
Head-to-Head Comparison of Fibroblast Activation Protein Inhibitors (FAPI) Radiotracers versus [18F]F-FDG in Oncology: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Results
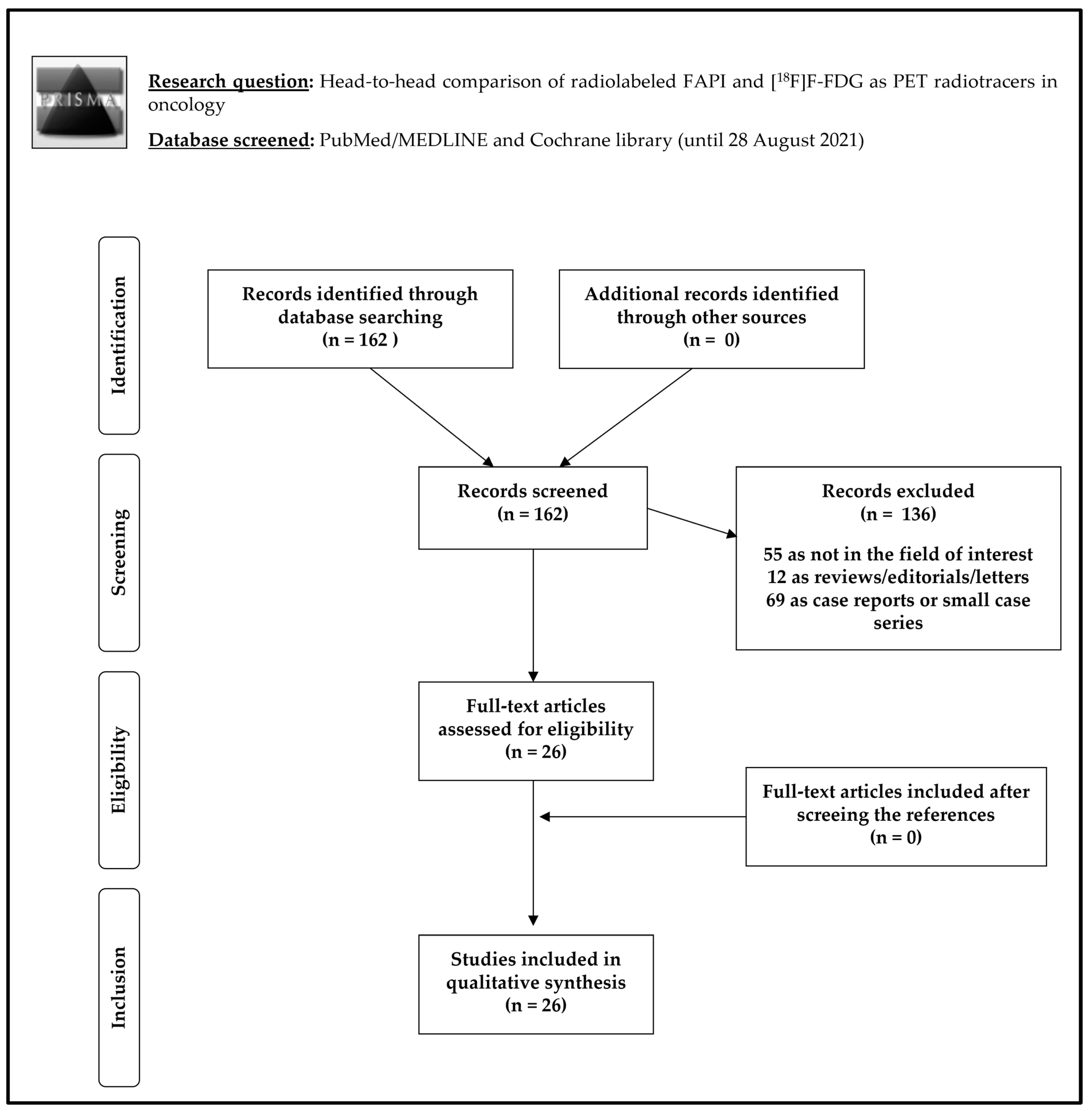
2.1. Literature Search
2.2. Qualitative Synthesis (Systematic Review)
2.2.1. Basic Study and Patient Characteristics
2.2.2. Technical Aspects
2.2.3. Radiotracer Biodistribution and Main Outcome Measures
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.2. Study Selection
4.3. Data Extraction
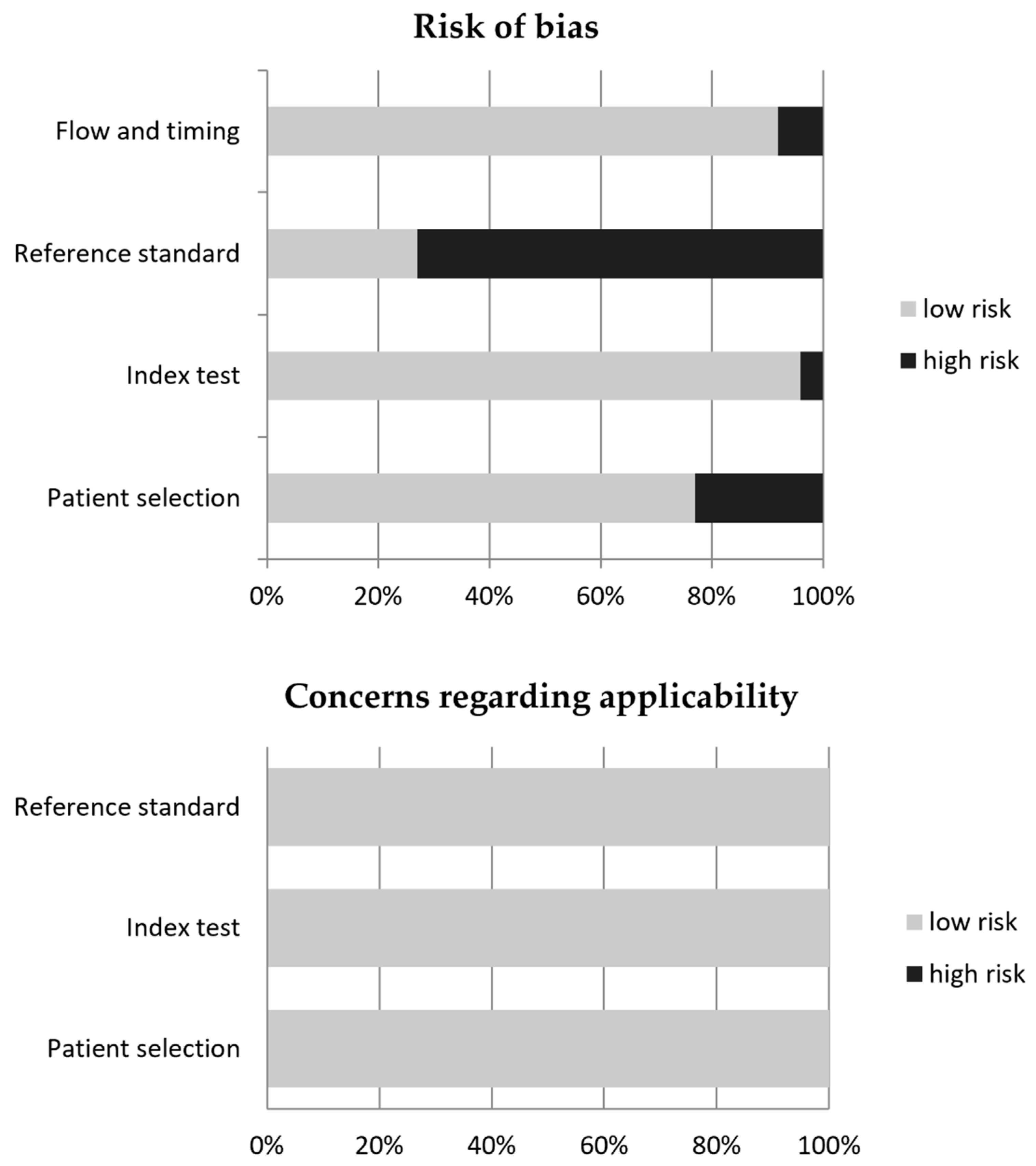
4.4. Quality Assessment
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vaz, S.C.; Oliveira, F.; Herrmann, K.; Veit-Haibach, P. Nuclear medicine and molecular imaging advances in the 21st century. Br. J. Radiol. 2020, 93, 20200095. [Google Scholar] [CrossRef] [PubMed]
- Treglia, G.; Sadeghi, R.; Del Sole, A.; Giovanella, L. Diagnostic performance of PET/CT with tracers other than F-18-FDG in oncology: An evidence-based review. Clin. Transl. Oncol. 2014, 16, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, A.H.; Glaudemans, A.W.; De Vries, E.F. PET beyond ¹⁸F-FDG: Second generation PET tracers in clinical oncology. Q. J. Nucl. Med. Mol. Imaging 2015, 59, 1–3. [Google Scholar]
- De Ruysscher, D.; Haustermans, K.; Thorwarth, D. FDG and Beyond. Recent Results Cancer Res. 2016, 198, 163–173. [Google Scholar] [CrossRef]
- Lindner, T.; Loktev, A.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Jäger, D.; Mier, W.; Haberkorn, U. Development of Quinoline-Based Theranostic Ligands for the Targeting of Fibroblast Activation Protein. J. Nucl. Med. 2018, 59, 1415–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loktev, A.; Lindner, T.; Mier, W.; Debus, J.; Altmann, A.; Jäger, D.; Giesel, F.; Kratochwil, C.; Barthe, P.; Roumestand, C.; et al. A Tumor-Imaging Method Targeting Cancer-Associated Fibroblasts. J. Nucl. Med. 2018, 59, 1423–1429. [Google Scholar] [CrossRef]
- Hamson, E.J.; Keane, F.M.; Tholen, S.; Schilling, O.; Gorrell, M.D. Understanding fibroblast activation protein (FAP): Substrates, activities, expression and targeting for cancer therapy. Proteom. Clin. Appl. 2014, 8, 454–463. [Google Scholar] [CrossRef]
- Windisch, P.; Zwahlen, D.R.; Giesel, F.L.; Scholz, E.; Lugenbiel, P.; Debus, J.; Haberkorn, U.; Adeberg, S. Clinical results of fibroblast activation protein (FAP) specific PET for non-malignant indications: Systematic review. EJNMMI Res. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Dendl, K.; Schlittenhardt, J.; Staudinger, F.; Kratochwil, C.; Altmann, A.; Haberkorn, U.; Giesel, F.L. The Role of Fibroblast Activation Protein Ligands in Oncologic PET Imaging. PET Clin. 2021, 16, 341–351. [Google Scholar] [CrossRef]
- Ballal, S.; Yadav, M.P.; Moon, E.S.; Kramer, V.S.; Roesch, F.; Kumari, S.; Tripathi, M.; ArunRaj, S.T.; Sarswat, S.; Bal, C. Biodistribution, pharmacokinetics, dosimetry of [68Ga]Ga-DOTA.SA.FAPi, and the head-to-head comparison with [18F]F-FDG PET/CT in patients with various cancers. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1915–1931. [Google Scholar] [CrossRef]
