
Mapping Dementia Care Technology: Tailored Digital Solutions across Stages
 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Literature Search
2.1. Method
2.2. Results Gained from the Literature and Changes Made to the Infographic
2.2.1. Screen to Screen
2.2.2. Medicine Dispenser
2.2.3. Key Safe or Electronic Lock
2.2.4. Communication Platform
2.2.5. Lifestyle Monitoring
2.2.6. Accident Notification/Prevention
2.2.7. GPS
2.2.8. Apps and Devices
2.2.9. Social Robots
2.2.10. Robot Pets
2.2.11. Smart Diapers
3. Expert Interviews
3.1. Participants
3.2. Study Protocol
3.3. Data Analysis
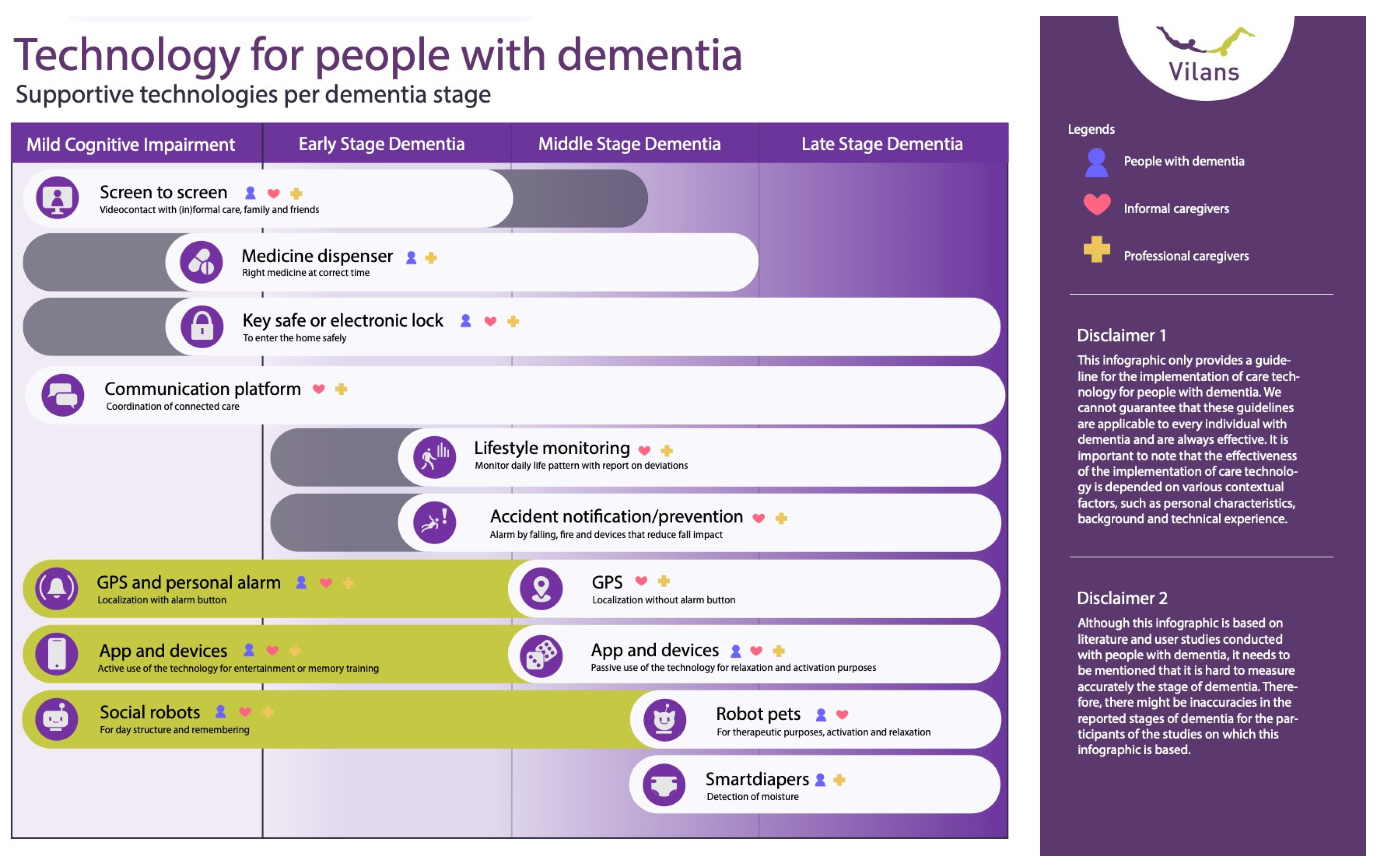
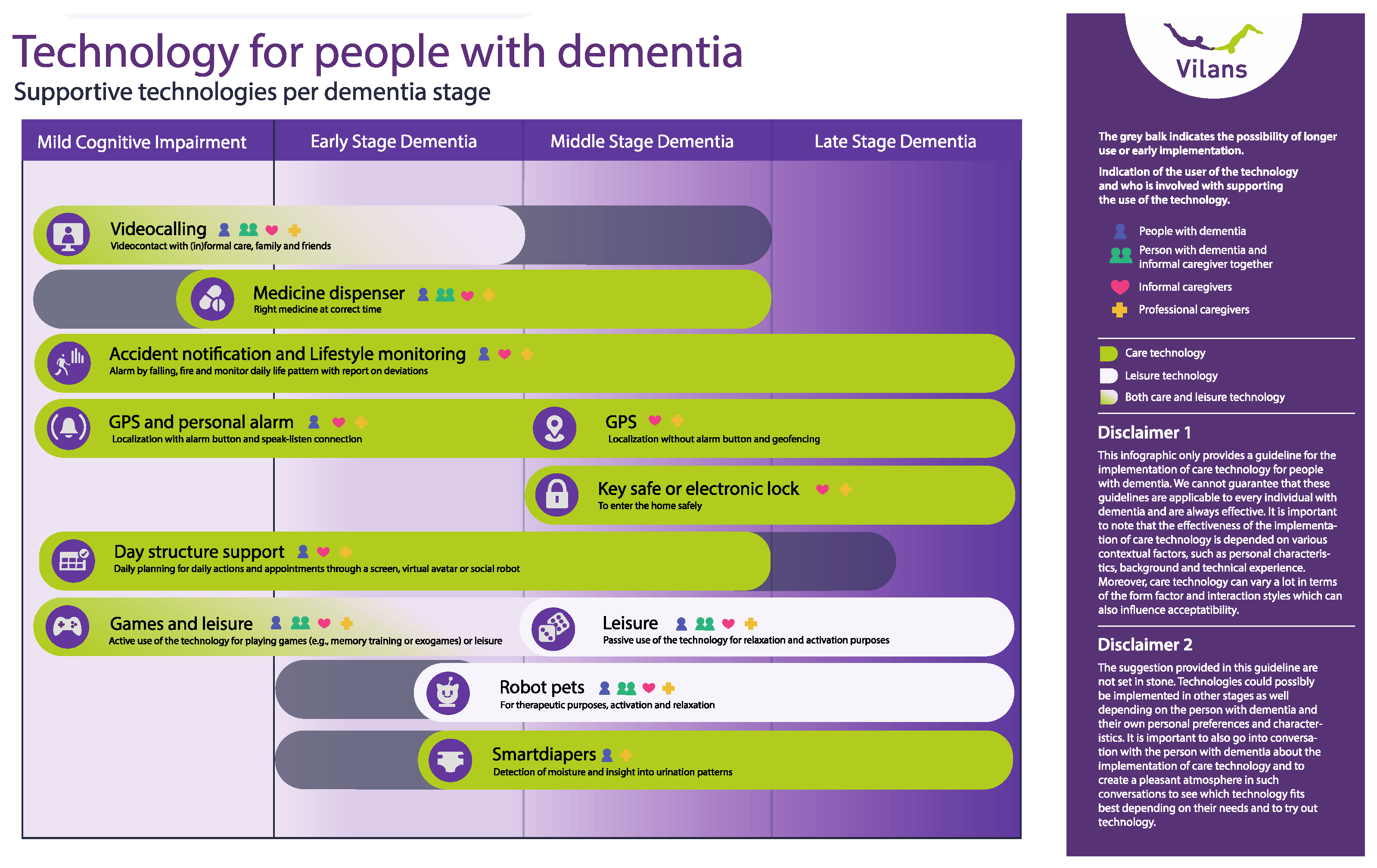
3.4. Revision of the Infographic
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Assistive Technology. Available online: https://www.who.int/news-room/fact-sheets/detail/assistive-technology (accessed on 2 April 2024).
- WHO Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 2 April 2024).
