
Optimising the Use of Ultrasound in Gout: A Review from the Ground Up

Abstract
:1. Introduction
2. Machine Setting Optimisation for Crystal Visualisation
3. US Definitions for Crystal Identification in Tissues
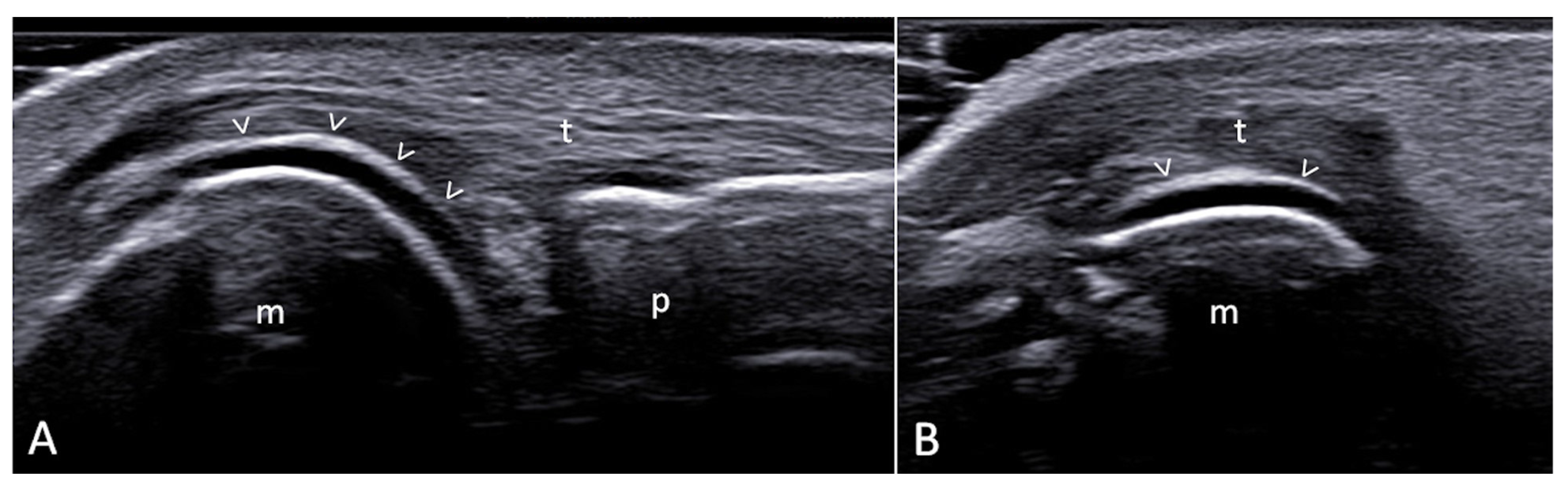
3.1. Double Contour Sign
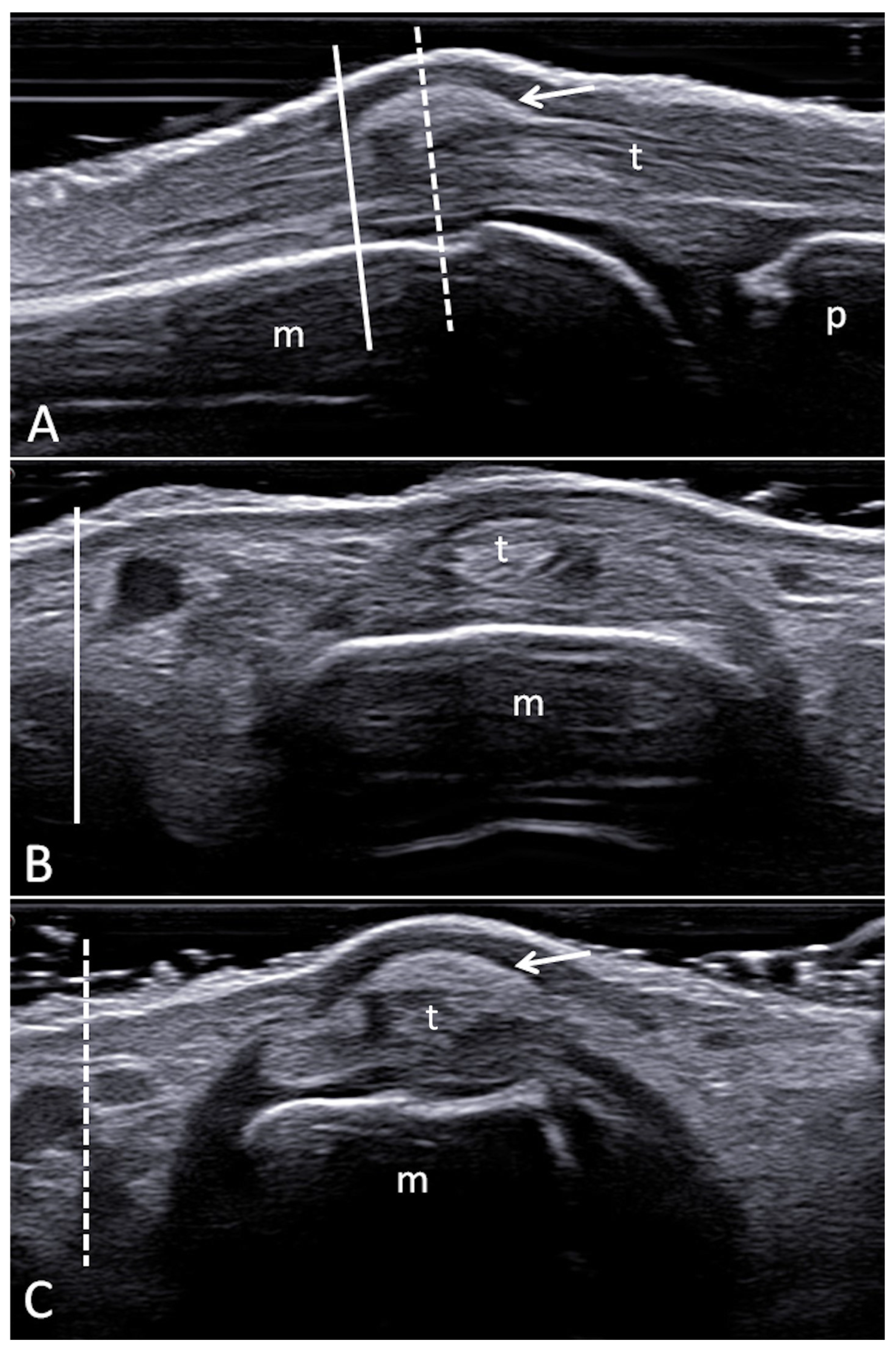
3.2. Tophi
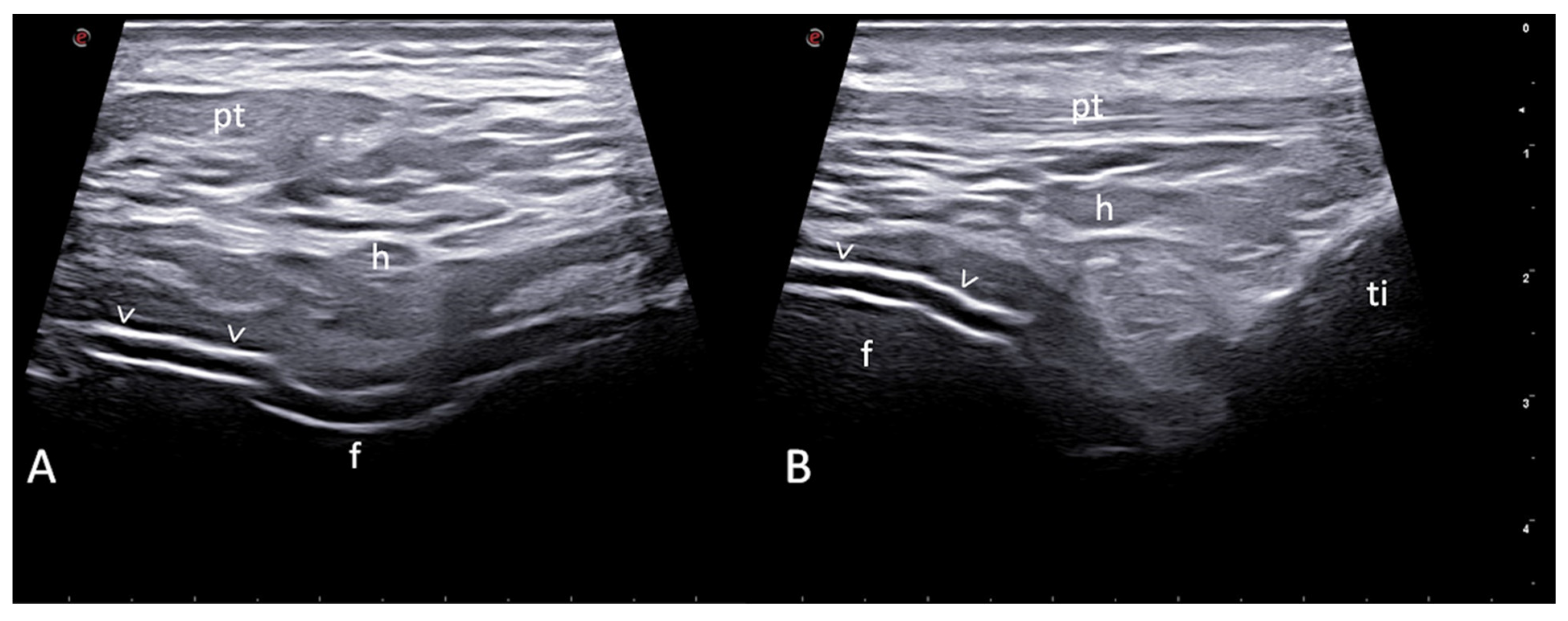
3.3. Aggregates
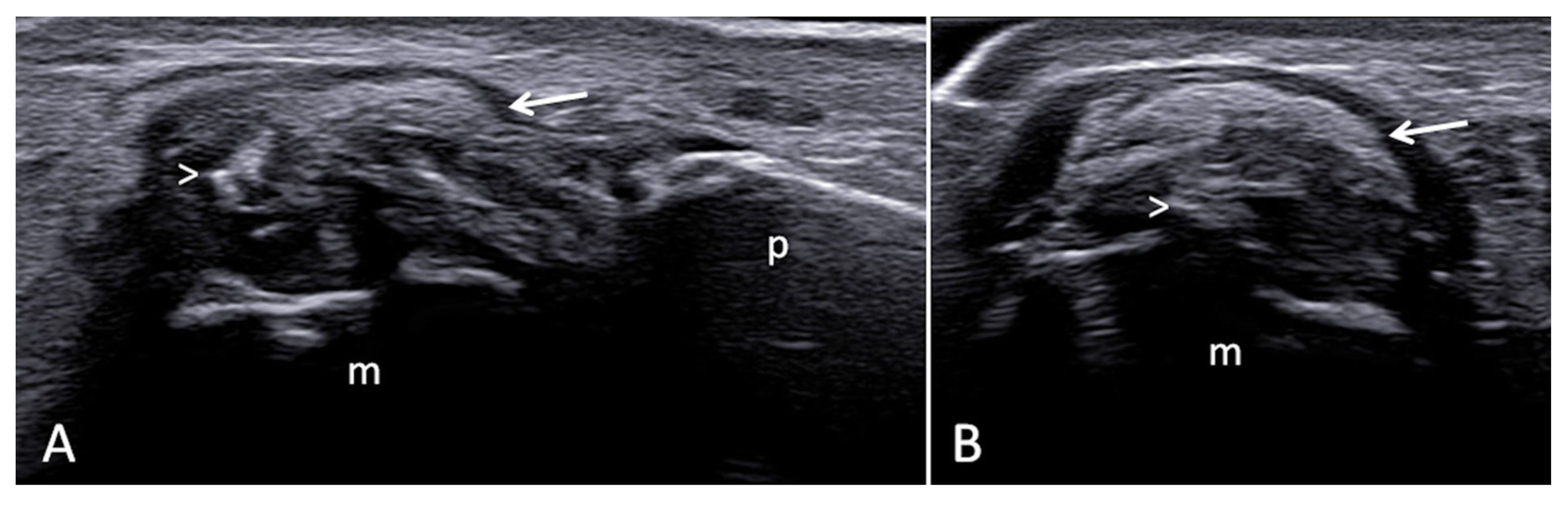
3.4. Bone Erosions
4. OMERACT Semiquantitative Scoring System
5. Main Applications of Ultrasound in Gout
6. Sonographic Diagnosis of Gout in the Inter-Critical Phases in Patients with Uncertain Diagnosis
7. Sonographic Diagnosis of Gout in Undiagnosed Mono- or Oligoarthritis
8. Sonographic Evaluation of MSU Burden in Patients Diagnosed with Gout for Prognosis and Treatment Monitoring
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dalbeth, N.; Merriman, T.R.; Stamp, L.K. Gout. Lancet 2016, 388, 2039–2052. [Google Scholar] [CrossRef] [PubMed]
- Dehlin, M.; Jacobsson, L.; Roddy, E. Global epidemiology of gout: Prevalence, incidence, treatment patterns and risk factors. Nat. Rev. Rheumatol. 2020, 16, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Prevalence of gout and hyperuricemia in the US general population: The National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum. 2011, 63, 3136–3141. [Google Scholar] [CrossRef]
- Singh, J.A.; Gaffo, A. Gout epidemiology and comorbidities. Semin. Arthritis Rheum. 2020, 50, S11–S16. [Google Scholar] [CrossRef]
- Cipolletta, E.; Tata, L.J.; Nakafero, G.; Avery, A.J.; Mamas, M.A.; Abhishek, A. Association Between Gout Flare and Subsequent Cardiovascular Events Among Patients with Gout. JAMA 2022, 328, 440–450. [Google Scholar] [CrossRef]
- Clarson, L.; Chandratre, P.; Hider, S.; Belcher, J.; Heneghan, C.; Roddy, E.; Mallen, C. Increased cardiovascular mortality associated with gout: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2015, 22, 335–343. [Google Scholar] [CrossRef]
- Neogi, T.; Jansen, T.L.T.A.; Dalbeth, N.; Fransen, J.; Schumacher, H.R.; Berendsen, D.; Brown, M.; Choi, H.; Edwards, N.L.; Janssens, H.J.E.M.; et al. 2015 Gout Classification Criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheumatol. 2015, 67, 2557–2568. [Google Scholar] [CrossRef] [PubMed]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castaneda, J.; Coyfish, M.; Guillo, S.; Jansen, T.; Janssens, H.; et al. 2018 updated European League Against Rheumatism evidence-based recommendations for the diagnosis of gout. Ann. Rheum. Dis. 2020, 79, 31–38. [Google Scholar] [CrossRef]