- Chen, H.; Pang, Y.; Wu, J.; Zhao, L.; Hao, B.; Wu, J.; Wei, J.; Wu, S.; Zhao, L.; Luo, Z.; et al. Comparison of [68Ga]Ga-DOTA-FAPI-04 and [18F] FDG PET/CT for the diagnosis of primary and metastatic lesions in patients with various types of cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1820–1832. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhao, L.; Ruan, D.; Pang, Y.; Hao, B.; Dai, Y.; Wu, X.; Guo, W.; Fan, C.; Wu, J.; et al. Usefulness of [68Ga]Ga-DOTA-FAPI-04 PET/CT in patients presenting with inconclusive [18F]FDG PET/CT findings. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Dendl, K.; Koerber, S.A.; Finck, R.; Mokoala, K.M.G.; Staudinger, F.; Schillings, L.; Heger, U.; Röhrich, M.; Kratochwil, C.; Sathekge, M.; et al. 68Ga-FAPI-PET/CT in patients with various gynecological malignancies. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4089–4100. [Google Scholar] [CrossRef] [PubMed]
- Elboga, U.; Sahin, E.; Kus, T.; Cayirli, Y.B.; Aktas, G.; Uzun, E.; Cinkir, H.Y.; Teker, F.; Sever, O.N.; Aytekin, A.; et al. Superiority of 68Ga-FAPI PET/CT scan in detecting additional lesions compared to 18FDG PET/CT scan in breast cancer. Ann. Nucl. Med. 2021, 1–11. [Google Scholar] [CrossRef]
- Giesel, F.L.; Kratochwil, C.; Schlittenhardt, J.; Dendl, K.; Eiber, M.; Staudinger, F.; Kessler, L.; Fendler, W.P.; Lindner, T.; Koerber, S.A.; et al. Head-to-head intra-individual comparison of biodistribution and tumor uptake of 68Ga-FAPI and 18F-FDG PET/CT in cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2021, 1–9. [Google Scholar] [CrossRef]
- Guo, W.; Pang, Y.; Yao, L.; Zhao, L.; Fan, C.; Ke, J.; Guo, P.; Hao, B.; Fu, H.; Xie, C.; et al. Imaging fibroblast activation protein in liver cancer: A single-center post hoc retrospective analysis to compare [68Ga]Ga-FAPI-04 PET/CT versus MRI and [18F]-FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1604–1617. [Google Scholar] [CrossRef]
- Jiang, D.; Chen, X.; You, Z.; Wang, H.; Zhang, X.; Li, X.; Ren, S.; Huang, Q.; Hua, F.; Guan, Y.; et al. Comparison of [68Ga]Ga-FAPI-04 and [18F]-FDG for the detection of primary and metastatic lesions in patients with gastric cancer: A bicentric retrospective study. Eur. J. Nucl. Med. Mol. Imaging 2021. [Google Scholar] [CrossRef]
- Kessler, L.; Ferdinandus, J.; Hirmas, N.; Bauer, S.; Dirksen, U.; Zarrad, F.; Nader, M.; Chodyla, M.-K.; Milosevic, A.; Umutlu, L.; et al. Ga-68-FAPI as diagnostic tool in sarcoma: Data from the FAPI-PET prospective observational trial. J. Nucl. Med. 2021. [Google Scholar] [CrossRef]
- Kömek, H.; Can, C.; Güzel, Y.; Oruç, Z.; Gündoğan, C.; Yildirim, Ö.A.; Kaplan, I.; Erdur, E.; Yıldırım, M.S.; Çakabay, B. 68Ga-FAPI-04 PET/CT, a new step in breast cancer imaging: A comparative pilot study with the 18F-FDG PET/CT. Ann. Nucl. Med. 2021, 35, 744–752. [Google Scholar] [CrossRef]
