
Guidelines for the Diagnosis and Treatment of Parkinson’s Disease †



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
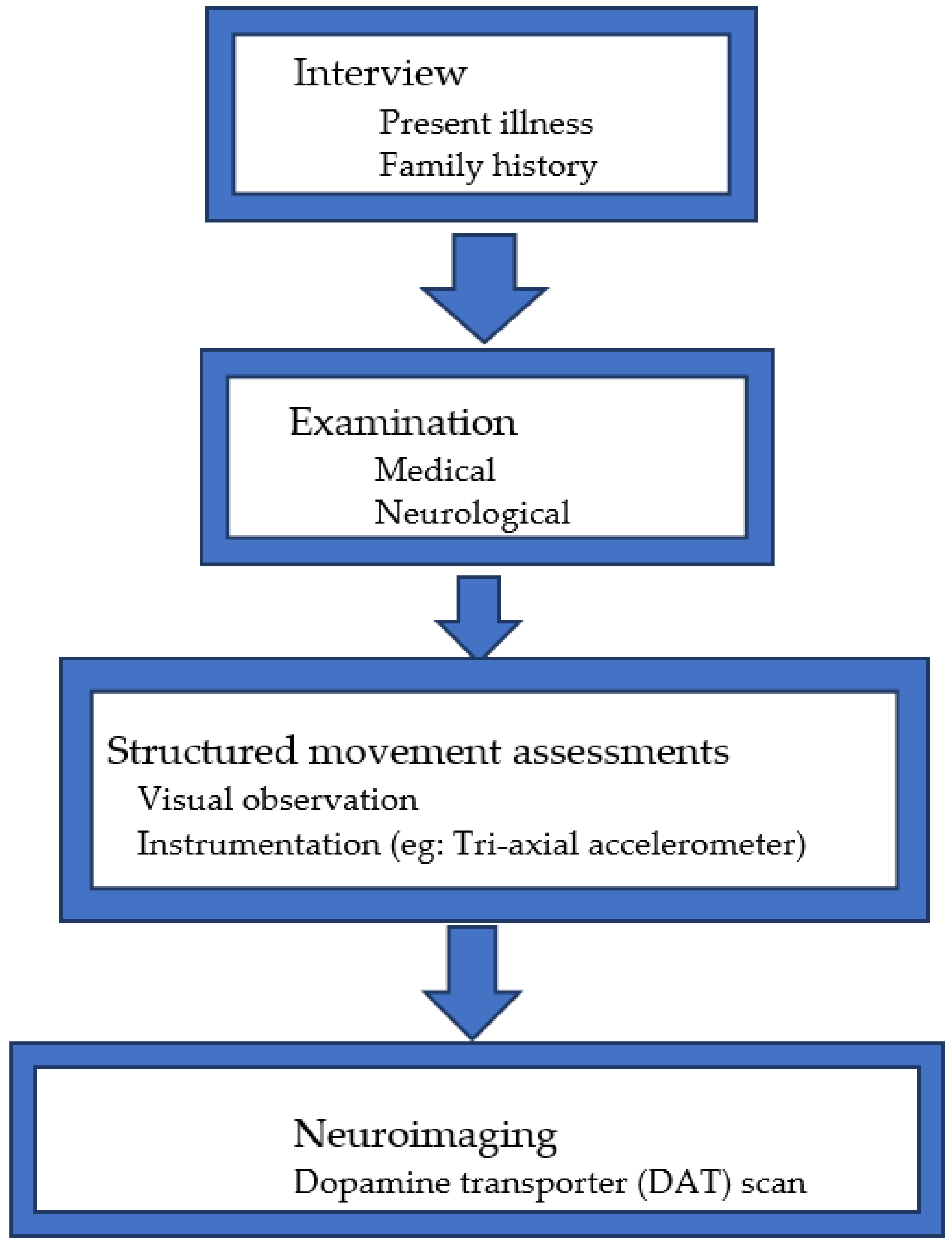
2. Methods
3. Results and Discussion