- Rogers, W.A.; Mitzner, T.L. Envisioning the Future for Older Adults: Autonomy, Health, Well-Being, and Social Connectedness with Technology Support. Futures 2017, 87, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Gaugler, J.E.; Zmora, R.; Peterson, C.M.; Mitchell, L.L.; Jutkowitz, E.; Duval, S. What Interventions Keep Older People out of Nursing Homes? A Systematic Review and Meta-analysis. J. Am. Geriatr. Soc. 2023, 71, 3609–3621. [Google Scholar] [CrossRef] [PubMed]
- Jutai, J.W.; Tuazon, J.R. The Role of Assistive Technology in Addressing Social Isolation, Loneliness and Health Inequities among Older Adults during the COVID-19 Pandemic. Disabil. Rehabil. Assist. Technol. 2022, 17, 248–259. [Google Scholar] [CrossRef]
- Ienca, M.; Fabrice, J.; Elger, B.; Caon, M.; Scoccia Pappagallo, A.; Kressig, R.W.; Wangmo, T. Intelligent Assistive Technology for Alzheimer’s Disease and Other Dementias: A Systematic Review. J. Alzheimer’s Dis. 2017, 56, 1301–1340. [Google Scholar] [CrossRef] [PubMed]
- Bodenheimer, T. Patient Self-Management of Chronic Disease in Primary Care. JAMA 2002, 288, 2469. [Google Scholar] [CrossRef]
- de Haes, H. Dilemmas in Patient Centeredness and Shared Decision Making: A Case for Vulnerability. Patient Educ. Couns. 2006, 62, 291–298. [Google Scholar] [CrossRef]
- Nap, H.H.; Buimer, H.; Wouters, E. Value-Based EHealth: Lifestyle Monitoring. Gerontechnology 2020, 19, 1–40. [Google Scholar] [CrossRef]
- Norman, C.D.; Skinner, H.A. EHealth Literacy: Essential Skills for Consumer Health in a Networked World. J. Med. Internet Res. 2006, 8, e9. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Wherton, J.; Papoutsi, C.; Lynch, J.; Hughes, G.; A’Court, C.; Hinder, S.; Fahy, N.; Procter, R.; Shaw, S. Beyond Adoption: A New Framework for Theorizing and Evaluating Nonadoption, Abandonment, and Challenges to the Scale-Up, Spread, and Sustainability of Health and Care Technologies. J. Med. Internet Res. 2017, 19, e367. [Google Scholar] [CrossRef]
- Getson, C.; Nejat, G. The Adoption of Socially Assistive Robots for Long-Term Care: During COVID-19 and in a Post-Pandemic Society. Healthc. Manag. Forum 2022, 35, 301–309. [Google Scholar] [CrossRef]
- Rantanen, T.; Leppälahti, T.; Porokuokka, J.; Heikkinen, S. Impacts of a Care Robotics Project on Finnish Home Care Workers’ Attitudes towards Robots. Int. J. Environ. Res. Public Health 2020, 17, 7176. [Google Scholar] [CrossRef] [PubMed]
- Holthe, T.; Jentoft, R.; Arntzen, C.; Thorsen, K. Benefits and Burdens: Family Caregivers’ Experiences of Assistive Technology (AT) in Everyday Life with Persons with Young-Onset Dementia (YOD). Disabil. Rehabil. Assist. Technol. 2018, 13, 754–762. [Google Scholar] [CrossRef]
- Yousaf, K.; Mehmood, Z.; Awan, I.A.; Saba, T.; Alharbey, R.; Qadah, T.; Alrige, M.A. A Comprehensive Study of Mobile-Health Based Assistive Technology for the Healthcare of Dementia and Alzheimer’s Disease (AD). Health Care Manag. Sci. 2020, 23, 287–309. [Google Scholar] [CrossRef] [PubMed]