- Kreppel, B.; Gonzalez-Carmona, M.A.; Feldmann, G.; Küppers, J.; Moon, E.S.; Marinova, M.; Bundschuh, R.A.; Kristiansen, G.; Essler, M.; Roesch, F.; et al. Fibroblast activation protein inhibitor (FAPi) positive tumour fraction on PET/CT correlates with Ki-67 in liver metastases of neuroendocrine tumours. Nuklearmedizin 2021, 60, 344–354. [Google Scholar] [CrossRef]
- Kuten, J.; Levine, C.; Shamni, O.; Pelles, S.; Wolf, I.; Lahat, G.; Mishani, E.; Even-Sapir, E. Head-to-head comparison of [68Ga]Ga-FAPI-04 and [18F]-FDG PET/CT in evaluating the extent of disease in gastric adenocarcinoma. Eur. J. Nucl. Med. Mol. Imaging 2021. [Google Scholar] [CrossRef]
- Lan, L.; Liu, H.; Wang, Y.; Deng, J.; Peng, D.; Feng, Y.; Wang, L.; Chen, Y.; Qiu, L. The potential utility of [68Ga]Ga-DOTA-FAPI-04 as a novel broad-spectrum oncological and non-oncological imaging agent—Comparison with [18F]FDG. Eur. J. Nucl. Med. Mol. Imaging 2021, 1–17. [Google Scholar] [CrossRef]
- Linz, C.; Brands, R.C.; Kertels, O.; Dierks, A.; Brumberg, J.; Gerhard-Hartmann, E.; Hartmann, S.; Schirbel, A.; Serfling, S.; Zhi, Y.; et al. Targeting fibroblast activation protein in newly diagnosed squamous cell carcinoma of the oral cavity—Initial experience and comparison to [18F]FDG PET/CT and MRI. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3951–3960. [Google Scholar] [CrossRef]
- Pang, Y.; Zhao, L.; Luo, Z.; Hao, B.; Wu, H.; Lin, Q.; Sun, L.; Chen, H. Comparison of 68Ga-FAPI and 18F-FDG Uptake in Gastric, Duodenal, and Colorectal Cancers. Radiology 2021, 298, 393–402. [Google Scholar] [CrossRef]
- Qin, C.; Shao, F.; Gai, Y.; Liu, Q.; Ruan, W.; Liu, F.; Hu, F.; Lan, X. 68Ga-DOTA-FAPI-04 PET/MR in the evaluation of gastric carcinomas: Comparison with 18F-FDG PET/CT. J. Nucl. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Liu, F.; Huang, J.; Ruan, W.; Liu, Q.; Gai, Y.; Hu, F.; Jiang, D.; Hu, Y.; Yang, K.; et al. A head-to-head comparison of 68Ga-DOTA-FAPI-04 and 18F-FDG PET/MR in patients with nasopharyngeal carcinoma: A prospective study. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3228–3237. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Song, Y.; Liu, X.; Gai, Y.; Liu, Q.; Ruan, W.; Liu, F.; Hu, F.; Lan, X. Increased uptake of 68Ga-DOTA-FAPI-04 in bones and joints: Metastases and beyond. Eur. J. Nucl. Med. Mol. Imaging 2021, 1–12. [Google Scholar] [CrossRef]
- Şahin, E.; Elboğa, U.; Çelen, Y.Z.; Sever, Ö.N.; Çayırlı, Y.B.; Çimen, U. Comparison of 68Ga-DOTA-FAPI and 18FDG PET/CT imaging modalities in the detection of liver metastases in patients with gastrointestinal system cancer. Eur. J. Radiol. 2021, 142, 109867. [Google Scholar] [CrossRef] [PubMed]
- Serfling, S.; Zhi, Y.; Schirbel, A.; Lindner, T.; Meyer, T.; Gerhard-Hartmann, E.; Lapa, C.; Hagen, R.; Hackenberg, S.; Buck, A.K.; et al. Improved cancer detection in Waldeyer’s tonsillar ring by 68Ga-FAPI PET/CT imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1178–1187. [Google Scholar] [CrossRef]
