Suppressing the Influence of Ectopic Beats by Applying a Physical Threshold-Based Sample Entropy



Abstract
:1. Introduction
2. Methods
2.1. Data
2.2. Physical Threshold-Based SampEn
3. Results
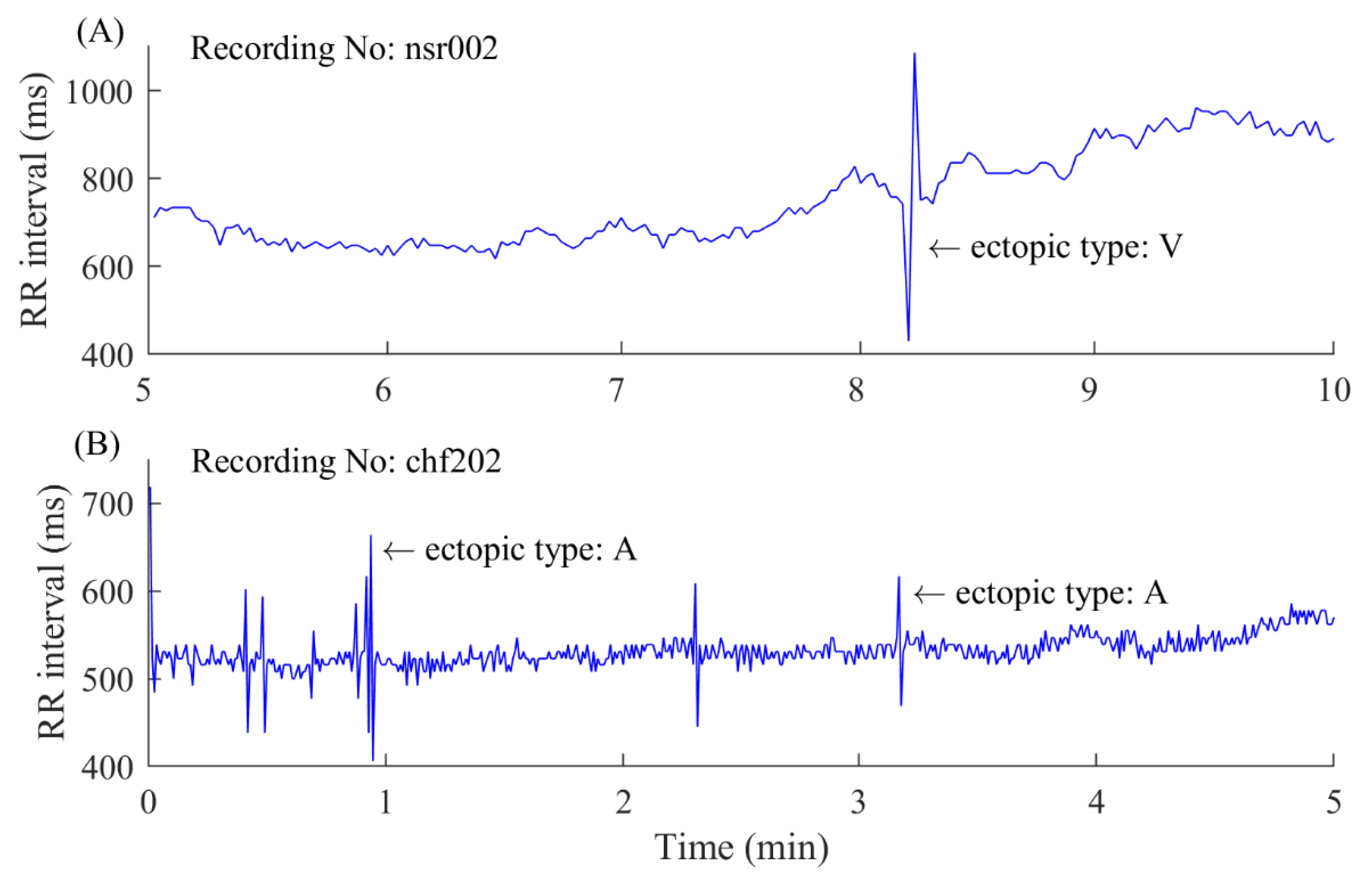
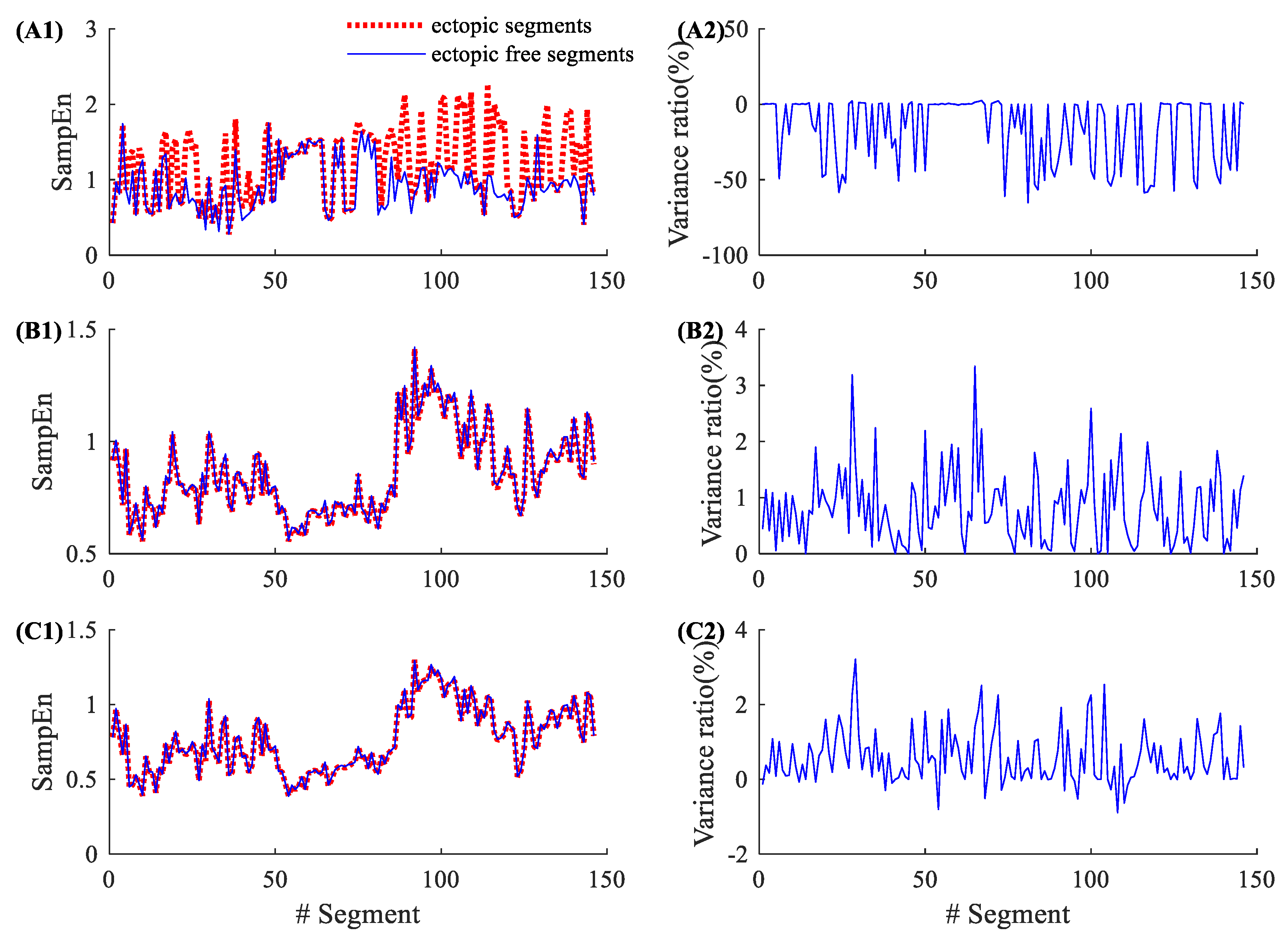
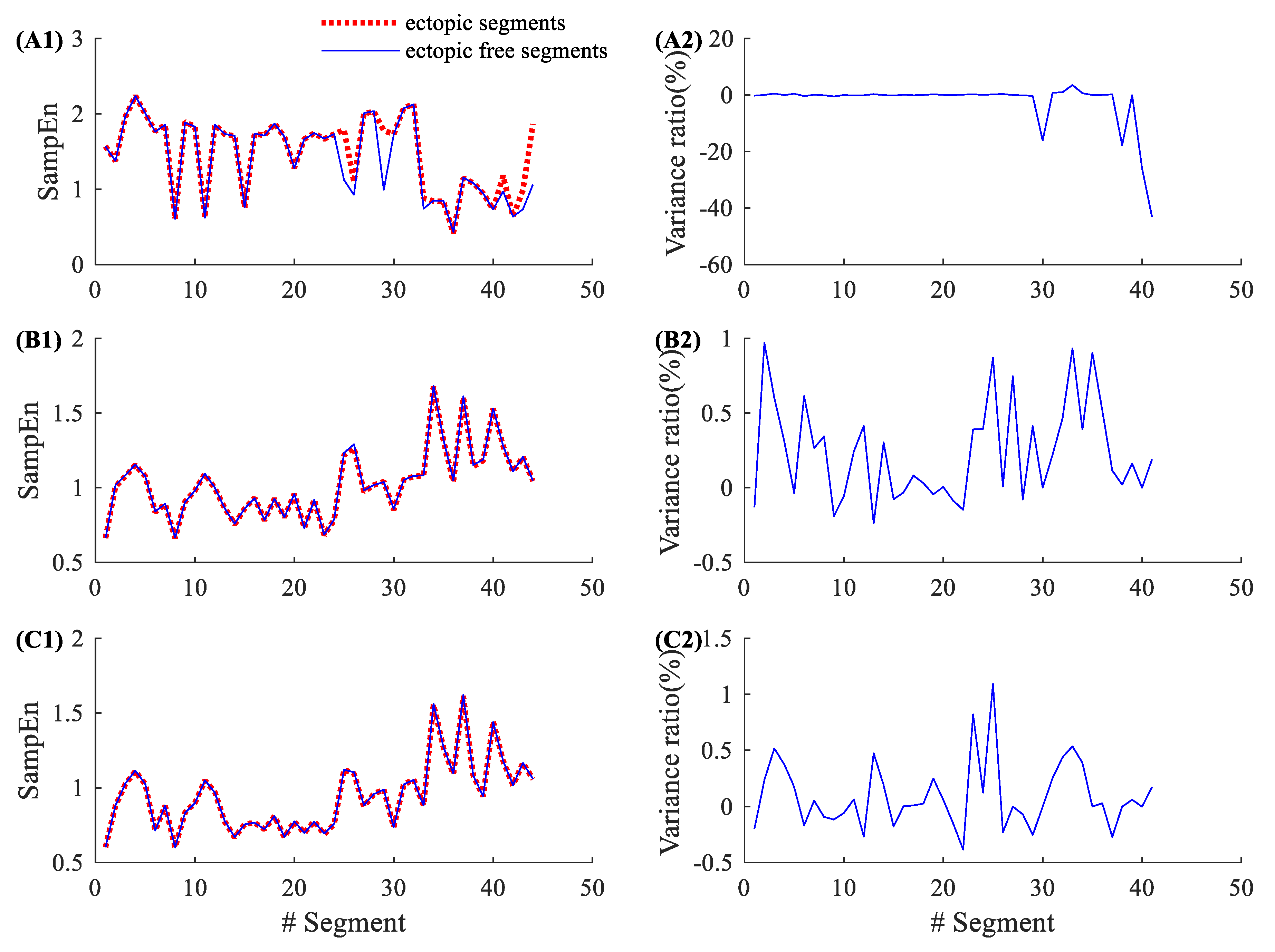
3.1. Demonstration of the Influence of Ectopic Beats on Entropy Values
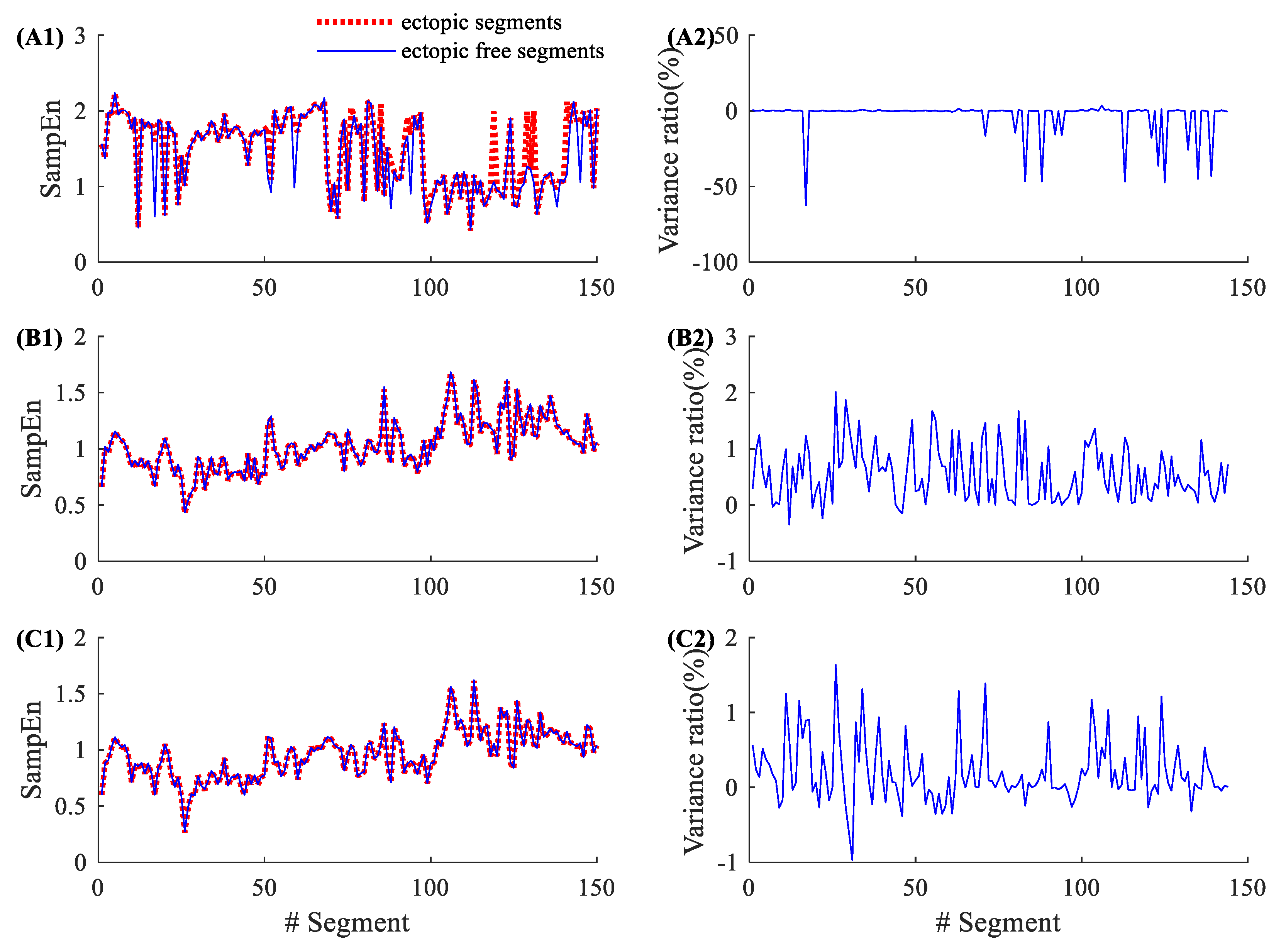
3.2. Demonstration of the Influence of Atrial Beats on Entropy Values
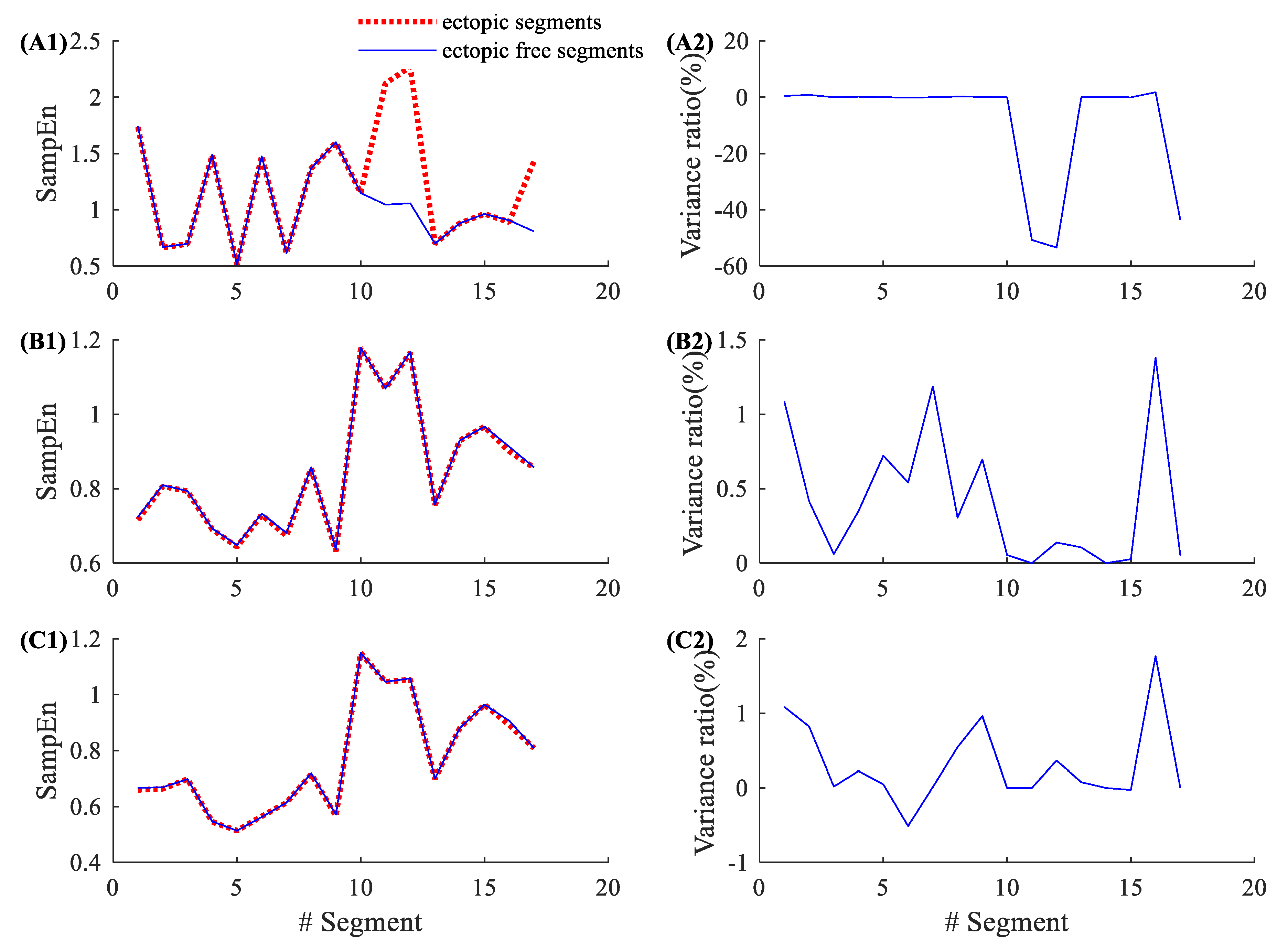
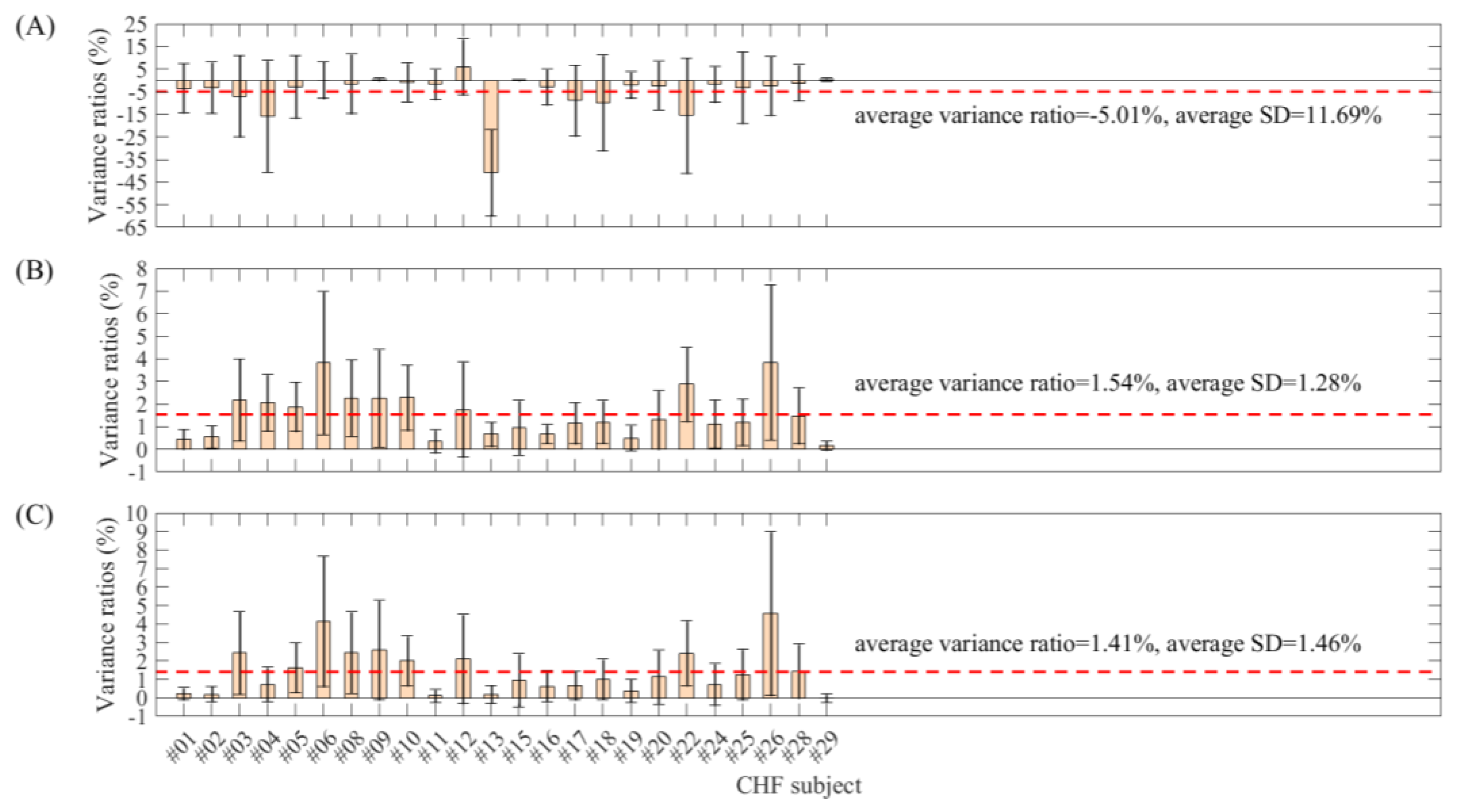
3.3. Demonstration of the Influence of Ventricular Beats on Entropy Values
3.4. Total Results
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shannon, C.E. A mathematical theory of communication. Bell Syst. Tech. J. 1948, 27, 379–423. [Google Scholar] [CrossRef] [Green Version]
- Pincus, S.M. Approximate entropy as a measure of system complexity. Proc. Natl. Acad. Sci. USA 1991, 88, 2297–2301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. -Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, L.N.; Wei, S.S.; Zhang, C.Q.; Zhang, Y.T.; Jiang, X.E.; Liu, F.; Liu, C.Y. Determination of sample entropy and fuzzy measure entropy parameters for distinguishing congestive heart failure from normal sinus rhythm subjects. Entropy 2015, 17, 6270–6288. [Google Scholar] [CrossRef] [Green Version]
- Mayer, C.C.; Bachler, M.; Hörtenhuber, M.; Stocker, C.; Holzinger, A.; Wassertheurer, S. Selection of entropy-measure parameters for knowledge discovery in heart rate variability data. BMC Bioinform. 2014, 15, S2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lake, D.E.; Richman, J.S.; Griffin, M.P.; Moorman, J.R. Sample entropy analysis of neonatal heart rate variability. Am. J. Physiol. -Regul. Integr. Comp. Physiol. 2002, 283, R789–R797. [Google Scholar] [CrossRef] [Green Version]
- Pincus, S.M.; Keefe, D.L. Quantification of hormone pulsatility via an approximate entropy algorithm. Am. J. Physiol. 1992, 262, 741–754. [Google Scholar] [CrossRef]
