
Network Motif Detection in the Network of Inflammatory Markers and Depression Symptoms among Patients with Stable Coronary Heart Disease: Insights from the Heart and Soul Study

Abstract
:1. Introduction
Study Aims
2. Materials and Methods
2.1. Dataset and Sample
2.2. Measures
2.2.1. Inflammation Markers and Covariates
2.2.2. Depression Symptoms
2.3. Statistical Analysis
2.3.1. Correlation Network Construction
2.3.2. Network Motif Analysis
3. Results
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bankier, B.; Barajas, J.; Martinez-Rumayor, A.; Januzzi, J.L. Association between major depressive disorder and C-reactive protein levels in stable coronary heart disease patients. J. Psychosom. Res. 2009, 66, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Howren, M.B.; Lamkin, D.M.; Suls, J. Associations of depression with C-reactive protein, IL-1, and IL-6: A meta-analysis. Psychosom. Med. 2009, 71, 171–186. [Google Scholar] [CrossRef]
- Lespérance, F.; Frasure-Smith, N.; Théroux, P.; Irwin, M. The association between major depression and levels of soluble intercellular adhesion molecule 1, interleukin-6, and C-reactive protein in patients with recent acute coronary syndromes. Am. J. Psychiatry 2004, 161, 271–277. [Google Scholar] [CrossRef]
- Davidson, K.W.; Schwartz, J.E.; Kirkland, S.A.; Mostofsky, E.; Fink, D.; Guernsey, D.; Shimbo, D. Relation of inflammation to depression and incident coronary heart disease (from the Canadian Nova Scotia Health Survey [NSHS95] Prospective Population Study). Am. J. Cardiol. 2009, 103, 755–761. [Google Scholar] [CrossRef]
- Whooley, M.A.; Caska, C.M.; Hendrickson, B.E.; Rourke, M.A.; Ho, J.; Ali, S. Depression and inflammation in patients with coronary heart disease: Findings from the Heart and Soul Study. Biol. Psychiatry 2007, 62, 314–320. [Google Scholar] [CrossRef]
- Fried, E.I.; Nesse, R.M.; Zivin, K.; Guille, C.; Sen, S. Depression is more than the sum score of its parts: Individual DSM symptoms have different risk factors. Psychol. Med. 2014, 44, 2067–2076. [Google Scholar] [CrossRef]
- Fried, E.I.; Nesse, R.M. Depression sum-scores don’t add up: Why analyzing specific depression symptoms is essential. BMC Med. 2015, 13, 72. [Google Scholar] [CrossRef]
- Hoen, P.W.; Whooley, M.A.; Martens, E.J.; Na, B.; van Melle, J.P.; de Jonge, P. Differential associations between specific depressive symptoms and cardiovascular prognosis in patients with stable coronary heart disease. J. Am. Coll. Cardiol. 2010, 56, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Whooley, M.A. Networks of C-reactive protein and depression symptoms in patients with stable coronary heart disease: Findings from the Heart and Soul Study. Int. J. Methods Psychiatr. Res. 2023, 32, e1968. [Google Scholar] [CrossRef]
- Borsboom, D.; Cramer, A.O. Network analysis: An integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 2013, 9, 91–121. [Google Scholar] [CrossRef]
- Fried, E.I.; Von Stockert, S.; Haslbeck, J.M.B.; Lamers, F.; Schoevers, R.A.; Penninx, B.W.J.H. Using network analysis to examine links between individual depressive symptoms, inflammatory markers, and covariates. Psychol. Med. 2020, 50, 2682–2690. [Google Scholar] [CrossRef]
