
FDG PET/CT as a Tool for Early Detection of Bleomycin-Induced Pulmonary Toxicity

 , ,
, ,
Abstract
:1. Introduction
2. Results
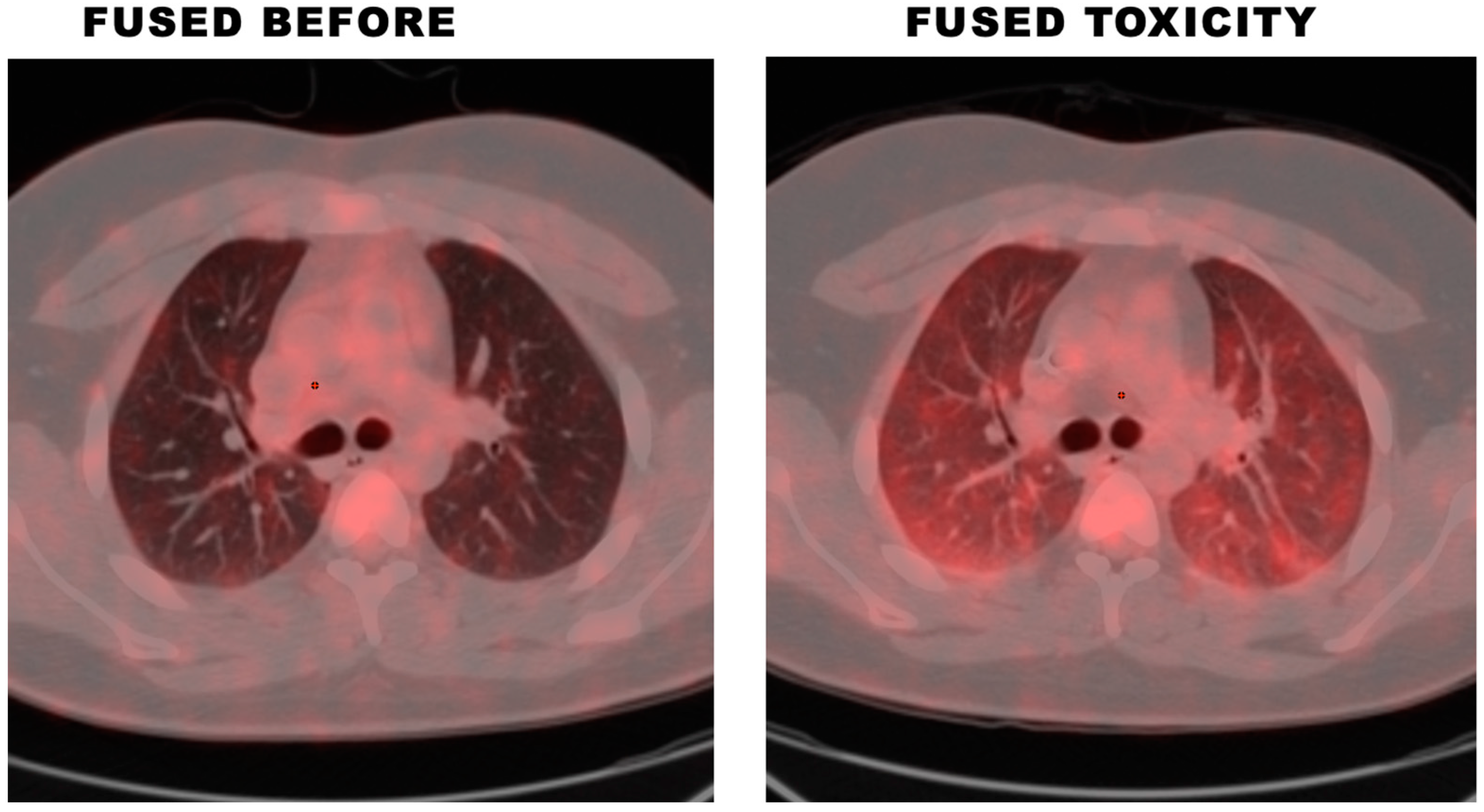
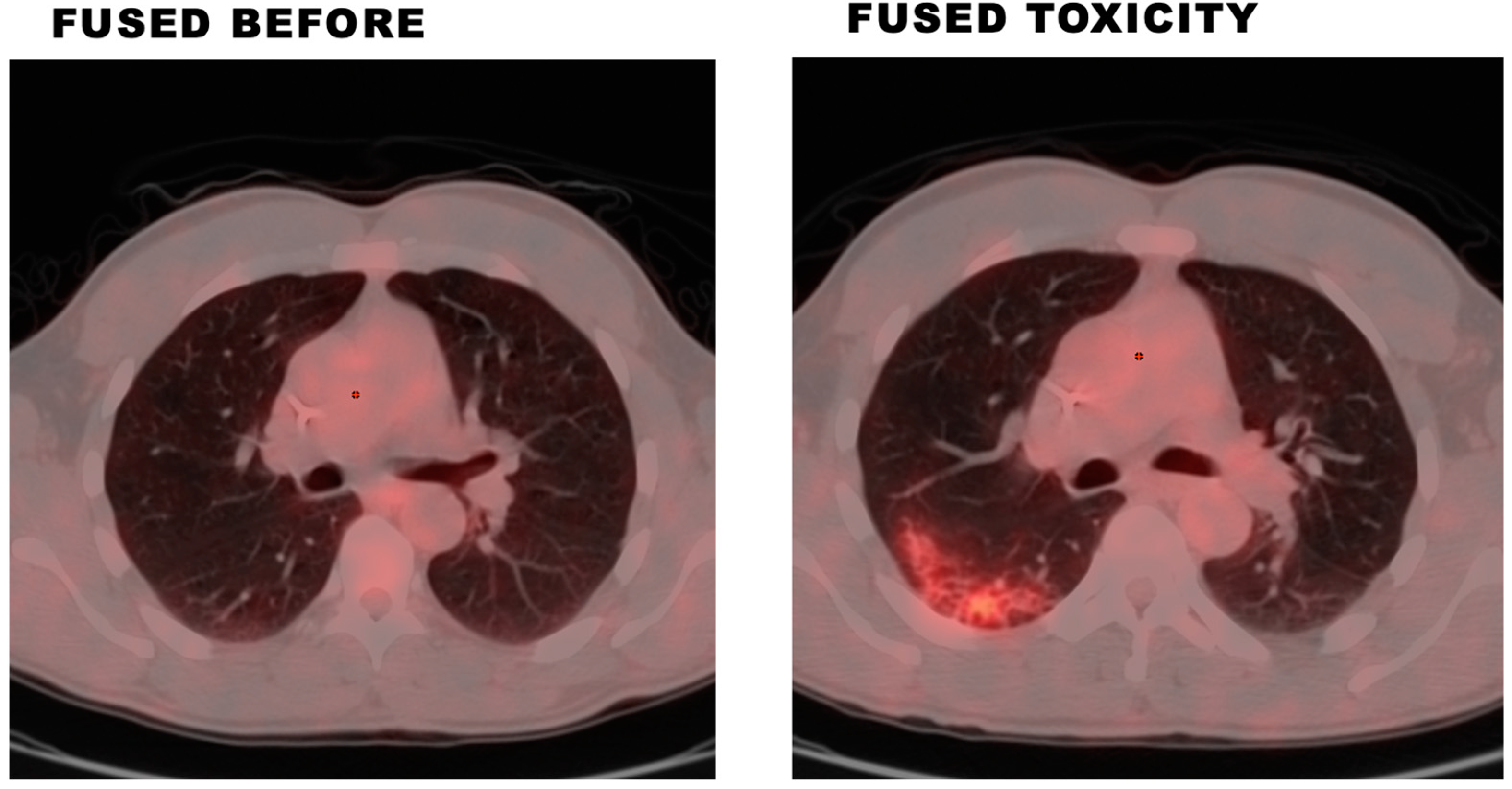
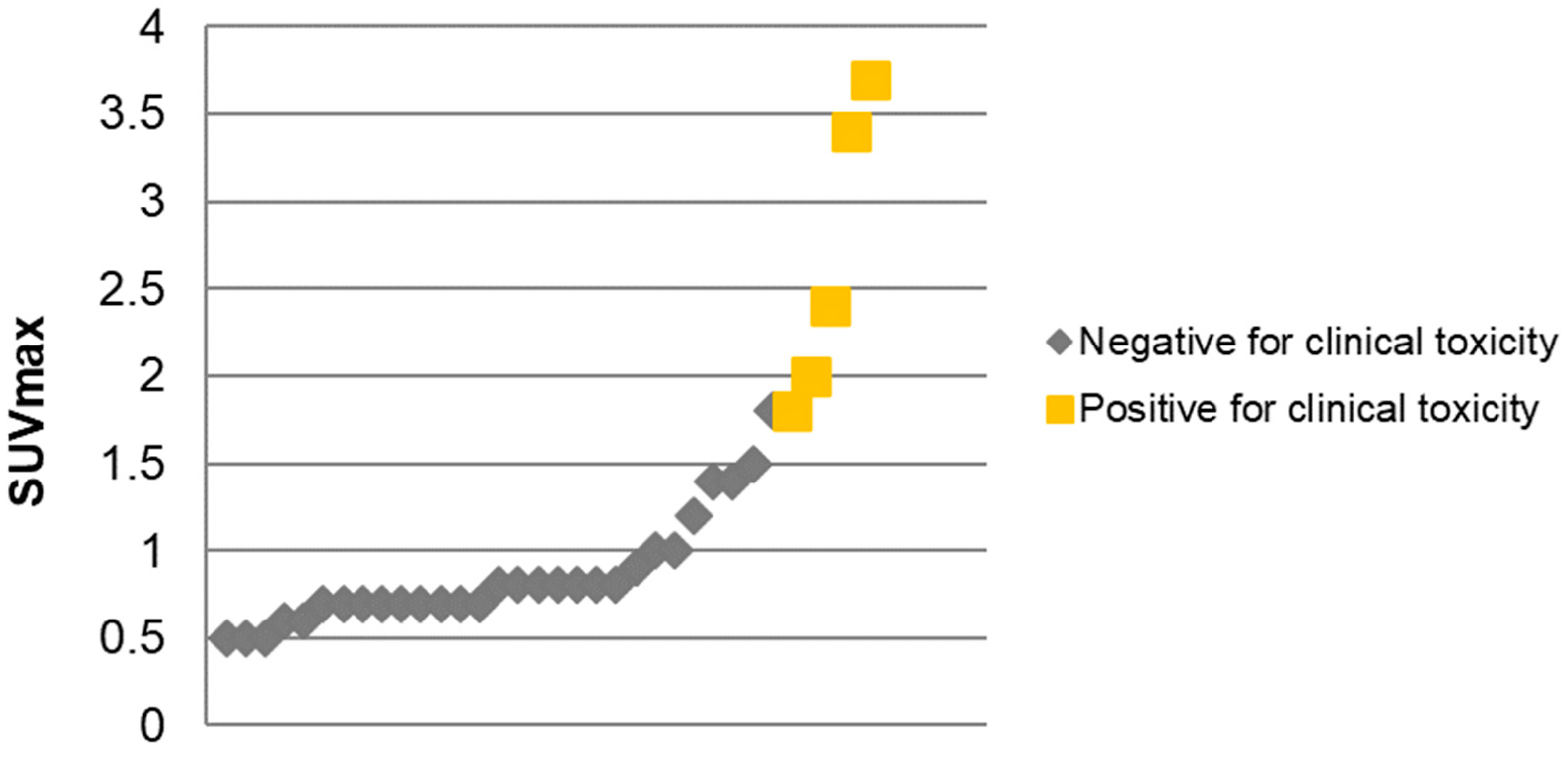
2.1. Cohort 1—Clinical BPT and 18F-FDG PET/CT Findings
2.2. Cohort 2—Demographics and Disease Characteristics
2.3. Cohort 2—Clinical BPT
2.4. Cohort 2—Risk Factors of Clinical BPT
3. Discussion
4. Materials and Methods
4.1. Data Collection
4.2. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martin, W.G.; Ristow, K.M.; Habermann, T.M.; Colgan, J.P.; Witzig, T.E.; Ansell, S.M. Bleomycin pulmonary toxicity has a negative impact on the outcome of patients with Hodgkin’s lymphoma. J. Clin. Oncol. 2005, 23, 7614–7620. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, A.; Vander Els, N.; Straus, D.J.; Gomez, E.G.; Leung, D.; Portlock, C.S.; Yahalom, J. Effect of ABVD chemotherapy with and without mantle or mediastinal irradiation on pulmonary function and symptoms in early-stage Hodgkin’s disease. J. Clin. Oncol. 1996, 14, 1297–1305. [Google Scholar] [CrossRef]
- Reinert, T.; Baldotto, C.S.d.R.; Nunes, F.A.P.; Scheliga, A.A.d.S. Bleomycin-Induced Lung Injury. J. Cancer Res. 2013, 2013, 480608. [Google Scholar] [CrossRef] [Green Version]
- Azambuja, E.; Fleck, J.F.; Batista, R.G.; Menna Barreto, S.S. Bleomycin lung toxicity: Who are the patients with increased risk? Pulm. Pharm. 2005, 18, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Blum, R.H.; Carter, S.K.; Agre, K. A clinical review of bleomycin—A new antineoplastic agent. Cancer 1973, 31, 903–914. [Google Scholar] [CrossRef] [PubMed]
- Cooper Jr, J.A.D.; White, D.A.; Matthay, R.A. Drug-induced pulmonary disease: Part 1: Cytotoxic drugs. Am. Rev. Respir. Dis. 1986, 133, 321–340. [Google Scholar]
