
The Impact of Simulated Ward Rounds on the Clinical Education of Final-Year Medical Students: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Literature Screening
2.4. Outcomes
2.5. Data Extraction
2.6. Quality and Risk of Bias Assessment
3. Results
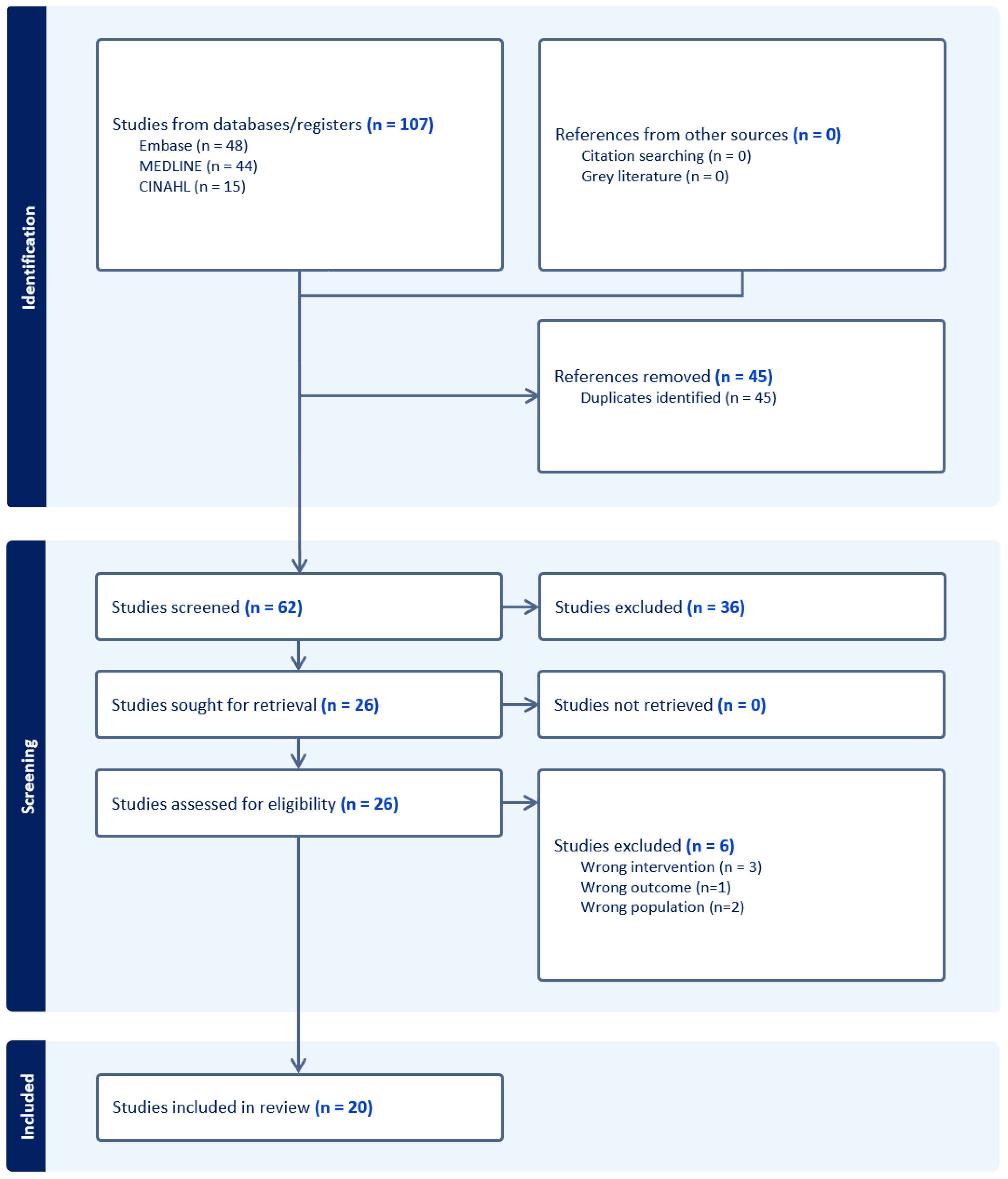
3.1. Literature Search Results
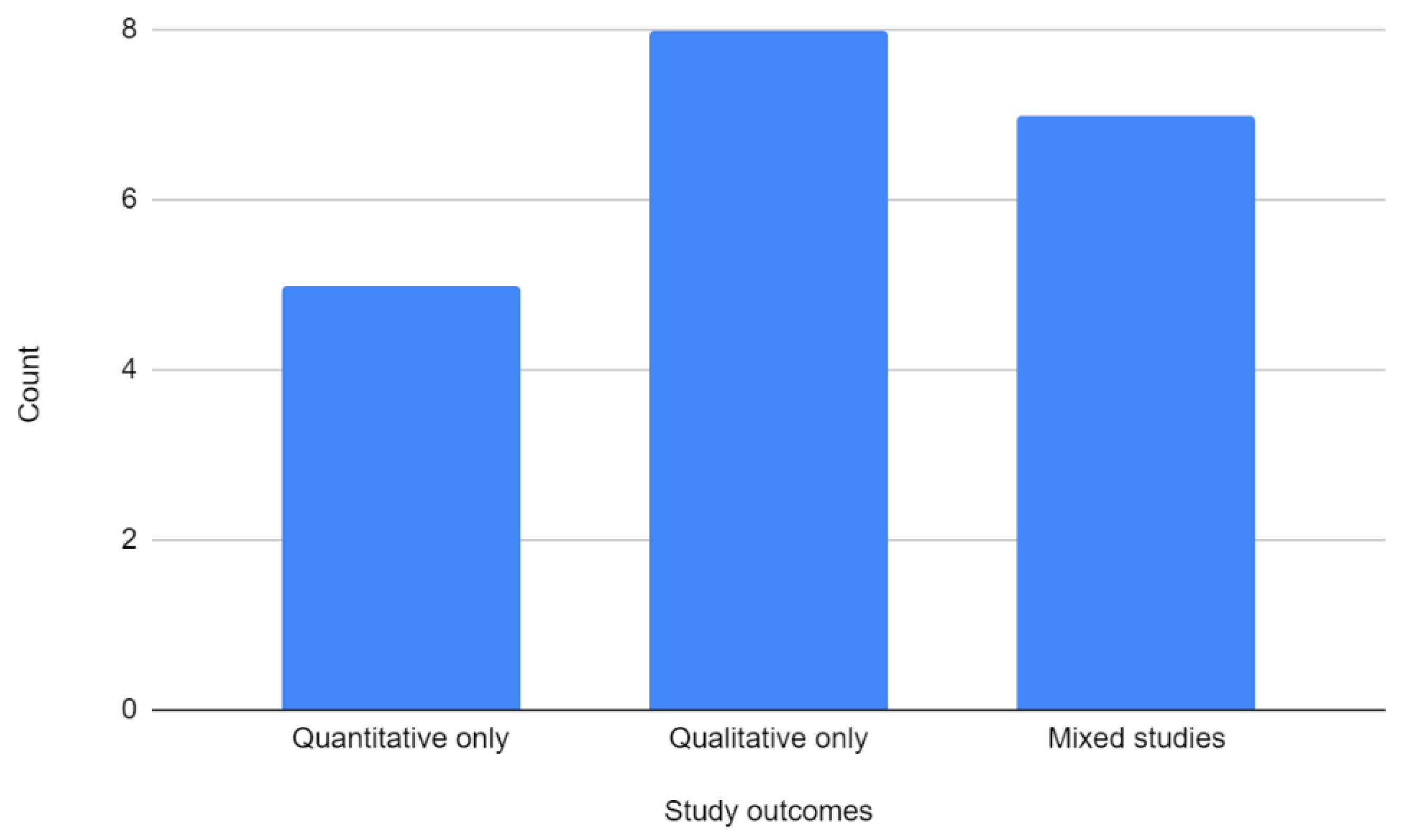
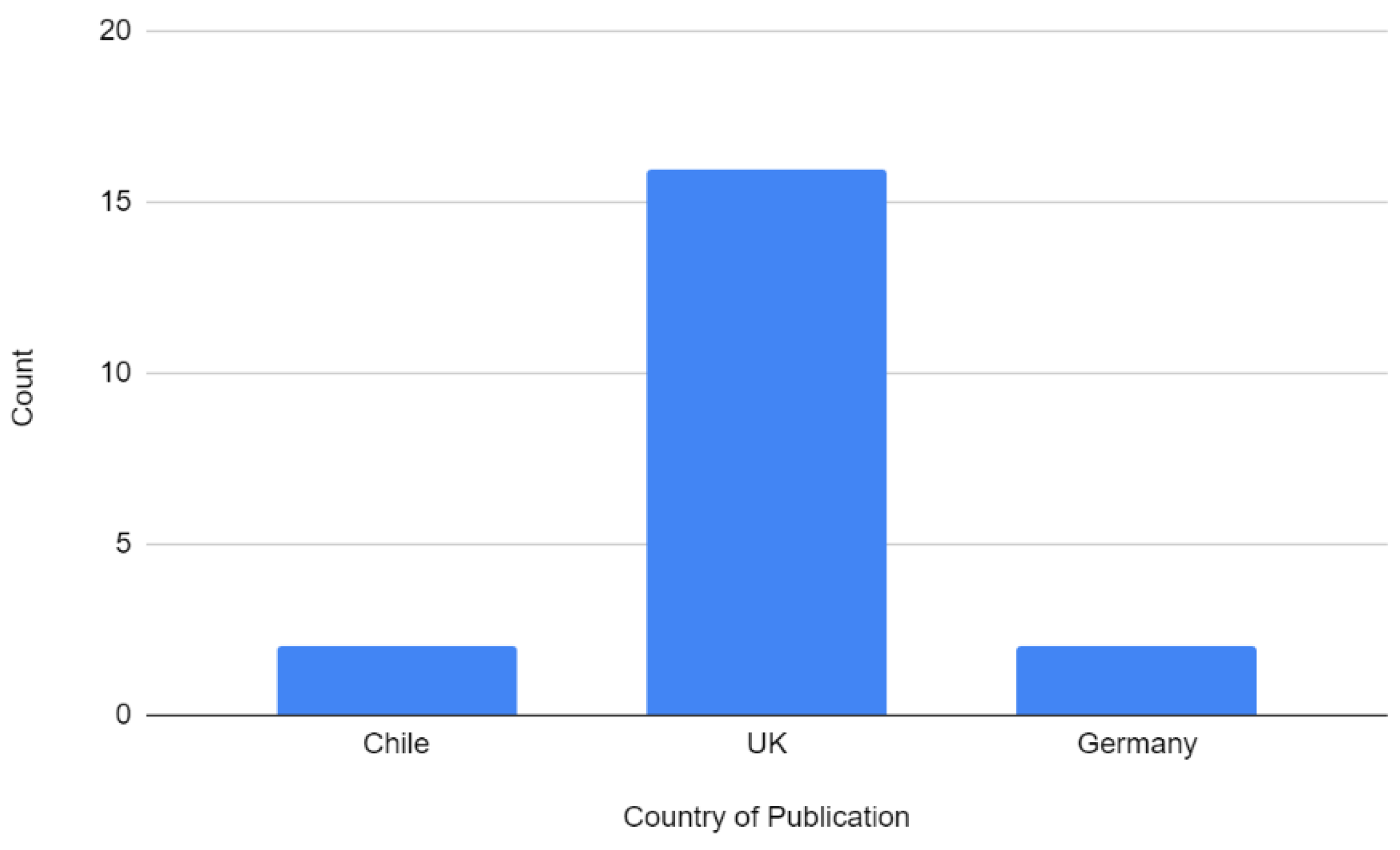
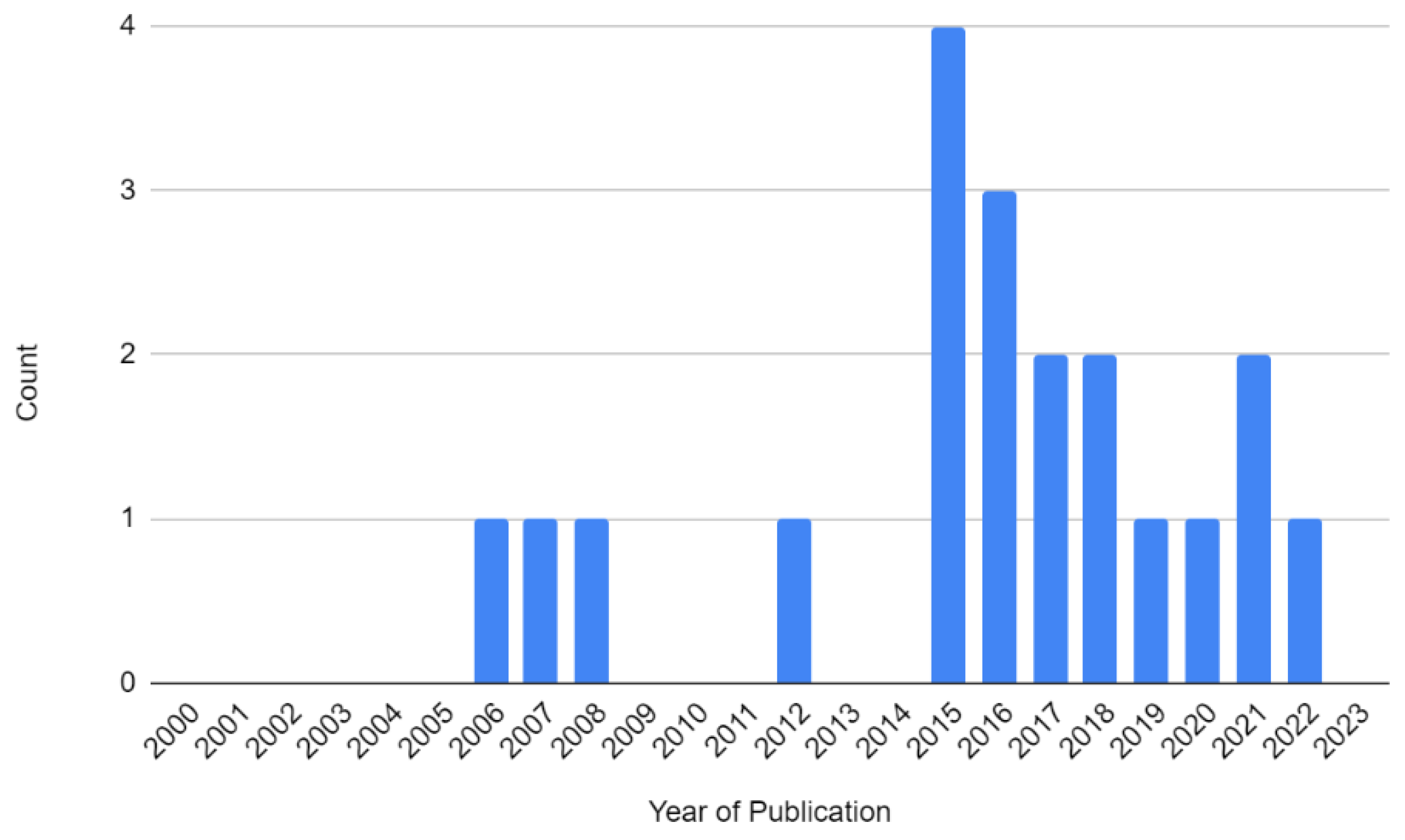
3.2. Overview of Included Studies
3.3. Key Themes from Quantitative and Qualitative Meta-Synthesis
3.3.1. Negative Emotions
3.3.2. Information Overload
3.3.3. Improving Relevant and Transferrable Skills
3.3.4. Realism
3.3.5. Feelings of Unpreparedness
3.3.6. Feedback
3.3.7. Application of Knowledge
3.3.8. Improving Confidence
3.3.9. Quality and Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldacre, M.J.; Lambert, T.W.; Svirko, E. Foundation doctors’ views on whether their medical school prepared them well for work: UK graduates of 2008 and 2009. Postgrad. Med. J. 2014, 90, 63–68. [Google Scholar] [CrossRef]
