
Deferoxamine Reduces Inflammation and Osteoclastogenesis in Avulsed Teeth

 , , , and
, , , and 
Abstract
:1. Introduction
2. Results
2.1. Cell Viability and Anti-Inflammatory Effect of DFO in RAW264.7 Cells
2.2. DFO Affects Osteoclast Differentiation in RAW264.7 Cells
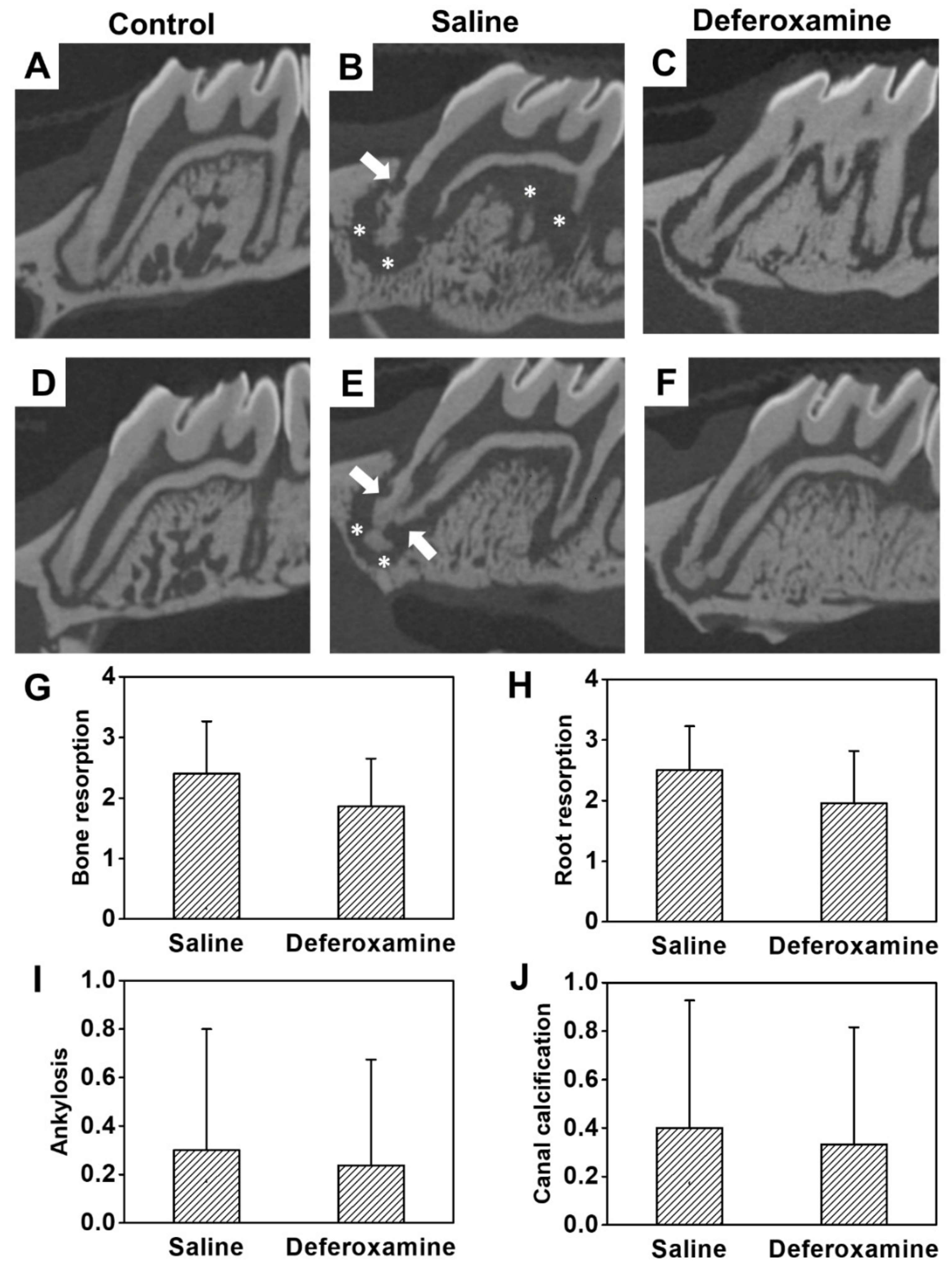
2.3. Anti-Inflammation and Reduced Bone Loss in Replanted Rat First Molars
3. Discussion
4. Materials and Methods
4.1. Cell Culture
4.2. Cell Viability Assay
4.3. Nitric Oxide Assay
4.4. In Vitro Osteoclastogenesis Assays
4.5. Tartrate-Resistant Acid Phosphatase (TRAP) Staining
4.6. ROS Assessment
4.7. Quantitative Real-Time Polymerase Chain Reaction
4.8. Rat Models
4.8.1. Replantation Procedure in Rat Maxillary First Molar
4.8.2. Micro-Computed Tomography Image Analysis and Histological Analysis
4.8.3. Histological Analysis
4.9. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Day, P.F.; Gregg, T.A.; Ashley, P.; Welbury, R.R.; Cole, B.O.; High, A.S.; Duggal, M.S. Periodontal healing following avulsion and replantation of teeth: A multi-centre randomized controlled trial to compare two root canal medicaments. Dent. Traumatol. 2012, 28, 55–64. [Google Scholar] [CrossRef]
- Poi, W.R.; Sonoda, C.K.; Martins, C.M.; Melo, M.E.; Pellizzer, E.P.; de Mendonça, M.R.; Panzarini, S.R. Storage media for avulsed teeth: A literature review. Braz. Dent. J. 2013, 24, 437–445. [Google Scholar] [CrossRef]
- Panzarini, S.R.; Gulinelli, J.L.; Poi, W.R.; Sonoda, C.K.; Pedrini, D.; Brandini, D.A. Treatment of root surface in delayed tooth replantation: A review of literature. Dent. Traumatol. 2008, 24, 277–282. [Google Scholar] [CrossRef]
- Trope, M. Clinical management of the avulsed tooth: Present strategies and future directions. Dent. Traumatol. 2002, 18, 1–11. [Google Scholar] [CrossRef]
- Sigalas, E.; Regan, J.D.; Kramer, P.R.; Witherspoon, D.E.; Opperman, L.A. Survival of human periodontal ligament cells in media proposed for transport of avulsed teeth. Dent. Traumatol. 2004, 20, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, S.K.; Sidhu, S.S. Effect of fluoride on root resorption of autogenous dental replants. Clinical study. Aust. Dent. J. 1981, 26, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Lustosa-Pereira, A.; Garcia, R.B.; de Moraes, I.G.; Bernardineli, N.; Bramante, C.M.; Bortoluzzi, E.A. Evaluation of the topical effect of alendronate on the root surface of extracted and replanted teeth. Microscopic analysis on rats’ teeth. Dent. Traumatol. 2006, 22, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Poi, W.R.; Carvalho, R.M.; Panzarini, S.R.; Sonoda, C.K.; Manfrin, T.M.; Rodrigues Tda, S. Influence of enamel matrix derivative (emdogain) and sodium fluoride on the healing process in delayed tooth replantation: Histologic and histometric analysis in rats. Dent. Traumatol. 