
Natural Polymers for the Maintenance of Oral Health: Review of Recent Advances and Perspectives


Abstract
:1. Introduction
2. Material and Methods
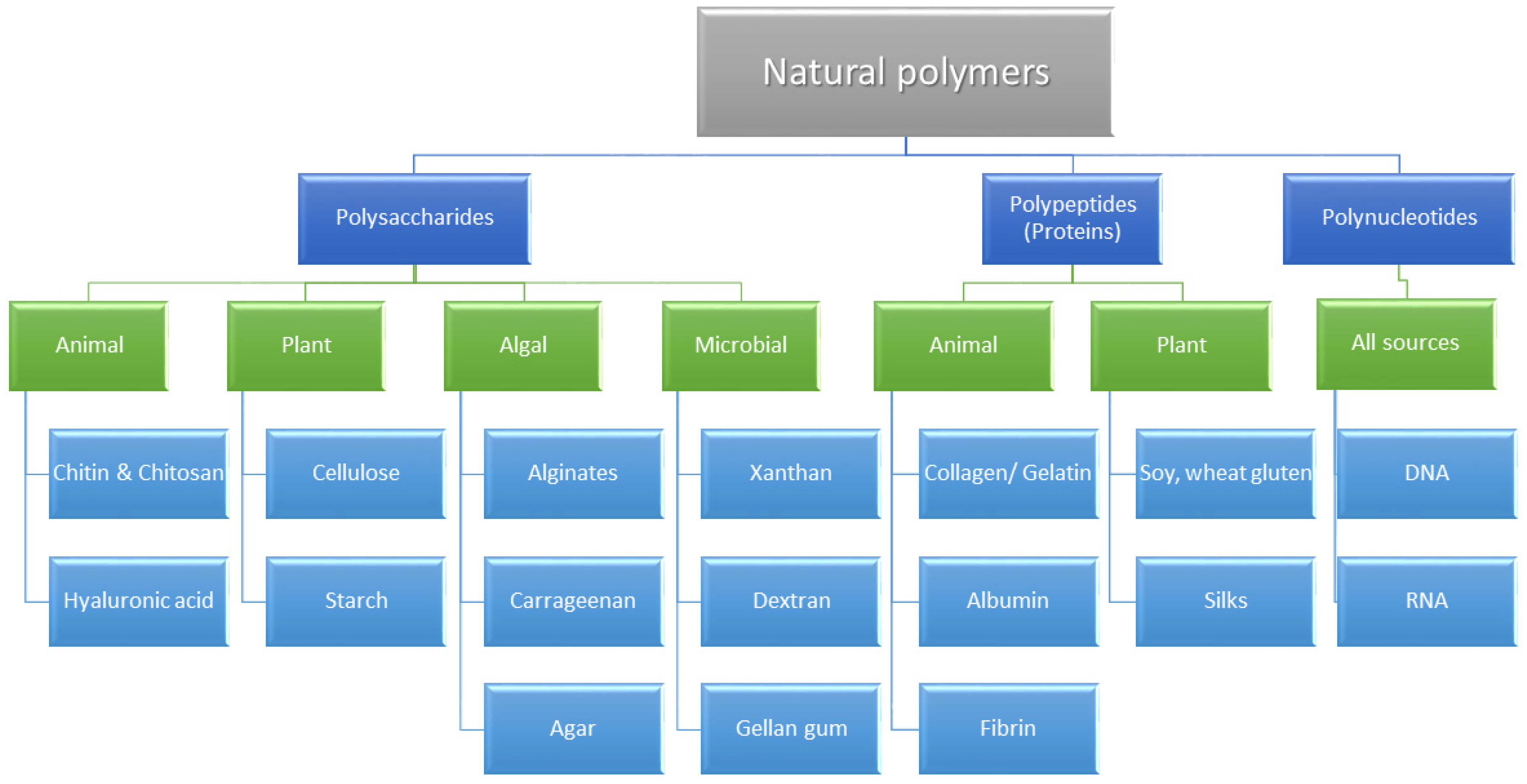
3. Chemical Classification and Biological Activity of Natural Dental Polymers
3.1. Polysaccharides
3.1.1. Chitosan
3.1.2. Cellulose
3.1.3. Hyaluronic Acid
3.1.4. Sodium Alginate
3.1.5. Agarose
3.1.6. Synthetic Polysaccharides Based on Monomers Obtained from Natural Resources
3.2. Proteins
3.2.1. Collagen
3.2.2. Fibrin
3.2.3. Gelatin
3.2.4. Bone Morphogenetic Proteins (BMPs)
3.3. Polynucleotides
4. Oral Applications of Natural Polymers
4.1. Caries Management
4.2. Periodontal and Oral Mucosa Disease Management
4.3. Manufacturing of Oral Appliances and Dentures
4.4. Oral Tissue Regeneration and Oral Surgery
4.5. Oral Drug Delivery Systems
4.6. Other Uses
5. Natural vs. Synthetic Polymers for Dental Application
6. Perspectives
7. Study’s Limitations
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Abdolahpour, Z.; Saneipour, Z.; Azarhoosh, M.J. Application of Biomaterials in Dentistry. Curr. Trends. Biomed. Eng. Biosci. 2017, 2, 44–47. [Google Scholar] [CrossRef]
- Vert, M.; Doi, Y.; Hellwich, K.-H.; Hess, M.; Hodge, P.; Kubisa, P.; Rinaudo, M.; Schué, F. Terminology for biorelated polymers and applications (IUPAC Recommendations 2012). Pure Appl. Chem. 2012, 84, 377–410. [Google Scholar] [CrossRef]
- Zakrzewski, W.; Dobrzynski, M.; Rybak, Z.; Szymonowicz, M.; Wiglusz, R.J. Selected Nanomaterials’ Application Enhanced with the Use of Stem Cells in Acceleration of Alveolar Bone Regeneration during Augmentation Process. Nanomaterials 2020, 10, 1216. [Google Scholar] [CrossRef]
- Lodge, T. Commentary: The promise of polymers. Phys. Today 2017, 70, 10–12. [Google Scholar] [CrossRef] [Green Version]
- Alla, R.; Swamy, K.; Vyas, R.C. Isolation of Textile Waste Cellulose Nanofibrillated Fibre Reinforced in Polylactic Acid-Chitin Biodegradable Composite for Green Packaging Application. Int. J. Appl. Dent. Sci. 2015, 1, 82–89. [Google Scholar]
- Yildiz, O.; Seyrek, M.; Guven Polat, G.; Marti Akgun, O.; Macit, E. Dental Polymers: Effects on Vascular Tone, Encyclopedia of Biomedical Polymers and Polymeric Biomaterials; Taylor & Francis: New York, NY, USA, 2014; pp. 1–13. [Google Scholar]
- Young, J.; Feng, Z.; Dimitropoulos, D.; Sala, R.; Westbrook, J.; Zhuravleva, M.; Shao, C.; Quesada, M.; Peisach, E.; Berman, H.M. Chemical annotation of small and peptide-like molecules at the Protein Data Bank. Database 2013, 2013, bat079. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D. Poly(Vinyl Alcohol) Recent Contributions to Engineering and Medicine. J. Compos. Sci. 2020, 4, 175. [Google Scholar] [CrossRef]
- Schlüter, A.D.; Payamyar, P.; Öttinger, H.C. How the World Changes by Going from One- to Two-Dimensional Polymers in Solution. Macromol. Rapid Commun. 2016, 37, 1638–1650. [Google Scholar] [CrossRef]
- Kliem, S.; Kreutzbruck, M.; Bonten, C. Review on the Biological Degradation of Polymers in Various Environments. Materials 2020, 13, 4586. [Google Scholar] [CrossRef] [PubMed]
- Ghanbarzadeh, B.; Almasi, H. Biodegradable Polymers; IntechOpen: London, UK, 2013. [Google Scholar] [CrossRef] [Green Version]
- Joyce, K.; Targa Fabra, G.; Bozkurt, Y.; Pandit, A. Bioactive potential of natural biomaterials: Identification, retention and assessment of biological properties. Signal Transduct. Target. Ther. 2021, 6, 122. [Google Scholar] [CrossRef]
- Zein, N.; Harmouch, E.; Lutz, J.-C.; De Grado, G.F.; Kuchler-Bopp, S.; Clauss, F.; Offner, D.; Hua, G.; Benkirane-Jessel, N.; Fioretti, F. Polymer-Based Instructive Scaffolds for Endodontic Regeneration. Materials 2019, 12, 2347. [Google Scholar] [CrossRef] [Green Version]
- Mohammed, A.S.A.; Naveed, M.; Jost, N. Polysaccharides; Classification, Chemical Properties, and Future Perspective Applications in Fields of Pharmacology and Biological Medicine (A Review of Current Applications and Upcoming Potentialities). J. Polym. Environ. 2021, 29, 2359–2371. [Google Scholar] [CrossRef] [PubMed]
- Weickert, M.O.; Pfeiffer, A.F.H. Metabolic Effects of Dietary Fiber Consumption and Prevention of Diabetes. J. Nutr. 2008, 138, 439–442. [Google Scholar] [CrossRef]
- Anderson, J.W.; Baird, P.; Davis, R.H., Jr.; Ferreri, S.; Knudtson, M.; Koraym, A.; Waters, V.; Williams, C.L. Health benefits of dietary fiber. Nutr. Rev. 2009, 67, 188–205. [Google Scholar] [CrossRef] [PubMed]
- Svenningsen, N.B.; García, E.M.; Nicolaisen, M.; De Lorenzo, V.; Nybroe, O. The biofilm matrix polysaccharides cellulose and alginate both protect Pseudomonas putida mt-2 against reactive oxygen species generated under matric stress and copper exposure. Microbiology 2018, 164, 883–888. [Google Scholar] [CrossRef]
- Zhang, G.; Liu, J.; Li, R.; Jiao, S.; Feng, C.; Wang, Z.A.; Du, Y. Conjugation of Inulin Improves Anti-Biofilm Activity of Chitosan. Mar. Drugs 2018, 16, 151. [Google Scholar] [CrossRef] [Green Version]
- Battistella, E.; Varoni, E.M.; Cochis, A.; Palazzo, B.; Rimondini, L. Degradable polymers may improve dental practice. J. Appl. Biomater. Biomech. 2011, 9, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Jia, S.; Yang, X.; Song, W.; Wang, L.; Fang, K.; Hu, Z.; Yang, Z.; Shan, C.; Lei, D. Incorporation of osteogenic and angiogenic small interfering RNAs into chitosan sponge for bone tissue engineering. Int. J. Nanomed. 2014, 9, 5307–5316. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Behl, T.; Uniyal, T.; Chadha, S. Synthesis of Nanostructured Lipid Carriers Loaded Chitosan/ Carbopol Hybrid Nanocomposite Gel for Oral Delivery of Artemether and Curcumin. Pharm. Nanotechnol. 2020, 8, 418–432. [Google Scholar] [CrossRef]
- VandeVord, P.J.; Matthew, H.; DeSilva, S.P.; Mayton, L.; Wu, B.; Wooley, P.H. Evaluation of the biocompatibility of a chitosan scaffold in mice. J. Biomed. Mater. Res. 2001, 59, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.B.; Sharma, C.P. Use of Chitosan as a Biomaterial: Studiens on its Safety and Hemostatic Potential. J. Biomed. Mat. Res. 1997, 34, 21–28. [Google Scholar] [CrossRef]
