
Food-Based Intervention Strategies for Iron Deficiency Prevention †



{kind=link}
Abstract
:1. Introduction
- initially, a mild form occurs due to low iron diets or excessive bleeding;
- its further progress is associated with a stage of more severe depletion of iron reserves in the body and a decrease in the number of red blood cells;
- ultimately all this leads to IDA, a condition characterized by depleted iron reserves and a significant loss of total red blood cells.
2. Statistical Data of Iron Deficiency
- the prevalence of anemia among the world’s population of all ages was 22.8%, which is on a downward trend, taking into account the 27.0% in 1990;
- as the prevalence of the disease has declined, the total number of cases of anemia has increased from 1.42 billion in 1990 to 1.74 billion in 2019;
- the population most susceptible to anemia is children under the age of five;
- according to the severity of the course of the disease, the following distribution was obtained: 54.1% of cases of anemia were mild, 42.5%—moderate, and 3.4%—severe;
- in 2019, anemia was responsible for 58.6 million DALYs.
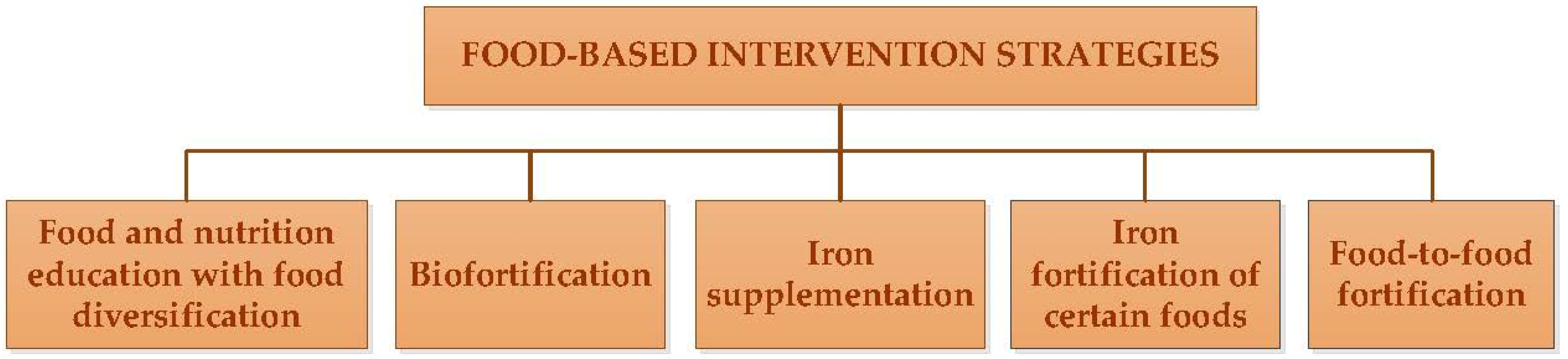
3. Iron Deficiency Medical Condition and Its Prevention Strategies
3.1. Food and Nutrition Education with Food Diversification
3.2. Biofortification
3.3. Iron Suplementions
- provides the ability to consume the optimal amount of a specific one or more nutrients in a highly absorbable form,
- the fastest way to control deficiency in individuals or populations [13].