- Lu, S.; Chen, X.; Kanters, J.K.; Solomon, I.C.; Chon, K.H. Automatic selection of the threshold value r for approximate entropy. IEEE Trans. Biomed. Eng. 2008, 55, 1966–1972. [Google Scholar]
- Castiglioni, P.; Di Rienzo, M. How the threshold ‘r’ influences approximate entropy analysis of heart-rate variability. In Proceedings of the 2008 Computers in Cardiology, Bologna, Italy, 14–17 September 2008; pp. 561–564. [Google Scholar]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of biological signals. Phys. Rev. E Stat. Nonlin. Soft Matter Phys. 2005, 71, 021906. [Google Scholar] [CrossRef] [Green Version]
- Costa, M.D.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett. 2002, 89, 068102. [Google Scholar] [CrossRef] [Green Version]
- Castiglioni, P.; Coruzzi, P.; Bini, M.; Parati, G.; Faini, A. Multiscale sample entropy of cardiovascular signals: Does the choice between fixed- or varying-tolerance among scales influence its evaluation and interpretation? Entropy 2017, 19, 590. [Google Scholar] [CrossRef] [Green Version]
- Gow, B.J.; Peng, C.K.; Wayne, P.M.; Ahn, A.C. Multiscale entropy analysis of center-of-pressure dynamics in human postural control: Methodological considerations. Entropy 2015, 17, 7926–7947. [Google Scholar] [CrossRef]
- Nikulin, V.V.; Brismar, T. Comment on “multiscale entropy analysis of complex physiologic time series”. Phys. Rev. Lett. 2004, 92, 089803. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.T.; Zhuang, J.; Yu, W.X.; Wang, Z.Z. Measuring complexity using fuzzyen, apen, and sampen. Med. Eng. Phys. 2009, 31, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Li, K.; Zhao, L.N.; Liu, F.; Zheng, D.C.; Liu, C.C.; Liu, S.T. Analysis of heart rate variability using fuzzy measure entropy. Comput. Biol. Med. 2013, 43, 100–108. [Google Scholar] [CrossRef]
- Liu, C.Y.; Zhao, L.N. Using fuzzy measure entropy to improve the stability of traditional entropy measures. In Proceedings of the 2011 Computing in Cardiology, Hangzhou, China, 18–21 September 2011; pp. 681–684. [Google Scholar]
- Zhao, L.N.; Liu, C.Y.; Wei, S.S.; Shen, Q.; Zhou, F.; Li, J.Q. A new entropy-based atrial fibrillation detection method for scanning wearable ecg recordings. Entropy 2018, 20, 904. [Google Scholar] [CrossRef] [Green Version]
