Pharmacogenomics of Cognitive Dysfunction and Neuropsychiatric Disorders in Dementia


Abstract
:1. Introduction
2. The Pharmacogenomic Machinery
3. CNS Drugs
4. Pharmacogenomics of Cognition
4.1. Donepezil
4.2. Galantamine
4.3. Rivastigmine
4.4. Memantine
4.5. Multifactorial Treatments
5. Pharmacogenomics of Neuropsychiatric Disorders
5.1. Psychotic Disorders
5.2. Depressive Disorders
5.3. Anxiety Disorders
5.4. Sleep Disorders
5.5. Epilepsy
6. Conclusions
7. Further Considerations
Funding
Acknowledgments
Conflicts of Interest
References
- Cacabelos, R.; Fernández-Novoa, L.; Lombardi, V.; Kubota, Y.; Takeda, M. Molecular genetics of Alzheimer’s disease and aging. Methods Find. Exp. Clin. Pharmacol. 2005, 27, 1–573. [Google Scholar]
- Cacabelos, R. Pharmacogenomics in Alzheimer’s disease. Methods Mol. Biol. 2008, 448, 213–357. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Cacabelos, P.; Torrellas, C.; Tellado, I.; Carril, J.C. Pharmacogenomics of Alzheimer’s disease: Novel therapeutic strategies for drug development. Methods Mol. Biol. 2014, 1175, 323–556. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Carril, J.C.; Cacabelos, P.; Teijido, O.; Goldgaber, D. Pharmacogenomics of Alzheimer’s Disease: Genetic determinants of phenotypic variation and therapeutic outcome. J. Genom. Med. Pharmacogenom. 2016, 1, 151–209. [Google Scholar]
- Cacabelos, R.; Carril, J.C.; Cacabelos, N.; Kazantsev, A.G.; Vostrov, A.V.; Corzo, L.; Cacabelos, P.; Goldgaber, D. Sirtuins in Alzheimer’s Disease: SIRT2-Related GenoPhenotypes and Implications for PharmacoEpiGenetics. Int. J. Mol. Sci. 2019, 20, 1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arvanitakis, Z.; Shah, R.C.; Bennett, D.A. Diagnosis and Management of Dementia: Review. JAMA 2019, 322, 1589–1599. [Google Scholar] [CrossRef]
- Cacabelos, R. Have there been improvement in Alzheimer’s disease drug discovery over the past 5 years? Expert Opin. Drug Discov. 2018, 13, 523–538. [Google Scholar] [CrossRef]
- Volicer, L. Behavioral Problems and Dementia. Clin. Geriatr. Med. 2018, 34, 637–651. [Google Scholar] [CrossRef] [PubMed]
- Defrancesco, M.; Marksteiner, J.; Kemmler, G.; Dal-Bianco, P.; Ransmayr, G.; Benke, T.; Mosbacher, J.; Holler, Y.; Schmidt, R. Specific Neuropsychiatric Symptoms Are Associated with Faster Progression in Alzheimer’s Disease: Results of the Prospective Dementia Registry (PRODEM-Austria). J. Alzheimers Dis. 2020, 73, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Sr, P.A.A.; DeFeis, B.; De Wit, L.; O’Shea, D.; Mejia, A.; Chandler, M.; Locke, D.E.C.; Fields, J.; Phatak, V.; Dean, P.M.; et al. Functional ability is associated with higher adherence to behavioral interventions in mild cognitive impairment. Clin. Neuropsychol. 2019, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilik, F.; Büyükgöl, H.; Kayhan, F.; Ertem, D.H.; Ekiz, T. Effects of Inappropriate Sexual Behaviors and Neuropsychiatric Symptoms of Patients with Alzheimer Disease and Caregivers’ Depression on Caregiver Burden. J. Geriatr. Psychiatry Neurol. 2019. 891988719874123. [Google Scholar] [CrossRef] [PubMed]
- Burhanullah, M.H.; Tschanz, J.T.; Peters, M.E.; Leoutsakos, J.M.; Matyi, J.; Lyketsos, C.G.; Nowrangi, M.A.; Rosenberg, P.B. Neuropsychiatric Symptoms as Risk Factors for Cognitive Decline in Clinically Normal Older Adults: The Cache County Study. Am. J. Geriatr. Psychiatry 2020, 28, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Lai, A.X.; Kaup, A.R.; Yaffe, K.; Byers, A.L. High Occurrence of Psychiatric Disorders and Suicidal Behavior Across Dementia Subtypes. Am. J. Geriatr. Psychiatry 2018, 26, 1191–1201. [Google Scholar] [CrossRef]
- Cummings, J.; Lai, T.J.; Hemrungrojn, S.; Mohandas, E.; Yun Kim, S.; Nair, G.; Dash, A. Role of Donepezil in the Management of Neuropsychiatric Symptoms in Alzheimer’s Disease and Dementia with Lewy Bodies. CNS Neurosci. Ther. 2016, 22, 159–166. [Google Scholar] [CrossRef]
- Deardorff, W.J.; Grossberg, G.T. Behavioral and psychological symptoms in Alzheimer’s dementia and vascular dementia. Handb. Clin. Neurol. 2019, 165, 5–32. [Google Scholar] [CrossRef] [PubMed]
- van de Beek, M.; van Steenoven, I.; Ramakers, I.H.G.B.; Aalten, P.; Koek, H.L.; Olde Rikkert, M.G.M.; Mannien, J.; de Jong, F.J.; Lemstra, A.W.; van der Flier, W.M. Trajectories and Determinants of Quality of Life in Dementia with Lewy Bodies and Alzheimer’s Disease. J. Alzheimers Dis. 2019, 70, 389–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Wilson, L.; Kornak, J.; Dudley, R.A.; Merrilees, J.; Bonasera, S.J.; Byrne, C.M.; Lee, K.; Chiong, W.; Miller, B.L.; et al. The costs of dementia subtypes to California Medicare fee-for-service. Alzheimers Dement 2019, 15, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.; Llibre Guerra, J.J. Frontotemporal dementia. Handb. Clin. Neurol. 2019, 165, 33–45. [Google Scholar] [CrossRef] [Green Version]
- Bussè, C.; Pettenuzzo, I.; Pompanin, S.; Roiter, B.; di Bernardo, G.A.; Zorzi, G.; Fragiacomo, F.; Gazzola, G.; Cecchin, D.; Pigato, G.; et al. Psychiatric Phenocopy Syndrome of Behavioral Frontotemporal Dementia: Behavioral and Cognitive Fingerprint. J. Alzheimers Dis. 2019, 72, 1159–1164. [Google Scholar] [CrossRef]
- Butler, P.M.; Chiong, W. Neurodegenerative disorders of the human frontal lobes. Handb. Clin. Neurol. 2019, 163, 391–410. [Google Scholar] [CrossRef]
- Bailey, K.C.; Burmaster, S.A.; Schaffert, J.; LoBue, C.; Vela, D.; Rossetti, H.; Cullum, C.M. Associations of Race-Ethnicity and History of Traumatic Brain Injury with Age at Onset of Alzheimer’s Disease. J. Neuropsychiatry Clin. Neurosci 2019. appineuropsych19010002. [Google Scholar] [CrossRef] [PubMed]
- Schwab, N.; Grenier, K.; Hazrati, L.N. DNA repair deficiency and senescence in concussed professional athletes involved in contact sports. Acta Neuropathol. Commun. 2019, 7, 182. [Google Scholar] [CrossRef] [PubMed]
- Keszycki, R.M.; Fisher, D.W.; Dong, H. The Hyperactivity-Impulsivity-Irritiability-Disinhibition-Aggression-Agitation Domain in Alzheimer’s Disease: Current Management and Future Directions. Front. Pharmacol. 2019, 10, 1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desmarais, P.; Weidman, D.; Wassef, A.; Bruneau, M.A.; Friedland, J.; Bajsarowicz, P.; Thibodeau, M.P.; Herrmann, N.; Nguyen, Q.D. The Interplay between Post-traumatic Stress Disorder and Dementia: A Systematic Review. Am. J. Geriatr. Psychiatry 2020, 28, 46–60. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Martínez-Bouza, R. Genomics and pharmacogenomics of schizophrenia. CNS Neurosci. Ther. 2011, 17, 541–565. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Torrellas, C. Epigenetics of Aging and Alzheimer’s Disease: Implications for Pharmacogenomics and Drug Response. Int. J. Mol. Sci. 2015, 16, 30483–30543. [Google Scholar] [CrossRef] [Green Version]
- Cacabelos, R.; Cacabelos, P.; Aliev, G. Genomics and pharmacogenomics of antipsychotic drugs. Open J. Psychiatry 2013, 3, 46–139. [Google Scholar] [CrossRef] [Green Version]
- Martins, L.B.; Monteze, N.M.; Calarge, C.; Ferreira, A.V.M.; Teixeira, A.L. Pathways linking obesity to neuropsychiatric disorders. Nutrition 2019, 66, 16–21. [Google Scholar] [CrossRef]
- Morton, R.E.; St John, P.D.; Tyas, S.L. Migraine and the risk of all-cause dementia, Alzheimer’s disease, and vascular dementia: A prospective cohort study in community-dwelling older adults. Int. J. Geriatr. Psychiatry 2019, 34, 1667–1676. [Google Scholar] [CrossRef]
- Blom, K.; Koek, H.L.; Zwartbol, M.H.T.; van der Graaf, Y.; Kesseler, L.; Biessels, G.J.; Geerlings, M.I.; SMART Study Group. Subjective cognitive decline, brain imaging biomarkers, and cognitive functioning in patients with a history of vascular disease: The SMART-Medea study. Neurobiol. Aging 2019, 84, 33–40. [Google Scholar] [CrossRef]
- Puzo, C.; Labriola, C.; Sugarman, M.A.; Tripodis, Y.; Martin, B.; Palmisano, J.N.; Steinber, E.G.; Stein, T.D.; Kowall, N.W. Independent effects of white matter hyperintensities on cognitive, neuropsychiatric, and functional decline: A longitudinal investigation using the National Alzheimer’s Coordinating Center Uniform Data Set. Alzheimers Res. Ther. 2019, 11, 64. [Google Scholar] [CrossRef] [PubMed]
- Rouch, I.; Dorey, J.M.; Padovan, C.; Trombert-Paviot, B.; Benoit, M.; Laurent, B.; PACO group; Boublay, N.; Krolak-Salmon, P. Does Personality Predict Behavioral and Psychological Symptoms of Dementia? Results from PACO Prospective Study. J. Alzheimers Dis. 2019, 69, 1099–1108. [Google Scholar] [CrossRef]
- Banning, L.C.P.; Ramakers, I.H.G.B.; Deckers, K.; Verhey, F.R.J.; Aalten, P. Affective symptoms and AT(N) biomarkers in mild cognitive impairment and Alzheimer’s disease: A systematic literature review. Neurosci. Biobehav. Rev. 2019, 107, 346–359. [Google Scholar] [CrossRef] [PubMed]
- Scaricamazza, E.; Colonna, I.; Sancesario, G.M.; Assogna, F.; Orfei, M.D.; Franchini, F.; Sancesario, G.; Mercuri, N.B.; Liguori, C. Neuropsychiatric symptoms differently affect mild cognitive impairment and Alzheimer’s disease patients: A retrospective observational study. Neurol. Sci. 2019, 40, 1377–1382. [Google Scholar] [CrossRef] [PubMed]
- Showraki, A.; Murari, G.; Ismail, Z.; Barfett, J.J.; Fornazzari, L.; Munoz, D.G. Cerebrospinal Fluid Correlates of Neuropsychiatric Symptoms in Patients with Alzheimer’s Disease/Mild Cognitive Impairment: A Systematic Review. J. Alzheimers Dis. 2019, 71, 477–501. [Google Scholar] [CrossRef]
- Ramusino, M.C.; Garibotto, V.; Bacchin, R.; Altomare, D.; Dodich, A.; Assal, F.; Mendes, A.; Costa, A.; Tinazzi, M.; Morbelli, S.D.; et al. Incremental value of amyloid-PET versus CSF in the diagnosis of Alzheimer’s disease. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 270–280. [Google Scholar] [CrossRef]
- Bayram, E.; Shan, G.; Cummings, J.L. Associations between Comorbid TDP-43, Lewy Body Pathology, and Neuropsychiatric Symptoms in Alzheimer’s Disease. J. Alzheimers Dis. 2019, 69, 953–961. [Google Scholar] [CrossRef] [Green Version]
- Sellami, L.; St-Onge, F.; Poulin, S.; Laforce, R., Jr. Schizophrenia Phenotype Preceding Behavioral Variant Frontotemporal Dementia Related to C9orf72 Repeat Expansion. Cogn. Behav. Neurol. 2019, 32, 120–123. [Google Scholar] [CrossRef]
- Latimer, C.S.; Burke, B.T.; Liachko, N.F.; Currey, H.N.; Kilgore, M.D.; Gibbons, L.E.; Henriksen, J.; Darvas, M.; Domoto-Reilly, K.; Jayadev, S.; et al. Resistance and resilience to Alzheimer’s disease pathology are associated with reduced cortical pTau and absence of limbic-predominant age-related TDP-43 encephalopathy in a community-based cohort. Acta Neuropathol. Commun. 2019, 7, 9. [Google Scholar] [CrossRef] [Green Version]
- Pirker-Kees, A.; Dal-Bianco, P.; Schmidt, R. Effects of Psychotropic Medication on Cognition, Caregiver Burden, and Neuropsychiatric Symptoms in Alzheimer’s Disease over 12 Months: Results from a Prospective Registry of Dementia in Austria (PRODEM). J. Alzheimers Dis. 2019, 71, 623–630. [Google Scholar] [CrossRef]
- Bravo-José, P.; Sáez-Lleó, C.I.; Peris-Martí, J.F. Deprescribing antipsychotics in long term care patients with dementia. Farm. Hosp. 2019, 43, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Mantri, S.; Fullard, M.; Gray, S.L.; Weintraub, D.; Hubbard, R.A.; Hennessy, S.; Willis, A.W. Patterns of Dementia Treatment and Frank Prescribing Errors in Older Adults With Parkinson Disease. JAMA Neurol. 2019, 76, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Cacabelos, N.; Carril, J.C. The role of pharmacogenomics in adverse drug reactions. Expert Rev. Clin. Pharmacol. 2019, 12, 407–442. [Google Scholar] [CrossRef]
- Zheng, W.Y.; Richardson, L.C.; Li, L.; Day, R.O.; Westbrook, J.I.; Baysari, M.T. Drug-drug interactions and their harmful effects in hospitalised patients: A systematic review and meta-analysis. Eur. J. Clin. Pharmacol. 2018, 74, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.I.; Beckett, R.D. Evaluation of resources for analyzing drug interactions. J. Med. Libr. Assoc. 2016, 104, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Shoshi, A.; Müller, U.; Shoshi, A.; Ogultarhan, V.; Hofestadt, R. KALIS—An eHealth System for Biomedical Risk Analysis of Drugs. Stud. Health Technol. Inform. 2017, 236, 128–135. [Google Scholar]
- Shoshi, A.; Hoppe, T.; Kormeier, B.; Ogultarhan, V.; Hofestadt, R. GraphSAW: A web-based system for graphical analysis of drug interactions and side effects using pharmaceutical and molecular data. BMC Med. Inform. Decis. Mak. 2015, 15, 15. [Google Scholar] [CrossRef] [Green Version]
- Huang, F.; Fu, Y. A review of clinical pharmacokinetics and pharmacodynamics of galantamine, a reversible acetylcholinesterase inhibitor for the treatment of Alzheimer’s disease, in healthy subjects and patients. Curr. Clin. Pharmacol. 2010, 5, 115–124. [Google Scholar] [CrossRef]
- Samwald, M.; Miñarro Giménez, J.A.; Boyce, R.D.; Frimuth, R.R.; Adlassnig, K.P.; Dumontier, M. Pharmacogenomic knowledge representation, reasoning and genome-based clinical decision support based on OWL 2 DL ontologies. BMC Med. Inform. Decis. Mak. 2015, 15, 12. [Google Scholar] [CrossRef] [Green Version]
- Zhang, G.; Zhang, Y.; Ling, Y.; Jia, J. Web resources for pharmacogenomics. Genom. Proteom. Bioinform. 2015, 13, 51–54. [Google Scholar] [CrossRef] [Green Version]
- PharmGKB. Available online: https://www.pharmgkb.org (accessed on 5 January 2020).
- Weinshilboum, R.M.; Wang, L. Pharmacogenomics: Precision Medicine and Drug Response. Mayo Clin. Proc. 2017, 92, 1711–1722. [Google Scholar] [CrossRef]
- Kozyra, M.; Ingelman-Sundberg, M.; Lauschke, V.M. Rare genetic variants in cellular transporters, metabolic enzymes, and nuclear receptors can be important determinants of interindividual differences in drug response. Genet. Med. 2017, 19, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.W.; Chen, X.W.; Sneed, K.B.; Yang, Y.X.; Zhang, X.; He, Z.X.; Chow, K.; Yang, T.; Duan, W.; Zhou, S.F. Clinical association between pharmacogenomics and adverse drug reactions. Drugs 2015, 75, 589–631. [Google Scholar] [CrossRef]
- Cacabelos, R. World Guide for Drug Use and Pharmacogenomics; EuroEspes Publishing: Corunna, Spain, 2012. [Google Scholar]
- EuroPharmaGenics (EPG). Available online: http://europharmagenics.com/ (accessed on 2 November 2019).
- Cacabelos, R. Population-level pharmacogenomics for precision drug development in dementia. Expert Rev. Precis. Med. Drug Dev. 2018, 3, 163–188. [Google Scholar] [CrossRef]
- Cacabelos, R. Epigenomic networking in drug development: From pathogenic mechanisms to pharmacogenomics. Drug Dev. Res. 2014, 75, 348–365. [Google Scholar] [CrossRef]
- Marcath, L.A.; Pasternak, A.L.; Hertz, D.L. Challenges to assess substrate-dependent allelic effects in CYP450 enzymes and the potential clinical implications. Pharmacogenom. J. 2019. [Google Scholar] [CrossRef] [PubMed]
- Lesche, D.; Mostafa, S.; Everall, I.; Pantelis, C.; Bousman, C. Impact of CYP1A2, CYP2C19, and CYP2D6 genotype- and phenoconversion-predicted enzyme activity on clozapine exposure and symptom severity. Pharmacogenom. J. 2019. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Tellado, I.; Cacabelos, P. The epigenetic machinery in the life cycle and pharmacoepigenetics. In Pharmacoepigenetics; Cacabelos, R., Ed.; Academic Press/Elsevier: Oxford, UK, 2019; pp. 1–100. [Google Scholar]
- Cacabelos, R.; Carril, J.C.; Sanmartín, A.; Cacabelos, P. Pharmacoepigenetic processors: Epigenetic drugs, Drug resistance, Toxicoepigenetics, and Nutriepigenetics. In Pharmacoepigenetics; Cacabelos, R., Ed.; Academic Press/Elsevier: Oxford, UK, 2019; pp. 191–424. [Google Scholar]
- Apostolova, L.G.; Risacher, S.L.; Duran, T.; Stage, E.C.; Goukasian, N.; West, J.D.; Do, T.M.; Grotts, J.; Wilhalme, H.; Nho, K.; et al. Alzheimer’s Disease Neuroimaging Initiative. Associations of the Top 20 Alzheimer Disease Risk Variants with Brain Amyloidosis. JAMA Neurol. 2018, 75, 328–341. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Meyyazhagan, A.; Carril, J.C.; Cacabelos, P.; Teijido, O. Pharmacogenetics of Vascular Risk Factors in Alzheimer’s Disease. J. Personalized Med. 2018, 8, 3. [Google Scholar] [CrossRef] [Green Version]
- Cacabelos, R. Pleiotropy and promiscuity in pharmacogenomics for the treatment of Alzheimer’s disease and related risk factors. Future Neurol. 2018. [Google Scholar] [CrossRef]
- Cacabelos, R.; Torrellas, C. Epigenetic drug discovery for Alzheimer’s disease. Expert Opin. Drug Discov. 2014, 9, 1059–1086. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Torrellas, C. Pharmacogenomics of antidepressants. HSOA J. Psychiatry Depress. Anxiety 2015, 1, 001. [Google Scholar] [CrossRef] [Green Version]
- Foraker, J.; Millard, S.P.; Leong, L.; Thomson, Z.; Chen, S.; Keene, C.D.; Bekris, L.M.; Yu, C.E. The APOE Gene is Differentially Methylated in Alzheimer’s Disease. J. Alzheimers Dis. 2015, 48, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Vogelgesang, S.; Cascorbi, I.; Schroeder, E.; Pahnke, J.; Kroemer, H.K.; Siegmund, W.; Kunert-Keil, C.; Walker, L.C.; Warzok, R.W. Deposition of Alzheimer’s beta-amyloid is inversely correlated with P-glycoprotein expression in the brains of elderly non-demented humans. Pharmacogenetics 2002, 12, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Szablewski, L. Glucose Transporters in Brain: In Health and in Alzheimer’s Disease. J. Alzheimers Dis. 2017, 55, 1307–1320. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; López-Muñoz, F. The ABCB1 transporter in Alzheimer’s disease. Clin. Exp. Pharmacol. 2014, 4, e128. [Google Scholar] [CrossRef] [Green Version]
- Cacabelos, R.; Cacabelos, P.; Carril, J.C. Epigenetics and pharmacoepigenetics of age-related neurodegenerative disorders. In Pharmacoepigenetics; Cacabelos, R., Ed.; Academic Press/Elsevier: Oxford, UK, 2019; pp. 903–950. [Google Scholar]
- Berg, C.N.; Sinha, N.; Gluck, M.A. The Effects of APOE and ABCA7 on Cognitive Function and Alzheimer’s Disease Risk in African Americans: A Focused Mini Review. Front. Hum. Neurosci. 2019, 13, 387. [Google Scholar] [CrossRef] [Green Version]
- Pereira, C.D.; Martins, F.; Wiltfang, J.; da Cruz E Silva, O.A.B.; Rebelo, S. ABC Transporters Are Key Players in Alzheimer’s Disease. J. Alzheimers Dis. 2018, 61, 463–485. [Google Scholar] [CrossRef]
- Marquez, B.; Van Bambeke, F. ABC multidrug transporters: Target for modulation of drug pharmacokinetics and drug-drug interactions. Curr. Drug Targets 2011, 12, 600–620. [Google Scholar] [CrossRef]
- Haufroid, V. Genetic polymorphisms of ATP-binding cassette transporters ABCB1 and ABCC2 and their impact on drug disposition. Curr. Drug Targets 2011, 12, 631–646. [Google Scholar] [CrossRef]
- van Assema, D.M.; Lubberink, M.; Rizzu, P.; van Swieten, J.C.; Schuit, R.C.; Eriksson, J.; Scheltens, P.; Koepp, M.; Lammertsma, A.A.; van Berckel, B.N. Blood-brain barrier P-glycoprotein function in healthy subjects and Alzheimer’s disease patients: Effect of polymorphisms in the ABCB1 gene. EJNMMI Res. 2012, 2, 57. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.D.; Chang, P.T.; Ping, Y.H.; Lee, H.C.; Yeh, C.W.; Wang, P.N. Gene expression profiling of peripheral blood leukocytes identifies and validates ABCB1 as a novel biomarker for Alzheimer’s disease. Neurobiol. Dis. 2011, 43, 698–705. [Google Scholar] [CrossRef]
- Elali, A.; Rivest, S. The role of ABCB1 and ABCA1 in beta-amyloid clearance at the neurovascular unit in Alzheimer’s disease. Front. Physiol. 2013, 4, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cascorbi, I.; Flüh, C.; Remmler, C.; Haenisch, S.; Grumbt, M.; Peters, M.; Brenn, A.; Thal, D.R.; Warzok, R.W.; Vogelgesang, S. Association of ATP-binding cassette transporter variants with the risk of Alzheimer’s disease. Pharmacogenomics 2013, 14, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Reitz, C.; Jun, G.; Naj, A.; Rajbhandary, R.; Vardarajan, B.N.; Wang, L.S.; Valladares, O.; Lin, C.F.; Larson, E.B.; Graff-Radford, N.R. Variants in the ATP-binding cassette transporter (ABCA7), apolipoprotein E ϵ4, and the risk of late-onset Alzheimer disease in African Americans. JAMA 2013, 309, 1483–1492. [Google Scholar] [CrossRef] [PubMed]
- Vasquez, J.B.; Simpson, J.F.; Harpole, R.; Estus, S. Alzheimer’s Disease Genetics and ABCA7 Splicing. J. Alzheimers Dis. 2017, 59, 633–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamazaki, K.; Yoshino, Y.; Mori, T.; Yoshida, T.; Ozaki, Y.; Sao, T.; Mori, Y.; Ochi, S.; Iga, J.I.; Ueno, S.I. Gene Expression and Methylation Analysis of ABCA7 in Patients with Alzheimer’s Disease. J. Alzheimers Dis. 2017, 57, 171–181. [Google Scholar] [CrossRef]
- Stepler, K.E.; Robinson, R.A.S. The Potential of ‘Omics to Link Lipid Metabolism and Genetic and Comorbidity Risk Factors of Alzheimer’s Disease in African Americans. Adv. Exp. Med. Biol. 2019, 1118, 1–28. [Google Scholar] [CrossRef]
- Ma, F.C.; Wang, H.F.; Cao, X.P.; Tan, C.C.; Tan, L.; Yu, J.T. Meta-Analysis of the Association between Variants in ABCA7 and Alzheimer’s Disease. J. Alzheimers Dis. 2018, 63, 1261–1267. [Google Scholar] [CrossRef]
- Zhou, G.; Mao, X.; Chu, J.; Chen, G.; Zhao, Q.; Wang, L.; Luo, Y. ATP binding cassette subfamily A member 7 rs3764650 polymorphism and the risk of Alzheimer’s disease. Pharmazie 2017, 72, 425–427. [Google Scholar] [CrossRef]
- De Roeck, A.; Duchateau, L.; Van Dongen, J.; Cacace, R.; Bjerke, M.; Van den Bossche, T.; Cras, P.; Vandernberghe, R.; De Deyn, P.P.; Engelborghs, S.; et al. An intronic VNTR affects splicing of ABCA7 and increases risk of Alzheimer’s disease. Acta Neuropathol. 2018, 135, 827–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamartinière, Y.; Boucau, M.C.; Dehouck, L.; Krohn, M.; Pahnke, J.; Candela, P.; Gosselet, F.; Fenart, L. ABCA7 Downregulation Modifies Cellular Cholesterol Homeostasis and Decreases Amyloid-β Peptide Efflux in an in vitro Model of the Blood-Brain Barrier. J. Alzheimers Dis. 2018, 64, 1195–1211. [Google Scholar] [CrossRef] [PubMed]
- Guven, G.; Vurgun, E.; Bilgic, B.; Hanagasi, H.; Gurvit, H.; Ozer, E.; Lohnmann, E.; Erginel-Unaltuna, N. Association between selected cholesterol-related gene polymorphisms and Alzheimer’s disease in a Turkish cohort. Mol. Biol. Rep. 2019, 46, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Jiang, Y.; Wei, S.; Shang, S.; Li, P.; Chen, C.; Dang, L.; Wang, J.; Huo, K.; Deng, M.; et al. The Level of Plasma Amyloid-β40 Is Correlated with Peripheral Transport Proteins in Cognitively Normal Adults: A Population-Based Cross-Sectional Study. J. Alzheimers Dis. 2018, 65, 951–961. [Google Scholar] [CrossRef] [PubMed]
- Davis, W.J.; Tew, K.D. ATP-binding cassette transporter-2 (ABCA2) as a therapeutic target. Biochem. Pharmacol. 2018, 151, 188–200. [Google Scholar] [CrossRef]
- Xu, X.; Wang, Y.; Wang, L.; Liao, Q.; Chang, L.; Xu, L.; Huang, Y.; Ye, H.; Xu, L.; Chen, C.; et al. Meta-analyses of 8 polymorphisms associated with the risk of the Alzheimer’s disease. PLoS ONE 2013, 8, e73129. [Google Scholar] [CrossRef] [Green Version]
- Fehér, Á.; Giricz, Z.; Juhász, A.; Pákáski, M.; Janka, Z.; Kálmán, J. ABCA1 rs2230805 and rs2230806 common gene variants are associated with Alzheimer’s disease. Neurosci Lett. 2018, 664, 79–83. [Google Scholar] [CrossRef]
- Hu, W.; Lin, X.; Zhang, H.; Zhao, N. ATP Binding Cassette Subfamily A Member 2 (ABCA2) Expression and Methylation are Associated with Alzheimer’s Disease. Med. Sci. Monit. 2017, 23, 5851–5861. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Sun, S.; Zhang, W.; Shi, Z. Polymorphisms of ABCG2 and its impact on clinical relevance. Biochem. Biophys. Res. Commun. 2018, 503, 408–413. [Google Scholar] [CrossRef]
- Fehér, Á.; Juhász, A.; László, A.; Pákáski, M.; Kálmán, J.; Janka, Z. Association between the ABCG2 C421A polymorphism and Alzheimer’s disease. Neurosci. Lett. 2013, 550, 51–54. [Google Scholar] [CrossRef]