2007, 23, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Ballas, S.K.; Zeidan, A.M.; Duong, V.H.; DeVeaux, M.; Heeney, M.M. The effect of iron chelation therapy on overall survival in sickle cell disease and β-thalassemia: A systematic review. Am. J. Hematol. 2018, 93, 943–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujisawa, K.; Takami, T.; Okada, S.; Hara, K.; Matsumoto, T.; Yamamoto, N.; Yamasaki, T.; Sakaida, I. Analysis of metabolomic changes in mesenchymal stem cells on treatment with desferrioxamine as a hypoxia mimetic compared with hypoxic conditions. Stem. Cells 2018, 36, 1226–1236. [Google Scholar] [CrossRef] [Green Version]
- Holden, P.; Nair, L.S. Deferoxamine: An angiogenic and antioxidant molecule for tissue regeneration. Tissue Eng. Part B Rev. 2019, 25, 461–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, J.H.; Kim, Y.S.; Noh, K.; Lee, Y.M.; Chang, S.W.; Kim, E.C. Deferoxamine promotes osteoblastic differentiation in human periodontal ligament cells via the nuclear factor erythroid 2-related factor-mediated antioxidant signaling pathway. J. Periodontal. Res. 2014, 49, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Mu, S.; Guo, S.; Wang, X.; Zhan, Y.; Li, Y.; Jiang, Y.; Zhang, R.; Zhang, B. Effects of deferoxamine on the osteogenic differentiation of human periodontal ligament cells. Mol. Med. Rep. 2017, 16, 9579–9586. [Google Scholar] [CrossRef]
- Wang, X.; Wu, T.T.; Jiang, L.; Rong, D.; Zhu, Y.Q. Deferoxamine-induced migration and odontoblast differentiation via ros-dependent autophagy in dental pulp stem cells. Cell. Physiol. Biochem. 2017, 43, 2535–2547. [Google Scholar] [CrossRef] [Green Version]
- Jiang, L.; Peng, W.W.; Li, L.F.; Du, R.; Wu, T.T.; Zhou, Z.J.; Zhao, J.J.; Yang, Y.; Qu, D.L.; Zhu, Y.Q. Effects of deferoxamine on the repair ability of dental pulp cells in vitro. J. Endod. 2014, 40, 1100–1104. [Google Scholar] [CrossRef]
- Foyer, C.H. Reactive oxygen species, oxidative signaling and the regulation of photosynthesis. Environ. Exp. Bot. 2018, 154, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Park, E.; Chung, S.W. Ros-mediated autophagy increases intracellular iron levels and ferroptosis by ferritin and transferrin receptor regulation. Cell Death Dis. 2019, 10, 822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tao, H.; Ge, G.; Liang, X.; Zhang, W.; Sun, H.; Li, M.; Geng, D. Ros signaling cascades: Dual regulations for osteoclast and osteoblast. Acta Biochim. Biophys. Sin. 2020, 52, 1055–1062. [Google Scholar] [CrossRef]