- Narin, A.; Isler, Y.; Ozer, M.; Perc, M. Early prediction of paroxysmal atrial fibrillation based on short-term heart rate variability. Phys. A Stat. Mech. Its Appl. 2018, 509, 56–65. [Google Scholar] [CrossRef]
- Liu, C.Y.; Oster, J.; Li, Q.; Zhao, L.N.; Nemati, S.; Clifford, G.D. A comparison of entropy approaches for af discrimination. Physiol. Meas. 2018, 39, 074002. [Google Scholar] [CrossRef]
- Ródenas, J.; García, M.; Alcaraz, R.; Rieta, J.J. Wavelet entropy automatically detects episodes of atrial fibrillation from single-lead electrocardiograms. Entropy 2015, 17, 6179–6199. [Google Scholar] [CrossRef]
- Xiong, J.L.; Liang, X.Y.; Liu, C.Y. A new entropy-based heart failure detector. In Proceedings of the 2019 Computing in Cardiology (CinC), Singapore, Singapore, 8–11 September 2019; p. 060. [Google Scholar]
- Isler, Y.; Narin, A.; Ozer, M.; Perc, M. Multi-stage classification of congestive heart failure based on short-term heart rate variability. ChaosSolitons Fractals 2019, 118, 145–151. [Google Scholar] [CrossRef]
- Costa, M.D.; Henriques, T.; Munshi, M.N.; Segal, A.R.; Goldberger, A.L. Dynamical glucometry: Use of multiscale entropy analysis in diabetes. Chaos 2014, 24, 033139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lake, D.E.; Moorman, J.R. Accurate estimation of entropy in very short physiological time series: The problem of atrial fibrillation detection in implanted ventricular devices. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H319–H325. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.L.; Liang, X.Y.; Zhu, T.T.; Zhao, L.N.; Li, J.Q.; Liu, C.Y. A new physically meaningful threshold of sample entropy for detecting cardiovascular diseases. Entropy 2019, 21, 830. [Google Scholar] [CrossRef] [Green Version]
- Mateo, J.; Laguna, P. Analysis of heart rate variability in the presence of ectopic beats using the heart timing signal. IEEE Trans. Biomed. Eng. 2003, 50, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Salo, M.A.; Huikuri, H.V.; Seppänen, T. Ectopic beats in heart rate variability analysis: Effects of editing on time and frequency domain measures. Ann. Noninvasive Electrocardiol. 2001, 6, 5–17. [Google Scholar] [CrossRef] [PubMed]