- Shi, X.; Xing, H.; Yang, X.; Li, F.; Yao, S.; Congwei, J.; Zhao, H.; Hacker, M.; Huo, L.; Li, X. Comparison of PET imaging of activated fibroblasts and 18F-FDG for diagnosis of primary hepatic tumours: A prospective pilot study. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1593–1603. [Google Scholar] [CrossRef]
- Wang, S.; Zhou, X.; Xu, X.; Ding, J.; Liu, S.; Hou, X.; Li, N.; Zhu, H.; Yang, Z. Clinical translational evaluation of Al18F-NOTA-FAPI for fibroblast activation protein-targeted tumour imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 1–13. [Google Scholar] [CrossRef]
- Wang, H.; Zhu, W.; Ren, S.; Kong, Y.; Huang, Q.; Zhao, J.; Guan, Y.; Jia, H.; Chen, J.; Lu, L.; et al. 68Ga-FAPI-04 Versus 18F-FDG PET/CT in the Detection of Hepatocellular Carcinoma. Front. Oncol. 2021, 11, 693640. [Google Scholar] [CrossRef]
- Zhao, L.; Chen, S.; Chen, S.; Pang, Y.; Dai, Y.; Hu, S.; Lin, L.; Fu, L.; Sun, L.; Wu, H.; et al. 68Ga-fibroblast activation protein inhibitor PET/CT on gross tumour volume delineation for radiotherapy planning of oesophageal cancer. Radiother. Oncol. 2021, 158, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Pang, Y.; Luo, Z.; Fu, K.; Yang, T.; Zhao, L.; Sun, L.; Wu, H.; Lin, Q.; Chen, H. Role of [68Ga]Ga-DOTA-FAPI-04 PET/CT in the evaluation of peritoneal carcinomatosis and comparison with [18F]-FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1944–1955. [Google Scholar] [CrossRef]
- Zhao, L.; Pang, Y.; Zheng, H.; Han, C.; Gu, J.; Sun, L.; Wu, H.; Wu, S.; Lin, Q.; Chen, H. Clinical utility of [68Ga]Ga-labeled fibroblast activation protein inhibitor (FAPI) positron emission tomography/computed tomography for primary staging and recurrence detection in nasopharyngeal carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3606–3617. [Google Scholar] [CrossRef] [PubMed]
- Windisch, P.; Zwahlen, D.R.; Koerber, S.A.; Giesel, F.L.; Debus, J.; Haberkorn, U.; Adeberg, S. Clinical Results of Fibroblast Activation Protein (FAP) Specific PET and Implications for Radiotherapy Planning: Systematic Review. Cancers 2020, 12, 2629. [Google Scholar] [CrossRef]
- Sollini, M.; Kirienko, M.; Gelardi, F.; Fiz, F.; Gozzi, N.; Chiti, A. State-of-the-art of FAPI-PET imaging: A systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 1–19. [Google Scholar] [CrossRef]
- Lindner, T.; Altmann, A.; Giesel, F.; Kratochwil, C.; Kleist, C.; Krämer, S.; Mier, W.; Cardinale, J.; Kauczor, H.-U.; Jäger, D.; et al. 18F-labeled tracers targeting fibroblast activation protein. EJNMMI Radiopharm. Chem. 2021, 6, 1–13. [Google Scholar] [CrossRef]
- Hicks, R.J.; Roselt, P.J.; Kallur, K.G.; Tothill, R.W.; Mileshkin, L. FAPI PET/CT: Will It End the Hegemony of 18F-FDG in Oncology? J. Nucl. Med. 2021, 62, 296–302. [Google Scholar] [CrossRef]