- Lauriks, S.; Reinersmann, A.; Van der Roest, H.G.; Meiland, F.J.M.; Davies, R.J.; Moelaert, F.; Mulvenna, M.D.; Nugent, C.D.; Dröes, R.M. Review of ICT-Based Services for Identified Unmet Needs in People with Dementia. Ageing Res. Rev. 2007, 6, 223–246. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, N.A.; Azad-Khaneghah, P.; Miguel-Cruz, A.; Liu, L. What Do We Know about Strategies to Manage Dementia-related Wandering? A Scoping Review. Alzheimer’s Dement.: Diagn. Assess. Dis. Monit. 2018, 10, 615–628. [Google Scholar] [CrossRef]
- Lee-Cheong, S.; Amanullah, S.; Jardine, M. New Assistive Technologies in Dementia and Mild Cognitive Impairment Care: A PubMed Review. Asian J. Psychiatr. 2022, 73, 103135. [Google Scholar] [CrossRef]
- Nap, H.H.; Lukkien, D.; Cornelisse, L.; van der Weegen, S.; van der Leeuw, J.; van der Sande, R. Whitepaper Leefstijlmonitoring; Vilans: Utrecht, The Netherlands, 2017. [Google Scholar]
- van Rooij, T. “Dit Is Nog Makkelijker”, Herken Bij Welke Zorgvraag Jij Je Cliënt Kan Ondersteunen Met Tessa; Tinybots BV: Rotterdam, The Netherlands, 2021. [Google Scholar]
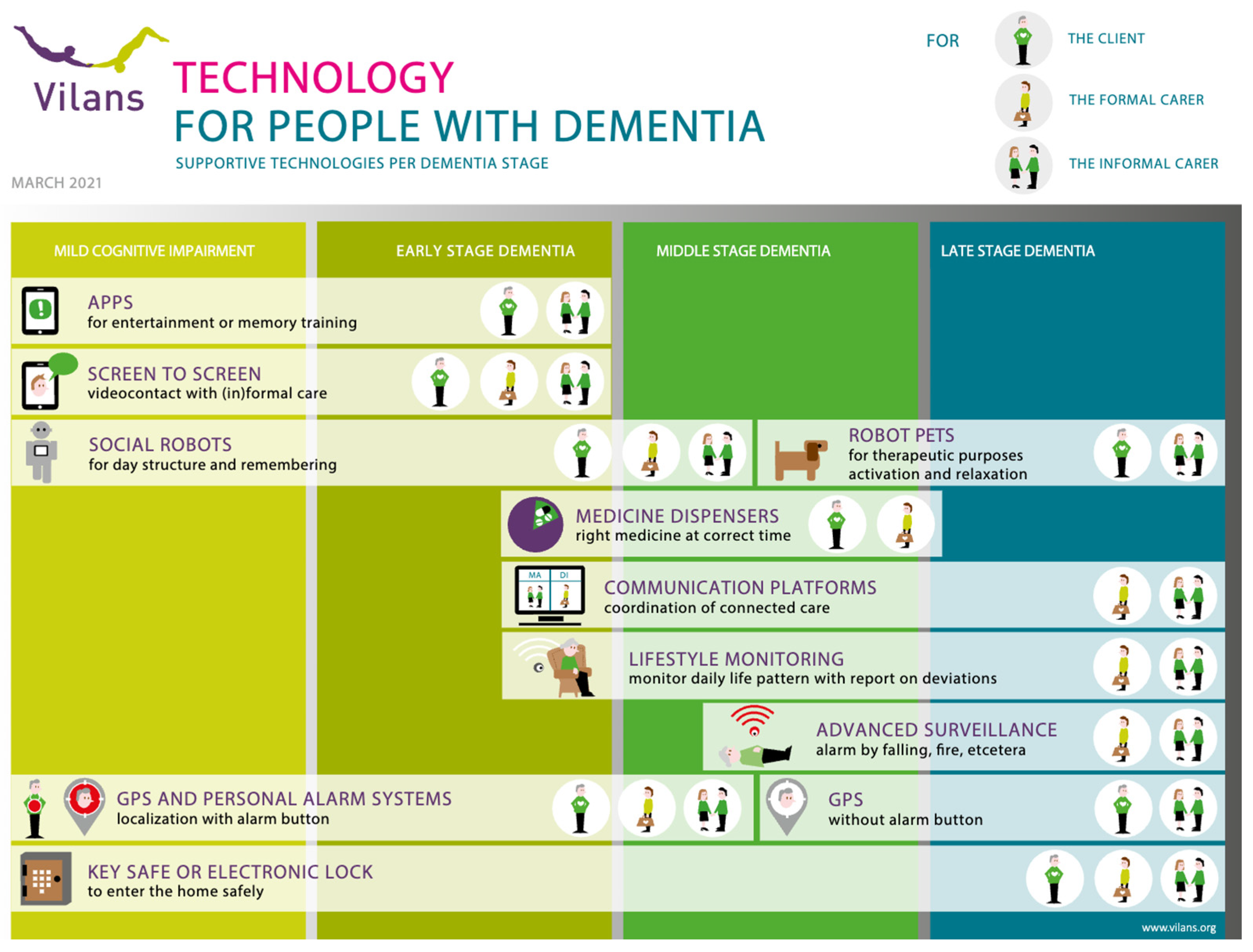
- van der Leeuw, J.; Cornelisse, C.C.L.; Suijkerbuijk, S.; Herman Nap, H. Infographic Technology for People with Dementia; Vilans: Utrecht, The Netherlands, 2021. [Google Scholar]
- Reisberg, B.; Ferris, S.H.; de Leon, M.J.; Crook, T. The Global Deterioration Scale for Assessment of Primary Degenerative Dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar] [CrossRef]
- Alzheimer’s Society. The Progression and Stages of Dementia; Alzheimer’s Society: London, UK, 2020. [Google Scholar]
- Hanson, E.; Magnusson, L.; Arvidsson, H.; Claesson, A.; Keady, J.; Nolan, M. Working Together with Persons with Early Stage Dementia and Their Family Members to Design a User-Friendly Technology-Based Support Service. Dementia 2007, 6, 411–434. [Google Scholar] [CrossRef]
- Poon, P.; Hui, E.; Dai, D.; Kwok, T.; Woo, J. Cognitive Intervention for Community-Dwelling Older Persons with Memory Problems: Telemedicine versus Face-to-Face Treatment. Int. J. Geriatr. Psychiatry 2005, 20, 285–286. [Google Scholar] [CrossRef]
- Svagård, I.S.; Boysen, E.S. Electronic Medication Dispensers Finding the Right Users—A Pilot Study in a Norwegian Municipality Home Care Service. In Proceedings of the 15th International Conference, ICCHP 2016, Linz, Austria, 13–15 July 2016; pp. 281–284. [Google Scholar]
- Lim, F.S.; Wallace, T.; Luszcz, M.A.; Reynolds, K.J. Usability of Tablet Computers by People with Early-Stage Dementia. Gerontology 2013, 59, 174–182. [Google Scholar] [CrossRef]
- Perälä, S.; Mäkelä, K.; Salmenaho, A.; Latvala, R. Technology for Elderly with Memory Impairment and Wandering Risk. Ehealth Telecommun. Syst. Netw. 2013, 02, 13–22. [Google Scholar] [CrossRef]
- Núñez-Naveira, L.; Alonso-Búa, B.; de Labra, C.; Gregersen, R.; Maibom, K.; Mojs, E.; Krawczyk-Wasielewska, A.; Millán-Calenti, J.C. UnderstAID, an ICT Platform to Help Informal Caregivers of People with Dementia: A Pilot Randomized Controlled Study. BioMed Res. Int. 2016, 2016, 5726465. [Google Scholar] [CrossRef]
- Boessen, A.B.C.G.; Verwey, R.; Duymelinck, S.; van Rossum, E. An Online Platform to Support the Network of Caregivers of People with Dementia. J. Aging Res. 2017, 2017, 3076859. [Google Scholar] [CrossRef] [PubMed]