- Kappelmann, N.; Czamara, D.; Rost, N.; Moser, S.; Schmoll, V.; Trastulla, L.; Stochl, J.; Lucae, S.; Binder, E.B.; Khandaker, G.M.; et al. Polygenic risk for immuno-metabolic markers and specific depressive symptoms: A multi-sample network analysis study. Brain Behav. Immun. 2021, 95, 256–268. [Google Scholar] [CrossRef]
- Moriarity, D.P.; Horn, S.R.; Kautz, M.M.; Haslbeck, J.M.; Alloy, L.B. How handling extreme C-reactive protein (CRP) values and regularization influences CRP and depression criteria associations in network analyses. Brain Behav. Immun. 2021, 91, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Min, S.H. Racial differences in C-reactive protein, depression symptoms, and social relationships in older adults: A moderated network analysis. Biol. Res. Nurs. 2023, 25, 480–490. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Min, S.H.; Niitsu, K. C-Reactive protein and specific depression symptoms among older adults: An exploratory investigation of multi-plane networks using cross-sectional data from NHANES (2017–2020). Biol. Res. Nurs. 2023, 25, 14–23. [Google Scholar] [CrossRef]
- Manfro, P.H.; Anselmi, L.; Barros, F.; Gonçalves, H.; Murray, J.; Oliveira, I.O.; Tovo-Rodrigues, L.; Wehrmeister, F.C.; Menezes, A.M.; Mondelli, V.; et al. Youth depression and inflammation: Cross-sectional network analyses of C-Reactive protein, interleukin-6 and symptoms in a population-based sample. J. Psychiatr. Res. 2022, 150, 197–201. [Google Scholar] [CrossRef]
- Santoso, A.M.; Jansen, F.; Peeters, C.F.; Baatenburg de Jong, R.J.; Brakenhoff, R.H.; Langendijk, J.A.; Verdonck-de Leeuw, I.M. Psychoneurological symptoms and biomarkers of stress and inflammation in newly diagnosed head and neck cancer patients: A network analysis. Curr. Oncol. 2022, 29, 7109–7121. [Google Scholar] [CrossRef]
- Henneghan, A.; Wright, M.L.; Bourne, G.; Sales, A.C. A cross-sectional exploration of cytokine–symptom networks in breast cancer survivors using network analysis. Can. J. Nurs. Res. 2021, 53, 303–315. [Google Scholar] [CrossRef]
- Mester, A.; Pop, A.; Mursa, B.E.M.; Greblă, H.; Dioşan, L.; Chira, C. Network analysis based on important node selection and community detection. Mathematics 2021, 9, 2294. [Google Scholar] [CrossRef]
- Smith, N.R.; Zivich, P.N.; Frerichs, L.M.; Moody, J.; Aiello, A.E. A guide for choosing community detection algorithms in social network studies: The question alignment approach. Am. J. Prev. Med. 2020, 59, 597–605. [Google Scholar] [CrossRef]
- Gunst, A.; Werner, M.; Waldorp, L.J.; Laan, E.; Källström, M.; Jern, P. A network analysis of female sexual function: Comparing symptom networks in women with decreased, increased, and stable sexual desire. Sci. Rep. 2018, 8, 15815. [Google Scholar] [CrossRef]
- Kim, W.; Li, M.; Wang, J.; Pan, Y. Biological network motif detection and evaluation. BMC Syst. Biol. 2011, 5, S5. Available online: http://www.biomedcentral.com/1752-0509/5/S3/S5 (accessed on 23 August 2023). [CrossRef] [PubMed]
