
Decline of Empathy among Healthcare Apprentices
{kind=link}
Abstract
:1. Introduction
2. Empathy
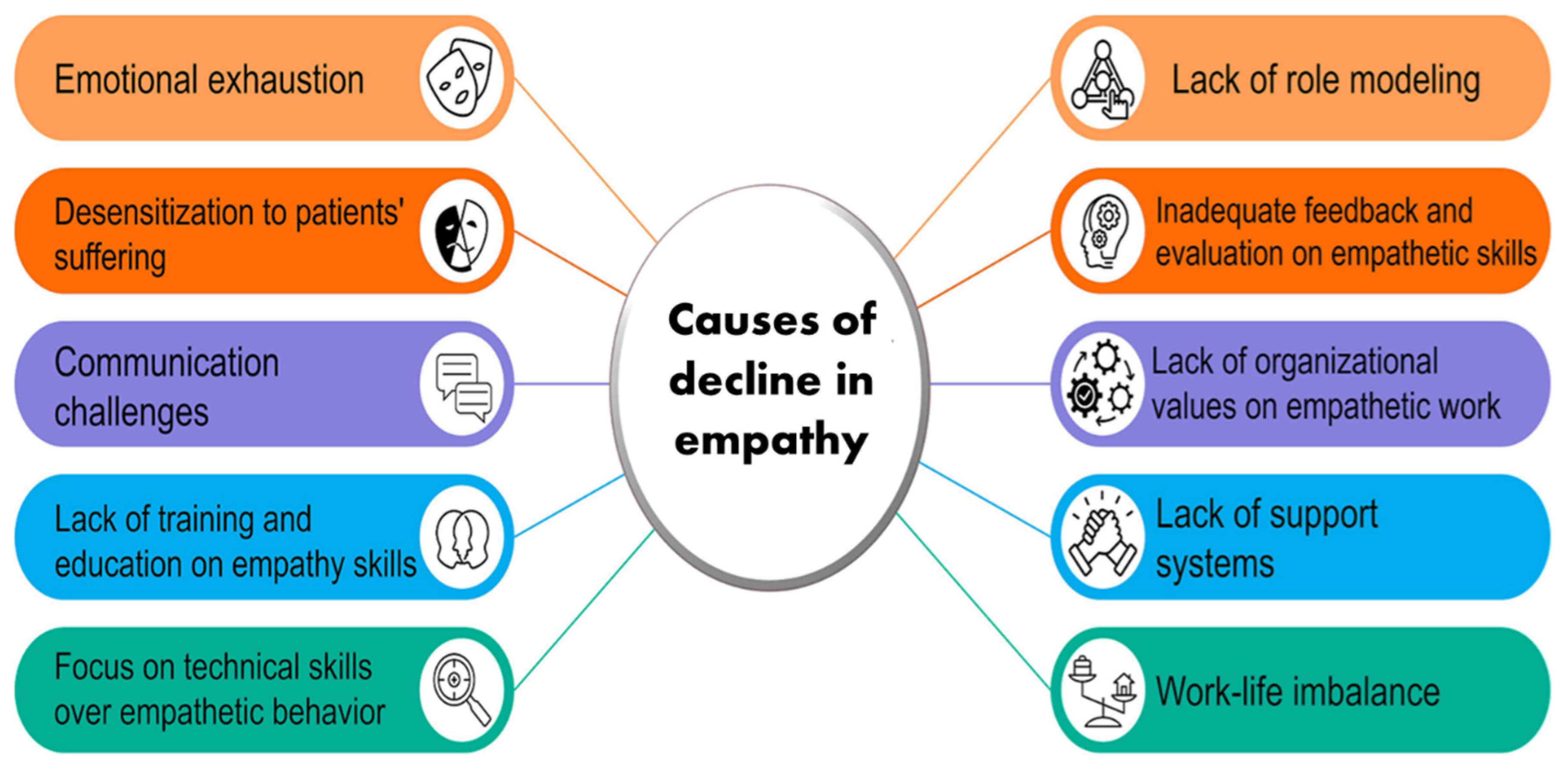
3. Decline of Empathy
- Medical student mistreatment ranges from humiliation to gender-specific discrimination and (sexual) harassment.
- Medical students and residents are vulnerable in facing the reality of life, including witnessing incurable illness and death of patients, to shift their attention to technology and objectivity.
