
Deep Compressive Sensing on ECG Signals with Modified Inception Block and LSTM

Abstract
:1. Introduction
- How to make the signals sparser? In the traditional CS methods, the signals should be originally sparse or become sparse after some transformation. However, not all of the signals are sparse in nature, so the key is to find a proper sparse presentation method. The popular methods mainly include wavelet transform [3], Fourier transform [4], short-time Fourier transform [5], Beamlet transform [6], Curvelet transform [7], Contourlet transform [8], Gabor dictionary [9], K-Singular Value Decomposition (K-SVD) algorithm [10], etc.;
- How to design a measuring matrix which is easy to realize on the hardware and can satisfy the Restricted Isometry Property (RIP) principle? The RIP principle can be expressed as follows:
- How to find a good solution to the non-convex optimization problem? Researchers always convert the non-convex optimization problem to the convex optimization problem by changing the objective function or discarding some of the constraints to solve this problem.
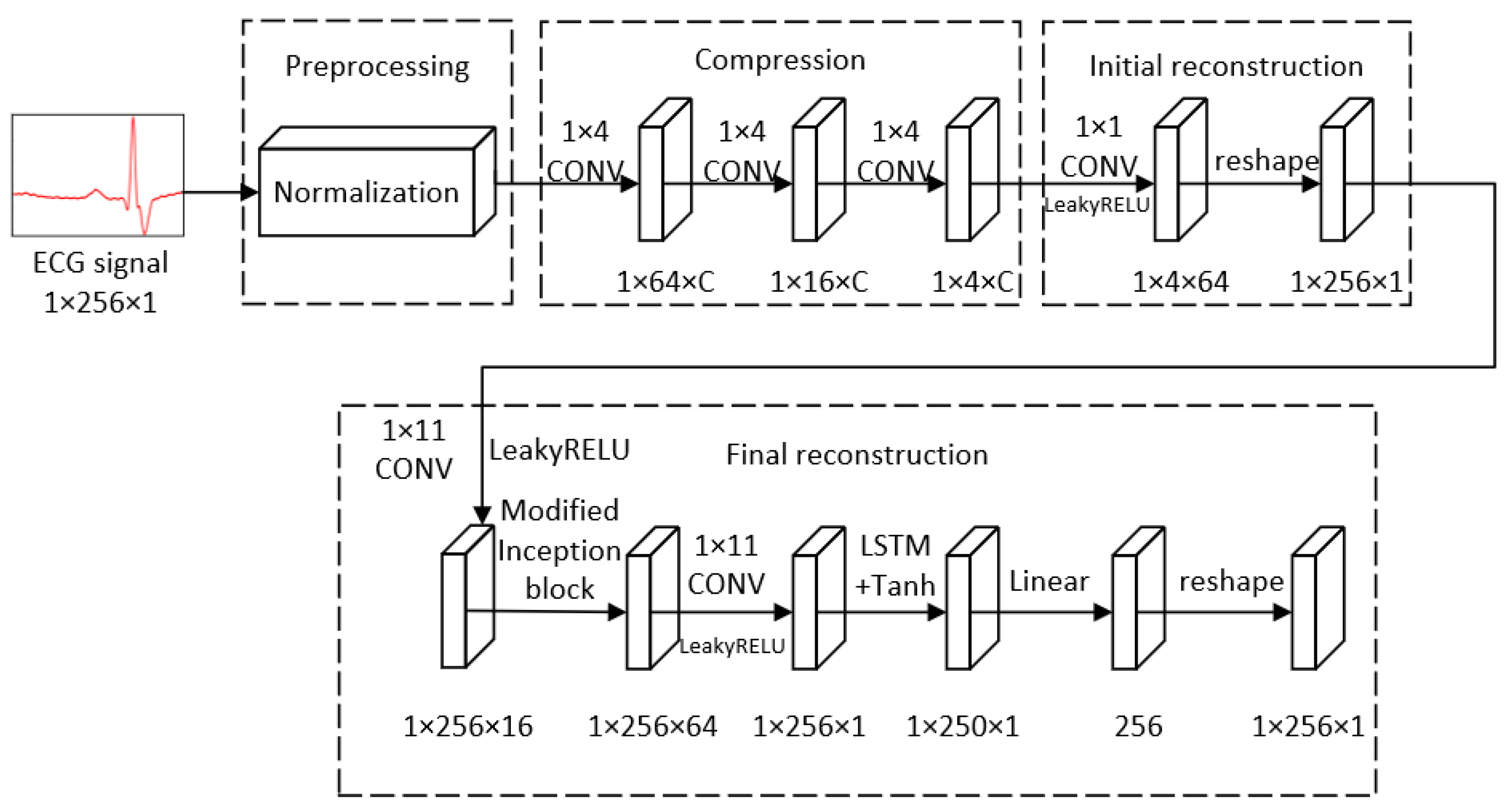
- We used three sequential convolutional layers to replace the traditional measuring matrixes to obtain the measurements adaptively, corresponding to the different dimension of original signals. In the convolutional layers, the number of the filters in each layer changed with the sensing rates in the experiment. We compared our compression method with two traditional fixed random matrixes;
