
The Impact of COVID-19 and Racial Injustices on Resilience of Incoming Medical Students
 ,
,
Abstract
:1. Introduction
1.1. Resilience
1.2. Racial Injustices in the United States
2. Materials and Methods
2.1. Quantitative Data Analysis
2.2. Qualitative Data Analysis
3. Results
3.1. Quantitative Analysis
3.2. Qualitative Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1


Appendix A.2


Appendix B
Appendix B.1

Appendix B.2

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Response Category | Criteria for Placement |
|---|---|
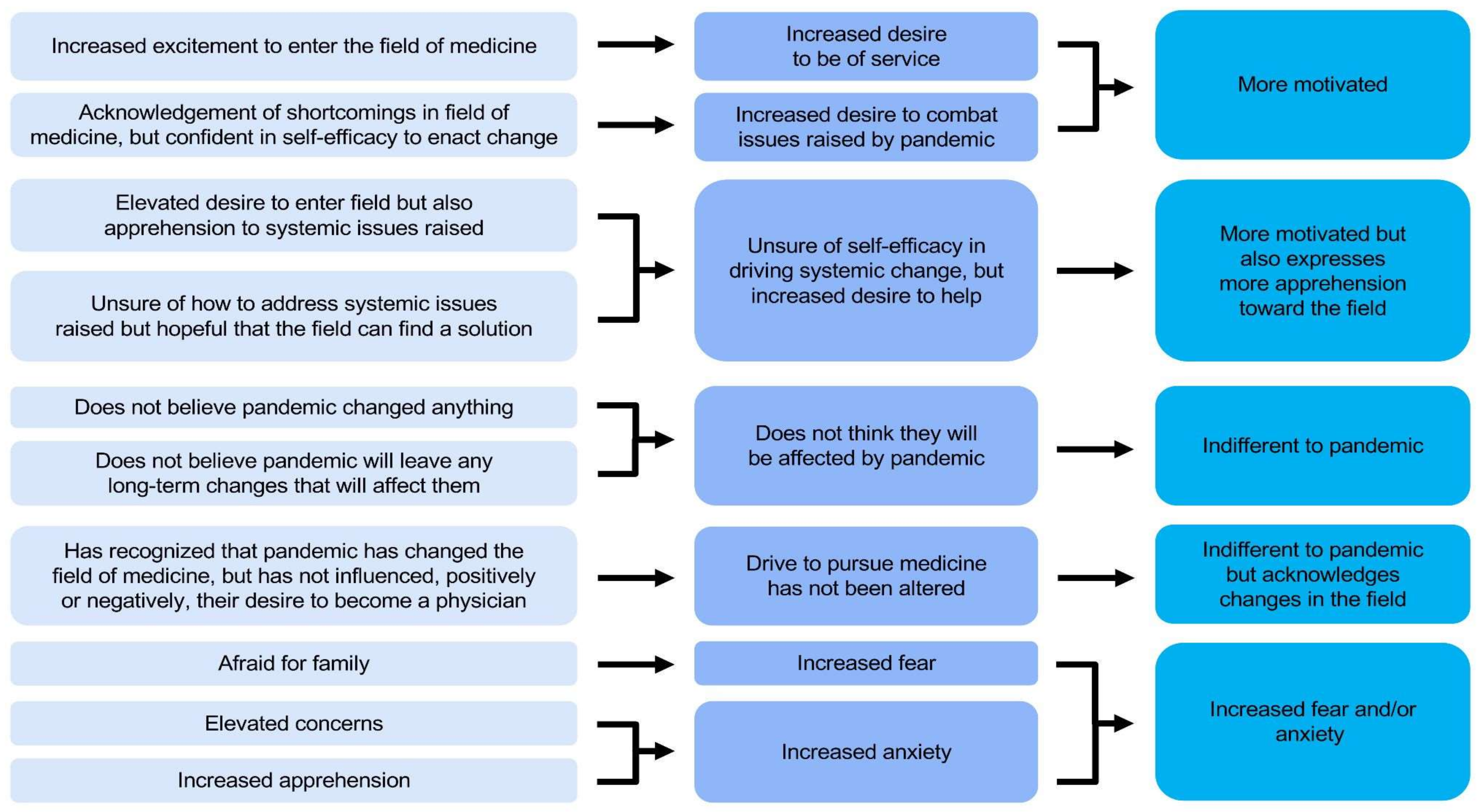
| Indifferent | The pandemic has not influenced participants’ opinions about entering the medical field. |
| Indifferent with caveat | The pandemic has not influenced participants’ personal opinions about entering the medical field, but acknowledges the change brought about by the pandemic. |
| Increased fear and/or anxiety | The pandemic has heightened the participants’ fear and/or anxiety about entering the medical field. |
| More motivated | The pandemic has increased the participants’ motivation to enter the medical field, often citing a desire to address issues the pandemic has highlighted or caused within the medical field. |
| More motivated with caveat | The pandemic has increased the participants’ motivation to enter the medical field, but participants are unsure of their capacity to enact positive change. |
References
- Zhu, Z.; Xu, S.; Wang, H.; Liu, Z.; Wu, J.; Li, G.; Miao, J.; Zhang, C.; Yang, Y.; Sun, W.; et al. COVID-19 in Wuhan: Sociodemographic characteristics and hospital support measures associated with the immediate psychological impact on healthcare workers. eClinicalMedicine 2020, 24, 100443. [Google Scholar] [CrossRef]
- Rolak, S.; Keefe, A.M.; Davidson, E.L.; Aryal, P.; Parajuli, S. Impacts and challenges of United States medical students during the COVID-19 pandemic. World J. Clin. Cases 2020, 8, 3136–3141. [Google Scholar] [CrossRef] [PubMed]
- O’Byrne, L.; Gavin, B.; McNicholas, F. Medical students and COVID-19: The need for pandemic preparedness. J. Med. Ethics 2020, 46, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Zis, P.; Artemiadis, A.; Bargiotas, P.; Nteveros, A.; Hadjigeorgiou, G.M. Medical Studies during the COVID-19 Pandemic: The Impact of Digital Learning on Medical Students’ Burnout and Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 349. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.Y.; Kim, K.H.; Joo, G.J.; Kim, B.N.; Roh, M.S.; Shin, M.S. Changing characteristics of the empathic communication network after empathy-enhancement program for medical students. Sci. Rep. 2018, 8, 15092. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Thomas, M.R.; Massie, F.S.; Power, D.V.; Eacker, A.; Harper, W.; Durning, S.; Moutier, C.; Szydlo, D.W.; Novotny, P.J.; et al. Burnout and suicidal ideation among U.S. medical students. Ann. Intern. Med. 2008, 149, 334–341. [Google Scholar] [CrossRef]