- Monrouxe, L.V.; Grundy, L.; Mann, M.; John, Z.; Panagoulas, E.; Bullock, A.; Mattick, K. How prepared are UK medical graduates for practice? A rapid review of the literature 2009–2014. BMJ Open 2017, 7, e013656. [Google Scholar] [CrossRef]
- Nikendei, C.; Kraus, B.; Schrauth, M.; Briem, S.; Jünger, J. Ward rounds: How prepared are future doctors? Med. Teach. 2008, 30, 88–91. [Google Scholar] [CrossRef]
- Pucher, P.H.; Aggarwal, R.; Darzi, A. Surgical ward round quality and impact on variable patient outcomes. Ann. Surg. 2014, 259, 222–226. [Google Scholar] [CrossRef]
- Brennan, N.; Corrigan, O.; Allard, J.; Archer, J.; Barnes, R.; Bleakley, A.; Collett, T.; de Bere, S.R. The transition from medical student to junior doctor: Today’s experiences of Tomorrow’s Doctors. Med. Educ. 2010, 44, 449–458. [Google Scholar] [CrossRef]
- Spencer, R.; Coiera, E.; Logan, P. Variation in communication loads on clinical staff in the emergency department. Ann. Emerg. Med. 2004, 44, 268–273. [Google Scholar] [CrossRef]