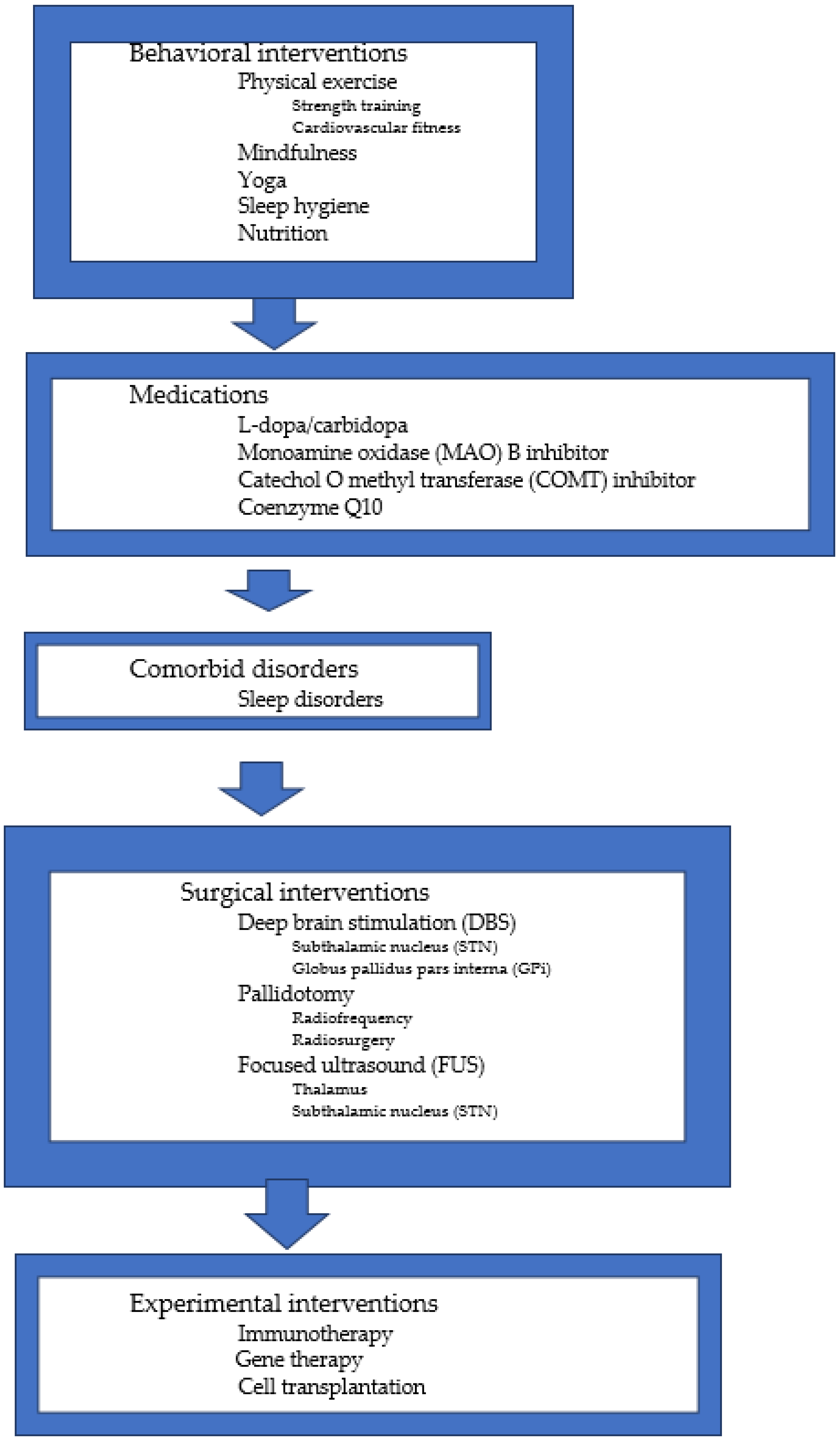
3.1. Behavioral Interventions
3.2. Nutrition
3.3. Medications
3.4. Comorbid Disorders
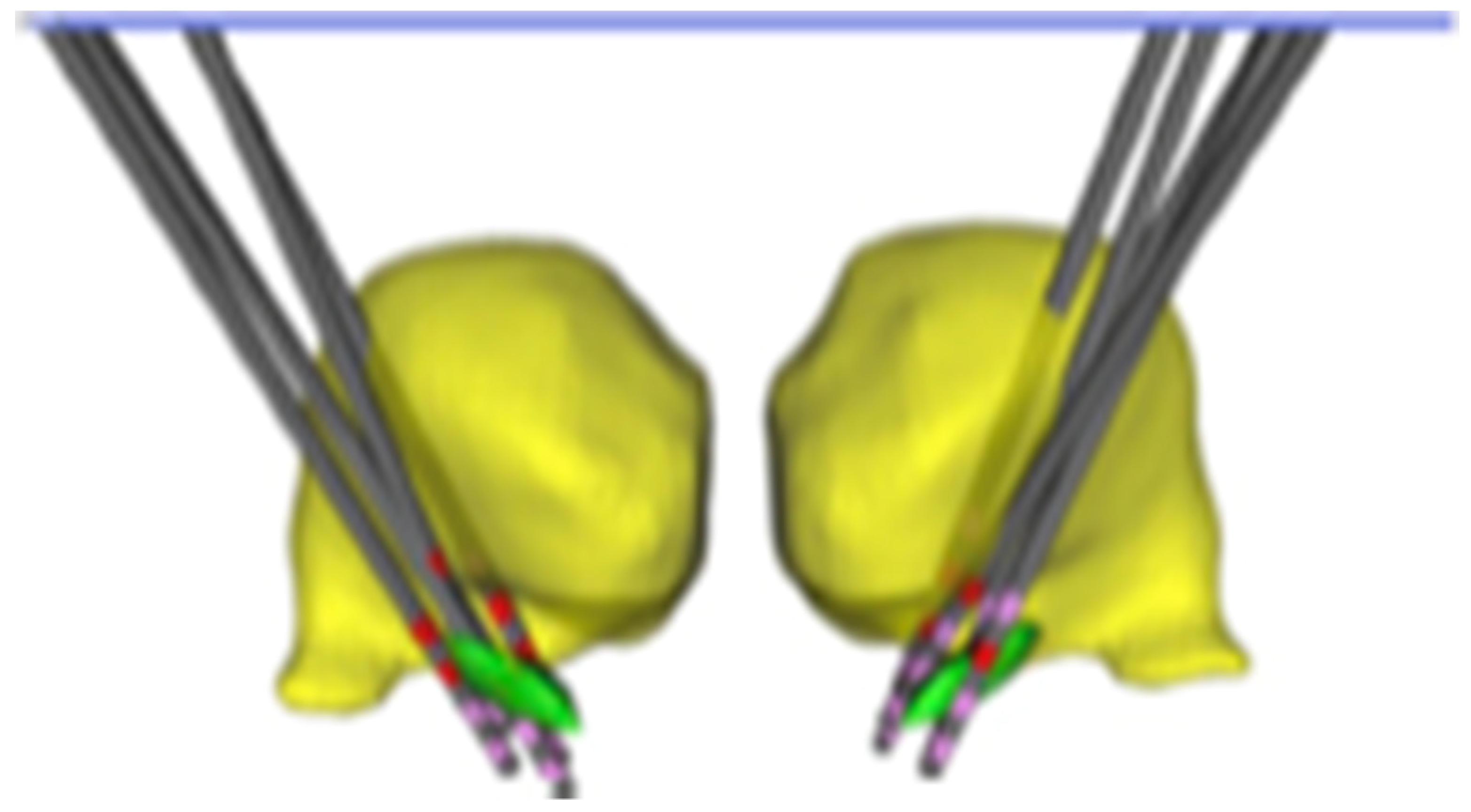
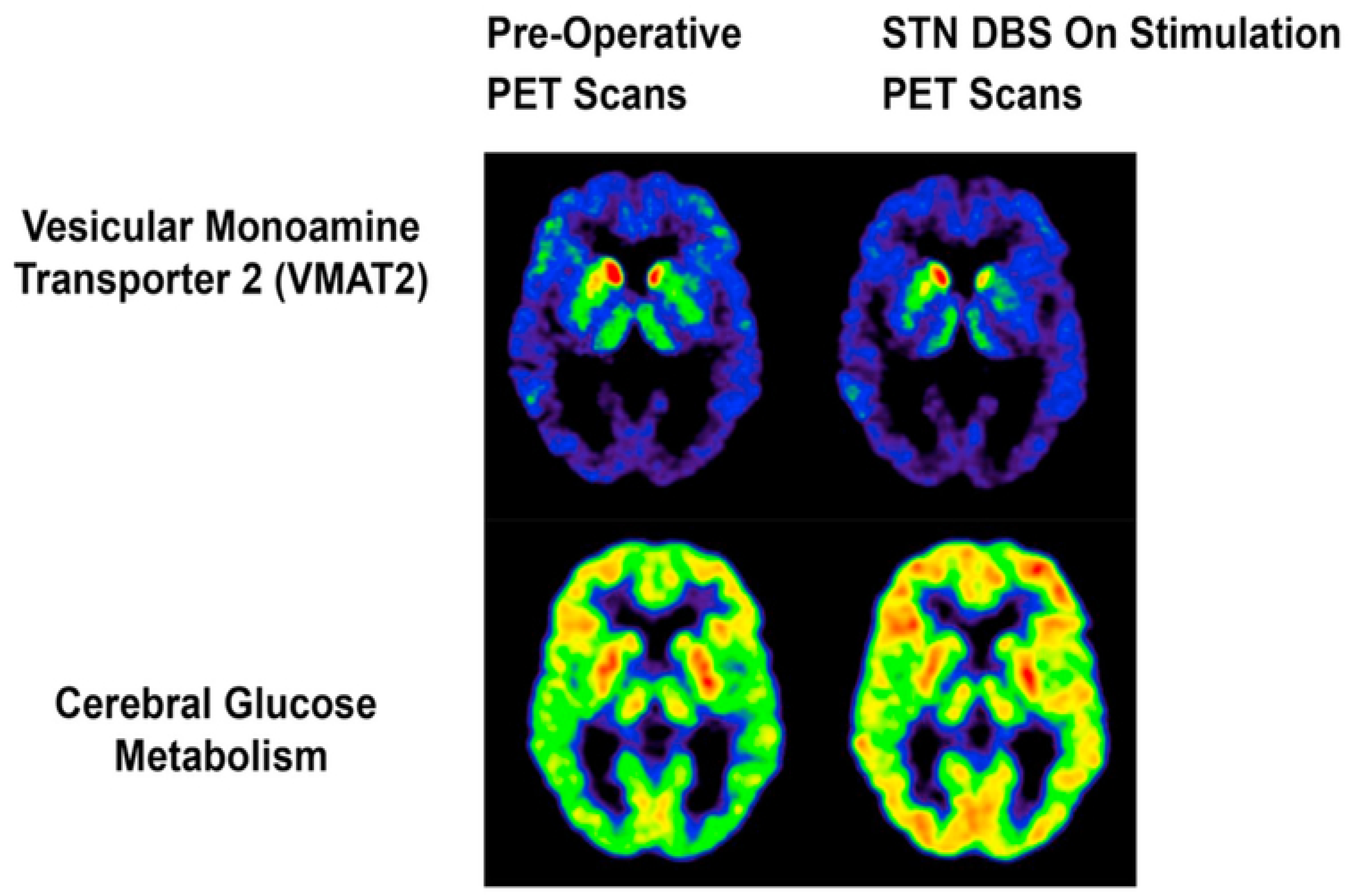
3.5. Surgical Interventions
3.6. Experimental Interventions
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Lau, L.M.L.; Breteler, M.M.B. Epidemiology of Parkinson’s disease. Lancet Neurol. 2006, 5, 525–535. [Google Scholar] [CrossRef]
- Parkinson Foundation, What Is Parkinson’s? 2022. Available online: http://www.parkinson.org/parkinson-s-disease/pd-101/what-is-parkinson-s-disease (accessed on 5 March 2022).
