
Effectiveness of Pharmacist-Led Appropriate Antimicrobial Therapy through the Implementation of Daily Prospective Audit and Feedback and Educational Intervention †

Abstract
:1. Introduction
2. Methods
2.1. Study Setting
2.2. Daily Intervention to Optimize Antimicrobial Therapy
2.3. Educational Intervention for Promoting ASPs
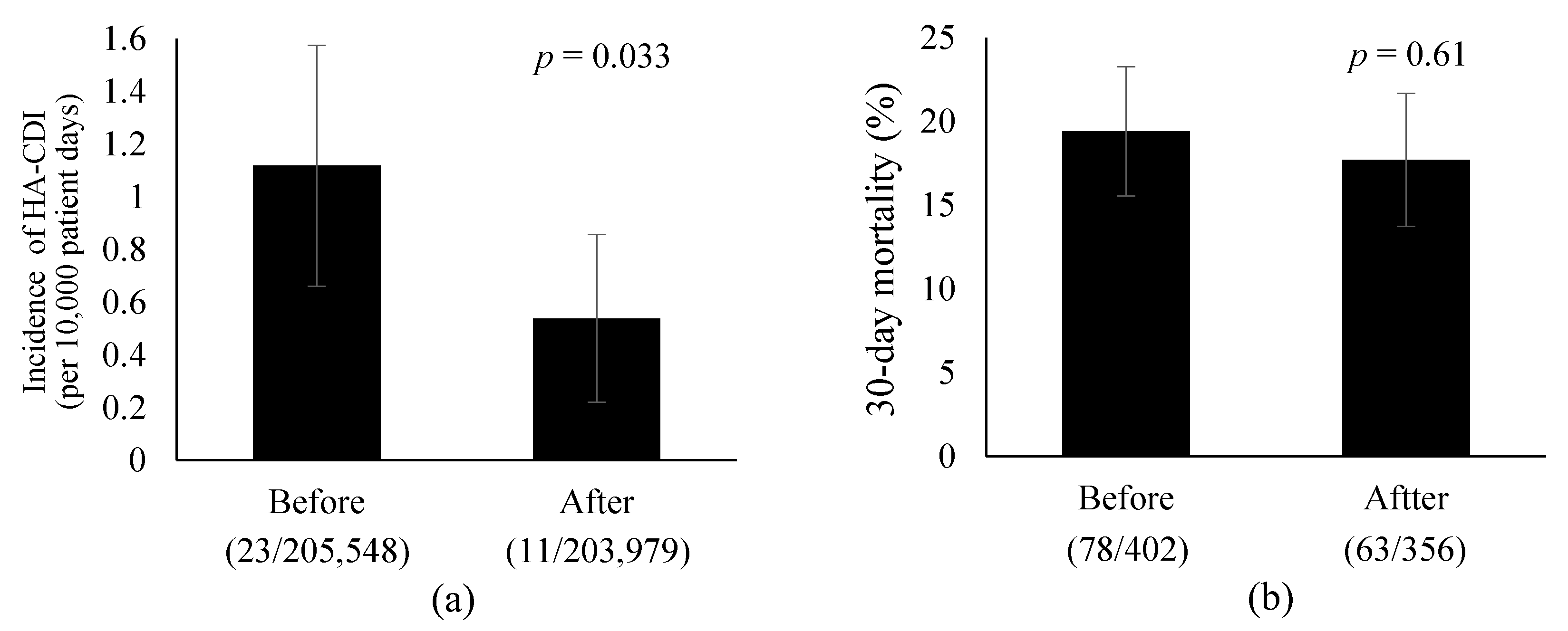
2.4. Outcomes
2.5. Statistical Analysis
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations/the Review on Antimicrobial Resistance Chaired by Jim O’Neill. Available online: https://wellcomecollection.org/works/rdpck35v (accessed on 6 April 2021).