- Tomihata, K.; Ikada, Y. In vitro and in vivo degradation of films of chitin and its deacetylated derivatives. Biomaterials 1997, 18, 567–575. [Google Scholar] [CrossRef]
- Lai, W.-F.; Oka, K.; Jung, H.-S. Advanced functional polymers for regenerative and therapeutic dentistry. Oral Dis. 2014, 21, 550–557. [Google Scholar] [CrossRef]
- Aguilar, A.; Zein, N.; Harmouch, E.; Hafdi, B.; Bornert, F.; Offner, D.; Clauss, F.; Fioretti, F.; Huck, O.; Benkirane-Jessel, N.; et al. Application of Chitosan in Bone and Dental Engineering. Molecules 2019, 24, 3009. [Google Scholar] [CrossRef] [Green Version]
- Barud, H.G.D.O.; Da Silva, R.R.; Borges, M.A.C.; Castro, G.R.; Ribeiro, S.J.L.; Barud, H.D.S. Bacterial Nanocellulose in Dentistry: Perspectives and Challenges. Molecules 2020, 26, 49. [Google Scholar] [CrossRef]
- Sun, B.; Zhang, M.; Shen, J.; He, Z.; Fatehi, P.; Ni, Y. Applications of Cellulose-based Materials in Sustained Drug Delivery Systems. Curr. Med. Chem. 2019, 26, 2485–2501. [Google Scholar] [CrossRef]
- Colangelo, M.; Belletti, S.; Govoni, P.; Guizzardi, S.; Galli, C. A Biomimetic Polynucleotides–Hyaluronic Acid Hydrogel Promotes Wound Healing in a Primary Gingival Fibroblast Model. Appl. Sci. 2021, 11, 4405. [Google Scholar] [CrossRef]
- Casale, M.; Moffa, A.; Vella, P.; Sabatino, L.; Capuano, F.; Salvinelli, B.; Lopez, M.A.; Carinci, F.; Salvinelli, F. Hyaluronic acid: Perspectives in dentistry. A systematic review. Int. J. Immunopathol. Pharmacol. 2016, 29, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Otterlei, M.; Østgaard, K.; Skjåk-Bræk, G.; Smidsrød, O.; Soon-Shiong, P.; Espevik, T. Induction of Cytokine Production from Human Monocytes Stimulated with Alginate. J. Immunother. 1991, 10, 286–291. [Google Scholar] [CrossRef]
- Ahmad, A.; Mubarak, N.; Jannat, F.T.; Ashfaq, T.; Santulli, C.; Rizwan, M.; Najda, A.; Bin-Jumah, M.; Abdel-Daim, M.M.; Hussain, S.; et al. A Critical Review on the Synthesis of Natural Sodium Alginate Based Composite Materials: An Innovative Biological Polymer for Biomedical Delivery Applications. Processes 2021, 9, 137. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Herford, A.S.; Laino, L.; Troiano, G.; Amoroso, G.; Crimi, S.; Matarese, M.; D’Amico, C.; Siniscalchi, E.N.; et al. Alginate Materials and Dental Impression Technique: A Current State of the Art and Application to Dental Practice. Mar. Drugs 2018, 17, 18. [Google Scholar] [CrossRef] [Green Version]
- Burzynski, J.A.; Firestone, A.R.; Beck, F.M.; Fields, H.W.; Deguchi, T. Comparison of digital intraoral scanners and alginate impressions: Time and patient satisfaction. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 534–541. [Google Scholar] [CrossRef]
- Reddy, M.; Ponnamma, D.; Choudhary, R.; Sadasivuni, K. A Comparative Review of Natural and Synthetic Biopolymer Composite Scaffolds. Polymers 2021, 13, 1105. [Google Scholar] [CrossRef]
- El Moshy, S.; Abbass, M.M.; El-Motayam, A.M. Biomimetic remineralization of acid etched enamel using agarose hydrogel model. F1000Research 2018, 7, 1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honduvilla, N.G.; Coca, A.; Ortega, A.M.; Trejo, C.; Román, J.; Peña, J.; Cabañas, V.; Regi, M.V.; Buján, J. Improved connective integration of a degradable 3D-nano-apatite/agarose scaffold subcutaneously implanted in a rat model. J. Biomater. Appl. 2018, 33, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Suzawa, Y.; Kubo, N.; Iwai, S.; Yura, Y.; Ohgushi, H.; Akashi, M. Biomineral/Agarose Composite Gels Enhance Proliferation of Mesenchymal Stem Cells with Osteogenic Capability. Int. J. Mol. Sci. 2015, 16, 14245–14258. [Google Scholar] [CrossRef]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An Overview of Poly(lactic-co-glycolic) Acid (PLGA)-Based Biomaterials for Bone Tissue Engineering. Int. J. Mol. Sci. 2014, 15, 3640–3659. [Google Scholar] [CrossRef] [PubMed]
- Ardejani, M.S.; Orner, B.P. Obey the Peptide Assembly Rules. Science 2013, 340, 561–562. [Google Scholar] [CrossRef]
- Filippi, M.; Born, G.; Chaaban, M.; Scherberich, A. Natural Polymeric Scaffolds in Bone Regeneration. Front. Bioeng. Biotechnol. 2020, 8, 474. [Google Scholar] [CrossRef]
- Kim, M.G.; Park, C.H. Tooth-Supporting Hard Tissue Regeneration Using Biopolymeric Material Fabrication Strategies. Molecules 2020, 25, 4802. [Google Scholar] [CrossRef]
- Bressan, E.; Favero, V.; Gardin, C.; Ferroni, L.; Iacobellis, L.; Favero, L.; Vindigni, V.; Berengo, M.; Sivolella, S.; Zavan, B. Biopolymers for Hard and Soft Engineered Tissues: Application in Odontoiatric and Plastic Surgery Field. Polymers 2011, 3, 509–526. [Google Scholar] [CrossRef]
- Shetty, A.; Imran, M.; Ahmed, N.; Gopalakrishna, V.; Nagraj, V. Efficacy of PRF vs PRF + Biodegradable Collagen Plug in Post-extraction Preservation of Socket. J. Contemp. Dent. Pract. 2019, 20, 1323–1328. [Google Scholar] [CrossRef]
- Sheikh, Z.; Qureshi, J.; Alshahrani, A.M.; Nassar, H.; Ikeda, Y.; Glogauer, M.; Ganss, B. Collagen based barrier membranes for periodontal guided bone regeneration applications. Odontology 2016, 105, 1–12. [Google Scholar] [CrossRef]
- Conte, R.; Di Salle, A.; Riccitiello, F.; Petillo, O.; Peluso, G.; Calarco, A. Biodegradable polymers in dental tissue engineering and regeneration. AIMS Mater. Sci. 2018, 5, 1073–1101. [Google Scholar] [CrossRef]
- Jazayeri, H.E.; Fahmy, M.D.; Razavi, M.; Stein, B.E.; Nowman, A.; Masri, R.M.; Tayebi, L. Dental Applications of Natural-Origin Polymers in Hard and Soft Tissue Engineering. J. Prosthodont. 2016, 25, 510–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisel, J.W.; Litvinov, R.I. Fibrin Formation, Structure and Properties. In Fibrous Proteins: Structures and Mechanisms; Springer: Cham, Switzerland, 2017; Volume 82, pp. 405–456. [Google Scholar] [CrossRef] [Green Version]
