
Fast and Sensitive Bioanalytical Method for the Determination of Deucravacitinib in Human Plasma Using HPLC-MS/MS: Application and Greenness Evaluation

 , , , and
, , , and 
Abstract
:1. Introduction
2. Results
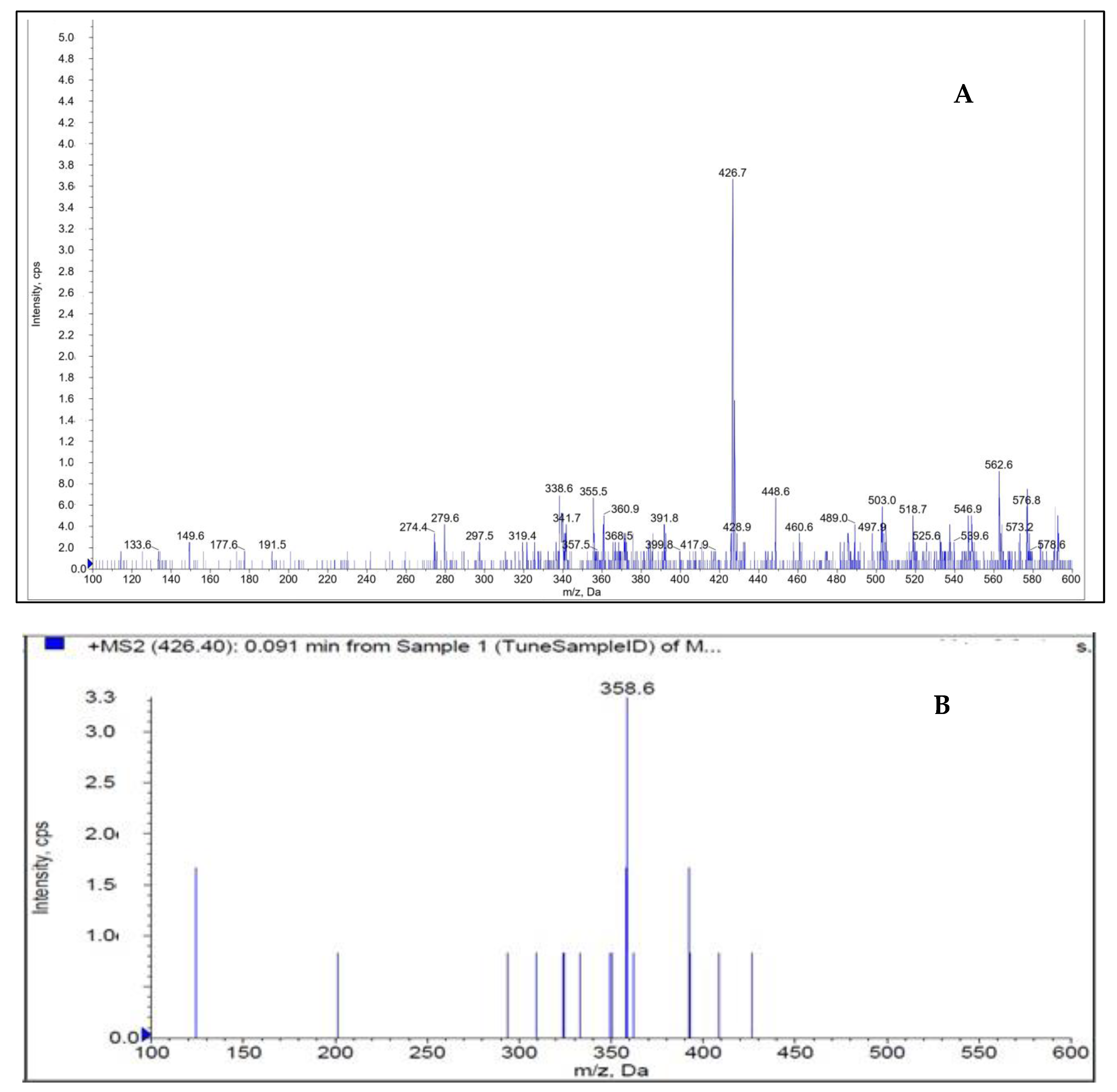
2.1. Mass Spectrophotometry
2.2. The Development of the Creative Approach
2.3. Chromatography
2.4. Method Validation
2.4.1. Specificity
2.4.2. Linearity
2.4.3. Accuracy and Precision
2.4.4. Recovery
2.4.5. Matrix Effects
2.4.6. Stability
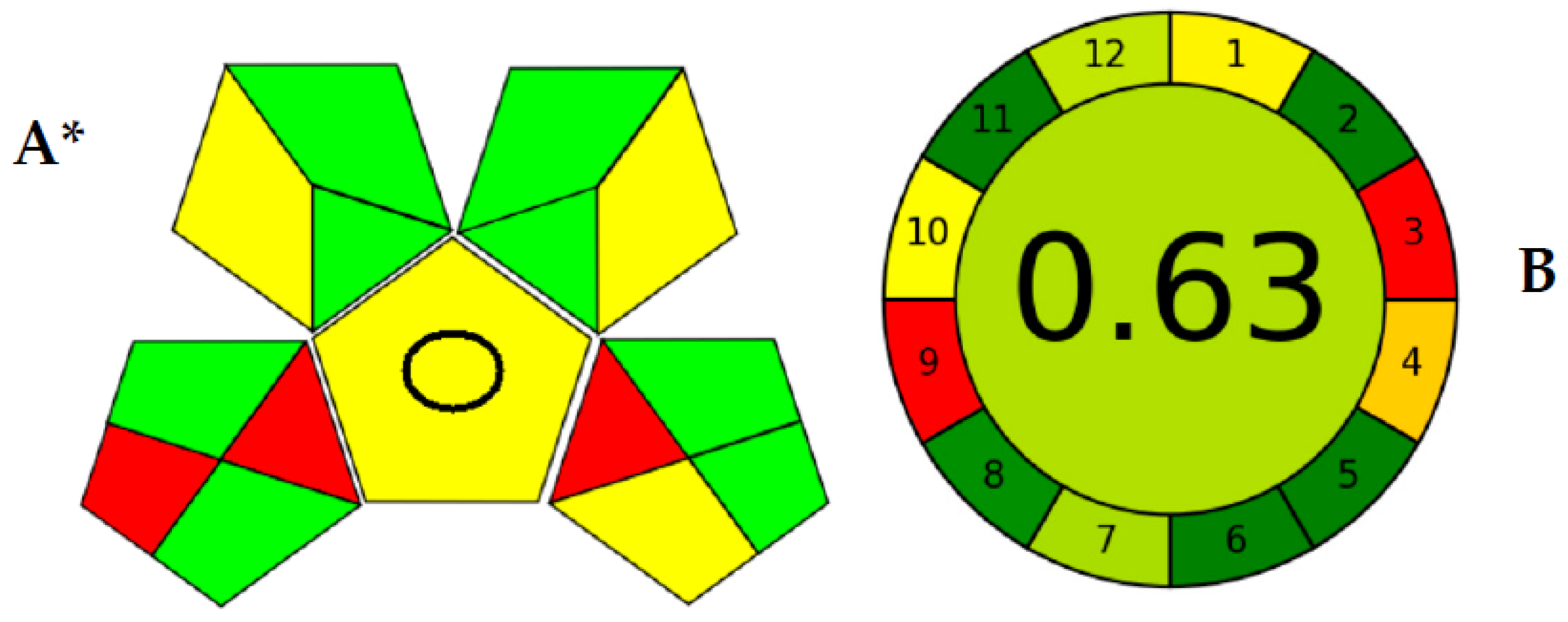
2.5. Evaluation of Method’s Analytical Greenness
3. Materials and Methods
3.1. Instrumentation
3.2. Materials
3.3. Chromatographic Conditions
3.4. Preparation of Standard Solutions
3.5. Linear Graph and Control Samples
3.6. Sample Processing
3.7. The Validation Process of Innovated Strategy
3.7.1. Selectivity
3.7.2. Precision and Accuracy of the Creative Strategy
3.7.3. Standardization and Calibration Graph
3.7.4. Stability Study of DEU
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
References
- Yao, Q.; Zhai, Y.; He, Z.; Wang, Q.; Sun, L.; Sun, T.; Lv, L.; Li, Y.; Yang, J.; Lv, D.; et al. Water-responsive gel extends drug retention and facilitates skin penetration for curcumin topical delivery against psoriasis. Asian J. Pharm. Sci. 2023, 18, 100782. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Read, C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA 2020, 323, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Omland, S.H.; Gniadecki, R. Psoriasis inversa: A separate identity or a variant of psoriasis vulgaris? Clin. Dermatol. 2015, 33, 456–461. [Google Scholar] [CrossRef]
- Sarac, G.; Koca, T.T.; Baglan, T. A brief summary of clinical types of psoriasis. North. Clin. Istanb. 2016, 3, 79. [Google Scholar] [PubMed] [Green Version]