- Narsis, A.; Mikko, K. Structural Analysis of Biological Networks. In Networks of Networks in Biology: Concepts, Tools and Applications; Kiani, N., Gomez-Cabrero, D., Bianconi, G., Eds.; Cambridge University Press: Cambridge, UK, 2021; pp. 35–55. [Google Scholar] [CrossRef]
- Kim, W.; Li, M.; Wang, J.; Pan, Y. Essential protein discovery based on network motif and gene ontology. In Proceedings of the 2011 IEEE International Conference on Bioinformatics and Biomedicine, Atlanta, GA, USA, 12–15 November 2011; pp. 470–475. [Google Scholar]
- Kai, S.; Lin, G.; Bo, W.B. An integrated network motif based approach to identify colorectal cancer related genes. In Proceedings of the 2015 34th Chinese Control Conference (CCC), Hangzhou, China, 28–30 July 2015; pp. 8573–8578. [Google Scholar]
- Jin, G.; Zhang, S.; Zhang, X.S.; Chen, L. Hubs with network motifs organize modularity dynamically in the protein-protein interaction network of yeast. PLoS ONE 2007, 2, e1207. [Google Scholar] [CrossRef] [PubMed]
- Duma, A.; Topirceanu, A. A network motif based approach for classifying online social networks. In Proceedings of the 2014 IEEE 9th IEEE International Symposium on Applied Computational Intelligence and Informatics (SACI), Timisoara, Romania, 15–17 May 2014; pp. 311–315. [Google Scholar]
- Chen, B.; Zhu, X.; Shui, H. Socio-semantic network motifs framework for discourse analysis. In Proceedings of the LAK22: 12th International Learning Analytics and Knowledge Conference, Online, 21–25 March 2022; pp. 500–506. [Google Scholar]
- Ruo, B.; Rumsfeld, J.S.; Hlatky, M.A.; Liu, H.; Browner, W.S.; Whooley, M.A. Depressive symptoms and health-related quality of life: The Heart and Soul Study. JAMA 2003, 290, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Kendler, K.S.; Aggen, S.H.; Neale, M.C. Evidence for multiple genetic factors underlying DSM-IV criteria for major depression. JAMA Psychiatry 2013, 70, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Hsu, Y.H.; Li, Z.; Mar, P.; Wang, Y. NemoSuite: Web-based Network Motif Analytic Suite. Adv. Sci. Technol. Eng. Syst. J. 2020, 5, 1545–1553. [Google Scholar] [CrossRef]
- Huynh, T.; Mbadiwe, S.; Kim, W. Nemomap: Improved motif-centric network motif discovery algorithm. Adv. Sci. Technol. Eng. Syst. 2018, 3, 186–199. [Google Scholar] [CrossRef]
- Kim, W.; Haukap, L. Nemoprofile: Effective representation for network motif and their instances. In Proceedings of the 12th International Symposium on Bioinformatics Research and Applications (ISBRA), Minsk, Belarus, 5–8 June 2016; pp. 5–8. [Google Scholar]
- Najjar, S.; Pearlman, D.M.; Devinsky, O.; Najjar, A.; Zagzag, D. Neurovascular unit dysfunction with blood-brain barrier hyperpermeability contributes to major depressive disorder: A review of clinical and experimental evidence. J. Neuroinflamm. 2013, 10, 142. [Google Scholar] [CrossRef]
- Suarez, E.C.; Krishnan, R.R.; Lewis, J.G. The relation of severity of depressive symptoms to monocyte-associated proinflammatory cytokines and chemokines in apparently healthy men. Psychosom. Med. 2003, 65, 362–368. [Google Scholar] [CrossRef]
- Laake, J.P.S.; Stahl, D.; Amiel, S.A.; Petrak, F.; Sherwood, R.A.; Pickup, J.C.; Ismail, K. The association between depressive symptoms and systemic inflammation in people with type 2 diabetes: Findings from the South London Diabetes Study. Diabetes Care 2014, 37, 2186–2192. [Google Scholar] [CrossRef] [PubMed]