- Jayadev, M.; Marshal, V.R.; Naik, B.; Karunakar, P. Role of Platelet rich fibrin in wound healing: A critical review. J. Conserv. Dent. 2013, 16, 284–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanaati, S.; Herrera-Vizcaino, C.; Al-Maawi, S.; Lorenz, J.; Miron, R.J.; Nelson, K.; Schwarz, F.; Choukroun, J.; Sader, R. Fifteen Years of Platelet Rich Fibrin in Dentistry and Oromaxillofacial Surgery: How High is the Level of Scientific Evidence? J. Oral Implant. 2018, 44, 471–492. [Google Scholar] [CrossRef]
- Kabiri, M.; Emami, S.H.; Rafinia, M.; Tahriri, M. Preparation and characterization of absorbable hemostat crosslinked gelatin sponges for surgical applications. Curr. Appl. Phys. 2011, 11, 457–461. [Google Scholar] [CrossRef]
- Lynch, C.; Kondiah, P.; Choonara, Y. Advanced Strategies for Tissue Engineering in Regenerative Medicine: A Biofabrication and Biopolymer Perspective. Molecules 2021, 26, 2518. [Google Scholar] [CrossRef]
- Thakur, G.; Mitra, A.; Basak, A.; Sheet, D. Characterization and scanning electron microscopic investigation of crosslinked freeze dried gelatin matrices for study of drug diffusivity and release kinetics. Micron 2012, 43, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, G.J.; Hatton, M.N. Prevention of alveolar osteitis. A Case report and review of literature. N. Y. State Dent. J. 2016, 82, 21–25. [Google Scholar]
- Ndlovu, S.P.; Ngece, K.; Alven, S.; Aderibigbe, B.A. Gelatin-Based Hybrid Scaffolds: Promising Wound Dressings. Polymers 2021, 13, 2959. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, T.; Watabe, T. Bone Morphogenetic Proteins. Cold Spring Harb. Perspect. Biol. 2016, 8, a021899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.N.; Green, J.; Wang, Z.; Deng, Y.; Qiao, M.; Peabody, M.; Zhang, Q.; Ye, J.; Yan, Z.; Denduluri, S.; et al. Bone Morphogenetic Protein (BMP) signaling in development and human diseases. Genes Dis. 2014, 1, 87–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz-Sanchez, R.M.; Yañez-Vico, R.; Fernández-Olavarría, A.; Mosquera-Pérez, R.; Iglesias-Linares, A.; Torres-Lagares, D. Current Approaches of Bone Morphogenetic Proteins in Dentistry. J. Oral Implant. 2015, 41, 337–342. [Google Scholar] [CrossRef]
- Regy, R.M.; Dignon, G.L.; Zheng, W.; Kim, Y.C.; Mittal, J. Sequence dependent phase separation of protein-polynucleotide mixtures elucidated using molecular simulations. Nucleic Acids Res. 2020, 48, 12593–12603. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Ren, J.; Yin, W.; Ding, H.; Lu, Q.; Tan, L.; Deng, S.; Liu, J.; Yang, Q.; Wang, J.; et al. Inhibition of Ctsk modulates periodontitis with arthritis via downregulation of TLR9 and autophagy. Cell Prolif. 2019, 53, e12722. [Google Scholar] [CrossRef] [PubMed]
- Ou, L.; Sun, T.; Liu, M.; Zhang, Y.; Zhou, Z.; Zhan, X.; Lu, L.; Zhao, Q.; Lai, R.; Shao, L. Efficient miRNA Inhibitor Delivery with Graphene Oxide-Polyethylenimine to Inhibit Oral Squamous Cell Carcinoma. Int. J. Nanomed. 2020, 15, 1569–1583. [Google Scholar] [CrossRef] [Green Version]
- Santarelli, A.; Mascitti, M.; Russo, L.L.; Sartini, D.; Troiano, G.; Emanuelli, M.; Muzio, L.L. Survivin-Based Treatment Strategies for Squamous Cell Carcinoma. Int. J. Mol. Sci. 2018, 19, 971. [Google Scholar] [CrossRef] [Green Version]
- Afrasiabi, S.; Pourhajibagher, M.; Raoofian, R.; Tabarzad, M.; Bahador, A. Therapeutic applications of nucleic acid aptamers in microbial infections. J. Biomed. Sci. 2020, 27, 6–13. [Google Scholar] [CrossRef]
- Vahed, S.Z.; Fathi, N.; Samiei, M.; Dizaj, S.M.; Sharifi, S. Targeted cancer drug delivery with aptamer-functionalized polymeric nanoparticles. J. Drug Target. 2018, 27, 292–299. [Google Scholar] [CrossRef]
- Hu, M.-L.; Zheng, G.; Zhang, Y.-D.; Yan, X.; Li, X.-C.; Lin, H. Effect of desensitizing toothpastes on dentine hypersensitivity: A systematic review and meta-analysis. J. Dent. 2018, 75, 12–21. [Google Scholar] [CrossRef]
- Binaljadm, T.; Moorehead, R.; Almela, T.; Franklin, K.; Tayebi, L.; Moharamzadeh, K. Biomodification of a Class-V Restorative Material by Incorporation of Bioactive Agents. Dent. J. 2019, 7, 110. [Google Scholar] [CrossRef] [Green Version]
- Moussa, D.G.; Aparicio, C. Present and future of tissue engineering scaffolds for dentin-pulp complex regeneration. J. Tissue Eng. Regen. Med. 2018, 13, 58–75. [Google Scholar] [CrossRef] [Green Version]
- Souza, B.M.; Machado, P.F.; Vecchia, L.R.; Magalhães, A.C. Effect of chitosan solutions with or without fluoride on the protection against dentin erosion in vitro. Eur. J. Oral. Sci. 2020, 128, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Galler, K.M.; Brandl, F.P.; Kirchhof, S.; Widbiller, M.; Eidt, A.; Buchalla, W.; Göpferich, A.; Schmalz, G. Suitability of Different Natural and Synthetic Biomaterials for Dental Pulp Tissue Engineering. Tissue Eng. Part A 2018, 24, 234–244. [Google Scholar] [CrossRef]
- Soares, D.G.; Rosseto, H.L.; Scheffel, D.; Basso, F.G.; Huck, C.; Hebling, J.; Costa, C.A.D.S. Odontogenic differentiation potential of human dental pulp cells cultured on a calcium-aluminate enriched chitosan-collagen scaffold. Clin. Oral Investig. 2017, 21, 2827–2839. [Google Scholar] [CrossRef]
- Shue, L.; Yufeng, Z.; Mony, U. Biomaterials for periodontal regeneration: A review of ceramics and polymers. Biomatter 2012, 2, 271–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toledano, M.; Toledano-Osorio, M.; Carrasco-Carmona, Á.; Vallecillo, C.; Lynch, C.D.; Osorio, M.T.; Osorio, R. State of the Art on Biomaterials for Soft Tissue Augmentation in the Oral Cavity. Part I: Natural Polymers-Based Biomaterials. Polymers 2020, 12, 1850. [Google Scholar] [CrossRef]
