

Application of Multiscale Sample Entropy in Assessing Effects of Exercise Training on Skin Blood Flow Oscillations in People with Spinal Cord Injury
 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Experimental Protocol
2.3. Time Domain Assessment of SBF
2.4. Multiscale Sample Entropy Analysis
2.5. Surrogate Tests
2.6. Statistical Analysis
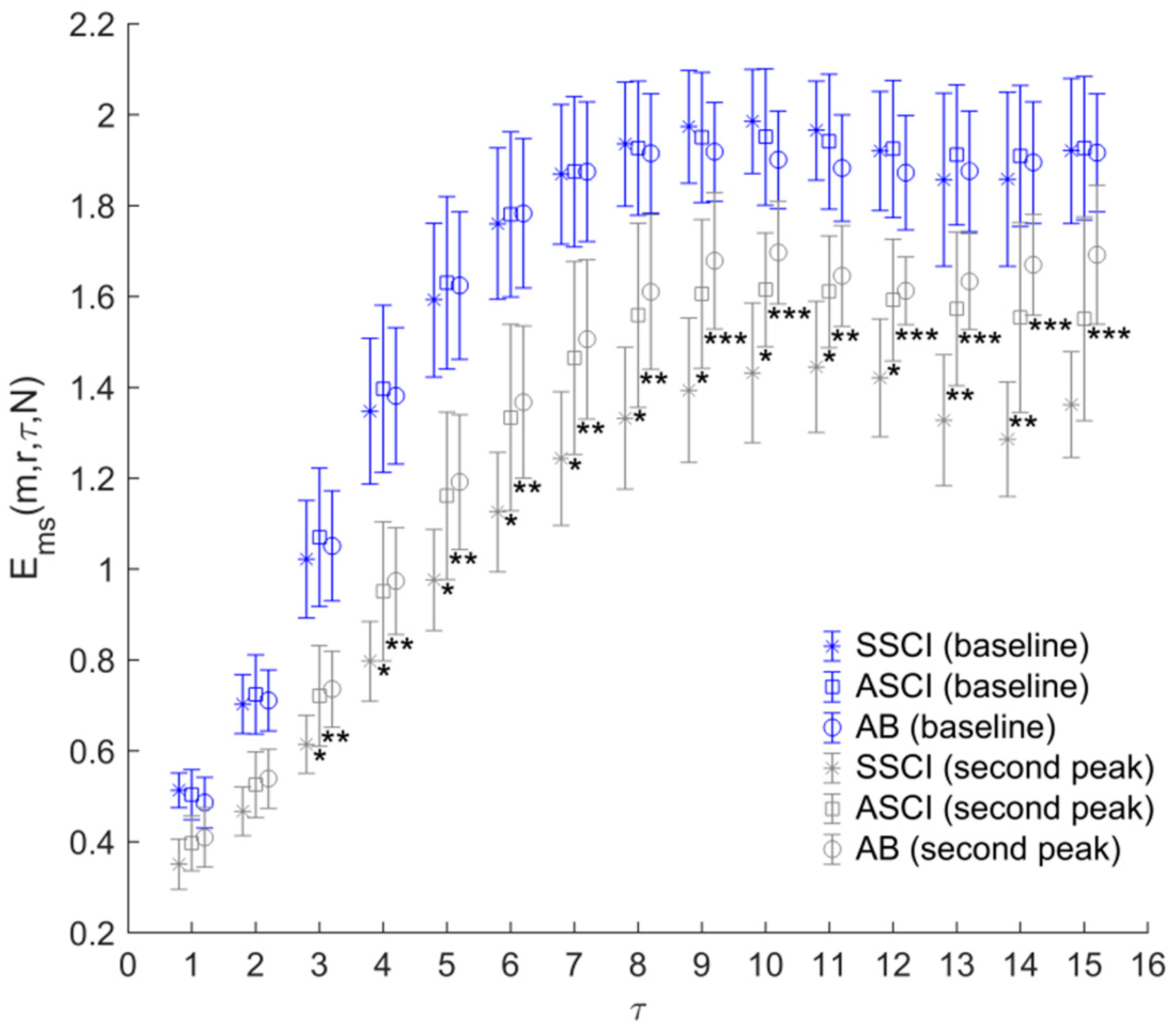
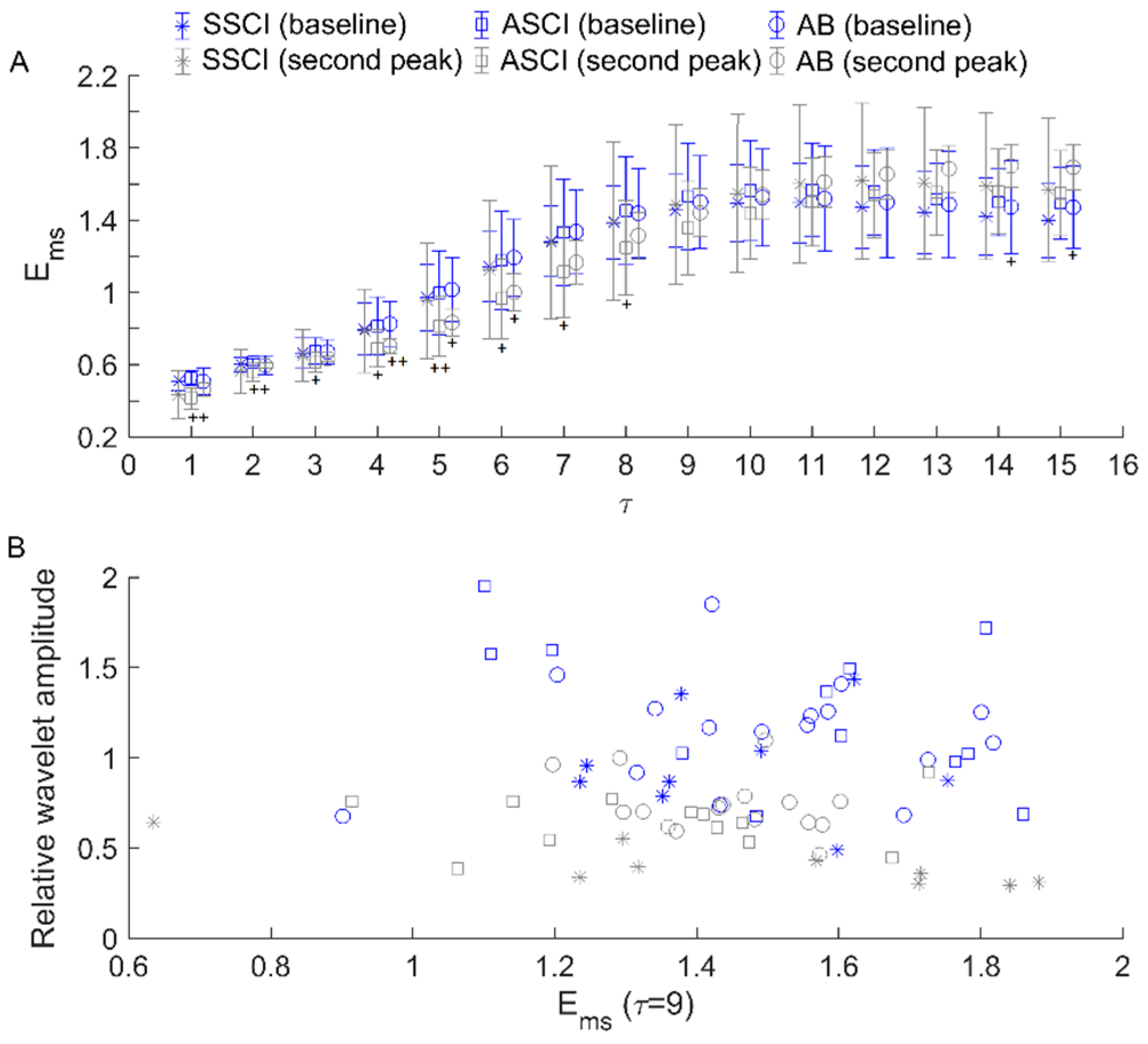
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Krassioukov, A.; Biering-Sorensen, C.F.; Donovan, W.; Kennelly, M.; Kirshblum, S.; Krogh, K.; Alexander, M.S.; Vogel, L.; Wecht, J. International Standards to document remaining Autonomic Function after Spinal Cord Injury (ISAFSCI), First Edition 2012. Top. Spinal Cord Inj. Rehabil. 2012, 18, 282–296. [Google Scholar] [CrossRef]
- Stoner, L.; Credeur, D.; Dolbow, D.R.; Gater, D.R. Vascular health toolbox for spinal cord injury: Recommendations for clinical practice. Atherosclerosis 2015, 243, 373–382. [Google Scholar] [CrossRef]
- Jan, Y.K.; Brienza, D.M.; Boninger, M.L.; Brenes, G. Comparison of skin perfusion response with alternating and constant pressures in people with spinal cord injury. Spinal Cord 2011, 49, 136–141. [Google Scholar] [CrossRef]
- Jan, Y.K. The effects of local cooling rates on perfusion of sacral skin under externally applied pressure in people with spinal cord injury: An exploratory study. Spinal Cord 2020, 58, 476–483. [Google Scholar] [CrossRef]
- Liao, F.; Burns, S.; Jan, Y.K. Skin blood flow dynamics and its role in pressure ulcers. J. Tissue Viability 2013, 22, 25–36. [Google Scholar] [CrossRef]
- Green, D.J.; O’Driscoll, G.; Joyner, M.J.; Cable, N.T. Exercise and cardiovascular risk reduction: Time to update the rationale for exercise? J. Appl. Physiol. 2008, 105, 766–768. [Google Scholar] [CrossRef]
- Phillips, A.A.; Cote, A.T.; Warburton, D.E. A systematic review of exercise as a therapeutic intervention to improve arterial function in persons living with spinal cord injury. Spinal Cord 2011, 49, 702–714. [Google Scholar] [CrossRef]
- Ginis, K.A.; Hicks, A.L.; Latimer, A.E.; Warburton, D.E.; Bourne, C.; Ditor, D.S.; Goodwin, D.L.; Hayes, K.C.; McCartney, N.; McIlraith, A.; et al. The development of evidence-informed physical activity guidelines for adults with spinal cord injury. Spinal Cord 2011, 49, 1088–1096. [Google Scholar] [CrossRef]