- Zisook, S.; Young, I.; Doran, N.; Downs, N.; Hadley, A.; Kirby, B.; McGuire, T.; Moutier, C.; Norcross, W.; Tiamson-Kassab, M. Suicidal Ideation Among Students and Physicians at a U.S. Medical School: A Healer Education, Assessment and Referral (HEAR) Program Report. OMEGA—J. Death Dying 2016, 74, 35–61. [Google Scholar]
- Mata, D.A.; Ramos, M.A.; Bansal, N.; Khan, R.; Guille, C.; Di Angelantonio, E.; Sen, S. Prevalence of Depression and Depressive Symptoms Among Resident Physicians: A Systematic Review and Meta-analysis. JAMA 2015, 314, 2373–2383. [Google Scholar] [CrossRef]
- Gold, K.J.; Sen, A.; Schwenk, T.L. Details on suicide among US physicians: Data from the National Violent Death Reporting System. Gen. Hosp. Psychiatry 2013, 35, 45–49. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Boone, S.; Tan, L.; Dyrbye, L.N.; Sotile, W.; Satele, D.; West, C.P.; Sloan, J.; Oreskovich, M.R. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch. Intern. Med. 2012, 172, 1377–1385. [Google Scholar] [CrossRef]
- Rothenberger, D.A. Physician Burnout and Well-Being: A Systematic Review and Framework for Action. Dis. Colon. Rectum 2017, 60, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; Balch, C.M.; Dyrbye, L.; Bechamps, G.; Russell, T.; Satele, D.; Rummans, T.; Swartz, K.; Novotny, P.J.; Sloan, J.; et al. Special report: Suicidal ideation among American surgeons. Arch. Surg. 2011, 146, 54–62. [Google Scholar] [CrossRef] [PubMed]
- DiMatteo, M.R.; Sherbourne, C.D.; Hays, R.D.; Ordway, L.; Kravitz, R.L.; McGlynn, E.A.; Kaplan, S.; Rogers, W.H. Physicians’ characteristics influence patients’ adherence to medical treatment: Results from the Medical Outcomes Study. Health Psychol. 1993, 12, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Linn, L.S.; Brook, R.H.; Clark, V.A.; Davies, A.R.; Fink, A.; Kosecoff, J. Physician and patient satisfaction as factors related to the organization of internal medicine group practices. Med. Care 1985, 23, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Grol, R.; Mokkink, H.; Smits, A.; van Eijk, J.; Beek, M.; Mesker, P.; Mesker-Niesten, J. Work satisfaction of general practitioners and the quality of patient care. Fam. Pract. 1985, 2, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Forycka, J.; Pawlowicz-Szlarska, E.; Burczynska, A.; Cegielska, N.; Harendarz, K.; Nowicki, M. Polish medical students facing the pandemic-Assessment of resilience, well-being and burnout in the COVID-19 era. PLoS ONE 2022, 17, e0261652. [Google Scholar] [CrossRef] [PubMed]
- Howe, A.; Smajdor, A.; Stockl, A. Towards an understanding of resilience and its relevance to medical training. Med. Educ. 2012, 46, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Neufeld, A.; Malin, G. Exploring the relationship between medical student basic psychological need satisfaction, resilience, and well-being: A quantitative study. BMC Med. Educ. 2019, 19, 405. [Google Scholar] [CrossRef]
- Abram, M.D.; Jacobowitz, W. Resilience and burnout in healthcare students and inpatient psychiatric nurses: A between-groups study of two populations. Arch. Psychiatr. Nurs. 2021, 35, 1–8. [Google Scholar] [CrossRef]