- Park, C.H.; Oh, J.-H.; Jung, H.-M.; Choi, Y.; Rahman, S.U.; Kim, S.; Kim, T.-I.; Shin, H.-I.; Lee, Y.-S.; Yu, F.H.; et al. Effects of the incorporation of ε-aminocaproic acid/chitosan particles to fibrin on cementoblast differentiation and cementum regeneration. Acta Biomater. 2017, 61, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, Z.; Hamdan, N.; Ikeda, Y.; Grynpas, M.; Ganss, B.; Glogauer, M. Natural graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive applications: A review. Biomater. Res. 2017, 21, 9. [Google Scholar] [CrossRef] [PubMed]
- Budai-Szűcs, M.; Ruggeri, M.; Faccendini, A.; Léber, A.; Rossi, S.; Varga, G.; Bonferoni, M.; Vályi, P.; Burián, K.; Csányi, E.; et al. Electrospun Scaffolds in Periodontal Wound Healing. Polymers 2021, 13, 307. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.-C.; Tai, W.-C.; Luo, H.-T.; Lai, C.-H.; Lin, H.-H.; Lin, Z.-J.; Chang, Y.-C.; Lee, B.-S. Core-Shell poly-(D,l-Lactide-co-Glycolide)-chitosan Nanospheres with simvastatin-doxycycline for periodontal and osseous repair. Int. J. Biol. Macromol. 2020, 158, 627–635. [Google Scholar] [CrossRef]
- Parker, K.; Marlow, B.; Patel, N.; Gill, D.S. A review of mouthguards: Effectiveness, types, characteristics and indications for use. Br. Dent. J. 2017, 222, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Gawlak, D.; Mańka-MAlara, K.; Mierzwińska-Nastalska, E.; Waśniewski, B.; Ryszkowska, J. Comparison of hardness, energy absorption and water absorbabity of polymeric materials used in the manufacture of mouthgouards. Dent. Med. Probl. 2015, 52, 78–85. [Google Scholar]
- Yamada, R.; Nozaki, K.; Horiuchi, N.; Yamashita, K.; Nemoto, R.; Miura, H.; Nagai, A. Ag nanoparticle–coated zirconia for antibacterial prosthesis. Mater. Sci. Eng. C 2017, 78, 1054–1060. [Google Scholar] [CrossRef]
- Walczak, K.; Schierz, G.; Basche, S.; Petto, C.; Boening, K.; Wieckiewicz, M. Antifungal and Surface Properties of Chitosan-Salts Modified PMMA Denture Base Material. Molecules 2020, 25, 5899. [Google Scholar] [CrossRef]
- Park, S.; Kim, H.-H.; Bin Yang, S.; Moon, J.-H.; Ahn, H.-W.; Hong, J. A Polysaccharide-Based Antibacterial Coating with Improved Durability for Clear Overlay Appliances. ACS Appl. Mater. Interfaces 2018, 10, 17714–17721. [Google Scholar] [CrossRef]
- Atai, Z.; Atai, M.; Amini, J.; Salehi, N. In vivo study of antifungal effects of low-molecular-weight chitosan against Candida albicans. J. Oral Sci. 2017, 59, 425–430. [Google Scholar] [CrossRef] [Green Version]
- Bohner, M. Resorbable biomaterials as bone graft substitutes. Mater. Today 2010, 13, 24–30. [Google Scholar] [CrossRef]
- Chung, J.-H.; Kim, Y.K.; Kim, K.-H.; Kwon, T.-Y.; Vaezmomeni, S.Z.; Samiei, M.; Aghazadeh, M.; Davaran, S.; Mahkam, M.; Asadi, G.; et al. Synthesis, characterization, biocompatibility of hydroxyapatite–natural polymers nanocomposites for dentistry applications. Artif. Cells Nanomed. Biotechnol. 2014, 44, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Bastami, F.; Paknejad, Z.; Jafari, M.; Salehi, M.; Rad, M.R.; Khojasteh, A. Fabrication of a three-dimensional β-tricalcium-phosphate/gelatin containing chitosan-based nanoparticles for sustained release of bone morphogenetic protein-2: Implication for bone tissue engineering. Mater. Sci. Eng. C 2017, 72, 481–491. [Google Scholar] [CrossRef]
- Awartani, F.A.; Tatakis, D.N. Interdental papilla loss: Treatment by hyaluronic acid gel injection: A case series. Clin. Oral Investig. 2015, 20, 1775–1780. [Google Scholar] [CrossRef] [PubMed]
- Suchánek, J.; Ivančaková, R.K.; Mottl, R.; Browne, K.Z.; Pilneyová, K.C.; Pilbauerová, N.; Schmidt, J.; Kleplová, T.S. Hyaluronic Acid-Based Medical Device for Treatment of Alveolar Osteitis-Clinical Study. Int. J. Environ. Res. Public Health 2019, 16, 3698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, N.; Wang, X.; Qin, L.; Zhai, M.; Yuan, J.; Chen, J.; Li, D. Effect of Hyaluronic Acid in Bone Formationa and its Appli-cations in Dentistry. J. Biomed. Mater. Res. A 2016, 104, 1560–1569. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.M.; Manzulli, N.; D’Angelo, A.; Lauritano, D.; Papalia, R.; Candotto, V. The use of hyaluronic acid as an adjuvant in the management of peri-implantitis. J. Boil. Regul. Homeost. Agents 2017, 31, 123–127. [Google Scholar]
- Neumann, A.H.; Broek, M.J.V.D. Increased collagen IV layer in the basal membrane area of the capillaries in severe chronic venous insufficiency. Vasa 1991, 20, 26–29. [Google Scholar]
- Wessing, B.; Lettner, S.; Zechner, W. Guided Bone Regeneration with Collagen Membranes and Particulate Graft Materials: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 87–100. [Google Scholar] [CrossRef]
- Tomakidi, P.; Fusenig, N.E.; Kohl, A.; Komposch, G. Histomorphological and biochemical differentiation capacity in organotypic co-cultures of primary gingival cells. J. Periodontal Res. 1997, 32, 388–400. [Google Scholar] [CrossRef]
- Jazayeri, H.E.; Tahriri, M.; Razavi, M.; Khoshroo, K.; Fahimipour, F.; Dashtimoghadam, E.; Almeida, L.; Tayebi, L. A current overview of materials and strategies for potential use in maxillofacial tissue regeneration. Mater. Sci. Eng. C 2017, 70, 913–929. [Google Scholar] [CrossRef] [Green Version]
- Van Bellinghen, X.; Idoux-Gillet, Y.; Pugliano, M.; Strub, M.; Bornert, F.; Clauss, F.; Schwinté, P.; Keller, L.; Benkirane-Jessel, N.; Kuchler-Bopp, S.; et al. Temporomandibular Joint Regenerative Medicine. Int. J. Mol. Sci. 2018, 19, 446. [Google Scholar] [CrossRef] [Green Version]
- Wieckiewicz, M.; Boening, K.; Wiland, P.; Shiau, Y.-Y.; Paradowska-Stolarz, A. Reported concepts for the treatment modalities and pain management of temporomandibular disorders. J. Headache Pain 2015, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Kutuk, S.G.; Gökçe, G.; Arslan, M.; Özkan, Y.; Kütük, M.; Arikan, O.K. Clinical and Radiological Comparison of Effects of Platelet-Rich Plasma, Hyaluronic Acid, and Corticosteroid Injections on Temporomandibular Joint Osteoarthritis. J. Craniofacial Surg. 2019, 30, 1144–1148. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, G. Biological interactions of dental cast alloys with oral tissues. Dent. Mater. 2002, 18, 396–406. [Google Scholar] [CrossRef]