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Kimura, T.; Uda, A.; Sakaue, T.; Yamashita, K.; Nishioka, T.; Nishimura, S.; Ebisawa, K.; Nagata, M.; Ohji, G.; Nakamura, T.; et al. Long-Term Efficacy of Comprehensive Multidisciplinary Antibiotic Stewardship Programs Centered on Weekly Prospective Audit and Feedback. Infection 2018, 46, 215–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanbeck, P.; Ragnarson Tennvall, G.; Resman, F. A Cost Analysis of Introducing an Infectious Disease Specialist-Guided Antimicrobial Stewardship in an Area with Relatively Low Prevalence of Antimicrobial Resistance. BMC Health Serv. Res. 2016, 16, 311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uda, A.; Shigemura, K.; Kitagawa, K.; Osawa, K.; Onuma, K.; Inoue, S.; Kotani, J.; Yan, Y.; Nakano, Y.; Nishioka, T.; et al. How Does Antimicrobial Stewardship Affect Inappropriate Antibiotic Therapy in Urological Patients? Antibiotics 2020, 9, 63. [Google Scholar] [CrossRef] [Green Version]
- Uda, A.; Kimura, T.; Izuta, R.; Kusuki, M.; Nishioka, T.; Yahata, M.; Yano, I.; Miyara, T. Effects of Intervention by a Pharmacist in the Antimicrobial Stewardship Team on Appropriate Antimicrobial Use. Jpn. J. Pharm. Health Care Sci. 2019, 45, 460–469. (In Japanese) [Google Scholar] [CrossRef]
- Medical Information Network Distribution Service. Available online: https://minds.jcqhc.or.jp/english (accessed on 5 January 2022).
- Johns Hopkins ABX Guide. Available online: https://www.hopkinsguides.com/hopkins (accessed on 5 January 2022).
- Sunford Guide. Available online: https://www.sanfordguide.com/ (accessed on 5 January 2022).
- UpToDate. Available online: https://www.uptodate.com/contents/search (accessed on 5 January 2022).
- Webb, B.J.; Subramanian, A.; Lopansri, B.; Goodman, B.; Jones, P.B.; Ferraro, J.; Stenehjem, E.; Brown, S.M. Antibiotic Exposure and Risk for Hospital-Associated Clostridioides Difficile Infection. Antimicrob. Agents Chemother. 2020, 64, e02169-19. [Google Scholar] [CrossRef] [PubMed]
- Louh, I.K.; Greendyke, W.G.; Hermann, E.A.; Davidson, K.W.; Falzon, L.; Vawdrey, D.K.; Shaffer, J.A.; Calfee, D.P.; Furuya, E.Y.; Ting, H.H. Clostridium Difficile Infection in Acute Care Hospitals: Systematic Review and Best Practices for Prevention. Infect. Control Hosp. Epidemiol 2017, 38, 476–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, T.V.; Kimura, T. The Epidemiology of Clostridium Difficile Infection in Japan: A Systematic Review. Infect. Dis. Ther. 2018, 7, 39–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, M.P.; Notermans, D.W.; van Benthem, B.H.; Brazier, J.S.; Wilcox, M.H.; Rupnik, M.; Monnet, D.L.; van Dissel, J.T.; Kuijper, E.J. Clostridium Difficile Infection in Europe: A Hospital-Based Survey. Lancet 2011, 377, 63–73. [Google Scholar] [CrossRef]
- Davies, K.A.; Longshaw, C.M.; Davis, G.L.; Bouza, E.; Barbut, F.; Barna, Z.; Delmée, M.; Fitzpatrick, F.; Ivanova, K.; Kuijper, E.; et al. Underdiagnosis of Clostridium Difficile across Europe: The European, Multicentre, Prospective, Biannual, Point-Prevalence Study of Clostridium Difficile Infection in Hospitalised Patients with Diarrhoea (EUCLID). Lancet Infect. Dis. 2014, 14, 1208–1219. [Google Scholar] [CrossRef]
- Vital Signs: Preventing Clostridium Difficile Infections. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6109a3.htm (accessed on 17 December 2020).