- Guglielmo, P.; Guerra, L. Radiolabeled fibroblast activation protein inhibitor (FAPI) PET in oncology: Has the time come for 18F-fluorodeoxyglucose to think to a well-deserved retirement? Clin. Transl. Imaging 2021, 9, 1–2. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, R.; Treglia, G. Systematic reviews and meta-analyses of diagnostic studies: A practical guideline. Clin. Transl. Imaging 2017, 5, 83–87. [Google Scholar] [CrossRef]
- Trimboli, P.; Treglia, G.; Giovanella, L.; Bongiovanni, M. The role of systematic review and meta-analysis in modern cytopathology. Cancer Cytopathol. 2020, 128, 89–91. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors | Year | Type of Study | Country | Cancer Evaluated | PET Radiopharmaceuticals | No. of Cases Compared | Age (Years) | Male% |
|---|---|---|---|---|---|---|---|---|
| Ballal et al. [10] | 2021 | P-Mo | India | Various cancers | [18F]F-FDG and [68Ga]Ga-DOTA.SA.FAPI | 54 | 48.4 (mean) | 37% |
| Chen et al. [11] | 2020 | P-Mo | China | Various cancers | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 75 | 61.5 (median) | 63% |
| Chen et al. [12] | 2021 | P-Mo | China | Various cancers | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 68 | 57 (median) | 59% |
| Dendl et al. [13] | 2021 | R-Bi | Germany and South Africa | Gynecological cancers | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI tracers (FAPI-02, FAPI-04 or FAPI-46) | 10 | 59.5 (median) | 0% |
| Elboga et al. [14] | 2021 | R-Mo | Turkey | Breast cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 48 | 53.3 (mean) | 0% |
| Giesel et al. [15] | 2021 | R-Mu | Germany, USA and South Africa | Various cancers | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI tracers (FAPI-02, FAPI-04, FAPI-46 or FAPI-74) | 71 | 60 (median) | 61% |
| Guo et al. [16] | 2021 | R-Mo | China | Liver cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 34 | 60.6 (mean) | 74% |
| Jiang et al. [17] | 2021 | R-Bi | China | Gastric cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 38 | 67.5 (median) | 76% |
| Kessler et al. [18] | 2021 | P-Mo | Germany | Sarcoma | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-46 | 43 | 48.1 (mean) | 51% |
| Kömek et al. [19] | 2021 | P-Mo | Turkey | Breast cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 20 | 44 (median) | 0% |
| Kreppel et al. [20] | 2021 | R-Mo | Germany | Liver metastases of NETs | [18F]F-FDG, [68Ga]Ga-DATA5m.SA.FAPI and [68Ga]Ga-DOTA-TOC | 13 | 66.8 (mean) | 62% |
| Kuten et al. [21] | 2021 | P-Mo | Israel | Gastric cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 13 | 70 (median) | 46% |
| Lan et al. [22] | 2021 | P-Mo | China | Various cancers | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 123 | 56.1 (mean) | 56% |
| Linz et al. [23] | 2021 | P-Mo | Germany | Oral cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 10 | 62 (mean) | 80% |
| Pang et al. [24] | 2021 | R-Mo | China | Gastrointestinal cancers | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 35 | 64 (median) | 72% |