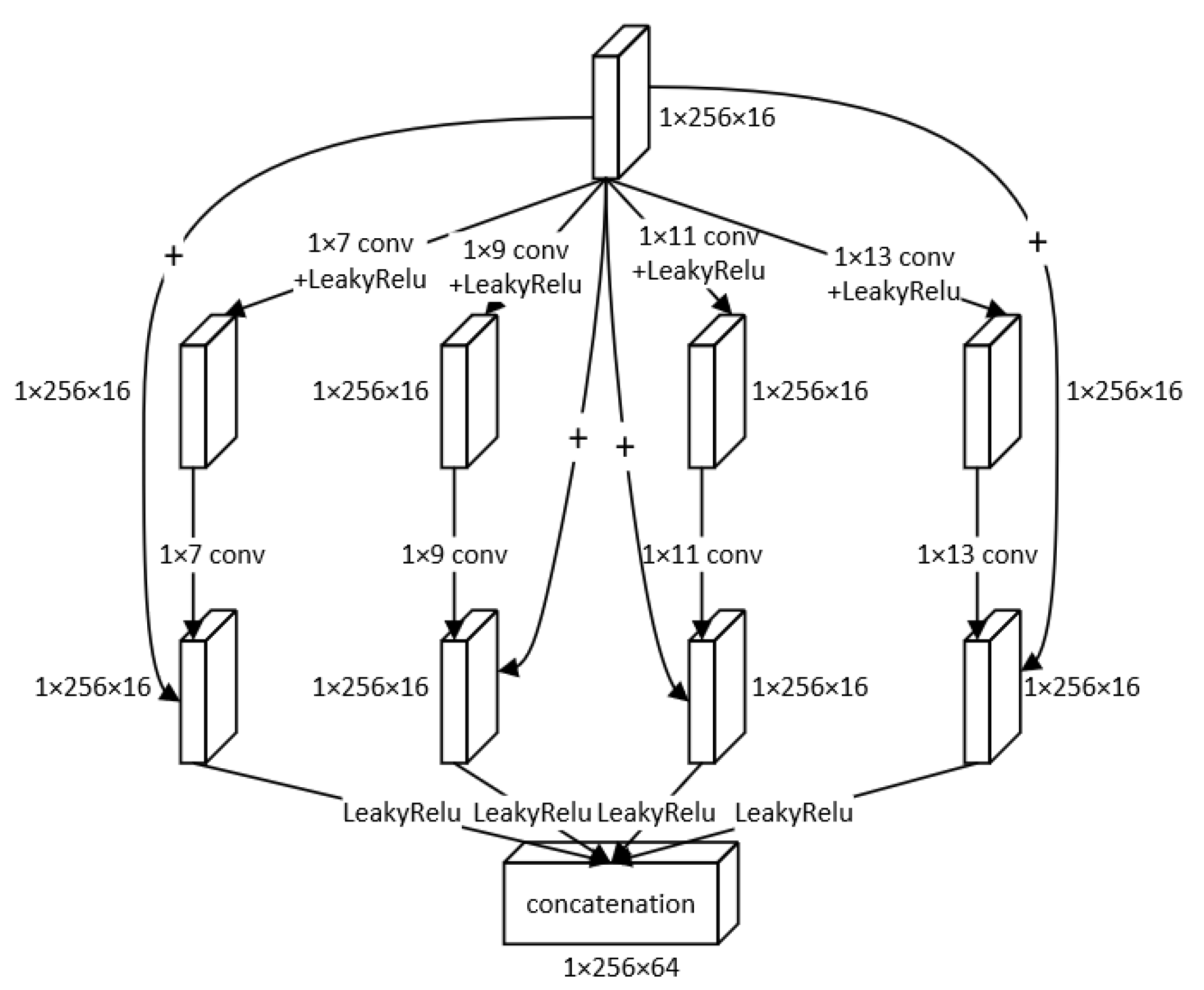
- We exploited a modified Inception block, in which we designed a structure containing a skip connection to use different kernel sizes to extract the features from the signals from different levels. We used the concatenation of those multi-level features to obtain more details of the data, to reconstruct the signals more accurately;
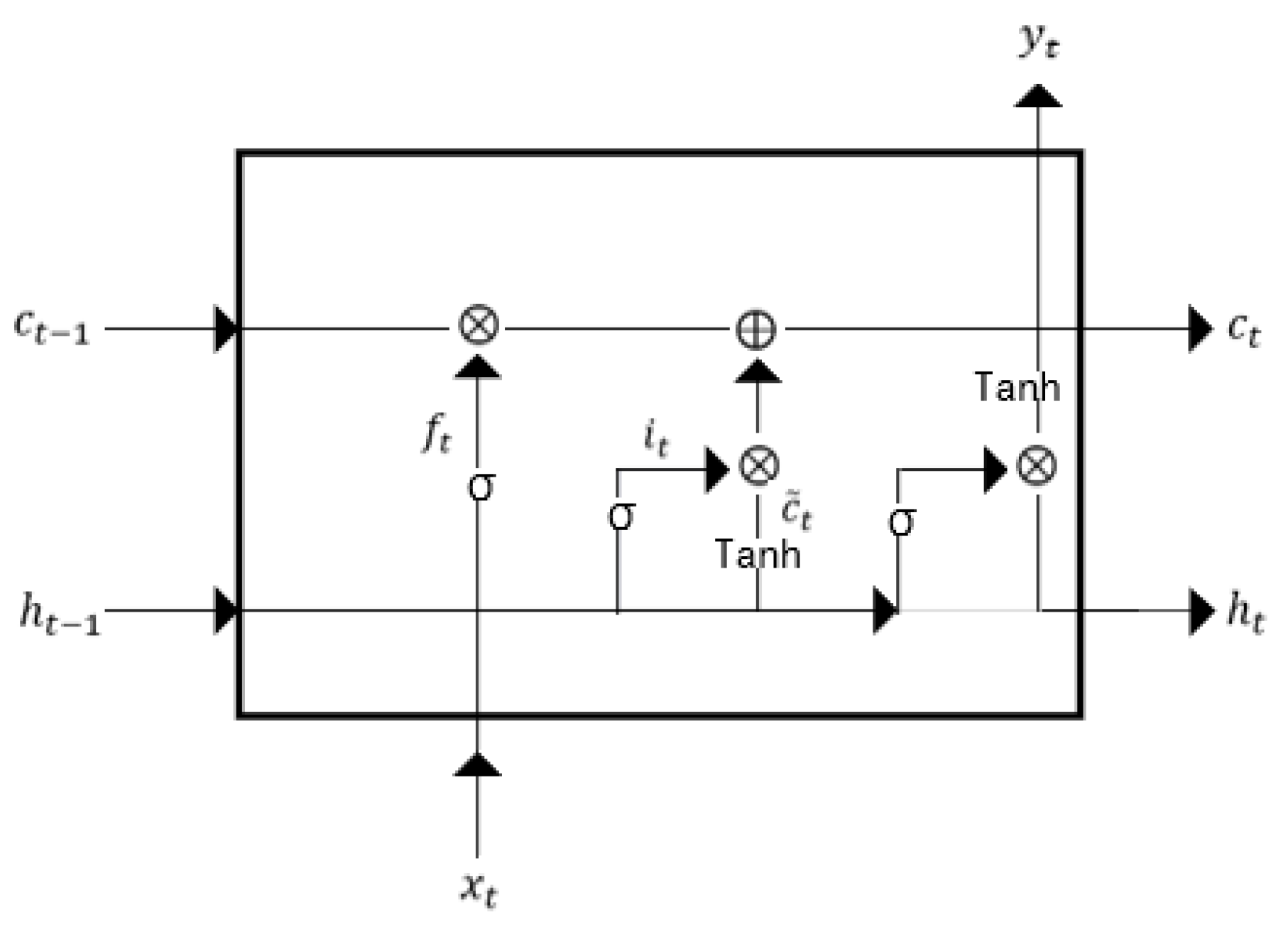
- ECG signals are time-series signals; thus, we adopted the long short-term memory (LSTM) to deal with the ECG signals. The LSTM is a variant of the Recurrent Neural Network (RNN), and it is appropriate to deal with long sequential signals avoiding the long dependency problems appearing in RNN and the vanishing gradient or exploding gradient in the meantime;
- We conducted our experiment on two different ECG databases to validate the robustness of our model. We evaluated our methods with other five methods, using the metrics Percentage Root-mean-square Difference (PRD) and Signal-to-Noise Ratio (SNR). From the experiment, we can see that our approach has good quality on both databases. Our methods have higher SNR and lower PRD than other methods, and the reconstructed signals have the best match with the original signals among all of the six methods.