- Edmonds, V.S.; Chatterjee, K.; Girardo, M.E.; Butterfield, R.J., 3rd; Stonnington, C.M. Evaluation of a Novel Wellness Curriculum on Medical Student Wellbeing and Engagement Demonstrates a Need for Student-Driven Wellness Programming. Teach. Learn. Med. 2023, 35, 52–64. [Google Scholar] [CrossRef]
- Snapp, C.; Bassett, C.; Baldwin, A.; Hill, J.R.; DeBusk, R. Peer-Assisted Learning in Undergraduate Medical Education for Resilience and Well-being. Med. Sci. Educ. 2023, 33, 5–6. [Google Scholar] [CrossRef]
- Yeager, D.S.; Dweck, C.S. Mindsets that promote resilience: When students believe that personal characteristics can be developed. Educ. Psychol. 2012, 47, 302–314. [Google Scholar] [CrossRef]
- Zeng, G.; Hou, H.; Peng, K. Effect of Growth Mindset on School Engagement and Psychological Well-Being of Chinese Primary and Middle School Students: The Mediating Role of Resilience. Front. Psychol. 2016, 7, 1873. [Google Scholar] [CrossRef] [PubMed]
- Windle, G.; Bennett, K.M.; Noyes, J. A methodological review of resilience measurement scales. Health Qual. Life Outcomes 2011, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Wagnild, G.; Young, H.M. Resilience among older women. Image J. Nurs. Sch. 1990, 22, 252–255. [Google Scholar] [CrossRef]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Wagnild, G. A review of the Resilience Scale. J. Nurs. Meas. 2009, 17, 105–113. [Google Scholar] [CrossRef]
- Tempski, P.; Santos, I.S.; Mayer, F.B.; Enns, S.C.; Perotta, B.; Paro, H.B.; Gannam, S.; Peleias, M.; Garcia, V.L.; Baldassin, S.; et al. Relationship among Medical Student Resilience, Educational Environment and Quality of Life. PLoS ONE 2015, 10, e0131535. [Google Scholar] [CrossRef]
- Oliveira, A.C.P.M.; Machado, A.P.G.M.; Aranha, R.N.M. Identification of factors associated with resilience in medical students through a cross-sectional census. BMJ Open 2017, 7, e017189. [Google Scholar] [CrossRef]
- Lin, Y.K.; Lin, C.D.; Lin, B.Y.; Chen, D.Y. Medical students’ resilience: A protective role on stress and quality of life in clerkship. BMC Med. Educ. 2019, 19, 473. [Google Scholar] [CrossRef]
- Barnett, J.E.; Baker, E.K.; Elman, N.S.; Schoener, G.R. In pursuit of wellness: The self-care imperative. Prof. Psychol. Res. Pract. 2007, 38, 603–612. [Google Scholar] [CrossRef]
- Weine, S.; Kohrt, B.A.; Collins, P.Y.; Cooper, J.; Lewis-Fernandez, R.; Okpaku, S.; Wainberg, M.L. Justice for George Floyd and a reckoning for global mental health. Glob. Ment. Health 2020, 7, e22. [Google Scholar] [CrossRef] [PubMed]
- O’Marr, J.M.; Chan, S.M.; Crawford, L.; Wong, A.H.; Samuels, E.; Boatright, D. Perceptions on Burnout and the Medical School Learning Environment of Medical Students Who Are Underrepresented in Medicine. JAMA Netw. Open 2022, 5, e220115. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Thomas, M.R.; Eacker, A.; Harper, W.; Massie, F.S., Jr.; Power, D.V.; Huschka, M.; Novotny, P.J.; Sloan, J.A.; Shanafelt, T.D. Race, ethnicity, and medical student well-being in the United States. Arch. Intern. Med. 2007, 167, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Wagnild, G.M. The Resilience Scale User’s Guide; Resilience Center: Worden, MT, USA, 2016. [Google Scholar]