- Shubbar, M.H.; Penny, J.I. Effect of amyloid beta on ATP-binding cassette transporter expression and activity in porcine brain microvascular endothelial cells. Biochim. Biophys. Acta Gen. Subj. 2018, 1862, 2314–2322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaller, L.; Lauschke, V.M. The genetic landscape of the human solute carrier (SLC) transporter superfamily. Hum. Genet. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, R.H.; Yu, J.T.; Tan, L. The Role of SORL1 in Alzheimer’s Disease. Mol. Neurobiol. 2015, 51, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Britzolaki, A.; Saurine, J.; Klocke, B.; Pitychoutis, P.M. A Role for SERCA Pumps in the Neurobiology of Neuropsychiatric and Neurodegenerative Disorders. Adv. Exp. Med. Biol. 2020, 1131, 131–161. [Google Scholar] [CrossRef]
- Heinemeyer, T.; Stemmet, M.; Bardien, S.; Neethling, A. Underappreciated Roles of the Translocase of the Outer and Inner Mitochondrial Membrane Protein Complexes in Human Disease. DNA Cell Biol. 2019, 38, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Belrose, J.C.; Jackson, M.F. TRPM2: A candidate therapeutic target for treating neurological diseases. Acta Pharmacol. Sin. 2018, 39, 722–732. [Google Scholar] [CrossRef] [Green Version]
- Pan, Y.; Omori, K.; Ali, I.; Tachikawa, M.; Terasaki, T.; Brouwer, K.L.R.; Nicolazzo, J.A. Altered Expression of Small Intestinal Drug Transporters and Hepatic Metabolic Enzymes in a Mouse Model of Familial Alzheimer’s Disease. Mol. Pharm. 2018, 15, 4073–4083. [Google Scholar] [CrossRef]
- Cacabelos, R. Pharmacogenomics of drugs used to treat brain disorders. Expert Rev. Precis. Med. Drug Dev. 2020. [Google Scholar] [CrossRef]
- Li, D.D.; Zhang, Y.H.; Zhang, W.; Zhao, P. Meta-Analysis of Randomized Controlled Trials on the Efficacy and Safety of Donepezil, Galantamine, Rivastigmine, and Memantine for the Treatment of Alzheimer’s Disease. Front. Neurosci. 2019, 13, 472. [Google Scholar] [CrossRef]
- Dekker, M.J.H.J.; Bouvy, J.C.; O’Rourke, D.; Thompson, R.; Makady, A.; Jonsson, P.; Gispen-de Wield, C.C. Alignment of European Regulatory and Health Technology Assessments: A Review of Licensed Products for Alzheimer’s Disease. Front. Med. 2019, 6, 73. [Google Scholar] [CrossRef] [Green Version]
- Cacabelos, R.; Llovo, R.; Fraile, C.; Fernández-Novoa, L. Pharmacogenetic aspects of therapy with cholinesterase inhibitors: The role of CYP2D6 in Alzheimer’s disease pharmacogenetics. Curr. Alzheimer Res. 2007, 4, 479–500. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R. Donepezil in Alzheimer’s disease: From conventional trials to pharmacogenetics. Neuropsychiatr. Dis. Treat. 2007, 3, 303–333. [Google Scholar] [PubMed]
- Cacabelos, R.; Takeda, M.; Winblad, B. The glutamatergic system and neurodegeneration in dementia: Preventive strategies in Alzheimer’s disease. Int. J. Geriatr. Psychiatry 1999, 14, 3–47. [Google Scholar] [CrossRef]
- Hays, C.C.; Zlatar, Z.Z.; Meloy, M.J.; Osuna, J.; Liu, T.T.; Galasko, D.R.; Wierenga, C.E. Anterior Cingulate Structure and Perfusion Is Associated with Cerebrospinal Fluid Tau Among Cognitively Normal Older Adult APOEε4 Carriers. J. Alzheimers Dis. 2019. [Google Scholar] [CrossRef]
- Weintraub, S.; Teylan, M.; Rader, B.; Chan, K.C.G.; Bollenbeck, M.; Kukull, W.A.; Coventry, C.; Rogalski, E.; Bigio, E.; Mesulam, M.M. APOE is a correlate of phenotypic heterogeneity in Alzheimer disease in a national cohort. Neurology 2019, 94, e607–e612. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R. Molecular pathology and pharmacogenomics in Alzheimer’s disease: Polygenic-related effects of multifactorial treatments on cognition, anxiety and depression. Methods Find. Exp. Clin. Pharmacol. 2007, 29, 1–91. [Google Scholar]
- Cacabelos, R.; Martínez, R.; Fernández-Novoa, L.; Carril, J.C.; Lombardi, V.; Carrera, I.; Corzo, L.; Tellado, I.; Leszek, J.; McKay, A.; et al. Genomics of Dementia: APOE- and CYP2D6-Related Pharmacogenetics. Int. J. Alzheimers Dis. 2012, 2012, 518901. [Google Scholar] [CrossRef] [Green Version]
- Cacabelos, R.; Torrellas, C.; Carrera, I. Opportunities in Pharmacogenomics for the treatment of Alzheimer’s Disease. Future Neurol. 2015, 10, 229–252. [Google Scholar] [CrossRef]
- Cacabelos, R.; Torrellas, C.; Teijido, O.; Carril, J.C. Pharmacogenetic considerations in the treatment of Alzheimer’s disease. Pharmacogenomics 2016, 17, 1041–1074. [Google Scholar] [CrossRef]
- Cacabelos, R.; Fernández-Novoa, L.; Pichel, V.; Lombardi, V.; Kubota, Y.; Takeda, M. Pharmacogenomic studies with a combination therapy in Alzheimer’s disease. In Molecular Neurobiology of Alzheimer’s Disease and Related Disorders; Takeda, M., Tanaka, T., Cacabelos, R., Eds.; Karger: Basel, Switzerland, 2004; pp. 94–107. [Google Scholar]
- Cacabelos, R.; Goldgaber, D.; Vostrov, A.; Matsuki, H.; Torrellas, C.; Corzo, D.; Carril, J.C.; Roses, A.D. APOE-TOMM40 in the Pharmacogenomics of demetia. J. Pharmacogenom. Pharmacoproteom. 2014, 5, 1. [Google Scholar] [CrossRef] [Green Version]
- Cacabelos, R.; Rodríguez, B.; Carrera, C.; Beyer, K.; Lao, J.I.; Sellers, M.A. Behavioral changes associated with different apolipoprotein E genotypes in dementia. Alzheimer’s Dis. Assoc. Dis. 1997, 11, S27–S37. [Google Scholar]
- Cacabelos, R. Pharmacogenomics of Alzheimer’s and Parkinson’s diseases. Neurosci. Lett. 2018, 133807. [Google Scholar] [CrossRef]
- Darreh-Shori, T.; Siawesh, M.; Mousavi, M.; Andreasen, N.; Nordberg, A. Apolipoprotein ε4 modulates phenotype of butyrylcholinesterase in CSF of patients with Alzheimer’s disease. J. Alzheimers Dis. 2012, 28, 443–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noetzli, M.; Eap, C.B. Pharmacodynamic, pharmacokinetic and pharmacogenetic aspects of drugs used in the treatment of Alzheimer’s Disease. Clin. Pharmacokinet. 2013, 52, 225–241. [Google Scholar] [CrossRef] [PubMed]
- Birks, J.S.; Harvey, R.J. Donepezil for dementia due to Alzheimer’s disease. Cochrane Database Syst. Rev. 2018, 6, CD001190. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, A.; Franceschi, M.; D’Onofrio, G.; Bizzarro, A.; Mangialasche, F.; Cascavilla, L.; París, F.; Matera, M.G.; Pilotto, A.; Deniele, A.; et al. Effect of a CYP2D6 polymorphism on the efficacy of donepezil in patients with Alzheimer disease. Neurology 2009, 73, 761–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noetzli, M.; Guidi, M.; Ebbing, K.; Eyer, S.; Wilhelm, L.; Michon, A.; Thoomazic, V.; Stancu, I.; Alnawaqil, A.M.; Bula, C.; et al. Population pharmacokinetic approach to evaluate the effect of CYP2D6, CYP3A, ABCB1, POR and NR1I2 genotypes on donepezil clearance. Br. J. Clin. Pharmacol. 2014, 78, 135–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albani, D.; Martinelli, B.F.; Biella, G.; Giiacalone, G.; Lupoli, S.; Clerici, F.; Benussi, L.; Ghidoni, R.; Galimberti, D.; Squitti, R.; et al. Replication study to confirm the role of CYP2D6 polymorphism rs1080985 on donepezil efficacy in Alzheimer’s disease patients. J. Alzheimers Dis. 2012, 30, 745–749. [Google Scholar] [CrossRef]
- Xiao, T.; Jiao, B.; Zhang, W.; Tang, B.; Shen, L. Effect of the CYP2D6 and APOE Polymorphisms on the Efficacy of Donepezil in Patients with Alzheimer’s Disease: A Systematic Review and Meta-Analysis. CNS Drugs 2016, 30, 899–907. [Google Scholar] [CrossRef]
- Seripa, D.; Bizzarro, A.; Pilotto, A.; D’onofrio, G.; Vecchione, G.; Gallo, A.P.; Cascavilla, L.; Paris, F.; Grandone, E.; Mecocci, P.; et al. Role of cytochrome P4502D6 functional polymorphisms in the efficacy of donepezil in patients with Alzheimer’s disease. Pharmacogenet. Genom. 2011, 21, 225–230. [Google Scholar]
- Zhong, Y.; Zheng, X.; Miao, Y.; Wan, L.; Yan, H.; Wang, B. Effect of CYP2D6*10 and APOE polymorphisms on the efficacy of donepezil in patients with Alzheimer’s disease. Am. J. Med. Sci. 2013, 345, 222–226. [Google Scholar] [CrossRef]
- Yaowaluk, T.; Senanarong, V.; Limwongse, C.; Boonprasert, R.; Kijsanayotin, P. Influence of CYP2D6, CYP3A5, ABCB1, APOE polymorphisms and nongenetic factors on donepezil treatment in patients with Alzheimer’s disease and vascular dementia. Pharmacogenom. Personalized Med. 2019, 12, 209–224. [Google Scholar] [CrossRef] [Green Version]
- Ma, S.L.; Tang, N.L.S.; Wat, K.H.Y.; Tang, J.H.Y.; Lau, K.H.; Law, C.B.; Chiue, J.; Tam, C.C.W.; Poon, T.K. Effect of CYP2D6 and CYP3A4 Genotypes on the Efficacy of Cholinesterase Inhibitors in Southern Chinese Patients With Alzheimer’s Disease. Am. J. Alzheimers Dis. Other Demen. 2019, 34, 302–307. [Google Scholar] [CrossRef]
- Magliulo, L.; Dahl, M.L.; Lombardi, G.; Fallarini, S.; Villa, L.M.; Biolcati, A.; Scordo, M.G. Do CYP3A and ABCB1 genotypes influence the plasma concentration and clinical outcome of donepezil treatment? Eur. J. Clin. Pharmacol. 2011, 67, 47–54. [Google Scholar] [CrossRef]
- Lu, J.; Fu, J.; Zhong, Y.; Yang, Q.; Huang, J.; Li, J.; Huo, Y.; Zhao, Y.; Wan, L.; Guo, C. Association between ABCA1 gene polymorphisms and the therapeutic response to donepezil therapy in Han Chinese patients with Alzheimer’s disease. Brain Res. Bull. 2018, 140, 1–4. [Google Scholar] [CrossRef]
- De Beaumont, L.; Pelleieux, S.; Lamarre-Théroux, L.; Dea, D.; Poirier, J. Alzheimer’s Disease Cooperative Study. Butyrylcholinesterase K and Apolipoprotein E-ε4 Reduce the Age of Onset of Alzheimer’s Disease, Accelerate Cognitive Decline, and Modulate Donepezil Response in Mild Cognitively Impaired Subjects. J. Alzheimers Dis. 2016, 54, 913–922. [Google Scholar] [CrossRef]
- Sokolow, S.; Li, X.; Chen, L.; Taylor, K.D.; Rotter, J.I.; Rissman, R.A.; Aisen, P.S.; Apostolova, L.G. Deleterious Effect of Butyrylcholinesterase K-Variant in Donepezil Treatment of Mild Cognitive Impairment. J. Alzheimers Dis. 2017, 56, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Zang, Y.; Song, Q.; Li, H.; Hu, L.; Zhao, W.; Feng, S.; Gu, F.; Zhao, F.; Zhang, C. The efficacy of a “cocktail therapy” on Parkinson’s disease with dementia. Neuropsychiatr. Dis. Treat. 2019, 15, 1639–1647. [Google Scholar] [CrossRef] [Green Version]
- Khuanjing, T.; Palee, S.; Chattipakorn, S.C.; Chattipakorn, N. The effects of acetylcholinesterase inhibitors on the heart in acute myocardial infarction and heart failure: From cells to patient reports. Acta Physiol. 2019, 228, e13396. [Google Scholar] [CrossRef]
- Kawashiri, T.; Shimizu, S.; Shigematsu, N.; Kobayashi, D.; Shimazoe, T. Donepezil ameliorates oxaliplatin-induced peripheral neuropathy via a neuroprotective effect. J. Pharmacol. Sci. 2019, 140, 291–294. [Google Scholar] [CrossRef]
- Wong, J.C.; Thelin, J.T.; Escayg, A. Donepezil increases resistance to induced seizures in a mouse model of Dravet syndrome. Ann. Clin. Transl. Neurol. 2019, 6, 1566–1571. [Google Scholar] [CrossRef] [Green Version]
- Jann, M.W.; Shirley, K.L.; Small, G.W. Clinical pharmacokinetics and pharmacodynamics of cholinesterase inhibitors. Clin. Pharmacokinet. 2002, 41, 719–739. [Google Scholar] [CrossRef] [PubMed]
- Lilienfeld, S. Galantamine-a novel cholinergic drug with a unique dual mode of action for the treatment of patients with Alzheimer’s disease. CNS Drug Rev. 2002, 8, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Brett, M.; Van Osselaer, N.; Huang, F.; Raoult, A.; Van Peer, A.; Verhaeghe, T.; Hust, R. Galantamine pharmacokinetics, safety, and tolerability profiles are similar in healthy Caucasian and Japanese subjects. J. Clin. Pharmacol. 2002, 42, 1002–1010. [Google Scholar] [CrossRef] [PubMed]
- Farlow, M.R. Clinical pharmacokinetics of galantamine. Clin. Pharmacokinet. 2003, 42, 1383–1392. [Google Scholar] [CrossRef]
- Mannens, G.S.; Snel, C.A.; Hendrickx, J.; Verhaeghe, T.; Le Jeune, L.; Bode, W.; van Beijsterveldt, L.; Lavrijsen, K.; Leempoels, J.; Van Osselaer, N.; et al. The metabolism and excretion of galantamine in rats, dogs, and humans. Drug Metab. Dispos. 2002, 30, 553–563. [Google Scholar] [CrossRef] [Green Version]
- Noetzli, M.; Guidi, M.; Ebbing, K.; Eyer, S.; Zumbach, S.; Giannakopoulos, P.; von Gunten, A.; Csajka, C.; Eap, C.B. Relationship of CYP2D6, CYP3A, POR, and ABCB1 genotypes with galantamine plasma concentrations. Ther. Drug Monit. 2013, 35, 270–275. [Google Scholar] [CrossRef]
- Clarke, J.A.; Cutler, M.; Gong, I.; Schwarz, U.I.; Freeman, D.; Dasgupta, M. Cytochrome P450 2D6 phenotyping in an elderly population with dementia and response to galantamine in dementia: A pilot study. Am. J. Geriatr. Pharmacother. 2011, 9, 224–233. [Google Scholar] [CrossRef]
- Bentué-Ferrer, D.; Tribut, O.; Polard, E.; Allain, H. Clinically significant drug interactions with cholinesterase inhibitors: A guide for neurologists. CNS Drugs 2003, 17, 947–963. [Google Scholar] [CrossRef]
- Zhai, X.J.; Lu, Y.N. Food-drug interactions: Effect of capsaicin on the pharmacokinetics of galantamine in rats. Xenobiotica 2012, 42, 1151–1155. [Google Scholar] [CrossRef]
- Carroll, K.M.; DeVito, E.E.; Yip, S.W.; Nich, C.; Sofuoglu, M. Double-Blind Placebo-Controlled Trial of Galantamine for Methadone-Maintained Individuals With Cocaine Use Disorder: Secondary Analysis of Effects on Illicit Opioid Use. Am. J. Addict. 2019, 28, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Sugarman, D.E.; De Aquino, J.P.; Poling, J.; Sofuoglu, M. Feasibility and effects of galantamine on cognition in humans with cannabis use disorder. Pharmacol. Biochem. Behav. 2019, 181, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Njoku, I.; Radabaugh, H.L.; Nicholas, M.A.; Kutash, L.A.; O’Neil, D.A.; Marshall, I.P.; Cheng, J.P.; Kline, A.E. Chronic treatment with galantamine rescues reversal learning in an attentional set-shifting test after experimental brain trauma. Exp. Neurol. 2019, 315, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Choueiry, J.; Blais, C.M.; Shah, D.; Smith, D.; Fisher, D.; Labelle, A.; Knott, V. Combining CDP-choline and galantamine, an optimized α7 nicotinic strategy, to ameliorate sensory gating to speech stimuli in schizophrenia. Int. J. Psychophysiol. 2019, 145, 70–82. [Google Scholar] [CrossRef]
- Koola, M.M. Potential Role of Antipsychotic-Galantamine-Memantine Combination in the Treatment of Positive, Cognitive, and Negative Symptoms of Schizophrenia. Mol. Neuropsychiatry 2018, 4, 134–148. [Google Scholar] [CrossRef]
- Birks, J.S.; Grimley Evans, J. Rivastigmine for Alzheimer’s disease. Cochrane Database Syst. Rev. 2015, 10, CD001191. [Google Scholar] [CrossRef]
- Jia, J.; Ji, Y.; Feng, T.; Ye, Q.; Peng, D.; Kuang, W.; Ning, Y. Sixteen-Week Interventional Study to Evaluate the Clinical Effects and Safety of Rivastigmine Capsules in Chinese Patients with Alzheimer’s Disease. J. Alzheimers Dis. 2019. [Google Scholar] [CrossRef]
- Polinsky, R.J. Clinical pharmacology of rivastigmine: A new-generation acetylcholinesterase inhibitor for the treatment of Alzheimer’s disease. Clin. Ther. 1998, 20, 634–647. [Google Scholar] [CrossRef]
- Sonali, N.; Tripathi, M.; Sagar, R.; Velpandian, T.; Subbiah, V. Clinical effectiveness of rivastigmine monotherapy and combination therapy in Alzheimer’s patients. CNS Neurosci. Ther. 2013, 19, 91–97. [Google Scholar] [CrossRef]
- Yoon, H.; Myung, W.; Lim, S.W.; Kang, H.S.; Kim, S.; Won, H.H.; Carroll, B.J.; Kim, D.K. Association of the choline acetyltransferase gene with responsiveness to acetylcholinesterase inhibitors in Alzheimer’s disease. Pharmacopsychiatry 2015, 48, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Clarelli, F.; Mascia, E.; Santangelo, R.; Mazzeo, S.; Giacalone, G.; Galimberti, D.; Fusco, F.; Zuffi, M.; Fenoglio, C.; Franceschi, M. CHRNA7 Gene and response to cholinesterase Inhibitors in an Italian cohort of Alzheimer’s disease patients. J. Alzheimers Dis. 2016, 52, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Martinelli-Boneschi, F.; Giacalone, G.; Magnani, G.; Biella, G.; Coppi, E.; Santangelo, R.; Brambilla, P.; Esposito, F.; Clerici, L.; Benussi, L.; et al. Pharmacogenomics in Alzheimer’s disease: A genome-wide association study of response to cholinesterase inhibitors. Neurobiol. Aging 2013, 34, 1711. [Google Scholar] [CrossRef] [PubMed]
- Ferris, S.; Nordberg, A.; Soininen, H.; Darreh-Shori, T.; Lane, R. Progression from mild cognitive impairment to Alzheimer’s disease: Effects of sex, butyrylcholinesterase genotype, and rivastigmine treatment. Pharmacogenet. Genom. 2009, 19, 635–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jasiecki, J.; Wasąg, B. Butyrylcholinesterase Protein Ends in the Pathogenesis of Alzheimer’s Disease-Could BCHE Genotyping Be Helpful in Alzheimer’s Therapy? Biomolecules 2019, 9, 592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henderson, E.J.; Lord, S.R.; Brodie, M.A.; Gaunt, D.M.; Lawrence, A.D.; Close, J.C.; Whone, A.L.; Ben-Shlomo, Y. Rivastigmine for gait stability in patients with Parkinson’s disease (ReSPonD): A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Neurol. 2016, 15, 249–258. [Google Scholar] [CrossRef] [Green Version]
- Kandiah, N.; Pai, M.; Senanarong, V.; Looi, I.; Ampil, E.; Park, K.W.; Karanam, A.K.; Christopher, S. Rivastigmine: The advantages of dual inhibition of acetylcholinesterase and butyrylcholinesterase and its role in subcortical vascular dementia and Parkinson’s disease dementia. Clin. Interv. Aging 2017, 12, 697–707. [Google Scholar] [CrossRef] [Green Version]
- Burgett, R.N.; Farley, T.M.; Beireis, L.A. Acute treatment of psychotic symptoms in a newly diagnosed Lewy body dementia patient with an accelerated titration schedule of rivastigmine and de-escalation of antipsychotics. BMJ Case Rep. 2019, 12, e230193. [Google Scholar] [CrossRef]
- Yang, Z.; Zhou, X.; Zhang, Q. Effectiveness and safety of memantine treatment for Alzheimer’s disease. J. Alzheimers Dis. 2013, 36, 445–458. [Google Scholar] [CrossRef]
- Noetzli, M.; Guidi, M.; Ebbing, K.; Eyer, S.; Wilhelm, L.; Michon, A.; Thomazic, V.; Alnawaqil, A.M.; Maurer, S.; Zumbach, S.; et al. Population pharmacokinetic study of memantine: Effects of clinical and genetic factors. Clin. Pharmacokinet. 2013, 52, 211–223. [Google Scholar] [CrossRef]
- Micuda, S.; Mundlova, L.; Anzenbacherova, E.; Anzenbacher, P.; Chladek, J.; Fuksa, L.; Fuksa, L.; Martinova, J. Inhibitory effects of memantine on human cytochrome P450 activities: Prediction of in vivo drug interactions. Eur. J. Clin. Pharmacol. 2004, 60, 583–589. [Google Scholar] [CrossRef]
- Marwick, K.F.M.; Skehel, P.A.; Hardingham, G.E.; Wyllie, D.J.A. The human NMDA receptor GluN2AN615K variant influences channel blocker potency. Pharmacol. Res. Perspect. 2019, 7, e00495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kishi, T.; Matsunaga, S.; Oya, K.; Nomura, I.; Ikuta, T.; Iwata, N. Memantine for Alzheimer’s Disease: An Updated Systematic Review and Meta-analysis. J. Alzheimers Dis. 2017, 60, 401–425. [Google Scholar] [CrossRef]
- Glinz, D.; Gloy, V.L.; Monsch, A.U.; Kressig, R.W.; Patel, C.; McCord, K.A.; Ademi, Z.; Tomonafa, Y.; Schwenkglenks, M.; Bucher, H.C.; et al. Acetylcholinesterase inhibitors combined with memantine for moderate to severe Alzheimer’s disease: A meta-analysis. Swiss Med. Wkly. 2019, 149, w20093. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Wang, L.; Xiao, W.; Su, Z.; Zheng, C.; Zhang, Z.; Wang, Y.; Xu, B.; yang, X.; Hoi, M.P.U. Memantine Improves Cognitive Function and Alters Hippocampal and Cortical Proteome in Triple Transgenic Mouse Model of Alzheimer’s Disease. Exp. Neurobiol. 2019, 28, 390–403. [Google Scholar] [CrossRef]
- Inoue, Y.; Ueda, M.; Masuda, T.; Misumi, Y.; Yamashita, T.; Ando, Y. Memantine, a Noncompetitive N-Methyl-D-Aspartate Receptor Antagonist, Attenuates Cerebral Amyloid Angiopathy by Increasing Insulin-Degrading Enzyme Expression. Mol. Neurobiol. 2019, 56, 8573–8588. [Google Scholar] [CrossRef]
- Tahami Monfared, A.A.; Meier, G.; Perry, R.; Joe, D. Burden of Disease and Current Management of Dementia with Lewy Bodies: A Literature Review. Neurol. Ther. 2019, 8, 289–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsunaga, S.; Kishi, T.; Nomura, I.; Sakuma, K.; Okuya, M.; Ikuta, T.; Iwata, N. The efficacy and safety of memantine for the treatment of Alzheimer’s disease. Expert. Opin. Drug Saf. 2018, 17, 1053–1061. [Google Scholar] [CrossRef]
- Lavretsky, H.; Laird, K.T.; Krause-Sorio, B.; Heimberg, B.F.; Yeargin, J.; Grzenda, A.; Wu, P.; Thana-Udom, K.; Ercoli, L.M.; Siddarth, P. A Randomized Double-Blind Placebo-Controlled Trial of Combined Escitalopram and Memantine for Older Adults with Major Depression and Subjective Memory Complaints. Am. J. Geriatr. Psychiatry 2020, 28, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Hassanpour, F.; Zarghami, M.; Mouodi, S.; Moosazadeh, M.; Barzegar, F.; Bagheri, M. Adjunctive Memantine Treatment of Schizophrenia: A Double-Blind, Randomized Placebo-Controlled Study. J. Clin. Psychopharmacol. 2019, 39, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, M.; Sarkar, S.; Theophil, I.; Leopold, K.; Heinz, A.; Gallinat, J. Acute and Long-term Memantine Add-on Treatment to Risperidone Improves Cognitive Dysfunction in Patients with Acute and Chronic Schizophrenia. Pharmacopsychiatry 2019. [Google Scholar] [CrossRef]
- Modarresi, A.; Chaibakhsh, S.; Koulaeinejad, N.; Koupaei, S.R. A systematic review and meta-analysis: Memantine augmentation in moderate to severe obsessive-compulsive disorder. Psychiatry Res. 2019, 282, 112602. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, S.; Karunaikadal, K.; Varadarajan, S.; Krishnan, M. Memantine Ameliorates Migraine Headache. Ann. Indian Acad. Neurol. 2019, 22, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Krishnan-Sarin, S.; O’Malley, S.S.; Franco, N.; Cavallo, D.A.; Tetrault, J.M.; Shi, J.; Gueorguieva, R.; Pittman, B.; Krystal, J.H. Influence of combined treatment with naltrexone and memantine on alcohol drinking behaviors: A phase II randomized crossover trial. Neuropsychopharmacology 2019. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Shi, Y.; Wang, G.; Li, Y.; Cheng, L.; Wang, Y. Memantine selectively prevented the induction of dynamic allodynia by blocking Kir2.1 channel and inhibiting the activation of microglia in spinal dorsal horn of mice in spared nerve injury model. Mol. Pain 2019, 15, 1744806919838947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, E.; Sorel, M.; Morel, V.; Marcaillou, F.; Picard, P.; Delage, N.; Tiberghien, F.; Crosmary, M.C.; Najjar, M.; Colamarino, R.; et al. Dextromethorphan and memantine after ketamine analgesia: A randomized control trial. Drug Des. Dev. Ther. 2019, 13, 2677–2688. [Google Scholar] [CrossRef] [Green Version]
- Fuller, J.T.; Choudhury, T.K.; Lowe, D.A.; Balsis, S. Alzheimer’s Disease Neuroimaging Initiative. Hallucinations and delusions signal Alzheimer’s associated cognitive dysfunction more strongly compared to other neuropsychiatric symptoms. J. Gerontol. B Psychol. Sci. Soc. Sci. 2019, gbz032. [Google Scholar] [CrossRef]
- Seifan, A.; Ganzer, C.A.; Ryon, K.; Lin, M.; Mahmudur, R.; Adolfo, H.; Shih, C.; Jacobs, A.R.; Greenwald, M.; Isaacson, R.S. Detecting Non-cognitive Features of Prodromal Neurodegenerative Diseases. Curr. Aging Sci. 2019, 11, 242–249. [Google Scholar] [CrossRef]
- Sundararajan, T.; Manzardo, A.M.; Butler, M.G. Functional analysis of schizophrenia genes using GeneAnalytics program and integrated databases. Gene 2018, 641, 25–34. [Google Scholar] [CrossRef]
- Garcia-Segura, M.E.; Fischer, C.E.; Schweizer, T.A.; Munoz, D.G. APOE ε4/ε4 Is Associated with Aberrant Motor Behavior Through Both Lewy Body and Cerebral Amyloid Angiopathy Pathology in High Alzheimer’s Disease Pathological Load. J. Alzheimers Dis. 2019. [Google Scholar] [CrossRef]