- O’Sullivan, J.M.; Huddart, R.A.; Norman, A.R.; Nicholls, J.; Dearnaley, D.P.; Horwich, A. Predicting the risk of bleomycin lung toxicity in patients with germ-cell tumours. Ann. Oncol. 2003, 14, 91–96. [Google Scholar] [CrossRef]
- Jules-Elysee, K.; White, D.A. Bleomycin-induced pulmonary toxicity. Clin. Chest Med. 1990, 11, 1–20. [Google Scholar] [CrossRef]
- Samuels, M.L.; Johnson, D.E.; Holoye, P.Y.; Lanzotti, V.J. Large-dose bleomycin therapy and pulmonary toxicity. A possible role of prior radiotherapy. Jama 1976, 235, 1117–1120. [Google Scholar] [CrossRef]
- Simpson, A.; Paul, J.; Graham, J.; Kaye, S. Fatal bleomycin pulmonary toxicity in the west of Scotland 1991-95: A review of patients with germ cell tumours. Br. J. Cancer 1998, 78, 1061–1066. [Google Scholar] [CrossRef] [Green Version]
- Sleijfer, S. Bleomycin-induced pneumonitis. Chest 2001, 120, 617–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piguet, P.F.; Collart, M.A.; Grau, G.E.; Kapanci, Y.; Vassalli, P. Tumor necrosis factor/cachectin plays a key role in bleomycin-induced pneumopathy and fibrosis. J. Exp. Med. 1989, 170, 655–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phan, S.H.; Kunkel, S.L. Lung cytokine production in bleomycin-induced pulmonary fibrosis. Exp. Lung Res. 1992, 18, 29–43. [Google Scholar] [CrossRef]
- Lauritsen, J.; Kier, M.G.; Bandak, M.; Mortensen, M.S.; Thomsen, F.B.; Mortensen, J.; Daugaard, G. Pulmonary Function in Patients With Germ Cell Cancer Treated With Bleomycin, Etoposide, and Cisplatin. J. Clin. Oncol. 2016, 34, 1492–1499. [Google Scholar] [CrossRef] [PubMed]
- White, D.A.; Stover, D.E. Severe bleomycin-induced pneumonitis. Clinical features and response to corticosteroids. Chest 1984, 86, 723–728. [Google Scholar] [CrossRef]