- Tipping, M.D.; Forth, V.E.; O’Leary, K.J.; Malkenson, D.M.; Magill, D.B.; Englert, K.; Williams, M.V. Where did the day go?—A time-motion study of hospitalists. J. Hosp. Med. 2010, 5, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Weigl, M.; Müller, A.; Sevdalis, N.; Angerer, P. Relationships of multitasking, physicians’ strain, and performance: An observational study in ward physicians. J. Patient Saf. 2013, 9, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Weigl, M.; Müller, A.; Zupanc, A.; Glaser, J.; Angerer, P. Hospital doctors’ workflow interruptions and activities: An observation study. BMJ Qual. Saf. 2011, 20, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Behrens, C.; Dolmans, D.H.J.M.; Leppink, J.; Gormley, G.J.; Driessen, E.W. Ward round simulation in final year medical students: Does it promote students learning? Med. Teach. 2018, 40, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Sirriyeh, R.; Lawton, R.; Gardner, P.; Armitage, G. Reviewing studies with diverse designs: The development and evaluation of a new tool. J. Eval. Clin. Pract. 2012, 18, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.; Jones, B.; Gardner, P.; Lawton, R. Quality assessment with diverse studies (QuADS): An appraisal tool for methodological and reporting quality in systematic reviews of mixed- or multi-method studies. BMC Health Serv. Res. 2021, 21, 144. [Google Scholar]
- Pluye, P.; Gagnon, M.P.; Griffiths, F.; Johnson-Lafleur, J. A scoring system for appraising mixed methods research, and concomitantly appraising qualitative, quantitative and mixed methods primary studies in Mixed Studies Reviews. Int. J. Nurs. Stud. 2009, 46, 529–546. [Google Scholar] [CrossRef] [PubMed]
- Pace, R.; Pluye, P.; Bartlett, G.; Macaulay, A.C.; Salsberg, J.; Jagosh, J.; Seller, R. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int. J. Nurs. Stud. 2012, 49, 47–53. [Google Scholar] [CrossRef] [PubMed]
- OCEBM Levels of Evidence Working Group. “The Oxford 2011 Levels of Evidence”. Oxford Centre for Evidence-Based Medicine. 2011. Available online: http://wwwcebmnet/indexaspx?o=5653 (accessed on 22 June 2023).