| Qin et al. [25] | 2021 | P-Mo | China | Gastric cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 20 | 56 (median) | 45% |
| Qin et al. [26] | 2021 | P-Mo | China | Nasopharyngeal cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 15 | 51.2 (mean) | 53% |
| Qin et al. [27] | 2021 | R-Mo | China | Bone metastases or bone and joint lesions | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 29 | 56.6 (mean) | 57% |
| Sahin et al. [28] | 2021 | R-Mo | Turkey | Liver metastases of gastrointestinal cancers | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 31 | 61.9 (mean) | 61% |
| Serfling et al. [29] | 2021 | R-Mo | Germany | Suspicious tonsillary tumor or CUP | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 8 | 62 (mean) | 75% |
| Shi et al. [30] | 2021 | P-Mo | China | Liver cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 20 | 58 (mean) | 90% |
| Wang et al. [31] | 2021 | P-Mo | China | Various cancers | [18F]F-FDG and Al [18F]F-NOTA-FAPI | 10 | 63.6 (mean) | 40% |
| Wang et al. [32] | 2021 | R-Mo | China | Liver cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 25 | 59.4 (mean) | 96% |
| Zhao et al. [33] | 2021 | R-Mo | China | Esophageal cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 21 | 60 (median) | 86% |
| Zhao et al. [34] | 2021 | R-Mo | China | Peritoneal carcinomatosis | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 46 | 57 (median) | 30% |
| Zhao et al. [35] | 2021 | R-Mo | China | Nasopharyngeal cancer | [18F]F-FDG and [68Ga]Ga-DOTA-FAPI-04 | 45 | 50 (median) | 78% |
| Authors | PET Hybrid Modality and Tomograph | Time between [18F]F-FDG and Radiolabeled FAPI PET | Mean [18F]F-FDG Injected Activity | Time between [18F]F-FDG injection and PET Acquisition | Mean Radiolabeled FAPI Injected Activity | Time between Radiolabeled FAPI Injection and PET Acquisition | PET Image Analysis | Reference Standard |
|---|---|---|---|---|---|---|---|---|
| Ballal et al. [10] | GE Discovery 710 PET/CT | within one week | 271 MBq | 1 h | 144.3 MBq | 1 h | Q and SQ | Composite |
| Chen et al. [11] | GE Discovery MI PET/CT | within one week | 3.7 MBq/kg | 1 h | 1.8–2.2 MBq/kg | 1 h | Q and SQ | Histology |
| Chen et al. [12] | GE Discovery MI PET/CT | within one week | 3.7 MBq/kg | 1 h | 1.8–2.2 MBq/kg | 1 h | Q and SQ | Composite |
| Dendl et al. [13] | Siemens Biograph mCT PET/CT | 1–89 days | 304 MBq | 1 h | 185 MBq | 1 h | Q and SQ | Composite |
| Elboga et al. [14] | GE Discovery IQ PET/CT | within one week | 3.5–5.5 MBq/kg | 1 h | 2 MBq/kg | 1 h | Q and SQ | Composite |
| Giesel et al. [15] | Siemens Biograph mCT or GE Discovery IQ PET/CT | 1–89 days | 316 MBq | 1 h | 185 MBq | 1 h | Q and SQ | Composite |
| Guo et al. [16] | GE Discovery MI PET/CT | within one week | 3.7 MBq/kg | 1 h | 148–259 MBq | 1 h | Q and SQ | Composite |
| Jiang et al. [17] | United Imaging uPMR790 TOF PET/MRI; Siemens Biograph mCT, Philips Ingenuity TF or United Imaging uMI510 PET/MRI | NR | NR | 1 h | 111–185 MBq | 1 h | Q and SQ | Histology |