- Gudjonsson, J.; Johnston, A.; Sigmundsdottir, H.; Valdimarsson, H. Immunopathogenic mechanisms in psoriasis. Clin. Exp. Immunol. 2004, 135, 1–8. [Google Scholar] [CrossRef]
- Brandrup, F.; Holm, N.; Grunnet, N.; Henningsen, K.; Hansen, H. Psoriasis in monozygotic twins: Variations in expression in individuals with identical genetic constitution. Acta Derm. Venereol. 1982, 62, 229–236. [Google Scholar] [PubMed]
- Roskoski, R. Deucravacitinib is an allosteric TYK2 protein kinase inhibitor FDA-approved for the treatment of psoriasis. Pharmacol. Res. 2023, 189, 106642. [Google Scholar] [CrossRef]
- Kaushik, S.B.; Lebwohl, M.G. Review of safety and efficacy of approved systemic psoriasis therapies. Int. J. Dermatol. 2019, 58, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Brownstone, N.D.; Hong, J.; Mosca, M.; Hadeler, E.; Liao, W.; Bhutani, T.; Koo, J. Biologic Treatments of Psoriasis: An Update for the Clinician. Biol. Targets Ther. 2021, 15, 39–51. [Google Scholar] [CrossRef]
- Nogueira, M.; Puig, L.; Torres, T. JAK inhibitors for treatment of psoriasis: Focus on selective TYK2 inhibitors. Drugs 2020, 80, 341–352. [Google Scholar] [CrossRef]
- Hoy, S.M. Deucravacitinib: First Approval. Drugs 2022, 82, 1671–1679. [Google Scholar] [CrossRef]
- Chimalakonda, A.; Burke, J.; Cheng, L.; Catlett, I.; Tagen, M.; Zhao, Q.; Patel, A.; Shen, J.; Girgis, I.G.; Banerjee, S. Selectivity profile of the tyrosine kinase 2 inhibitor deucravacitinib compared with Janus kinase 1/2/3 inhibitors. Dermatol. Ther. 2021, 11, 1763–1776. [Google Scholar] [CrossRef] [PubMed]
- Catlett, I.M.; Aras, U.; Hansen, L.; Liu, Y.; Bei, D.; Girgis, I.G.; Murthy, B. First-in-human study of deucravacitinib: A selective, potent, allosteric small-molecule inhibitor of tyrosine kinase 2. Clin. Transl. Sci. 2023, 16, 151–164. [Google Scholar] [CrossRef] [PubMed]