- Dalbeth, N.; Doyle, A.J. Imaging of gout: An overview. Best. Pract. Res. Clin. Rheumatol. 2012, 26, 823–838. [Google Scholar] [CrossRef]
- Ogdie, A.; Taylor, W.J.; Neogi, T.; Fransen, J.; Jansen, T.L.; Schumacher, H.R.; Louthrenoo, W.; Vazquez-Mellado, J.; Eliseev, M.; McCarthy, G.; et al. Performance of Ultrasound in the Diagnosis of Gout in a Multicenter Study: Comparison with Monosodium Urate Monohydrate Crystal Analysis as the Gold Standard. Arthritis Rheumatol. 2017, 69, 429–438. [Google Scholar] [CrossRef]
- Grassi, W.; Okano, T.; Filippucci, E. Use of ultrasound for diagnosis and monitoring of outcomes in crystal arthropathies. Curr. Opin. Rheumatol. 2015, 27, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Filippucci, E.; Reginato, A.M.; Thiele, R.G. Imaging of crystalline arthropathy in 2020. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101595. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, S.N.; Østergaard, M.; Terslev, L. Ultrasonography in gout: Utility in diagnosis and monitoring. Clin. Exp. Rheumatol. 2018, 36 (Suppl. S114), 61–67. [Google Scholar] [PubMed]
- Peiteado, D.; De Miguel, E.; Villalba, A.; Ordóñez, M.C.; Castillo, C.; Martín-Mola, E. Value of a short four-joint ultrasound test for gout diagnosis: A pilot study. Clin. Exp. Rheumatol. 2012, 30, 830–837. [Google Scholar] [PubMed]
- Naredo, E.; Uson, J.; Jiménez-Palop, M.; Martínez, A.; Vicente, E.; Brito, E.; Rodríguez, A.; Cornejo, F.J.; Castañeda, S.; Martínez, M.J.; et al. Ultrasound-detected musculoskeletal urate crystal deposition: Which joints and what findings should be assessed for diagnosing gout? Ann. Rheum. Dis. 2014, 73, 1522–1528. [Google Scholar] [CrossRef] [PubMed]
- Terslev, L.; Gutierrez, M.; Christensen, R.; Balint, P.V.; Bruyn, G.A.; Sedie, A.D.; Filippucci, E.; Garrido, J.; Hammer, H.B.; Iagnocco, A.; et al. Assessing Elementary Lesions in Gout by Ultrasound: Results of an OMERACT Patient-based Agreement and Reliability Exercise. J. Rheumatol. 2015, 42, 2149–2154. [Google Scholar] [CrossRef] [PubMed]