3.4. Iron Fortification of Certain Foods
3.5. Food-to-Food Fortification
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Camaschella, C. New Insights into Iron Deficiency and Iron Deficiency Anemia. Blood Rev. 2017, 31, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.-R.; Drakesmith, H.; Black, J.; Hipgrave, D.; Biggs, B.-A. Control of Iron Deficiency Anemia in Low- and Middle-Income Countries. Blood 2013, 121, 2607–2617. [Google Scholar] [CrossRef] [PubMed]
- Barragán-Ibañez, G.; Santoyo-Sánchez, A.; Ramos-Peñafiel, C.O. Iron Deficiency Anaemia. Rev. Médica. Del. Hosp. Gen. México 2016, 79, 88–97. [Google Scholar] [CrossRef]
- Lozoff, B.; Smith, J.B.; Kaciroti, N.; Clark, K.M.; Guevara, S.; Jimenez, E. Functional Significance of Early-Life Iron Deficiency: Outcomes at 25 Years. J. Pediatr. 2013, 163, 1260–1266. [Google Scholar] [CrossRef] [PubMed]
- Powers, J.M.; Buchanan, G.R. Disorders of Iron Metabolism. Hematol. Oncol. Clin. N. Am. 2019, 33, 393–408. [Google Scholar] [CrossRef]
- Pasricha, S.-R.; Tye-Din, J.; Muckenthaler, M.U.; Swinkels, D.W. Iron Deficiency. Lancet 2021, 397, 233–248. [Google Scholar] [CrossRef]
- Lopez, A.; Cacoub, P.; Macdougall, I.C.; Peyrin-Biroulet, L. Iron Deficiency Anaemia. Lancet 2016, 387, 907–916. [Google Scholar] [CrossRef]
- Bouri, S.; Martin, J. Investigation of Iron Deficiency Anaemia. Clin. Med. J. R. Coll. Physicians Lond. 2018, 18, 242–244. [Google Scholar] [CrossRef]
- Osendarp, S.J.M.; Eilander, A. Iron Deficiency and Cognitive Development. In Lifetime Nutritional Influences on Cognition, Behaviour and Psychiatric Illness; Benton, D., Ed.; Woodhead Publishing: Sawston, UK, 2011. [Google Scholar] [CrossRef]
- Tao, Z.; Xu, J.; Chen, W.; Yang, Z.; Xu, X.; Liu, L.; Chen, R.; Xie, J.; Liu, M.; Wu, J.; et al. Anemia Is Associated with Severe Illness in COVID-19: A Retrospective Cohort Study. J. Med. Virol. 2021, 93, 1478–1488. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Kurniawan, A. Anemia Is Associated with Severe Coronavirus Disease 2019 (COVID-19) Infection. Transfus. Apher. Sci. 2020, 59, 102926. [Google Scholar] [CrossRef]
- WHO. The Global Prevalence of Anaemia in 2011; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Allen, L.; de Benoist, B.; Dary, O.; Hurrell, R. Guidelines on Food Fortification with Micronutrients; Allen, L., de Benoist, B., Dary, O., Hurrell, R., Eds.; World Health Organization and Food and Agriculture Organization of the United Nations: Geneva, Switzerland, 2006. [Google Scholar]
- Gardner, W.; Kassebaum, N. Global, Regional, and National Prevalence of Anemia and Its Causes in 204 Countries and Territories, 1990–2019. Curr. Dev. Nutr. 2020, 4 (Suppl. S2), 830. [Google Scholar] [CrossRef]
- FAO/WHO. Human Vitamin and Mineral Requirements: Report of a Joint FAO/WHO Expert Consultation; Food and Nutrition Division FAO: Bangkok, Thailand, 2001. [Google Scholar]
- Abbaspour, N.; Hurrell, R.; Kelishadi, R. Review on Iron and Its Importance for Human Health. J. Res. Med. Sci. 2014, 19, 164–174. [Google Scholar] [PubMed]
- Pasricha, S.R.; Drakesmith, H. Iron Deficiency Anemia: Problems in Diagnosis and Prevention at the Population Level. Hematol. Oncol. Clin. N. Am. 2016, 30, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Kruger, J.; Taylor, J.R.N.; Ferruzzi, M.G.; Debelo, H. What Is Food-to-food Fortification? A Working Definition and Framework for Evaluation of Efficiency and Implementation of Best Practices. Compr. Rev. Food Sci. Food Saf. 2020, 19, 3618–3658. [Google Scholar] [CrossRef]
- Kiran, K. Advanced Approaches for Biofortification. In Advances in Agri-Food Biotechnology; Springer: Singapore, 2020; pp. 29–55. [Google Scholar] [CrossRef]