- Shen, P.; Huang, Y.; Ba, X.; Lin, W.; Qin, K.; Wang, H.; Du, M.; Haung, Y.; Wang, Y.; Chen, Z.; et al. Si miao san attenuates inflammation and oxidative stress in rats with cia via the modulation of the nrf2/are/pten pathway. Evid. Based Complement. Alternat. Med. 2021, 2021, 2843623. [Google Scholar] [CrossRef] [PubMed]
- Phull, A.R.; Nasir, B.; Haq, I.U.; Kim, S.J. Oxidative stress, consequences and ros mediated cellular signaling in rheumatoid arthritis. Chem. Biol. Interact. 2018, 281, 121–136. [Google Scholar] [CrossRef] [PubMed]
- Schröder, K. Nadph oxidases in bone homeostasis and osteoporosis. Free Radic. Biol. Med. 2019, 132, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Malkovskiy, A.V.; Tian, W.; Sung, Y.K.; Sun, W.; Hsu, J.L.; Manickam, S.; Wagh, D.; Joubert, L.-M.; Semenza, G.L. Promotion of airway anastomotic microvascular regeneration and alleviation of airway ischemia by deferoxamine nanoparticles. Biomaterials 2014, 35, 803–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temraz, S.; Santini, V.; Musallam, K.; Taher, A. Iron overload and chelation therapy in myelodysplastic syndromes. Crit. Rev. Oncol. Hematol. 2014, 91, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Nolan, G.P.; Ghosh, S.; Liou, H.C.; Tempst, P.; Baltimore, D. DNA binding and i kappa b inhibition of the cloned p65 subunit of nf-kappa b, a rel-related polypeptide. Cell 1991, 64, 961–969. [Google Scholar] [CrossRef]
- Kong, X.; Wang, R.; Xue, Y.; Liu, X.; Zhang, H.; Chen, Y.; Fang, F.; Chang, Y. Sirtuin 3, a new target of pgc-1alpha, plays an important role in the suppression of ros and mitochondrial biogenesis. PLoS ONE 2010, 5, e11707. [Google Scholar] [CrossRef] [Green Version]
- Pohl, Y.; Filippi, A.; Kirschner, H. Results after replantation of avulsed permanent teeth. Ii. Periodontal healing and the role of physiologic storage and antiresorptive-regenerative therapy. Dent. Traumatol. 2005, 21, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.Y.; Cao, J.B.; Zhang, L.M.; Li, Y.F.; Mi, W.D. Deferoxamine attenuates lipopolysaccharide-induced neuroinflammation and memory impairment in mice. J. Neuroinflammation 2015, 12, 20. [Google Scholar] [CrossRef] [Green Version]
- Hershko, C.; Konijn, A.M.; Nick, H.P.; Breuer, W.; Cabantchik, Z.I.; Link, G. Icl670a: A new synthetic oral chelator: Evaluation in hypertransfused rats with selective radioiron probes of hepatocellular and reticuloendothelial iron stores and in iron-loaded rat heart cells in culture. Blood 2001, 97, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Bajbouj, K.; Shafarin, J.; Hamad, M. High-dose deferoxamine treatment disrupts intracellular iron homeostasis, reduces growth, and induces apoptosis in metastatic and nonmetastatic breast cancer cell lines. Technol. Cancer Res. Treat. 2018, 17, 1533033818764470. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.J.; Wei, H.; Frei, B. The iron chelator, desferrioxamine, reduces inflammation and atherosclerotic lesion development in experimental mice. Exp. Biol. Med. 2010, 235, 633–641. [Google Scholar] [CrossRef] [Green Version]