- Cazenave, T.; Pan-American League of Associations for Rheumatology (PANLAR) Ultrasound Study Group; Martire, V.; Reginato, A.M.; Gutierrez, M.; Waimann, C.A.; Pineda, C.; Rosa, J.E.; Ruta, S.; Sedano-Santiago, O.; et al. Reliability of OMERACT ultrasound elementary lesions in gout: Results from a multicenter exercise. Rheumatol. Int. 2019, 39, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, S.N.; Filippou, G.; Scirè, C.A.; Balint, P.V.; Bruyn, G.A.; Dalbeth, N.; Dejaco, C.; Sedie, A.D.; Filippucci, E.; Hammer, H.B.; et al. Consensus-based semi-quantitative ultrasound scoring system for gout lesions: Results of an OMERACT Delphi process and web-reliability exercise. Semin. Arthritis Rheum. 2021, 51, 644–649. [Google Scholar] [CrossRef]
- Filippou, G.; Sirotti, S.; Cipolletta, E.; Filippucci, E. Optimising the use of ultrasound in CPPD: A review from the ground up. Gout Urate Cryst. Depos. Dis. 2024, 2, 17–33. [Google Scholar] [CrossRef]
- Filippou, G.; Pacini, G.; Sirotti, S.; Zadory, M.; Carboni, D.; Damiani, A.; Fiorentini, E.; Cipolletta, E.; Filippucci, E.; Froehlich, J.M.; et al. Comparison of ultrasound attenuation by calcium pyrophosphate, hydroxyapatite and monosodium urate crystals: A proof-of-concept study. Ann. Rheum. Dis. 2022, 81, 1199–1201. [Google Scholar] [CrossRef]
- Filippucci, E.; Di Geso, L.; Grassi, W. Tips and tricks to recognize microcrystalline arthritis. Rheumatology 2012, 51 (Suppl. S7), vii18–vii21. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Song, G.G. Diagnostic accuracy of ultrasound in patients with gout: A meta-analysis. Semin. Arthritis Rheum. 2018, 47, 703–709. [Google Scholar] [CrossRef]
- Cipolletta, E.; Di Matteo, A.; Smerilli, G.; Di Carlo, M.; Di Battista, J.; Abhishek, A.; Grassi, W.; Filippucci, E. Ultrasound findings of calcium pyrophosphate deposition disease at metacarpophalangeal joints. Rheumatology 2022, 61, 3997–4005. [Google Scholar] [CrossRef] [PubMed]
- Löffler, C.; Sattler, H.; Peters, L.; Löffler, U.; Uppenkamp, M.; Bergner, R. Distinguishing gouty arthritis from calcium pyrophosphate disease and other arthritides. J. Rheumatol. 2015, 42, 513–520. [Google Scholar] [CrossRef]
- Löffler, C.; Sattler, H.; Löffler, U.; Krämer, B.K.; Bergner, R. Size matters: Observations regarding the sonographic double contour sign in different joint sizes in acute gouty arthritis. Die Größe macht den Unterschied: Beobachtungen zum sonographischen Doppelkonturzeichen in unterschiedlichen Gelenken bei akuter Gichtarthritis. Z. Rheumatol. 2018, 77, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Filippucci, E.; Riveros, M.G.; Georgescu, D.; Salaffi, F.; Grassi, W. Hyaline cartilage involvement in patients with gout and calcium pyrophosphate deposition disease. An. Ultrasound Study Osteoarthr. Cartil. 2009, 17, 178–181. [Google Scholar] [CrossRef]