- Bargagli, A.M.; Cascini, S.; Agabiti, N.; Kirchmayer, U.; Marino, C.; Davoli, M. Determinants Of Antipsychotic Drugs Prescription Among Community Living Older Adults With Dementia A Population Based Study Using Health Information Systems In The Lazio Region, Italy. Clin. Interv. Aging 2019, 14, 2071–2083. [Google Scholar] [CrossRef] [Green Version]
- Ohno, Y.; Kunisawa, N.; Shimizu, S. Antipsychotic Treatment of Behavioral and Psychological Symptoms of Dementia (BPSD): Management of Extrapyramidal Side Effects. Front. Pharmacol. 2019, 10, 1045. [Google Scholar] [CrossRef] [Green Version]
- Xu, M.; Xing, Q.; Li, S.; Zheng, Y.; Wu, S.; Gao, R.; Yu, L.; Guo, T.; Yang, Y.; Liu, J.; et al. Pharacogenetic effects of dopamine transporter gene polymorphisms on response to chlorpromazine and clozapine and on extrapyramidal syndrome in schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2010, 34, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Zivković, M.; Mihaljević-Peles, A.; Bozina, N.; Sagud, M.; Mikolac-Perkovic, M.; Vuksan-Cusa, B.; Muck-Seler, D. The association study of polymorphisms in DAT, DRD2, and COMT genes and acute extrapyramidal adverse effects in male schizophrenic patients treated with haloperidol. J. Clin. Psychopharmacol. 2013, 33, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Mas, S.; Gassó, P.; Lafuente, A.; Bioque, M.; Lobo, A.; González-Pinto, A.; Olmeda, M.S.; Corropio, I.; Llerena, A.; Cabrera, B.; et al. Pharmacogenetic study of antipsychotic induced acute extrapyramidal symptoms in a first episode psychosis cohort: Role of dopamine, serotonin and glutamate candidate genes. Pharmacogenom. J. 2016, 16, 439–445. [Google Scholar] [CrossRef]
- Turčin, A.; Dolžan, V.; Porcelli, S.; Serretti, A.; Plesničar, B.K. Adenosine Hypothesis of Antipsychotic Drugs Revisited: Pharmacogenomics Variation in Nonacute Schizophrenia. OMICS 2016, 20, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Gareeva, A.E.; Zakirov, D.F.; Valinurov, R.G. Polymorphism of RGS2 gene: Genetic markers of risk for schizophrenia and pharmacogenetic markers of typical neuroleptics efficiency. Mol. Biol. 2013, 47, 934–941. [Google Scholar] [CrossRef]
- Mas, S.; Gassó, P.; Ritter, M.A.; Malagelada, C.; Bernardo, M.; Lafuente, A. Pharmacogenetic predictor of extrapyramidal symptoms induced by antipsychotics: Multilocus interaction in the mTOR pathway. Eur. Neuropsychopharmacol. 2015, 25, 51–59. [Google Scholar] [CrossRef]
- Lee, H.J.; Kang, S.G. Genetics of tardive dyskinesia. Int. Rev. Neurobiol. 2011, 98, 231–264. [Google Scholar] [CrossRef]
- Koola, M.M.; Tsapakis, E.M.; Wright, P.; Smith, S.; Kerwin Rip, R.W.; Nugent, K.L.; Aitchison, K.J. Association of tardive dyskinesia with variation in CYP2D6: Is there a role for active metabolites? J. Psychopharmacol. 2014, 28, 665–670. [Google Scholar] [CrossRef] [Green Version]
- Lanning, R.K.; Zai, C.C.; Müller, D.J. Pharmacogenetics of tardive dyskinesia: An updated review of the literature. Pharmacogenomics 2016, 17, 1339–1351. [Google Scholar] [CrossRef]
- Tanaka, S.; Syu, A.; Ishiguro, H.; Inada, T.; Horiuchi, Y.; Ishikawa, M.; Koga, M.; Noguchi, E.; Ozaki, N.; Someya, T.; et al. DPP6 as a candidate gene for neuroleptic-induced tardive dyskinesia. Pharmacogenom. J. 2013, 13, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Greenbaum, L.; Alkelai, A.; Zozulinsky, P.; Kohn, Y.; Lerer, B. Support for association of HSPG2 with tardive dyskinesia in Caucasian populations. Pharmacogenom. J. 2012, 12, 513–520. [Google Scholar] [CrossRef] [Green Version]
- Tiwari, A.K.; Zai, C.C.; Likhodi, O.; Voineskos, A.N.; Metzer, H.Y.; Lieberman, J.A.; Potkin, S.G.; Remington, G.; Muller, D.J.; Kennedy, J.L. Association study of cannabinoid receptor 1 (CNR1) gene in tardive dyskinesia. Pharmacogenom. J. 2012, 12, 260–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zai, C.C.; Tiwari, A.K.; Mazzoco, M.; de Luca, V.; Muller, D.J.; Shaikh, S.A.; Lohoff, F.W.; Freeman, N.; Voineskos, A.N.; Potkin, S.G.; et al. Association study of the vesicular monoamine transporter gene SLC18A2 with tardive dyskinesia. J. Psychiatr. Res. 2013, 47, 1760–1765. [Google Scholar] [CrossRef] [PubMed]
- Zai, C.C.; Maes, M.S.; Tiwari, A.K.; Zai, G.C.; Remington, G.; Kennedy, J.L. Genetics of tardive dyskinesia: Promising leads and ways forward. J. Neurol. Sci. 2018, 389, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Zai, C.C.; Tiwari, A.K.; Zai, G.C.; Maes, M.S.; Kennedy, J.L. New findings in pharmacogenetics of schizophrenia. Curr. Opin. Psychiatry 2018, 31, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.Y.; Tiwari, A.K.; Zai, G.C.; Rastogi, A.; Shaikh, S.A.; Muller, D.J.; Voineskos, A.N.; Potkin, S.G.; Lieberman, J.A.; Meltzer, H.Y.; et al. Association study of Disrupted-In-Schizophrenia-1 gene variants and tardive dyskinesia. Neurosci. Lett. 2018, 686, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Hongkaew, Y.; Medhasi, S.; Pasomsub, E.; Ngamsamut, N.; Puangpetch, A.; Vanwong, N.; Chamnanphon, M.; Limsila, P.; Suthiasisang, C.; Wilffert, B.; et al. UGT1A1 polymorphisms associated with prolactin response in risperidone-treated children and adolescents with autism spectrum disorder. Pharmacogenom. J. 2018, 18, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Manu, P.; Dima, L.; Shulman, M.; Vancampfort, D.; De Hert, M.; Correll, C.U. Weight gain and obesity in schizophrenia: Epidemiology, pathobiology, and management. Acta Psychiatr. Scand. 2015, 132, 97–108. [Google Scholar] [CrossRef]
- Chan, L.F.; Zai, C.; Monda, M.; Potkin, S.; Kennedy, J.L.; Remington, G.; Lieberman, J.; Meltzer, H.Y.; De Luca, V. Role of ethnicity in antipsychotic-induced weight gain and tardive dyskinesia: Genes or environment? Pharmacogenomics 2013, 14, 1273–1281. [Google Scholar] [CrossRef]
- Corfitsen, H.T.; Krantz, B.; Larsen, A.; Drago, A. Molecular pathway analysis associates alterations in obesity-related genes and antipsychotic-induced weight gain. Acta Neuropsychiatr. 2019, 17, 1–12. [Google Scholar] [CrossRef]
- Xie, C.; Wang, Z.C.; Liu, X.F.; Wang, L.; Yang, M.S. Association between schizophrenia and single nucleotide polymorphisms in lipoprotein lipase gene in a Han Chinese population. Psychiatr. Genet. 2011, 21, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, A.; Li, J.; Meltzer, H.Y. A functional HTR1A polymorphism, rs6295, predicts short-term response to lurasidone: Confirmation with meta-analysis of other antipsychotic drugs. Pharmacogenom. J. 2020, 20, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Kohlrausch, F.B.; Severino-Gama, C.; Lobato, M.I.; Belmonte-de-Abreu, P.; Carracedo, A.; Hutz, M.H. The CYP1A2 -163C>A polymorphism is associated with clozapine-induced generalized tonic-clonic seizures in Brazilian schizophrenia patients. Psychiatry Res. 2013, 209, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Schuhmacher, A.; Becker, T.; Rujescu, D.; Quednow, B.B.; Lennertz, L.; Wagner, M.; Benninghoff, J.; Rietschel, M.; Hafner, H.; Franke, P.; et al. Investigation of tryptophan hydroxylase 2 (TPH2) in schizophrenia and in the response to antipsychotics. J. Psychiatr. Res. 2012, 46, 1073–1080. [Google Scholar] [CrossRef] [Green Version]
- Chi, S.; Wang, C.; Jiang, T.; Zhu, X.C.; Yu, J.T.; Tan, L. The prevalence of depression in Alzheimer’s disease: A systematic review and meta-analysis. Curr. Alzheimer Res. 2015, 12, 189–198. [Google Scholar] [CrossRef]
- Kuring, J.K.; Mathias, J.L.; Ward, L. Prevalence of Depression, Anxiety and PTSD in People with Dementia: A Systematic Review and Meta-Analysis. Neuropsychol. Rev. 2018, 28, 393–416. [Google Scholar] [CrossRef]
- Sol, K.; Zaheed, A.B.; Kraal, A.Z.; Sharifian, N.; Arce Rentería, M.; Zahodne, L.B. Psychological Predictors of Memory Decline in a Racially and Ethnically Diverse Longitudinal Sample of Older Adults in the United States. Int. J. Geriatr. Psychiatry 2019. [Google Scholar] [CrossRef]
- Bennett, S.; Thomas, A.J. Depression and dementia: Cause, consequence or coincidence? Maturitas 2014, 79, 184–190. [Google Scholar] [CrossRef]
- Norton, J.; Carrière, I.; Pérès, K.; Gabelle, A.; Berr, C.; Ritchie, K.; Ancelin, M.L. Sex-specific depressive symptoms as markers of pre-Alzheimer dementia: Findings from the Three-City cohort study. Transl. Psychiatry 2019, 9, 291. [Google Scholar] [CrossRef] [Green Version]
- Youn, H.; Lee, S.; Han, C.; Kim, S.H.; Jeong, H.G. Association between brain amyloid accumulation and neuropsychological characteristics in elders with depression and mild cognitive impairment. Int. J. Geriatr. Psychiatry 2019, 34, 1907–1915. [Google Scholar] [CrossRef] [PubMed]
- Capogna, E.; Manca, R.; De Marco, M.; Hall, A.; Soininen, H.; Venneri, A. Understanding the effect of cognitive/brain reserve and depression on regional atrophy in early Alzheimer’s disease. Postgrad. Med. 2019, 131, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Amieva, H.; Meillon, C.; Proust-Lima, C.; Dartigues, J.F. Is Low Psychomotor Speed a Marker of Brain Vulnerability in Late Life? Digit Symbol Substitution Test in the Prediction of Alzheimer, Parkinson, Stroke, Disability, and Depression. Dement. Geriatr. Cogn. Disord. 2019, 47, 297–305. [Google Scholar] [CrossRef]
- Fischer, C.E.; Kortebi, I.; Karameh, W.K.; Kumar, S.; Gallagher, D.; Golas, A.; Munoz, D.; Barfett, J.; Butter, M.A.; Bowie, C.R.; et al. Examining the Link Between Cardiovascular Risk Factors and Neuropsychiatric Symptoms in Mild Cognitive Impairment and Major Depressive Disorder in Remission. J. Alzheimers Dis. 2019, 67, 1305–1311. [Google Scholar] [CrossRef]
- Marshe, V.S.; Islam, F.; Maciukiewicz, M.; Bousman, C.; Eyre, H.A.; Lavretsky, H.; Mulsant, B.H.; Reynolds, C.F.; Lenze, E.J.; Müller, D.J. Pharmacogenetic Implications for Antidepressant Pharmacotherapy in Late-Life Depression: A Systematic Review of the Literature for Response, Pharmacokinetics and Adverse Drug Reactions. Am. J. Geriatr. Psychiatry. 2020. [Google Scholar] [CrossRef]
- Banning, L.C.P.; Ramakers, I.H.G.B.; Deckers, K.; Verhey, F.R.J.; Aalten, P. Apolipoprotein E and affective symptoms in mild cognitive impairment and Alzheimer’s disease dementia: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2019, 96, 302–315. [Google Scholar] [CrossRef] [PubMed]
- Ni, H.; Xu, M.; Zhan, G.L.; Fan, Y.; Zhou, H.; Jiang, H.Y.; Lu, W.H.; Tan, L.; Zhang, D.F.; Yao, Y.G.; et al. The GWAS Risk Genes for Depression May Be Actively Involved in Alzheimer’s Disease. J. Alzheimers Dis. 2018, 64, 1149–1161. [Google Scholar] [CrossRef]
- Burke, A.D.; Goldfarb, D.; Bollam, P.; Khokher, S. Diagnosing and Treating Depression in Patients with Alzheimer’s Disease. Neurol. Ther. 2019, 8, 325–350. [Google Scholar] [CrossRef] [Green Version]
- Orgeta, V.; Tabet, N.; Nilforooshan, R.; Howard, R. Efficacy of Antidepressants for Depression in Alzheimer’s Disease: Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2017, 58, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Cassano, T.; Calcagnini, S.; Carbone, A.; Bukke, V.N.; Orkisz, S.; Villani, R.; Romano, A.; Avolio, C.; Gaetani, S. Pharmacological Treatment of Depression in Alzheimer’s Disease: A Challenging Task. Front. Pharmacol. 2019, 10, 1067. [Google Scholar] [CrossRef] [Green Version]
- Cacabelos, R. Trial-and-Error versus Personalized Treatment in Depression: The Power of Pharmacogenomics. J. Psychiatry Depress Anxiety 2016, 2. [Google Scholar] [CrossRef] [Green Version]
- Torrellas, C.; Carril, J.C.; Cacabelos, R. Optimization of antidepressant use with pharmacogenetic strategies. Curr. Genom. 2017, 18, 442–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thase, M.E.; Parikh, S.V.; Rothschild, A.J.; Dunlop, B.W.; DeBattista, C.; Conway, C.R.; Mondimore, F.M.; Shelton, R.C.; Macaluso, M.; Li, J.; et al. Impact of Pharmacogenomics on Clinical Outcomes for Patients Taking Medications With Gene-Drug Interactions in a Randomized Controlled Trial. J. Clin. Psychiatry 2019, 80, 19m12910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maggo, S.D.S.; Sycamore, K.L.V.; Miller, A.L.; Kennedy, M.A. The Three Ps: Psychiatry, Pharmacy, and Pharmacogenomics, a Brief Report from New Zealand. Front. Psychiatry 2019, 10, 690. [Google Scholar] [CrossRef] [PubMed]
- Eugene, A.R. Optimizing drug selection in psychopharmacology based on 40 significant CYP2C19- and CYP2D6-biased adverse drug reactions of selective serotonin reuptake inhibitors. PeerJ 2019, 7, e7860. [Google Scholar] [CrossRef] [PubMed]
- Danese, A.; Federico, A.; Martini, A.; Mantovani, E.; Zucchella, C.; Tagliapietra, M.; Tamburin, S.; Cavallaro, T.; Marafioti, V.; Monaco, S.; et al. QTc Prolongation in Patients with Dementia and Mild Cognitive Impairment: Neuropsychological and Brain Imaging Correlations. J. Alzheimers Dis. 2019, 72, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Kanders, S.H.; Pisanu, C.; Bandstein, M.; Jonsson, J.; Castelao, E.; Pistis, G.; Gholam-Rezaee, M.; Eap, C.B.; Preisig, M.; Schioth, H.B.; et al. A pharmacogenetic risk score for the evaluation of major depression severity under treatment with antidepressants. Drug Dev. Res. 2020, 81, 102–113. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira, F.F.; Berretta, J.M.; de Almeida Junior, G.V.; de Almeida, S.S.; Chen, E.S.; Smith, M.C.; Bertolucci, P.H.F. Pharmacogenetic analyses of variations of measures of cardiovascular risk in Alzheimer’s dementia. Indian J. Med. Res. 2019, 150, 261–271. [Google Scholar] [CrossRef]
- Hicks, J.K.; Bishop, J.R.; Gammal, R.S.; Sangkuhl, K.; Bousman, C.A.; Leeder, J.S. A Call for Clear and Consistent Communications Regarding the Role of Pharmacogenetics in Antidepressant Pharmacotherapy. Clin. Pharmacol. Ther. 2019. [Google Scholar] [CrossRef]
- Caudle, K.E.; Sangkuhl, K.; Whirl-Carrillo, M.; Swen, J.J.; Haidar, C.E.; Klein, T.E.; Gammal, R.S.; Relling, M.V.; Scott, S.A.; Hertz, D.L.; et al. Standardizing CYP2D6 Genotype to Phenotype Translation: Consensus Recommendations from the Clinical Pharmacogenetics Implementation Consortium and Dutch Pharmacogenetics Working Group. Clin. Transl. Sci. 2020, 13, 116–124. [Google Scholar] [CrossRef] [Green Version]
- Nofziger, C.; Turner, A.J.; Sangkuhl, K.; Whirl-Carrillo, M.; Agúndez, J.A.G.; Black, J.L.; Dunnenberger, H.M.; Ruano, G.; Kennedy, M.A.; Phillips, M.S.; et al. PharmVar GeneReview: CYP2D. Clin. Pharmacol. Ther. 2020, 107, 154–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagani, R.; Gasparini, A.; Ielmini, M.; Caselli, I.; Poloni, N.; Ferrari, M.; Marino, F.; Callegari, C. Twenty years of Lithium pharmacogenetics: A systematic review. Psychiatry Res. 2019, 278, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Becker, E.; Orellana Rios, C.L.; Lahmann, C.; Rücker, G.; Bauer, J.; Boeker, M. Anxiety as a risk factor of Alzheimer’s disease and vascular dementia. Br. J. Psychiatry 2018, 213, 654–660. [Google Scholar] [CrossRef] [Green Version]
- Santabárbara, J.; Lipnicki, D.M.; Bueno-Notivol, J.; Olaya-Guzmán, B.; Villagrasa, B.; López-Antón, R. Updating the evidence for an association between anxiety and risk of Alzheimer’s disease: A meta-analysis of prospective cohort studies. J. Affect. Disord. 2019, 262, 397–404. [Google Scholar] [CrossRef]
- Baillon, S.; Gasper, A.; Wilson-Morkeh, F.; Pritchard, M.; Jesu, A.; Velayudhan, L. Prevalence and Severity of Neuropsychiatric Symptoms in Early- Versus Late-Onset Alzheimer’s Disease. Am. J. Alzheimers Dis. Other Demen. 2019, 34, 433–438. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, X.; Wang, Y.; Dong, H.; Lu, J.; Scheininger, T.; Ewers, M.; Jesse, F.; Zuo, X.; Han, Y. Anxiety correlates with cortical surface area in subjective cognitive decline: APOE ε4 carriers versus APOE ε4 non-carriers. Alzheimers Res. Ther. 2019, 11, 50. [Google Scholar] [CrossRef]
- Vlachos, G.S.; Cosentino, S.; Kosmidis, M.H.; Anastasiou, C.A.; Yannakoulia, M.; Dardiotis, E.; Hadjigeorgiou, G.; Sakka, P.; Ntanasi, E.; Scarmeas, N. Prevalence and determinants of subjective cognitive decline in a representative Greek elderly population. Int. J. Geriatr. Psychiatry. 2019, 34, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Nafti, M.; Sirois, C.; Kröger, E.; Carmichael, P.H.; Laurin, D. Is Benzodiazepine Use Associated With the Risk of Dementia and Cognitive Impairment-Not Dementia in Older Persons? The Canadian Study of Health and Aging. Ann. Pharmacother. 2020, 54, 219–225. [Google Scholar] [CrossRef]
- Thomas, J.; Overeem, S.; Claassen, J.A.H.R. Long-Term Occupational Sleep Loss and Post-Retirement Cognitive Decline or Dementia. Dement. Geriatr. Cogn. Disord. 2019, 48, 105–112. [Google Scholar] [CrossRef]
- Leng, Y.; Musiek, E.S.; Hu, K.; Cappuccio, F.P.; Yaffe, K. Association between circadian rhythms and neurodegenerative diseases. Lancet Neurol. 2019, 18, 307–318. [Google Scholar] [CrossRef]
- Minakawa, E.N.; Wada, K.; Nagai, Y. Sleep Disturbance as a Potential Modifiable Risk Factor for Alzheimer’s Disease. Int. J. Mol. Sci. 2019, 20, 803. [Google Scholar] [CrossRef] [Green Version]
- Duncan, M.J. Interacting influences of aging and Alzheimer’s disease on circadian rhythms. Eur. J. Neurosci. 2020, 51, 310–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yesavage, J.A.; Noda, A.; Heath, A.; McNerney, M.W.; Domingue, B.W.; Hernandez, Y.; Benson, G.; Hallmayer, J.; O’Hara, R.; Williams, L.M.; et al. Sleep-wake disorders in Alzheimer’s disease: Further genetic analyses in relation to objective sleep measures. Int. Psychogeriatr. 2019, 1–7. [Google Scholar] [CrossRef]
- Wu, M.; Zhou, F.; Cao, X.; Yang, J.; Bai, Y.; Yan, X.; Cao, J.; Qi, J. Abnormal circadian locomotor rhythms and Per gene expression in six-month-old triple transgenic mice model of Alzheimer’s disease. Neurosci. Lett. 2018, 676, 13–18. [Google Scholar] [CrossRef]
- Rainey-Smith, S.R.; Mazzucchelli, G.N.; Villemagne, V.L.; Brown, B.M.; Porter, T.; Weinborn, M.; Bucks, R.S.; Milicic, L.; Sohrabi, H.R.; Taddei, K.; et al. Genetic variation in Aquaporin-4 moderates the relationship between sleep and brain Aβ-amyloid burden. Transl. Psychiatry 2018, 8, 47. [Google Scholar] [CrossRef] [Green Version]
- Martin, S.C.; Monroe, S.K.; Diering, G.H. Homer1a and mGluR1/5 Signaling in Homeostatic Sleep Drive and Output. Yale J. Biol. Med. 2019, 92, 93–101. [Google Scholar]
- Manni, R.; Cremascoli, R.; Perretti, C.; De Icco, R.; Picascia, M.; Ghezzi, C.; Cerri, S.; Sinforiani, E.; Terzaghi, M. Evening melatonin timing secretion in real life conditions in patients with Alzheimer disease of mild to moderate severity. Sleep Med. 2019, 63, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, A.K.; Mallick, B.N. Association between autophagy and rapid eye movement sleep loss-associated neurodegenerative and patho-physio-behavioral changes. Sleep Med. 2019, 63, 29–37. [Google Scholar] [CrossRef]
- You, J.C.; Jones, E.; Cross, D.E.; Lyon, A.C.; Kang, H.; Newberg, A.B.; Lippa, C.F. Association of β-Amyloid Burden With Sleep Dysfunction and Cognitive Impairment in Elderly Individuals With Cognitive Disorders. JAMA Netw. Open 2019, 2, e1913383. [Google Scholar] [CrossRef]
- Wang, C.; Holtzman, D.M. Bidirectional relationship between sleep and Alzheimer’s disease: Role of amyloid, tau, and other factors. Neuropsychopharmacology 2020, 45, 104–120. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Liu, P.; Wei, M.; Li, Y.; Liu, J.; Ma, L.; Shang, S.; Jiang, Y.; Huo, K.; Wang, J.; et al. Chronic Sleep Restriction Induces Aβ Accumulation by Disrupting the Balance of Aβ Production and Clearance in Rats. Neurochem. Res. 2019, 44, 859–873. [Google Scholar] [CrossRef]
- Zhang, F.; Zhong, R.; Li, S.; Fu, Z.; Wang, R.; Wang, T. Alteration in sleep architecture and electroencephalogram as an early sign of Alzheimer’s disease preceding the disease pathology and cognitive decline. Alzheimers Dement. 2019, 15, 590–597. [Google Scholar] [CrossRef]
- Taillard, J.; Sagaspe, P.; Berthomier, C.; Brandewinder, M.; Amieva, H.; Dartigues, J.F.; Rainfrau, M.; Harston, S.; Micoulaud-Franchi, J.A.; Philip, P. Non-REM Sleep Characteristics Predict Early Cognitive Impairment in an Aging Population. Front. Neurol. 2019, 10, 197. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Wang, F.; Tang, M.; Zhao, Y.; Wang, X. Amyloid β and tau are involved in sleep disorder in Alzheimer’s disease by orexin A and adenosine A(1) receptor. Int. J. Mol. Med. 2019, 43, 435–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herring, W.J.; Roth, T.; Krystal, A.D.; Michelson, D. Orexin receptor antagonists for the treatment of insomnia and potential treatment of other neuropsychiatric indications. J. Sleep Res. 2019, 28, e12782. [Google Scholar] [CrossRef] [PubMed]
- Nicastro, N.; Assal, F.; Seeck, M. From here to epilepsy: The risk of seizure in patients with Alzheimer’s disease. Epileptic Disord. 2016, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- von Rüden, E.L.; Zellinger, C.; Gedon, J.; Walker, A.; Bierling, V.; Deeg, C.A. Regulation of Alzheimer’s Disease-Associated Proteins During the Course of Epileptogenesis: Differential Proteomic Analysis in a Rat Model. Neuroscience 2020, 424, 102–120. [Google Scholar] [CrossRef]
- Zelano, J.; Brigo, F.; Garcia-Patek, S. Increased risk of epilepsy in patients registered in the Swedish Dementia Registry. Eur. J. Neurol. 2020, 27, 129–135. [Google Scholar] [CrossRef]
- Tábuas-Pereira, M.; Durães, J.; Lopes, J.; Sales, F.; Bento, C.; Duro, D.; Santiago, B.; Almeida, M.R.; Leitao, M.J.; Balderias, I.; et al. Increased CSF tau is associated with a higher risk of seizures in patients with Alzheimer’s disease. Epilepsy Behav. 2019, 98, 207–209. [Google Scholar] [CrossRef]
- Zhou, X.; Tao, H.; Cai, Y.; Cui, L.; Zhao, B.; Li, K. Stage-dependent involvement of ADAM10 and its significance in epileptic seizures. J. Cell Mol. Med. 2019, 23, 4494–4504. [Google Scholar] [CrossRef] [Green Version]
- Gan, J.; Cai, Q.; Galer, P.; Mas, D.; Chen, X.; Huang, J.; Bao, S.; Luo, R. Mapping the knowledge structure and trends of epilepsy genetics over the past decade: A co-word analysis based on medical subject headings terms. Medicine 2019, 98, e16782. [Google Scholar] [CrossRef] [PubMed]
- Al-Eitan, L.N.; Al-Dalalah, I.M.; Mustafa, M.M.; Alghamdi, M.A.; Elshammari, A.K.; Khreisat, W.H.; Aljamal, H.A. Effects of MTHFR and ABCC2 gene polymorphisms on antiepileptic drug responsiveness in Jordanian epileptic patients. Pharmgenom. Personalized Med. 2019, 12, 87–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vossel, K.A.; Tartaglia, M.C.; Nygaard, H.B.; Zeman, A.Z.; Miller, B.L. Epileptic activity in Alzheimer’s disease: Causes and clinical relevance. Lancet Neurol. 2017, 16, 311–322. [Google Scholar] [CrossRef] [Green Version]
- Giorgi, F.S.; Guida, M.; Vergallo, A.; Bonuccelli, U.; Zaccara, G. Treatment of epilepsy in patients with Alzheimer’s disease. Expert Rev. Neurother. 2017, 17, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Thijs, R.D.; Surges, R.; O’Brien, T.J.; Sander, J.W. Epilepsy in adults. Lancet 2019, 393, 689–701. [Google Scholar] [CrossRef]
- He, Z.W.; Qu, J.; Zhang, Y.; Mao, C.X.; Wang, Z.B.; Mao, X.Y.; Deng, Z.; Zhou, B.; Yin, J.; Long, H.; et al. PRRT2 mutations are related to febrile seizures in epileptic patients. Int. J. Mol. Sci. 2014, 15, 23408–23417. [Google Scholar] [CrossRef]
- Haerian, B.S.; Baum, L.; Kwan, P.; Cherry, S.S.; Shin, J.G.; Kim, S.E. Contribution of GABRG2 polymorphisms to risk of epilepsy and febrile seizure: A multicenter cohort study and meta-analysis. Mol. Neurobiol. 2016, 53, 5457–5467. [Google Scholar] [CrossRef]
- Zhu, M.M.; Li, H.L.; Shi, L.H.; Chen, X.P.; Luo, J.; Zhang, Z.L. The pharmacogenomics of valproic acid. J. Hum. Genet. 2017, 62, 1009–1014. [Google Scholar] [CrossRef]
- Zhu, X.; Yun, W.; Sun, X.; Qiu, F.; Zhao, L.; Guo, Y. Effects of major transporter and metabolizing enzyme gene polymorphisms on carbamazepine metabolism in Chinese patients with epilepsy. Pharmacogenomics 2014, 15, 1867–1879. [Google Scholar] [CrossRef]