- Rigacci, L.; Vitolo, U.; Nassi, L.; Merli, F.; Gallamini, A.; Pregno, P.; Alvarez, I.; Salvi, F.; Sancetta, R.; Castagnoli, A.; et al. Positron emission tomography in the staging of patients with Hodgkin’s lymphoma. A prospective multicentric study by the Intergruppo Italiano Linfomi. Ann. Hematol. 2007, 86, 897–903. [Google Scholar] [CrossRef]
- Gallamini, A.; Hutchings, M.; Rigacci, L.; Specht, L.; Merli, F.; Hansen, M.; Patti, C.; Loft, A.; Di Raimondo, F.; D’Amore, F.; et al. Early Interim 2-[18F]Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography Is Prognostically Superior to International Prognostic Score in Advanced-Stage Hodgkin’s Lymphoma: A Report From a Joint Italian-Danish Study. J. Clin. Oncol. 2007, 25, 3746–3752. [Google Scholar] [CrossRef] [Green Version]
- Buchler, T.; Bomanji, J.; Lee, S.M. FDG-PET in bleomycin-induced pneumonitis following ABVD chemotherapy for Hodgkin’s disease-a useful tool for monitoring pulmonary toxicity and disease activity. Haematologica 2007, 92, e120–e121. [Google Scholar] [CrossRef] [Green Version]
- Connerotte, T.; Lonneux, M.; de Meeûs, Y.; Hermans, C.; Vekemans, M.-C.; Ferrant, A.; Van Den Neste, E. Use of 2-[18F]fluoro-2-deoxy-D-glucose positron emission tomography in the early diagnosis of asymptomatic bleomycin-induced pneumonitis. Ann. Hematol. 2008, 87, 943–945. [Google Scholar] [CrossRef]
- Rohr, L.; Klaeser, B.; Joerger, M.; Kluckert, T.; Cerny, T.; Gillessen, S. Increased Pulmonary FDG Uptake in Bleomycin-Associated Pneumonitis. Oncol. Res. Treat. 2007, 30, 320–323. [Google Scholar] [CrossRef]
- Hain, S.F.; Beggs, A.D. Bleomycin-induced alveolitis detected by FDG positron emission tomography. Clin. Nucl. Med. 2002, 27, 522–523. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, J.; Arrossi, A.V.; Yoon, J.K.; Wu, G.; Neumann, D.R. FDG positron emission tomography/computerized tomography features of bleomycin-induced pneumonitis. J. Thorac. Imaging 2006, 21, 228–230. [Google Scholar] [CrossRef] [PubMed]