- Lack of social support for the students and residents reduces contact with the families and peer groups.
- The high workload of the students and residents reduces sleeping time and inadequate recreation time.
4. Positive Impact of Empathy
5. Improving Empathy
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Riess, H. The Science of Empathy. J. Patient Exp. 2017, 4, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Roff, S. Reconsidering the “decline” of medical student empathy as reported in studies using the Jefferson Scale of Physician Empathy-Student version (JSPE-S). Med. Teach. 2015, 37, 783–786. [Google Scholar] [CrossRef]
- Derksen, F.; Bensing, J.; Lagro-Janssen, A. Effectiveness of empathy in general practice: A systematic review. Br. J. Gen. Pract. 2013, 63, e76–e84. [Google Scholar] [CrossRef] [PubMed]
- Halpern, J. What is clinical empathy? J. Gen. Intern. Med. 2003, 18, 670–674. [Google Scholar] [CrossRef] [PubMed]
- Decety, J.; Fotopoulou, A. Why empathy has a beneficial impact on others in medicine: Unifying theories. Front. Behav. Neurosci. 2014, 8, 457. [Google Scholar] [CrossRef]
- Singer, T.; Klimecki, O.M. Empathy and compassion. Curr. Biol. 2014, 24, R875–R878. [Google Scholar] [CrossRef]
- Guidi, C.; Traversa, C. Empathy in patient care: From ‘Clinical Empathy’ to ‘Empathic Concern’. Med. Health Care Philos. 2021, 24, 573–585. [Google Scholar] [CrossRef]
- Dohrenwend, A.M. Defining Empathy to Better Teach, Measure, and Understand Its Impact. Acad. Med. 2018, 93, 1754–1756. [Google Scholar] [CrossRef]
- Mercer, S.W.; Reynolds, W.J. Empathy and quality of care. Br. J. Gen. Pract. 2020, 52, S9–S12. [Google Scholar]
- Blatt, B.; LeLacheur, S.F.; Galinsky, A.D.; Simmens, S.J.; Greenberg, L. Does perspective-taking increase patient satisfaction in medical encounters? Acad. Med. 2010, 85, 1445–1452. [Google Scholar] [CrossRef]
- Neumann, M.; Edelhauser, F.; Tauschel, D.; Fischer, M.R.; Wirtz, M.; Woopen, C.; Haramati, A.; Scheffer, C. Empathy decline and its reasons: A systematic review of studies with medical students and residents. Acad. Med. 2011, 86, 996–1009. [Google Scholar] [CrossRef] [PubMed]
- Decety, J.; Yang, C.Y.; Cheng, Y. Physicians down-regulate their pain empathy response: An event-related brain potential study. Neuroimage 2010, 50, 1676–1682. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.; Hu, W.; Griffin, B. Cultures of Success: How elite students develop and realise aspirations to study Medicine. Aust. Educ. Res. 2020, 50, 1127–1147. [Google Scholar] [CrossRef]
- Howick, J.; Dudko, M.; Feng, S.N.; Ahmed, A.A.; Alluri, N.; Nockels, K.; Winter, R.; Holland, R. Why might medical student empathy change throughout medical school? a systematic review and thematic synthesis of qualitative studies. BMC Med. Educ. 2023, 23, 270. [Google Scholar] [CrossRef]
- Kim, S.S.; Kaplowitz, S.; Johnston, M.V. The effects of physician empathy on patient satisfaction and compliance. Eval. Health Prof. 2004, 27, 237–251. [Google Scholar] [CrossRef]
- Moudatsou, M.; Stavropoulou, A.; Philalithis, A.; Koukouli, S. The Role of Empathy in Health and Social Care Professionals. Healthcare 2020, 8, 26. [Google Scholar] [CrossRef]
- Del Canale, S.; Louis, D.Z.; Maio, V.; Wang, X.; Rossi, G.; Hojat, M.; Gonnella, J.S. The relationship between physician empathy and disease complications: An empirical study of primary care physicians and their diabetic patients in Parma, Italy. Acad. Med. 2012, 87, 1243–1249. [Google Scholar] [CrossRef]