- NabilF, D.; Reguig, F.B. Ectopic beats detection and correction methods: A review. Biomed. Signal Process. Control 2015, 18, 228–244. [Google Scholar] [CrossRef]
- Singh, B.; Singh, D.; Jaryal, A.K.; Deepak, K.K. Ectopic beats in approximate entropy and sample entropy-based hrv assessment. Int. J. Syst. Sci. 2012, 43, 884–893. [Google Scholar] [CrossRef]
- Berntson, G.G.; Stowell, J.R. ECG artifacts and heart period variability: Don’t miss a beat. Psychophysiology 1998, 35, 127–132. [Google Scholar] [CrossRef]
- Peltola, M.A. Role of editing of r-r intervals in the analysis of heart rate variability. Front Physiol. 2012, 3, 148. [Google Scholar] [CrossRef] [Green Version]
- Tarkiainen, T.H.; Kuusela, T.A.; Tahvanainen, K.U.; Hartikainen, J.E.; Tiittanen, P.; Timonen, K.L.; Vanninen, E.J. Comparison of methods for editing of ectopic beats in measurements of short-term non-linear heart rate dynamics. Clin. Physiol. Funct. Imaging 2007, 27, 126–133. [Google Scholar] [CrossRef]
- Liu, C.Y.; Li, L.P.; Zhao, L.N.; Zheng, D.C.; Li, P.; Liu, C.C. A combination method of improved impulse rejection filter and template matching for identification of anomalous intervals in RR sequences. J. Med. Biol. Eng. 2012, 32, 245–250. [Google Scholar] [CrossRef]
- Liu, C.Y.; Zhang, X.Y.; Zhao, L.N.; Liu, F.F.; Chen, X.W.; Yao, Y.J.; Li, J.Q. Signal quality assessment and lightweight QRS detection for wearable ECG smartvest system. IEEE Internet Things J. 2019, 6, 1363–1374. [Google Scholar] [CrossRef]
- Perc, M. Nonlinear time series analysis of the human electrocardiogram. Eur. J. Phys. 2005, 26, 757. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.F.; Wei, S.S.; Li, Y.B.; Jiang, X.E.; Zhang, Z.M.; Liu, C.Y. Performance analysis of ten common QRS detectors on different ECG application cases. J. Healthc. Eng. 2018, 2018, 9050812. [Google Scholar] [CrossRef] [Green Version]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. Physiobank, physiotoolkit, and physionet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Chon, K.H.; Scully, C.G.; Lu, S. Approximate entropy for all signals. IEEE Eng. Med. Biol. Mag. 2009, 28, 18–23. [Google Scholar] [CrossRef]