- Catlett, I.M.; Hu, Y.; Gao, L.; Banerjee, S.; Gordon, K.; Krueger, J.G. Molecular and clinical effects of selective tyrosine kinase 2 inhibition with deucravacitinib in psoriasis. J. Allergy Clin. Immunol. 2022, 149, 2010–2020.e2018. [Google Scholar] [CrossRef]
- Lé, A.M.; Puig, L.; Torres, T. Deucravacitinib for the treatment of psoriatic disease. Am. J. Clin. Dermatol. 2022, 23, 813–822. [Google Scholar] [CrossRef] [PubMed]
- Morand, E.; Pike, M.; Merrill, J.T.; van Vollenhoven, R.; Werth, V.P.; Hobar, C.; Delev, N.; Shah, V.; Sharkey, B.; Wegman, T. Deucravacitinib, a tyrosine kinase 2 inhibitor, in systemic lupus erythematosus: A phase II, randomized, double-blind, placebo-controlled trial. Arthritis Rheumatol. 2023, 75, 242–252. [Google Scholar] [CrossRef]
- Chimalakonda, A.; Singhal, S.; Darbenzio, R.; Dockens, R.; Marchisin, D.; Banerjee, S.; Girgis, I.G.; Throup, J.; He, B.; Aras, U.; et al. Lack of Electrocardiographic Effects of Deucravacitinib in Healthy Subjects. Clin. Pharmacol. Drug Dev. 2022, 11, 442–453. [Google Scholar] [CrossRef]
- Committee for Human Medicinal Products. ICH Guideline M13A on bioequivalence for immediate-release solid oral dosage forms. In Proceedings of the International Conference on Harmonization, Geneva, Switzerland, 26 January 2023; pp. 1–32. [Google Scholar]
- El-Hela, A.A.; Bakr, M.S.A.; Hegazy, M.M.; Dahab, M.A.; Elmaaty, A.A.; Ibrahim, A.E.; El Deeb, S.; Abbass, H.S. Phytochemical Characterization of Pterocephalus frutescens with In-Silico Evaluation as Chemotherapeutic Medicine and Oral Pharmacokinetics Prediction Study. Sci. Pharm. 2023, 91, 7. [Google Scholar] [CrossRef]
- Hegazy, M.M.; Afifi, W.M.; Metwaly, A.M.; Radwan, M.M.; Abd-Elraouf, M.; Mehany, A.B.M.; Ahmed, E.; Enany, S.; Ezzeldin, S.; Ibrahim, A.E.; et al. Antitrypanosomal, Antitopoisomerase-I, and Cytotoxic Biological Evaluation of Some African Plants Belonging to Crassulaceae; Chemical Profiling of Extract Using UHPLC/QTOF-MS/MS. Molecules 2022, 27, 8809. [Google Scholar] [CrossRef] [PubMed]