- Cipolletta, E.; Abhishek, A.; Di Matteo, A.; Grassi, W.; Filippucci, E. Dynamic assessment of the double contour sign by ultrasonography helps to distinguish between gout and calcium pyrophosphate deposition disease. RMD Open 2023, 9, e002940. [Google Scholar] [CrossRef]
- Christiansen, S.N.; Østergaard, M.; Slot, O.; Fana, V.; Terslev, L. Ultrasound for the diagnosis of gout-the value of gout lesions as defined by the Outcome Measures in Rheumatology ultrasound group. Rheumatology 2021, 60, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Wright, S.A.; Filippucci, E.; McVeigh, C.; Grey, A.; McCarron, M.; Grassi, W.; Wright, G.D.; Taggart, A.J. High-resolution ultrasonography of the first metatarsal phalangeal joint in gout: A controlled study. Ann. Rheum. Dis. 2007, 66, 859–864. [Google Scholar] [CrossRef]
- Hammer, H.B.; Karoliussen, L.; Terslev, L.; Haavardsholm, E.A.; Kvien, T.K.; Uhlig, T. Ultrasound shows rapid reduction of crystal depositions during a treat-to-target approach in gout patients: 12-month results from the NOR-Gout study. Ann. Rheum. Dis. 2020, 79, 1500–1505. [Google Scholar] [CrossRef]
- Zayat, A.S.; Ellegaard, K.; Conaghan, P.G.; Terslev, L.; Hensor, E.M.A.; Freeston, J.E.; Emery, P.; Wakefield, R.J. The specificity of ultrasound-detected bone erosions for rheumatoid arthritis. Ann. Rheum. Dis. 2015, 74, 897–903. [Google Scholar] [CrossRef]
- Cipolletta, E.; Smerilli, G.; Di Matteo, A.; Di Battista, J.; Di Carlo, M.; Grassi, W.; Filippucci, E. The sonographic identification of cortical bone interruptions in rheumatoid arthritis: A morphological approach. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211004326. [Google Scholar] [CrossRef]
- Christiansen, S.N.; Østergaard, M.; Slot, O.; Keen, H.; Bruyn, G.A.W.; D’Agostino, M.A.; Terslev, L. Assessing the sensitivity to change of the OMERACT ultrasound structural gout lesions during urate-lowering therapy. RMD Open 2020, 6, e001144. [Google Scholar] [CrossRef] [PubMed]
- Bursill, D.; Taylor, W.J.; Terkeltaub, R.; Abhishek, A.; So, A.K.; Vargas-Santos, A.B.; Gaffo, A.L.; Rosenthal, A.; Tausche, A.-K.; Reginato, A.; et al. Gout, Hyperuricaemia and Crystal-Associated Disease Network (G-CAN) consensus statement regarding labels and definitions of disease states of gout. Ann. Rheum. Dis. 2019, 78, 1592–1600. [Google Scholar] [CrossRef]