- den Hollander, M.W.; Westerink, N.D.; Lubberts, S.; Bongaerts, A.H.; Wolf, R.F.; Altena, R.; Nuver, J.; Oosting, S.F.; de Vries, E.G.; Walenkamp, A.M.; et al. Bleomycin-Induced Pulmonary Changes on Restaging Computed Tomography Scans in Two Thirds of Testicular Cancer Patients Show No Correlation With Fibrosis Markers. Oncologist 2016, 21, 995–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falay, O.; Öztürk, E.; Bölükbaşı, Y.; Gümüş, T.; Örnek, S.; Özbalak, M.; Çetiner, M.; Demirkol, O.; Ferhanoğlu, B. Use of fluorodeoxyglucose positron emission tomography for diagnosis of bleomycin-induced pneumonitis in Hodgkin lymphoma. Leuk. Lymphoma 2017, 58, 1114–1122. [Google Scholar] [CrossRef]
- Duggan, D.B.; Petroni, G.R.; Johnson, J.L.; Glick, J.H.; Fisher, R.I.; Connors, J.M.; Canellos, G.P.; Peterson, B.A. Randomized comparison of ABVD and MOPP/ABV hybrid for the treatment of advanced Hodgkin’s disease: Report of an intergroup trial. J. Clin. Oncol. 2003, 21, 607–614. [Google Scholar] [CrossRef]
- Stamatoullas, A.; Brice, P.; Bouabdallah, R.; Mareschal, S.; Camus, V.; Rahal, I.; Franchi, P.; Lanic, H.; Tilly, H. Outcome of patients older than 60 years with classical Hodgkin lymphoma treated with front line ABVD chemotherapy: Frequent pulmonary events suggest limiting the use of bleomycin in the elderly. Br. J. Haematol. 2015, 170, 179–184. [Google Scholar] [CrossRef]
- Tayshetye, P.; Padhi, P.; Rao, R.; Sklyar, T.Y.; Chilkulwar, A.; Miller, R.; Tang, A.; Mao, S. Bleomycin-induced pulmonary toxicity: A retrospective review of incidence and risk factors. J. Clin. Oncol. 2018, 36, e16532. [Google Scholar] [CrossRef]
- Iacovino, J.R.; Leitner, J.; Abbas, A.K.; Lokich, J.J.; Snider, G.L. Fatal pulmonary reaction from low doses of bleomycin. An idiosyncratic tissue response. JAMA 1976, 235, 1253–1255. [Google Scholar] [CrossRef]