- Behrens, C.C.; Driessen, E.W.; Dolmans, D.H.; Gormley, G.J. ‘A roller coaster of emotions’: A phenomenological study on medical students lived experiences of emotions in complex simulation. Adv. Simul. 2021, 6, 24. [Google Scholar] [CrossRef]
- Harvey, R.; Mellanby, E.; Dearden, E.; Medjoub, K.; Edgar, S. Developing non-technical ward-round skills. Clin. Teach. 2015, 12, 336–340. [Google Scholar] [CrossRef]
- Hawkins, A.; Tredgett, K. Use of high-fidelity simulation to improve communication skills regarding death and dying: A qualitative study. BMJ Support. Palliat. Care 2016, 6, 474–478. [Google Scholar] [CrossRef]
- Hawkins, N.; Younan, H.-C.; Fyfe, M.; Parekh, R.; McKeown, A. Exploring why medical students still feel underprepared for clinical practice: A qualitative analysis of an authentic on-call simulation. BMC Med. Educ. 2021, 21, 165. [Google Scholar] [CrossRef]
- Lewis, G.; McCullough, M.; Maxwell, A.P.; Gormley, G.J. Ethical reasoning through simulation: A phenomenological analysis of student experience. Adv. Simul. 2016, 1, 26. [Google Scholar] [CrossRef]
- Morgan, J.; Green, V.; Blair, J. Using simulation to prepare for clinical practice. Clin. Teach. 2018, 15, 57–61. [Google Scholar] [CrossRef]
- Smith, S.D.; Henn, P.; Gaffney, R.; Hynes, H.; McAdoo, J.; Bradley, C. A study of innovative patient safety education. Clin. Teach. 2012, 9, 37–40. [Google Scholar] [CrossRef]
- Thomas, I. Student views of stressful simulated ward rounds. Clin. Teach. 2015, 12, 346–352. [Google Scholar] [CrossRef]
- Manalayil, J.; Muston, A.; Ball, A.; Chevalier, D. 1HR ON-CALL—Using Simulated ON-CALL to Underpin Experiential Learning in Final Year Medical Students. J. Eur. CME. 2020, 9, 1832749. [Google Scholar] [CrossRef] [PubMed]
- MacDowall, J. The assessment and treatment of the acutely ill patient--the role of the patient simulator as a teaching tool in the undergraduate programme. Med. Teach. 2006, 28, 326–329. [Google Scholar] [CrossRef] [PubMed]
- Harvey, R.; Murray, K.; McKenzie, K.; Mellanby, E.; Crichton, F.; Henderson, D. Improving the non-technical ward round skills of medical students. Br. J. Hosp. Med. 2016, 77, 481–484. [Google Scholar] [CrossRef] [PubMed]
- Ford, H.; Cleland, J.; Thomas, I. Simulated ward round: Reducing costs, not outcomes. Clin. Teach. 2017, 14, 49–54. [Google Scholar] [CrossRef]
- Nikendei, C.; Kraus, B.; Lauber, H.; Schrauth, M.; Weyrich, P.; Zipfel, S.; Jünger, J.; Briem, S. An innovative model for teaching complex clinical procedures: Integration of standardised patients into ward round training for final year students. Med. Teach. 2007, 29, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Pollard, J.; Tombs, M. Teaching Undergraduate Medical Students Non-Technical Skills: An Evaluation Study of a Simulated Ward Experience. Adv. Med. Educ. Pract. 2022, 13, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Teagle, A.R.; George, M.; Gainsborough, N.; Haq, I.; Okorie, M. Preparing medical students for clinical practice: Easing the transition. Perspect. Med. Educ. 2017, 6, 277–280. [Google Scholar] [CrossRef]
- Parker, R.; Hodierne, L.; Anderson, E.S.; Davies, R.S.; Elloy, M. Academic ability and teamworking in medical students. Clin. Teach. 2019, 16, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Thomas, I.; Nicol, L.; Regan, L.; Cleland, J.; Maliepaard, D.; Clark, L.; Walker, K.; Duncan, J. Driven to distraction: A prospective controlled study of a simulated ward round experience to improve patient safety teaching for medical students. BMJ Qual. Saf. 2015, 24, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Powell, N.; Bruce, C.G.; Redfern, O. Teaching a ‘good’ ward round. Clin. Med. 2015, 15, 135–138. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Location | Study Type | Sample Size | Outcome Data | Intervention | OCEBMa Level of Evidence |