2. Background
2.1. Compressed Sensing
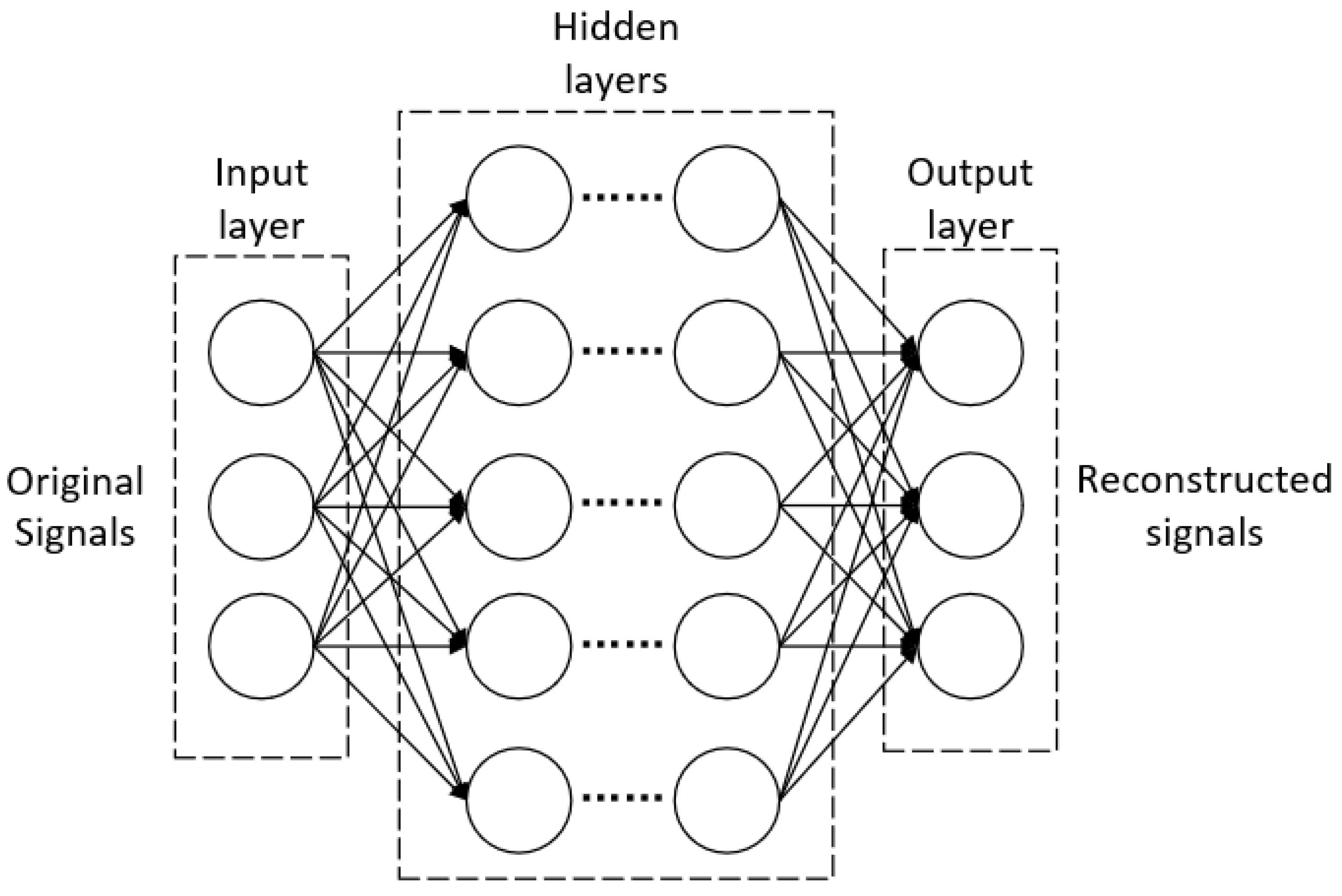
2.2. Deep Learning CS Methods
3. Materials and Methods
3.1. Preprocessing
3.2. Compression
3.3. Initial Reconstruction
3.4. Final Reconstruction
3.4.1. Overall Framework
3.4.2. Modified Inception Block
3.4.3. LSTM
4. Results
4.1. Experiment Setting
4.1.1. Dataset
4.1.2. Evaluation Metrics
4.1.3. Training Parameters
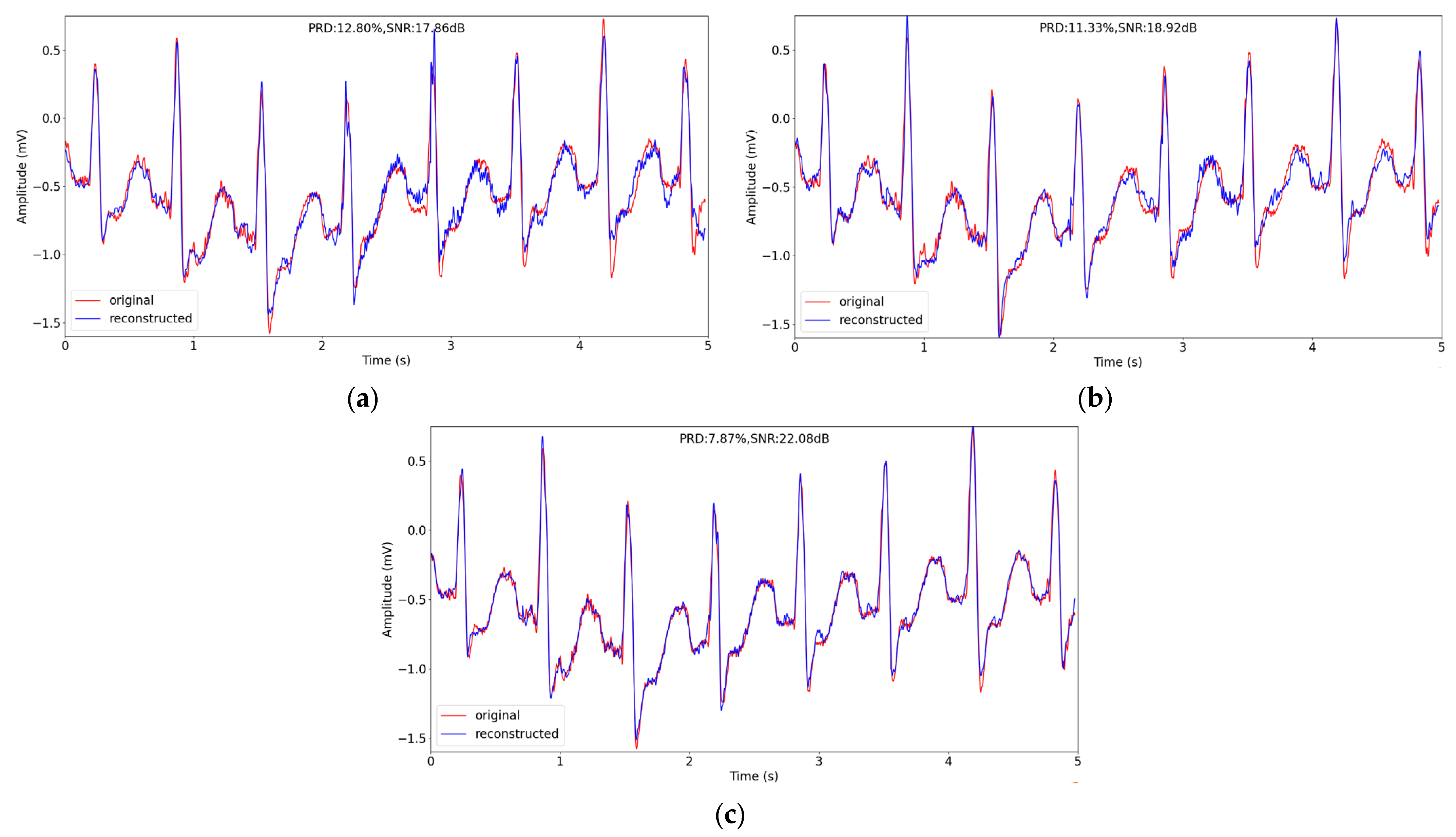
4.2. Comparison of Different Compression Methods
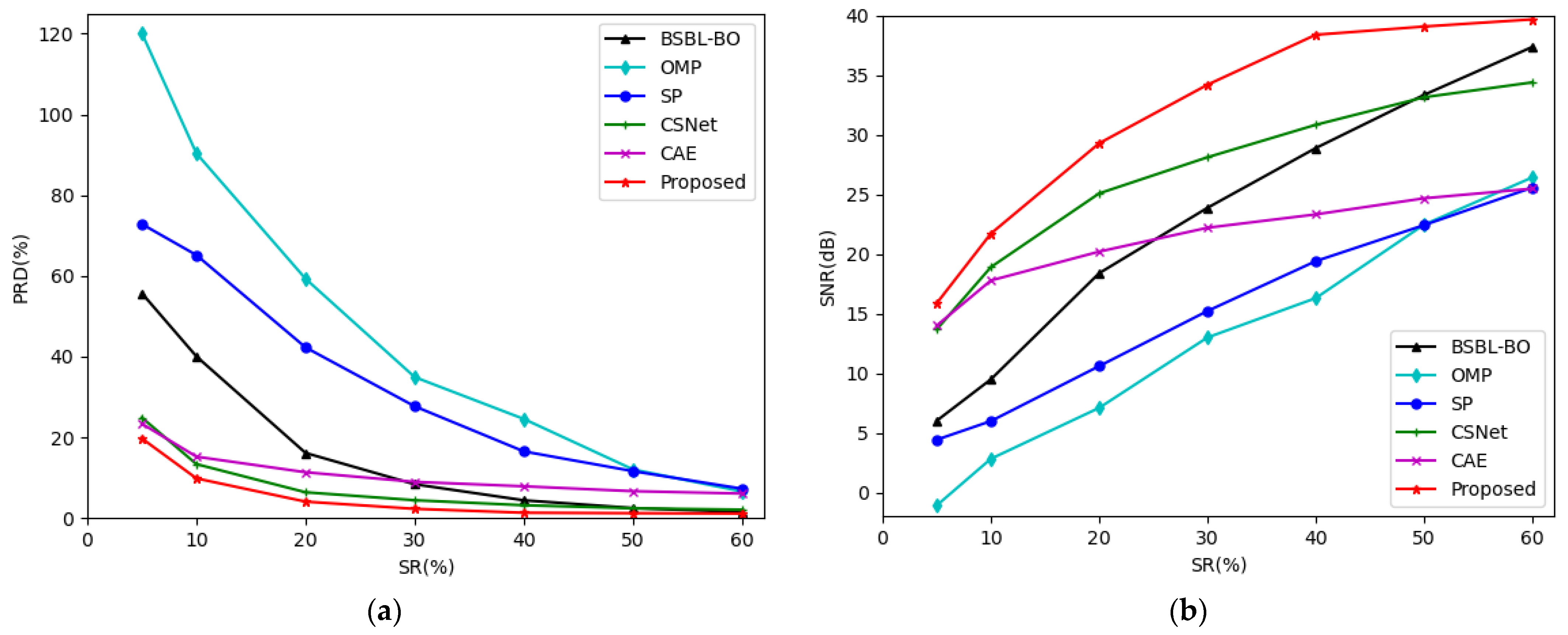
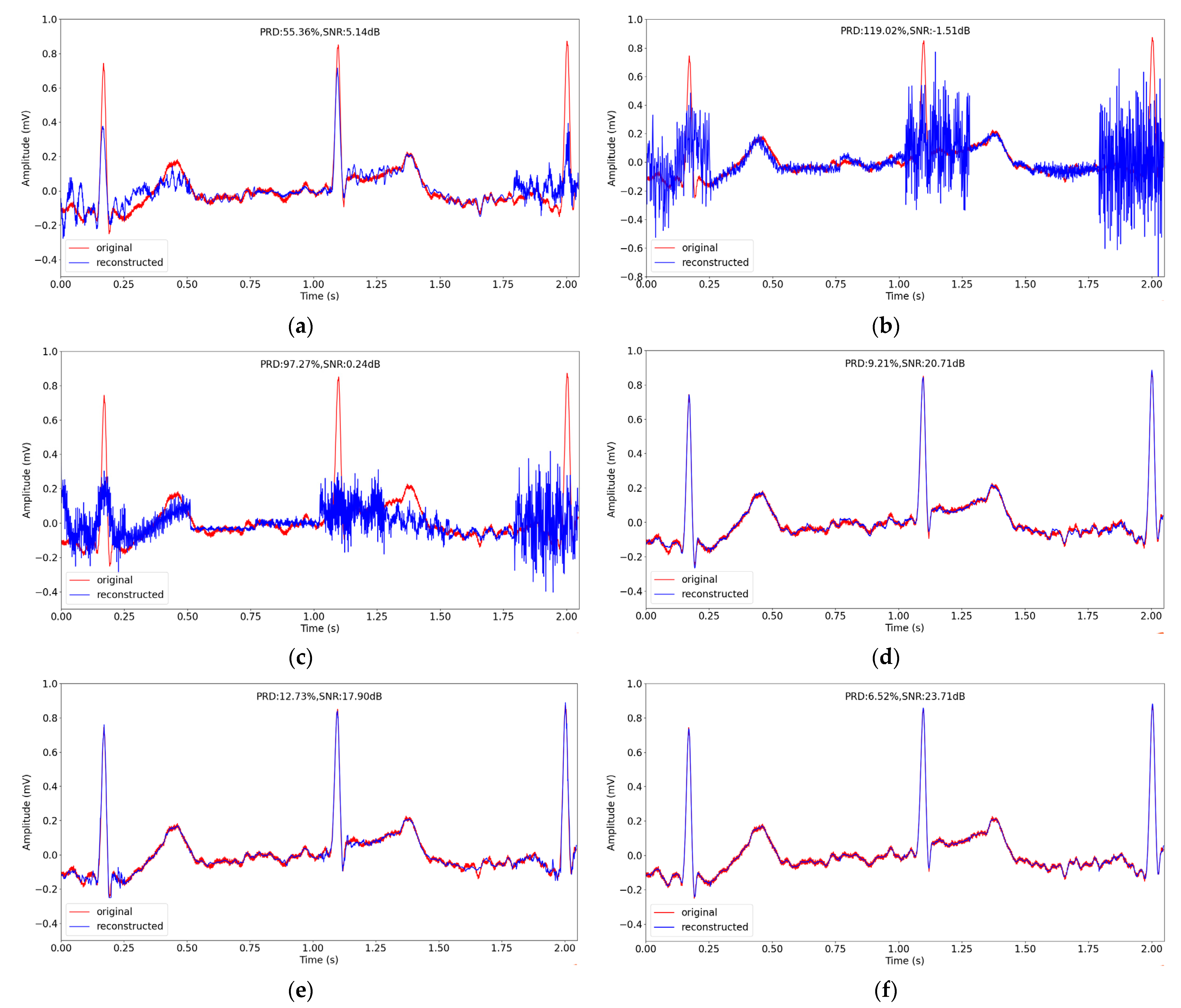
4.3. Comparison with Other CS Methods
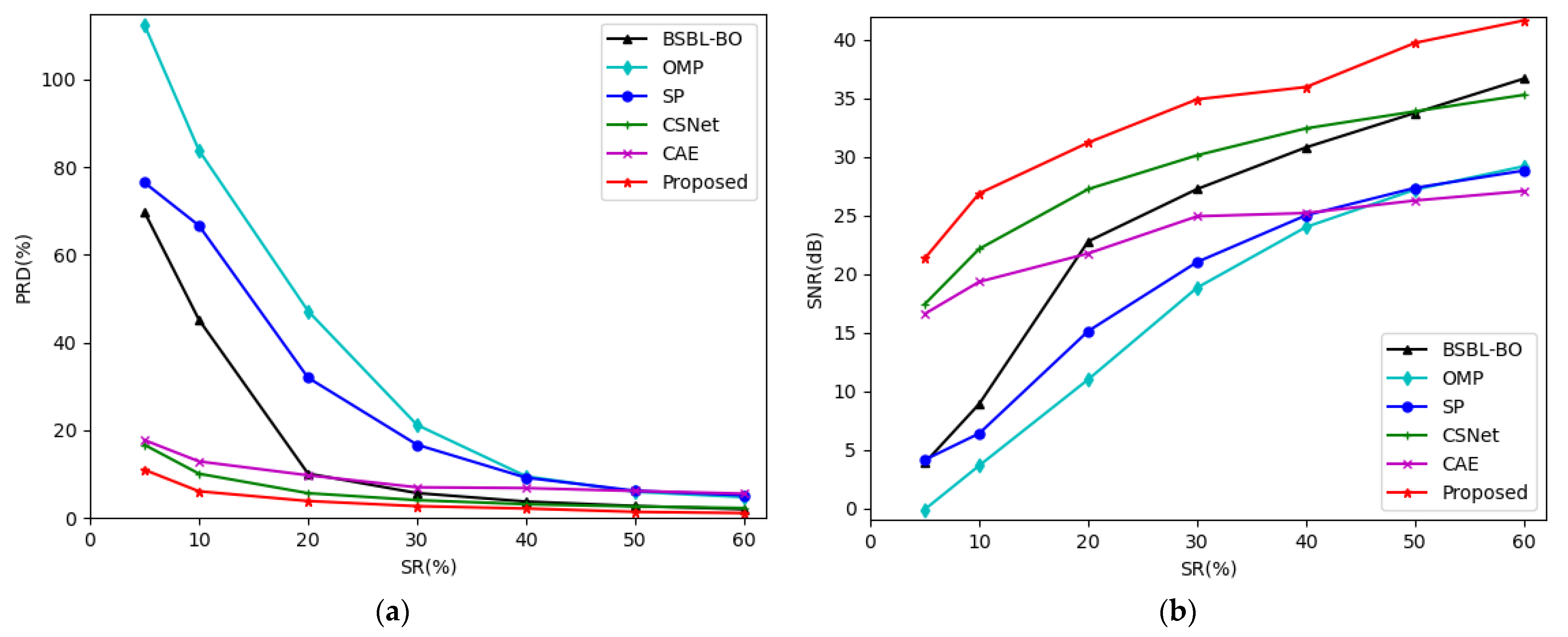
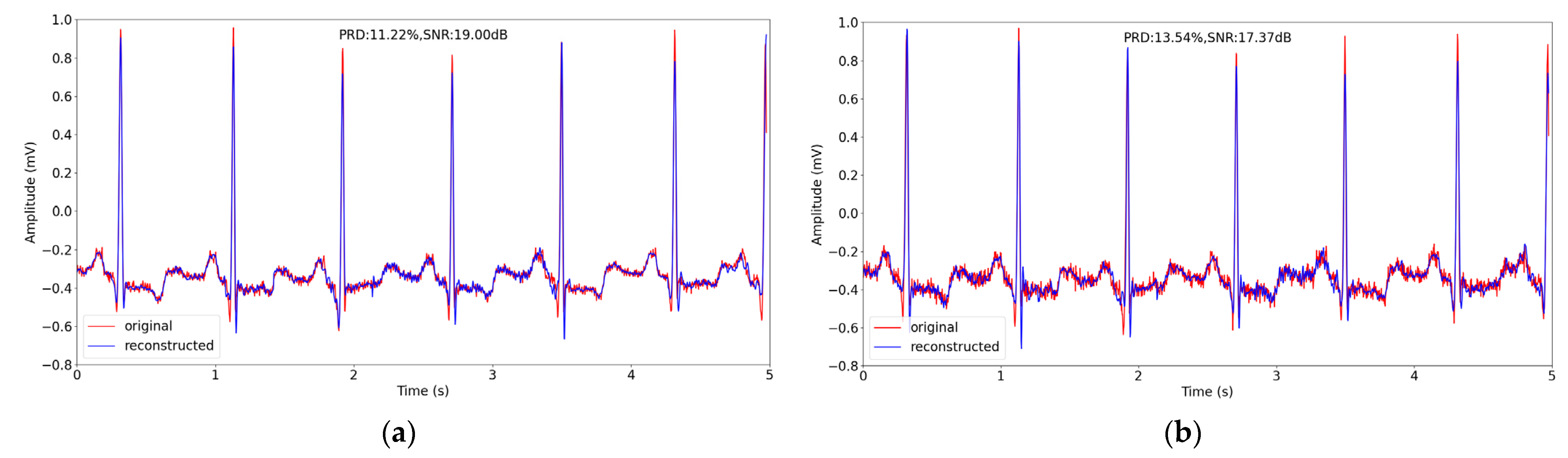
4.4. Experiment on Another Database
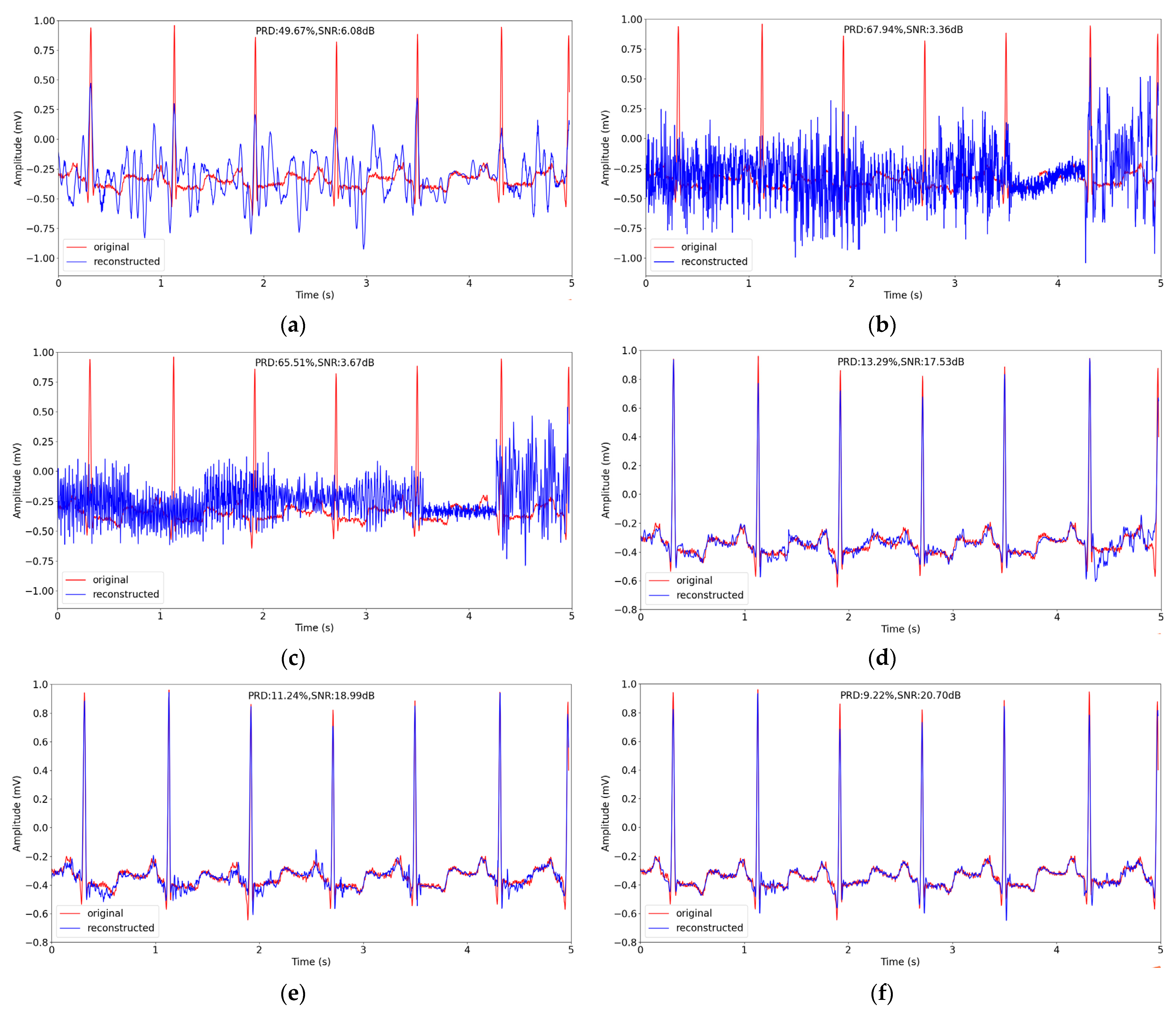
4.5. Performance on Noisy ECG Signals
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hua, J.; Zhang, H.; Liu, J.; Xu, Y.; Guo, F. Direct Arrhythmia Classification from Compressive ECG Signals in Wearable Health Monitoring System. J. Circuit. Syst. Comp. 2018, 27, 1850088. [Google Scholar] [CrossRef]
- Hua, J.; Tang, J.; Liu, J.; Yang, F.; Zhu, W. A Novel ECG Heartbeat Classification Approach Based on Compressive Sensing in Wearable Health Monitoring System. In Proceedings of the 2019 International Conference on Internet of Things (iThings) and IEEE Green Computing and Communications (GreenCom) and IEEE Cyber, Physical and Social Computing (CPSCom) and IEEE Smart Data (SmartData), Atlanta, GA, USA, 14–17 July 2019; pp. 581–586. [Google Scholar] [CrossRef]
- Mishra, A.; Thakkar, F.; Modi, C.; Kher, R. ECG Signal Compression Using Compressive Sensing and Wavelet Transform. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 3404–3407. [Google Scholar] [CrossRef]
- Gamper, U.; Boesiger, P.; Kozerke, S. Compressed Sensing in Dynamic MRI. Magn. Reson. Med. 2010, 59, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Eldar, Y.C.; Sidorenko, P.; Mixon, D.G.; Barel, S.; Cohen, O. Sparse Phase Retrieval from Short-Time Fourier Measurements. IEEE Signal. Proc. Lett. 2015, 22, 638–642. [Google Scholar] [CrossRef] [Green Version]
- Donoho, D.L.; Huo, X. Beamlet pyramids: A New Form of Multiresolution Analysis Suited for Extracting Lines, Curves, and Objects from Very Noisy Image Data. In Proceedings of the Spie the International Symposium on Optical Science and Technology, San Diego, CA, USA, 30 July 2000; pp. 434–444. [Google Scholar] [CrossRef]