- Afzal, O.; Alshammari, H.A.; Altamimi, M.A.; Hussain, A.; Almohaywi, B.; Altamimi, A.S. Hansen solubility parameters and green nanocarrier based removal of trimethoprim from contaminated aqueous solution. J. Mol. Liq. 2022, 361, 119657. [Google Scholar] [CrossRef]
- DrugBank Release, Version 5.1.9; 2022. Available online: https://www.drugbank.ca (accessed on 18 June 2023).
- Sharaf, Y.A.; Ibrahim, A.E.; El Deeb, S.; Sayed, R.A. Green Chemometric Determination of Cefotaxime Sodium in the Presence of Its Degradation Impurities Using Different Multivariate Data Processing Tools; GAPI and AGREE Greenness Evaluation. Molecules 2023, 28, 2187. [Google Scholar] [CrossRef]
- Putnam, W.C.; Kallem, R.R.; Subramaniyan, I.; Beg, M.S.; Edpuganti, V. Bioanalytical method development and validation of a liquid chromatography-tandem mass spectrometry method for determination of β-lapachone in human plasma. J. Pharm. Biomed. Anal. 2020, 188, 113466. [Google Scholar] [CrossRef] [PubMed]
- El-Zaher, A.A.; Hashem, H.A.; Elkady, E.F.; Allam, M.A. A validated LC-MS/MS bioanalytical method for the simultaneous determination of dapagliflozin or saxagliptin with metformin in human plasma. Microchem. J. 2019, 149, 104017. [Google Scholar] [CrossRef]
- Chae, Y.-J.; Song, Y.-K.; Chae, S.-H.; Kim, M.J.; Kang, J.S.; Lee, J.-Y.; Koo, T.-S.; Lee, K.-R. Development and validation of an LC-MS/MS method for monitoring larotrectinib, a tropomyosin-related kinase inhibitor, in mouse and human plasma and application to pharmacokinetic studies. J. Anal. Sci. Technol. 2020, 11, 20. [Google Scholar] [CrossRef]
- United States Pharmacopoeia USP 43-NF 38; United States Pharmacopeia: Rockville, MD, USA, 2021.