|---|---|---|---|---|---|---|---|
| Nikendei et al. [3] | 2008 | Germany | Prospective Trial | 45 | Quantitative | 2 h ward round simulation with three standardised patient scenarios | 2C |
| Behrens et al. [10] | 2018 | Chile | Prospective Trial | 56 | Mixed | Emergency ward round simulation session with 3 patients | 2C |
| Behrens et al. [17] | 2021 | Chile | Prospective Trial | 8 | Qualitative | Emergency ward round simulation session with 3 patients | 3 |
| Harvey et al. [18] | 2015 | United Kingdom | Prospective Trial | 217 | Qualitative | 30 min simulated ward round | 3 |
| Hawkins et al. [19] | 2016 | United Kingdom | Prospective Trial | 7 | Qualitative | Mock ward environment in simulation suite with high fidelity simulation mannequin (SimMan) | 3 |
| Hawkins et al. [20] | 2021 | United Kingdom | Prospective Trial | 30 | Qualitative | 90 min on-call ward simulation | 3 |
| Lewis et al. [21] | 2016 | United Kingdom | Prospective Trial | 8 | Qualitative | Interprofessional ward-based simulation | 3 |
| Morgan et al. [22] | 2018 | United Kingdom | Prospective Trial | 133 | Mixed | 60 min 4-bed ward simulation session | 2C |
| Smith et al. [23] | 2012 | United Kingdom | Prospective Trial | 20 | Mixed | Simulated ward environment with clinical scenarios | 2C |
| Thomas et al. [24] | 2015 | United Kingdom | Prospective Trial | 27 | Qualitative | Simulated ward round with common clinical scenarios | 3 |
| Manalayil et al. [25] | 2020 | United Kingdom | Prospective Trial | 17 | Mixed | 60 min hospital ward simulation with pager | 2C |
| MacDowall et al. [26] | 2006 | United Kingdom | Prospective Trial | 23 | Mixed | Simulated ward session with three scenarios using high-fidelity simulation mannequin (SimMan) | 2C |
| Harvey et al. [27] | 2016 | United Kingdom | Prospective Trial | 217 | Quantitative | 19 simulated ward rounds with 70 patient interactions in total | 2C |
| Ford et al. [28] | 2017 | United Kingdom | Prospective Trial | 23 | Mixed | 20 min simulated ward round | 2C |
| Nikendei et al. [29] | 2007 | Germany | Prospective Trial | 45 | Qualitative | 2 h ward round simulation with three standardised patient scenarios | 3 |
| Pollard et al. [30] | 2022 | United Kingdom | Prospective Trial | 13 | Qualitative | Simulated ward experience with three patient scenarios | 3 |
| Teagle et al. [31] | 2017 | United Kingdom | Prospective Trial | 120 | Mixed | Three-day course with four stations including simulated ward rounds, prescribing, handover, and lessons learnt sessions | 2C |
| Parker et al. [32] | 2019 | United Kingdom | Prospective Trial | 119 | Quantitative | 22 bed fully immersive simulated ward | 2C |
| Thomas et al. [33] | 2015 | United Kingdom | Prospective Trial | 14 | Quantitative | Simulated ward round with 3 patients | 2C |
| Powell et al. [34] | 2015 | United Kingdom | Prospective Trial | 68 | Quantitative | 3 h simulation based ward round session | 2C |
| Key Theme | Number of Articles Reporting Outcome |
|---|---|
| Negative emotions | 8 |
| Information overload | 5 |
| Relevant and transferrable skills | 12 |
| Realism | 10 |
| Unpreparedness | 2 |
| Valuable feedback | 6 |
| Difficulty in applying knowledge | 1 |
| Improved confidence | 3 |