- Starck, J.; Donoho, D.L.; Candès, E.J. The Curvelet Transform for Image Denoising. IEEE Trans. Image Process. 2002, 11, 670–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Do, M.N.; Vetterli, M. Contourlets: A New Directional Multiresolution Image Representation. In Proceedings of the Conference Record of the Thirty-Sixth Asilomar Conference on Signals, Systems and Computers, Pacific Grove, CA, USA, 3–6 November 2002; pp. 497–501. [Google Scholar] [CrossRef]
- Bergeaud, F.; Mallat, S.G. Matching Pursuit: Adaptive Representations of Images and Sounds. Comput. Appl. Math. 1996, 15, 97–110. [Google Scholar] [CrossRef]
- Aharon, M.; Elad, M.; Bruckstein, A. K-SVD: An Algorithm for Designing Overcomplete Dictionaries for Sparse Representation. IEEE Trans. Signal. Process. 2006, 54, 4311–4322. [Google Scholar] [CrossRef]
- Yang, C.; Pan, P.; Ding, Q. Image Encryption Scheme Based on Mixed Chaotic Bernoulli Measurement Matrix Block Compressive Sensing. Entropy 2022, 24, 273. [Google Scholar] [CrossRef] [PubMed]
- Dimakis, A.G.; Smarandache, R.; Vontobel, P.O. LDPC Codes for Compressed Sensing. IEEE Trans. Inf. Theory 2010, 58, 3093–3114. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Barbot, J.P.; Zheng, G.; Sun, H. Compressive Sensing with Chaotic Sequence. IEEE Signal. Proc. Lett. 2010, 17, 731–734. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Jung, T.; Makeig, S.; Rao, B.D. Compressed Sensing for Energy-Efficient Wireless Telemonitoring of Noninvasive Fetal ECG Via Block Sparse Bayesian Learning. IEEE Trans. Biomed. Eng. 2013, 60, 300–309. [Google Scholar] [CrossRef] [Green Version]
- Izadi, V.; Shahri, P.K.; Ahani, H. A Compressed-sensing-based Compressor for ECG. Biomed. Eng. Lett. 2020, 10, 299–307. [Google Scholar] [CrossRef]
- Abhishek, S.; Veni, S.; Narayanankutty, K.A. Biorthogonal Wavelet Filters for Compressed Sensing ECG Reconstruction. Biomed. Signal. Process. Control. 2019, 47, 183–195. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, X.; Wei, S.; Gan, H.; Liu, F.; Li, Y.; Liu, C.; Liu, F. Electrocardiogram Reconstruction Based on Compressed Sensing. IEEE Access 2019, 7, 37228–37237. [Google Scholar] [CrossRef]