- Wang, P.; Lin, X.Q.; Cai, W.K.; Xu, G.L.; Zhou, M.D.; Yang, M.; He, G.H. Effect of UGT2B7 genotypes on plasma concentration of valproic acid: A meta-analysis. Eur. J. Clin. Pharmacol. 2018, 74, 433–442. [Google Scholar] [CrossRef]
- Hung, C.C.; Ho, J.L.; Chang, W.L.; Tai, J.J.; Hsieh, T.J.; Liou, H.H. Association of genetic variants in six candidate genes with valproic acid therapy optimization. Pharmacogenomics 2011, 12, 1107–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balestrini, S.; Sisodiya, S.M. Pharmacogenomics in epilepsy. Neurosci. Lett. 2018, 667, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhang, J.; Wu, X.; Yan, H.; Zhang, Y.; He, R.H.; Tang, Y.J.; He, Y.J.; Tan, D.; Mao, X.Y.; et al. Polymorphisms of ABAT, SCN2A and ALDH5A1 may affect valproic acid responses in the treatment of epilepsy in Chinese. Pharmacogenomics 2016, 17, 2007–2014. [Google Scholar] [CrossRef] [PubMed]
- Noai, M.; Soraoka, H.; Kajiwara, A.; Tanamachi, Y.; Oniki, K.; Nakagawa, K.; Ishitsu, T.; Saruwatari, J. Cytochrome P450 2C19 polymorphisms and valproic acid-induced weight gain. Acta Neurol. Scand. 2016, 133, 216–223. [Google Scholar] [CrossRef]
- Li, H.; Wang, X.; Zhou, Y.; Zhou, Y.; Ni, G.; Su, Q.; Chen, Z.; Chen, Z.; Li, J.; Chen, X.; et al. Association of LEPR and ANKK1 Gene Polymorphisms with Weight Gain in Epilepsy Patients Receiving Valproic Acid. Int. J. Neuropsychopharmacol. 2015, 18, pyv021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, S.; Chen, Y.; Zhao, M.; Guo, Y.; Wang, Z.; Zhao, L. Population pharmacokinetics of valproic acid in epileptic children: Effects of clinical and genetic factors. Eur. J. Pharm. Sci. 2018, 122, 170–178. [Google Scholar] [CrossRef]
- Wen, Z.P.; Fan, S.S.; Du, C.; Yin, T.; Zhou, B.T.; Peng, Z.F.; Xie, X.Y.; Zhang, W.; Chen, Y.; Tang, J.; et al. Influence of acylpeptide hydrolase polymorphisms on valproic acid level in Chinese epilepsy patients. Pharmacogenomics 2016, 17, 1219–1225. [Google Scholar] [CrossRef]
- Li, Q.; Li, Q.Q.; Jia, J.N.; Cao, S.; Wang, Z.B.; Wang, X. Sodium valproate ameliorates neuronal apoptosis in a kainic acid model of epilepsy via enhancing PKC-dependent GABAAR γ2 serine 327 phosphorylation. Neurochem. Res. 2018, 43, 2343–2352. [Google Scholar] [CrossRef] [PubMed]
- Ogusu, N.; Saruwatari, J.; Nakashima, H.; Noai, M.; Nishimura, M.; Deguchi, M.; Oniki, K.; Yasui-Furokori, N.; Kaneko, S.; Ishitsu, T.; et al. Impact of the superoxide dismutase 2 Val16Ala polymorphism on the relationship between valproic acid exposure and elevation of γ-glutamyltransferase in patients with epilepsy: A population pharmacokinetic-pharmacodynamic analysis. PLoS ONE 2014, 9, e111066. [Google Scholar] [CrossRef] [PubMed]
- Shirzadi, M.; Reimers, A.; Helde, G.; Sjursen, W.; Brodtkorb, E. No association between non-bullous skin reactions from lamotrigine and heterozygosity of UGT1A4 genetic variants *2(P24T) or *3(L48V) in Norwegian patients. Seizure 2017, 45, 169–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Xu, S.; Wang, Z.; Zhao, M.; Wang, H.; Lu, T.; Zhao, L. A population Pharmacokinetic-Pharmacogenetic model of lamotrigine in Chinese children with epilepsy. Ther. Drug Monit. 2018, 40, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.H.; Zhang, Y.X.; Lu, R.Y.; Jin, B.; Wang, S.; Liu, Z.R.; Tang, Y.L.; Ding, M.P. Specific OCT1 and ABCG2 polymorphisms are associated with Lamotrigine concentrations in Chinese patients with epilepsy. Epilepsy Res. 2016, 127, 186–190. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, X.; Li, H.; Zhang, J.; Chen, Z.; Xie, W.; Zhang, J.; Li, J.; Zhou, L.; Huang, M. Polymorphisms of ABCG2, ABCB1 and HNF4α are associated with Lamotrigine trough concentrations in epilepsy patients. Drug Metab. Pharmacokinet. 2015, 30, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Phillips, E.J.; Sukasem, C.; Whirl-Carrillo, M.; Müller, D.J.; Dunnenberger, H.M.; Chantratita, W.; Goldspiel, B.; Chen, Y.T.; Carleton, B.C. Clinical Pharmacogenetics Implementation Consortium Guideline for HLA Genotype and Use of Carbamazepine and Oxcarbazepine: 2017 Update. Clin. Pharmacol. Ther. 2018, 103, 574–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Yu, Y.; Nie, X.; Zhao, L.; Wang, X. Association between HLA-B*15:02 and oxcarbazepine-induced cutaneous adverse reaction: A meta-analysis. Pharmacogenomics 2018, 19, 547–552. [Google Scholar] [CrossRef]
- Cheung, Y.K.; Cheng, S.H.; Chan, E.J.; Lo, S.V.; Ng, M.H.; Kwan, P. HLA-B alleles associated with severe cutaneous reactions to antiepileptic drugs in Han Chinese. Epilepsia 2013, 54, 1307–1314. [Google Scholar] [CrossRef]
- Aoki, M.; Hosono, N.; Takata, S.; Nsksmura, Y.; Kamatani, N.; Kubo, M. New pharmacogenetic test for detecting an HLA-A*31: 01 allele using the InvaderPlus assay. Pharmacogenet. Genom. 2012, 22, 441–446. [Google Scholar] [CrossRef]
- Simper, G.S.; Gräser, L.S.; Celik, A.A.; Kuhn, J.; Kunze-Schumacher, H.; Hò, G.T. The Mechanistic Differences in HLA-Associated Carbamazepine Hypersensitivity. Pharmaceutics 2019, 11, 536. [Google Scholar] [CrossRef] [Green Version]
- Zhou, B.T.; Zhou, Q.H.; Yin, J.Y.; Li, G.L.; Qu, J.; Xu, X.J.; Liu, D.; Zhou, H.H.; Liu, Z.Q. Effects of SCN1A and GABA receptor genetic polymorphisms on carbamazepine tolerability and efficacy in Chinese patients with partial seizures: 2-year longitudinal clinical follow-up. CNS Neurosci. Ther. 2012, 18, 566–572. [Google Scholar] [CrossRef]
- Shen, C.; Zhang, B.; Liu, Z.; Tang, Y.; Zhang, Y.; Wang, S.; Guo, Y.; Ding, Y.; Wang, S.; Ding, M. Effects of ABCB1, ABCC2, UGT2B7 and HNF4α genetic polymorphisms on oxcarbazepine concentrations and therapeutic efficacy in patients with epilepsy. Seizure 2017, 51, 102–106. [Google Scholar] [CrossRef] [Green Version]
- Djordjevic, N.; Jankovic, S.M.; Milovanovic, J.R. Pharmacokinetics and Pharmacogenetics of Carbamazepine in Children. Eur. J. Drug Metab. Pharmacokinet. 2017, 42, 729–744. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Yin, T.; Ma, H.Y.; Liu, D.Q.; Sheng, Y.H.; Wang, C.; Zhou, B.T. Effects of CYP3A4/5 and ABCB1 genetic polymorphisms on carbamazepine metabolism and transport in Chinese patients with epilepsy treated with carbamazepine in monotherapy and bitherapy. Epilepsy Res. 2015, 117, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.L.; Jiao, Z.; Wu, X.Y.; Hong, Z.; Wu, Z.Y.; Zhong, M.K. Association between PK/PD-involved gene polymorphisms and carbamazepine-individualized therapy. Pharmacogenomics 2015, 16, 1499–1512. [Google Scholar] [CrossRef]
- Ma, C.L.; Wu, X.Y.; Jiao, Z.; Hong, Z.; Wu, Z.Y.; Zhong, M.K. SCN1A, ABCC2 and UGT2B7 gene polymorphisms in association with individualized oxcarbazepine therapy. Pharmacogenomics 2015, 16, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.C.; Chang, W.L.; Ho, J.L.; Tai, J.J.; Hsieh, T.J.; Huang, H.C.; Hsieh, Y.; Liou, H. Association of polymorphisms in EPHX1, UGT2B7, ABCB1, ABCC2, SCN1A and SCN2A genes with carbamazepine therapy optimization. Pharmacogenomics 2012, 13, 159–169. [Google Scholar] [CrossRef]
- Hung, C.C.; Huang, H.C.; Gao, Y.H.; Chang, W.L.; Ho, J.L.; Chiou, M.H.; Hsieh, Y.W.; Liou, H.H. Effects of polymorphisms in six candidate genes on phenytoin maintenance therapy in Han Chinese patients. Pharmacogenomics 2012, 13, 1339–1349. [Google Scholar] [CrossRef]
- Chung, W.H.; Chang, W.C.; Lee, Y.S.; Wu, Y.Y.; Yang, C.H.; Ho, H.C.; Chen, M.J.; Lin, J.Y.; Hui, R.C.; Ho, J.C.; et al. Genetic variants associated with phenytoin-related severe cutaneous adverse reactions. JAMA 2014, 312, 525–534. [Google Scholar] [CrossRef] [Green Version]
- McCormack, M.; Gui, H.; Ingason, A.; Speed, D.; Wright, G.E.B.; Zhang, E.J.; Secolin, R.; Yasuda, C.; Kwok, M.; Wolkings, S.; et al. Genetic variation in CFH predicts phenytoin-induced maculopapular exanthema in European-descent patients. Neurology 2018, 90, e332–e341. [Google Scholar] [CrossRef] [Green Version]
- Glauser, T.A.; Holland, K.; O’Brien, V.P.; Keddache, M.; Martin, L.J.; Clark, P.O.; Cnaan, A.; Dlugos, D.; Hirtz, D.G.; Shinnar, S.; et al. Pharmacogenetics of antiepileptic drug efficacy in childhood absence epilepsy. Ann. Neurol. 2017, 81, 444–453. [Google Scholar] [CrossRef]
- Rogawski, M.A. The intrinsic severity hypothesis of pharmacoresistance to antiepileptic drugs. Epilepsia 2013, 54, 33–40. [Google Scholar] [CrossRef]
- Haerian, B.S.; Roslan, H.; Raymond, A.A.; Tan, C.T.; Lim, K.S.; Zulkifli, S.Z.; Mohamed, E.H.; Tan, H.J.; Mohamed, Z. ABCB1 C3435T polymorphism and the risk of resistance to antiepileptic drugs in epilepsy: A systematic review and meta-analysis. Seizure 2010, 19, 339–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajmi, M.; Boujaafar, S.; Zouari, N.; Amor, D.; Nasr, A.; Rejeb, N.B.; Amor, S.B.; Omezzine, A.; Benammou, S.; Bouslama, A. Association between ABCB1 polymorphisms and response to first-generation antiepileptic drugs in a Tunisian epileptic population. Int. J. Neurosci. 2018, 128, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Qu, J.; Zhou, B.T.; Yin, J.Y.; Xu, X.J.; Zhao, Y.C.; Lei, G.H.; Tang, Q.; Zhou, H.H.; Liu, Z.Q. ABCC2 polymorphisms and haplotype are associated with drug resistance in Chinese epileptic patients. CNS Neurosci. Ther. 2012, 18, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Lv, N.; Qu, J.; Long, H.; Zhou, L.; Cao, Y.; Long, L.; Liu, Z.; Xiao, B. Association study between polymorphisms in the CACNA1A, CACNA1C, and CACNA1H genes and drug-resistant epilepsy in the Chinese Han population. Seizure 2015, 30, 64–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daci, A.; Bozalija, A.; Jashari, F.; Krasniqi, S. Individualizing treatment approaches for epileptic patients with glucose transporter type1 (GLUT-1) deficiency. Int. J. Mol. Sci. 2018, 19, 122. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.L.; Wu, X.Y.; Zheng, J.; Wu, Z.Y.; Hong, Z.; Zhong, M.K. Association of SCN1A, SCN2A and ABCC2 gene polymorphisms with the response to antiepileptic drugs in Chinese Han patients with epilepsy. Pharmacogenomics 2014, 15, 1323–1336. [Google Scholar] [CrossRef] [PubMed]
- Sha’ari, H.M.; Haerian, B.S.; Baum, L.; Saruwatari, J.; Tan, H.J.; Rafia, M.H.; Ali, R.A.; Kwan, P.; Ishitu, T.; Nakagawa, K.; et al. ABCC2 rs2273697 and rs3740066 polymorphisms and resistance to antiepileptic drugs in Asia Pacific epilepsy cohorts. Pharmacogenomics 2014, 15, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Lotte, J.; Bast, T.; Borusiak, P.; Coppola, A.; Cross, J.H.; Dimova, P. Effectiveness of antiepileptic therapy in patients with PCDH19 mutations. Seizure 2016, 35, 106–110. [Google Scholar] [CrossRef] [Green Version]
- Kouga, T.; Shimbo, H.; Iai, M.; Yamashita, S.; Ishii, A.; Ihara, Y.; Hirose, S.; Yamakawa, K.; Osaka, H. Effect of CYP2C19 polymorphisms on stiripentol administration in Japanese cases of Dravet syndrome. Brain Dev. 2015, 37, 243–249. [Google Scholar] [CrossRef]
- Hung, C.C.; Chen, P.L.; Huang, W.M.; Tai, J.J.; Hsieh, T.J.; Ding, S.T.; Hsieh, Y.W.; Liou, H.H. Gene-wide tagging study of the effects of common genetic polymorphisms in the α subunits of the GABA(A) receptor on epilepsy treatment response. Pharmacogenomics 2013, 14, 1849–1856. [Google Scholar] [CrossRef]
- Kickinger, S.; Hellsberg, E.; Frølund, B.; Schousboe, A.; Ecker, G.F.; Wellendorph, P. Structural and molecular aspects of betaine-GABA transporter 1 (BGT1) and its relation to brain function. Neuropharmacology 2019, 161, 107644. [Google Scholar] [CrossRef] [PubMed]
- Heath, L.; Gray, S.L.; Boudreau, D.M.; Thummel, K.; Edwards, K.L.; Fullerton, S.M.; Crane, P.K.; Larson, E.B. Cumulative antidepressant use and risk of dementia in a prospective cohort study. J. Am. Geriatr. Soc. 2018, 66, 1948–1955. [Google Scholar] [CrossRef]
- Kirgaval, R.S.; Revanakar, S.; Srirangapattna, C. Prevalence of extrapyramidal side effects in patients on antipsychotics drugs at a Tertiary Care Center. J. Psychiatry 2017, 20, 419. [Google Scholar] [CrossRef]
- Patterson, S.M.; Hughes, C.M.; Crealey, G.; Cardwell, C.; Lapane, K.L. An evaluation of an adapted U.S. model of pharmaceutical care to improve psychoactive prescribing for nursing home residents in Northern Ireland (Fleetwood Northern Ireland study). J. Am. Geriatr. Soc. 2010, 58, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Barber, N.D.; Alldred, D.P.; Raynor, D.K.; Dickinson, R.; Garfield, S.; Jesson, B.; Lim, R.; Savagem, I.; Standage, C.; Buckle, P.; et al. Care homes’ use of medicines study: Prevalence, causes and potential harm of medication errors in care homes for older people. Qual. Saf. Health Care 2009, 18, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.M.; Lapane, K.L. Pharmacy interventions on prescribing in nursing homes: From evidence to practice. Ther. Adv. Drug Saf. 2011, 2, 103–112. [Google Scholar] [CrossRef]
- Eshetie, T.C.; Nguyen, T.A.; Gillam, M.H.; Kalisch Ellett, L.M. Potentially inappropriate prescribing in people with dementia: An Australian population-based study. Int. J. Geriatr. Psychiatry 2019, 34, 1498–1505. [Google Scholar] [CrossRef]
- Bernal, C.J.; Aka, I.; Carroll, R.J.; Coco, J.R.; Lima, J.J.; Acra, S.A.; Roden, D.M.; Van Driest, S.L. CYP2C19 Phenotype and Risk of Proton Pump Inhibitor-Associated Infections. Pediatrics 2019, 144, e20190857. [Google Scholar] [CrossRef]
- Mega, J.L.; Walker, J.R.; Ruff, C.T.; Vandell, A.G.; Nordio, F.; Deenadayalu, N.; Murphy, S.A.; Lee, J.; Mercuri, M.F.; Giugliano, R.P.; et al. Genetics and the clinical response to warfarin and edoxaban: Findings from the randomised, double-blind ENGAGE AF-TIMI 48 trial. Lancet 2015, 385, 2280–2287. [Google Scholar] [CrossRef]
- Chen, W.; Wu, L.; Liu, X.; Shen, Y.; Liang, Y.; Zhu, J.; Tan, H.; Yang, Y.; Liu, Q.; Wang, M.; et al. Warfarin dose requirements with different genotypes of CYP2C9 and VKORC1 for patients with atrial fibrillation and valve replacement. Int. J. Clin. Pharmacol. Ther. 2017, 55, 126–132. [Google Scholar] [CrossRef]
- Kamali, X.; Wulasihan, M.; Yang, Y.C.; Lu, W.H.; Liu, Z.Q.; He, P.Y. Association of GGCX gene polymorphism with warfarin dose in atrial fibrillation population in Xinjiang. Lipids Health Dis. 2013, 12, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magvanjav, O.; McDonough, C.W.; Gong, Y.; McClure, L.A.; Talbert, R.L.; Horenstein, R.B.; Shuldiner, A.R.; Benavente, O.R.; Mitchell, B.D.; Johnson, J.A.; et al. Pharmacogenetic associations of β1-adrenergic receptor polymorphisms with cardiovascular outcomes in the SPS3 Trial (Secondary Prevention of Small Subcortical Strokes). Stroke 2017, 48, 1337–1343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, X.; Zhou, Q.; Wang, C.; Lin, J.; Liu, P.; Fu, C. Platelet receptor Gene (P2Y12, P2Y1) and platelet glycoprotein Gene (GPIIIa) polymorphisms are associated with antiplatelet drug responsiveness and clinical outcomes after acute minor ischemic stroke. Eur. J. Clin. Pharmacol. 2017, 73, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, I.F.; Vazquez, A.I.; Irvin, M.R.; Sørensen, P.; Davis, B.R.; Ford, C.E.; Boerwinkle, E.; Eckfeldt, J.H.; Arnett, D.K. Pharmacogenetic effects of ‘candidate gene complexes’ on stroke in the GenHAT study. Pharmacogenet. Genom. 2014, 24, 556–563. [Google Scholar] [CrossRef] [Green Version]
- Sychev, D.; Minnigulov, R.; Bochkov, P.; Ryzhikova, K.; Yudina, I.; Lychagin, A.; Morozova, T. Effect of CYP3A4, CYP3A5, ABCB1 Gene Polymorphisms on Rivaroxaban Pharmacokinetics in Patients Undergoing Total Hip and Knee Replacement Surgery. High Blood Press. Cardiovasc. Prev. 2019, 26, 413–420. [Google Scholar] [CrossRef]
- McDonough, C.W.; McClure, L.A.; Mitchell, B.D.; Gong, Y.; Horenstein, R.B.; Lewis, J.P.; Lewis, J.P.; Field, T.S.; Talbert, R.L.; Benavente, O.R.; et al. CYP2C19 metabolizer status and clopidogrel efficacy in the Secondary Prevention of Small Subcortical Strokes (SPS3) study. J. Am. Heart Assoc. 2015, 4, e001652. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Zhou, Y.; Pan, Y.; Zhao, X.; Liu, L.; Wang, D.; Li, H.; Johnston, S.C.; Meng, X.; Wang, Y.; et al. Impact of CYP2C19 polymorphism in prognosis of minor stroke or TIA patients with declined eGFR on dual antiplatelet therapy: CHANCE substudy. Pharmacogenom. J. 2018, 18, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Duconge, J.; Hernandez-Suarez, D.F. Potential usefulness of clopidogrel Pharmacogenetics in cerebral endovascular procedures and carotid artery stenting. Curr. Clin. Pharmacol. 2017, 12, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapedanovska-Nestorovska, A.; Dimovski, A.J.; Sterjev, Z.; Matevska-Geskovska, N.; Suturkova, L.; Ugurov, P.; Mitrev, Z.; Rosalia, R. The AKR1D1*36 (rs1872930) allelic variant is independently associated with clopidogrel treatment outcome. Pharmacogenom. Personalized Med. 2019, 12, 287–295. [Google Scholar] [CrossRef] [Green Version]
- Gallego-Fabrega, C.; Carrera, C.; Reny, J.L.; Fontana, P.; Slowik, A.; Pera, J.; Pezzini, A.; Serrano-Heras, G.; Segura, T.; Martí-Fábregas, J.; et al. TRAF3 epigenetic regulation is associated with vascular recurrence in patients with ischemic stroke. Stroke 2016, 47, 1180–1186. [Google Scholar] [CrossRef]
- Kampouraki, E.; Kamali, F. Pharmacogenetics of anticoagulants used for stroke prevention in patients with atrial fibrillation. Expert Opin. Drug Metab. Toxicol. 2019, 15, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Miller-Rhodes, P.; Kong, C.; Baht, G.S.; Saminathan, P.; Rodriguiz, R.M.; Wetsel, W.; Gelbard, H.A.; Terrando, N. The broad spectrum mixed-lineage kinase 3 inhibitor URMC-099 prevents acute microgliosis and cognitive decline in a mouse model of perioperative neurocognitive disorders. J. Neuroinflamm. 2019, 16, 193. [Google Scholar] [CrossRef] [Green Version]
- Ettienne, E.B.; Ofoegbu, A.; Maneno, M.K.; Briggs, J.; Ezeude, G.; Williams, S.; Walker, C.; Chapman, E. Pharmacogenomics and OUD: Clinical Decision Support in an African American Cohort. J. Natl. Med. Assoc. 2019, 11, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Narayan, S.W.; Pearson, S.A.; Litchfield, M.; Le Couteur, D.G.; Buckley, N.; McLachlan, A.J.; Zoega, H. Anticholinergic medicines use among older adults before and after initiating dementia medicines. Br. J. Clin. Pharmacol. 2019, 85, 1957–1963. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Gi, M.; Fujioka, M.; Teramoto, I.; Wanibuchi, H. Long-term administration of excess zinc impairs learning and memory in aged mice. J. Toxicol. Sci. 2019, 44, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Thomson, E.M. Air Pollution, Stress, and Allostatic Load: Linking Systemic and Central Nervous System Impacts. J. Alzheimers Dis. 2019, 69, 597–614. [Google Scholar] [CrossRef] [Green Version]
- Exley, C.; Mold, M.J. Aluminium in human brain tissue: How much is too much? J. Biol. Inorg. Chem. 2019, 54, 1279–1282. [Google Scholar] [CrossRef] [Green Version]
- Kalilani, L.; Sun, X.; Pelgrims, B.; Noack-Rink, M.; Villanueva, V. The epidemiology of drug-resistant epilepsy: A systematic review and meta-analysis. Epilepsia 2018, 59, 2179–2193. [Google Scholar] [CrossRef] [Green Version]
- Kong, S.T.; Hom, C.S.; Ho, P.C.; Lium, S.H. Prevalence of drug resistant epilepsy in adults with epilepsy attending a neurology clinic of a tertiary referral hospital in Singapore. Epilepsy Res. 2014, 108, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Kalozoumi, G.; Kel-Margoulis, O.; Vafiadaki, E.; Greenberg, D.; Bernard, H.; Soreq, H.; Depaulis, A.; Sanoudou, D. Glial responses during epileptogenesis in Mus musculus point to potential therapeutic targets. PLoS ONE 2018, 13, e0201742. [Google Scholar] [CrossRef] [Green Version]
- Orlandi, A.; Paolino, M.C.; Striano, P.; Parisi, P. Clinical reappraisal of the influence of drug-transporter polymorphisms in epilepsy. Expert Opin. Drug Metab. Toxicol. 2018, 14, 505–512. [Google Scholar] [CrossRef] [PubMed]







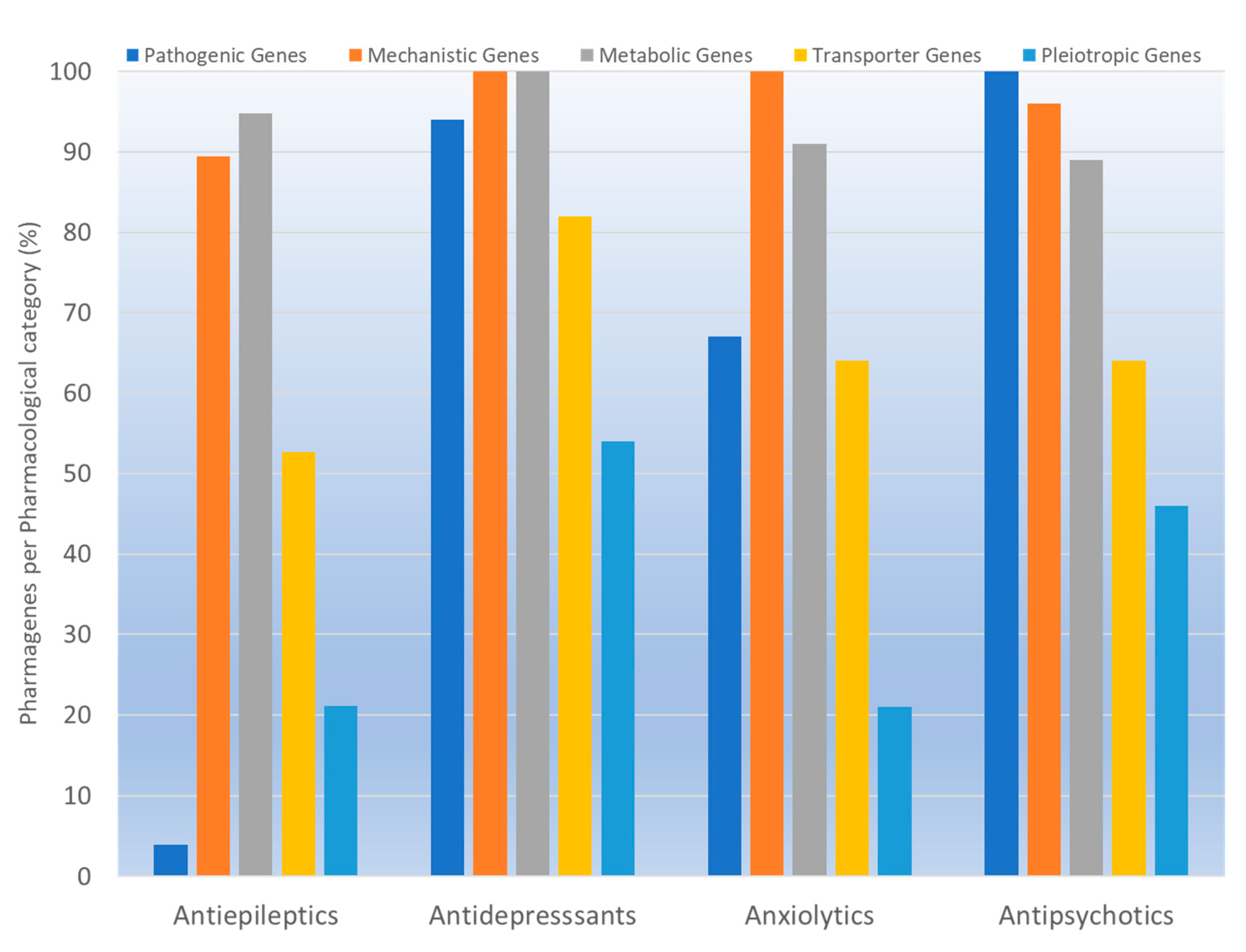{kind=link}
{kind=link}
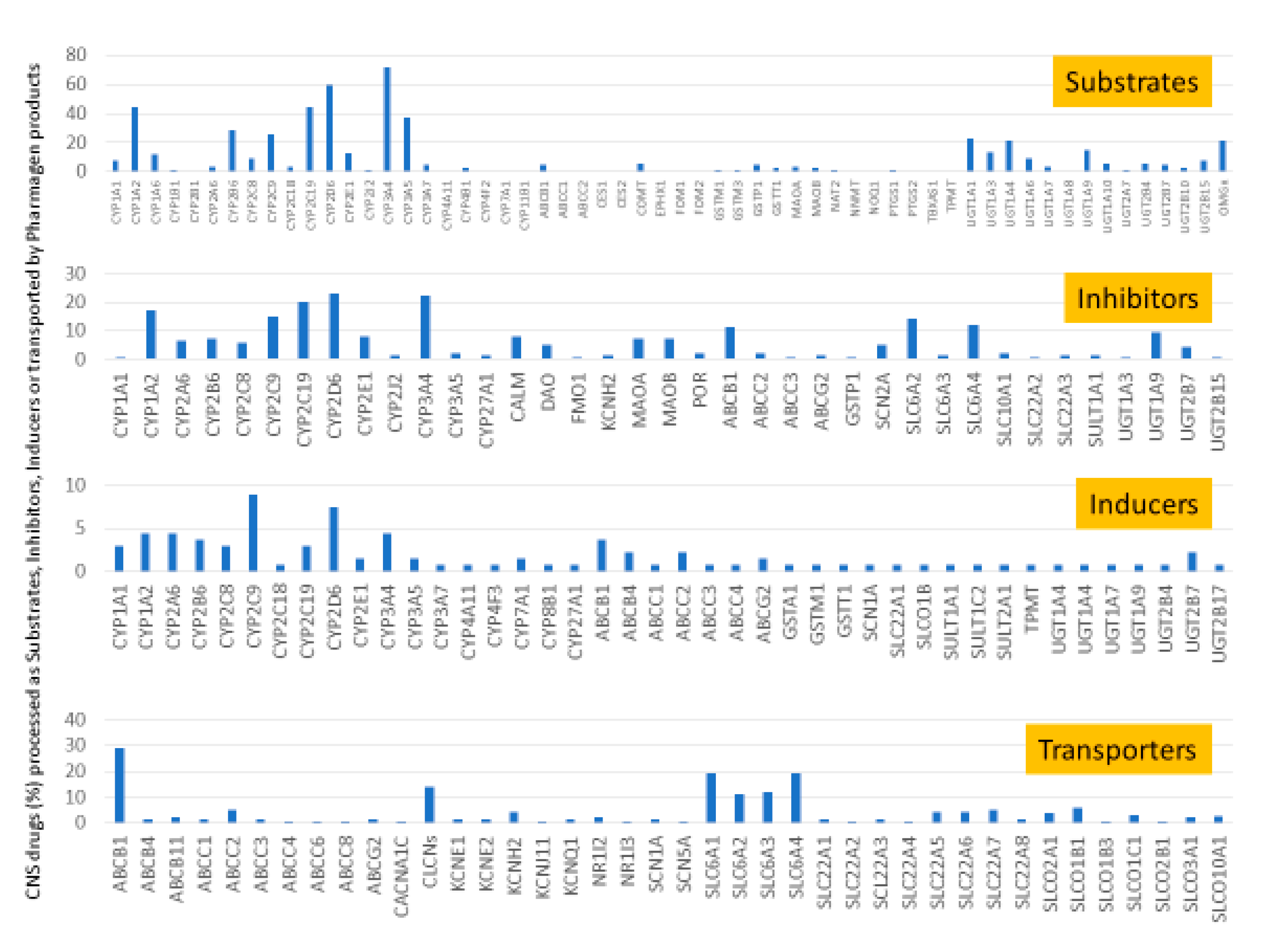{kind=link}
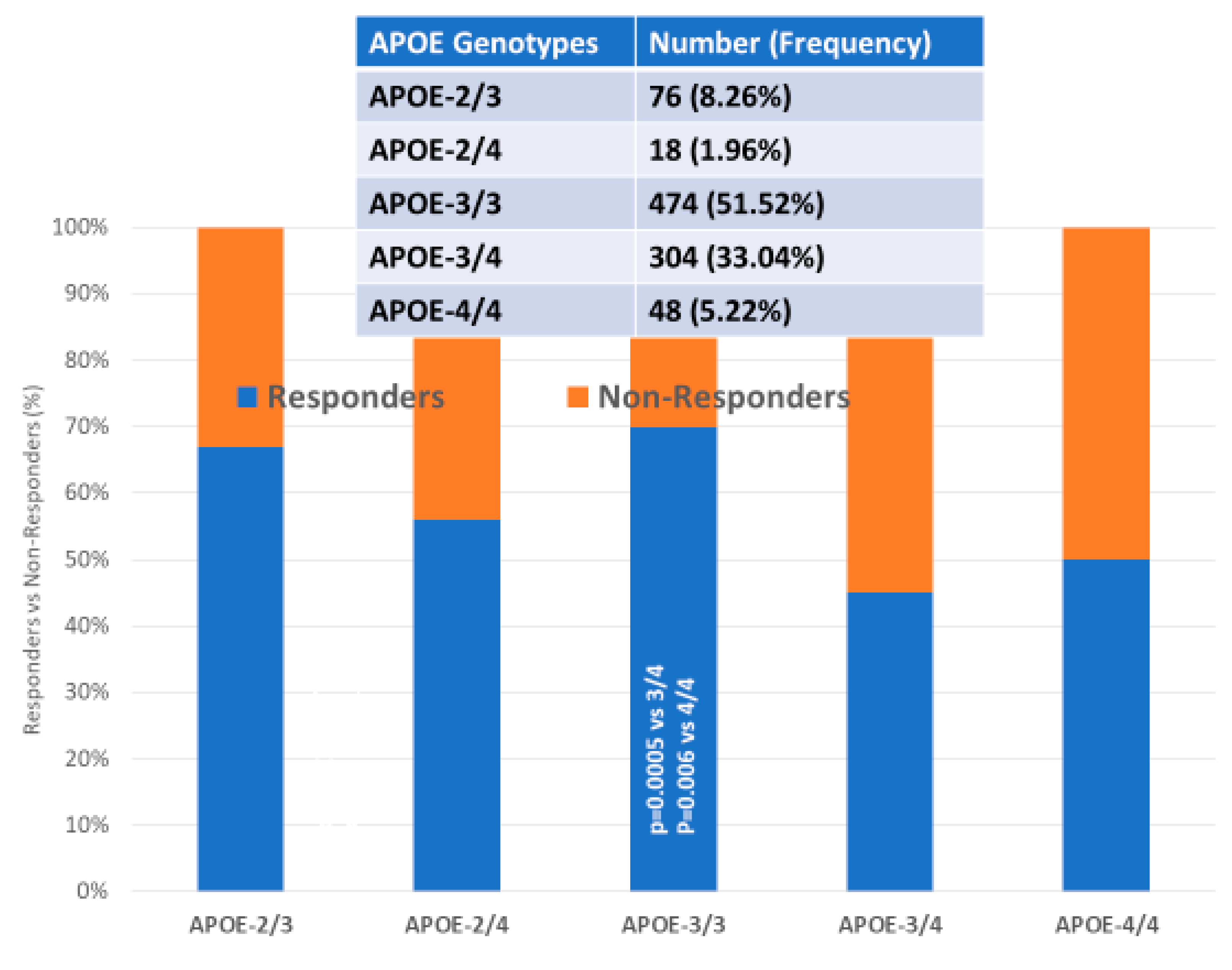{kind=link}
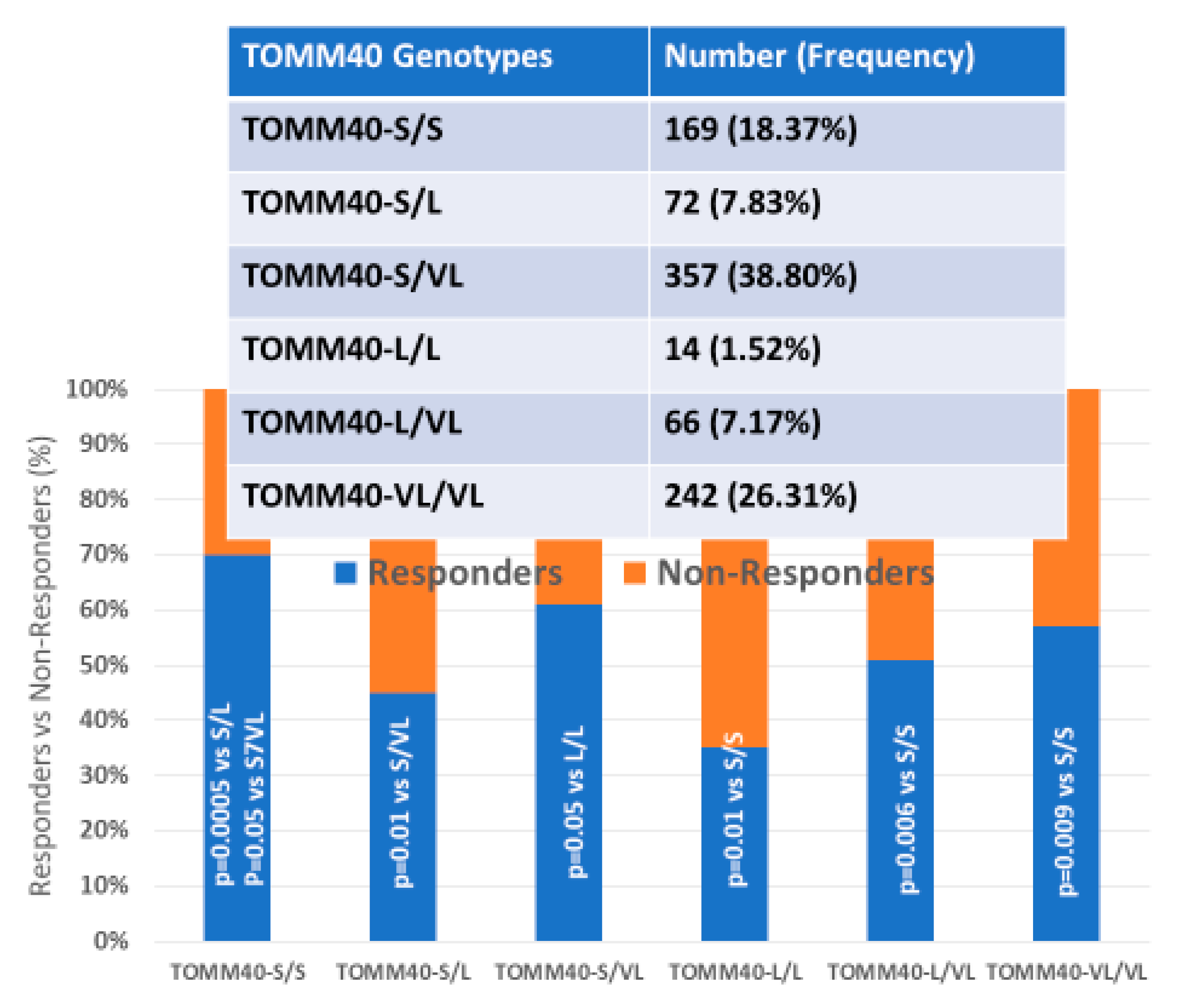{kind=link}
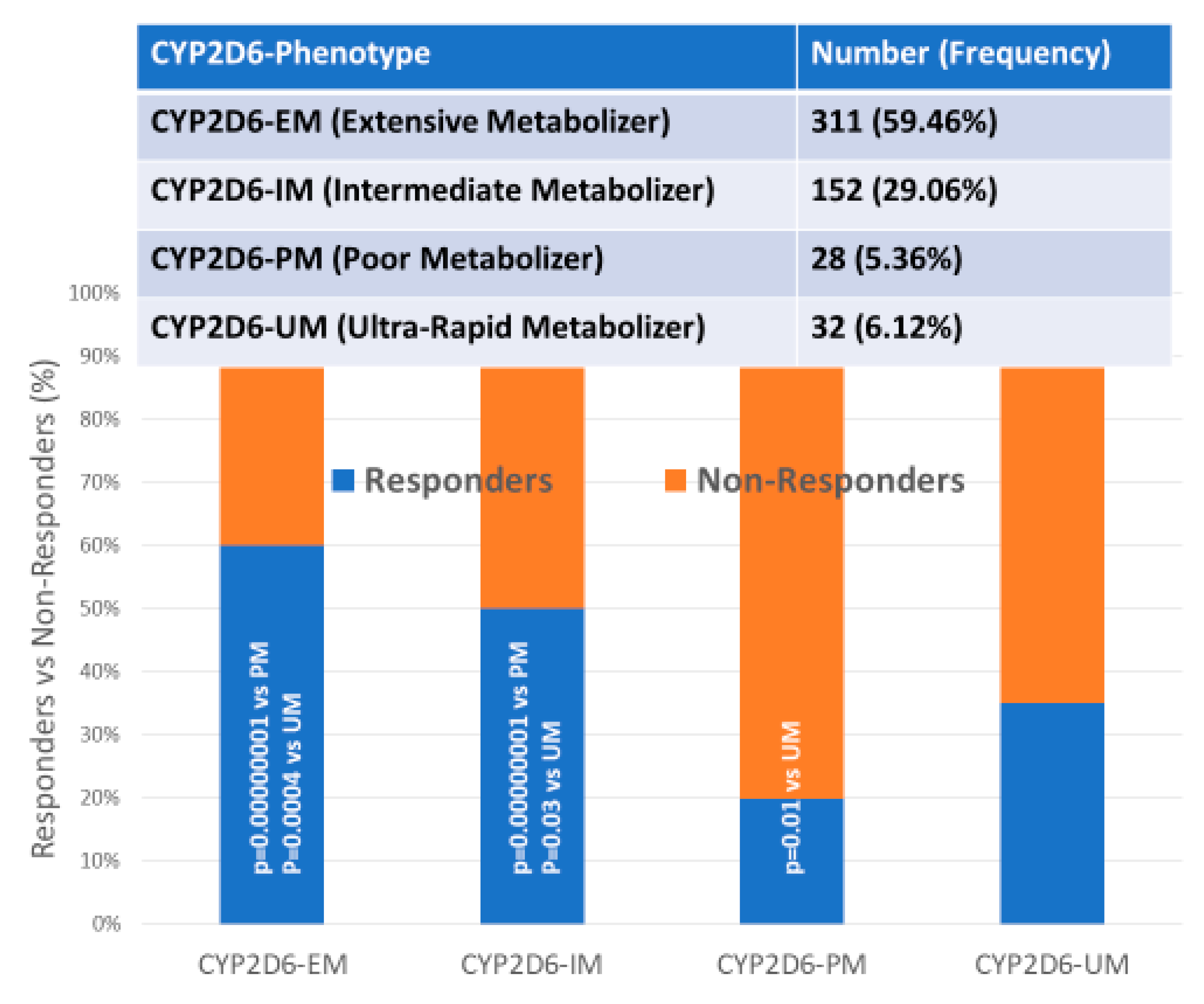{kind=link}
| Gene Symbol | Gene Name | Gene ID | OMIM # | Locus | dbSNP ID | Risk Allele | MAF |
|---|---|---|---|---|---|---|---|
| ABCA7 | ATP binding cassette subfamily A member | 10347 | 605414 | 19p13.3 | rs3764650 | G | 0.20 (G) |
| APOE | Apolipoprotein E | 348 | 107741 | 19q13.32 | rs429358; rs7412 | *4 | 0.15 (C); 0.08 (T) |
| APP | Amyloid beta precursor protein | 351 | 104760 | 21q21.3 | 52 SNPs | <0.01 | |
| BIN1 | Bridging integrator 1 | 274 | 601248 | 2q14.3 | rs744373 | C | 0.36 (C) |
| BUB3 | BUB3, mitotic checkpoint protein | 9184 | 603719 | 10q26.13 | rs4980270 | T | 0.10 (T) |
| C9ORF72 | Chromosome 9 open reading frame 72 | 203228 | 614260 | 9p21.2 | rs3849942 | T | 0.22 (T) |
| CD2AP | CD2 associated protein | 23607 | 604241 | 6p12.3 | rs9349407 | C | 0.25 (C) |
| CD33 | CD33 molecule | 945 | 159590 | 19q13.41 | rs3865444 | T | 0.01 (T) |
| CLU | Clusterin | 1191 | 185430 | 8p21.1 | rs11136000 | T | 0.38 (T) |
| CPZ | Carboxypeptidase Z | 8532 | 603105 | 4p16.1 | rs7436874 | C | 0.36 (C) |
| CR1 | Complement C3b/C4b receptor 1 | 185430 | 120620 | 1q32.2 | rs3818361 | T | 0.25 (T) |
| DISC1 | Disrupted in schizophrenia 1 | 27185 | 605210 | 1q42.2 | rs16856202 | G | 0.03 (G) |
| ENPP1 | Ectonucleotide pyrophosphatase/phosphodiesterase 1 | 5167 | 173335 | 6q23.2 | rs7767170 | T | 0.02 (T) |
| EXO1 | Exonuclease 1 | 9156 | 606063 | 1q43 | rs1776148 | A | 0.27 (A) |
| LAMA3 | Laminin subunit alpha 3 | 64231 | 606548 | 11q12.2 | rs11082762 | A | 0.47 (A) |
| LHFP | Lipoma HMGIC fusion partner | 10186 | 606710 | 13q13.3-q14.11 | rs7995844 | G | 0.35 (G) |
| MAPT | Microtubule associated protein tau | 4137 | 157140 | 17q21.31 | 15 SNPs | <0.01 | |
| MS4A4E | Membrane spanning 4-domains A4E | 643680 | 608401 | 8p21.1 | rs670139 | A | 0.38 (A) |
| MS4A6A | Membrane spanning 4-domains A6A | 64231 | 606548 | 11q12.2 | rs610932 | A | 0.45 (A) |
| NLRP4 | NLR family pyrin domain containing 4 | 147945 | 609645 | 19q13.43 | rs12462372 | A | 0.08 (A) |
| NTNG1 | Netrin G1 | 3909 | 600805 | 18q11.2 | rs11803905 | T | 0.32 (T) |
| PICALM | Phosphatidylinositol binding clathrin assembly protein | 8301 | 603025 | 11q14.2 | rs3851179 | A | 0.31 (A) |
| PIWIL2 | Piwi like RNA-mediated gene silencing 2 | 55124 | 610312 | 8p21.3 | rs4266653 | G | 0.47 (G) |
| PSEN1 | Presenilin 1 | 5663 | 104311 | 14q24.2 | 241 SNPs | < 0.01 | |
| PSEN2 | Presenilin 2 | 5664 | 600759 | 1q42.13 | 43 SNPs | < 0.01 | |
| STK36 | Serine/threonine kinase 36 | 27148 | 607652 | 2q35 | rs2303565 | C | 0.33 (C) |
| STX17 | Syntaxin 17 | 55014 | 604204 | 9q31.1 | rs1997368 | G | 0.32 (G) |
| SUN3 | Sad1 and UNC84 domain containing 3 | 256979 | 607723 | 7p12.3 | rs2708909 | G | 0.39 (G) |
| TBC1D5 | TBC1 domain family member 5 | 9779 | 615740 | 3p24.3 | rs10510480 | C | 0.11 (C) |
| USP6NL | USP6 N-terminal like | 9712 | 605405 | 10p14 | rs3847437 | T | 0.04 (T) |
| ZSWIM7 | Zinc finger SWIM-type containing 7 | 125150 | 614535 | 17p12 | rs10491104 | T | 0.41 (T) |
| Drug | Properties | Pharmacogenetics |
|---|---|---|
 | Name: Donepezil hydrochloride, Aricept, 120011-70-3, Donepezil HCl, BNAG, E-2020, E2020 | Pathogenic genes:APOE, CHAT Mechanistic genes:CHAT, ACHE, BCHE Metabolic genes: Substrate:CYP2D6 (major), CYP3A4 (major), UGTs, ACHE Inhibitor: ACHE, BCHE Transporter genes: ABCB1 |
| IUPAC Name: 2-[(1-benzylpiperidin-4-yl)methyl]-5,6-dimethoxy-2,3-dihydroinden-1-one;hydrochloride | ||
| Molecular Formula: C24H30ClNO3 | ||
| Molecular Weight: 415.9529 g/mol | ||
| Category: Cholinesterase inhibitor | ||
| Mechanism: Centrally active, reversible acetylcholinesterase inhibitor; increases the acetylcholine available for synaptic transmission in the CNS | ||