| Quality Assessment Tool (QATSDD) Scores for All Reviewed Papers | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Paper | Item 1: Explicit Theoretical Framework | Item 2: Statement of Aims/Objectives in Main Report | Item 3: Clear Description of Research Setting | Item 4: Evidence Of Sample Size Considered in Terms of Analysis | Item 5: Representative Sample of Target Group of a Reasonable Size | Item 6: Description of Procedure for Data Collection | Item 7: Rationale for Choice of Data Collection Tool(s) | Item 8: Detailed Recruitment Data | Item 9: Statistical Assessment of Reliability and Validity of Measurement Tool(s) (Quantitative Studies Only) | Item 10: Fit between Research Question and Method of Data Collection (Quantitative Studies only) | Item 11: Fit between Research Question and Format and Content of Data Collection Tool e.g., Interview Schedule (Qualitative Studies only) | Item 12: Fit between Research Question and Method of Analysis (Quantitative Studies Only) | Item 13: Good Justification for Analytic Method Selected | Item 14: Assessment of Reliability of Analytic Process (Qualitative Studies Only) | Item 15: Evidence of User Involvement in Design | Item 16: Strengths and Limitations Critically Discussed | Score | % |
| 1 Behrens, 2021 [17] | 3 | 3 | 3 | 3 | 1 | 3 | 3 | 2 | N/A | N/A | 3 | N/A | 3 | 3 | 3 | 1 | 34/39 | 87.2 |
| 2 Behrens, 2018 [10] | 3 | 3 | 3 | 0 | 2 | 3 | 3 | 1 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 1 | 39/48 | 81.3 |
| 3 Ford, 2017 [28] | 3 | 3 | 3 | 0 | 2 | 1 | 0 | 3 | 0 | 3 | 3 | 1 | 0 | 0 | 3 | 1 | 26/48 | 54.2 |
| 5 Harvey, 2015 [18] | 2 | 3 | 1 | 0 | 3 | 3 | 2 | 0 | N/A | N/A | 3 | N/A | 2 | 3 | 3 | 2 | 27/39 | 69.2 |
| 6 Harvey, 2016 [27] | 3 | 3 | 3 | 0 | 3 | 3 | 0 | 0 | 3 | 3 | N/A | 3 | 0 | N/A | 3 | 1 | 26/42 | 66.7 |
| 7 Hawkins, 2016 [19] | 3 | 3 | 3 | 3 | 1 | 3 | 0 | 3 | N/A | N/A | 3 | N/A | 1 | 0 | 3 | 3 | 29/39 | 74.4 |
| 8 Hawkins, 2021 [20] | 3 | 3 | 3 | 0 | 1 | 3 | 1 | 3 | N/A | N/A | 3 | N/A | 3 | 2 | 3 | 2 | 30/39 | 76.9 |
| 10 Lewis, 2016 [21] | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | N/A | N/A | 3 | N/A | 3 | 2 | 3 | 3 | 38/39 | 97.4 |
| 11 MacDowall, 2006 [26] | 3 | 3 | 3 | 0 | 1 | 1 | 0 | 0 | 0 | 2 | 2 | 1 | 0 | 0 | 3 | 1 | 20/48 | 41.7 |
| 12 Manalayil, 2020 [25] | 3 | 3 | 3 | 0 | 1 | 1 | 2 | 1 | 0 | 3 | 3 | 1 | 3 | 0 | 3 | 1 | 28/48 | 58.3 |
| 14 Morgan, 2018 [22] | 3 | 3 | 3 | 1 | 2 | 2 | 1 | 1 | 2 | 3 | 3 | 2 | 1 | 1 | 3 | 2 | 33/48 | 68.8 |
| 15 Nikendei, 2007 [29] | 3 | 3 | 3 | 0 | 3 | 3 | 2 | 1 | N/A | N/A | 3 | N/A | 1 | 1 | 3 | 3 | 29/39 | 74.4 |
| 16 Nikendei, 2008 [3] | 3 | 3 | 3 | 0 | 3 | 2 | 0 | 1 | 0 | 3 | N/A | 2 | 0 | N/A | 3 | 1 | 24/42 | 57.1 |
| 17 Parker, 2019 [32] | 3 | 3 | 3 | 3 | 2 | 3 | 3 | 2 | 3 | 3 | N/A | 3 | 1 | N/A | 3 | 3 | 38/42 | 90.5 |
| 18 Pollard, 2022 [30] | 3 | 3 | 3 | 1 | 1 | 3 | 3 | 3 | N/A | N/A | 3 | N/A | 2 | 2 | 3 | 3 | 33/39 | 84.6 |
| 19 Powell, 2015 [34] | 3 | 2 | 3 | 3 | 2 | 2 | 1 | 2 | 3 | 3 | N/A | 3 | 1 | N/A | 3 | 1 | 32/42 | 76.2 |
| 21 Smith, 2012 [23] | 3 | 1 | 3 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 3 | 1 | 0 | 0 | 3 | 1 | 18/48 | 37.5 |
| 22 Teagle, 2017 [31] | 3 | 3 | 3 | 0 | 2 | 3 | 2 | 3 | 0 | 3 | 3 | 2 | 0 | 0 | 3 | 1 | 31/48 | 64.6 |
| 23 Thomas, 2015 [24] | 3 | 3 | 3 | 0 | 2 | 3 | 3 | 2 | N/A | N/A | 3 | N/A | 2 | 0 | 3 | 1 | 28/39 | 71.8 |
| 24 Thomas, 2015 [33] | 3 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 3 | 3 | N/A | 3 | 3 | N/A | 3 | 3 | 41/42 | 97.6 |