- Totosy de Zepetnek, J.O.; Pelletier, C.A.; Hicks, A.L.; MacDonald, M.J. Following the Physical Activity Guidelines for Adults with Spinal Cord Injury for 16 Weeks Does Not Improve Vascular Health: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2015, 96, 1566–1575. [Google Scholar] [CrossRef]
- Jansen, E.; de Groot, S. Vascular adaptations in nonstimulated areas during hybrid cycling or handcycling in people with a spinal cord injury: A pilot study of 10 cases. Spinal Cord Ser. Cases 2021, 7, 54. [Google Scholar] [CrossRef]
- Martins de Abreu, R.; Porta, A.; Rehder-Santos, P.; Cairo, B.; Donisete da Silva, C.; De Favari Signini, E.; Sakaguchi, C.A.; Catai, A.M. Effects of inspiratory muscle-training intensity on cardiovascular control in amateur cyclists. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2019, 317, R891–R902. [Google Scholar] [CrossRef]
- Introna, R.; Yodlowski, E.; Pruett, J.; Montano, N.; Porta, A.; Crumrine, R. Sympathovagal effects of spinal anesthesia assessed by heart rate variability analysis. Anesth. Analg. 1995, 80, 315–321. [Google Scholar]
- Vesterinen, V.; Nummela, A.; Heikura, I.; Laine, T.; Hynynen, E.; Botella, J.; Hakkinen, K. Individual Endurance Training Prescription with Heart Rate Variability. Med. Sci. Sports Exerc. 2016, 48, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Jan, Y.K.; Anderson, M.; Soltani, J.; Burns, S.; Foreman, R.D. Comparison of changes in heart rate variability and sacral skin perfusion in response to postural changes in people with spinal cord injury. J. Rehabil. Res. Dev. 2013, 50, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Jan, Y.K.; Liao, F.; Cheing, G.L.Y.; Pu, F.; Ren, W.; Choi, H.M.C. Differences in skin blood flow oscillations between the plantar and dorsal foot in people with diabetes mellitus and peripheral neuropathy. Microvasc. Res 2019, 122, 45–51. [Google Scholar] [CrossRef]
- Liao, F.; Garrison, D.W.; Jan, Y.K. Relationship between nonlinear properties of sacral skin blood flow oscillations and vasodilatory function in people at risk for pressure ulcers. Microvasc. Res. 2010, 80, 44–53. [Google Scholar] [CrossRef]