- Verwey, R.; van Berlo, M.; Duymelinck, S.; Willard, S.; van Rossum, E. Development of an Online Platform to Support the Network of Caregivers of People with Dementia. Stud. Health Technol. Inform. 2016, 225, 567–571. [Google Scholar]
- Zwierenberg, E.; Nap, H.H.; Lukkien, D.; Cornelisse, L.; Finnema, E.; Dijkstra, A.; Hagedoorn, M.; Sanderman, R. A Lifestyle Monitoring System to Support (in)Formal Caregivers of People with Dementia: Analysis of Users Need, Benefits, and Concerns. Gerontechnology 2019, 17, 194–205. [Google Scholar] [CrossRef]
- van der Leeuw, J.; Jacobs, E. Leefstijlmonitoring in de Dagelijkse Praktijk; Vilans: Utrecht, The Netherlands, 2021. [Google Scholar]
- Stokke, R. The Personal Emergency Response System as a Technology Innovation in Primary Health Care Services: An Integrative Review. J. Med. Internet Res. 2016, 18, e187. [Google Scholar] [CrossRef]
- Lach, H.W.; Chang, Y.-P. Caregiver Perspectives on Safety in Home Dementia Care. West. J. Nurs. Res. 2007, 29, 993–1014. [Google Scholar] [CrossRef]
- Pynoos, J.; Ohta, R.J. In-Home Interventions for Persons with Alzheimer’s Disease and Their Caregivers. Phys. Occup. Ther. Geriatr. 1991, 9, 83–92. [Google Scholar] [CrossRef]
- Marquardt, G.; Johnston, D.; Black, B.S.; Morrison, A.; Rosenblatt, A.; Lyketsos, C.G.; Samus, Q.M. Association of the Spatial Layout of the Home and ADL Abilities among Older Adults with Dementia. Am. J. Alzheimer’s Dis. Other Dement. 2011, 26, 51–57. [Google Scholar] [CrossRef]
- Bradley, A. Crossing the Bridge—Connecting with People in the Later Stages of Dementia. Work. Older People 2015, 19, 177–181. [Google Scholar] [CrossRef]
- Pot, A.M.; Willemse, B.M.; Horjus, S. A Pilot Study on the Use of Tracking Technology: Feasibility, Acceptability, and Benefits for People in Early Stages of Dementia and Their Informal Caregivers. Aging Ment. Health 2012, 16, 127–134. [Google Scholar] [CrossRef] [PubMed]
- van Boekel, L.; Wouters, E.; Grimberg, B.; van der Meer, N.; Luijkx, K. Perspectives of Stakeholders on Technology Use in the Care of Community-Living Older Adults with Dementia: A Systematic Literature Review. Healthcare 2019, 7, 73. [Google Scholar] [CrossRef] [PubMed]
- Ehn, M.; Richardson, M.X.; Landerdahl Stridsberg, S.; Redekop, K.; Wamala-Andersson, S. Mobile Safety Alarms Based on GPS Technology in the Care of Older Adults: Systematic Review of Evidence Based on a General Evidence Framework for Digital Health Technologies. J. Med. Internet Res. 2021, 23, e27267. [Google Scholar] [CrossRef] [PubMed]
- Øderud, T.; Landmark, B.; Eriksen, S.; Fossberg, A.B.; Brørs, K.F.; Mandal, T.B.; Ausen, D. Exploring the Use of GPS for Locating Persons with Dementia. Assist. Technol. Res. Ser. 2013, 33, 776–783. [Google Scholar]
- Dahl, Y.; Holbø, K. Value Biases of Sensor-Based Assistive Technology. In Proceedings of the Designing Interactive Systems Conference on DIS ’12, Newcastle Upon Tyne, UK, 11–15 June 2012; ACM Press: New York, NY, USA, 2012; p. 572. [Google Scholar]