- Uda, A.; Kimura, T.; Nishimura, S.; Ebisawa, K.; Ohji, G.; Kusuki, M.; Yahata, M.; Izuta, R.; Sakaue, T.; Nakamura, T.; et al. Efficacy of Educational Intervention on Reducing the Inappropriate Use of Oral Third-Generation Cephalosporins. Infection 2019, 47, 1037–1045. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Classes | Antibiotics (ATC Codes) |
|---|---|
| Antipseudomonal agents | |
| Antipseudomonal penicillins | Piperacillin (J01CA12) and piperacillin/tazobactam (J01CR05) |
| Antipseudomonal third generation cephalosporins | Ceftazidime (J01DD02) |
| Antipseudomonal fourth generation cephalosporins | Cefepime (J01DE01) and cefozopran (J01DE03) |
| Monobactams | Aztreonam (J01DF01) |
| Carbapenems | Meropenem (J01DH02) and doripenem (J01DH04) |
| Fluoroquinolones | Ciprofloxacin (J01MA02), levofloxacin (J01MA12), and pazufloxacin (J01MA18) |
| Aminoglycosides | Amikacin (J01GB06), tobramycin (J01GB01), and gentamicin (J01GB03) |
| Polymyxins | Colistin (J01XB01) |
| Anti-MRSA agents | Vancomycin (J01XA01), teicoplanin (J01XA02), daptomycin (J01XX09), and linezolid (J01XX08) |
| Before Intervention | After Intervention | p | |
|---|---|---|---|
| Blood culture collections before each antibiotic, n (%) | |||
| Broad-spectrum antibiotics (Antipseudomonal agents and anti-MRSA agents) | 562/792 (71) | 578/707 (82) | <0.001 |
| Antipseudomonal agents | 539/758 (71) | 563/681 (83) | <0.001 |
| Anti-MRSA agents | 76/95 (80) | 66/83 (80) | 1 |
| Antimicrobial de-escalation therapy, n (%) | |||
| Broad-spectrum antibiotics (Antipseudomonal agents and anti-MRSA agents) | 36/66 (55) | 67/86 (78) | 0.004 |
| Antipseudomonal agents | 33/61 (54) | 62/81 (77) | 0.008 |
| Anti-MRSA agents | 7/12 (58) | 16/16 (100) | 0.019 |
| Before Intervention | After Intervention | p | |
|---|---|---|---|
| Broad-spectrum antibiotics (Antipseudomonal agents and anti-MRSA agents) | 68.9 (65.7–77.7) | 65.2 (54.2–66.1) | 0.11 |
| Antipseudomonal agents | 50.5 (47.5–55.4) | 41.8 (37.0–45.8) | 0.01 |
| Anti-MRSA agents | 19.4 (17.3–21.5) | 20.3 (17.7–22.4) | 0.88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uda, A.; Kimura, T.; Kusuki, M.; Izuta, R.; Yahata, M.; Yano, I.; Miyara, T. Effectiveness of Pharmacist-Led Appropriate Antimicrobial Therapy through the Implementation of Daily Prospective Audit and Feedback and Educational Intervention. Biol. Life Sci. Forum 2021, 9, 12. https://doi.org/10.3390/ECCM-10862
Uda A, Kimura T, Kusuki M, Izuta R, Yahata M, Yano I, Miyara T. Effectiveness of Pharmacist-Led Appropriate Antimicrobial Therapy through the Implementation of Daily Prospective Audit and Feedback and Educational Intervention. Biology and Life Sciences Forum. 2021; 9(1):12. https://doi.org/10.3390/ECCM-10862
Chicago/Turabian StyleUda, Atsushi, Takeshi Kimura, Mari Kusuki, Rie Izuta, Mariko Yahata, Ikuko Yano, and Takayuki Miyara. 2021. "Effectiveness of Pharmacist-Led Appropriate Antimicrobial Therapy through the Implementation of Daily Prospective Audit and Feedback and Educational Intervention" Biology and Life Sciences Forum 9, no. 1: 12. https://doi.org/10.3390/ECCM-10862