- Burgis-Kasthala, S.; Elmitt, N.; Smyth, L.; Moore, M. Predicting future performance in medical students. A longitudinal study examining the effects of resilience on low and higher performing students. Med. Teach. 2019, 41, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kyngas, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Morrison, N.; Machado, M.; Blackburn, C. Student perspectives on barriers to performance for black and minority ethnic graduate-entry medical students: A qualitative study in a West Midlands medical school. BMJ Open 2019, 9, e032493. [Google Scholar] [CrossRef]
- Bazargan-Hejazi, S.; Negrete Manriquez, J.A.; McDermoth-Grimes, M.; Parra, E.A.; Prothrow-Stith, D. Underrepresented in medicine students’ perspectives on impactful medical education. BMC Med. Educ. 2022, 22, 904. [Google Scholar] [CrossRef]
- Bauerle, A.; Teufel, M.; Musche, V.; Weismuller, B.; Kohler, H.; Hetkamp, M.; Dorrie, N.; Schweda, A.; Skoda, E.M. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: A cross-sectional study in Germany. J. Public Health 2020, 42, 672–678. [Google Scholar] [CrossRef]
- Myran, D.T.; Cantor, N.; Rhodes, E.; Pugliese, M.; Hensel, J.; Taljaard, M.; Talarico, R.; Garg, A.X.; McArthur, E.; Liu, C.W.; et al. Physician Health Care Visits for Mental Health and Substance Use During the COVID-19 Pandemic in Ontario, Canada. JAMA Netw. Open 2022, 5, e2143160. [Google Scholar] [CrossRef]
- Brazeau, C.M.; Shanafelt, T.; Durning, S.J.; Massie, F.S.; Eacker, A.; Moutier, C.; Satele, D.V.; Sloan, J.A.; Dyrbye, L.N. Distress among matriculating medical students relative to the general population. Acad. Med. 2014, 89, 1520–1525. [Google Scholar] [CrossRef] [PubMed]
- Lyons, Z.; Wilcox, H.; Leung, L.; Dearsley, O. COVID-19 and the mental well-being of Australian medical students: Impact, concerns and coping strategies used. Australas. Psychiatry 2020, 28, 649–652. [Google Scholar] [CrossRef]
- Jordan, R.K.; Shah, S.S.; Desai, H.; Tripi, J.; Mitchell, A.; Worth, R.G. Variation of stress levels, burnout, and resilience throughout the academic year in first-year medical students. PLoS ONE 2020, 15, e0240667. [Google Scholar] [CrossRef] [PubMed]
- Voltmer, E.; Koslich-Strumann, S.; Voltmer, J.B.; Kotter, T. Stress and behavior patterns throughout medical education—A six year longitudinal study. BMC Med. Educ. 2021, 21, 454. [Google Scholar] [CrossRef] [PubMed]
- Redwood, S.K.; Pollak, M.H. Student-led stress management program for first-year medical students. Teach. Learn. Med. 2007, 19, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Slavin, S.J.; Schindler, D.L.; Chibnall, J.T. Medical student mental health 3.0: Improving student wellness through curricular changes. Acad. Med. 2014, 89, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Yang, R.; Briskin, C.; Alper, D.; Morant, K.; Palmer, J.; Petersen, K.H. Resiliency Among Medical Students and Initial Review of a Student-Run Resiliency Curriculum. In Proceedings of the AMA Research Symposium, Virtual Meeting, 16–19 November 2020. [Google Scholar]