- Abhishek, A.; Courtney, P.; Jenkins, W.; Sandoval-Plata, G.; Jones, A.C.; Zhang, W.; Doherty, M. Brief Report: Monosodium Urate Monohydrate Crystal Deposits Are Common in Asymptomatic Sons of Patients with Gout: The Sons of Gout Study. Arthritis Rheumatol. 2018, 70, 1847–1852. [Google Scholar] [CrossRef]
- Cipolletta, E.; Filippucci, E.; Abhishek, A.; Di Battista, J.; Smerilli, G.; Di Carlo, M.; Silveri, F.; De Angelis, R.; Salaffi, F.; Grassi, W.; et al. In patients with acute mono/oligoarthritis, a targeted ultrasound scanning protocol shows great accuracy for the diagnosis of gout and CPPD. Rheumatology 2023, 62, 1493–1500. [Google Scholar] [CrossRef]
- Norkuviene, E.; Petraitis, M.; Apanaviciene, I.; Virviciute, D.; Baranauskaite, A. An optimal ultrasonographic diagnostic test for early gout: A prospective controlled study. J. Int. Med. Res. 2017, 45, 1417–1429. [Google Scholar] [CrossRef] [PubMed]
- Lamers-Karnebeek, F.B.; Van Riel, P.L.; Jansen, T.L. Additive value for ultrasonographic signal in a screening algorithm for patients presenting with acute mono-/oligoarthritis in whom gout is suspected. Clin. Rheumatol. 2014, 33, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Zufferey, P.; Valcov, R.; Fabreguet, I.; Dumusc, A.; Omoumi, P.; So, A. A prospective evaluation of ultrasound as a diagnostic tool in acute microcrystalline arthritis. Arthritis Res. Ther. 2015, 17, 188. [Google Scholar] [CrossRef]
- Pattamapaspong, N.; Vuthiwong, W.; Kanthawang, T.; Louthrenoo, W. Value of ultrasonography in the diagnosis of gout in patients presenting with acute arthritis. Skeletal Radiol. 2017, 46, 759–767. [Google Scholar] [CrossRef]
- Christiansen, S.N.; Østergaard, M.; Slot, O.; Fana, V.; Terslev, L. Retrospective longitudinal assessment of ultrasound gout lesions using the OMERACT semi-quantitative scoring system. Rheumatology 2022, 61, 4711–4721. [Google Scholar] [CrossRef]
- Peiteado, D.; Villalba, A.; Martín-Mola, E.; Balsa, A.; De Miguel, E. Ultrasound sensitivity to changes in gout: A longitudinal study after two years of treatment. Clin. Exp. Rheumatol. 2017, 35, 746–751. [Google Scholar] [PubMed]