- Melek, M.; Khattab, A. ECG Compression Using Wavelet-based Compressed Sensing with Prior Support Information. Biomed. Signal. Process. Control. 2021, 68, 102786. [Google Scholar] [CrossRef]
- Jahanshahi, J.A.; Danyali, H.; Helfroush, M.S. Compressive Sensing Based the Multi-channel ECG Reconstruction in Wireless Body Sensor Networks. Biomed. Signal. Process. Control. 2020, 61, 102047. [Google Scholar] [CrossRef]
- Šaliga, J.; Andráš, I.; Dolinský, P.; Michaeli, L.; Kováč, O.; Kromka, J. ECG Compressed Sensing Method with High Compression Ratio and Dynamic Model Reconstruction. Measurement 2021, 183, 109803. [Google Scholar] [CrossRef]
- Rezaii, T.Y.; Beheshti, S.; Shamsi, M.; Eftekharifar, S. ECG Signal Compression and Denoising via Optimum Sparsity Order Selection in Compressed Sensing Framework. Biomed. Signal. Process. Control. 2018, 41, 161–171. [Google Scholar] [CrossRef]
- Hua, J.; Zhang, H.; Liu, J.; Zhou, J. Compressive Sensing of Multichannel Electrocardiogram Signals in Wireless Telehealth System. J. Circuits Syst. Comp. 2016, 25, 1650103. [Google Scholar] [CrossRef]
- Muduli, P.R.; Gunukula, R.R.; Mukherjee, A. A Deep Learning Approach to Fetal-ECG Signal Reconstruction. In Proceedings of the 2016 Twenty Second National Conference on Communication (NCC), Guwahati, India, 4–6 March 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Polanía, L.F.; Plaza, R.I. Compressed Sensing ECG Using Restricted Boltzmann Machines. Biomed. Signal. Process. Control. 2018, 45, 237–245. [Google Scholar] [CrossRef] [Green Version]
- Mangia, M.; Prono, L.; Marchioni, A.; Pareschi, F.; Rovatti, R.; Setti, G. Deep Neural Oracles for Short-Window Optimized Compressed Sensing of Biosignals. IEEE Trans. Biomed. Circuits Syst. 2020, 14, 545–557. [Google Scholar] [CrossRef]
- Shrivastwa, R.R.; Pudi, V.; Duo, C.; So, R.; Chattopadhyay, A.; Cuntai, G. A Brain–Computer Interface Framework Based on Compressive Sensing and Deep Learning. IEEE Consum. Electr. Mag. 2020, 9, 90–96. [Google Scholar] [CrossRef]
- Mangi, M.; Marchioni, A.; Prono, L.; Pareschi, F.; Rovatti, R.; Setti, G. Low-power ECG Acquisition by Compressed Sensing with Deep Neural Oracles. In Proceedings of the 2020 2nd IEEE International Conference on Artificial Intelligence Circuits and Systems (AICAS), Genova, Italy, 31 August–2 September 2020; pp. 158–162. [Google Scholar] [CrossRef]