- Udhayakumar, R.K.; Karmakar, C.; Palaniswami, M. Understanding irregularity characteristics of short-term hrv signals using sample entropy profile. IEEE Trans. Biomed. Eng. 2018, 65, 2569–2579. [Google Scholar] [CrossRef]
- Angelini, L.; Maestri, R.; Marinazzo, D.; Nitti, L.; Pellicoro, M.; Pinna, G.D.; Stramaglia, S.; Tupputi, S.A. Multiscale analysis of short term heart beat interval, arterial blood pressure, and instantaneous lung volume time series. Artif. Intell. Med. 2007, 41, 237–250. [Google Scholar] [CrossRef]
- Silva, L.E.; Lataro, R.M.; Castania, J.A.; da Silva, C.A.; Valencia, J.F.; Murta, L.O.; Salgado, H.C.; Fazan, R.; Porta, A. Multiscale entropy analysis of heart rate variability in heart failure, hypertensive, and sinoaortic-denervated rats: Classical and refined approaches. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2016, 311, R150–R156. [Google Scholar] [CrossRef]
- Clifford, G.D.; Tarassenko, L. Quantifying errors in spectral estimates of hrv due to beat replacement and resampling. IEEE Trans. Biomed. Eng. 2005, 52, 630–638. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Record | # Ectopic Beats | # Ectopic Segments | Record | # Ectopic Beats | # Ectopic Segments |
|---|---|---|---|---|---|
| NSR001 | 81 | 58 | NSR028 | 166 | 95 |
| NSR002 | 233 | 146 | NSR029 | 24 | 18 |
| NSR003 | 50 | 37 | NSR030 | 92 | 58 |
| NSR004 | 36 | 33 | NSR031 | 630 | 191 |
| NSR005 | 611 | 198 | NSR032 | 490 | 188 |
| NSR006 | 96 | 40 | NSR033 | 15 | 14 |
| NSR007 | 113 | 81 | NSR034 | 21 | 18 |
| NSR008 | 70 | 50 | NSR035 | 43 | 29 |
| NSR009 | 30 | 25 | NSR036 | 169 | 28 |
| NSR010 | 206 | 107 | NSR037 | 31 | 29 |
| NSR011 | 152 | 92 | NSR038 * | 6 | 4 |
| NSR012 | 46 | 40 | NSR039 | 131 | 87 |
| NSR013 | 38 | 32 | NSR040 | 40 | 17 |
| NSR014 | 305 | 112 | NSR041 | 32 | 29 |