- West, C.P.; Huschka, M.M.; Novotny, P.J.; Sloan, J.A.; Kolars, J.C.; Habermann, T.M.; Shanafelt, T.D. Association of Perceived Medical Errors With Resident Distress and EmpathyA Prospective Longitudinal Study. JAMA 2016, 296, 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- Howick, J.; Mittoo, S.; Abel, L.; Halpern, J.; Mercer, S.W. A price tag on clinical empathy? Factors influencing its cost-effectiveness. J. R. Soc. Med. 2020, 113, 389–393. [Google Scholar] [CrossRef]
- Wang, C.X.Y.; Pavlova, A.; Fernando, A.T., 3rd; Consedine, N.S. Beyond empathy decline: Do the barriers to compassion change across medical training? Adv. Health Sci. Educ. Theory Pract. 2022, 27, 521–536. [Google Scholar] [CrossRef]
- Yu, C.C.; Tan, L.; Le, M.K.; Tang, B.; Liaw, S.Y.; Tierney, T.; Ho, Y.Y.; Lim, B.E.E.; Lim, D.; Ng, R.; et al. The development of empathy in the healthcare setting: A qualitative approach. BMC Med. Educ. 2022, 22, 245. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Guo, H.; Xu, Z.; Xiao, H. Empathy variation of undergraduate medical students after early clinical contact: A cross-sectional study in China. BMJ Open 2020, 10, e035690. [Google Scholar] [CrossRef]
- Fragkos, K.C.; Crampton, P.E.S. The Effectiveness of Teaching Clinical Empathy to Medical Students: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Acad. Med. 2020, 95, 947–957. [Google Scholar] [CrossRef]
- Ardenghi, S.; Rampoldi, G.; Pepe, A.; Bani, M.; Salvarani, V.; Strepparava, M.G. An Exploratory Cross-Sectional Study on the Relationship between Dispositional Mindfulness and Empathy in Undergraduate Medical Students. Teach. Learn. Med. 2021, 33, 154–163. [Google Scholar] [CrossRef]
- da Silva, C.C.G.; Bolognani, C.V.; Amorim, F.F.; Imoto, A.M. Effectiveness of training programs based on mindfulness in reducing psychological distress and promoting well-being in medical students: A systematic review and meta-analysis. Syst. Rev. 2023, 12, 79. [Google Scholar] [CrossRef] [PubMed]
- Gleichgerrcht, E.; Decety, J. Empathy in clinical practice: How individual dispositions, gender, and experience moderate empathic concern, burnout, and emotional distress in physicians. PLoS ONE 2013, 8, e61526. [Google Scholar] [CrossRef] [PubMed]
- Decety, J.; Lamm, C. Human empathy through the lens of social neuroscience. Sci. World J. 2006, 6, 1146–1163. [Google Scholar] [CrossRef]
- Miller, E.; Balmer, D.; Hermann, N.; Graham, G.; Charon, R. Sounding narrative medicine: Studying students’ professional identity development at Columbia University College of Physicians and Surgeons. Acad. Med. 2014, 89, 335–342. [Google Scholar] [CrossRef]
- Pollak, K.I.; Arnold, R.; Alexander, S.C.; Jeffreys, A.S.; Olsen, M.K.; Abernethy, A.P.; Rodriguez, K.L.; Tulsky, J.A. Do patient attributes predict oncologist empathic responses and patient perceptions of empathy? Support. Care Cancer 2010, 18, 1405–1411. [Google Scholar] [CrossRef]
- Standford-Medicine. Standardized Patient Program. Available online: https://cisl.stanford.edu/standardized–patient–program.html (accessed on 13 September 2023).
- Weissman, S. Faculty empathy and the hidden curriculum. Acad. Med. 2012, 87, 389. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Razi, M.O.; Fouzia, R.; Razzaque, M.S. Decline of Empathy among Healthcare Apprentices. Int. Med. Educ. 2023, 2, 232-238. https://doi.org/10.3390/ime2040022
Razi MO, Fouzia R, Razzaque MS. Decline of Empathy among Healthcare Apprentices. International Medical Education. 2023; 2(4):232-238. https://doi.org/10.3390/ime2040022
Chicago/Turabian StyleRazi, Mohammed O., Rinat Fouzia, and Mohammed S. Razzaque. 2023. "Decline of Empathy among Healthcare Apprentices" International Medical Education 2, no. 4: 232-238. https://doi.org/10.3390/ime2040022