- Shrivastwa, R.R.; Pudi, V.; Chattopadhyay, A. An FPGA-Based Brain Computer Interfacing Using Compressive Sensing and Machine Learning. In Proceedings of the 2018 IEEE Computer Society Annual Symposium on VLSI (ISVLSI), Hong Kong, China, 8–11 July 2018; pp. 726–731. [Google Scholar] [CrossRef]
- Zheng, R.; Zhang, Y.; Huang, D.; Chen, Q. Sequential Convolution and Runge-Kutta Residual Architecture for Image Compressed Sensing. In Computer Vision-ECCV 2020; Lecture Notes in Computer Science; Vedaldi, A., Bischof, H., Brox, T., Frahm, J.M., Eds.; Springer: Cham, Switzerland, 2020; Volume 12354, pp. 232–248. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going Deeper with Convolutions. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef] [Green Version]
- Hochreiter, S.; Schmidhuber, J. Long Short-Term Memory. Neural. Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef] [PubMed]
- Moody, G.B.; Mark, R.G. The Impact of the MIT-BIH Arrhythmia Database. IEEE Eng. Med. Biol. Mag. 2001, 20, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Dias, F.M.; Khosravy, M.; Cabral, T.W.; Monteiro, H.L.M.; Filho, L.M.A.; Honório, L.M.; Naji, R.; Duque, C.A. Chapter 9—Compressive Sensing of Electrocardiogram. In Advances in Ubiquitous Sensing Applications for Healthcare, Compressive Sensing in Healthcare; Khosravy, M., Dey, N., Duque, C.A., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 165–184. [Google Scholar] [CrossRef]
- Xie, X.; Wang, Y.; Shi, G.; Wang, C.; Du, J.; Han, X. Adaptive Measurement Network for CS Image Reconstruction. In Computer Vision. CCCV 2017. Communications in Computer and Information Science; Yang, J., Hu, Q., Cheng, M., Wang, L., Liu, Q., Bai, X., Meng, D., Eds.; Springer: Singapore, 2017; Volume 772, pp. 407–417. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Rao, B.D. Extension of SBL Algorithms for the Recovery of Block Sparse Signals with Intra-Block Correlation. IEEE Trans. Signal. Process. 2013, 61, 2009–2015. [Google Scholar] [CrossRef] [Green Version]
- Tropp, J.A.; Gilbert, A.C. Signal Recovery from Random Measurements via Orthogonal Matching Pursuit. IEEE Trans. Inf. Theory 2007, 53, 4655–4666. [Google Scholar] [CrossRef] [Green Version]