- Ebstein, E.; Forien, M.; Norkuviene, E.; Richette, P.; Mouterde, G.; Daien, C.; Ea, H.-K.; Brière, C.; Lioté, F.; Petraitis, M.; et al. Ultrasound evaluation in follow-up of urate-lowering therapy in gout: The USEFUL study. Rheumatology 2019, 58, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Bhadu, D.; Das, S.K.; Wakhlu, A.; Dhakad, U.; Sharma, M. Ultrasonographic detection of double contour sign and hyperechoic aggregates for diagnosis of gout: Two sites examination is as good as six sites examination. Int. J. Rheum. Dis. 2018, 21, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Yang, M.; Wang, H. Diagnostic value of ultrasound versus dual-energy computed tomography in patients with different stages of acute gouty arthritis. Clin. Rheumatol. 2020, 39, 1649–1653. [Google Scholar] [CrossRef] [PubMed]
- Cipolletta, E.; Di Battista, J.; Di Carlo, M.; Di Matteo, A.; Salaffi, F.; Grassi, W.; Filippucci, E. Sonographic estimation of monosodium urate burden predicts the fulfillment of the 2016 remission criteria for gout: A 12-month study. Arthritis Res. Ther. 2021, 23, 185. [Google Scholar] [CrossRef] [PubMed]
- Cipolletta, E.; Abhishek, A.; Di Battista, J.; Grassi, W.; Filippucci, E. Ultrasonography in the prediction of gout flares: A 12-month prospective observational study. Rheumatology 2023, 62, 1108–1116. [Google Scholar] [CrossRef]
- Zou, Z.; Yang, M.; Wang, Y.; Zhang, B. Association of urate deposition shown by ultrasound and frequent gout attacks. Zusammenhang zwischen sonographisch darstellbarer Uratablagerung und häufigen Gichtanfällen. Z. Rheumatol. 2021, 80, 565–569. [Google Scholar] [CrossRef]
- Ebstein, E.; Forien, M.; Norkuviene, E.; Richette, P.; Mouterde, G.; Daien, C.; Ea, H.-K.; Brière, C.; Lioté, F.; Petraitis, M.; et al. UltraSound evaluation in follow-up of urate-lowering therapy in gout phase 2 (USEFUL-2): Duration of flare prophylaxis. Jt. Bone Spine 2020, 87, 647–651. [Google Scholar] [CrossRef]
- Perez-Ruiz, F.; Martin, I.; Canteli, B. Ultrasonographic measurement of tophi as an outcome measure for chronic gout. J. Rheumatol. 2007, 34, 1888–1893. [Google Scholar]
- Pascart, T.; Grandjean, A.; Norberciak, L.; Ducoulombier, V.; Motte, M.; Luraschi, H.; Vandecandelaere, M.; Godart, C.; Houvenagel, E.; Namane, N.; et al. Ultrasonography and dual-energy computed tomography provide different quantification of urate burden in gout: Results from a cross-sectional study. Arthritis Res. Ther. 2017, 19, 171. [Google Scholar] [CrossRef] [PubMed]