- Eyre, H.A.; Air, T.; Pradhan, A.; Johnston, J.; Lavretsky, H.; Stuart, M.J.; Baune, B.T. A meta-analysis of chemokines in major depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2016, 68, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Proma, M.A.; Daria, S.; Nahar, Z.; Ashraful Islam, S.M.; Bhuiyan, M.A.; Islam, M.R. Monocyte chemoattractant protein-1 levels are associated with major depressive disorder. J. Basic Clin. Physiol. Pharmacol. 2022, 33, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Xiong, G.L.; Prybol, K.; Boyle, S.H.; Hall, R.; Streilein, R.D.; Steffens, D.C.; SADHART-CHF Investigators. Inflammation markers and major depressive disorder in patients with chronic heart failure: Results from the sertraline against depression and heart disease in chronic heart failure study. Psychosom. Med. 2015, 77, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.; Haroon, E.; Felger, J. Inflammation Effects on Motivation and Motor Activity: Dopamine as Mediator and Treatment Target. Biol. Psychiatry 2018, 83, S62–S63. [Google Scholar] [CrossRef]
- Goldsmith, D.R.; Haroon, E.; Woolwine, B.J.; Jung, M.Y.; Wommack, E.C.; Harvey, P.D.; Miller, A.H. Inflammatory markers are associated with decreased psychomotor speed in patients with major depressive disorder. Brain Behav. Immun. 2016, 56, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, D.R.; Massa, N.; Pearce, B.D.; Wommack, E.C.; Alrohaibani, A.; Goel, N.; Duncan, E. Inflammatory markers are associated with psychomotor slowing in patients with schizophrenia compared to healthy controls. NPJ Schizophr. 2020, 6, 8. [Google Scholar] [CrossRef] [PubMed]
- Kazmi, N.; Wallen, G.R.; Yang, L.; Alkhatib, J.; Schwandt, M.L.; Feng, D.; Barb, J.J. An exploratory study of pro-inflammatory cytokines in individuals with alcohol use disorder: MCP-1 and IL-8 associated with alcohol consumption, sleep quality, anxiety, depression, and liver biomarkers. Front. Psychiatry 2022, 13, 931280. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Mohammadi, M.; Brühl, A.B.; Sadeghi-Bahmani, D.; Brand, S. Association of blood MCP-1 levels with risk of obstructive sleep apnea: A systematic review and meta-analysis. Medicina 2022, 58, 1266. [Google Scholar] [CrossRef]
- Martínez-Cengotitabengoa, M.; Mac-Dowell, K.S.; Leza, J.C.; Micó, J.A.; Fernandez, M.; Echevarría, E.; González-Pinto, A. Cognitive impairment is related to oxidative stress and chemokine levels in first psychotic episodes. Schizophr. Res. 2012, 137, 66–72. [Google Scholar] [CrossRef]
- Yuan, L.; Liu, A.; Qiao, L.; Sheng, B.; Xu, M.; Li, W.; Chen, D. The relationship of CSF and plasma cytokine levels in HIV infected patients with neurocognitive impairment. BioMed Res. Int. 2015, 2015, 506872. [Google Scholar] [CrossRef]
- Galimberti, D.; Fenoglio, C.; Lovati, C.; Venturelli, E.; Guidi, I.; Corrà, B.; Scarpini, E. Serum MCP-1 levels are increased in mild cognitive impairment and mild Alzheimer’s disease. Neurobiol. Aging 2006, 27, 1763–1768. [Google Scholar] [CrossRef]