- Kim, H.; Cohen, A.; Evans, K.; Lee, K.R.; Longo, J.L.; McCafferty, J.; Morant, K.; Palmer, J.S.; Zhang, S.; Ludmer, P.; et al. NYMC Resiliency Curriculum. In Proceedings of the The AAMC Annual Meeting: Learn Serve Lead, Phoenix, AZ, USA, 8–12 November 2019. [Google Scholar]
- Bacchi, S.; Licinio, J. Resilience and Psychological Distress in Psychology and Medical Students. Acad. Psychiatry 2017, 41, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Sznajder, K.; Cheng, D.; Wang, S.; Cui, C.; Yang, X. Coping Styles for Mediating the Effect of Resilience on Depression Among Medical Students in Web-Based Classes During the COVID-19 Pandemic: Cross-sectional Questionnaire Study. J. Med. Internet Res. 2021, 23, e25259. [Google Scholar] [CrossRef]
- Said, D.; Kypri, K.; Bowman, J. Risk factors for mental disorder among university students in Australia: Findings from a web-based cross-sectional survey. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 935–944. [Google Scholar] [CrossRef]
- Wathelet, M.; Duhem, S.; Vaiva, G.; Baubet, T.; Habran, E.; Veerapa, E.; Debien, C.; Molenda, S.; Horn, M.; Grandgenevre, P.; et al. Factors Associated With Mental Health Disorders Among University Students in France Confined During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2025591. [Google Scholar] [CrossRef]
- Ehmke, M.D.; Katare, B.; Kiesel, K.; Bergtold, J.S.; Penn, J.M.; Boys, K.A. U.S. agricultural university students’ mental well-being and resilience during the first wave of COVID-19: Discordant expectations and experiences across genders. Appl. Econ. Perspect. Policy 2022, 44, 129–161. [Google Scholar] [CrossRef] [PubMed]
- Amendola, S.; von Wyl, A.; Volken, T.; Zysset, A.; Huber, M.; Dratva, J. A Longitudinal Study on Generalized Anxiety Among University Students During the First Wave of the COVID-19 Pandemic in Switzerland. Front. Psychol. 2021, 12, 643171. [Google Scholar] [CrossRef] [PubMed]
- Wathelet, M.; Vincent, C.; Fovet, T.; Notredame, C.E.; Habran, E.; Martignene, N.; Baubet, T.; Vaiva, G.; D’Hondt, F. Evolution in French University Students’ Mental Health One Month After the First COVID-19 Related Quarantine: Results From the COSAMe Survey. Front. Psychiatry 2022, 13, 868369. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Hasan, S.; Malik, S.; Sreeramareddy, C.T. Perceived stress, sources and severity of stress among medical undergraduates in a Pakistani medical school. BMC Med. Educ. 2010, 10, 2. [Google Scholar] [CrossRef] [PubMed]
- Langness, S.; Rajapuram, N.; Marshall, M.; Rahman, A.S.; Sammann, A. Risk factors associated with student distress in medical school: Associations with faculty support and availability of wellbeing resources. PLoS ONE 2022, 17, e0265869. [Google Scholar] [CrossRef] [PubMed]