- Modjinou, D.V.; Krasnokutsky, S.; Gyftopoulos, S.; Pike, V.C.; Karis, E.; Keenan, R.T.; Lee, K.; Crittenden, D.B.; Samuels, J.; Pillinger, M.H. Comparison of dual-energy CT, ultrasound and surface measurement for assessing tophus dissolution during rapid urate debulking. Clin. Rheumatol. 2017, 36, 2101–2107. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Image Acquisition |
|
|
|
|
|
| US machine settings |
|
|
|
|
| Disease State as Proposed by the G-CAN [34] | Clinical Question for US |
|---|---|
| Preclinical states | To provide evidence of MSU crystal deposition in asymptomatic hyperuricemia |
| Clinical states | To establish a diagnosis of gout during inter-critical phases by the visualisation of MSU deposits and by guiding the aspiration of synovial fluid |
| To evaluate the burden of MSU crystal deposits, subclinical inflammation, and structural damage | |
| To monitor the efficacy of treatments on crystal deposition, structural damage, and subclinical inflammation | |
| Gout flares | To diagnose gout during the first or recurrent gout flare |
| To recognise painful musculoskeletal conditions not related to gout | |
| To treat gout flares by guiding local injections |
| Authors | Anatomical Areas Evaluated | Bilateral Assessment | US Findings | OMERACT Definitions | RS | SE | SP | PPV | NPV |
|---|---|---|---|---|---|---|---|---|---|
| Diagnostic purposes in intercritical gout | |||||||||
| Peiteado et al. [14] | two joints: MTP1 joint (dorsal, medial, and plantar aspects) and knee (medial and lateral recesses and hyaline cartilage of the trochlea) | Y | Hyperechoic cloudy areas DC sign | N | SFA | 97% | NR | NR | NR |
| Naredo et al. [15] | one joint: radiocarpal joint two tendons: patellar tendon and triceps tendon three articular cartilages: I metatarsal head dorsal and plantar cartilage, talar cartilage, and either second metacarpal cartilage (dorsal aspect) or femoral condyle cartilage | Y | Tophi DC sign Hyperechoic linear bands | N | SFA | 84.6% | 83.3% | 91.7% | 71.4% |
| four joints: radiocarpal joint, midcarpal joint, MTP1 joint and knee two tendons: patellar tendon and triceps tendon three articular cartilages: I metatarsal head dorsal and plantar cartilage, talar cartilage, and either second metacarpal cartilage (dorsal aspect) or femoral condyle cartilage | Y | 94.5% | 71.4% | 87.8% | 85.7% | ||||