- Westin, K.; Buchhave, P.; Nielsen, H.; Minthon, L.; Janciauskiene, S.; Hansson, O. CCL2 is associated with a faster rate of cognitive decline during early stages of Alzheimer’s disease. PLoS ONE 2012, 7, e30525. [Google Scholar] [CrossRef] [PubMed]
- Mack, W.J.; Ducruet, A.F.; Hickman, Z.L.; Zurica, J.; Starke, R.M.; Garrett, M.C.; Sander Connolly, E. Elevation of monocyte chemoattractant protein-1 in patients experiencing neurocognitive decline following carotid endarterectomy. Acta Neurochir. 2008, 150, 779–784. [Google Scholar] [CrossRef]
- Torres-Platas, S.G.; Cruceanu, C.; Chen, G.G.; Turecki, G.; Mechawar, N. Evidence for increased microglial priming and macrophage recruitment in the dorsal anterior cingulate white matter of depressed suicides. Brain Behav. Immun. 2014, 42, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Vares, E.A.; Salum, G.A.; Spanemberg, L.; Caldieraro, M.A.; Fleck, M.P. Depression dimensions: Integrating clinical signs and symptoms from the perspectives of clinicians and patients. PLoS ONE 2015, 10, e0136037. [Google Scholar] [CrossRef]
- Gotlib, I.H.; Hamilton, J.P. Neuroimaging and depression: Current status and unresolved issues. Curr. Dir. Psychol. Sci. 2008, 17, 159–163. [Google Scholar] [CrossRef]
- Lehto, S.M.; Niskanen, L.; Herzig, K.H.; Tolmunen, T.; Huotari, A.; Viinamäki, H.; Hintikka, J. Serum chemokine levels in major depressive disorder. Psychoneuroendocrinology 2010, 35, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Lindqvist, D.; Janelidze, S.; Erhardt, S.; Träskman-Bendz, L.; Engström, G.; Brundin, L. CSF biomarkers in suicide attempters–a principal component analysis. Acta Psychiatr. Scand. 2011, 124, 52–61. [Google Scholar] [CrossRef]
- Goyal, R.; Faizy, A.F.; Siddiqui, S.S.; Singhai, M. Evaluation of TNF-α and IL-6 levels in obese and non-obese diabetics: Pre-and postinsulin effects. N. Am. J. Med. Sci. 2012, 4, 180–184. [Google Scholar] [CrossRef]
- Maggio, M.; Guralnik, J.M.; Longo, D.L.; Ferrucci, L. Interleukin-6 in aging and chronic disease: A magnificent pathway. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.J.; Ghouri, N.; McKeigue, P.; Forouhi, N.G.; Sattar, N. Circulating IL-6 concentrations and associated anthropometric and metabolic parameters in South Asian men and women in comparison to European whites. Cytokine 2013, 61, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Moriarity, D.P.; Mengelkoch, S.; Slavich, G.M. Incorporating causal inference perspectives into psychoneuroimmunology: A simulation study highlighting concerns about controlling for adiposity in immunopsychiatry. Brain Behav. Immun. 2023, 113, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Coppack, S.W. Pro-inflammatory cytokines and adipose tissue. Proc. Nutr. Soc. 2001, 60, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Au, B.; Smith, K.J.; Gariépy, G.; Schmitz, N. Estimating the longitudinal associations between C-reactive protein and depressive symptoms: Evidence from the English Longitudinal Study of Ageing (ELSA). Int. J. Geriatr. Psychiatry 2015, 30, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Haukap, L. NemoProfile as an efficient approach to network motif analysis with instance collection. BMC Bioinform. 2017, 18, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Lü, J.; Yu, X. Identification of important nodes in directed biological networks: A network motif approach. PLoS ONE 2014, 9, e106132. [Google Scholar] [CrossRef]