| NSR015 | 36 | 24 | NSR042 * | 11 | 10 |
| NSR016 | 47 | 42 | NSR043 | 241 | 123 |
| NSR017 | 958 | 265 | NSR044 | 5225 | 270 |
| NSR018 | 547 | 213 | NSR045 | 233 | 149 |
| NSR019 | 42 | 33 | NSR046 | 302 | 94 |
| NSR020 | 169 | 108 | NSR047 | 22 | 22 |
| NSR021 | 12 | 12 | NSR048 | 31 | 21 |
| NSR022 | 56 | 47 | NSR049 * | 3 | 3 |
| NSR023 | 53 | 34 | NSR050 * | 3 | 3 |
| NSR024 | 8033 | 272 | NSR051 * | 6 | 6 |
| NSR025 | 492 | 120 | NSR052 * | 13 | 10 |
| NSR026 | 92 | 44 | NSR053 * | 1 | 1 |
| NSR027 * | 5 | 5 | NSR054 * | 9 | 8 |
| Record | # Ectopic Beats | # Ectopic Segments | Record | # Ectopic Beats | # Ectopic Segments |
|---|---|---|---|---|---|
| CHF201 | 61 | 36 | CHF216 | 18 | 14 |
| CHF202 | 273 | 150 | CHF217 | 779 | 228 |
| CHF203 | 496 | 187 | CHF218 | 2667 | 217 |
| CHF204 | 2297 | 247 | CHF219 | 37 | 28 |
| CHF205 | 1356 | 245 | CHF220 | 820 | 143 |
| CHF206 | 11,112 | 240 | CHF221 * | 11,608 | 276 |
| CHF207 * | 15,189 | 249 | CHF222 | 2792 | 274 |
| CHF208 | 3073 | 257 | CHF223 * | 5410 | 274 |
| CHF209 | 507 | 156 | CHF224 | 356 | 150 |
| CHF210 | 2122 | 258 | CHF225 | 242 | 121 |
| CHF211 | 14 | 11 | CHF226 | 1638 | 257 |
| CHF212 | 3483 | 205 | CHF227 * | 5649 | 275 |
| CHF213 | 10,968 | 281 | CHF228 | 1467 | 204 |
| CHF214 * | 21,160 | 204 | CHF229 | 22 | 20 |
| CHF215 | 5851 | 166 |
| Record | Variance Ratios (%) | Standard Deviation (%) | ||||
|---|---|---|---|---|---|---|
| m = 2, r = 0.2 | m = 1, r = 12 ms | m = 2, r = 12 ms | m = 2, r = 0.2 | m = 1, r = 12 ms | m = 2, r = 12 ms | |
| NSR001 | −5.62 | 0.64 | 0.41 | 14.43 | 0.74 | 0.69 |
| NSR002 | −16.32 | 0.81 | 0.57 | 21.93 | 0.66 | 0.72 |
| NSR003 | −10.60 | 0.45 | 0.30 | 16.37 | 0.49 | 0.64 |
| NSR004 | −10.41 | 0.32 | 0.18 | 18.24 | 0.35 | 0.33 |
| NSR005 | −4.91 | 0.79 | 0.55 | 12.72 | 0.86 | 0.83 |
| NSR006 | −10.24 | 0.35 | 0.26 | 18.68 | 0.33 | 0.44 |
| NSR007 | −2.81 | 0.67 | 0.53 | 10.74 | 0.46 | 0.64 |
| NSR008 | −6.07 | 0.42 | 0.37 | 14.75 | 0.42 | 0.66 |
| NSR009 | −0.17 | 0.29 | 0.21 | 2.27 | 0.36 | 0.42 |
| NSR010 | −8.40 | 0.46 | 0.38 | 13.15 | 0.48 | 0.60 |
| NSR011 | −6.05 | 0.50 | 0.43 | 14.07 | 0.45 | 0.57 |