- Chung, C.; Burdick, J.A. Influence of Three-Dimensional Hyaluronic Acid Microenvironments on Mesenchymal Stem Cell Chondrogenesis. Tissue Eng. Part A 2009, 15, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.-K.; Ding, S.-J. Acid-resistant calcium silicate-based composite implants with high-strength as load-bearing bone graft substitutes and fracture fixation devices. J. Mech. Behav. Biomed. Mater. 2016, 62, 366–383. [Google Scholar] [CrossRef]
- Lett, A.; Sundareswari, M.; Ravichandran, K.; Latha, B.; Sagadevan, S. Fabrication and characterization of porous scaffolds for bone replacements using gum tragacanth. Mater. Sci. Eng. C 2018, 96, 487–495. [Google Scholar] [CrossRef]
- Lett, J.A.; Sagadevan, S.; Fatimah, I.; Hoque, E.; Lokanathan, Y.; Léonard, E.; Alshahateet, S.F.; Schirhagl, R.; Oh, W.C. Recent advances in natural polymer-based hydroxyapatite scaffolds: Properties and applications. Eur. Polym. J. 2021, 148, 110360. [Google Scholar] [CrossRef]
- Rokaya, D.; Srimaneepong, V.; Sapkota, J.; Qin, J.; Siraleartmukul, K.; Siriwongrungson, V. Polymeric materials and films in dentistry: An overview. J. Adv. Res. 2018, 14, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Sankar, V.; Hearnden, V.; Hull, K.; Juras, D.V.; Greenberg, M.S.; Kerr, A.R.; Lockhart, P.B.; Patton, L.; Porter, S.; Thornhill, M. Local drug delivery for oral mucosal diseases: Challenges and opportunities. Oral Dis. 2011, 17, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Wieckiewicz, M.; Boening, K.W.; Grychowska, N.; Paradowska-Stolarz, A. Clinical Application of Chitosan in Dental Specialities. Mini-Rev. Med. Chem. 2017, 17, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Nayef, L.; Mekhail, M.; Benameur, L.; Rendon, J.S.; Hamdy, R.; Tabrizian, M. A combinatorial approach towards achieving an injectable, self-contained, phosphate-releasing scaffold for promoting biomineralization in critical size bone defects. Acta Biomater. 2016, 29, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Junka, A.; Bartoszewicz, M.; Dziadas, M.; Szymczyk, P.; Dydak, K.; Żywicka, A.; Owczarek, A.; Bil-Lula, I.; Czajkowska, J.; Fijałkowski, K. Application of bacterial cellulose experimental dressings saturated with gentamycin for management of bone biofilm in vitro and ex vivo. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 108, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Karolewicz, B. A review of polymers as multifunctional excipients in drug dosage form technology. Saudi Pharm. J. 2015, 24, 525–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deirram, N.; Zhang, C.; Kermaniyan, S.S.; Johnston, A.P.R.; Such, G.K. pH-Responsive Polymer Nanoparticles for Drug Delivery. Macromol. Rapid Commun. 2019, 40, e1800917. [Google Scholar] [CrossRef] [Green Version]
- Timur, S.S.; Yüksel, S.; Akca, G.; Şenel, S. Localized drug delivery with mono and bilayered mucoadhesive films and wafers for oral mucosal infections. Int. J. Pharm. 2019, 559, 102–112. [Google Scholar] [CrossRef]
- Joshi, D.; Garg, T.; Goyal, A.K.; Rath, G. Advanced drug delivery approaches against periodontitis. Drug Deliv. 2014, 23, 363–377. [Google Scholar] [CrossRef]
- Gómez-Guillén, M.C.; Montero, M.P. Enhancement of oral bioavailability of natural compounds and probiotics by mucoadhesive tailored biopolymer-based nanoparticles: A review. Food Hydrocoll. 2021, 118, 106772. [Google Scholar] [CrossRef]
- Garg, T.; Rath, G.; Goyal, A.K. Comprehensive review on additives of topical dosage forms for drug delivery. Drug Deliv. 2014, 22, 969–987. [Google Scholar] [CrossRef] [Green Version]
- Garg, T.; Singh, S.; Goyal, A.K. Stimuli-sensitive hydrogels: An excellent carrier for drug and cell delivery. Crit. Rev. Ther. Drug Carr. Syst. 2013, 30, 369–409. [Google Scholar] [CrossRef] [PubMed]
- Ji, Q.X.; Zhao, Q.S.; Deng, J.; Lu, R. A novel injectable chlorhexidine thermosensitive hydrogel for periodontal application: Preparation, antibacterial activity and toxicity evaluation. J. Mater. Sci. Mater. Electron. 2010, 21, 2435–2442. [Google Scholar] [CrossRef] [PubMed]
- Swain, G.P.; Patel, S.; Gandhi, J.; Shah, P. Development of Moxifloxacin Hydrochloride loaded in-situ gel for the treatment of periodontitis: In-vitro drug release study and antibacterial activity. J. Oral Biol. Craniofacial Res. 2019, 9, 190–200. [Google Scholar] [CrossRef]
- Hirata, A.N.; Bruschi, M.L. Development and Characterisation of Semisolid Systems to Deliver Propolis in the Oral Cavity. Rev. Ciênc. Farm. Básica Apl. 2010, 31, 33–39. [Google Scholar]
- Tsirigotis-Maniecka, M.; Szyk-Warszyńska, L.; Lamch, Ł.; Weżgowiec, J.; Warszyński, P.; Wilk, K.A. Benefits of pH-responsive polyelectrolyte coatings for carboxymethyl cellulose-based microparticles in the controlled release of esculin. Mater. Sci. Eng. C 2020, 118, 111397. [Google Scholar] [CrossRef] [PubMed]
- Khan, G.; Yadav, S.K.; Patel, R.R.; Nath, G.; Bansal, M.; Mishra, B. Development and Evaluation of Biodegradable Chitosan Films of Metronidazole and Levofloxacin for the Management of Periodontitis. AAPS PharmSciTech 2015, 17, 1312–1325. [Google Scholar] [CrossRef] [Green Version]
- Kassem, A.; Issa, D.A.E.; Kotry, G.S.; Farid, R.M. Thiolated alginate-based multiple layer mucoadhesive films of metformin forintra-pocket local delivery: In vitro characterization and clinical assessment. Drug Dev. Ind. Pharm. 2016, 43, 120–131. [Google Scholar] [CrossRef] [PubMed]
- Tihan, G.T.; Ungureanu, C.; Barbaresso, R.C.; Zgârian, R.G.; Rau, I.; Meghea, A.; Albu, M.G.; Ghica, M.V. Chloramphenicol collagen sponges for local drug delivery in dentistry. C. R. Chim. 2015, 18, 986–992. [Google Scholar] [CrossRef]