- Wilson, K.S.; Worth, A.; Richards, A.G.; Ford, H.S. Low-dose bleomycin lung. Med. Pediatr. Oncol. 1982, 10, 283–288. [Google Scholar] [CrossRef]
- Bastion, Y.; Coiffier, B. Pulmonary toxicity of bleomycin: Is G-CSF a risk factor? Lancet 1994, 344, 474. [Google Scholar] [CrossRef]
- Azoulay, E.; Herigault, S.; Levame, M.; Brochard, L.; Schlemmer, B.; Harf, A.; Delclaux, C. Effect of granulocyte colony-stimulating factor on bleomycin-induced acute lung injury and pulmonary fibrosis. Crit. Care Med. 2003, 31, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.L.; Atenafu, E.G.; Tsang, R.; Kukreti, V.; Marras, T.K.; Crump, M.; Kuruvilla, J. Bleomycin pulmonary toxicity does not adversely affect the outcome of patients with Hodgkin lymphoma. Leuk. Lymphoma 2017, 58, 2607–2614. [Google Scholar] [CrossRef] [PubMed]
- Saxman, S.B.; Nichols, C.R.; Einhorn, L.H. Pulmonary toxicity in patients with advanced-stage germ cell tumors receiving bleomycin with and without granulocyte colony stimulating factor. Chest 1997, 111, 657–660. [Google Scholar] [CrossRef] [PubMed]
- Fosså, S.D.; Kaye, S.B.; Mead, G.M.; Cullen, M.; de Wit, R.; Bodrogi, I.; van Groeningen, C.J.; De Mulder, P.H.; Stenning, S.; Lallemand, E.; et al. Filgrastim during combination chemotherapy of patients with poor-prognosis metastatic germ cell malignancy. European Organization for Research and Treatment of Cancer, Genito-Urinary Group, and the Medical Research Council Testicular Cancer Working Party, Cambridge, United Kingdom. J. Clin. Oncol. 1998, 16, 716–724. [Google Scholar] [CrossRef]
- Dirix, L.Y.; Schrijvers, D.; Druwe, P.; Van den Brande, J.; Verhoeven, D.; Van Oosterom, A.T. Pulmonary toxicity and bleomycin. Lancet 1994, 344, 56. [Google Scholar] [CrossRef]