- Müller, D.D.; Bissinger, R.; Reymus, M.; Bücher, K.; Hickel, R.; Kühnisch, J. Survival and complication analyses of avulsed and replanted permanent teeth. Sci. Rep. 2020, 10, 2841. [Google Scholar] [CrossRef] [Green Version]
- Gowen, M.; Wood, D.D.; Ihrie, E.J.; McGuire, M.K.; Russell, R.G. An interleukin 1 like factor stimulates bone resorption in vitro. Nature 1983, 306, 378–380. [Google Scholar] [CrossRef]
- Pfeilschifter, J.; Chenu, C.; Bird, A.; Mundy, G.R.; Roodman, G.D. Interleukin-1 and tumor necrosis factor stimulate the formation of human osteoclastlike cells in vitro. J. Bone Miner. Res. 1989, 4, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Yang, H.; Shi, Q. Macrophages and bone inflammation. J. Orthop. Translat. 2017, 10, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Levin, L.; Bryson, E.C.; Caplan, D.; Trope, M. Effect of topical alendronate on root resorption of dried replanted dog teeth. Dent. Traumatol. 2001, 17, 120–126. [Google Scholar] [CrossRef]
- van’t Hof, R.J.; Armour, K.J.; Smith, L.M.; Armour, K.E.; Wei, X.Q.; Liew, F.Y.; Ralston, S.H. Requirement of the inducible nitric oxide synthase pathway for il-1-induced osteoclastic bone resorption. Proc. Natl. Acad. Sci. USA 2000, 97, 7993–7998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.H.; Lee, N.K.; Lee, S.Y. Current understanding of rank signaling in osteoclast differentiation and maturation. Mol. Cells 2017, 40, 706–713. [Google Scholar] [PubMed] [Green Version]
- Feng, X.; Teitelbaum, S.L. Osteoclasts: New insights. Bone Res. 2013, 1, 11–26. [Google Scholar] [PubMed] [Green Version]
- Zhang, J.; Hu, W.; Ding, C.; Yao, G.; Zhao, H.; Wu, S. Deferoxamine inhibits iron-uptake stimulated osteoclast differentiation by suppressing electron transport chain and mapks signaling. Toxicol. Lett. 2019, 313, 50–59. [Google Scholar] [CrossRef]
- Hatcher, H.C.; Singh, R.N.; Torti, F.M.; Torti, S.V. Synthetic and natural iron chelators: Therapeutic potential and clinical use. Future Med. Chem. 2009, 1, 1643–1670. [Google Scholar] [CrossRef] [Green Version]