- Dai, W.; Milenkovic, O. Subspace Pursuit for Compressive Sensing Signal Reconstruction. IEEE Trans. Inf. Theory 2009, 55, 2230–2249. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Dong, Z.; Wang, Z.; Guo, L.; Wang, Z. CSNet: A Deep Learning Approach for ECG Compressed Sensing. Biomed. Signal. Process. Control. 2021, 70, 103065. [Google Scholar] [CrossRef]
- Al-Marridi, A.Z.; Mohamed, A.; Erbad, A. Convolutional Autoencoder Approach for EEG Compression and Reconstruction in m-Health Systems. In Proceedings of the 2018 14th International Wireless Communications & Mobile Computing Conference (IWCMC), Limassol, Cyprus, 25–29 June 2018; pp. 370–375. [Google Scholar] [CrossRef]
- Behar, J.A.; Bonnemains, L.; Shulgin, V.; Oster, J.; Ostras, O.; Lakhno, I. Noninvasive Fetal Electrocardiography for the Detection of Fetal Arrhythmias. Prenatal. Diag. 2019, 39, 178–187. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PRD(%) | Signals Reconstruction Quality |
|---|---|
| 0–2 | Very good |
| 2–9 | Good |
| 9–19 | No good |
| 19–60 | Bad |
| SR | Gaussian | Bernoulli | Proposed | |||
|---|---|---|---|---|---|---|
| PRD | SNR | PRD | SNR | PRD | SNR | |
| 0.05 | 26.85% | 13.08 dB | 24.85% | 13.85 dB | 19.72% | 15.86 dB |
| 0.1 | 12.27% | 19.62 dB | 12.19% | 19.61 dB | 9.83% | 21.70 dB |
| 0.2 | 6.18% | 25.35 dB | 6.55% | 24.86 dB | 4.07% | 29.27 dB |
| 0.3 | 4.25% | 28.53 dB | 4.66% | 27.73 dB | 2.29% | 34.18 dB |
| 0.4 | 3.29% | 30.67 dB | 3.29% | 30.90 dB | 1.32% | 38.37 dB |
| 0.5 | 2.71% | 32.34 dB | 2.72% | 32.30 dB | 1.21% | 39.66 dB |
| 0.6 | 2.44% | 33.23 dB | 2.44% | 33.97 dB | 1.12% | 39.06 dB |
| SR | BSBL-BO | OMP | SP | CSNet | CAE | Proposed | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PRD | SNR | PRD | SNR | PRD | SNR | PRD | SNR | PRD | SNR | PRD | SNR | |
| 0.05 | 55.69% | 6.01 dB | 120.10% | −1.09 dB | 72.82% | 4.42 dB | 24.89% | 13.67 dB | 23.38% | 13.99 dB | 19.72% | 15.86 dB |
| 0.1 | 40.04% | 9.48 dB | 90.33% | 2.82 dB | 65.14% | 5.98 dB | 13.36% | 18.89 dB | 15.21% | 17.77 dB | 9.83% | 21.70 dB |
| 0.2 | 16.13% | 18.38 dB | 59.27% | 7.09 dB | 42.27% | 10.59 dB | 6.39% | 25.07 dB | 11.35% | 20.19 dB | 4.07% | 29.27 dB |
| 0.3 | 8.37% | 23.86 dB | 34.91% | 12.99 dB | 27.68% | 15.21 dB | 4.42% | 28.10 dB | 8.97% | 22.19 dB | 2.29% | 34.18 dB |
| 0.4 | 4.40% | 28.87 dB | 24.54% | 16.29 dB | 16.51% | 19.39 dB | 3.18% | 30.82 dB | 7.87% | 23.31 dB | 1.32% | 38.37 dB |