- Olsson, A.; Engström, M.; Skovdahl, K.; Lampic, C. My, Your and Our Needs for Safety and Security: Relatives’ Reflections on Using Information and Communication Technology in Dementia Care. Scand. J. Caring Sci. 2012, 26, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, K.; Mehmood, Z.; Saba, T.; Rehman, A.; Munshi, A.M.; Alharbey, R.; Rashid, M. Mobile-Health Applications for the Efficient Delivery of Health Care Facility to People with Dementia (PwD) and Support to Their Carers: A Survey. BioMed Res. Int. 2019, 2019, 7151475. [Google Scholar] [CrossRef] [PubMed]
- Houben, M.; Brankaert, R.; Dhaeze, E.; Kenning, G.; Bongers, I.; Eggen, B. Enriching Everyday Lived Experiences in Dementia Care. In Proceedings of the Sixteenth International Conference on Tangible, Embedded, and Embodied Interaction; ACM: New York, NY, USA, 2022; pp. 1–13. [Google Scholar]
- Pappadà, A.; Chattat, R.; Chirico, I.; Valente, M.; Ottoboni, G. Assistive Technologies in Dementia Care: An Updated Analysis of the Literature. Front. Psychol. 2021, 12, 644587. [Google Scholar] [CrossRef]
- Kerkhof, Y.; Bergsma, A.; Graff, M.; Dröes, R. Selecting Apps for People with Mild Dementia: Identifying User Requirements for Apps Enabling Meaningful Activities and Self-Management. J. Rehabil. Assist. Technol. Eng. 2017, 4, 205566831771059. [Google Scholar] [CrossRef] [PubMed]
- Groenewoud, J.H.; de Lange, J. Evaluatie van Individuele Happy Games Op de IPad Voor Mensen Met Dementie; Hogeschool Rotterdam: Rotterdam, The Netherlands, 2014. [Google Scholar]
- Orpwood, R.; Bjørneby, S.; Hagen, I.; Mäki, O.; Faulkner, R.; Topo, P. User Involvement in Dementia Product Development. Dementia 2004, 3, 263–279. [Google Scholar] [CrossRef]
- Bjørneby, S.; Topo, P.; Cahill, S.; Begley, E.; Jones, K.; Hagen, I.; Macijauskiene, J.; Holthe, T. Ethical Considerations in the ENABLE Project. Dementia 2004, 3, 297–312. [Google Scholar] [CrossRef]
- Clare, L.; Wilson, B.A.; Carter, G.; Breen, K.; Gosses, A.; Hodges, J.R. Intervening with Everyday Memory Problems in Dementia of Alzheimer Type: An Errorless Learning Approach. J. Clin. Exp. Neuropsychol. 2000, 22, 132–146. [Google Scholar] [CrossRef] [PubMed]
- Gilliard, J.; Hagen, I. Enabling Technologies for People with Dementia: Cross-National Analysis Report; Enable; WorldCat: Dublin, OH, USA, 2004. [Google Scholar]
- Hofmann, M.; Hock, C.; Kühler, A.; Müller-Spahn, F. Interactive Computer-Based Cognitive Training in Patients with Alzheimer’s Disease. J. Psychiatr. Res. 1996, 30, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Darragh, M.; Ahn, H.S.; MacDonald, B.; Liang, A.; Peri, K.; Kerse, N.; Broadbent, E. Homecare Robots to Improve Health and Well-Being in Mild Cognitive Impairment and Early Stage Dementia: Results From a Scoping Study. J. Am. Med. Dir. Assoc. 2017, 18, e1–e1099. [Google Scholar] [CrossRef] [PubMed]
- Hirt, J.; Ballhausen, N.; Hering, A.; Kliegel, M.; Beer, T.; Meyer, G. Social Robot Interventions for People with Dementia: A Systematic Review on Effects and Quality of Reporting. J. Alzheimer’s Dis. 2021, 79, 773–792. [Google Scholar] [CrossRef]
- de Jong, E.S. ADL Assistive Robot for Older Adults with Dementia. Master’s Thesis, Eindhoven University of Technology, Eindhoven, The Netherlands, 2017. [Google Scholar]