- Agidigbi, T.S.; Kim, C. Reactive oxygen species in osteoclast differentiation and possible pharmaceutical targets of ros-mediated osteoclast diseases. Int. J. Mol. Sci. 2019, 20, 3576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, H.; Ward, W.F. Pgc-1alpha: A key regulator of energy metabolism. Adv. Physiol. Educ. 2006, 30, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Xu, J.; Lazarovici, P.; Quirion, R.; Zheng, W. Camp response element-binding protein (creb): A possible signaling molecule link in the pathophysiology of schizophrenia. Front. Mol. Neurosci. 2018, 11, 255. [Google Scholar] [CrossRef] [PubMed]
- Araujo, J.A.; Zhang, M.; Yin, F. Heme oxygenase-1, oxidation, inflammation, and atherosclerosis. Front. Pharmacol. 2012, 3, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwerina, J.; Tzima, S.; Hayer, S.; Redlich, K.; Hoffmann, O.; Hanslik-Schnabel, B.; Smolen, J.S.; Kollias, G.; Schett, G. Heme oxygenase 1 (ho-1) regulates osteoclastogenesis and bone resorption. FASEB J. 2005, 19, 2011–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.C.; Lii, C.K.; Wei, Y.L.; Li, C.C.; Lu, C.Y.; Liu, K.L.; Chen, H.W. Docosahexaenoic acid inhibition of inflammation is partially via cross-talk between nrf2/heme oxygenase 1 and ikk/nf-κb pathways. J. Nutr. Biochem. 2013, 24, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Poi, W.R.; Sonoda, C.K.; Amaral, M.F.; Queiroz, A.F.; França, A.B.; Brandini, D.A. Histological evaluation of the repair process of replanted rat teeth after storage in resveratrol dissolved in dimethyl sulphoxide. Dent. Traumatol. 2018, 34, 254–263. [Google Scholar] [CrossRef]
- Kang, C.M.; Mo, S.; Jeon, M.; Jung, U.W.; Shin, Y.; Shin, J.S.; Shin, B.Y.; Lee, S.K.; Choi, H.J.; Song, J.S. Intranuclear delivery of nuclear factor-kappa b p65 in a rat model of tooth replantation. Int. J. Mol. Sci 2021, 22, 1987. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Forward Primer Sequence (5′–3′) | Reverse Primer Sequence (5′–3′) |
|---|---|---|
| CTSK | GGGATGTTGGCGATGCA | CCAGCTACTTGAGGTCCATCTTC |
| CREB1 | TGTACCACCGGTATCCATGC | TGGATAACGCCATGGACCTG |
| GAPDH | CTGGCACAGGGTATACAGGGTTAG | ACTGGTGCCGTTTATGCCTTG |
| HIF1a | AGCTTGCTCATCAGTTGCCA | CCAGAAGTTTCCTCACACGC |
| HO-1 | GAAATCATCCCTTGCACGCC | CCTGAGAGGTCACCCAGGTA |
| IL 1β | GTTCCCCAACTGGTACATCA | CCATACTTTAGGAAGACACGG |
| IL 6 | GTTGCCTTCTTGGGACTGATG | ATCAGAATTGCCATTGCACAA |
| NFATc1 | CACTGGCGCTGCAACAAGA | CATTCCGGAGCTCAGCAGAATAA |
| Nrf-2 | TGAAGCTCAGCTCGCATTGA | TGCTCCAGCTCGACAATGTT |
| PGC-1β | CTCTGACACGCAGGGTGG | AGTCAAAGTCACTGGCGTCC |
| RelA | CTCCTGAACCAGGGTGTGTC | GAGAGACCATTGGGAAGCCC |
| TRAF6 | CTACCCGCTTTGACATGGGT | CACCTCTCCCACTGCTTGTT |
| TRAP | CAAAGGTGCAGCCTTTGTGTC | TCACAGTCCGGATTGAGCTCA |
| VEGF | TCCGAAACCATGAACTTTCTGC | AGCTTCGCTGGTAGACATCC |
| ACTB | TCACCATGGATGATGATATCGC | GGAATCCTTCTGACCCATGC |
| Characterization | Score |
|---|---|
| A. Bone resorption | |
| No resorption present | 0 |