- Chauhan, S.; Bansal, M.; Khan, G.; Yadav, S.K.; Singh, A.; Prakash, P.; Mishra, B. Development, optimization and evaluation of curcumin loaded biodegradable crosslinked gelatin film for the effective treatment of periodontitis. Drug Dev. Ind. Pharm. 2018, 44, 1212–1221. [Google Scholar] [CrossRef] [PubMed]
- Aduba, D.J.; Hammer, J.A.; Yuan, Q.; Yeudall, W.A.; Bowlin, G.L.; Yang, H. Semi-interpenetrating network (sIPN) gelatin nanofiber scaffolds for oral mucosal drug delivery. Acta Biomater. 2013, 9, 6576–6584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, S.; Hiorth, M.; Rykke, M.; Smistad, G. Polymer coated liposomes for dental drug delivery—Interactions with parotid saliva and dental enamel. Eur. J. Pharm. Sci. 2013, 50, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Kilicarslan, M.; Gumustas, M.; Yildiz, S.; Baykara, T. Preparation and characterization of chitosan-based spray-dried microparticles for the delivery of clindamycin phosphate to periodontal pockets. Curr. Drug Deliv. 2014, 11, 98–111. [Google Scholar] [CrossRef]
- Yang, S.-J.; Lin, C.-F.; Kuo, M.-L.; Tan, C.-T. Photodynamic Detection of Oral Cancers with High-Performance Chitosan-Based Nanoparticles. Biomacromolecules 2013, 14, 3183–3191. [Google Scholar] [CrossRef] [PubMed]
- Lamch, Ł.; Pucek, A.; Kulbacka, J.; Chudy, M.; Jastrzebska, E.; Tokarska, K.; Bułka, M.; Brzozka, Z.; Wilk, K.A. Recent progress in the engineering of multifunctional colloidal nanoparticles for enhanced photodynamic therapy and bioimaging. Adv. Colloid Interface Sci. 2018, 261, 62–81. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, J.; Lee, J.-Y.; Kang, D.S.; Anil, S.; Kim, S.-K.; Shim, M.S.; Kim, D.G. Antimicrobial and anticancer activities of porous chitosan-alginate biosynthesized silver nanoparticles. Int. J. Biol. Macromol. 2017, 98, 515–525. [Google Scholar] [CrossRef]
- Akıncıbay, H.; Şenel, S.; Ay, Z.Y. Application of chitosan gel in the treatment of chronic periodontitis. J. Biomed. Mater. Res. Part B Appl. Biomater. 2007, 80, 290–296. [Google Scholar] [CrossRef]
- Cid, Y.P.; Pedrazzi, V.; De Sousa, V.P.; Pierre, M.B.R. In Vitro Characterization of Chitosan Gels for Buccal Delivery of Celecoxib: Influence of a Penetration Enhancer. AAPS PharmSciTech 2011, 13, 101–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özdoğan, A.I.; İlarslan, Y.D.; Kösemehmetoğlu, K.; Akca, G.; Kutlu, H.B.; Comerdov, E.; Iskit, A.B.; Şenel, S. In vivo evaluation of chitosan based local delivery systems for atorvastatin in treatment of periodontitis. Int. J. Pharm. 2018, 550, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Pignatello, R.; Basile, L.; Puglisi, G. Chitosan glutamate hydrogels with local anesthetic activity for buccal application. Drug Deliv. 2009, 16, 176–181. [Google Scholar] [CrossRef]
- Ganguly, A.; Ian, C.K.; Sheshala, R.; Sahu, P.S.; Al-Waeli, H.; Meka, V.S. Application of diverse natural polymers in the design of oral gels for the treatment of periodontal diseases. J. Mater. Sci. Mater. Med. 2017, 28, 39. [Google Scholar] [CrossRef]
- Hasnain, S.; Rishishwar, P.; Ali, S.; Nayak, A.K. Preparation and evaluation of aceclofenac dental pastes using dillenia fruit gum for periodontitis treatment. SN Appl. Sci. 2020, 2, 425. [Google Scholar] [CrossRef] [Green Version]
- Mehta, C.J.; Shah, S.A.; Vijayakar, H.N.; Rodrigues, S.V.; Mitra, D.K.; Shah, R.A. To compare the effect of the local delivery of hyaluronan as an adjunct to scaling and root planing versus scaling and root planing alone in the treatment of chronic periodontitis. J. Indian Soc. Periodontol. 2016, 20, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Karoyo, A.; Wilson, L. A Review on the Design and Hydration Properties of Natural Polymer-Based Hydrogels. Materials 2021, 14, 1095. [Google Scholar] [CrossRef] [PubMed]
- Vasilyev, A.; Kuznetsova, V.; Bukharova, T.; Grigoriev, T.; Zagoskin, Y.; Korolenkova, M.; Zorina, O.; Chvalun, S.; Goldshtein, D.; Kulakov, A. Development prospects of curable osteoplastic materials in dentistry and maxillofacial surgery. Heliyon 2020, 6, e04686. [Google Scholar] [CrossRef]
- Skoskiewicz-Malinowska, K.; Kaczmarek, U.; Malicka, B.; Walczak, K.; Zietek, M. Application of chitosan and propolis in endodontic treatment: A review. Mini-Rev. Med. Chem. 2017, 17, 410–434. [Google Scholar] [CrossRef] [PubMed]
- Pradeep, G.; Raghu, R.; Shetty, A.; Gautham, P.; Puneetha, P.; Reddy, T.V.S. Retrievability of calcium hydroxide intracanal medicament with three calcium chelators, ethylenediaminetetraacetic acid, citric acid, and chitosan from root canals: An in vitro cone beam computed tomography volumetric analysis. J. Conserv. Dent. 2017, 20, 25–29. [Google Scholar] [CrossRef]
- Bukhari, S.N.A.; Roswandi, N.L.; Waqas, M.; Habib, H.; Hussain, F.; Khan, S.; Sohail, M.; Ramli, N.A.; Thu, H.E.; Hussain, Z. Hyaluronic acid, a promising skin rejuvenating biomedicine: A review of recent updates and pre-clinical and clinical investigations on cosmetic and nutricosmetic effects. Int. J. Biol. Macromol. 2018, 120, 1682–1695. [Google Scholar] [CrossRef] [PubMed]
- Müllner, M. Functional Natural and Synthetic Polymers. Macromol. Rapid Commun. 2019, 40, 1900151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coenen, A.M.; Bernaerts, K.; Harings, J.A.; Jockenhoevel, S.; Ghazanfari, S. Elastic materials for tissue engineering applications: Natural, synthetic, and hybrid polymers. Acta Biomater. 2018, 79, 60–82. [Google Scholar] [CrossRef]
- Iovene, A.; Zhao, Y.; Wang, S.; Amoako, K. Bioactive Polymeric Materials for the Advancement of Regenerative Medicine. J. Funct. Biomater. 2021, 12, 14. [Google Scholar] [CrossRef]
- Williams, D.F. On the mechanisms of biocompatibility. Biomaterials 2008, 29, 2941–2953. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, D.R.; Biswal, T. Alginate and its application to tissue engineering. SN Appl. Sci. 2021, 3, 30. [Google Scholar] [CrossRef]