- Wurth, S.; Sader, J.; Cerutti, B.; Broers, B.; Bajwa, N.M.; Carballo, S.; Escher, M.; Galetto-Lacour, A.; Grosgurin, O.; Lavallard, V.; et al. Medical students’ perceptions and coping strategies during the first wave of the COVID-19 pandemic: Studies, clinical implication, and professional identity. BMC Med. Educ. 2021, 21, 620. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.M.; Taylor, D.L.; Fitzgerald, A.A.; Kuo, C.C.; Graves, K.D. Build & Belong: A Peer-Based Intervention to Reduce Medical Student Social Isolation. Teach. Learn. Med. 2022, 34, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Lucey, C.R.; Saguil, A. The Consequences of Structural Racism on MCAT Scores and Medical School Admissions: The Past Is Prologue. Acad. Med. 2020, 95, 351–356. [Google Scholar] [CrossRef]
- Nguemeni Tiako, M.J.; Ray, V.; South, E.C. Medical Schools as Racialized Organizations: How Race-Neutral Structures Sustain Racial Inequality in Medical Education-a Narrative Review. J. Gen. Intern. Med. 2022, 37, 2259–2266. [Google Scholar] [CrossRef]
- Cyrus, K.D. A piece of my mind: Medical Education and the Minority Tax. JAMA 2017, 317, 1833–1834. [Google Scholar] [CrossRef]
- Hardeman, R.R.; Przedworski, J.M.; Burke, S.; Burgess, D.J.; Perry, S.; Phelan, S.; Dovidio, J.F.; van Ryn, M. Association Between Perceived Medical School Diversity Climate and Change in Depressive Symptoms Among Medical Students: A Report from the Medical Student CHANGE Study. J. Natl. Med. Assoc. 2016, 108, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Hardeman, R.R.; Przedworski, J.M.; Burke, S.E.; Burgess, D.J.; Phelan, S.M.; Dovidio, J.F.; Nelson, D.; Rockwood, T.; van Ryn, M. Mental Well-Being in First Year Medical Students: A Comparison by Race and Gender: A Report from the Medical Student CHANGE Study. J. Racial Ethn. Health Disparities 2015, 2, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Garcia, L.C.; Shanafelt, T.D.; West, C.P.; Sinsky, C.A.; Trockel, M.T.; Nedelec, L.; Maldonado, Y.A.; Tutty, M.; Dyrbye, L.N.; Fassiotto, M. Burnout, Depression, Career Satisfaction, and Work-Life Integration by Physician Race/Ethnicity. JAMA Netw. Open 2020, 3, e2012762. [Google Scholar] [CrossRef] [PubMed]
- Leigh, J.K. “What are you signing up for?”: Pre-medical students’ perception of physicians’ risk and responsibility during COVID-19. Soc. Sci. Med. 2021, 287, 114320. [Google Scholar] [CrossRef] [PubMed]
- Tempski, P.; Arantes-Costa, F.M.; Kobayasi, R.; Siqueira, M.A.M.; Torsani, M.B.; Amaro, B.; Nascimento, M.; Siqueira, S.L.; Santos, I.S.; Martins, M.A. Medical students’ perceptions and motivations during the COVID-19 pandemic. PLoS ONE 2021, 16, e0248627. [Google Scholar] [CrossRef] [PubMed]
- Abrams, M.P.; Salzman, J.; Espina Rey, A.; Daly, K. Impact of Providing Peer Support on Medical Students’ Empathy, Self-Efficacy, and Mental Health Stigma. Int. J. Environ. Res. Public Health 2022, 19, 5135. [Google Scholar] [CrossRef]
- Ortega, M.V.; Hidrue, M.K.; Lehrhoff, S.R.; Ellis, D.B.; Sisodia, R.C.; Curry, W.T.; Del Carmen, M.G.; Wasfy, J.H. Patterns in Physician Burnout in a Stable-Linked Cohort. JAMA Netw. Open 2023, 6, e2336745. [Google Scholar] [CrossRef] [PubMed]
- Horne, I.M.T.; Veggeland, F.; Bååthe, F.; Drewes, C.; Rø, K.I. Understanding peer support: A qualitative interview study of doctors one year after seeking support. BMC Health Serv. Res. 2023, 23, 324. [Google Scholar] [CrossRef]