| Resorption occurred in <1/3 of the bone surface | 1 |
| Resorption occurred in >1/3 and <2/3 of the bone surface | 2 |
| Resorption occurred in >2/3 of the bone surface | 3 |
| B. Root resorption | |
| No resorption present | 0 |
| Resorption occurred in <1/3 of the bone surface | 1 |
| Resorption occurred in >1/3 and <2/3 of the bone surface | 2 |
| Resorption occurred in >2/3 of the bone surface | 3 |
| C. Ankylosis (direct fusion of bone to root) | |
| Absence | 0 |
| Presence | 1 |
| D. Canal calcification | |
| Absence | 0 |
| Presence | 1 |
| Characterization | Score |
|---|---|
| A. Bone resorption | |
| No resorption present | 0 |
| Resorption occurred in <1/3 of the bone surface | 1 |
| Resorption occurred in >1/3 and <2/3 of the bone surface | 2 |
| Resorption occurred in >2/3 of the bone surface | 3 |
| B. Root resorption | |
| No resorption present | 0 |
| Resorption occurred in <1/3 of the bone surface | 1 |
| Resorption occurred in >1/3 and <2/3 of the bone surface | 2 |
| Resorption occurred in >2/3 of the bone surface | 3 |
| C. Inflammation at the epithelial insertion | |
| Absence or occasional presence of inflammatory cells | 0 |
| Inflammatory process restricted to the lamina propria of the internal part of the epithelium | 1 |
| Inflammatory process extending apically to the small portion of the connective tissue underlying the lamina propria of the internal portion of the gingival epithelium | 2 |
| Inflammatory process reaching the proximity of the alveolar bone crest | 3 |
| D. Inflammation in the periodontal ligament | |
| Absence or occasional presence of inflammatory cells | 0 |
| Inflammatory process presents only in the apical, coronal, or small lateral area of the PDL | 1 |
| Inflammatory process reaching more than half of the lateral PDL of the root | 2 |
| Inflammatory process in the whole PDL | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.E.; Mo, S.; Lee, H.-S.; Jeon, M.; Song, J.S.; Choi, H.-J.; Cho, H.; Kang, C.-M. Deferoxamine Reduces Inflammation and Osteoclastogenesis in Avulsed Teeth. Int. J. Mol. Sci. 2021, 22, 8225. https://doi.org/10.3390/ijms22158225
Lee KE, Mo S, Lee H-S, Jeon M, Song JS, Choi H-J, Cho H, Kang C-M. Deferoxamine Reduces Inflammation and Osteoclastogenesis in Avulsed Teeth. International Journal of Molecular Sciences. 2021; 22(15):8225. https://doi.org/10.3390/ijms22158225
Chicago/Turabian StyleLee, Ko Eun, Seunghan Mo, Hyo-Seol Lee, Mijeong Jeon, Je Seon Song, Hyung-Jun Choi, Hyunsoo Cho, and Chung-Min Kang. 2021. "Deferoxamine Reduces Inflammation and Osteoclastogenesis in Avulsed Teeth" International Journal of Molecular Sciences 22, no. 15: 8225. https://doi.org/10.3390/ijms22158225