- Cicciù, M.; Fiorillo, L.; Cervino, G. Chitosan Use in Dentistry: A Systematic Review of Recent Clinical Studies. Mar. Drugs 2019, 17, 417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seddiqi, H.; Oliaei, E.; Honarkar, H.; Jin, J.; Geonzon, L.C.; Bacabac, R.G.; Klein-Nulend, J. Cellulose and its derivatives: Towards biomedical applications. Cellulose 2021, 28, 1893–1931. [Google Scholar] [CrossRef]
- Al-Khateeb, R.; Olszewska-Czyz, I. Biological molecules in dental applications: Hyaluronic acid as a companion biomaterial for diverse dental applications. Heliyon 2020, 6, e03722. [Google Scholar] [CrossRef]
- Yazdi, M.K.; Taghizadeh, A.; Taghizadeh, M.; Stadler, F.J.; Farokhi, M.; Mottaghitalab, F.; Zarrintaj, P.; Ramsey, J.D.; Seidi, F.; Saeb, M.R.; et al. Agarose-based biomaterials for advanced drug delivery. J. Control. Release 2020, 326, 523–543. [Google Scholar] [CrossRef]
- Patino, M.G.; Neiders, M.E.; Andreana, S.; Noble, B.; Cohen, R.E. Collagen as an Implantable Material in Medicine and Dentistry. J. Oral Implant. 2002, 28, 220–225. [Google Scholar] [CrossRef]
- Friess, W. Collagen–biomaterial for drug delivery. Eur. J. Pharm Biopharm. 1998, 45, 113–136. [Google Scholar] [CrossRef]
- Bhowmik, S.; Islam, J.M.M.; Debnath, T.; Miah, M.Y.; Bhattacharjee, S.; Khan, M.A. Reinforcement of Gelatin-Based Nanofilled Polymer Biocomposite by Crystalline Cellulose from Cotton for Advanced Wound Dressing Applications. Polymers 2017, 9, 222. [Google Scholar] [CrossRef] [Green Version]
- Noori, A.; Ashrafi, S.J.; Vaez-Ghaemi, R.; Hatamian-Zaremi, A.; Webster, T.J. A review of fibrin and fibrin composites for bone tissue engineering. Int. J. Nanomed. 2017, 12, 4937–4961. [Google Scholar] [CrossRef] [Green Version]
- Soares, D.G.; Bordini, E.; Cassiano, F.; Bronze-Uhle, E.S.; Pacheco, L.E.; Zabeo, G.; Hebling, J.; Lisboa-Filho, P.N.; Bottino, M.C.; Costa, C.A.D.S. Characterization of novel calcium hydroxide-mediated highly porous chitosan-calcium scaffolds for potential application in dentin tissue engineering. J. Biomed. Mater. Res. Part B Appl. Biomater. 2020, 108, 2546–2559. [Google Scholar] [CrossRef]
- Maged, A.; Abdelkhalek, A.A.; Mahmoud, A.A.; Salah, S.; Ammar, M.M.; Ghorab, M.M. Mesenchymal stem cells associated with chitosan scaffolds loaded with rosuvastatin to improve wound healing. Eur. J. Pharm. Sci. 2018, 127, 185–198. [Google Scholar] [CrossRef]
- Zhang, B.; Gao, L.; Ma, L.; Luo, Y.; Yang, H.; Cui, Z. 3D Bioprinting: A Novel Avenue for Manufacturing Tissues and Organs. Engineering 2019, 5, 777–794. [Google Scholar] [CrossRef]
- Puertas-Bartolomé, M.; Mora-Boza, A.; García-Fernández, L. Emerging Biofabrication Techniques: A Review on Natural Polymers for Biomedical Applications. Polymers 2021, 13, 1209. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-De-Leyva, Á.; Linares, V.; Casas, M.; Caraballo, I. 3D Printed Drug Delivery Systems Based on Natural Products. Pharmaceutics 2020, 12, 620. [Google Scholar] [CrossRef]
- Liu, J.; Sun, L.; Xu, W.; Wang, Q.; Yu, S.; Sun, J. Current advances and future perspectives of 3D printing natural-derived biopolymers. Carbohydr. Polym. 2018, 207, 297–316. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Abdalla, A.M.; Xiao, L.; Yang, G. Biopolymer-Based Microcarriers for Three-Dimensional Cell Culture and Engineered Tissue Formation. Int. J. Mol. Sci. 2020, 21, 1895. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Chen, Q.; Liu, C.; Ao, Q.; Tian, X.; Fan, J.; Tong, H.; Wang, X. Natural Polymers for Organ 3D Bioprinting. Polymers 2018, 10, 1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoeini, R.; Nosrati, H.; Akbarzadeh, A.; Eftekhari, A.; Kavetskyy, T.; Khalilov, R.; Ahmadian, E.; Nasibova, A.; Datta, P.; Roshangar, L.; et al. Natural and Synthetic Bioinks for 3D Bioprinting. Adv. NanoBiomed Res. 2021, 1, 2000097. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Polymer | API | Effect | Ref. |
|---|---|---|---|
| chitosan and its derivatives | chlorhexidine | Antimicrobial, biodegradable and thermosensitive carrier, releasing chlorhexidine in a prolonged manner, potentially useful in the treatment of periodontal diseases. | [114] |
| metronidazole | The synergistic activity of the polymer and substances in the form of hydrogel, used in the treatment of chronic periodontitis. | [128] | |
| metronidazole and levofloxacin | Films based on cross-linked chitosan provide a long-term release of the substance for up to 7 days. Clinical trials confirmed the therapeutic efficacy of the films in reducing the clinical indicators of periodontitis, i.e., gingival index, plaque index and periodontal pocket depth. | [118] | |
| clindamycin phosphate | Microparticles for local drug delivery to the periodontal pocket for sustained release of the antimicrobial drug; promising in the treatment of periodontal diseases. | [124] | |
| celecoxib | Mucoadhesive chitosan gels with laurocapram as non-ionic surfactant considered as a potential system for buccal administration of celecoxib in the chemoprevention of oral cancer. | [129] | |
| 5-aminolevulinic acid (ALA) | Succinate-modified chitosan (SCHI) nanoparticles complexed with folic acid, forming nanostructures with high ALA incorporation efficiency and improving ALA release in cell lysosomes. The obtained nanoparticles are an excellent vector for the specific oral delivery of 5-ALA for the photodynamic detection of oral cavity cancer cells. | [125] | |
| atorvastatin | Chitosan-based mucoadhesive gels containing 2% atorvastatin were evaluated in periodontitis rats. There was a reduction in the release of the pro-inflammatory cytokines IL-1β, IL-6 and IL-8 and the anti-inflammatory cytokines TGF-β1 and TGF-β2, with significant healing of the alveolar bone, comparing to the control group. The anti-inflammatory effect was increased when atorvastatin was delivered using chitosan-based gel. The developed gels are potential carriers for substances from the group of statins in the treatment of periodontitis. | [130] | |