- Jóna, Á.; Miltényi, Z.; Ujj, Z.; Garai, I.; Szilasi, M.; Illés, Á. Late pulmonary complications of treating Hodgkin lymphoma: Bleomycin-induced toxicity. Expert. Opin. Drug. Saf. 2014, 13, 1291–1297. [Google Scholar] [CrossRef]
- Macann, A.; Bredenfeld, H.; Müller, R.P.; Diehl, V.; Engert, A.; Eich, H.T. Radiotherapy does not influence the severe pulmonary toxicity observed with the administration of gemcitabine and bleomycin in patients with advanced-stage Hodgkin’s lymphoma treated with the BAGCOPP regimen: A report by the German Hodgkin’s Lymphoma Study Group. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 161–165. [Google Scholar] [CrossRef]
- Higa, G.M.; AlKhouri, N.; Auber, M.L. Elevation of the erythrocyte sedimentation rate precedes exacerbation of bleomycin-induced pulmonary toxicity: Report of two cases and review of literature. Pharmacotherapy 1997, 17, 1315–1321. [Google Scholar] [CrossRef]
- Maruyama, Y.; Sadahira, T.; Araki, M.; Mitsui, Y.; Wada, K.; Edamura, K.; Kobayashi, Y.; Watanabe, M.; Watanabe, T.; Nasu, Y. Comparison of the predictive value among inflammation-based scoring systems for bleomycin pulmonary toxicity in patients with germ cell tumors. Int. J. Urol. 2019, 26, 813–819. [Google Scholar] [CrossRef]
- Uzel, I.; Ozguroglu, M.; Uzel, B.; Kaynak, K.; Demirhan, O.; Akman, C.; Oz, F.; Yaman, M. Delayed onset bleomycin-induced pneumonitis. Urology 2005, 66, 195. [Google Scholar] [CrossRef]
- White, D.A.; Schwartzberg, L.S.; Kris, M.G.; Bosl, G.J. Acute chest pain syndrome during bleomycin infusions. Cancer 1987, 59, 1582–1585. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient No. | Radiation Field | Radiation Dose (Gy) |
|---|---|---|
| 2 | Mediastinum and bilateral supraclavicular area | 30 |
| 5 | Whole lung irradiation | 10.5 * |
| 9 | Mediastinum | 30.6 |