| 0.5 | 2.48% | 33.33 dB | 12.05% | 22.45 dB | 11.62% | 22.41 dB | 2.42% | 33.13 dB | 6.66% | 24.66 dB | 1.21% | 39.06 dB |
| 0.6 | 1.49% | 37.35 dB | 6.57% | 26.41 dB | 7.26% | 25.56 dB | 2.08% | 34.38 dB | 6.08% | 25.47 dB | 1.12% | 39.66 dB |
| SR | BSBL-BO | OMP | SP | CSNet | CAE | Proposed | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PRD | SNR | PRD | SNR | PRD | SNR | PRD | SNR | PRD | SNR | PRD | SNR | |
| 0.05 | 69.74% | 3.86 dB | 112.40% | -0.11 dB | 76.46% | 4.13 dB | 16.68% | 17.42 dB | 17.76% | 16.59 dB | 10.99% | 21.32 dB |
| 0.1 | 45.19% | 8.90 dB | 83.80% | 3.64 dB | 66.66% | 6.38 dB | 10.10% | 22.14 dB | 12.90% | 19.33 dB | 6.09% | 26.87 dB |
| 0.2 | 10.13% | 22.78 dB | 47.20% | 10.99 dB | 31.99% | 15.12 dB | 5.66% | 27.24 dB | 9.74% | 21.75 dB | 3.87% | 31.21 dB |
| 0.3 | 5.68% | 27.25 dB | 21.22% | 18.83 dB | 16.70% | 21.02 dB | 4.07% | 30.13 dB | 7.00% | 24.92 dB | 2.70% | 34.91 dB |
| 0.4 | 3.75% | 30.81 dB | 9.51% | 24.01 dB | 9.19% | 25.01 dB | 3.14% | 32.43 dB | 6.82% | 25.20 dB | 2.16% | 35.96 dB |
| 0.5 | 2.74% | 33.75 dB | 5.97% | 27.20 dB | 6.22% | 27.35 dB | 2.63% | 33.88 dB | 6.16% | 26.27 dB | 1.40% | 39.73 dB |
| 0.6 | 2.01% | 36.68 dB | 4.74% | 29.20 dB | 5.17% | 28.83 dB | 2.27% | 35.29 dB | 5.56% | 27.08 dB | 1.12% | 41.65 dB |
| SR | Noisy Data (32 dB) | Noisy Data (24 dB) | ||
|---|---|---|---|---|
| PRD | SNR | PRD | SNR | |
| 0.05 | 19.76% | 15.49 dB | 22.71% | 13.81 dB |
| 0.1 | 11.11% | 20.22 dB | 12.73% | 18.47 dB |
| 0.2 | 5.19% | 26.29 dB | 7.78% | 22.36 dB |
| 0.3 | 3.18% | 30.28 dB | 5.99% | 24.52 dB |
| 0.4 | 2.45% | 32.35 dB | 5.25% | 25.63 dB |
| 0.5 | 2.30% | 32.85 dB | 5.11% | 25.86 dB |
| 0.6 | 2.17% | 33.36 dB | 4.79% | 26.42 dB |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hua, J.; Rao, J.; Peng, Y.; Liu, J.; Tang, J. Deep Compressive Sensing on ECG Signals with Modified Inception Block and LSTM. Entropy 2022, 24, 1024. https://doi.org/10.3390/e24081024
Hua J, Rao J, Peng Y, Liu J, Tang J. Deep Compressive Sensing on ECG Signals with Modified Inception Block and LSTM. Entropy. 2022; 24(8):1024. https://doi.org/10.3390/e24081024
Chicago/Turabian StyleHua, Jing, Jue Rao, Yingqiong Peng, Jizhong Liu, and Jianjun Tang. 2022. "Deep Compressive Sensing on ECG Signals with Modified Inception Block and LSTM" Entropy 24, no. 8: 1024. https://doi.org/10.3390/e24081024