| two tendons: patellar tendon and triceps tendon | Y | 46.2% | 97.6% | 97.7% | 45.6% | ||||
| Norkuviene et al. [37] | two joints: MTP1 joint and ankle | Y | Tophi DC sign | N | SFA | 84.0% | 81.0% | NR | NR |
| Diagnostic purposes in acute mono/oligoarthritis | |||||||||
| Lamers-Karnebeek et al. [38] | three joints: the most inflamed joint, MTP1 joint and knee (when the most inflamed joint was MTP1j or knee the ankle should be included) | Y | Tophi DC sign Snowstorm sign | N | SFA | 96% | 68% | 74% | 95% |
| Zufferey et al. [39] | one joint: the symptomatic one | N | Tophi, DC sign Aggregates | Y | SFA | 60% | 92% | 92% | 62% |
| four joints: symptomatic one + knee, ankle and the MTP1 joint | Y | Y | SFA | 84% | 78% | 82% | 77% | ||
| Pattamapaspong et al. [40] | one joint: the symptomatic one | N | Tophi, DC sign Aggregates | Y | SFA | 75% | 89% | 91% | 71% |
| Christiansen et al. [28] | six joints: MTP1–5 joints (for tophi and DC) and knee (for DC) two tendons: peroneus tendons | Y | Tophi, DC sign | Y | SFA | 93% | / | / | / |
| Cipolletta et al. [36] | Five joints: knees, MTP1 joints (for tophi and DC), plus the symptomatic joint One tendon: patellar tendon | Y | Tophi, DC sign | Y | SFA | 91% | 91% | 71% | 98% |
| Monitoring treatment efficacy and prognostic purposes | |||||||||
| Christiansen et al. [41] | Three joints: MTP1 joint (for tophi and DC), MTP2 joint, and knee (for DC) Two tendons: peroneal tendons and distal portion of patellar tendon (for tophi) | Y | Tophi, DC sign | Y | SFA | / | / | / | / |
| Peiteado [42] and Ebstein [43] | Two joints: MTP1 joint and knee (for tophi and DC) | Y | Tophi, DC sign | Y | SFA | / | / | / | / |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filippucci, E.; Cipolletta, E.; Sirotti, S.; Filippou, G. Optimising the Use of Ultrasound in Gout: A Review from the Ground Up. Gout Urate Cryst. Depos. Dis. 2024, 2, 86-100. https://doi.org/10.3390/gucdd2020009
Filippucci E, Cipolletta E, Sirotti S, Filippou G. Optimising the Use of Ultrasound in Gout: A Review from the Ground Up. Gout, Urate, and Crystal Deposition Disease. 2024; 2(2):86-100. https://doi.org/10.3390/gucdd2020009
Chicago/Turabian StyleFilippucci, Emilio, Edoardo Cipolletta, Silvia Sirotti, and Georgios Filippou. 2024. "Optimising the Use of Ultrasound in Gout: A Review from the Ground Up" Gout, Urate, and Crystal Deposition Disease 2, no. 2: 86-100. https://doi.org/10.3390/gucdd2020009