- Stefanovska, A. Coupled oscillators. Complex but not complicated cardiovascular and brain interactions. IEEE Eng. Med. Biol. Mag. 2007, 26, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Jan, Y.K.; Liao, F.; Rice, L.A.; Woods, J.A. Using reactive hyperemia to assess the efficacy of local cooling on reducing sacral skin ischemia under surface pressure in people with spinal cord injury: A preliminary report. Arch. Phys. Med. Rehabil. 2013, 94, 1982–1989. [Google Scholar] [CrossRef]
- Porta, A.; Bari, V.; De Maria, B.; Cairo, B.; Vaini, E.; Malacarne, M.; Pagani, M.; Lucini, D. On the Relevance of Computing a Local Version of Sample Entropy in Cardiovascular Control Analysis. IEEE Trans. Biomed. Eng. 2019, 66, 623–631. [Google Scholar] [CrossRef]
- Liao, F.; Jan, Y.K. Nonlinear dynamics of skin blood flow response to mechanical and thermal stresses in the plantar foot of diabetics with peripheral neuropathy. Clin. Hemorheol. Microcirc. 2017, 66, 197–210. [Google Scholar] [CrossRef]
- Liao, F.; Cheing, G.L.Y.; Ren, W.; Jain, S.; Jan, Y.K. Application of Multiscale Entropy in Assessing Plantar Skin Blood Flow Dynamics in Diabetics with Peripheral Neuropathy. Entropy 2018, 20, 127. [Google Scholar] [CrossRef]
- Liao, F.; Jan, Y.K. Using Modified Sample Entropy to Characterize Aging-Associated Microvascular Dysfunction. Front. Physiol. 2016, 7, 126. [Google Scholar] [CrossRef]
- Jan, Y.K.; Struck, B.D.; Foreman, R.D.; Robinson, C. Wavelet analysis of sacral skin blood flow oscillations to assess soft tissue viability in older adults. Microvasc. Res. 2009, 78, 162–168. [Google Scholar] [CrossRef]
- Liao, F.; Jan, Y.K. Using multifractal detrended fluctuation analysis to assess sacral skin blood flow oscillations in people with spinal cord injury. J. Rehabil. Res. Dev. 2011, 48, 787–800. [Google Scholar] [CrossRef]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef]
- Kaffashi, F.; Foglyano, R.; Wilson, C.G.; Loparo, K.A. The effect of time delay on approximate & sample entropy calculations. Phys. D Nonlinear Phenom. 2008, 23, 3069–3074. [Google Scholar]
- Hoyer, D.; Leder, U.; Hoyer, H.; Pompe, B.; Sommer, M.; Zwiener, U. Mutual information and phase dependencies: Measures of reduced nonlinear cardiorespiratory interactions after myocardial infarction. Med. Eng. Phys. 2002, 24, 33–43. [Google Scholar] [CrossRef]
- Liao, F.; Yang, T.D.; Wu, F.L.; Cao, C.; Mohamed, A.; Jan, Y.K. Using Multiscale Entropy to Assess the Efficacy of Local Cooling on Reactive Hyperemia in People with a Spinal Cord Injury. Entropy 2019, 21, 90. [Google Scholar] [CrossRef]