| lidocaine hydrochloride | The anesthetic effect of mucoadhesive hydrogels based on chitosan glutamate was evaluated in vivo after application to the buccal mucosa, in comparison with commercial semi-solid formulations containing lidocaine hydrochloride. The obtained mucoadhesive hydrogels may be useful in reducing pain symptoms in aphthosis and other painful lesions of the oral mucosa. | [131] | |
| gellan gum | moxifloxacin hydrochloride | In situ gelling carriers were prepared based on ion-sensitive gellan gum and temperature-sensitive Poloxamer 407, finally to obtain prolonged retention at the application site. The optimized formulation with 19.072% Poloxamer 407 and 0.245% gellan gum has shown appropriate properties as an in situ carrier for drug delivery in dental application. | [115] |
| karaya gum/badam gum | moxifloxacin hydrochloride | Gels based on natural polymers (karaya gum (1, 2, 3%), badam gum (1, 2, 3%) and chitosan) with moxifloxacin hydrochloride showed potential for their application in the treatment of periodontitis. | [132] |
| gum extracted from ripe dillenia fruit | aceclofenac | Toothpastes containing 1% aceclofenac and dillenia fruit gum had beneficial rheological properties for better extrusion from the tube and spread. The in vitro release of aceclofenac from dental pastes was sustained for 6 hours. The pastes showed excellent mucoadhesion to the mucosa of porcine cheek, which may be beneficial for applications in the treatment of pain and periodontitis. | [133] |
| hyaluronic acid | - | Gels containing 0.8% hyaluronic acid were proposed for subgingival application as an adjunct for scaling and root planing (SRP) in the treatment of generalized chronic periodontitis. The statistically significant reduction in periodontal pocket depth, as well as the increase in the relative attachment level (RAL), were observed when compared to the control group. | [134] |
| pectin | - | Pectin-coated liposomes were described as promising oral drug carriers, able to adsorb onto hydroxyapatite as a model substance for human tooth enamel. | [123] |
| alginate/derivatives | metformin hydrochloride | Mucoadhesive multilayer film containing metformin hydrochloride with osteogenic activity was developed for intrapocket application in the treatment of periodontitis. The inner layer containing the drug was formed by carboxymethyl cellulose sodium salt (CMC) or sodium alginate. Thiolated sodium alginate (TSA) (2 or 4%) was the drug-free outer layer used to increase mucoadhesion and to achieve controlled release of the substance. A film based on CMC in the outer layer with 4% TSA with enhanced mucoadhesion and in vitro controlled drug release (83.73% within 12 h) was clinically evaluated in 20 patients. Clinical trials revealed improvement in all clinical parameters after six months of treatment, suggesting that the local use of mucoadhesive multilayer films with metformin hydrochloride may become an effective treatment method for moderate chronic periodontitis. | [119] |
| gelatin | ethanolic propolis extract | Formulations based on 1% gelatin revealed thermosensitive properties (Tsol/gel), appropriate for the oral mucosa application. Modified kinetics of in vitro release of substances from gelling formulations, inconsistent with Fick’s law of diffusion, was achieved. | [116] |
| nystatin | Gelatin-based electrospun nanofibrous scaffolds for sustained drug release in the mouth were prepared. To improve the structural stability of the scaffolds and to enable the non-invasive incorporation of substances, photoreactive polyethylene glycol diacrylate was used as a cross-linking agent stabilizing by forming semi-interpenetrating network gelatin nanofiber scaffolds. The cross-linked structures effectively increased the structural stability of the obtained nystatin scaffold with statin in aqueous solutions. | [122] | |
| curcumin | The cross-linked gelatin film released the substance in vitro over a period of up to 7 days. The carrier may be potentially used for topical drug delivery to periodontal pockets. | [121] | |
| collagen | chloramphenicol | Collagen sponges cross-linked with glutaraldehyde with chloramphenicol showed resistance to degradation by collagenase and strong antibacterial activity. Considering requirements for oral cavity drug carriers, i.e., low water absorption, slow drug release, high drug loading, high antimicrobial activity and resistance to enzymatic activity, optimal properties were obtained for 0.5% glutaraldehyde content in a sponge. The properties of the obtained formulations showed that sponges may be useful in the treatment and/or prevention of infected oral cavity lesions. | [120] |
| Polymer | Disadvantages and Risk of Use as a Drug Carrier | Reference |
|---|---|---|
| Generally |
| [143] |
| Alginate derivatives |
| [144] |
| Chitosan and its derivatives |
| [145] |
| Cellulose derivatives |
| [146] |
| Hyaluronic acid |
| [147] |
| Agarose |
| [148] |
| Collagen |
| [149,150] |
| Gelatin |
| [151] |
| Fibrin |
| [152] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paradowska-Stolarz, A.; Wieckiewicz, M.; Owczarek, A.; Wezgowiec, J. Natural Polymers for the Maintenance of Oral Health: Review of Recent Advances and Perspectives. Int. J. Mol. Sci. 2021, 22, 10337. https://doi.org/10.3390/ijms221910337
Paradowska-Stolarz A, Wieckiewicz M, Owczarek A, Wezgowiec J. Natural Polymers for the Maintenance of Oral Health: Review of Recent Advances and Perspectives. International Journal of Molecular Sciences. 2021; 22(19):10337. https://doi.org/10.3390/ijms221910337
Chicago/Turabian StyleParadowska-Stolarz, Anna, Mieszko Wieckiewicz, Artur Owczarek, and Joanna Wezgowiec. 2021. "Natural Polymers for the Maintenance of Oral Health: Review of Recent Advances and Perspectives" International Journal of Molecular Sciences 22, no. 19: 10337. https://doi.org/10.3390/ijms221910337