- Jøranson, N.; Pedersen, I.; Rokstad, A.M.M.; Ihlebæk, C. Effects on Symptoms of Agitation and Depression in Persons with Dementia Participating in Robot-Assisted Activity: A Cluster-Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2015, 16, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Valentí Soler, M.; Agüera-Ortiz, L.; Olazarán Rodríguez, J.; Mendoza Rebolledo, C.; Pérez Muñoz, A.; Rodríguez Pérez, I.; Osa Ruiz, E.; Barrios Sánchez, A.; Herrero Cano, V.; Carrasco Chillón, L.; et al. Social Robots in Advanced Dementia. Front. Aging Neurosci. 2015, 7, 133. [Google Scholar] [CrossRef] [PubMed]
- Neal, I.; du Toit, S.H.J.; Lovarini, M. The Use of Technology to Promote Meaningful Engagement for Adults with Dementia in Residential Aged Care: A Scoping Review. Int. Psychogeriatr. 2020, 32, 913–935. [Google Scholar] [CrossRef]
- Bernabei, V.; De Ronchi, D.; La Ferla, T.; Moretti, F.; Tonelli, L.; Ferrari, B.; Forlani, M.; Atti, A.R. Animal-Assisted Interventions for Elderly Patients Affected by Dementia or Psychiatric Disorders: A Review. J. Psychiatr. Res. 2013, 47, 762–773. [Google Scholar] [CrossRef]
- Moyle, W.; Cooke, M.; Beattie, E.; Jones, C.; Klein, B.; Cook, G.; Gray, C. Exploring the Effect of Companion Robots on Emotional Expression in Older Adults with Dementia: A Pilot Randomized Controlled Trial. J. Gerontol. Nurs. 2013, 39, 46–53. [Google Scholar] [CrossRef]
- Tamura, T.; Yonemitsu, S.; Itoh, A.; Oikawa, D.; Kawakami, A.; Higashi, Y.; Fujimooto, T.; Nakajima, K. Is an Entertainment Robot Useful in the Care of Elderly People with Severe Dementia? J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, M83–M85. [Google Scholar] [CrossRef]
- Obayashi, K.; Kodate, N.; Masuyama, S. Measuring the Impact of Age, Gender and Dementia on Communication-robot Interventions in Residential Care Homes. Geriatr. Gerontol. Int. 2020, 20, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Naumann, A.; Hurtienne, J.; Göllner, S.; Langdon, P.; Clarkson, P. Technology Supporting the Everyday Life of People with Dementia. In Proceedings of the Conference on Inclusive Design and Communications—The Role of Inclusive Design in Making Social Innovation Happen, London, UK, 18–20 April 2011; pp. 318–327. [Google Scholar]
- Lindenberger, U.; Lövdén, M.; Schellenbach, M.; Li, S.-C.; Krüger, A. Psychological Principles of Successful Aging Technologies: A Mini-Review. Gerontology 2008, 54, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, T.B.; Storm, M.; Holm, A.L. Safety for Older Adults Using Telecare: Perceptions of Homecare Professionals. Nurs. Open 2019, 6, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Mutesi, P. Using Medicine Dispensers in Home Healthcare Services for People with Dementia. Benefits, Challenges and Strategies. Master’s Thesis, Oslo Metropolitan University, Oslo, Norway, 2021. [Google Scholar]
- Lucero, R.J.; Fehlberg, E.A.; Patel, A.G.M.; Bjarnardottir, R.I.; Williams, R.; Lee, K.; Ansell, M.; Bakken, S.; Luchsinger, J.A.; Mittelman, M. The Effects of Information and Communication Technologies on Informal Caregivers of Persons Living with Dementia: A Systematic Review. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2019, 5, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Nijhof, N.; Van Gemert-Pijnen, L.J.; Woolrych, R.; Sixsmith, A. An Evaluation of Preventive Sensor Technology for Dementia Care. J. Telemed. Telecare 2013, 19, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Vermeer, Y.; Higgs, P.; Charlesworth, G. What Do We Require from Surveillance Technology? A Review of the Needs of People with Dementia and Informal Caregivers. J. Rehabil. Assist. Technol. Eng. 2019, 6, 205566831986951. [Google Scholar] [CrossRef]