| Effect: Nootropic agent, cholinesterase inhibitor, parasympathomimetic effect | ||
 | Name: Galantamine hydrobromide | Pathogenic genes:APOE, APP Mechanistic genes:ACHE, BCHE, CHRNA4, CHRNA7, CHRNB2 Metabollic genes: Substrate:CYP2D6 (major), CYP3A4 (major), UGT1A1 Inhibitor: ACHE, BCHE |
| IUPAC Name: (1S,12S,14R)-9-methoxy-4-methyl-11-oxa-4-azatetracyclo[8.6.1.0^{1,12}.0^{6,17}]heptadeca-6,8,10(17),15-tetraen-14-ol | ||
| Molecular Formula: C17H22BrNO3 | ||
| Molecular Weight: 368.26548 g/mol | ||
| Category: Cholinesterase inhibitor | ||
| Mechanism: Reversible and competitive acetylcholinesterase inhibition leading to an increased concentration of acetylcholine at cholinergic synapses; modulates nicotinic acetylcholine receptor; may increase glutamate and serotonin levels | ||
| Effect: Nootropic agent, cholinesterase inhibitor, parasympathomimetic effect | ||
 | Name: Memantine Hydrochloride, 41100-52-1, Namenda, Memantine HCL, Axura, 3,5-Dimethyl-1-adamantanamine hydrochloride, 3,5-dimethyladamantan-1-amine hydrochloride | Pathogenic genes:APOE, MAPT, PSEN1 Mechanistic genes:CHRFAM7A, DLGAP1, FOS, GRIN2A, GRIN2B, GRIN3A, HOMER1, HTR3A Metabolic genes: Inhibitor:CYP1A2 (weak), CYP2A6 (weak), CYP2B6 (strong), CYP2C9 (weak), CYP2C19 (weak), CYP2D6 (strong), CYP2E1 (weak), CYP3A4 (weak), NR1I2 Transporter genes: NR1I2; Pleiotropic genes: APOE, MAPT, MT-TK, PSEN1 |
| IUPAC Name: 3,5-dimethyladamantan-1-amine;hydrochloride | ||
| Molecular Formula: C12H22ClN | ||
| Molecular Weight: 215.76278 g/mol | ||
| Category: N-Methyl-D-Aspartate receptor antagonist | ||
| Mechanism: Binds preferentially to NMDA receptor-operated cation channels; may act by blocking actions of glutamate, mediated in part by NMDA receptors | ||
| Effect: Dopamine agent, antiparkinson agent, excitatory amino acid antagonist, antidyskinetic | ||
 | Name: Rivastigmine tartrate, 129101-54-8, SDZ-ENA 713, Rivastigmine hydrogentartrate, Rivastigmine Hydrogen Tartrate, ENA 713, ENA-713 | Pathogenic genes:APOE, APP, CHAT Mechanistic genes:ACHE, BCHE, CHAT, CHRNA4, CHRNB2 Metabolic genes: Inhibitor:ACHE, BCHE Pleiotropic genes:APOE, MAPT |
| IUPAC Name: (2R,3R)-2,3-dihydroxybutanedioic acid;[3-[(1S)-1-(dimethylamino)ethyl]phenyl] N-ethyl-N-methylcarbamate | ||
| Molecular Formula: C18H28N2O8 | ||
| Molecular Weight: 400.42352 g/mol | ||
| Category: Cholinesterase inhibitor | ||
| Mechanism: Increases acetylcholine in CNS through reversible inhibition of its hydrolysis by cholinesterase | ||
| Effect: Neuroprotective agent, cholinesterase inhibitor, cholinergic agent | ||
 | Name: Tacrine Hydrochloride, Tacrine HCl, 1684-40-8, Hydroaminacrine, tacrine.HCl, 9-AMINO-1,2,3,4-TETRAHYDROACRIDINE HYDROCHLORIDE, Tenakrin | Pathogenic genes:APOE Mechanistic genes:ACHE, BCHE, CHRNA4, CHRNB2 Metabolic genes: Substrate:CYP1A2 (major), CYP2D6 (minor), CYP3A4 (major) Inhibitor:ACHE, BCHE, CYP1A2 (weak) Transporter genes:SCN1A Pleiotropic genes:APOE, CES1, GSTM1, GSTT1, LEPR, MTHFR |
| IUPAC Name: 1,2,3,4-tetrahydroacridin-9-amine;hydrochloride | ||
| Molecular Formula: C13H15ClN2 | ||
| Molecular Weight: 234.7246 g/mol | ||
| Category: Cholinesterase inhibitor | ||
| Mechanism: Elevates acetylcholine in cerebral cortex by slowing degradation of acetylcholine | ||
| Effect: Nootropic agent, cholinesterase inhibitor, Parasympathomimetic effect |
| Atypical Antipsychotics | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Aripiprazole; 129722-12-9; Abilify; Abilitat; Abilify Discmelt; OPC-1459 | Pathogenic genes:DRD2, DRD3, HTR1A, HTR2A, HTR2C Mechanistic genes:ADRA1A, DRD2, DRD3, DRD4, HRHs, HTR1A, HTR2A, HTR2B, HTR2C, HTR7 Metabolic genes: Substrate:CYP2D6 (major), CYP3A4 (major), CYP3A5 Transporter genes: ABCB1 |
| IUPAC Name: 7-{4-[4-(2,3-dichlorophenyl) piperazin-1-yl]butoxy}-1,2,3,4-tetrahydroquinolin-2-one | ||
| Molecular Formula: 448.38538 g/mol | ||
| Molecular Weight: C23H27Cl2N3O2 | ||
| Mechanism: Partial agonist at the D2 and 5-HT1A receptors, and as an antagonist at the 5-HT2A receptor | ||
| Effect: Antipsychotic agent; H1-receptor antagonist; Serotonergic agonist | ||
 | Name: Asenapine maleate; Saphris; Org5222 maleate; 85650-56-2; Org 5222 maleate; Org-5222 maleate | Pathogenic genes:ADRA2A, DRD1, DRD2, DRD3, DRD4, HTR1A, HTR2A, HTR2C, HTR7 Mechanistic genes:ADRA1A, ADRA2A, ADRA2B, ADRA2C, DRD1, DRD2, DRD3, DRD4, HRH1, HRH2, HTR1A, HTR1B, HTR2A, HTR2B, HTR2C, HTR5A, HTR6, HTR7 Metabolic genes: Substrate:CYP1A1, CYP1A2 (major), CYP2D6 (minor), CYP3A4 (minor), UGT1A4 Inhibitor: CYP2D6 (weak) |
| IUPAC Name: (2Z)-but-2-enedioic acid; 17-chloro-4-methyl-13-oxa-4-azatetracyclo[12.4.0.02,6.07,12]octadeca-1(14),7,9,11,15,17-hexaene | ||
| Molecular Formula: C21H20ClNO5 | ||
| Molecular Weight: 401.8402 g/mol | ||
| Mechanism: Its main activity is associated to combination of antagonistic actions at D2 and 5-HT2A receptors | ||
| Effect: Antipsychotic agent; Dopaminergic antagonist; Serotonergic antagonist; Alpha-adrenergic antagonist; Beta-adrenergic antagonist | ||
 | Name: Clozapine; Leponex; Fazaclo; Iprox; CLOZARIL; Clozapin | Pathogenic genes:ADRA2A, DRD1, DRD2, DRD3, DRD4, DTNBP1, HTR2A, LPL, NRXN1, TNF Mechanistic genes:ADRAs, CHRMs, DRD1, DRD2, DRD3, DRD4, HRH1, HTR1F, HTR2A, HTR2C, HTR3A, HTR6, NRXN1 Metabolic genes: Substrate:CYP1A2 (major), CYP2A6 (minor), CYP2C8 (minor), CYP2C9 (minor), CYP2C19 (minor), CYP2D6 (minor), CYP3A4/5 (major), FMO3, UGT1A1, UGT1A3, UGT1A4 Inhibitor: CYP1A2 (weak), CYP2C9 (moderate), CYP2C19 (moderate), CYP2D6 (moderate), CYP2E1 (weak), CYP3A4 (weak) Transporter genes: ABCB1 Pleiotropic genes: APOA5, APOC3, APOD, CNR1, FABP1, GNB3, GSK3B, LPL, RGS2, TNF |
| IUPAC Name: 6-chloro-10-(4-methylpiperazin-1-yl)-2,9-diazatricyclo[9.4.0.03,8]pentadeca-1(15),3,5,7,9,11,13-heptaene | ||
| Molecular Formula: C18H19ClN4 | ||
| Molecular Weight: 326.82326 g/mol | ||
| Mechanism: It shows serotonergic, adrenergic, and cholinergic neurotransmitter systems in addition to more selective, regionally specific effects on the mesolimbic dopaminergic system. It also displays antagonistic activity at H1-receptors | ||
| Effect: Dopaminergic antagonist; Serotonergic antagonist; Histamine antagonist; Muscarinic antagonist; GABA antagonist; GABA modulator; Antipsychotic agent | ||
 | Name: Iloperidone; Zomaril; 133454-47-4; Fanapt; Fanapta; HP 873 | Pathogenic genes:ADRA2A, CNTF, DRD1, DRD2, DRD3, DRD4, HTR2A, HTR7, NRG3 Mechanistic genes:ADRA1A, ADRA2A, ADRA2B, ADRA2C, ADRB1, ADRB2, DRD1, DRD2, DRD3, DRD4, DRD5, GFRA2, GRIA4, HRH1, HTR1A, HTR2A, HTR2C, HTR6, HTR7, NPAS3, NUDT9P1, TNR, XKR4 Metabolic genes: Substrate:CYP1A2, CYP2E1, CYP2D6 (major), CYP3A4 (major) Transporter genes: SLC6A2, SLCO3A1 Pleiotropic genes: ADRB2, CELF4, CERKL, DRD5, HTR1F, NPAS3, NRG3, NUBPL, PALLD |
| IUPAC Name: 1-(4-{3-[4-(6-fluoro-1,2-benzoxazol-3-yl)piperidin-1-yl]propoxy}-3-methoxyphenyl)ethan-1-one | ||
| Molecular Formula: C24H27FN2O4 | ||
| Molecular Weight: 426.480583 g/mol | ||
| Mechanism: It has mixed D2/5-HT2 antagonist activity. It exhibits high affinity for 5-HT2A, D2, and D3 receptors, low to moderate affinity for D1, D4, H1, 5-HT1A, 5-HT6, 5HT7, and ADRα1/α2C receptors, and no affinity for muscarinic receptors. It has low affinity for histamine H1 receptors | ||
| Effect: Antipsychotic agent; Dopaminergic antagonist; Serotonergic antagonist; Antidepressant effects; Anxiolytic activity; Reduction of risk for weight gain; Cognitive Function Improved | ||
 | Name: Olanzapine; Zyprexa; 132539-06-1; Zyprexa Zydis; Olansek; Symbyax | Pathogenic genes:COMT, DRD1, DRD2, DRD3, DRD4, GRM3, HTR2A, HTR2C, LPL Mechanistic genes:ABCB1, ADRA1A, ADRB3, AHR, BDNF, CHRM1, CHRM2, CHRM3, CHRM4, CHRM5, COMT, DRD1, DRD2, DRD3, DRD4, GABRs, GRIN2B, HRH1, HTR2A, HTR2C, HTR3A, HTR6, LEP, RGS2, RGS7, SLC6A4, STAT3, TMEM163 Metabolic genes: Substrate:COMT, CYP1A2 (major), CYP2C9, CYP2D6 (major), CYP3A43, CYP3A5, FMO1, FMO3, GSTM3, TPMT, UGT1A1, UGT1A4, UGT2B10 Inhibitor: ABCB1, CYP1A2 (weak), CYP2C9 (weak), CYP2C19 (weak), CYP2D6 (weak), CYP3A4 (weak) Inducer: GSTM1, MAOB, SLCO3A1 Transporter genes: KCNH2, SLC6A2, SLC6A4, SLCO3A1 Pleiotropic genes: APOA5, APOC3, GNB3, LEP, LEPR, LPL |
| IUPAC Name: 5-methyl-8-(4-methylpiperazin-1-yl)-4-thia-2,9-diazatricyclo[8.4.0.0³,⁷]tetradeca-1(14),3(7),5,8,10,12-hexaene | ||
| Molecular Formula: C17H20N4S | ||
| Molecular Weight: 312.4325 g/mol | ||
| Mechanism: It displays potent antagonism of serotonin 5-HT2A and 5-HT2C, dopamine D1-4, histamine H1 and α1-adrenergic receptors. It shows moderate antagonism of 5-HT3 and muscarinic M1-5 receptors, and weak binding to GABA-A, BZD, and β-adrenergic receptors. | ||
| Effect: Antipsychotic agent; GABA modulator; Muscarinic antagonist; Serotonin uptake inhibitor; Dopaminergic antagonist; Serotonergic antagonist; Histamine antagonist; Antiemetic activity | ||
 | Name: Paliperidone; Paliperidone; 9-Hydroxyrisperidone; Invega; 144598-75-4; 9-OH-risperidone; Invega Sustenna | Pathogenic genes:ADRA2A, DRD2, HTR2A Mechanistic genes:ADRA1A, ADRA1B, ADRA1D, ADRA2s, BDNF, DRD2, HRH1, HTR1A, HTR2A, HTR2C Metabolic genes: Substrate:ADH, CYP2D6(minor), CYP3A4/5 (major), UGTs Inhibitor: ABCB1, CYP2D6 (moderate), CYP3A4/5 (moderate) Transporter genes: ABCB1 |
| IUPAC Name: 3-{2-[4-(6-fluoro-1,2-benzoxazol-3-yl)piperidin-1-yl]ethyl}-9-hydroxy-2-methyl-4H,6H,7H,8H,9H-pyrido[1,2-a]pyrimidin-4-one | ||
| Molecular Formula: C23H27FN4O3 | ||
| Molecular Weight: 426.483883 g/mol | ||
| Mechanism: Mixed central serotonergic and dopaminergic antagonism. Demonstrates high affinity to α1, D2, H1, and 5-HT2C receptors, and low affinity for muscarinic and 5-HT1A receptors | ||
| Effect: Antipsychotic agent; Neuroprotective agent; H1-receptor antagonist; Alpha-adrenergic antagonist; Serotonergic antagonist; Dopaminergic antagonist | ||
 | Name: Quetiapine Fumarate; Seroquel; Quetiapine hemifumarate; 111974-72-2; Seroquel XR; UNII-2S3PL1B6UJ | Pathogenic genes:ADRA2A, DRD1, DRD2, DRD4, HTR1A, HTR2A, RGS4 Mechanistic genes:ADRA1s, ADRA2s, BDNF, CHRM1, CHRM3, CHRM5, DRD1, DRD2, DRD4, HRH1, HTR1A, HTR1E, HTR2A, HTR2B, HTR7 Metabolic genes: Substrate:CYP2D6 (minor), CYP3A4/5 (major), CYP3A7, CYP2C19 Inhibitor: ABCB1, SLC6A2 Transporter genes: ABCB1, KCNE1, KCNE2, KCNH2, KCNQ1, SCN5A, SLC6A2 |
| IUPAC Name: 2-[2-(4-{2-thia-9-azatricyclo[9.4.0.0³,⁸]pentadeca-1(15),3,5,7,9,11,13-heptaen-10-yl}piperazin-1-yl)ethoxy]ethan-1-ol | ||
| Molecular Formula: C46H54N6O8S2 | ||
| Molecular Weight: 883.08636 g/mol | ||
| Mechanism: Antagonist at multiple neurotransmitter receptors: serotonin 5-HT1A and 5-HT2, dopamine D1 and D2, histamine H1, and adrenergic α1- and α2-receptors | ||
| Effect: Antipsychotic agent; Adrenergic antagonist; Histamine antagonist; Serotonergic antagonist; Dopaminergic antagonist; Sedative activity; Orthostatic hypotension | ||
 | Name: Risperidone; Risperdal; Risperidal; 106266-06-2; Risperdal Consta; Rispolept | Pathogenic genes:ADRA2A, BDNF, COMT, DRD1, DRD2, DRD3, DRD4, GRM3, HTR2A, HTR2C, HTR7, PON1, RGS4 Mechanistic genes:ADRA1A, ADRA1B, ADRA2s, DRD1, DRD2, DRD3, DRD4, FOS, HTR2A, HTR2C, HTR3A, HTR3C, HTR6, HTR7, NR1I2, STAT3 Metabolic genes: Substrate:COMT, CYP2D6 (major), CYP3A4/5 (minor) Inhibitor: ABCB1, CYP2D6 (weak), CYP3A4 (weak) Inducer: MAOB Transporter genes: ABCB1, KCNH2, SLC6A4 Pleiotropic genes: APOA5, BDNF, RGS2 |
| IUPAC Name: 3-{2-[4-(6-fluoro-1,2-benzoxazol-3-yl)piperidin-1-yl]ethyl}-2-methyl-4H,6H,7H,8H,9H-pyrido[1,2-a]pyrimidin-4-one | ||
| Molecular Formula: C23H27FN4O2 | ||
| Molecular Weight: 410.484483 g/mol | ||
| Mechanism: Antagonist at multiple neurotransmitter receptors: serotonin 5-HT1A and 5-HT2, dopamine D1 and D2, histamine H1, and adrenergic α1- and α2-receptors | ||
| Effect: Antipsychotic agent; H1-receptor antagonist; Dopaminergic antagonist; Alpha-adrenergic antagonist; Serotonergic antagonist; Somnolence; Orthostatic hypotension | ||
 | Name: Ziprasidone; Geodon; 146939-27-7; Zeldox; Ziprazidone; Ziprasidone hydrochloride | Pathogenic genes:DRD2, DRD3, DRD4, HTR1A, HTR2A, HTR2C, RGS4 Mechanistic genes:ADRA1A, DRD2, DRD3, HRH1, HTR1A, HTR1B, HTR1D, HTR2A, HTR2C Metabolic genes: Substrate:AOX1 (major), CYP1A2 (minor), CYP3A4 (major) Inhibitor: CYP2D6 (moderate), CYP3A4 (moderate), SLC6A2, SLC6A4 Transporter genes: KCNH2, SLC6A2, SLC6A4 Pleiotropic genes: CHRM1, RRAS2 |
| IUPAC Name: 5-{2-[4-(1,2-benzothiazol-3-yl)piperazin-1-yl]ethyl}-6-chloro-2,3-dihydro-1H-indol-2-one | ||
| Molecular Formula: C21H21ClN4OS | ||
| Molecular Weight: 412.93564 g/mol | ||
| Mechanism: It has high affinity for D2, D3, 5-HT2A, 5-HT1A, 5-HT2C, 5-HT1D, and α1-adrenergic, and moderate affinity for histamine H1 receptors. It functions as antagonist at D2, 5-HT2A, and 5-HT1D receptors and as agonist at 5-HT1A receptor. It moderately inhibits reuptake of serotonin and norepinephrine | ||
| Effect: Antipsychotic agent; Histamine antagonist; Dopaminergic antagonist; Serotonergic antagonist; Muscarinic antagonist; Serotonin–norepinephrine reuptake inhibitor | ||
| Typical Antipsychotics | ||
| Butyrophenones | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Bromperidol; Impromen; Bromoperidol; Tesoprel; 10457-90-6; Azurene | Pathogenic genes:DRD2, HTR2A Mechanistic genes:DRD2, HTR2A Metabolic genes: Substrate:CYP2D6 (minor), CYP3A4 (major), UGTs Inhibitor: CYP2D6 (moderate) Transporter genes: ABCB1 |
| IUPAC Name: 4-[4-(4-bromophenyl)-4-hydroxypiperidin-1-yl]-1-(4-fluorophenyl)butan-1-one | ||
| Molecular Formula: C21H23BrFNO2 | ||
| Molecular Weight: 420.315223 g/mol | ||
| Mechanism: Potent dopaminergic D2 antagonist. Has weak α1-adrenolitic activity. It is a moderate serotonin 5-HT2 antagonist. Has no antihistaminic or anticholinergic effects. It acts on the mesocortex, limbic system, and basal ganglia (nigrostriate pathway) | ||
| Effect: Antipsychotic agent; Dopamine antagonist; α1-adrenolitic activity | ||
 | Name: Haloperidol; Haldol; Eukystol; Serenace; Aloperidin; Aloperidol | Pathogenic genes:ADRA2A, BDNF, DRD1, DRD2, DRD4, DTNBP1, GRIN2B, HTR2A Mechanistic genes:ANKK1, BDNF, COMT, DRD1, DRD2, DTNBP1, GRIN2A, GRIN3B, GRIN2C, GRIN2B, SLC6A3 Metabolic genes: Substrate:CBR1, CYP1A1 (minor), CYP1A2 (minor), CYP2A6, CYP2C8 (minor), CYP2C9 (minor), CYP2C19 (minor), CYP2D6 (major), CYP3A4/5 (major), GSTP1, UGTs Inhibitor: ABCB1, CYP2D6 (moderate), CYP3A4 (moderate) Transporter genes: ABCB1, ABCC1, KCNE1, KCNE2, KCNH2, KCNJ11, KCNQ1, SLC6A3 Pleiotropic genes: CHRM2, FOS, GSK3B, HRH1, HTR2A, HTT, IL1RN |
| IUPAC Name: 4-[4-(4-chlorophenyl)-4-hydroxypiperidin-1-yl]-1-(4-fluorophenyl)butan-1-one | ||
| Molecular Formula: C21H23ClFNO2 | ||
| Molecular Weight: 375.864223 g/mol | ||
| Mechanism: Haloperidol is a butyrophenone antipsychotic which blocks postsynaptic mesolimbic dopaminergic D1 and D2 receptors in brain. Depresses release of hypothalamic and hypophyseal hormones. Believed to depress reticular activating system | ||
| Effect: Antipsychotic agent; Serotonergic antagonist; Dopaminergic antagonist; Antiemetic; Antidyskinesia agent; Sedative effects; Hypotension | ||
| Phenothiazines | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Chlorpromazine; Largactil; Thorazine; Contomin; Chloropromazine; Aminazine | Pathogenic genes:BDNF, DRD1, DRD2, DRD3, DRD4, HTR2A Mechanistic genes:ADRA1A, ADRA1B, CHRM1, CHRM2, DRD1, DRD2, DRD3, DRD4, HRH1, HTR1A, HTR2A, HTR2C Metabolic genes: Substrate:CYP1A2 (minor), CYP2A6, CYP2C9, CYP2C19, CYP2D6 (major), CYP3A4 (minor), FMO1, UGT1A3, UGT1A4 Inhibitor: CYP1A2, CYP2D6 (strong), CYP2C19, CYP2E1 (weak), CYP3A4, DAO Transporter genes: ABCB1, CFTR Pleiotropic genes: ACACA, BDNF, FABP1, LEP, NPY |
| IUPAC Name: [3-(2-chloro-10H-phenothiazin-10-yl)propyl]dimethylamine | ||
| Molecular Formula: C17H19ClN2S | ||
| Molecular Weight: 318.86416 g/mol | ||
| Mechanism: Blocks postsynaptic mesolimbic dopaminergic receptors in the brain. Has actions at all levels of CNS, particularly at subcortical levels; also acts on multiple organ systems. Also exhibits weak ganglionic blocking, has a strong α-adrenergic blocking effect and depresses the release of hypothalamic and hypophyseal hormones. Depresses the reticular activating system | ||
| Effect: Antipsychotic agent; Dopaminergic antagonist; Antiemetic; Anticholinergic effects; Sedative effects; Antihistaminic effects; Anti-serotonergic activity; Hypotension | ||
 | Name: Fluphenazine; Triflumethazine; Fluorophenazine; Fluorfenazine; Fluorphenazine; Siqualine | Pathogenic genes:DRD1, DRD2 Mechanistic genes:CALM1, DRD1, DRD2 Metabolic genes: Substrate:CYP2B6, CYP2D6 (major) Inhibitor: ABCB1, CYP1A2 (weak), CYP2A6, CYP2C9 (weak), CYP2C19, CYP2D6 (strong), CYP2E1 (weak), CYP3A4 Transporter genes: ABCB1 |
| IUPAC Name: 2-(4-{3-[2-(trifluoromethyl)-10H-phenothiazin-10-yl]propyl}piperazin-1-yl)ethan-1-ol | ||
| Molecular Formula: C22H26F3N3OS | ||
| Molecular Weight: 437.52155 g/mol | ||
| Mechanism: Blocks postsynaptic mesolimbic dopaminergic D1 and D2 receptors in the brain. Depresses release of hypothalamic and hypophyseal hormones. Believed to depress reticular activating system, thus affecting basal metabolism, body temperature, wakefulness, vasomotor tone, and emesis | ||
| Effect: Antipsychotic agent; Dopaminergic antagonist; Antiemesis; Anticholinergic effects; Sedative effects | ||
 | Name: Perphenazine; Trilafon; Perphenazin; Etaperazine; Perfenazine; Fentazin | Pathogenic genes:ADRA2A, DRD1, DRD2, HTR2A, HTR2C, RGS4 Mechanistic genes:ADRA1A, ADRA2A, DRD1, DRD2, HTR2A, HTR2C, RGS4 Metabolic genes: Substrate:CYP1A2 (major), CYP2C8 (major), CYP2C9 (major), CYP2C18 (major), CYP2C19 (major), CYP2D6 (minor), CYP3A4/5 (major) Inhibitor: CYP1A2 (weak), CYP2D6 (strong) Transporter genes: ABCB1 |
| IUPAC Name: 2-[4-[3-(2-chlorophenothiazin-10-yl)propyl]piperazin-1-yl]ethanol | ||
| Molecular Formula: C21H26ClN3OS | ||
| Molecular Weight: 403.96864 g/mol | ||
| Mechanism: Blocks postsynaptic mesolimbic dopaminergic receptors in brain. Exhibits α-adrenergic-blocking effect and depresses release of hypothalamic and hypophyseal hormones. Binds to the dopamine D1 and D2 receptors and inhibits their activity | ||
| Effect: Antipsychotic agent; Antiemetic; Dopaminergic antagonist; Antiemesis | ||
 | Name: Thioridazine; Mellaril; Melleril; Thioridazin; Meleril; Sonapax | Pathogenic genes:ADRA2A, DRD1, DRD2 Mechanistic genes:ADRA1s, ADRA2s, DRD1, DRD2 Metabolic genes: Substrate:CYP1A2 (major), CYP2C19 (minor), CYP2A6, CYP2D6 (major), CYP2J2 (major), CYP3A4 (major) Inhibitor: ABCB1, CYP1A2 (weak), CYP2A6, CYP2C9 (weak), CYP2C19 (weak), CYP2D6 (moderate), CYP2E1 (weak), CYP3A4 (weak), KCNH Transporter genes: ABCB1, KCNE1, KCNE2, KCNH2, KCNJ11, KCNQ1 Pleiotropic genes: ADRBs, CHRM2, FABP1, HRH1 |
| IUPAC Name: 10-[2-(1-methylpiperidin-2-yl)ethyl]-2-methylsulfanylphenothiazine | ||
| Molecular Formula: C21H26N2S2 | ||
| Molecular Weight: 370.57454 g/mol | ||
| Mechanism: Blocks postsynaptic mesolimbic dopaminergic receptors in brain. Exhibits strong α-adrenergic-blocking effect and depresses release of hypothalamic and hypophyseal hormones | ||
| Effect: Antipsychotic agent; Dopaminergic antagonist; Alpha-adrenergic antagonist; H1-receptor antagonist; Serotonergic antagonist | ||
 | Name: Trifluoperazine; Trifluperazine; Trifluoroperazine; Trifluoperazina; Triflurin; Triperazine | Pathogenic genes:DRD2, IL12B Mechanistic genes:ABCB1, ADRA1A, ADRA1B, CALMs, DRD2, HRH1 Metabolic genes: Substrate:CYP1A2 (major), UGT1A4 Inhibitor: CALMs, POR Transporter genes: ABCB1 Pleiotropic genes: IL12B |
| IUPAC Name: 10-[3-(4-methylpiperazin-1-yl)propyl]-2-(trifluoromethyl)-10H-phenothiazine | ||
| Molecular Formula: C21H24F3N3S | ||
| Molecular Weight: 407.49557 g/mol | ||
| Mechanism: Blocks postsynaptic mesolimbic dopaminergic receptors in brain. Exhibits α-adrenergic-blocking effect and depresses release of hypothalamic and hypophyseal hormones. This agent also functions as a calmodulin inhibitor | ||
| Effect: Antipsychotic agent; Dopaminergic antagonist; Antiemesis; Cytosolic calcium elevation | ||
| Thioxanthenes | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Thiothixene, Tiotixene; Cis-Thiothixene; Navane; Thiothixine; Navan | Pathogenic genes:ADRA2A, DRD1, DRD2, DRD3, DRD4, HTR2A Mechanistic genes:ADRA1s, ADRA2s, CHRM1, CHRM2, DRD1, DRD2, DRD3, DRD4, HRH1, HRH2, HTR1s, HTR2s Metabolic genes: Substrate:CYP1A2 (major) Inhibitor: CYP2D6 (moderate) Transporter genes: KCNE1, KCNE2, KCNH6, KCNQ1, SCN5A |
| IUPAC Name: (9Z)-N,N-dimethyl-9-[3-(4-methylpiperazin-1-yl)propylidene]thioxanthene-2-sulfonamide | ||
| Molecular Formula: C23H29N3O2S2 | ||
| Molecular Weight: 443.62526 g/mol | ||
| Mechanism: Elicits antipsychotic activity by postsynaptic blockade of CNS dopamine receptors resulting in inhibition of dopamine-mediated effects. Also has α-adrenergic blocking activity. Antagonistic effect on dopaminergic (D1, D2, D3, D4), histaminergic (H1), sertoninergic (5-HT1, 5-HT2), adrenergic (α1- and α2) and muscarinic (M1 and M2) receptors | ||
| Effect: Antipsychotic agent; Dopamine antagonist; Antisympathomimetic properties; Anticholinergic effects; Antidepressant effects, Antiaggressive properties; H1-receptor antagonist; Serotonergic agonist | ||
 | Name: Zuclopenthixol; Zuclopentixol; Clopixol; Zuclopenthixolum; Acuphase; Cisordinol | Pathogenic genes:ADRA2A, DRD1, DRD2 Mechanistic genes:ADRA1s, ADRA2s, CHRMs, DRD1, DRD2, HRH1, HTR2s Metabolic genes: Substrate:CYP2D6 (major), CYP3A4 (major) |
| IUPAC Name: 2-[4-[(3Z)-3-(2-chlorothioxanthen-9-ylidene)propyl]piperazin-1-yl]ethanol | ||
| Molecular Formula: C22H25ClN2OS | ||
| Molecular Weight: 400.9647 g/mol | ||
| Mechanism: It mainly acts by antagonism of D1 and D2 dopamine receptors. It also has high affinity for alpha1-adrenergic and 5-HT2 receptors. It has weaker histamine H1 receptor blocking activity, and even lower affinity for muscarinic cholinergic and alpha2-adrenergic receptors | ||
| Effect: Antipsychotic agent; Dopaminergic antagonist; H1-receptor antagonist; Serotonergic antagonist; Alpha-adrenergic antagonist. | ||
| Typical Antipsychotics, Miscellaneous | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Loxapine Succinate; 27833-64-3; Loxapac; Loxapine succinate salt; Cloxazepin; Daxolin | Pathogenic genes:DRD1, DRD2, HTR2A Mechanistic genes:DRD1, DRD2, HTR2A Metabolic genes: Substrate:CYP1A2 (major), CYP2D6 (major), CYP3A4 (major), FMOs, UGT1A4 Pleiotropic genes: HTR2A |
| IUPAC Name: butanedioic acid;8-chloro-6-(4-methylpiperazin-1-yl)benzo[b][1,4]benzoxazepine | ||
| Molecular Formula: C22H24ClN3O5 | ||
| Molecular Weight: 445.89606 g/mol | ||
| Mechanism: Blocks postsynaptic mesolimbic D1 and D2 receptors in brain; also possesses serotonin 5-HT2-blocking activity | ||
| Effect: Antipsychotic agent; Dopamine antagonist; Serotonergic antagonist | ||
 | Name: Pimozide; Orap; Opiran; Neoperidole; Pimozidum; 2062-78-4 | Mechanistic genes:ADRA1A, CACNs, DRD1, DRD2, KCNH2 Metabolic genes: Substrate:CYP1A2 (minor), CYP2D6 (minor), CYP3A4 (major) Inhibitor: ABCB1, CYP2C19 (weak), CYP2D6 (strong), CYP2E1 (weak), CYP3A4 (moderate), KCNH2 Transporter genes: KCNE1, KCNE2, KCNH2, KCNJ11, KCNKs, KCNQ1, SCN5A Pleiotropic genes: CHRM2 |
| IUPAC Name: 3-[1-[4,4-bis(4-fluorophenyl)butyl]piperidin-4-yl]-1H-benzimidazol-2-one | ||
| Molecular Formula: C28H29F2N3O | ||
| Molecular Weight: 461.546166 g/mol | ||
| Mechanism: It is a potent centrally-acting dopamine-receptor antagonist resulting in its characteristic neuroleptic effects. Binds and inhibits the dopamine D2 receptor in the CNS. It is antagonist of ADRA1A | ||
| Effect: Antipsychotic agent; H1-receptor antagonist; Dopaminergic antagonist; Antidyskinesia agent; Serotonergic antagonist | ||
 | Name: Sulpiride; Sulpyrid; Aiglonyl; Dogmatil; Dolmatil; Sulpirid | Pathogenic genes:DRD2, DRD Mechanistic genes:DRD2, DRD3, PRLH Metabolic genes: Substrate:CYP1A2, CYP2B1, CYP3As Inhibitor:CYP1A2, CYP2B1, CYP3As |