| NSR012 | −3.70 | 0.41 | 0.24 | 10.15 | 0.52 | 0.58 |
| NSR013 | −3.13 | 0.67 | 0.51 | 12.16 | 0.62 | 0.62 |
| NSR014 | −2.55 | 0.40 | 0.09 | 8.06 | 0.55 | 0.93 |
| NSR015 | −1.66 | 0.63 | 0.49 | 9.53 | 0.61 | 0.64 |
| NSR016 | −5.86 | 0.48 | 0.32 | 16.40 | 0.53 | 0.60 |
| NSR017 | −6.81 | 0.83 | 0.42 | 13.86 | 0.74 | 0.84 |
| NSR018 | −14.06 | 0.77 | 0.62 | 19.45 | 0.70 | 0.85 |
| NSR019 | −0.31 | 0.60 | 0.64 | 3.52 | 0.55 | 0.75 |
| NSR020 | −5.11 | 0.58 | 0.52 | 12.63 | 0.51 | 0.68 |
| NSR021 | −4.51 | 0.35 | 0.00 | 12.49 | 0.42 | 0.28 |
| NSR022 | −7.99 | 0.44 | 0.20 | 14.61 | 0.46 | 0.59 |
| NSR023 | −4.27 | 0.52 | 0.24 | 13.01 | 0.50 | 0.48 |
| NSR024 | −2.79 | 1.00 | 0.34 | 8.37 | 0.79 | 0.44 |
| NSR025 | −2.64 | 0.57 | 0.28 | 8.69 | 0.55 | 0.60 |
| NSR026 | −3.59 | 0.96 | 0.77 | 11.62 | 1.42 | 1.25 |
| NSR028 | −13.87 | 0.76 | 0.66 | 22.18 | 0.79 | 0.85 |
| NSR029 | −5.62 | 0.69 | 0.35 | 14.90 | 0.62 | 0.55 |
| NSR030 | −6.30 | 0.60 | 0.29 | 15.06 | 0.65 | 0.57 |
| NSR031 | −5.44 | 1.40 | 0.88 | 14.75 | 1.30 | 1.10 |
| NSR032 | −18.85 | 1.73 | 1.61 | 25.99 | 1.92 | 2.43 |
| NSR033 | −2.27 | 0.41 | 0.14 | 6.77 | 0.42 | 0.64 |
| NSR034 | −2.58 | 0.52 | 0.22 | 11.91 | 0.49 | 0.30 |
| NSR035 | −8.24 | 0.66 | 0.45 | 17.83 | 0.55 | 0.69 |
| NSR036 | −13.94 | 0.25 | 0.10 | 20.16 | 0.36 | 0.31 |
| NSR037 | −3.47 | 0.46 | 0.37 | 12.94 | 0.57 | 0.75 |
| NSR039 | −12.35 | 0.78 | 0.64 | 20.96 | 0.67 | 0.77 |
| NSR040 | −4.44 | 0.85 | 0.71 | 13.05 | 0.49 | 0.78 |
| NSR041 | −2.20 | 0.36 | 0.30 | 9.36 | 0.43 | 0.52 |
| NSR043 | −16.28 | 0.97 | 0.74 | 23.58 | 0.82 | 0.82 |
| NSR044 | −20.46 | 1.04 | 0.92 | 22.74 | 0.93 | 1.09 |
| NSR045 | −13.36 | 0.53 | 0.39 | 18.43 | 0.52 | 0.67 |
| NSR046 | −8.72 | 0.60 | 0.33 | 17.58 | 0.58 | 0.69 |
| NSR047 | 0.18 | 0.37 | 0.13 | 0.35 | 0.23 | 0.30 |
| NSR048 | −2.10 | 0.46 | 0.05 | 6.53 | 0.54 | 0.19 |
| Average | −6.91 | 0.63 | 0.43 | 13.93 | 0.62 | 0.68 |
| Record | Variance Ratios (%) | Standard Deviation (%) | ||||
|---|---|---|---|---|---|---|
| m = 2, r = 0.2 | m = 1, r = 12 ms | m = 2, r = 12 ms | m = 2, r = 0.2 | m = 1, r = 12 ms | m = 2, r = 12 ms | |