- Liao, F.; Zhang, K.; Zhou, L.; Chen, Y.; Jan, Y.K. Effect of Different Local Vibration Frequencies on the Multiscale Regularity of Plantar Skin Blood Flow. Entropy 2020, 22, 1288. [Google Scholar] [CrossRef]
- Schreiber, T.; Schmitz, A. Surrogate time series. Phys. D. Nonlinear Phenom. 2000, 142, 346–382. [Google Scholar] [CrossRef]
- Porta, A.; Baselli, G.; Guzzetti, S.; Pagani, M.; Malliani, A.; Cerutti, S. Prediction of short cardiovascular variability signals based on conditional distribution. IEEE Trans. Biomed. Eng. 2000, 47, 1555–1564. [Google Scholar] [PubMed]
- Zhaohua, W.U.; Huang, N.E. Ensemble empirical mode decomposition: A noise-assisted data analysis method. Adv. Adapt. Data Anal. 2011, 1, 1–41. [Google Scholar]
- Ticcinelli, V.; Stankovski, T.; Iatsenko, D.; Bernjak, A.; Bradbury, A.E.; Gallagher, A.R.; Clarkson, P.B.M.; McClintock, P.V.E.; Stefanovska, A. Coherence and Coupling Functions Reveal Microvascular Impairment in Treated Hypertension. Front. Physiol 2017, 8, 749. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | SSCI | ASCI | AB |
|---|---|---|---|
| Number of subjects | 9 | 12 | 16 |
| Gender (M/F) | 5/4 | 9/3 | 11/5 |
| Age (year) | 35.8 ± 11.0 | 35.1 ± 11.9 | 29.4 ± 6.2 |
| Body mass index (kg/m2) | 23.3 ± 2.5 | 25.8 ± 4.9 | 23.4 ± 2.9 |
| Duration of injury (year) | 9.7 ± 3.8 | 6.7 ± 5.9 | / |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, F.; Zhao, H.; Lin, C.-F.; Chen, P.; Chen, P.; Onyemere, K.; Jan, Y.-K. Application of Multiscale Sample Entropy in Assessing Effects of Exercise Training on Skin Blood Flow Oscillations in People with Spinal Cord Injury. Entropy 2023, 25, 690. https://doi.org/10.3390/e25040690
Liao F, Zhao H, Lin C-F, Chen P, Chen P, Onyemere K, Jan Y-K. Application of Multiscale Sample Entropy in Assessing Effects of Exercise Training on Skin Blood Flow Oscillations in People with Spinal Cord Injury. Entropy. 2023; 25(4):690. https://doi.org/10.3390/e25040690
Chicago/Turabian StyleLiao, Fuyuan, Hengyang Zhao, Cheng-Feng Lin, Panpan Chen, Philbert Chen, Kingsley Onyemere, and Yih-Kuen Jan. 2023. "Application of Multiscale Sample Entropy in Assessing Effects of Exercise Training on Skin Blood Flow Oscillations in People with Spinal Cord Injury" Entropy 25, no. 4: 690. https://doi.org/10.3390/e25040690