| IUPAC Name: N-[(1-ethylpyrrolidin-2-yl)methyl]-2-methoxy-5-sulfamoylbenzamide | ||
| Molecular Formula: C15H23N3O4S | ||
| Molecular Weight: 341.42582 g/mol | ||
| Mechanism: It is a selective antagonist at postsynaptic D2 and D3-receptors. It appears to lack effects on norepinephrine, acetylcholine, serotonin, histamine, or GABA receptors. It also stimulates secretion of prolactin | ||
| Effect: Antipsychotic agent; Dopaminergic antagonist; Antidepressant effect; Antiemesis. Sedation (>600 mg/day); Dopamine reuptake inhibition (<200 mg/day); Antiemesis, Antimigraine effects; Antivertiginous activity; Prolactin-releasing stimulation | ||
| Monoamine Oxidase Inhibitors (MAOIs) | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Moclobemide; Aurorix; Moclamine; Manerix; Moclobemidum; Moclobemid | Pathogenic genes:MAOA Mechanistic genes:MAOA Metabolic genes: Substrate:CYP2C19 (major), CYP2D6 (major), CYP2E1 Inhibitor: CYP1A2 (weak), CYP2C19 (weak), CYP2D6 (weak), MAOA (strong), MAOB (moderate) |
| IUPAC Name: 4-chloro-N-[2-(morpholin-4-yl)ethyl]benzamide | ||
| Molecular Formula: C13H17ClN2O2 | ||
| Molecular Weight: 268.73928 g/mol | ||
| Category: Monoamine oxidase A inhibitors | ||
| Mechanism: Involves the selective, reversible inhibition of MAO-A. This inhibition leads to a decrease in the metabolism and destruction of monoamines in the neurotransmitters. This results in an increase in the monoamines. | ||
| Effect: Antidepressant agent; Monoamine Oxidase inhibition. | ||
 | Name: Phenelzine sulfate; Estinerval; Nardelzine; Kalgan; Phenethylhydrazin; Phenelzine sulfate salt | Pathogenic genes:MAOA Mechanistic genes:MAOA, MAOB Metabolic genes: Substrate:COMT, MAOA, MAOB Inhibitor:CYP2C8 (moderate), CYP2D6, CYP3A4 (moderate), MAOA, MAOB |
| IUPAC Name: (2-phenylethyl)hydrazine | ||
| Molecular Formula: C8H14N2O4S | ||
| Molecular Weight: 234.27276 g/mol | ||
| Category: Monoamine oxidase inhibitors, non-selective | ||
| Mechanism: Irreversible, non-selective inhibition of MAO. It causes an increase in the levels of serotonin, norepinephrine, and dopamine in the neuron | ||
| Effect: Antidepressant activity; Monoamine Oxidase inhibition | ||
 | Name: Rasagiline mesylate; 161735-79-1; Azilect; Rasagiline mesilate; TVP-1012; Agilect | Pathogenic genes:PARK2 Mechanistic genes:BCL2, BCL2L1, MAOB Metabolic genes: Substrate:CYP1A2 (major), CYP2D6, UGT1A1, UGT1A3, UGT1A4, UGT1A6, UGT1A7, UGT1A9, UGT1A10, UGT2B7, UGT2B15 Inhibitor: MAOB |
| IUPAC Name: (1R)-N-(prop-2-yn-1-yl)-2,3-dihydro-1H-inden-1-amine | ||
| Molecular Formula: C13H17NO3S | ||
| Molecular Weight: 267.34398 g/mol | ||
| Category: Monoamine oxidase B inhibitors | ||
| Mechanism: Potent, irreversible, selective inhibitor of brain monoamine oxidase (MAO) type B, which plays a major role in catabolism of dopamine. | ||
| Effect: Antidepressant activity; Monoamine Oxidase inhibition; Neuroprotective agent; Antiparkinsonian agent. | ||
 | Name: Selegiline; Selegiline hydrochloride; L-Deprenyl hydrochloride; 14611-52-0; Eldepryl; Selegiline Hcl; Zelapar | Pathogenic genes:MAOA, PARK2 Mechanistic genes:MAOA, MAOB Metabolic genes: Substrate:CYP1A2 (minor), CYP2A6 (minor), CYP2B6 (major), CYP2C8 (minor), CYP2C19 (major), CYP2D6 (minor), CYP2E1 (minor), CYP3A4 (minor), MAOA Inhibitor: CYP1A2 (weak), CYP2A6 (weak), CYP2C9 (weak), CYP2C19 (weak), CYP2D6 (weak), CYP2E1 (weak), CYP3A4 (weak), MAOB (strong), MAOA Transporter genes: SCNA |
| IUPAC Name: methyl(1-phenylpropan-2-yl)(prop-2-yn-1-yl)amine | ||
| Molecular Formula: C13H18ClN | ||
| Molecular Weight: 223.74172 g/mol | ||
| Category: Monoamine oxidase B inhibitors | ||
| Mechanism: Selective, irreversible inhibition of MAO-B. It binds to MAO-B within the nigrostriatal pathways in the central nervous system, thus blocking microsomal metabolism of dopamine and enhancing the dopaminergic activity in the substantia nigra. It may also increase dopaminergic activity through mechanisms other than inhibition of MAO-B. At higher doses, it can also inhibit MAO-A. | ||
| Effect: Antidepressant activity; Monoamine Oxidase inhibition Neuroprotective agent; Antiparkinsonian agent. | ||
 | Name: Tranylcypromine sulphate; Tylciprine; Phenylcyclopromine sulfate; Dl-Tranylcypromine sulfate; EINECS 236-807-1; 1-Amino-2-phenylcyclopropane sulfate | Pathogenic genes:MAOA, NTRK2, SLC6A4 Mechanistic genes:MAOA, MAOB Metabolic genes: Substrate:CYP2A6 (major) Inhibitor: CYP1A2 (moderate), CYP2A6 (strong), CYP2C8 (weak), CYP2C9 (weak), CYP2C19 (moderate), CYP2D6 (moderate), CYP2E1 (weak), CYP3A4 (weak), MAOA, MAOB Transporter genes: SLC6A4 Pleiotropic genes: FOS, NTRK2 |
| IUPAC Name: (1R)-2-phenylcyclopropan-1-amine | ||
| Molecular Formula: C18H24N2O4S | ||
| Molecular Weight: 364.45916 g/mol | ||
| Category: Monoamine oxidase inhibitors, non-selective | ||
| Mechanism: It increases endogenous concentrations of epinephrine, norepinephrine, dopamine, serotonin through inhibition of MAO responsible for breakdown of these neurotransmitters | ||
| Effect: Monoamine Oxidase inhibition; Antidepressant activity; Anti-anxiety activity | ||
| Tricyclics (TCA) and other Norepinephrinereuptake inhibitors | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Amitriptyline Hydrochloride; Annoyltin; Amitriptyline HCl; 549-18-8; Tryptizol; Domical | Pathogenic genes:ABCB1, GNB3, HTRs, NTRK2, SLC6A4, TNF Mechanistic genes:ADRA1A, HTRs, NTRK1, NTRK2 Metabolic genes: Substrate:ABCB1, CYP1A2 (minor), CYP2B6 (minor), CYP2C9 (minor), CYP2C19 (minor), CYP2D6 (major), CYP3A4/5 (major), GSTP1, UGT1A3, UGT1A4, UGT2B10 Inhibitor: ABCB1, ABCC2, ABCG2, CYP1A2 (moderate), CYP2C9 (moderate), CYP2C19 (moderate), CYP2D6 (moderate), CYP2E1 (weak) Transporter genes: ABCB1, ABCC2, ABCG2, KCNE2, KCNH2, KCNQ1, SCN5A, SLC6A4 Pleiotropic genes: FABP1, GNAS, GNB3, NTRK1, TNF |
| IUPAC Name: dimethyl(3-{tricyclo[9.4.0.0³,⁸]pentadeca-1(15),3,5,7,11,13-hexaen-2-ylidene}propyl)amine | ||
| Molecular Formula: C20H24ClN | ||
| Molecular Weight: 313.86426 g/mol | ||
| Category: Tricyclics | ||
| Mechanism: Increases synaptic concentration of serotonin and/or norepinephrine in the central nervous system by inhibiting their reuptake in the presynaptic neuronal membrane | ||
| Effect: Adrenergic Uptake inhibition; Antimigraine activity; Analgesic (nonnarcotic) activity; Antidepressant action | ||
 | Name: Amoxapine; Asendin; Demolox; 14028-44-5; Asendis; Moxadi | Pathogenic genes:GNB3, SLC6A4 Mechanistic genes:ADRA1A, ADRA2A, CHRMs, DRD1, DRD2, GABRs, GABBRs, HTRs Metabolic genes: Substrate:CYP2D6 (major) Transporter genes: SLC6A2, SLC6A4 Pleiotropic genes: DRD2, GNAS, GNB3 |
| IUPAC Name: 13-chloro-10-(piperazin-1-yl)-2-oxa-9-azatricyclo[9.4.0.0³,⁸]pentadeca-1(11),3,5,7,9,12,14-heptaene | ||
| Molecular Formula: C17H16ClN3O | ||
| Molecular Weight: 313.78144 g/mol | ||
| Category: Tricyclics | ||
| Mechanism: Reduces reuptake of serotonin and norepinephrine. The metabolite, 7-OH-amoxapine, has significant dopamine receptor-blocking activity | ||
| Effect: Serotonin uptake inhibition; Adrenergic uptake inhibition; Dopamine antagonism; Neurotransmitter uptake inhibition; Antidepressant action; Anti-anxiety activity | ||
 | Name: Clomipramine Hydrochloride; Anafranil; Clomipramine HCL; 17321-77-6; Anaphranil; 3-(3-chloro-10,11-dihydro-5H-dibenzo[b,f]azepin-5-yl)-N,N-dimethylpropan-1-amine hydrochloride | Pathogenic genes:HTR2A, SLC6A4 Mechanistic genes:ADRA1s, CHRMs, CHRNs, HRH1, HTR2s, HTR3 Metabolic genes: Substrate:CYP1A2 (major), CYP2A6, CYP2B6, CYP2C19 (major), CYP2D6 (minor), CYP3A4 (major), CYP3A5 (major), UGT1A4 Inhibitor: CYP2C9 (moderate), CYP2C19 (strong), CYP2D6 (moderate), GSTP1, SLC6A4 Transporter genes: SLC6A4 Pleiotropic genes: FABP1, PTGS2 |
| IUPAC Name: (3-{14-chloro-2-azatricyclo[9.4.0.0³,⁸]pentadeca-1(11),3,5,7,12,14-hexaen-2-yl}propyl)dimethylamine | ||
| Molecular Formula: C19H24Cl2N2 | ||
| Molecular Weight: 351.31326 g/mol | ||
| Category: Tricyclics | ||
| Mechanism: It is a strong, but not completely selective serotonin reuptake inhibitor; as its active main metabolite desmethyclomipramine acts preferably as an inhibitor of noradrenaline reuptake. α1-receptor blockage and β-down-regulation have been noted and most likely play a role in its short term effects. A blockade of sodium-channels and NDMA-receptors | ||
| Effect: Serotonin uptake inhibition; Antidepressant action; Anti-anxiety activity; Antiobsessional effects; Analgesic effects | ||
 | Name: Desipramine Hydrochloride; Norpramin; Desipramine Hcl; DMI hydrochloride; Pertofrane; Pertofran | Pathogenic genes:ABCB1, CRHR1, CRHR2, FKBP5, HTR1A, IL1B, NR3C1, NTRK2, PDE5A, SLC6A4, TBX21 Mechanistic genes:ADCY1, ADRA1A, ADRBs, CHRMs, HTR1A, IFNA1, PDE1C, PSMD9, PRKCSH, STAT3 Metabolic genes: Substrate:CYP1A2 (minor), CYP2C9, CYP2D6 (major) Inhibitor: ABCB1, CYP2A6 (moderate), CYP2B6 (moderate), CYP2C19 (moderate), CYP2D6 (moderate), CYP2E1 (weak), CYP3A4 (moderate), SLC6A2, SLC22A3 Transporter genes: ABCB1, SLC6A2, SLC6A3, SLC6A4, SLC22A3 Pleiotropic genes: NTRK2, FOS |
| IUPAC Name: (3-{2-azatricyclo[9.4.0.0³,8]pentadeca-1(15),3,5,7,11,13-hexaen-2-yl}propyl)(methyl)amine | ||
| Molecular Formula: C18H23ClN2 | ||
| Molecular Weight: 302.84162 g/mol | ||
| Category: Tricyclics | ||
| Mechanism: Increases the synaptic concentration of norepinephrine in the CNS by inhibition of its reuptake by the presynaptic neuronal membrane. Additional receptor effects including desensitization of adenyl cyclase, down-regulation of β-adrenergic receptors, and down-regulation of serotonin receptors | ||
| Effect: Enzyme inhibition; Adrenergic uptake inhibition; Antidepressant action; Analgesic activity | ||
 | Name: Doxepin Hydrochloride; Silenor; Adapin; Novoxapin; Toruan; Curatin | Pathogenic genes:ABCB1, SLC6A4 Mechanistic genes:ADRBs, CHRMs, HRH1, HRH2, HTRs Metabolic genes: Substrate:CYP1A1 (minor), CYP1A2 (minor), CYP2C9 (minor), CYP2C19 (major), CYP2D6 (major), CYP3A4/5 (minor), GSTP1, UGT1A3, UGT1A4 Inhibitor: CYP2C19 (strong), CYP2D6 (moderate) Transporter genes: ABCB1, KCNH2, SLC6A2, SLC6A4 |
| IUPAC Name: dimethyl(3-{9-oxatricyclo[9.4.0.0³,⁸]pentadeca-1(15),3,5,7,11,13-hexaen-2-ylidene}propyl)amine | ||
| Molecular Formula: C19H22ClNO | ||
| Molecular Weight: 315.83708 g/mol | ||
| Category: Tricyclics | ||
| Mechanism: It increases the synaptic concentration of serotonin and norepinephrine in the CNS by inhibition of their reuptake by the presynaptic neuronal membrane | ||
| Effect: Adrenergic uptake inhibition; Histamine Antagonism; Antidepressant action; Analgesic effects; Pruritus reduction | ||
 | Name: Imipramine Hydrochloride; Tofranil; Imipramine Hcl; 113-52-0; Chimoreptin; Feinalmin | Pathogenic genes:ABCB1, BDNF, HTR2A, SLC6A4 Mechanistic genes:ADRB2, DRD2, CHRMs, HTR2A, SCNs Metabolic genes: Substrate:CYP1A2 (minor), CYP2B6 (minor), CYP2C19 (major), CYP2D6 (major), CYP3A4 (minor), CYP3A7, GSTP1, UGT1A3, UGT1A4, UGT2B10 Inhibitor: CYP1A2 (weak), CYP2C9 (moderate), CYP2C19 (weak), CYP2D6 (moderate), CYP2E1 (weak), CYP3A4 (moderate), FMO1, SLC22A2, SLC22A3 Transporter genes: ABCB1, SLC6A2, SLC6A4, SLC22A2, SLC22A3 Pleiotropic genes: ADRB2, BDNF, FABP1, FOS, ORM1 |
| IUPAC Name: (3-{2-azatricyclo[9.4.0.0³,⁸]pentadeca-1(15),3,5,7,11,13-hexaen-2-yl}propyl)dimethylamine | ||
| Molecular Formula: C19H25ClN2 | ||
| Molecular Weight: 316.8682 g/mol | ||
| Category: Tricyclics | ||
| Mechanism: It binds the sodium-dependent serotonin transporter and sodium-dependent norepinephrine transporter preventing or reducing the reuptake of norepinephrine and serotonin by nerve cells. It causes down-regulation of cerebral cortical beta-adrenergic receptors | ||
| Effect: Adrenergic uptake inhibition; Antidepressant action; Antienuretic effects; Analgesic activity; attention enhancer | ||
 | Name: Nortriptyline Hydrochloride; Pamelor; Allegron; Altilev; Nortrilen; 894-71-3 | Pathogenic genes:ABCB1, GNB3, HTR1B, NR3C1, SLC6A4 Mechanistic genes:ADCY1, ADRA2s, ADRBs, GNB3, HRH1, HTRs Metabolic genes: Substrate:CYP1A2 (minor), CYP2C19 (minor), CYP2D6 (major), CYP3A4 (minor), UGTs Inhibitor: CYP2C8 (moderate), CYP2C9 (moderate), CYP2C19 (moderate), CYP2D6 (weak), CYP2E1 (weak), CYP3A4 (moderate) Transporter genes: ABCB1, SLC6A2, SLC6A4 Pleiotropic genes: HTR1B |
| IUPAC Name: methyl(3-{tricyclo[9.4.0.0³,⁸]pentadeca-1(15),3,5,7,11,13-hexaen-2-ylidene}propyl)amine | ||
| Molecular Formula: C19H22ClN | ||
| Molecular Weight: 299.83768 g/mol | ||
| Category: Tricyclics | ||
| Mechanism: Inhibits the reuptake of the neurotransmitter serotonin at the neuronal membrane or acts at beta-adrenergic receptors. It has additional receptor effects including desensitization of adenyl cyclase, down-regulation of β-adrenergic receptors, and down-regulation of serotonin receptors | ||
| Effect: Adrenergic uptake inhibitor; Antidepressant agent; Analgesic activity; Hypno-sedative activity | ||
 | Name: Protriptyline Hydrochloride | Mechanistic genes:SLC6A2, SLC6A4 Metabolic genes: Substrate:CYP1A2 (minor), CYP2C19 (minor), CYP2D6 (major), CYP3A4 (minor) Inhibitor: CYP1A2 (moderate), CYP2C9 (moderate), CYP2C19 (moderate), CYP2D6 (moderate), CYP3A4 (moderate) Transporter genes: SLC6A2, SLC6A4 Pleiotropic genes: ADRA1A, GNAS, ITGB3 |
| IUPAC Name: methyl(3-{tricyclo[9.4.0.0³,⁸]pentadeca-1(15),3,5,7,9,11,13-heptaen-2-yl}propyl)amine | ||
| Molecular Formula: C19H22ClN | ||
| Molecular Weight: 299.83768 g/mol | ||
| Category: Tricyclics | ||
| Mechanism: Increases synaptic concentration of serotonin and/or norepinephrine in CNS by inhibition of their reuptake by presynaptic neuronal membrane | ||
| Effect: Adrenergic uptake inhibitor; Antidepressant agent; Analgesic activity; Anti-migraine effect | ||
 | Name: Trimipramine; Sapilent; Surmontil; Beta-Methylimipramine; Trimeprimina | Pathogenic genes:ABCB1, SLC6A4 Mechanistic genes:SLC6A2, SLC6A4, SLC22A1, SLC22A2 Metabolic genes: Substrate:CYP2C19 (major), CYP2D6 (major), CYP3A4/5 (major) Inhibitor: ABCB1 Transporter genes: SLC6A2, SLC6A4, SLC22A1, SLC22A2 |
| IUPAC Name: (3-{2-azatricyclo[9.4.0.0³,8]pentadeca-1(15),3,5,7,11,13-hexaen-2-yl}-2-methylpropyl)dimethylamine | ||
| Molecular Formula: C20H26N2 | ||
| Molecular Weight: 294.43384 g/mol | ||
| Category: Tricyclics | ||
| Mechanism: Increases synaptic concentration of serotonin and/or norepinephrine in CNS by inhibition of their reuptake by presynaptic neuronal membrane | ||
| Effect: Adrenergic uptake inhibition; Antidepressant action; Antihistaminic activity; Sedative effect | ||
| Selective Serotonin and Norepinephrine Reuptake Inhibitors (SSNRI) | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Desvenlafaxine; O-Desmethylvenlafaxine; 93413-62-8; 4-(2-(Dimethylamino)-1-(1-hydroxycyclohexyl)ethyl)phenol; 4-[2-(Dimethylamino)-1-(1-hydroxycyclohexyl)ethyl]phenol; Desvenlafaxine (INN) | Pathogenic genes:ABCB1, SLC6A4 Mechanistic genes:HTR1A, SLC6A2, SLC6A3, SLC6A4 Metabolic genes: Substrate:CYP3A4 (minor), UGTs Inhibitor: CYP2D6 (weak), SLC6A2, SLC6A4 Transporter genes: ABCB1, SLC6A2, SLC6A4 |
| IUPAC Name: 4-[2-(dimethylamino)-1-(1-hydroxycyclohexyl)ethyl]phenol | ||
| Molecular Formula: C16H25NO2 | ||
| Molecular Weight: 263.3752 g/mol | ||
| Mechanism: It is a potent and selective serotonin and norepinephrine reuptake inhibitor | ||
| Effect: Serotonin uptake inhibition; Norepinephrine uptake inhibition; Antidepressant activity | ||
 | Name: Duloxetine Hydrochloride; 136434-34-9; Duloxetine HCl; Cymbalta; (S)-N-Methyl-3-(naphthalen-1-yloxy)-3-(thiophen-2-yl)propan-1-amine hydrochloride; (S)-Duloxetine HCl | Pathogenic genes:ABCB1, SLC6A4 Mechanistic genes:COMT, HTR1A, SLC6A2, SLC6A4 Metabolic genes: Substrate:CYP1A2 (major), CYP2D6 (major) Inhibitor: ABCB1, CYP1A2 (moderate), CYP2B6 (moderate), CYP2C19 (moderate), CYP2D6 (moderate), CYP3A4/5 (moderate), SLC6A2, SLC6A4 Transporter genes: ABCB1, SLC6A2, SLC6A4 |
| IUPAC Name: methyl[(3S)-3-(naphthalen-1-yloxy)-3-(thiophen-2-yl)propyl]amine | ||
| Molecular Formula: C18H20ClNOS | ||
| Molecular Weight: 333.8755 g/mol | ||
| Mechanism: It is a selective serotonin- and norepinephrine-reuptake inhibitor and a weak inhibitor of dopamine reuptake | ||
| Effect: Antidepressant activity; Anti-anxiety activity; Serotonin uptake inhibition; Norepinephrine uptake inhibition; Anti-Fibromyalgia agent; Analgesic activity; Urinary continence improvement | ||
 | Name: Levomilnacipran; UNII-UGM0326TXX; UGM0326TXX; Fetzima; (1S,2R)-2-(aminomethyl)-N,N-diethyl-1-phenylcyclopropane-1-carboxamide; F2695 | Pathogenic genes:SLC6A4 Mechanistic genes:HCRTR1, HCRTR2, HDC, HRH1, SLC6A2, SLC6A4 Metabolic genes: Substrate:ABCB1 (minor), CYP2C19 (minor), CYP2C8 (minor), CYP2D6 (minor), CYP2J2 (minor), CYP3A4 (major) Transporter genes: SLC6A2, SLC6A4 |
| IUPAC Name: (1S,2R)-2-(aminomethyl)-N,N-diethyl-1-phenylcyclopropane-1-carboxamide | ||
| Molecular Formula: C15H22N2O | ||
| Molecular Weight: 246.34798 g/mol | ||
| Mechanism: Potentiation of serotonin and norephinephrine in the central nervous system through inhibition of reuptake at serotonin and norepinephrine transporters | ||
| Effect: Serotonin uptake inhibition; Norepinephrine uptake inhibition; Antidepressant activity | ||
 | Name: Milnacipran Hydrochloride; Toledomin; Midalcipran; Ixel; Savella; Milnacipranum | Pathogenic genes:BDNF Mechanistic genes:ADRA2A, BDNF, SLC6A2, SLC6A4 Metabolic genes: Substrate:COMT, CYP1A2 (minor), CYP2A6 (minor), CYP2B6 (minor), CYP2C8, CYP2C9 (minor), CYP2C19 (minor), CYP2D6 (minor), CYP2E1 (minor), CYP3A4/5 (minor), UGTs Inhibitor: CYP3A4/5 (moderate) Inducer: CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP3A4/5 Transporter genes: SLC6A2, SLC6A4 |
| IUPAC Name: (1R,2S)-2-(aminomethyl)-N,N-diethyl-1-phenylcyclopropane-1-carboxamide | ||
| Molecular Formula: C15H22N2O | ||
| Molecular Weight: 246.34798 g/mol | ||
| Mechanism: It is a potent inhibitor of neuronal norepinephrine and serotonin reuptake. It inhibits norepinephrine uptake with approximately 3-fold higher potency in vitro than serotonin without directly affecting the uptake of dopamine or other neurotransmitters | ||
| Effect: Analgesic action; Anti-fibromyalgia action; Serotonin uptake inhibition; Adrenergic uptake inhibition; Antidepressant activity | ||
 | Name: Venlafaxine Hydrochloride; 99300-78-4; VENLAFAXINE HCl; Effexor XR; Dobupal; Trevilor | Pathogenic genes:ABCB1, BDNF, CREB1, FKBP5, HTR1A, HTR2A, NR3C1, SLC6A3, SLC6A4, TPH2 Mechanistic genes:BDNF, FKBP5 Metabolic genes: Substrate: ABCB1, CYP2C9 (minor), CYP2C19 (minor), CYP2D6 (major), CYP3A4 (major) Inhibitor: ABCB1, CYP1A2 (weak), CYP2B6 (weak), CYP2D6 (weak), CYP3A4 (weak), SLC6A2, SLC6A3, SLC6A4 Transporter genes: ABCB1, ABCC1, ABCG2, SLC6A2, SLC6A3, SLC6A4 Pleiotropic genes: DRD2, HTR2A, TPH2 |
| IUPAC Name: 1-[2-(dimethylamino)-1-(4-methoxyphenyl)ethyl]cyclohexan-1-ol | ||
| Molecular Formula: C17H28ClNO2 | ||
| Molecular Weight: 313.86272 g/mol | ||
| Mechanism: Active metabolite, O-desmethylvenlafaxine (ODV), are potent inhibitors of neuronal serotonin and norepinephrine reuptake and weak inhibitors of dopamine reuptake | ||
| Effect: Serotonin uptake inhibition; Norepinephrine uptake inhibition; Antidepressant activity; Anti-anxiety activity, Analgesic effects | ||
| Selective Serotonin Reuptake Inhibitors (SSRI) | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Citalopram Hydrobromide; Nitalapram; Cipram; Celexa; Celapram; Ciprapine | Pathogenic genes:ABCB1, BDNF, CREB1, CRHR1, CRHR2, FKBP5, GRIA3, GRIK2, GRIK4, GSK3B, HTR1A, HTR1B, HTR2A, MAOA, SLC6A4, TPH1, TPH2 Mechanistic genes:ADRs, CHRMs, DRDs, FKBP5, GABRs, GRIK4, HRHs, HTR1A, HTR1B, HTR1D, HTR2A, SLC6A4, TPH1 Metabolic genes: Substrate:ABCC1, COMT, CYP2C19 (major), CYP2D6 (minor), CYP3A4 (major), CYP3A5 Inhibitor: ABCB1, CYP1A2 (weak), CYP2B6 (weak), CYP2C19 (weak), CYP2D6 (weak), MAOA, MAOB Transporter genes: ABCB1, SLC6A4 Pleiotropic genes: BDNF |
| IUPAC Name: 1-[3-(dimethylamino)propyl]-1-(4-fluorophenyl)-1,3-dihydro-2-benzofuran-5-carbonitrile | ||
| Molecular Formula: C20H21FN2O | ||
| Molecular Weight: 324.391943 g/mol | ||
| Mechanism: Selectively inhibits serotonin reuptake in the presynaptic neurons and has minimal effects on norepinephrine or dopamine | ||
| Effect: Serotonin uptake inhibition; Serotonergic neurotransmission enhancer; Antidepressive activity, Agitation reduction, Anti-Anxiety activity | ||
 | Name: Escitalopram oxalate; Lexapro; Cipralex; 219861-08-2; UNII-5U85DBW7LO; Esertia | Pathogenic genes:ABCB1, CREB1, FKBP5, GRIA3, GRIK2, GRIK4, NR3C1, SLC6A4 Mechanistic genes:ADRAs, ADRBs, DDC, DRDs, CHRMs, GABRs, HRHs, HTRs, IL6 Metabolic genes: Substrate:ABCB1, CYP2C9 (minor), CYP2C19 (major), CYP2D6 (major), CYP3A4 (major) Inhibitor: ABCB1, CYP1A2 (weak), CYP2C9 (weak), CYP2C19 (weak), CYP2D6 (moderate), CYP2E1 (weak), CYP3A4 (weak), SLC6A4 Transporter genes: ABCB1, SLC6A4 Pleiotropic genes: IL6 |
| IUPAC Name: (1S)-1-[3-(dimethylamino)propyl]-1-(4-fluorophenyl)-1,3-dihydro-2-benzofuran-5-carbonitrile | ||
| Molecular Formula: C22H23FN2O5 | ||
| Molecular Weight: 414.426823 g/mol | ||
| Mechanism: Inhibits the reuptake of serotonin with little to no effect on norepinephrine or dopamine reuptake. It has very low affinity for 5-HT1-7, α - and β-adrenergic, D1-5, H1-3, M1-5, and benzodiazepine receptors | ||
| Effect: Serotonin uptake inhibition; Serotonergic neurotransmission enhancer; Antidepressive activity; Anti-anxiety activity | ||
 | Name: Fluoxetine Hydrochloride; Prozac; Fluoxetine Hcl; 59333-67-4; Sarafem; Fluctin | Pathogenic genes:ABCB1, BDNF, CREB1, FKBP5, GSK3B, HTR1A, HTR2A, MAOA, NR3C1, NTRK2, SLC6A4, TBX21, TPH1, TPH2 Mechanistic genes:BDNF, CHRMs, CREB1, DRD3, GSK3B, HTRs, MAOA, SLC6A4, TPH2 Metabolic genes: Substrate:CYP1A2 (major), CYP2B6 (major), CYP2C8 (major), CYP2C9 (major), CYP2C19 (major), CYP2D6 (major), CYP2E1 (minor), CYP3A4/5 (major), POR Inhibitor: ABCB1, CYP1A2 (moderate), CYP2B6 (weak), CYP2C8 (moderate), CYP2C9 (weak), CYP2C19 (moderate), CYP2D6 (strong), CYP3A4 (moderate), MAOA, SLC6A4 Transporter genes: ABCB1, KCNH2, SLC6A4 Pleiotropic genes: DRD3, FABP1, HTR2A, IFNA1, NTRK2, PDE5A, TPH1 |
| IUPAC Name: methyl({3-phenyl-3-[4-(trifluoromethyl)phenoxy]propyl})amine | ||
| Molecular Formula: C17H19ClF3NO | ||
| Molecular Weight: 345.78707 g/mol | ||
| Mechanism: Potentiates serotonergic activity in CNS resulting from its inhibition of CNS neuronal reuptake of serotonin | ||
| Effect: Serotonin uptake inhibition; Serotonin agent; Antidepressive activity; Anti-obsessive activity; Anti-anxiety activity; Anorexigenic effects | ||
 | Name: Fluvoxamine Maleate; Luvox; 61718-82-9; Fevarin; Faverin; Floxyfral | Pathogenic genes:BDNF, HTR2A, SIGMAR1, TPH1 Mechanistic genes:BDNF, HTRs, SLC6A4, SIGMAR1 Metabolic genes: Substrate:CYP1A2 (major), CYP2C19 (major), CYP2D6 (major), CYP3A4 (major) Inhibitor: ABCB1, CYP1A2 (strong), CYP2B6 (weak), CYP2C9 (moderate), CYP2C19 (moderate), CYP2D6 (moderate), CYP3A4 (weak), MAOA, SLC6A4 Transporter genes: ABCB1, KCNH2, SCL6A4 Pleiotropic genes: CREB1, TPH1 |
| IUPAC Name: (2-aminoethoxy)({5-methoxy-1-[4-(trifluoromethyl)phenyl]pentylidene})amine | ||
| Molecular Formula: C19H25F3N2O6 | ||
| Molecular Weight: 434.40681 g/mol | ||
| Mechanism: Inhibits CNS neuron serotonin uptake | ||
| Effect: Antidepressive activity; Anti-anxiety activity; Serotonin uptake inhibition | ||
 | Name: Paroxetine; Paxil; Aropax; Paxil CR; Seroxat; Pexeva | Pathogenic genes:ABCB1, CREB1, HTR1B, HTR2A, HTR3B, MAOA, SLC6A3, SLC6A4, TNF, TPH1, TPH2 Mechanistic genes:CREB1, HTR2A, HTR3A, SLC6A4, STAT3, TNF Metabolic genes: Substrate:ABCB1, COMT, CYP1A2 (minor), CYP2C19 (minor), CYP2D6 (major), CYP3A4 (major), MAOA, MAOB Inhibitor: ABCB1, CYP1A2 (weak), CYP2B6 (moderate), CYP2C9 (weak), CYP2C19 (weak), CYP2D6 (strong), CYP3A4 (weak), SLC6A3, SLC6A4 Transporter genes: ABCB1, SLC6A3, SLC6A4 Pleiotropic genes: HTR1D, HTR3C, HTR6, HTT, TPH1, TPH2 |