- Elshourbagy, T.; Syed, A.B.; Amer, M.A.M.; Brasic, J.R. Precision medicine to identify optimal diagnostic and therapeutic interventions for Parkinson’s Disease. Med. Sci. Discov. 2021, 8, 514–519. [Google Scholar] [CrossRef]
- Young, J.G.; Kaplan, D.; Pascualvaca, D.M.; Brasic, J.R. Psychiatric examination of the infant, child, and adolescent. In Comprehensive Textbook of Psychiatry/VI, 6th ed.; Kaplan, H.I., Sadock, B.J., Eds.; Williams & Wilkins: Baltimore, MD, USA, 1995; Volume 2, pp. 2169–2206. [Google Scholar]
- Brašić, J.R. Treatment of movement disorders in autism spectrum disorders. In Autism Spectrum Disorders; Hollander, E., Ed.; Medical Psychiatry Series; Marcel Dekker, Inc.: New York, NY, USA, 2003; Volume 24, ISBN 0-8247-0715-X. [Google Scholar]
- Brašić, J.R.; Mohamed, M. Human brain imaging of autism spectrum disorders. In Imaging of the Human Brain in Health and Disease; Seeman, P., Madras, B., Eds.; Academic Press, Elsevier Science: Oxford, UK, 2014; pp. 373–406. [Google Scholar]
- McKay, G.N.; Harrigan, T.P.; Brašić, J.R. Alow-cost quantitative continuous measurement of movements in the extremities of people with Parkinson’s disease. MethodsX 2019, 6, 169–189. [Google Scholar] [CrossRef] [PubMed]
- Oliveira de Carvalho, A.; Filho, A.S.S.; Murillo-Rodriguez, E.; Rocha, N.B.; Carta, M.G.; Machado, S. Physical exercise for Parkinson’s disease: Clinical and experimental evidence. Clin. Pract. Epidemiol. Ment. Health 2018, 14, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Mischley, L.K.; Lau, R.C.; Bennett, R.D. Role of diet and nutritional supplements in Parkinson’s disease progression. Oxid. Med. Cell. Longev. 2017, 2017, 6405278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeWitt, P.A. Levodopa therapy for Parkinson’s disease: Pharmacokinetics and pharmacodynamics. Mov. Disord. 2015, 30, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, D.M.; Goyal, V. Parkinson’s disease: A review. Neurol. India 2018, 66 (Suppl. S1), 26–35. [Google Scholar] [CrossRef]
- Prasuhn, J.; Brüggemann, N.; Hessler, N.; Berg, D.; Gasser, T.; Brockmann, K.; Olbrich, D.; Ziegler, A.; König, I.R.; Klein, C.; et al. An omics-based strategy using coenzyme Q10 in patients with Parkinson’s disease: Concept evaluation in a double-blind randomized placebo-controlled parallel group trial. Neurol. Res. Pract. 2019, 1, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefani, A.; Högl, B. Sleep in Parkinson’s disease. Neuropsychopharmacology 2020, 45, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.S.; Mills, K.A.; Pontone, G.M.; Anderson, W.S.; Perepezko, K.M.; Brasic, J.; Zhou, Y.; Brandt, J.; Butson, C.R.; Holt, D.P.; et al. Effect of STN DBS on vesicular monoamine transporter 2 and glucose metabolism in Parkinson’s disease. Parkinsonism Relat. Disord. 2019, 64, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.; Dallapiazza, R.F.; De Vloo, P.; Lozano, A.M. Current surgical treatments for Parkinson’s disease and potential therapeutic targets. Neural. Regen. Res. 2018, 13, 1342–1345. [Google Scholar] [CrossRef] [PubMed]
- Gendelman, H.E.; Zhang, Y.; Santamaria, P.; Olson, K.E.; Schutt, C.R.; Bhatti, D.; Shetty, B.L.D.; Lu, Y.; Estes, K.A.; Standaert, D.G.; et al. Evaluation of the safety and immunomodulatory effects of sargramostim in a randomized, double-blind phase 1 clinical Parkinson’s disease trial. NPJ Parkinson’s Dis. 2017, 3, 10. [Google Scholar] [CrossRef] [PubMed]
- Axelsen, T.M.; Woldbye, D.P.D. Gene therapy for Parkinson’s disease, an update. J. Parkinson’s Dis. 2018, 8, 195–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoddard-Bennett, T.; Pera, R.R. Stem cell therapy for Parkinson’s disease: Safety and modeling. Neural Regen. Res. 2020, 15, 36–40. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elshourbagy, T.; Brašić, J.R.; Syed, A.B. Guidelines for the Diagnosis and Treatment of Parkinson’s Disease. Biol. Life Sci. Forum 2021, 9, 9. https://doi.org/10.3390/ECCM-10859
Elshourbagy T, Brašić JR, Syed AB. Guidelines for the Diagnosis and Treatment of Parkinson’s Disease. Biology and Life Sciences Forum. 2021; 9(1):9. https://doi.org/10.3390/ECCM-10859
Chicago/Turabian StyleElshourbagy, Tarek, James Robert Brašić, and Alveena Batool Syed. 2021. "Guidelines for the Diagnosis and Treatment of Parkinson’s Disease" Biology and Life Sciences Forum 9, no. 1: 9. https://doi.org/10.3390/ECCM-10859