ | PTC—classical type |
| N24 | HRAS p.Q61K | / | 15 | Cytoplasmic (granular) | 1+ | PTC—follicular variant |
| N28 | NRAS p.Q61R | / | 70 | Cytoplasmic (granular) | 2+ | PTC—metastasis |
| Sample Name | NTRK Gene | NTRK Status Assessed by | Fusion Partner | Non-NTRK Driver Alteration | Histology |
|---|---|---|---|---|---|
| P1 | NTRK1 | FISH | unknown | / | PTC—diffuse sclerosing variant |
| P2 | NTRK1 | RT-PCR | unknown | / | PTC—classical type |
| P3 | NTRK1 | FISH | unknown | / | PTC—classical type |
| P4 | NTRK1 | RT-PCR | unknown | / | PTC—classical type |
| P5 | NTRK1 | FISH | unknown | / | PTC—classical type |
| P6 | NTRK1 | NGS | TPM3 | / | PDTC |
| P7 | NTRK3 | RT-PCR | ETV6 | / | PTC—follicular variant |
| P8 | NTRK3 | FISH | unknown | / | PTC—classical type |
| P9 | NTRK3 | RT-PCR | ETV6 | / | PTC—classical type |
| P10 | NTRK3 | RT-PCR | ETV6 | / | PTC—follicular variant |
| P11 | NTRK3 | FISH | unknown | / | PTC—follicular variant |
| P12 | NTRK3 | FISH | unknown | / | PTC—classical type |
| P13 | NTRK3 | FISH | unknown | / | PTC—classical type |
| P14 | NTRK3 | RT-PCR | ETV6 | / | PTC—solid variant |
| P15 | NTRK3 | RT-PCR | ETV6 | / | PTC—classical type |
| P16 | NTRK3 | RT-PCR | ETV6 | / | PTC—classical type |
| P17 | NTRK3 | RT-PCR | ETV6 | / | PTC—classical type |
| P18 | NTRK3 | FISH | unknown | / | PTC—classical type |
| P19 | NTRK3 | RT-PCR | ETV6 | / | PTC—classical type |
| P20 | NTRK3 | RT-PCR | ETV6 | / | PTC—classical type |
| P21 | NTRK3 | FISH | unknown | / | PTC—classical type |
| P22 | NTRK3 | NGS | SQSTM1 | / | PTC—classical type |
| P23 | NTRK3 | NGS | ETV6 | / | PTC—classical type |
| P24 | NTRK3 | NGS | ETV6 | / | PTC—classical type |
| P25 | NTRK3 | NGS | ETV6 | / | PTC—classical type |
| P26 | NTRK3 | RT-PCR | ETV6 | / | ATC |
| N1 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N2 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N3 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N4 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N5 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N6 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N7 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N8 | / | FISH | / | NRAS p.Q61R | PTC—follicular variant |
| N9 | / | FISH | / | RET fusion | PTC—solid variant |
| N10 | / | FISH | / | RET fusion | PTC—classical type |
| N11 | / | FISH | / | PPARG fusion | PTC—follicular variant |
| N12 | / | FISH | / | NRAS p.Q61K | PTC—follicular variant |
| N13 | / | FISH | / | RET fusion | PTC—classical type |
| N14 | / | FISH | / | ALK fusion | PTC—follicular variant |
| N15 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N16 | / | FISH | / | RET fusion | PTC—classical type |
| N17 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N18 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N19 | / | FISH | / | ALK fusion | PTC—follicular variant |
| N20 | / | NGS | / | RET fusion | PTC—classical type |
| N21 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N22 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N23 | / | FISH | / | BRAF p.V600E | PTC—classical type |
| N24 | / | FISH | / | HRAS p.Q61K | PTC—follicular variant |
| N25 | / | FISH | / | BRAF p.V600E | PDTC |
| N26 | / | RT-PCR | / | BRAF p.V600E | PTC—lymph node recurrence |
| N27 | / | RT-PCR | / | BRAF p.V600E | PTC—local recurrence |
| N28 | / | RT-PCR | / | NRAS p. Q61R | PTC—local recurrence |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macerola, E.; Proietti, A.; Poma, A.M.; Vignali, P.; Sparavelli, R.; Ginori, A.; Basolo, A.; Elisei, R.; Santini, F.; Basolo, F. Limited Accuracy of Pan-Trk Immunohistochemistry Screening for NTRK Rearrangements in Follicular-Derived Thyroid Carcinoma. Int. J. Mol. Sci. 2022, 23, 7470. https://doi.org/10.3390/ijms23137470
Macerola E, Proietti A, Poma AM, Vignali P, Sparavelli R, Ginori A, Basolo A, Elisei R, Santini F, Basolo F. Limited Accuracy of Pan-Trk Immunohistochemistry Screening for NTRK Rearrangements in Follicular-Derived Thyroid Carcinoma. International Journal of Molecular Sciences. 2022; 23(13):7470. https://doi.org/10.3390/ijms23137470
Chicago/Turabian StyleMacerola, Elisabetta, Agnese Proietti, Anello Marcello Poma, Paola Vignali, Rebecca Sparavelli, Alessandro Ginori, Alessio Basolo, Rossella Elisei, Ferruccio Santini, and Fulvio Basolo. 2022. "Limited Accuracy of Pan-Trk Immunohistochemistry Screening for NTRK Rearrangements in Follicular-Derived Thyroid Carcinoma" International Journal of Molecular Sciences 23, no. 13: 7470. https://doi.org/10.3390/ijms23137470