| IUPAC Name: (3S,4R)-3-[(2H-1,3-benzodioxol-5-yloxy)methyl]-4-(4-fluorophenyl)piperidine | ||
| Molecular Formula: C19H20FNO3 | ||
| Molecular Weight: 329.365403 g/mol | ||
| Mechanism: It is an SSRI. Presumably acts by inhibiting serotonin reuptake from brain synapse stimulating its activity in the brain | ||
| Effect: Serotonin uptake inhibition; Serotonergic neurotransmission enhancer; Antidepressant activity; Anti-anxiety activity; Anti-obsessive activity. | ||
 | Name: Sertraline Hydrochloride; 79559-97-0; Sertraline HCl; Zoloft; Lustral; Gladem | Pathogenic genes:ABCB1, CREB1, GNB3, HTR1B, MAOA, SIGMAR1, SLC6A4, TNF, TPH1, TPH2 Mechanistic genes:HTR1B, HTR1D, SIGMAR1, SLC6A2, SLC6A3, SLC6A4, TNF Metabolic genes: Substrate:CYP2A6, CYP2B6 (minor), CYP2C9 (minor), CYP2C19 (major), CYP2D6 (minor), CYP3A4 (minor), MAOA, MAOB, UGT1A1, UGT2B7 Inhibitor: ABCB1, ACHE, CYP1A1, CYP1A2 (weak), CYP2B6 (moderate), CYP2C8 (weak), CYP2C9 (weak), CYP2C19 (moderate), CYP2D6 (moderate), CYP3A4 (moderate), SLC6A4 Transporter genes: ABCB1, SLC6A2, SLC6A3, SLC6A4 Pleiotropic genes: FABP1, FOS, GNB3, TPH1, TPH2 |
| IUPAC Name: (1S,4S)-4-(3,4-dichlorophenyl)-N-methyl-1,2,3,4-tetrahydronaphthalen-1-amine | ||
| Molecular Formula: C17H18Cl3N | ||
| Molecular Weight: 342.69052 g/mol | ||
| Mechanism: It has selective inhibitory effects on presynaptic serotonin reuptake and only very weak effects on norepinephrine and dopamine neuronal uptake | ||
| Effect: Serotonin uptake inhibition; Serotonergic neurotransmission enhancer; Antidepressant activity; Anti-anxiety activity; Anti-obsessive activity | ||
| Serotonin Modulators | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Nefazodone Hydrochloride; Serzone; Nefazodone Hcl; Dutonin; 82752-99-6; Menfazon | Pathogenic genes:ABCB1, HTR1A, HTR2A Mechanistic genes:ADRA1A, HTR1s, HTR2s Metabolic genes: Substrate:CYP2D6 (major), CYP3A4 (major), CYP3A5 (major) Inhibitor: ABCB1, ABCC2, CYP1A2 (weak), CYP2B6 (weak), CYP2C8 (weak), CYP2D6 (weak), CYP3A4 (strong), SLC6A2 Transporter genes: ABCB1, ABCC2, ABCB11, SLC6A2 |
| IUPAC Name: 1-{3-[4-(3-chlorophenyl)piperazin-1-yl]propyl}-3-ethyl-4-(2-phenoxyethyl)-4,5-dihydro-1H-1,2,4-triazol-5-one | ||
| Molecular Formula: C25H33Cl2N5O2 | ||
| Molecular Weight: 506.46782 g/mol | ||
| Mechanism: Blocks potently and selectively postsynaptic 5-HT2A receptors and moderately inhibits serotonin and noradrenaline reuptake. Also blocks α1 receptors. Antagonist of adrenoceptors alpha 1 and 5-hydroxytryptamine receptors 2 | ||
| Effect: Serotonin uptake inhibition; Noradrenaline uptake inhibition; Alpha-adrenergic antagonism; Antidepressant activity; Muscle relaxation, Sedation | ||
 | Name: Trazodone Hydrochloride; Desyrel; 25332-39-2; Trazodone Hcl; Molipaxin; Trittico | Pathogenic genes:ABCB1, GNB3, HTR1A, HTR2A, SLC6A4 Mechanistic genes:ADRA1s, ADRA2s, HRH1, HTR2A, HTR2C Metabolic genes: Substrate:CYP1A2 (minor), CYP2D6 (minor), CYP3A4 (major), GSTs, SOD2 Inhibitor: CYP2D6 (moderate), CYP3A4 (weak), SLC6A4 Inducer: ABCB1 Transporter genes: ABCB1, SLC6A4 Pleiotropic genes: GNAS, GNB3, HTR2A |
| IUPAC Name: 2-{3-[4-(3-chlorophenyl)piperazin-1-yl]propyl}-2H,3H-[1,2,4]triazolo[4,3-a]pyridin-3-one | ||
| Molecular Formula: C19H23Cl2N5O | ||
| Molecular Weight: 408.32482 g/mol | ||
| Mechanism: Inhibits reuptake of serotonin, causes adrenoreceptor subsensitivity, and induces significant changes in 5-HT presynaptic receptor adrenoreceptors. Also significantly blocks histamine (H1) and α1-adrenergic receptors | ||
| Effect: Serotonin uptake inhibitor; Anti-anxiety activity; Antidepressant agent; Hypnotic effects | ||
| Miscellaneous Antidepressants | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Agomelatine; 138112-76-2; Valdoxan; Thymanax; Melitor; N-(2-(7-Methoxynaphthalen-1-yl)ethyl)acetamide | Mechanistic genes:HTR2C, MTNR1A, MTNR1B Metabolic genes: Substrate:CYP1A1 (major), CYP1A2 (major), CYP2C9 (minor), CYP2C19 (minor) |
| IUPAC Name: N-[2-(7-methoxynaphthalen-1-yl)ethyl]acetamide | ||
| Molecular Formula: C15H17NO2 | ||
| Molecular Weight: 243.30098 g/mol | ||
| Category: Melatonergic agonist and 5-HT2C antagonists | ||
| Mechanism: It behaves as an agonist at melatonin receptors and as an antagonist at serotonin (5-HT)(2C) receptors | ||
| Effect: Norepinephrine-dopamine disinhibitor; Antidepressant activity; Anti-anxiety activity; Sleep induction; Circadian rhythms resynchronization; Psychological excitement reduction | ||
 | Name: Bupropion Hydrochloride; 31677-93-7; Wellbutrin; Zyban; Bupropion Hcl | Pathogenic genes:SLC6A3, SLC6A4 Mechanistic genes:ADRA1A, CHRNB2, DRD2 Metabolic genes: Substrate:COMT, CYP1A2 (minor), CYP2A6 (minor), CYP2B6 (major) CYP2C9 (minor), CYP2C19 (minor), CYP2D6 (minor), CYP2E1 (minor), CYP3A4 (minor) Inhibitor: CYP2D6 (strong) Transporter genes: SLC6A2, SLC6A3, SLC6A4 Pleiotropic genes: DRD2 |
| IUPAC Name: 2-(tert-butylamino)-1-(3-chlorophenyl)propan-1-one | ||
| Molecular Formula: C13H19Cl2NO | ||
| Molecular Weight: 276.20206 g/mol | ||
| Category: Dopamine-Reuptake Inhibitor | ||
| Mechanism: It is a relatively weak inhibitor of the neuronal uptake of norepinephrine and dopamine | ||
| Effect: Dopamine uptake inhibition; Anti-addiction/Substance abuse treatment agent; Smoking cessation enhancer; Antidepressant activity | ||
 | Name: Mirtazapine; Zispin; Remergil; Remeron; 6-Azamianserin; Remergon | Pathogenic genes:ABCB1, FKBP5, HTR1A, HTR2A, MAOA, SLC6A3, SLC6A4, TPH2 Mechanistic genes:ADRA1s, ADRA2A, CHRMs, FKBP5, HRH1, HTR2s, HTR3s Metabolic genes: Substrate:CYP1A2 (major), CYP2C9 (minor), CYP2D6 (major), CYP3A4 (major), UGT1A1, UGT1A3, UGT1A4, UGT1A6, UGT1A7, UGT1A9, UGT1A10, UGT2B7, UGT2B15 Inhibitor: CYP1A2 (weak), CYP3A4 (weak), CYP2D6 (weak), MAOA, MAOB Inducer: CYP1A2, CYP2D6, CYP3A4 Transporter genes: ABCB1, SLC6A3, SLC6A4 Pleiotropic genes: TPH2 |
| IUPAC Name: 5-methyl-2,5,19-triazatetracyclo[13.4.0.02, .08,13]nonadeca-1(15),8,10,12,16,18-hexaene | ||
| Molecular Formula: C17H19N3 | ||
| Molecular Weight: 265.35286 g/mol | ||
| Category: α2-Adrenergic Antagonist | ||
| Mechanism: It has central presynaptic α2-adrenergic antagonist effects, which result in increased release of norepinephrine and serotonin. Also a potent antagonist of 5-HT2 and 5-HT3 serotonin receptors, H1 histamine receptors and a moderate peripheral α1-adrenergic and muscarinic antagonist | ||
| Effect: Histamine H1 antagonism; Adrenergic alpha-antagonism; Antidepressant activity; Anxiolytic effects | ||
 | Name: Reboxetine Mesylate; Vestra mesylate; Davedax mesylate; Reboxetine mesilate; Edronax; 98769-84-7 | Pathogenic genes:ABCB1, SLC6A3, SLC6A4 Mechanistic genes:ADRs, CHRMs, CHRNs, HRHs, DRDs, GH1, HTRs, POMC, PRL Metabolic genes: Substrate:CYP3A4 (major) Inhibitor: ABCB1, CYP2D6 (weak), CYP3A4 (weak) Transporter genes: ABCB1, SLC6A2, SLC6A3, SLC6A4 Pleiotropic genes: ADRB2, POMC |
| IUPAC Name: (2S)-2-[(S)-2-ethoxyphenoxy(phenyl)methyl]morpholine | ||
| Molecular Formula: C20H27NO6S | ||
| Molecular Weight: 409.49648 g/mol | ||
| Category: Norepinephrine inhibitor | ||
| Mechanism: It is a highly selective and potent inhibitor of noradrenaline reuptake. Only has weak effect on 5-HT reuptake | ||
| Effect: Adrenergic uptake inhibitor; Antidepressant activity; Anti-anxiety activity; Attention enhancer | ||
| Barbiturates | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Amobarbital; Amylobarbitone; Barbamyl; Pentymal; Amytal; Barbamil | Pathogenic genes:GABRs Mechanistic genes:CHRNAs, CLCNs, GABRAs, GABRBs, GRIA2, NDUFs Metabolic genes: Substrate:UGT2B7, UGT2B15 Inducer:CYP2A6 Transporter genes:CLCNs |
| IUPAC Name: 5-ethyl-5-(3-methylbutyl)-1,3-diazinane-2,4,6-trione | ||
| Molecular Formula: C11H18N2O3 | ||
| Molecular Weight: 226.27222 g/mol | ||
| Mechanism: Interferes with transmission of impulses resulting in an imbalance in central inhibitory and facilitatory mechanisms. Binds to alpha or beta subunits of GABA-A receptor. Decreases input resistance, depresses burst and tonic firing, especially in ventrobasal and intralaminar neurons. Increases burst duration and mean conductance at individual chloride channels and the amplitude and decay time of inhibitory postsynaptic currents. Blocks the AMPA receptor and appears to bind neuronal nicotinic acetylcholine receptors. | ||
| Effect: Hypnotic activity; Sedation; GABA modulator | ||
 | Name: Mephobarbital; Mebaral; Mephobarbitone; Enphenemal; Prominal; Methylphenobarbitone | Pathogenic genes:GABRA1, GABRB3, GABRG2, GABRD Mechanistic genes:GABRAs, GABRBs, GABRD, GABRE, GABRGs, GABRP, GABRQ, GABRRs Metabolic genes: Substrate:CYP2B6 (minor), CYP2C9 (minor), CYP2C19 (major), CYP2D6 Inhibitor: CYP2C19 (weak) Inducer: CYP2A6 |
| IUPAC Name: 5-ethyl-1-methyl-5-phenyl-1,3-diazinane-2,4,6-trione | ||
| Molecular Formula: C13H14N2O3 | ||
| Molecular Weight: 246.26186 g/mol | ||
| Mechanism: Increases seizure threshold in motor cortex. Depresses monosynaptic and polysynaptic transmission in CNS. | ||
| Effect: Hypnotic activity; Sedation; Anti-anxiety; GABA Modulator, Anticonvulsant | ||
 | Name: Pentobarbital; Pentobarbitone; Nembutal; Mebubarbital; Mebumal; Ethamina | Pathogenic genes:BDNF, IL6, TNF Mechanistic genes:GABRA6, GABRB3, GRIA1, GRIA2, NPY Metabolic genes: Substrate:CYP1A2, CYP2B6, CYP2D6, PTGS1, PTGS2 Inducer: CYP2A6, CYP3A4 Transporter genes: KCNE1, KCNH2, NR1I2, NR1I3, Pleiotropic genes: APP, BDNF, BLK, CNR1, CRHR1, FOS, ICAM1, IL1B, IL6, KRAS, NPPA, NPY, TNF, TNFRSF1A |
| IUPAC Name: 5-ethyl-5-pentan-2-yl-1,3-diazinane-2,4,6-trione | ||
| Molecular Formula: C11H18N2O3 | ||
| Molecular Weight: 226.27222 g/mol | ||
| Mechanism: Prolongs the post-synaptic inhibitory effect of GABA in the thalamus. Inhibits the excitatory AMPA-type glutamate receptors, resulting in a profound suppression of glutamatergic neurotransmission | ||
| Effect: Hypnotic activity; Sedation; GABA Modulator; Anticonvulsant; Anesthesia (Adjuvant) | ||
 | Name: Phenobarbital; Luminal; Phenobarbitone; Phenobarbitol; Gardenal; Phenemal | Pathogenic genes:CASR, GABRA6, LEP, PSEN1, PTGS2, TGFB1, TNF Mechanistic genes:CACNs, CLCNs, GABRAs, GRIAs, GSTA1, NR1I3 Metabolic genes: Substrate:ABCC2, ACSL4, CBR3, CES1, CES2, COMT, CYP1A2 (minor), CYP2C9 (minor), CYP2C19 (major), CYP2E1 (minor), CYP4B1, CYP7A1, EPHX1, GSTM1, GSTP1, GSTT1, NNMT, NQO1, TBXAS1, TPMT Inhibitor: ABCB1, ABCC2, ABCC4, ABCG2, CYP2C19 (strong), CYP2J2 (strong), CYP27A1 (strong), SLC10A1, SULT1A1 Inducer: ABCB1, ABCC1, ABCC2, ABCC3, ABCC4, CYP1A1, CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C18, CYP2C19, CYP2D6, CYP2E1, CYP3A4, CYP4A11, CYP4F3, CYP7A1, CYP8B1, CYP24A1, SCN1A, SLC22A1, SLCO1B1, SULT1C2, SULT2A1, TPMT, UGT1A1, UGT1A4, UGT1A7, UGT1A9, UGT2B7 Transporter genes: ABCB1, ABCB11, ABCC1, ABCC2, ABCC3, ABCC4, ABCC6, ABCG2, SCN1A, SLC22A1, SLCO1B1, SLCO1B3, SLCO2B1, SLC10A1 Pleiotropic genes: ACHE, ADIPOQ, AHR, APOA1, APOE, CAT, CBS, CCND1, CDA, CXCR2, DDC, DPP4, FGB, FKBP5, GH1, GNAS, GRK5, HLA-B, HNF4A, IGF1, IL1B, IL6, LEP, LEPR, LIPC, MET, MTNR1A, NR1I2, NR3C1, PPARGC1A, PRKAB1, PSEN2, RB1, RXRA, TGFB1, TNF |
| IUPAC Name: 5-ethyl-5-phenyl-1,3-diazinane-2,4,6-trione | ||
| Molecular Formula: C12H12N2O3 | ||
| Molecular Weight: 232.23528 g/mol | ||
| Mechanism: It is a barbituric acid derivative that acts as a nonselective central nervous system depressant. It potentiates action on GABA-A receptors, and modulates chloride currents through receptor channels. It also inhibits glutamate induced depolarizations | ||
| Effect: Hypnotic activity; Sedation; GABA Modulator; Anticonvulsant; Carcinogen; Central Nervous System Depressant; Excitatory Amino Acid Antagonist; Respiratory depression (dose-dependent) | ||
| Benzodiazepines | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Alprazolam; Xanax; Trankimazin; Tafil; Cassadan; Tranquinal | Pathogenic genes: GABRs Mechanistic genes: CLCNs, GABRs Metabolic genes: Substrate: CYP1A1 (minor), CYP1A2 (minor), CYP2B6, CYP2C9, CYP2C19 (minor), CYP2D6 (minor), CYP3A4/5 (major) Transporter genes: CLCNs |
| IUPAC Name: 8-chloro-1-methyl-6-phenyl-4H-[1,2,4]triazolo[4,3-a][1,4]benzodiazepine | ||
| Molecular Formula: C17H13ClN4 | ||
| Molecular Weight: 308.76492 g/mol | ||
| Mechanism: Binds to the GABA benzodiazepine receptor complex, particularly in the limbic system and reticular formation. The inhibitory effect of GABA on neuronal excitability increases the neuronal membrane permeability to chloride ions resulting in hyperpolarization and stabilization | ||
| Effect: Anti-Anxiety Agent; Hypnotic activity; Sedation; GABA Modulator | ||
 | Name: Bromazepam; Compedium; Creosedin; Lectopam; Lexaurin; Lexilium | Pathogenic genes:GABRs Mechanistic genes:CLCNs, GABRs Metabolic genes: Substrate:CYP1A2, CYP2C19, CYP3A4 (major), CYP3A5 Inhibitor: CYP2E1 (weak) Transporter genes: ABCB1, CLCNs |
| IUPAC Name: 7-bromo-5-pyridin-2-yl-1,3-dihydro-1,4-benzodiazepin-2-one | ||
| Molecular Formula: C14H10BrN3O | ||
| Molecular Weight: 316.1527 g/mol | ||
| Mechanism: Binds to stereospecific benzodiazepine receptors on the postsynaptic GABA neuron in the Central Nervous System (limbic system, reticular formation). Enhances the inhibitory GABA-effect on neuronal excitability by increasing cellular permeability to chloride ions, resulting in hyperpolarization (a less excitable state) and stabilization of cellular membrane | ||
| Effect: Anti-Anxiety Agent; GABA Modulator; Skeletal muscle relaxant | ||
 | Name: Chlordiazepoxide; Chlozepid; Elenium; Chlorodiazepoxide; Methaminodiazepoxide; Chlordiazepoxid | Pathogenic genes:BDNF, CLCNs, GABRs Mechanistic genes:CLCNs, GABRs Metabolic genes: Substrate:CYP2D6, CYP3A4 (major) Transporter genes: ABCB1, CLCNs Pleiotropic genes: BDNF |
| IUPAC Name: 7-chloro-4-hydroxy-N-methyl-5-phenyl-3H-1,4-benzodiazepin-2-imine | ||
| Molecular Formula: C16H14ClN3O | ||
| Molecular Weight: 299.75486 g/mol | ||
| Mechanism: Binds to the GABA receptor type A and increases the inhibitory effect of GABA on neuronal excitability by enhancing neuronal membrane permeability to chloride ions, thus resulting in hyperpolarization and stabilization | ||
| Effect: Sedation; Anti-Anxiety Agent; GABA Modulator, Skeletal muscle relaxant, Anticonvulsant; Amnesic properties, Anesthesia (Adjuvant) | ||
 | Name: Clobazam; Urbanyl; Chlorepin; Clorepin; Frisium; Clobazamum | Pathogenic genes:GABRA1, GABRB3, GABRG2, GABRD Mechanistic genes:CLCNs, GABRs Metabolic genes: Substrate:CYP2B6 (minor), CYP2C18 (minor), CYP2C19 (major), CYP3A4 (major), CYP3A5 (major) Transporter genes: CLCNs |
| IUPAC Name: 7-chloro-1-methyl-5-phenyl-1,5-benzodiazepine-2,4-dione | ||
| Molecular Formula: C16H13ClN2O2 | ||
| Molecular Weight: 300.73962 g/mol | ||
| Mechanism: Binds to stereospecific receptors on the postsynaptic GABA neuron at several sites within the CNS (limbic system, reticular formation). Enhances the inhibitory effect of GABA on neuronal excitability by increasing neuronal membrane permeability to chloride ions, which results in hyperpolarization (a less excitable state) and stabilization | ||
| Effect: Anti-Anxiety Agent; GABA Modulator; Anticonvulsant | ||
 | Name: Clonazepam; Rivotril; Antelepsin; Iktorivil; Chlonazepam; Cloazepam | Pathogenic genes:GABRA1 Mechanistic genes:GABRAsMetabolic genes: Substrate:CYP3A4/5 (major), NAT2 |
| IUPAC Name: 5-(2-chlorophenyl)-7-nitro-1,3-dihydro-1,4-benzodiazepin-2-one | ||
| Molecular Formula: C15H10ClN3O3 | ||
| Molecular Weight: 315.7112 g/mol | ||
| Mechanism: Enhance the activity of γ-aminobutyric acid (GABA). Suppresses the spike-and-wave discharge in absence seizures by depressing nerve transmission in the motor cortex. Depresses all levels of the CNS, including the limbic and reticular formation, by binding to the benzodiazepine site on the GABA receptor complex and modulating GABA | ||
| Effect: Anticonvulsant; GABA Modulator; Antipanic effect | ||
 | Name: Clorazepate Dipotassium; Tranxilium; Tranxene; Abbott-35616; 4306 CB; Dipotassium clorazepate | Pathogenic genes:GABRs Mechanistic genes:CLCNs, GABRs Metabolic genes: Substrate:CYP3A4 (major), CYP3A5 (major) Transporter genes: CLCNs |
| IUPAC Name: dipotassium;7-chloro-2-oxo-5-phenyl-1,3-dihydro-1,4-benzodiazepine-3-carboxylate;hydroxide | ||
| Molecular Formula: C16H11ClK2N2O4 | ||
| Molecular Weight: 408.91914 g/mol | ||
| Mechanism: Depresses all levels of the CNS, including the limbic and reticular formation, by binding to the benzodiazepine site on the γ-aminobutyric acid (GABA) receptor complex and modulating GABA, resulting in an increased neuronal membrane permeability to chloride ions which produces a hyperpolarization and stabilization | ||
| Effect: Skeletal muscle relaxant. Anti-Anxiety Agent; GABA Modulator; Anticonvulsant | ||
 | Name: Diazepam; Valium; Ansiolisina; Diazemuls; Apaurin; Faustan | Pathogenic genes:BDNF, CNR1, GABRD Mechanistic genes:ACHE, BCHE, BDNF, CACNA1C, CHRMs, GABRs, TSPO Metabolic genes: Substrate:CYP1A2 (minor), CYP2B6 (minor), CYP2C9 (minor), CYP2C19 (minor), CYP3A4/5 (major), UGTs Inhibitor: CYP2C19 (weak), CYP3A4 (weak), UGT2B7 Transporter genes: ABCB1 Pleiotropic genes: FOS, IL6, SPG7 |
| IUPAC Name: 7-chloro-1-methyl-5-phenyl-3H-1,4-benzodiazepin-2-one | ||
| Molecular Formula: C16H13ClN2O | ||
| Molecular Weight: 284.74022 g/mol | ||
| Mechanism: Binds to stereospecific benzodiazepine receptors on the postsynaptic GABA neuron at several sites within the CNS. Enhancement of the inhibitory effect of GABA on neuronal excitability results by increased neuronal membrane permeability to chloride ions, thus resulting in hyperpolarization and stabilization. It antagonizes with translocator protein | ||
| Effect: Sedation; Anti-Anxiety Agent; GABA Modulator, Skeletal muscle relaxant, Anticonvulsant; Amnesic properties, Anesthesia; Antiemetics | ||
 | Name: Estazolam; Eurodin; Nuctalon; ProSom; Esilgan; Julodin | Pathogenic genes:GABRB3 Mechanistic genes:CLCNs, GABRAs, GABRBs, GABRD, GABRE, GABRGs, GABRP, GABRQ, GABRRs, TSPO Metabolic genes: Substrate:CYP1A2, CYP2A6, CYP2C9, CYP2C19, CYP2D6, CYP2E1, CYP3A4 (major), CYP3A5 (major) Transporter genes:CLCNs |
| IUPAC Name: 8-chloro-6-phenyl-4H-[1,2,4]triazolo[4,3-a][1,4]benzodiazepine | ||
| Molecular Formula: C16H11ClN4 | ||
| Molecular Weight: 294.73834 g/mol | ||
| Mechanism: Binds to stereospecific benzodiazepine receptors on the postsynaptic GABA neuron at several sites within the CNS, including the limbic system, reticular formation. Enhancement of the inhibitory effect of GABA on neuronal excitability results by increased neuronal membrane permeability to chloride ions. This shift in chloride ions results in hyperpolarization (a less excitable state) and stabilization | ||
| Effect: Anti-Anxiety Agent; GABA Modulator; Hypnotic activity; Sedation; Skeletal muscle relaxant; Anticonvulsant | ||
 | Name: Flurazepam; Dalmane; Dalmadorm; Flurazepamum; Felmane; Noctosom | Pathogenic genes:GABRB3 Mechanistic genes:CACNA1C, CLCNs, GABRs Metabolic genes: Substrate:CYP3A4 (major), CYP3A5 (major), MAO Inhibitor: ABCB1, CYP2E1 (weak) Transporter genes: ABCB1, CACNA1C, CLCNs |
| IUPAC Name: 7-chloro-1-[2-(diethylamino)ethyl]-5-(2-fluorophenyl)-3H-1,4-benzodiazepin-2-one | ||
| Molecular Formula: C21H23ClFN3O | ||
| Molecular Weight: 387.878223 g/mol | ||
| Mechanism: Binds to stereospecific benzodiazepine receptors on the postsynaptic GABA neuron at several sites within the CNS, including the limbic system, reticular formation. Enhancement of inhibitory effect of GABA on neuronal excitability results by increased neuronal membrane permeability to chloride ions | ||
| Effect: Anti-Anxiety Agent; GABA Modulator; Sedation | ||
 | Name: Lorazepam; Ativan; Temesta; O-Chloroxazepam; O-Chlorooxazepam; Almazine | Pathogenic genes:GABRs Mechanistic genes:CLCNs, GABRs, TSPO Metabolic genes: Substrate:CYP3A4 (minor), UGT1A1, UGT1A3, UGT1A4, UGT1A6, UGT1A7, UGT1A9, UGT1A10, UGT2B4, UGT2B7, UGT2B15 Transporter genes: CLCNs |
| IUPAC Name: 7-chloro-5-(2-chlorophenyl)-3-hydroxy-1,3-dihydro-1,4-benzodiazepin-2-one | ||
| Molecular Formula: C15H10Cl2N2O2 | ||
| Molecular Weight: 321.1581 g/mol | ||
| Mechanism: Binds to stereospecific benzodiazepine receptors on postsynaptic GABA neuron at several sites within CNS, including limbic system, reticular formation. Enhancement of inhibitory effect of GABA on neuronal excitability results by increased neuronal membrane permeability to chloride ions. This shift in chloride ions results in hyperpolarization (a less excitable state) and stabilization. Binds to GABAA receptors enhancing the effects of GABA by increasing GABA affinity for its receptor | ||
| Effect: Anti-Anxiety Agent; GABA Modulator; Sedation; Skeletal muscle relaxant; Anticonvulsant. Antiemetic; Hypnotic activity; Preanesthetic agent | ||
 | Name: Midazolam; Versed; Dormicum; Midazolamum; 59467-70-8; Midazolamum | Mechanistic genes:CLCNs, GABRs Metabolic genes: Substrate:CYP1A2, CYP2A6, CYP2B6 (minor), CYP2C19 (minor), CYP2D6, CYP2E1, CYP3A4 (major), CYP3A5 (major), CYP3A7, UGT1A4, UGT2B7, UGT2B10 Inhibitor: CYP2C8 (weak), CYP2C9 (weak), CYP3A4 (strong) Inducer: CYP3A4 Transporter genes: ABCB1, CLCNs, NR1I2 |
| IUPAC Name: 8-chloro-6-(2-fluorophenyl)-1-methyl-4H-imidazo[1,5-a][1,4]benzodiazepine | ||
| Molecular Formula: C18H13ClFN3 | ||
| Molecular Weight: 325.767323 g/mol | ||
| Mechanism: Binds to stereospecific benzodiazepine receptors on postsynaptic GABA neuron. Enhancement of inhibitory effect of GABA on neuronal excitability results by increased neuronal membrane permeability to chloride ions. This shift in chloride ions results in hyperpolarization (a less excitable state) and stabilization | ||
| Effect: Sedation; Hypnotic activity; Anti-Anxiety Agent; GABA Modulator, Skeletal muscle relaxant; Amnestic properties; Anesthesia; Preanesthetia | ||
 | Name: Nitrazepam; Benzalin; Mogadon; Remnos; Nitrados; Imeson | Pathogenic genes:GABRA1, GABRB3, GABRG2, GABRD Mechanistic genes:CLCNs, GABRs, GLRs Metabolic genes: Substrate:CYP3A4 (major) Transporter genes: CLCNs |
| IUPAC Name: 7-nitro-5-phenyl-1,3-dihydro-1,4-benzodiazepin-2-one | ||
| Molecular Formula: C15H11N3O3 | ||
| Molecular Weight: 281.26614 g/mol | ||
| Mechanism: Binds to stereospecific benzodiazepine receptors on postsynaptic GABA neuron at CNS (limbic system, reticular formation). Enhances inhibitory effect of GABA on neuronal excitability by increasing neuronal membrane permeability to chloride ions | ||
| Effect: Sedation; Hypnotic activity; Anticonvulsant; Anti-Anxiety Agent; GABA Modulator | ||
 | Name: Oxazepam; Adumbran; Tazepam; Serax; Anxiolit; Praxiten | Pathogenic genes:GABRs Mechanistic genes:CLCNs, GABRs Metabolic genes: Substrate:CYP2D6, UGT2B7, UGT2B15 Inhibitor:UGT2B7 Inducer: CYP1A2 Transporter genes: CLCNs |
| IUPAC Name: 7-chloro-3-hydroxy-5-phenyl-1,3-dihydro-1,4-benzodiazepin-2-one | ||
| Molecular Formula: C15H11ClN2O2 | ||
| Molecular Weight: 286.71304 g/mol | ||
| Mechanism: Effects appear to be mediated through inhibitory neurotransmitter GABA; site and mechanism of action within the CNS appear to involve macromolecular complex (GABAA-receptor-chloride ionophore complex) which includes GABAA receptors, high-affinity benzodiazepine receptors, and chloride channels. Enhancement of inhibitory effect of GABA on neuronal excitability results by increased neuronal membrane permeability to chloride ions. This shift in chloride ions results in hyperpolarization (less excitable state) and stabilization | ||
| Effect: Sedation; GABA Modulator; Anti-Anxiety Agent; Anti-Alcohol withdrawal agent | ||