| CHF201 | −3.48 | 0.44 | 0.22 | 10.98 | 0.44 | 0.33 |
| CHF202 | −3.18 | 0.55 | 0.20 | 11.36 | 0.49 | 0.42 |
| CHF203 | −7.00 | 2.19 | 2.43 | 18.09 | 1.82 | 2.24 |
| CHF204 | −15.87 | 2.06 | 0.73 | 24.74 | 1.25 | 0.94 |
| CHF205 | −2.81 | 1.88 | 1.64 | 13.97 | 1.09 | 1.36 |
| CHF206 | 0.09 | 3.82 | 4.14 | 8.16 | 3.17 | 3.53 |
| CHF208 | −1.49 | 2.27 | 2.45 | 13.20 | 1.70 | 2.21 |
| CHF209 | 0.45 | 2.26 | 2.59 | 0.61 | 2.16 | 2.70 |
| CHF210 | −0.85 | 2.28 | 2.01 | 8.64 | 1.45 | 1.35 |
| CHF211 | −1.74 | 0.35 | 0.11 | 6.69 | 0.51 | 0.36 |
| CHF212 | 6.02 | 1.76 | 2.10 | 12.43 | 2.11 | 2.41 |
| CHF213 | −40.79 | 0.66 | 0.19 | 19.12 | 0.54 | 0.49 |
| CHF215 | 0.20 | 0.96 | 0.95 | 0.28 | 1.21 | 1.44 |
| CHF216 | −2.91 | 0.68 | 0.63 | 7.90 | 0.43 | 0.84 |
| CHF217 | −8.92 | 1.15 | 0.66 | 15.62 | 0.91 | 0.79 |
| CHF218 | −9.88 | 1.21 | 1.00 | 21.18 | 0.95 | 1.10 |
| CHF219 | −2.05 | 0.50 | 0.38 | 5.81 | 0.57 | 0.63 |
| CHF220 | −2.24 | 1.30 | 1.13 | 10.77 | 1.30 | 1.46 |
| CHF222 | −15.62 | 2.87 | 2.41 | 25.51 | 1.64 | 1.76 |
| CHF224 | −1.79 | 1.12 | 0.72 | 7.89 | 1.06 | 1.13 |
| CHF225 | −3.22 | 1.19 | 1.26 | 15.88 | 1.03 | 1.38 |
| CHF226 | −2.36 | 3.85 | 4.56 | 13.11 | 3.43 | 4.44 |
| CHF228 CHF201 | −1.06 | 1.48 | 1.44 | 7.95 | 1.24 | 1.47 |
| CHF229 | 0.24 | 0.17 | −0.01 | 0.70 | 0.21 | 0.24 |
| Average | −5.01 | 1.54 | 1.41 | 11.69 | 1.28 | 1.46 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, L.; Li, J.; Xiong, J.; Liang, X.; Liu, C. Suppressing the Influence of Ectopic Beats by Applying a Physical Threshold-Based Sample Entropy. Entropy 2020, 22, 411. https://doi.org/10.3390/e22040411
Zhao L, Li J, Xiong J, Liang X, Liu C. Suppressing the Influence of Ectopic Beats by Applying a Physical Threshold-Based Sample Entropy. Entropy. 2020; 22(4):411. https://doi.org/10.3390/e22040411
Chicago/Turabian StyleZhao, Lina, Jianqing Li, Jinle Xiong, Xueyu Liang, and Chengyu Liu. 2020. "Suppressing the Influence of Ectopic Beats by Applying a Physical Threshold-Based Sample Entropy" Entropy 22, no. 4: 411. https://doi.org/10.3390/e22040411