- Liberal, Â.; Pinela, J.; Vívar-Quintana, A.M.; Ferreira, I.C.F.R.; Barros, L. Fighting Iron-Deficiency Anemia: Innovations in Food Fortificants and Biofortification Strategies. Foods 2020, 9, 1871. [Google Scholar] [CrossRef]
- Olson, R.; Gavin-Smith, B.; Ferraboschi, C.; Kraemer, K. Food Fortification: The Advantages, Disadvantages and Lessons from Sight and Life Programs. Nutrients 2021, 13, 1118. [Google Scholar] [CrossRef]
- The National Academies of Sciences, Engineering, and Medicine. Iron. In Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press: Washington, DC, USA, 2001. [Google Scholar] [CrossRef]
- Hurrell, R.F. Efficacy and Safety of Iron Fortification. In Food Fortification in a Globalized World; Elsevier: Amsterdam, The Netherlands, 2018; pp. 195–212. [Google Scholar] [CrossRef]
- Mehansho, H. Iron Fortification Technology Development: New Approaches. J. Nutr. 2006, 136, 1059–1063. [Google Scholar] [CrossRef]
- Evlash, V.; Pogozhikh, M.; Aksonova, O.; Gubsky, S. Heme Iron–Containing Dietary Supplements and Their Application in Fortified Foods. In Bioenhancement and Fortification of Foods for a Healthy Diet; Paredes-López, O., Shevchenko, O., Stabnikov, V., Ivanov, V., Eds.; CRC Press: Boca Raton, FL, USA, 2022; pp. 237–268. [Google Scholar] [CrossRef]
- Polo, J.; Rodríguez, C. Heme Iron as Source of Iron in Food Fortification. In Handbook of Food Fortification and Health; Preedy, V.R., Srirajaskanthan, R., Patel, V.B., Eds.; Springer: New York, NY, USA, 2013; Volume 1, pp. 133–146. [Google Scholar] [CrossRef]
- Blanco-Rojo, R.; Vaquero, M.P. Iron Bioavailability from Food Fortification to Precision Nutrition. A Review. Innov. Food Sci. Emerg. Technol. 2019, 51, 126–138. [Google Scholar] [CrossRef]
- Mannar, M.G.V.; van Ameringen, M. Role of Public-Private Partnership in Micronutrient Food Fortification. Food Nutr. Bull. 2003, 24 (Suppl. S2), S151–S154. [Google Scholar] [CrossRef]
- Baltussen, R.; Knai, C.; Sharan, M. Iron Fortification and Iron Supplementation Are Cost-Effective Interventions to Reduce Iron Deficiency in Four Subregions of the World. J. Nutr. 2004, 134, 2678–2684. [Google Scholar] [CrossRef]
- Martínez-Navarrete, N.; Camacho, M.M.; Martínez-Lahuerta, J.; Martínez-Monzó, J.; Fito, P. Iron Deficiency and Iron Fortified Foods—A Review. Food Res. Int. 2002, 35, 225–231. [Google Scholar] [CrossRef]
- Huma, N.; Salim-Ur-Rehman; Anjum, F.M.; Murtaza, M.A.; Sheikh, M.A. Food Fortification Strategy—Preventing Iron Deficiency Anemia: A Review. Crit. Rev. Food Sci. Nutr. 2007, 47, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Derbyshire, E.; Brennan, C.S.; Li, W.; Bokhari, F. Iron Deficiency—Is There a Role for the Food Industry? Int. J. Food Sci. Technol. 2010, 45, 2443–2448. [Google Scholar] [CrossRef]
- Hurrell, R.F.; Cook, J.D. Strategies for Iron Fortification of Foods. Trends Food Sci. Technol. 1990, 1, 56–61. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evlash, V.; Aksonova, O.; Gubsky, S. Food-Based Intervention Strategies for Iron Deficiency Prevention. Biol. Life Sci. Forum 2022, 18, 52. https://doi.org/10.3390/Foods2022-12962
Evlash V, Aksonova O, Gubsky S. Food-Based Intervention Strategies for Iron Deficiency Prevention. Biology and Life Sciences Forum. 2022; 18(1):52. https://doi.org/10.3390/Foods2022-12962
Chicago/Turabian StyleEvlash, Victoria, Olena Aksonova, and Sergey Gubsky. 2022. "Food-Based Intervention Strategies for Iron Deficiency Prevention" Biology and Life Sciences Forum 18, no. 1: 52. https://doi.org/10.3390/Foods2022-12962