- Gu, H.; Liu, G.; Wang, J.; Aubry, A.-F.; Arnold, M.E. Selecting the correct weighting factors for linear and quadratic calibration curves with least-squares regression algorithm in bioanalytical LC-MS/MS assays and impacts of using incorrect weighting factors on curve stability, data quality, and assay performance. Anal. Chem. 2014, 86, 8959–8966. [Google Scholar] [PubMed]
- Salman, B.I.; Hara, M.A.; El Deeb, S.; Ibrahim, A.E.; Saraya, R.E.; Ali, M.F.B. Zinc(II) complexation strategy for ultra-sensitive fluorimetric estimation of molnupiravir: Applications and greenness evaluation. Arch. Pharm. 2023, 356, 2300005. [Google Scholar] [CrossRef] [PubMed]
- Gałuszka, A.; Migaszewski, Z.M.; Konieczka, P.; Namieśnik, J. Analytical Eco-Scale for assessing the greenness of analytical procedures. TrAC Trends Anal. Chem. 2012, 37, 61–72. [Google Scholar] [CrossRef]
- Płotka-Wasylka, J. A new tool for the evaluation of the analytical procedure: Green Analytical Procedure Index. Talanta 2018, 181, 204–209. [Google Scholar] [CrossRef]
- Pena-Pereira, F.; Wojnowski, W.; Tobiszewski, M. AGREE—Analytical GREEnness Metric Approach and Software. Anal. Chem. 2020, 92, 10076–10082. [Google Scholar] [CrossRef]
- Nowak, P.M.; Wietecha-Posłuszny, R.; Pawliszyn, J. White Analytical Chemistry: An approach to reconcile the principles of Green Analytical Chemistry and functionality. TrAC Trends Anal. Chem. 2021, 138, 116223. [Google Scholar] [CrossRef]
- Nowak, P.M.; Kościelniak, P. What color is your method? Adaptation of the RGB additive color model to analytical method evaluation. Anal. Chem. 2019, 91, 10343–10352. [Google Scholar] [CrossRef] [PubMed]
- Ballester-Caudet, A.; Campíns-Falcó, P.; Pérez, B.; Sancho, R.; Lorente, M.; Sastre, G.; González, C. A new tool for evaluating and/or selecting analytical methods: Summarizing the information in a hexagon. TrAC Trends Anal. Chem. 2019, 118, 538–547. [Google Scholar] [CrossRef]
- Ibrahim, A.E.; Elmaaty, A.A.; El-Sayed, H.M. Determination of six drugs used for treatment of common cold by micellar liquid chromatography. Anal. Bioanal. Chem. 2021, 413, 5051–5065. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, D. New US FDA draft guidance on bioanalytical method validation versus current FDA and EMA guidelines: Chromatographic methods and ISR. Bioanalysis 2014, 6, 13–19. [Google Scholar] [CrossRef]
- Salman, B.I. A Novel Design Eco-friendly Microwave-assisted Cu–N@ CQDs Sensor for the Quantification of Eravacycline via Spectrofluorimetric Method; Application to Greenness Assessments, Dosage Form and Biological Samples. J. Fluoresc. 2023, 1–10. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Name | Q1 Mass (amu) | Q3 Mass (amu) | Dwell (ms) | DP (V) | EP (V) | CE (V) | CXP (V) |
|---|---|---|---|---|---|---|---|
| Deucravacitinib | 426.7 | 358.6 | 200 | 110 | 10 | 32 | 10.30 |
| Trimethoprim | 291.1 | 261.1 | 200 | 110 | 10 | 32 | 10.30 |