| 10 | Right neck and retrosternal nodes | 27 |
| 11 | Mantle field | 30.6 |
| Negative for Clinical Toxicity | Positive for Clinical Toxicity | |
|---|---|---|
| N | 6 | 5 |
| Age (years) | 40.7 ± 15.4 | 40.6 ± 20.1 |
| Gender (Males/Females) | 5/1 | 3/2 |
| Mean SUVmax of Lungs | 0.86 (CI 0.4–1.9) | 2.66 (CI 1.8–3.7) |
| Demographics | |||
|---|---|---|---|
| Age, median (range) | 30 (19–68) years | ||
| Males, n (%) | 18/25 (72%) | ||
| ECOG PS a, n (%) | 0 | 15/23 (65%) | |
| 1 | 8/23 (35%) | ||
| DISEASE CHARACTERISTICS | |||
| Bulky disease a, n (%) | 3/24 (12.5%) | ||
| B symptoms, n (%) | 13/25 (52%) | ||
| Stage a, n (%) | I | 1/24 (4.17%) | |
| II | 13/24 (54.17%) | ||
| III | 6/24 (25%) | ||
| IV | 4/24 (16.67%) | ||
| Histology, n (%) | Classical | 8/25 (32%) | |
| Nodular lymphocyte predominant | 2/25 (8%) | ||
| Nodular sclerosing | 14/25 (56%) | ||
| Nodular sclerosing/Mixed cellularity overlap | 1/25 (4%) | ||
| Albumin, median (range) | 4.1 (3–4.9) g/dL | ||
| Hemoglobin, median (range) | 12.5 (6.9–16.3) mg/dL | ||
| ESR, median (range) | 38 (2–106) mm/h | ||
| ALC, median (range) | 1495.5 (1.69–2292)/µL | ||
| At Diagnosis | N (%) | Clinical BPT | No Clinical BPT | p Value | |
|---|---|---|---|---|---|
| Gender | Females | 7/25 (28%) | 3 (42.86%) | 4 (57.14%) | 1 |
| Males | 18/25 (72%) | 6 (37.5%) | 10 (62.5%) | ||
| Stage a | I | 1/24 (4.17%) | 1 (100%) | 0 (0%) | 0.6003 |
| II | 12/24 (54.17%) | 4 (33.33%) | 8 (66.67%) | ||
| III | 5/24 (25%) | 2 (40%) | 3 (60%) | ||
| IV | 4/24 (16.67%) | 2 (50%) | 2 (50%) | ||
| Histology | Classical | 8/25 (32%) | 3 (42.86%) | 4 (57.14%) | 0.5110 |
| Nodular lymphocyte predominant | 2/25 (8%) | 1 (100%) | 0 (0%) | ||
| Nodular sclerosing | 14/25 (56%) | 5 (33.33%) | 9 (66.67%) | ||
| Nodular sclerosing/Mixed cellularity overlap | 1/25 (4%) | 0 (0%) | 1 (100%) | ||