| Mixed Methods Appraisal Tool (MMAT) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Quantitative Studies | Are There Clear Research Questions? | Do the Collected Data Allow Us to Address the Research Questions? | Is the Sampling Strategy Relevant to Address the Research Question? | Is the Sample Representative of the Target Population? | Are the Measurements Appropriate? | Is the Risk of Nonresponse Bias Low? | Is Statistical Analysis Appropriate to Answer the Research Question? | Score (/7) |
| 6 Harvey, 2016 [27] | + | + | + | + | + | + | + | 7 |
| 16 Nikendei, 2008 [3] | + | + | + | − | − | + | − | 4 |
| 17 Parker, 2019 [32] | + | + | + | − | + | − | + | 5 |
| 19 Powell, 2015 [34] | + | + | + | − | + | + | + | 6 |
| 24 Thomas, 2015 [33] | + | + | + | + | + | + | + | 7 |
| Qualitative studies | Are there clear research questions? | Do the collected data allow us to address the research questions? | Is the qualitative approach appropriate to answer the research question? | Are the qualitative data collection methods adequate to address the research question? | Are the findings adequately derived from the data? | Is the interpretation of results sufficiently substantiated by data? | Is there coherence between qualitative data sources, collection, analysis and interpretation? | Score (/7) |
| 1 Behrens, 2021 [17] | + | + | + | + | + | + | + | 7 |
| 5 Harvey, 2015 [18] | + | + | + | + | − | + | − | 5 |
| 7 Hawkins, 2016 [19] | + | + | + | + | + | + | + | 7 |
| 8 Hawkins, 2021 [20] | + | + | + | + | + | + | + | 7 |
| 10 Lewis, 2016 [21] | + | + | + | + | + | + | + | 7 |
| 15 Nikendei, 2007 [29] | + | + | + | + | + | + | + | 7 |
| 18 Pollard, 2022 [30] | + | + | + | + | + | + | + | 7 |
| 23 Thomas, 2015 [24] | + | + | + | + | + | + | + | 7 |
| Mixed studies | Are there clear research questions? | Do the collected data allow us to address the research questions? | Is there an adequate rationale for using a mixed methods design to address the research question? | Are the different components of the study effectively integrated to answer the research question? | Are the outputs of the integration of qualitative and quantitative components adequately interpreted? | Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? | Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? | Score (/7) |
| 2 Behrens, 2018 [10] | + | + | + | + | + | + | + | 7 |
| 3 Ford, 2017 [28] | + | + | + | − | − | − | − | 3 |
| 11 MacDowall, 2006 [26] | + | + | + | − | + | − | − | 4 |
| 12 Manalayil, 2020 [25] | + | + | + | − | − | − | − | 3 |
| 14 Morgan, 2018 [22] | + | + | + | + | − | − | − | 4 |
| 21 Smith, 2012 [23] | + | + | − | − | − | − | − | 2 |
| 22 Teagle, 2017 [31] | + | + | + | − | − | − | − | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, K.D.R.; Downie, E.; Azidis-Yates, E.; Shaw, C. The Impact of Simulated Ward Rounds on the Clinical Education of Final-Year Medical Students: A Systematic Review. Int. Med. Educ. 2024, 3, 100-115. https://doi.org/10.3390/ime3010009
Le KDR, Downie E, Azidis-Yates E, Shaw C. The Impact of Simulated Ward Rounds on the Clinical Education of Final-Year Medical Students: A Systematic Review. International Medical Education. 2024; 3(1):100-115. https://doi.org/10.3390/ime3010009
Chicago/Turabian StyleLe, Khang Duy Ricky, Emma Downie, Elizabeth Azidis-Yates, and Cameron Shaw. 2024. "The Impact of Simulated Ward Rounds on the Clinical Education of Final-Year Medical Students: A Systematic Review" International Medical Education 3, no. 1: 100-115. https://doi.org/10.3390/ime3010009