| CUR (psi) | CAD (psi) | Ion Spray Voltage (V) | TEM (°C) | GAS 1 (psi) | GAS 2 (psi) | Scan Type | Polarity |
| 20 | 10 | 5500 | 500 | 40 | 40 | MRM | Positive |
| Parameter | Details |
|---|---|
| Column | ACE C18 (100 × 4.6 mm, 5 µm) |
| Pump mode | Isocratic |
| Column temperature | Ambient |
| Flow rate | 0.9 mL min−1 |
| Injection volume | 5.0 µL |
| Run time | 3.0 min |
| Detector | Tandem mass spectrometry (MRM mode) |
| Mobile phase | Methanol: 2 mM ammonium formate (80:20, v/v) |
| Calibration Standard ID | Nominal Conc. (ng mL−1) | Calculated Conc. (ng mL−1) |
|---|---|---|
| STD1 | 0.500 | 0.488 |
| STD2 | 1.001 | 1.082 |
| STD3 | 2.502 | 2.271 |
| STD4 | 10.007 | 10.447 |
| STD5 | 50.037 | 43.694 |
| STD6 | 200.150 | 264.329 |
| STD7 | 540.945 | 468.146 |
| STD8 | 601.050 | 687.353 |
| Slope | 0.0362 | |
| Intercept | 0.000404 | |
| Correlation Coefficient (r2) | 0.9941 | |
| Standard/Concentration | LQC (1.444 ng mL−1) | MQC (240.733 ng mL−1) | HQC (456.798 ng mL−1) | Sensitivity LLQC (0.4803 ng mL−1) | ||||
|---|---|---|---|---|---|---|---|---|
| R% | RSD | R% | RSD | R% * | RSD ** | R% | RSD | |
| Accuracy | 108.14 | 5.34 | 108.59 | 3.03 | 95.98 | 3.65 | 96.07 | 9.5 |
| Intra-day Precision | 108.43 | 5.79 | 108.58 | 3.29 | 95.78 | 3.50 | ||
| Inter-day Precision | 105.08 | 6.25 | 106.94 | 3.22 | 97.41 | 3.15 | ||
| n | n = 6 | |||||||
| QC Sample | Recovery ± RSD% (n = 6) |
|---|---|
| LQC | 60.89 ± 1.50 |
| MQC | 66.82 ± 2.02 |
| HQC | 68.36 ± 1.88 |
| Average ± RSD% | 65.35 ± 1.50 |
| Parameter | DEU | IS | IS Normalization |
|---|---|---|---|
| Matrix factor | 0.94 | 0.95 | 0.99 |
| RSD | 2.37 | 4.20 | 2.89 |
| Standard (ng/mL) | Room Temperature Stability | Auto-Sampler Stability | Refrigerator Stability | |||
|---|---|---|---|---|---|---|
| R% | RSD | R% | RSD | R% * | RSD ** | |
| LQC (1.444) | 107.96 | 1.47 | 108.07 | 2.36 | 107.63 | 2.50 |
| HQC (456.798) | 102.66 | 0.60 | 102.58 | 0.51 | 98.96 | 2.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahesh, P.; Haque, M.A.; Salman, B.I.; Belal, T.S.; Ibrahim, A.E.; El Deeb, S. Fast and Sensitive Bioanalytical Method for the Determination of Deucravacitinib in Human Plasma Using HPLC-MS/MS: Application and Greenness Evaluation. Molecules 2023, 28, 5471. https://doi.org/10.3390/molecules28145471
Mahesh P, Haque MA, Salman BI, Belal TS, Ibrahim AE, El Deeb S. Fast and Sensitive Bioanalytical Method for the Determination of Deucravacitinib in Human Plasma Using HPLC-MS/MS: Application and Greenness Evaluation. Molecules. 2023; 28(14):5471. https://doi.org/10.3390/molecules28145471
Chicago/Turabian StyleMahesh, Pottabattula, M. Akiful Haque, Baher I. Salman, Tarek S. Belal, Adel Ehab Ibrahim, and Sami El Deeb. 2023. "Fast and Sensitive Bioanalytical Method for the Determination of Deucravacitinib in Human Plasma Using HPLC-MS/MS: Application and Greenness Evaluation" Molecules 28, no. 14: 5471. https://doi.org/10.3390/molecules28145471