| Kessler et al. [18] | Siemens Biograph mMR PET/MRI; Siemens Biograph mCT PET/CT | within four weeks | 214 MBq | 1 h | 144 MBq | 10 min | Q and SQ | Histology |
| Kömek et al. [19] | GE Discovery IQ PET/CT | within one week | 3.5–5.5 MBq/kg | 1 h | 2 MBq/kg | 1 h | Q and SQ | Composite |
| Kreppel et al. [20] | Siemens Biograph 2, Philips Gemini GXL, or GE Discovery STE PET/CT | NR | 267 MBq | 74 min | 184 MBq | 79 min | Q and SQ | Histology |
| Kuten et al. [21] | GE Discovery MI PET/CT | 1–23 days | 3.7 MBq/kg | 1 h | 1.8–2.2 MBq/kg | 1 h | Q and SQ | Composite |
| Lan et al. [22] | United Imaging uMI780 PET/CT | within three days | 3.7 MBq/kg | 45–60 min | 1.85 MBq/kg | 1 h | Q and SQ | Composite |
| Linz et al. [23] | Siemens Biograph mCT PET/CT | 2–16 days | 269 MBq | 1 h | 119 MBq | 1 h | Q and SQ | Histology |
| Pang et al. [24] | GE Discovery MI PET/CT | within one week | 3.7 MBq/kg | 1 h | 1.8–2.2 MBq/kg | 1 h | Q and SQ | Histology |
| Qin et al. [25] | GE SIGNA PET/MRI; GE Discovery VCT PET/CT | within one week | 3.7–5.55 MBq/kg | 1 h | 1.85–3.7 MBq/kg | 30–60 min | Q and SQ | Composite |
| Qin et al. [26] | GE SIGNA PET/MRI; GE Discovery VCT PET/CT | within one week | 3.7–5.4 MBq/kg | 1 h | 1.85–3.7 MBq/kg | 30–60 min | Q and SQ | Composite |
| Qin et al. [27] | GE SIGNA PET/MRI; GE Discovery VCT PET/CT | within one week | NR | NR | 1.85–3.7 MBq/kg | 20–60 min | Q and SQ | Composite |
| Sahin et al. [28] | GE Discovery IQ PET/CT | at least two weeks | 5 MBq/kg | 1 h | 2–3 MBq/kg | 45 min | Q and SQ | Composite |
| Serfling et al. [29] | Siemens Biograph mCT PET/CT | within one week | 292 MBq | 1 h | 145 MBq | 1 h | Q and SQ | Histology |
| Shi et al. [30] | Sinounion Healthcare PoleStar m660 PET/CT | within three days | 3.7 MBq/kg | 60–90 min | 3.59 MBq/kg | 40–50 min | Q and SQ | Composite |
| Wang et al. [31] | Siemens Biograph mCT PET/CT | NR | NR | NR | 173.5–256.8 MBq | 60–90 min | Q and SQ | Composite |
| Wang et al. [32] | Siemens Biograph mCT or Union Imaging uMI510 PET/CT | within one day | NR | NR | 185 MBq | 1 h | Q and SQ | Composite |
| Zhao et al. [33] | GE Discovery MI PET/CT | within one week | 3.7–5.5 MBq/kg | 1 h | 1.8–2.2 MBq/kg | 1 h | Q and SQ | Composite |
| Zhao et al. [34] | GE Discovery MI PET/CT | within one week | 3.7 MBq/kg | 1 h | 1.8–2.2 MBq/kg | 1 h | Q and SQ | Composite |
| Zhao et al. [35] | GE Discovery MI PET/CT | NR | 3.7 MBq/kg | 40 min | 1.8–2.2 MBq/kg | 40 min | Q and SQ | Composite |
| Authors | Cancer Evaluated | Significant Higher Uptake of Radiolabeled FAPI Compared to [18F]F-FDG | Significant Higher TBR of Radiolabeled FAPI Compared to [18F]F-FDG | Comparison in the Detection of Primary Tumors | Comparison in the Detection of Metastases |
|---|---|---|---|---|---|
| Ballal et al. [10] | Various cancers | only for brain metastases | only for brain metastases | NR | NR |
| Chen et al. [11] | Various cancers | yes | yes | FAPI > FDG | FAPI > FDG |