- Bruce, S.M.; Conaglen, H.M.; Conaglen, J.V. Burnout in physicians: A case for peer-support. Intern. Med. J. 2005, 35, 272–278. [Google Scholar] [CrossRef]
| CO23 (Pre-Pandemic) | CO24 (Pandemic) | |
|---|---|---|
| Total study participants/Total students | 178/215 | 181/217 |
| Female, n (%) | 101 (56.7%) | 95 (52.5%) |
| URiM students, n (%) | 29 (16.3%) | 37 (20.4%) |
| FAP participants, n (%) | 22 (12.4%) | 13 (7.2%) |
| SED by self-report, n (%) | 18 (10.1%) | 38 (21.0%) |
| Accommodation status, n (%) | 15 (8.4%) | 20 (11.0%) |
| Comparison of Cohorts | Overall Resilience | Self-Assuredness | Drive | |||||||
| Mann–Whitney U | z | p | Mann–Whitney U | z | p | Mann–Whitney U | z | p | ||
| All students CO23 vs. CO24 | 16,032.5 | −0.08 | 0.938 | 16,088 | −0.02 | 0.983 | 15,856 | −0.26 | 0.796 | |
| Comparison by demographic subcategories | Overall Resilience | Self-Assuredness | Drive | |||||||
| CO23 | CO24 | p | CO23 | CO24 | p | CO23 | CO24 | p | ||
| Female | 78.76 (13.24) | 79.85 (9.23) | 0.578 | 5.55 (0.96) | 5.59 (0.77) | 0.687 | 5.68 (1.04) | 5.82 (0.78) | 0.22 | |
| FAP | 81.23 (8.783) | 85.15 (6.53) | 0.388 | 5.72 (0.64) | 5.99 (0.53) | 0.382 | 5.91 (0.99) | 6.10 (0.55) | 0.631 | |
| UriM | 81.76 (14.45) | 79.54 (13.513) | 0.304 | 5.79 (1.07) | 5.65 (1.01) | 0.459 | 6.07 (1.00) | 5.54 (1.26) | 0.011 * | |
| SED | 76.78 (15.44) | 79.97 (9.04) | 0.38 | 5.46 (0.99) | 5.58 (0.73) | 0.641 | 5.74 (1.38) | 5.81 (0.77) | 0.822 | |
| Comparison of Cohorts | “I currently have the tools to be resilient and maintain my mental health in medical school.” | “I would benefit from open discussion with fellow students about the emotional challenges of medical school.” | “Resiliency is a skill that can be taught.” | |||||||
| Mann–Whitney U | z | p | Mann–Whitney U | z | p | Mann–Whitney U | z | p | ||
| All students CO23 vs. CO24 | 15,299.5 | −0.85 | 0.395 | 13,755 | −2.46 | 0.014 * | 15,369 | −0.78 | 0.438 | |
| URiM vs. Non-URiM | Mann–Whitney U | z | p | |
|---|---|---|---|---|
| CO23 | Self-assuredness | 1769.5 | −1.54 | 0.123 |
| Drive | 1481 | −2.69 | 0.007 * | |
| CO24 | Self-assuredness | 2422 | −0.85 | 0.394 |
| Drive | 2658.5 | −0.02 | 0.984 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matari, Y.; Starkman, R.; Briskin, C.; Alper, D.P.; Petersen, K.K.; Yang, R.; Petersen, K.H. The Impact of COVID-19 and Racial Injustices on Resilience of Incoming Medical Students. Int. Med. Educ. 2024, 3, 78-91. https://doi.org/10.3390/ime3010007
Matari Y, Starkman R, Briskin C, Alper DP, Petersen KK, Yang R, Petersen KH. The Impact of COVID-19 and Racial Injustices on Resilience of Incoming Medical Students. International Medical Education. 2024; 3(1):78-91. https://doi.org/10.3390/ime3010007
Chicago/Turabian StyleMatari, Yanal, Rebecca Starkman, Camille Briskin, David P. Alper, Kellen K. Petersen, Rebecca Yang, and Kristina H. Petersen. 2024. "The Impact of COVID-19 and Racial Injustices on Resilience of Incoming Medical Students" International Medical Education 3, no. 1: 78-91. https://doi.org/10.3390/ime3010007