- İnel Manav, A.; Simsek, N. The Effect of Reminiscence Therapy with Internet-Based Videos on Cognitive Status and Apathy of Older People with Mild Dementia. J. Geriatr. Psychiatry Neurol. 2019, 32, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Topo, P.; Saarikalle, K.; Begley, E.; Cahill, S.; Holthe, T.; Macijauskiene, J. “I Don’t Know about the Past or the Future, but Today It’s Friday”—Evaluation of a Time Aid for People with Dementia. Technol. Disabil. 2007, 19, 121–131. [Google Scholar] [CrossRef]
- Lekeu, F.; Wojtasik, V.; Van der Linden, M.; Salmon, E. Training Early Alzheimer Patients to Use a Mobile Phone. Acta Neurol. Belg. 2002, 102, 114–121. [Google Scholar]
- Tyack, C.; Camic, P.M. Touchscreen Interventions and the Well-Being of People with Dementia and Caregivers: A Systematic Review. Int. Psychogeriatr. 2017, 29, 1261–1280. [Google Scholar] [CrossRef]
- Kong, A.P.-H. Conducting Cognitive Exercises for Early Dementia with the Use of Apps on IPads. Commun. Disord. Q. 2015, 36, 102–106. [Google Scholar] [CrossRef]
- Bastoni, S.; Wrede, C.; da Silva, M.C.; Sanderman, R.; Gaggioli, A.; Braakman-Jansen, A.; van Gemert-Pijnen, L. Factors Influencing Implementation of EHealth Technologies to Support Informal Dementia Care: Umbrella Review. JMIR Aging 2021, 4, e30841. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.J.; Nugent, C.D.; Donnelly, M.P.; Hettinga, M.; Meiland, F.J.; Moelaert, F.; Mulvenna, M.D.; Bengtsson, J.E.; Craig, D.; Dröes, R.-M. A User Driven Approach to Develop a Cognitive Prosthetic to Address the Unmet Needs of People with Mild Dementia. Pervasive Mob. Comput. 2009, 5, 253–267. [Google Scholar] [CrossRef]
- Hettinga, M.; Janssen, R. Een Stem in Huis: De Betekenis van Sociale Robots Voor Thuiswonende Mensen Met Dementie; Windesheim University of Applied Sciences: Zwolle, The Netherlands, 2018. [Google Scholar]
- Takayanagi, K.; Kirita, T.; Shibata, T. Comparison of Verbal and Emotional Responses of Elderly People with Mild/Moderate Dementia and Those with Severe Dementia in Responses to Seal Robot, PARO. Front. Aging Neurosci. 2014, 6, 257. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ipakchian Askari, S.; Vasseur, D.; Hofstede, B.; Koowattanataworn, P.; Nap, H.H. Mapping Dementia Care Technology: Tailored Digital Solutions across Stages. Int. Med. Educ. 2024, 3, 140-151. https://doi.org/10.3390/ime3020012
Ipakchian Askari S, Vasseur D, Hofstede B, Koowattanataworn P, Nap HH. Mapping Dementia Care Technology: Tailored Digital Solutions across Stages. International Medical Education. 2024; 3(2):140-151. https://doi.org/10.3390/ime3020012
Chicago/Turabian StyleIpakchian Askari, Sima, Dianne Vasseur, Bob Hofstede, Piyakorn Koowattanataworn, and Henk Herman Nap. 2024. "Mapping Dementia Care Technology: Tailored Digital Solutions across Stages" International Medical Education 3, no. 2: 140-151. https://doi.org/10.3390/ime3020012