| Chen et al. [12] | Various cancers | yes | yes | FAPI > FDG | FAPI > FDG |
| Dendl et al. [13] | Gynecological cancers | no | only for distant metastases | NR | NR |
| Elboga et al. [14] | Breast cancer | yes | NR | FAPI > FDG | FAPI > FDG |
| Giesel et al. [15] | Various cancers | no | only for liver and bone metastases | NR | NR |
| Guo et al. [16] | Liver cancer | yes | yes | FAPI > FDG | FAPI > FDG |
| Jiang et al. [17] | Gastric cancer | no | yes | FAPI > FDG | FAPI = FDG |
| Kessler et al. [18] | Sarcoma | no | yes | FAPI = FDG | FAPI = FDG |
| Kömek et al. [19] | Breast cancer | yes | yes | FAPI > FDG | FAPI > FDG |
| Kreppel et al. [20] | Liver metastases of NETs | yes | NR | NR | FAPI > FDG |
| Kuten et al. [21] | Gastric cancer | no | yes | FAPI > FDG | FAPI > FDG |
| Lan et al. [22] | Various cancers | yes | no | FAPI > FDG | FAPI > FDG |
| Linz et al. [23] | Oral cancer | no | NR | FAPI = FDG | FAPI = FDG |
| Pang et al. [24] | Gastrointestinal cancers | yes | NR | FAPI > FDG | FAPI > FDG |
| Qin et al. [25] | Gastric cancer | yes | yes | FAPI > FDG | FAPI > FDG |
| Qin et al. [26] | Nasopharyngeal cancer | no | NR | FAPI = FDG | FAPI > FDG |
| Qin et al. [27] | Bone metastases or bone and joint lesions | no | NR | NR | FAPI > FDG |
| Sahin et al. [28] | Liver metastases of gastrointestinal cancers | no | yes | NR | FAPI > FDG |
| Serfling et al. [29] | Suspicious tonsillary tumor or CUP | no | yes | FAPI = FDG | FAPI < FDG |
| Shi et al. [30] | Liver cancer | yes | yes | FAPI > FDG | FAPI > FDG |
| Wang et al. [31] | Various cancers | no | yes | FAPI = FDG | FAPI > FDG |
| Wang et al. [32] | Liver cancer | no | yes | FAPI > FDG | FAPI > FDG |
| Zhao et al. [33] | Esophageal cancer | yes | NR | NR | NR |
| Zhao et al. [34] | Peritoneal carcinomatosis | yes | NR | NR | FAPI > FDG |
| Zhao et al. [35] | Nasopharyngeal cancer | yes | NR | FAPI = FDG | FAPI > FDG |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Treglia, G.; Muoio, B.; Roustaei, H.; Kiamanesh, Z.; Aryana, K.; Sadeghi, R. Head-to-Head Comparison of Fibroblast Activation Protein Inhibitors (FAPI) Radiotracers versus [18F]F-FDG in Oncology: A Systematic Review. Int. J. Mol. Sci. 2021, 22, 11192. https://doi.org/10.3390/ijms222011192
Treglia G, Muoio B, Roustaei H, Kiamanesh Z, Aryana K, Sadeghi R. Head-to-Head Comparison of Fibroblast Activation Protein Inhibitors (FAPI) Radiotracers versus [18F]F-FDG in Oncology: A Systematic Review. International Journal of Molecular Sciences. 2021; 22(20):11192. https://doi.org/10.3390/ijms222011192
Chicago/Turabian StyleTreglia, Giorgio, Barbara Muoio, Hessamoddin Roustaei, Zahra Kiamanesh, Kamran Aryana, and Ramin Sadeghi. 2021. "Head-to-Head Comparison of Fibroblast Activation Protein Inhibitors (FAPI) Radiotracers versus [18F]F-FDG in Oncology: A Systematic Review" International Journal of Molecular Sciences 22, no. 20: 11192. https://doi.org/10.3390/ijms222011192