| Bulky disease a | No | 21/24 (87.5%) | 7 (35%) | 13 (65%) | 0.6791 |
| Yes | 3/24 (12.5%) | 2 (66.67%) | 1 (33.33%) | ||
| History of lung disease | No | 23/25 (92%) | 7 (33.33%) | 14 (66.67%) | 0.2767 |
| Yes | 2/25 (8%) | 2 (100%) | 0 (0%) | ||
| History of lung radiation | No | 21/25 (84%) | 8 (42.11%) | 11 (57.89%) | 0.9414 |
| Yes | 4/25 (16%) | 1 (25%) | 3 (75%) | ||
| Prior G-CSF exposure a | No | 18/21 (85.71%) | 7 (38.89%) | 11 (61.11%) | 1 |
| Yes | 3/21 (14.29%) | 1 (33.33%) | 2 (66.67%) | ||
| Steroid use a | No | 1/4 (25%) | 1 (100%) | 0 (0%) | - |
| Yes | 3/4 (75%) | 3 (100%) | 0 (0%) | ||
| Age, years | mean (SD) | 25/25 (100%) | 36.11 (15.41) | 33.07 (12) | 0.6235 |
| Albumin, g/dL | mean (SD) | 25/25 (100%) | 3.92 (0.51) | 3.97 (0.6) | 0.8572 |
| Hemoglobin, g/dL | mean (SD) | 25/25 (100%) | 10.87 (2.34) | 13.29 (2.58) | 0.0370 * |
| ESR, mm/h | mean (SD) | 25/25 (100%) | 63.62 (31.03) | 30.18 (27.44) | 0.0289 * |
| ALC, /µL | mean (SD) | 25/25 (100%) | 1042 (556.39) | 1449.89 (785.02) | 0.1798 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaikh, H.; Omer, Z.; Jandarov, R.A.; McBee, M.P.; Scheler, J.; Mahoney, B.; Latif, T. FDG PET/CT as a Tool for Early Detection of Bleomycin-Induced Pulmonary Toxicity. Lymphatics 2023, 1, 45-54. https://doi.org/10.3390/lymphatics1010006
Shaikh H, Omer Z, Jandarov RA, McBee MP, Scheler J, Mahoney B, Latif T. FDG PET/CT as a Tool for Early Detection of Bleomycin-Induced Pulmonary Toxicity. Lymphatics. 2023; 1(1):45-54. https://doi.org/10.3390/lymphatics1010006
Chicago/Turabian StyleShaikh, Hira, Zulfa Omer, Roman A. Jandarov, Morgan P. McBee, Jennifer Scheler, Bruce Mahoney, and Tahir Latif. 2023. "FDG PET/CT as a Tool for Early Detection of Bleomycin-Induced Pulmonary Toxicity" Lymphatics 1, no. 1: 45-54. https://doi.org/10.3390/lymphatics1010006