- Wang, Y.; Kim, W. Identification of Essential Genes with NemoProfile and Various Machine Learning Models. In Bioinformatics Research and Applications: 16th International Symposium, ISBRA 2020, Moscow, Russia, 1–4 December 2020, Proceedings 16; Springer: Cham, Switzerland, 2020; pp. 319–326. [Google Scholar]
- Borsboom, D.; Deserno, M.K.; Rhemtulla, M.; Epskamp, S.; Fried, E.I.; McNally, R.J.; Robinaugh, D.J.; Perugini, M.; Dalege, J.; Costantini, G.; et al. Network analysis of multivariate data in psychological science. Nat. Rev. Methods Primers 2021, 1, 58. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
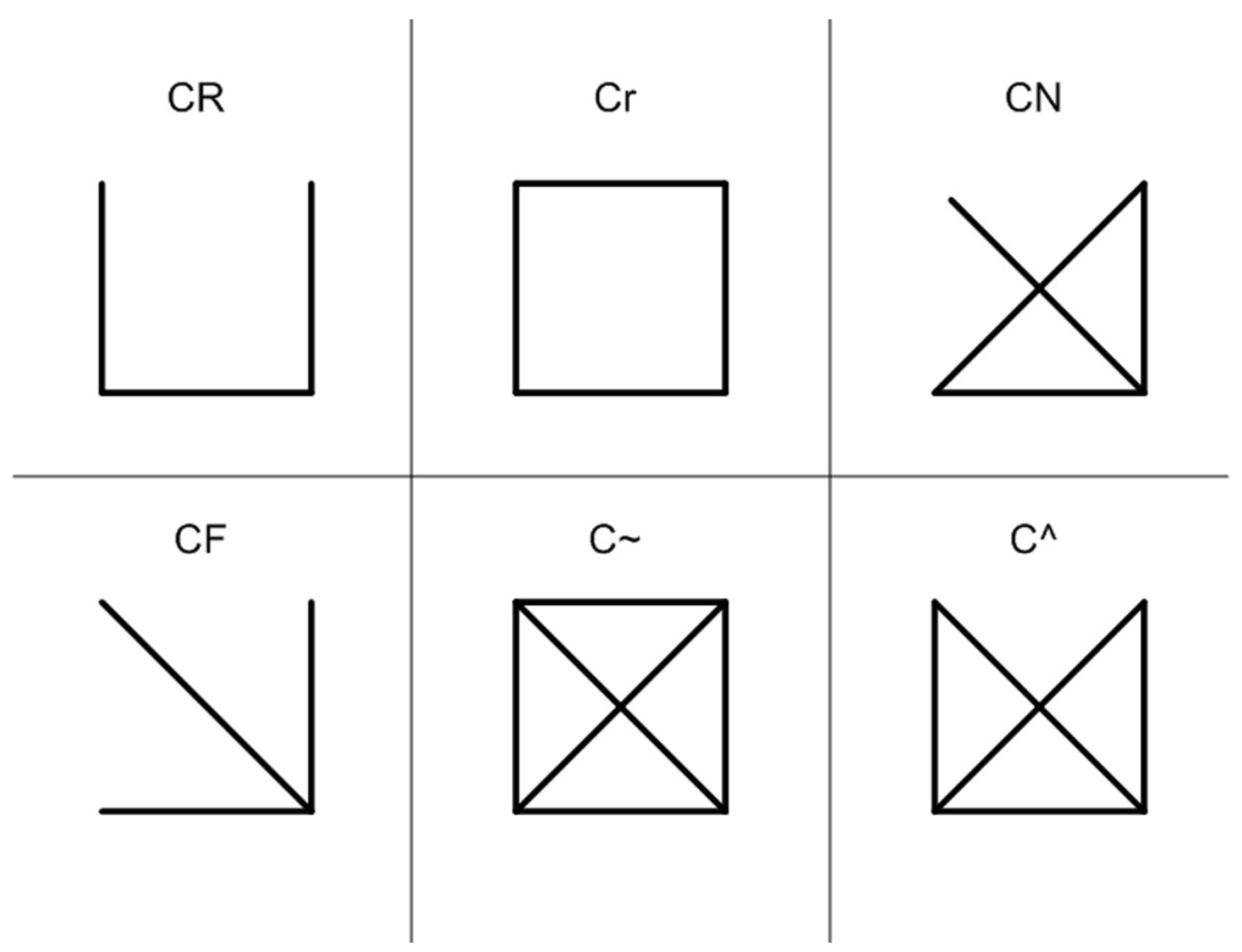
| Label | Pattern | Frequency [Original] | Mean Frequency in the Randomized Networks | z-Score | p-Value |
|---|---|---|---|---|---|
| CR |  | 48.8% | 61.7% | −3.54 | 1.000 |
| Cr |  | 3.9% | 4.1% | −0.07 | 0.400 |
| CN |  | 26.1% | 13.9% | 3.87 | 0.000 |
| CF |  | 9.9% | 18.6% | −2.68 | 1.000 |
| C~ |  | 0.5% | 0.1% | 2.21 | 0.100 |
| C^ |  | 10.8% | 1.8% | 7.33 | 0.000 |
| Node | CR | Cr | CN | CF | C~ | C^ |
|---|---|---|---|---|---|---|
| | | | | | |
| Psychomotor problems | 28 | 6 | 22 | 8 | 1 | 11 |
| Feelings of worthlessness | 37 | 4 | 17 | 6 | 0 | 10 |
| Concentration difficulty | 25 | 2 | 16 | 6 | 0 | 14 |
| Suicidal ideation | 25 | 5 | 14 | 6 | 0 | 6 |
| Loss of interest | 41 | 4 | 14 | 10 | 0 | 8 |
| Feelings of sadness | 15 | 0 | 3 | 3 | 0 | 0 |
| Appetite changes | 34 | 4 | 33 | 7 | 1 | 17 |
| Fatigue | 41 | 3 | 25 | 9 | 1 | 6 |
| Sleep disturbance | 31 | 2 | 21 | 6 | 1 | 8 |
| CRP | 3 | 0 | 2 | 1 | 0 | 0 |
| IL-6 | 17 | 0 | 7 | 1 | 0 | 1 |
| TNF-α | 8 | 0 | 2 | 2 | 0 | 1 |
| MCP-1 | 17 | 0 | 8 | 4 | 0 | 2 |
| Age | 38 | 1 | 17 | 8 | 0 | 3 |
| BMI | 32 | 1 | 11 | 3 | 0 | 1 |
| Label | Pattern | Examples | |||
|---|---|---|---|---|---|
| CN | |  |  |  |  |
 |  |  |  | ||
 |  |  |  | ||
 | |||||
| C~ | |  | |||
| C^ | |  |  | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.; Whooley, M.; Niitsu, K.; Kim, W. Network Motif Detection in the Network of Inflammatory Markers and Depression Symptoms among Patients with Stable Coronary Heart Disease: Insights from the Heart and Soul Study. Psychol. Int. 2024, 6, 440-453. https://doi.org/10.3390/psycholint6020027
Lee C, Whooley M, Niitsu K, Kim W. Network Motif Detection in the Network of Inflammatory Markers and Depression Symptoms among Patients with Stable Coronary Heart Disease: Insights from the Heart and Soul Study. Psychology International. 2024; 6(2):440-453. https://doi.org/10.3390/psycholint6020027
Chicago/Turabian StyleLee, Chiyoung, Mary Whooley, Kosuke Niitsu, and Wooyoung Kim. 2024. "Network Motif Detection in the Network of Inflammatory Markers and Depression Symptoms among Patients with Stable Coronary Heart Disease: Insights from the Heart and Soul Study" Psychology International 6, no. 2: 440-453. https://doi.org/10.3390/psycholint6020027