 | Name: Quazepam; Doral; Dormalin; Prosedar; Oniria; Quazium | Pathogenic genes:GABRB3 Mechanistic genes:CLCNs, GABRs Metabolic genes: Substrate:CYP2C9 (minor), CYP2C19 (minor), CYP3A4 (major), FMO1, FMO3 Transporter genes: CLCNs |
| IUPAC Name: 7-chloro-5-(2-fluorophenyl)-1-(2,2,2-trifluoroethyl)-3H-1,4-benzodiazepine-2-thione | ||
| Molecular Formula: C17H11ClF4N2S | ||
| Molecular Weight: 386.794253 g/mol | ||
| Mechanism: Binds to stereospecific benzodiazepine receptors on postsynaptic GABA neuron at several sites within CNS (limbic system, reticular formation). Enhances inhibitory effect of GABA on neuronal excitability by increasing neuronal membrane permeability to chloride ions, resulting in hyperpolarization and stabilization | ||
| Effect: Hypnotic activity; Sedation; GABA Modulator; Anti-Anxiety Agent | ||
 | Name: Temazepam; Euhypnos; Restoril; Hydroxydiazepam; Methyloxazepam; Crisonar | Pathogenic genes:GABRB3 Mechanistic genes:CLCNs, GABRs, TSPO Metabolic genes: Substrate:CYP2B6 (major), CYP2C9 (major), CYP2C19 (major), CYP3A4 (major), UGT1A1, UGT1A3, UGT1A4, UGT1A6, UGT1A9, UGT1A10, UGT2B7, UGT2B15 Inhibitor: UGT1A3, UGT2B7 Transporter genes: CLCNs |
| IUPAC Name: 7-chloro-3-hydroxy-1-methyl-5-phenyl-3H-1,4-benzodiazepin-2-one | ||
| Molecular Formula: C16H13ClN2O2 | ||
| Molecular Weight: 300.73962 g/mol | ||
| Mechanism: A short half-life benzodiazepine. Binds to stereospecific benzodiazepine receptors on postsynaptic GABA neuron at several sites within CNS, including limbic system. Enhances inhibitory effect of GABA on neuronal excitability results by increased neuronal membrane permeability to chloride ions. This shift in chloride ions results in hyperpolarization (a less excitable state) and stabilization. It antagonizes with translocator protein | ||
| Effect: Hypnotic activity; Sedation; GABA Modulator; Anti-Anxiety Agent; Antidepressant activity; Anticonvulsant | ||
 | Name: Triazolam; Halcion; Songar; Clorazolam; Novidorm; Trilam | Pathogenic genes:GABRB3 Mechanistic genes:CLCNs, GABRs, TSPO Metabolic genes: Substrate:CYP3A4 (major), CYP3A5 (major) Inhibitor: CYP2C8 (weak), CYP2C9 (weak) Transporter genes: CLCNs |
| IUPAC Name: 8-chloro-6-(2-chlorophenyl)-1-methyl-4H-[1,2,4]triazolo[4,3-a][1,4]benzodiazepine | ||
| Molecular Formula: C17H12Cl2N4 | ||
| Molecular Weight: 343.20998 g/mol | ||
| Mechanism: Binds to stereospecific benzodiazepine receptors on postsynaptic GABA neuron at several sites within CNS, including limbic system, reticular formation. Enhancement of inhibitory effect of GABA on neuronal excitability results by increased neuronal membrane permeability to chloride ions. This shift in chloride ions results in hyperpolarization (less excitable state) and stabilization. | ||
| Effect: Sedation; GABA Modulator; Anesthesia (Adjuvant) | ||
| Miscellaneous | ||
| Drug | Properties | Pharmacogenetics |
 | Name: Buspirone; Ansial; Buspirona; Buspironum; Bespar; Anxiron | Mechanistic genes:DRD2, HTR1A, HTR2A, HTR3s Metabolic genes: Substrate:CYP2D6 (minor), CYP3A4 (major), CYP3A5 (minor) Inducer: CYP3A4 Pleiotropic genes: DRD2, HTR2A |
| IUPAC Name: 8-[4-(4-pyrimidin-2-ylpiperazin-1-yl)butyl]-8-azaspiro[4.5]decane-7,9-dione | ||
| Molecular Formula: C21H31N5O2 | ||
| Molecular Weight: 385.50314 g/mol | ||
| Mechanism: Decreases the spontaneous firing of serotonin-containing neurons in the CNS by selectively binding to and acting as agonist at presynaptic CNS serotonin 5-HT1A receptors. Possesses partial agonist activity (mixed agonist/antagonist) at postsynaptic 5-HT2A receptors. Does not bind to benzodiazepine-GABA receptors. Binds to dopamine D2 receptors | ||
| Effect: Serotonin receptor agonist; Anti-Anxiety Agent | ||
 | Name: Chloral Hydrate; Noctec; Tosyl; 302-17-0; 2,2,2-Trichloroethane-1,1-diol; Trichloroacetaldehyde hydrate | Pathogenic genes:GABRAs Mechanistic genes:GABRAs; GLRs; HTR3s Pleiotropic genes:FOS, IL1B, IL6 |
| IUPAC Name: 2,2,2-trichloroethane-1,1-diol | ||
| Molecular Formula: C2H3Cl3O2 | ||
| Molecular Weight: 165.40302 g/mol | ||
| Mechanism: It is converted to the active compound trichloroethanol by hepatic alcohol dehydrogenase. The agent interacts with various neurotransmitter-operated ion channels, thereby enhancing gamma-aminobutyric acid (GABA)-A receptor mediated chloride currents and inhibiting amino acid receptor-activated ion currents. Enhances the agonistic effects of glycine receptors, inhibits AMPA-induced calcium influx in cortical neurons, and facilitates 5-HT 3 receptor-mediated currents in ganglionic neurons. Overall, this results in a depressive effect on the central nervous system | ||
| Effect: Hypnotic activity; Sedation; Anticonvulsant; Anesthesia; Analgesic activity; GABA Modulator | ||
 | Name: Dexmedetomidine Hydrochloride; Dexmedetomidina; Dexmedetomidinum; MPV 1440; Precedex; CHEBI:4466 | Mechanistic genes:ADRA2A, ADRA2B, ADRA2C Metabolic genes: Substrate:CYP2A6 (major), UGT1A4, UGT2B10 Inhibitor: CYP1A2 (weak), CYP2C9 (weak), CYP2D6 (strong), CYP3A4 (weak) Inducer: ABCC2, CYP7A1, CYP27A1 Transporter genes: ABCC2 |
| IUPAC Name: 5-[(1S)-1-(2,3-dimethylphenyl)ethyl]-1H-imidazole | ||
| Molecular Formula: C13H16N2 | ||
| Molecular Weight: 200.27954 g/mol | ||
| Mechanism: Binds to the presynaptic alpha-2 adrenoceptors and inhibits the release of norepinephrine, therefore, terminate the propagation of pain signals. Activation of the postsynaptic alpha-2 adrenoceptors inhibits the sympathetic activity | ||
| Effect: α2-Adrenergic Agonist; Anesthesia; Sedation; Analgesia | ||
 | Name: Promethazine Hydrochloride; Phenergan; Promethazine Hcl; 58-33-3; Fenergan; Atosil | Mechanistic genes:ADRA1A, CHRM2, DRD2, HRH1 Metabolic genes: Substrate:CYP2B6 (major), CYP2D6 (major) Inhibitor: CYP2C9 (weak), CYP2D6 (weak) Transporter genes: ABCB1 |
| IUPAC Name: N,N-dimethyl-1-phenothiazin-10-ylpropan-2-amine;hydrochloride | ||
| Molecular Formula: C17H21ClN2S | ||
| Molecular Weight: 320.88004 g/mol | ||
| Mechanism: Blocks postsynaptic mesolimbic dopaminergic receptors in brain. Exhibits strong α-adrenergic-blocking effect and depresses release of hypothalamic and hypophyseal hormones. Competes with histamine for H1-receptor. Reduces stimuli to brainstem reticular system. The relief of nausea is related to central anticholinergic actions | ||
| Effect: Sedation; Anti-Allergic Agent; Antiemetic; Antipruritic; Histamine H1 Antagonist | ||
 | Name: Ramelteon; Rozerem; 196597-26-9; TAK-375; Rozerem | Pathogenic genes:MTNR1A, MTNR1B Mechanistic genes:MTNR1A, MTNR1B Metabolic genes: Substrate:CYP1A2 (major), CYP2C19 (minor), CYP3A4 (minor) |
| IUPAC Name: N-[2-[(8S)-2,6,7,8-tetrahydro-1H-cyclopenta[e][1]benzofuran-8-yl]ethyl]propanamide | ||
| Molecular Formula: C16H21NO2 | ||
| Molecular Weight: 259.34344 g/mol | ||
| Mechanism: Potent, selective agonist of melatonin receptors MT1 and MT2 (with little affinity for MT3) within suprachiasmic nucleus of hypothalamus | ||
| Effect: Melatonin receptor agonist; Hyptonic activity; circadian rhythm regulation | ||
 | Name: Zaleplon; Sonata; 151319-34-5; CL-284846; Zerene; CL 284846 | Mechanistic genes:GABRA1 Metabolic genes: Substrate:AOX1, CYP3A4 (major), CYP2D6, POR Pleiotropic genes: HRH1 |
| IUPAC Name: N-[3-(3-cyanopyrazolo[1,5-a]pyrimidin-7-yl)phenyl]-N-ethylacetamide | ||
| Molecular Formula: C17H15N5O | ||
| Molecular Weight: 305.3339 g/mol | ||
| Mechanism: Interacts with benzodiazepine GABA receptor complex. Nonclinical studies have shown that it binds selectively to brain ω1 receptor situated on α-subunit of GABA-A receptor complex | ||
| Effect: Hypnotic activity; Sedation; Skeletal muscle relaxant; Anti-anxiety agent; Anticonvulsant; GABA Modulator | ||
 | Name: Zolpidem Tartrate; 99294-93-6; schembl40721; MLS001401453; Bio-0153; chembl1723343 | Mechanistic genes:CLCNs, GABRA1, TSPO Metabolic genes: Substrate:CYP1A2 (minor), CYP2C9 (minor), CYP2C19 (minor), CYP2D6 (minor), CYP3A4 (major) Inhibitor: CYP3A4 (strong) Transporter genes: CLCNs, NR1I2 |
| IUPAC Name: 2,3-dihydroxybutanedioic acid;N,N-dimethyl-2-[6-methyl-2-(4-methylphenyl)imidazo[1,2-a]pyridin-3-yl]acetamide | ||
| Molecular Formula: C23H27N3O7 | ||
| Molecular Weight: 457.47638 g/mol | ||
| Mechanism: Enhances activity of inhibitory neurotransmitter, GABA, via selective agonism at benzodiazepine-1 (BZ1) receptor. Result is increased chloride conductance, neuronal hyperpolarization, inhibition of action potential, and decrease in neuronal excitability | ||
| Effect: Central nervous system depression; GABA-A receptor agonist; Hypnotic activity; Sedation | ||
 | Name: Zopiclone; Imovane; Zimovane; Amoban; (+-)-Zopiclone; 43200-80-2 | Mechanistic genes:CLCNs, GABRAs Metabolic genes: Substrate:CYP2C8 (major), CYP2C9 (major), CYP2C19 (minor), CYP2D6, CYP3A4 (major) Transporter genes: CLCNs |
| IUPAC Name: [6-(5-chloropyridin-2-yl)-5-oxo-7H-pyrrolo[3,4-b]pyrazin-7-yl] 4-methylpiperazine-1-carboxylate | ||
| Molecular Formula: C17H17ClN6O3 | ||
| Molecular Weight: 388.80828 g/mol | ||
| Mechanism: Reduces sleep latency, increases duration of sleep, and decreases number of nocturnal awakenings. Binds to the benzodiazepine receptor complex and modulates the GABABZ receptor chloride channel macromolecular complex. Acts on α1, α2, α3 and α5 GABAA containing receptors as a full agonist causing an enhancement of the inhibitory actions of GABA. | ||
| Effect: Hypnotic activity; Sedation | ||
| Antiepileptics | ||
|---|---|---|
| Drug | Properties | Pharmacogenetics |
 | Name: Carbamazepine | Mechanistic genes:EPHX1,HSPA1L, MTHFR, SCN1A Metabolic genes: Substrate:CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C19, CYP2E1, CYP3A4, CYP3A5, CYP3A7, GSTM1, GSTT1, UGT2B7 Inhibitor:CYP1A2 Inducer: ABCB1, ABCB4, ABCC2, ABCG2, CYP1A1, CYP1A2, CYP2A6, CYP2B6; CYP2C8; CYP2C9; CYP2C19; CYP2D6, CYP3A4, GSTA1, SULT1A1, UGT1A4 Transporter genes: ABCB1, ABCB4, ABCC2 Pleiotropic genes: HLA-A, HLA-B, IL6 |
| IUPAC Name: 5H-Dibenz[b,f]azepine-5-carboxamide | ||
| Molecular Formula: C15H12N2O | ||
| Molecular Weight: 236.27 g/mol | ||
| Mechanism: The anticonvulsant activity of carbamazepine, like phenytoin, principally involves limitation of seizure propagation by reduction of post-tetanic potentiation of synaptic transmission. Carbamazepine has only slight analgesic properties. Carbamazepine appears to provide relief of pain in trigeminal neuralgia by reducing synaptic transmission within the trigeminal nucleus. The drug has also demonstrated sedative, anticholinergic, antidepressant, muscle relaxant, antiarrhythmic, antidiuretic, and neuromuscular transmission-inhibitory actions. May depress activity in the nucleus ventralis of the thalamus or decrease synaptic transmission or decrease summation of temporal stimulation leading to neural discharge by limiting influx of sodium ions across cell membrane or other unknown mechanism. May decrease the turnover of γ- aminobutyric acid (GABA). Stimulates the release of ADH and potentiates its action in promoting reabsorption of water. Chemically related to tricyclic antidepressants. | ||
| Effect: Anticonvulsants, Miscellaneous. Antimanic Agents | ||
 | Name: Clonazepam | Mechanistic genes:ALB, GABA-A Metabolic genes: Substrate:CYP2E1, CYP3A4, NAT2 |
| IUPAC Name: 2H-1,4-Benzodiazepin-2-one, 5-(2-chlorophenyl)-1,3-dihydro-7-nitro-; 5-(o-Chlorophenyl)-1,3-dihydro-7-nitro-2H-1,4-benzodiazepin-2-one | ||
| Molecular Formula: C15H10ClN3O3 | ||
| Molecular Weight: 315.71 g/mol | ||
| Mechanism: Exact mechanism of anticonvulsant, sedative, and antipanic effects is unknown; however, mechanism appears to be related to the drug’s ability to enhance the activity of γ-aminobutyric acid (GABA). Suppresses the spike-and-wave discharge in absence seizures by depressing nerve transmission in the motor cortex. Depresses all levels of the CNS, including the limbic and reticular formation, by binding to the benzodiazepine site on the GABA receptor complex and modulating GABA | ||
| Effect: Anxiolytics, Sedatives, and Hypnotics; Benzodiazepines. Anticonvulsants; Benzodiazepines | ||
 | Name: Eslicarbazepine | Metabolic genes: Substrate:ABCB1, UGT1A1, UGT1A4, UGT1A9, UGT2B7 Inhibitor:CYP2C19 Inducer:CYP3A4, UGT1A4, UGT1A9, UGT2B4, UGT2B7, UGT2B17 Pleiotropic genes:HLA-B |
| IUPAC Name: [S-(-)-10-acetoxy-10,11-dihydro-5H-dibenz[b,f]azepine-5-carboxamide]; BIA 2-093 | ||
| Molecular Formula: C17H16N2O3 | ||
| Molecular Weight: 296.32 g/mol | ||
| Mechanism: The precise mechanisms of action of eslicarbazepine acetate are unknown. However, in vitro electrophysiological studies indicate that both eslicarbazepine acetate and its metabolites stabilize the inactivated state of voltage-gated sodium channels, preventing their return to the activated state and thereby sustaining repetitive neuronal firing | ||
| Effect: Anticonvulsants, Miscellaneous. Antiepileptics, Carboxamide Derivatives | ||
 | Name: Ethosuximide | Mechanistic genes:CACNA1G Metabolic genes: Substrate:CYP2E1, CYP3A4, CYP3A5 |
| IUPAC Name: 2,5-Pyrrolidinedione, 3-ethyl-3-methyl-, (±)-; (±)-2-Ethyl-2-methylsuccinimide | ||
| Molecular Formula: C7H11NO2 | ||
| Molecular Weight: 141.17 g/mol | ||
| Mechanism: A succinimide-derivative anticonvulsant. Exact mechanism of anticonvulsant action unknown. Increases seizure threshold in cortex and basal ganglia and reduces synaptic response to low-frequency repetitive stimulation. Suppresses paroxysmal spike and wave activity of the EEG associated with lapses of consciousness common in absence seizures | ||
| Effect: Anticonvulsants; Succinimides | ||
 | Name: Felbamate | Mechanistic genes:GABR, GRIN1, GRIN2B Metabolic genes: Substrate:CYP2E1, CYP3A4, CYP3A5 Inhibitor:CYP2C19 Inducer:CYP3A4 Transporter genes:ABCB1 |
| IUPAC Name: 2-Phenyl-1,3-propanediol dicarbamate | ||
| Molecular Formula: C11H14N2O4 | ||
| Molecular Weight: 238.24 g/mol | ||
| Mechanism: Felbamate, a dicarbamate, is an anticonvulsant agent. Exact mechanism of action unknown, but it is suggested that it increases seizure threshold and reduces seizure spread. In vitro studies indicate that felbamate has weak inhibitory effects on binding at GABA receptors and benzodiazepine receptors. The monocarbamate, p-hydroxy, and 2-hydroxy metabolites of felbamate appear to contribute little, if any, to the anticonvulsant action of the drug | ||
| Effect: Anticonvulsants | ||
 | Name: Gabapentin | Mechanistic genes:GABRR1, GABRR2, KCNH2, SCN2A Metabolic genes: Inhibitor:CYP2A6 Transporter genes:ABCB1, SLC22A4 |
| IUPAC Name: 2-[1-(aminomethyl) cyclohexyl] acetic acid | ||
| Molecular Formula: C9H17NO2. | ||
| Molecular Weight: 171.24 g/mol | ||
| Mechanism: Gabapentin is an anticonvulsant agent structurally related to the inhibitory CNS neurotransmitter GABA | ||
| Effect: Anticonvulsants, Analgesics and Antipyretics | ||
 | Name: Lamotrigine | Mechanistic genes:ADORA1, ADORA2A, ADRA1A, ADRA2A, ADRB1, CACNA1E, CHRM1, CHRM2, CHRM3, CHRM4, CHRM5, DRD1, DRD2, GABRA1, GABRA2, GABRA3, GABRA5, GABRA6, GABRB1, GABRB2, GABRB3, GABRG1, GABRG2, GABRG3, GABRD, GABRE, GABRP, GABRR1, GABRR2, GABRR3, GABRQ, HRH1, HTR2A, HTR3A, OPRK1, SCN2A Metabolic genes: Substrate:DHFR, UGT1A1, UGT1A3, UGT1A4, UGT2A7 Transporter genes:ABCB1, SLC22A2 Pleiotropic genes:HLA-B |
| IUPAC Name: 1,2,4-Triazine-3,5-diamine, 6-(2,3-dichlorophenyl)-; (2) 3,5-Diamino-6-(2,3-dichlorophenyl)-as-triazine | ||
| Molecular Formula: C9H7Cl2N5 | ||
| Molecular Weight: 256.09 g/mol | ||
| Mechanism: Possibly involves inhibition of voltage-sensitive sodium channels, which stabilizes neuronal membranes and consequently modulates release of excitatory amino acid neurotransmitters (e.g. glutamate, aspartate) which play a role in generation and spread of epileptic seizures | ||
| Effect: Anticonvulsants, Miscellaneous | ||
 | Name: Levetiracetam | Metabolic genes: Substrate:CYP2D6 Transporter genes:ABCB1 |
| IUPAC Name: 1-Pyrrolidineacetamide, α-ethyl-2-oxo-, (α S)-; (2)(-)-(S) - α-Ethyl-2-oxo-1-pyrrolidineacetamide | ||
| Molecular Formula: C8H14N2O2 | ||
| Molecular Weight: 170.21 g/mol | ||
| Mechanism: The precise mechanism by which levetiracetam exerts its antiepileptic effect is unknown and does not appear to derive from any interaction with known mechanisms involved in inhibitory and excitatory neurotransmission | ||
| Effect: Anticonvulsants | ||
 | Name: Oxcarbazepine | Mechanistic genes:SCN2A Metabolic genes: Substrate:CYP3A4, UGT1A1, UGT1A3, UGT1A4, UGT1A6, UGT1A7, UGT1A9, UGT1A10, UGT2B7, UGT2B15 Inhibitor:CYP2C19 Inducer:ABCB1, CYP3A4, CYP3A5 |
| IUPAC Name: 5H-Dibenz[b,f]azepine-5-carboxamide, 10,11-dihydro-10-oxo-; 10,11-Dihydro-10-oxo-5H-dibenz[b,f]azepine-5-carboxamide | ||
| Molecular Formula: C15H12N2O2 | ||
| Molecular Weight: 252.27 g/mol | ||
| Mechanism: Pharmacological activity results from both oxcarbazepine and its monohydroxy metabolite (MHD). Oxcarbazepine and MHD block voltage-sensitive sodium channels, stabilizing hyperexcited neuronal membranes, inhibiting repetitive firing, and decreasing propagation of synaptic impulses. These actions are believed to prevent spread of seizures. Oxcarbazepine and MHD also increase potassium conductance and modulate activity of high-voltage activated calcium channels. Protects against electrically induced tonic extension seizures and, to a lesser degree, chemically-induced clonic seizures. May abolish or reduce frequency of chronically recurring focal seizures | ||
| Effect: Anticonvulsants | ||
 | Name: Phenobarbital | Mechanistic genes:COMT, GABRA1, CHRNA4, CHRNA7, GRIA2, GRIK2, GRIN1, GRIN2A, GRIN2B, GRIN2C, GRIN2D, GRIN3A, GRIN3B, NR1I2 Metabolic genes: Substrate:CYP1A1, CYP1A2, CYP1B1, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C18, CYP2C19, CYP2E1, CYP3A4, CYP3A5, CYP3A7, CYP4A11, CYP4B1, EPHX1, UGT1A1 Inhibitor:CYP2C19, CYP2J2, CYP27A1, SLC10A1, SULT1A1 Transporter genes:ABCB1, ABCB11, ABCC1, ABCC2, ABCC3, SLCO2A1 |
| IUPAC Name: 2,4,6(1H,3H,5H)-Pyrimidinetrione, 5-ethyl-5-phenyl-; (2) 5-Ethyl-5-phenylbarbituric acid | ||
| Molecular Formula: C12H12N2O3 | ||
| Molecular Weight: 232.24 g/mol | ||
| Mechanism: Long-acting barbiturate with sedative, hypnotic, and anticonvulsant properties. Barbiturates depress sensory cortex, decrease motor activity, alter cerebellar function, and produce drowsiness, sedation, and hypnosis. In high doses, barbiturates exhibit anticonvulsant activity. They also produce dose-dependent respiratory depression | ||
| Effect: Anticonvulsants; Barbiturates. Anxiolytics, Sedatives, and Hypnotics; Barbiturates | ||
 | Name: Phenytoin | Mechanistic genes:NR1I2, SCN1A, SCN1B, SCN3A, SCN5A Metabolic genes: Substrate:CYP2B6, CYP2C8, CYP2C9, CYP2C18, CYP2C19, CYP2D6, CYP3A4, CYP3A5, CYP3A7, CYP11B1, EPHX1, UGT1A1, UGT1A6, UGT1A9 Inhibitor:SCN2A, SULT1A1 Transporter genes:ALB, ABCB1, ABCC2, SLCO1B1, SLCO1C1 Pleiotropic genes:HLA-B |
| IUPAC Name: 5,5-Diphenylhydantoin | ||
| Molecular Formula: C15H12N2O2 | ||
| Molecular Weight: 252.27 g/mol | ||
| Mechanism: Stabilizes neuronal membranes and decreases seizure activity by increasing efflux or decreasing influx of sodium ions across cell membranes in motor cortex during generation of nerve impulses. Prolongs effective refractory period and suppresses ventricular pacemaker automaticity, shortens action potential in heart | ||
| Effect: Class Ib Antiarrhythmics. Anticonvulsants; Hydantoins | ||
 | Name: Primidone | Mechanistic genes:GABRAs Metabolic genes: Inducer:CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP3A4 |
| IUPAC Name: 4,6(1H,5H)-Pyrimidinedione, 5-ethyldihydro-5-phenyl-; 5-Ethyldihydro-5-phenyl-4,6(1H,5H)-pyrimidinedione | ||
| Molecular Formula: C12H14N2O2 | ||
| Molecular Weight: 218.25 g/mol | ||
| Mechanism: Decreases neuron excitability, raises seizure threshold similar to phenobarbital. Primidone has two active metabolites, phenobarbital and phenylethylmalonamide | ||
| Effect: Anticonvulsants; Barbiturates | ||
 | Name: Rufinamide | Mechanistic genes:MAPK10, SCN1A Metabolic genes: Substrate:CES Inhibitor:CYP2E1 Inducer:CYP3A4 |
| IUPAC Name: 1-[(2,6-difluorophenyl)methyl]-1H-1,2,3-triazole-4 carboxamide | ||
| Molecular Formula: C10H8F2N4O | ||
| Molecular Weight: 238.2 g/mol | ||
| Mechanism: The precise mechanism(s) by which rufinamide exerts its antiepileptic effect are unknown. The results of in vitro studies suggest that the principal mechanism of action of rufinamide is modulation of the activity of sodium channels and, in particular, prolongation of the inactive state of the channel. Rufinamide (≥ 1 μM) significantly slowed sodium channel recovery from inactivation after a prolonged prepulse in cultured cortical neurons, and limited sustained repetitive firing of sodium-dependent action potentials | ||
| Effect: Anticonvulsants; Triazole Derivative | ||
 | Name: Tiagabine | Mechanistic genes:ABAT Metabolic genes: Substrate:CYP3A4 Transporter genes:SLC6A1 |
| IUPAC Name: 3-Piperidinecarboxylic acid, 1-[4,4-bis(3-methyl-2-thienyl)-3-butenyl]-, hydrochloride, (R)-; (-)-(R)-1-[4,4-Bis(3-methyl-2-thienyl)-3-butenyl]nipecotic acid, hydrochloride. | ||
| Molecular Formula: C20H25NO2S2 HCl | ||
| Molecular Weight: 412.01 g/mol | ||
| Mechanism: Exact mechanism not definitively known; however, in vitro experiments demonstrate that it enhances activity of gamma-aminobutyric acid (GABA). It is thought that binding to GABA uptake carrier inhibits uptake of GABA into presynaptic neurons, allowing availability of increased amount of GABA to postsynaptic neurons. Based on in vitro studies, tiagabine does not inhibit uptake of dopamine, norepinephrine, serotonin, glutamate, or choline | ||
| Effect: Anticonvulsants | ||
 | Name: Topimarate | Mechanistic genes:ACSL4, AGXT, CA1-5, GABRA1, IGF1, KCNH2, NR1I2, SCN1A, SCN2A Metabolic genes: Substrate:CYP3A4 Inhibitor:CYP2C19 Inducer:ABCB1, CYP3A4 Transporter genes:ABCB1 |
| IUPAC Name: β-D-Fructopyranose, 2,3:4,5-bis-O-(1-methylethylidene)-, sulfamate; 2,3:4,5-di-O-isopropylidene-β-D-fructopyranose sulfamate | ||
| Molecular Formula: C12H21NO8S | ||
| Molecular Weight: 339.36 g/mol | ||
| Mechanism: Blocks neuronal voltage-dependent sodium channels, enhances GABA(A) activity, antagonizes AMPA/kainate glutamate receptors, and weakly inhibits carbonic anhydrase | ||
| Effect: Anticonvulsants | ||
 | Name: Valproic acid | Mechanistic genes:ABAT, ACADSB, ALDH5A1, HDAC2, HDAC9, OGDH, PPARA, PPARD, PPARG Metabolic genes: Substrate:CYP1A1, CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C18, CYP2C19, CYP2E1, CYP3A4, CYP3A5, CYP4B1, CYP4F2, PTGS1, UGT1A1, UGT1A3, UGT1A4, UGT1A6, UGT1A8, UGT1A9, UGT1A10, UGT2B7, UGT2B15 Inhibitor:CYP2A6, CYP2C9, CYP2C19, CYP2D6, CYP3A4, HDAC9, UGT1A9, UGT2B7, UGT2B15 Transporter genes:ALB, SLC16A1, SLC22A5, SLC22A6, SLC22A7, SLC22A8, SLCO2B1 |
| IUPAC Name: Pentanoic acid, 2-propyl-; (2) Propylvaleric acid | ||
| Molecular Formula: C8H16O2 | ||
| Molecular Weight: 144.21 g/mol | ||
| Mechanism: Causes increased availability of gamma-aminobutyric acid (GABA), to brain neurons or may enhance action of GABA or mimic its action at postsynaptic receptor sites | ||
| Effect: Anticonvulsants, Miscellaneous. Antimanic Agents; Histone Deacetylase Inhibitor | ||
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cacabelos, R. Pharmacogenomics of Cognitive Dysfunction and Neuropsychiatric Disorders in Dementia. Int. J. Mol. Sci. 2020, 21, 3059. https://doi.org/10.3390/ijms21093059
Cacabelos R. Pharmacogenomics of Cognitive Dysfunction and Neuropsychiatric Disorders in Dementia. International Journal of Molecular Sciences. 2020; 21(9):3059. https://doi.org/10.3390/ijms21093059
Chicago/Turabian StyleCacabelos, Ramon. 2020. "Pharmacogenomics of Cognitive Dysfunction and Neuropsychiatric Disorders in Dementia" International Journal of Molecular Sciences 21, no. 9: 3059. https://doi.org/10.3390/ijms21093059